-
8/12/2019 ACR Safety Guidelines 2004
1/24
ACR WHITE PAPER ON MAGNETIC RESONANCE (MR) SAFETYCombined Papers
of 2002 and 2004
INTRODUCTION
There are potential risks in the MR environment, not only for
the patient,1,2but also for the accompanying
family members, attending health care professionals, and others
who find themselves only occasionally or
rarely in the magnetic fields of MR scanners, such as security
or housekeeping personnel, firefighters,
police, etc. There have been reports in the medical literature
and print media detailing MRI adverse
incidents involving patients, equipment, and personnel that
spotlighted the need for a safety review by anexpert panel. The
following is the combined paper of 2 reports3,4issued by the
American College of
Radiology Blue Ribbon Panel on MR Safety, chaired by Emanuel
Kanal, MD, FACR. The panel
originally met in November 2001 and was charged with reviewing
the existing MR safe practices and
guidelines5-9and issuing new ones as appropriate for MR
examinations. The panel consisted of thefollowing members: A. James
Barkovich, MD, Charlotte Bell, MD (Anesthesia Patient Safety
Foundation), James P. Borgstede, MD, FACR, William G. Bradley,
MD, PhD, FACR, Joel Felmlee, PhD,
Jerry W. Froelich, MD, Ellisa M. Kaminski, RT(R)(MR), Emanuel
Kanal, MD, FACR, Elaine K. Keeler,
PhD (NEMA), James W. Lester, MD, Elizabeth Scoumis, RN, BSN,
Loren A. Zaremba, PhD (FDA),
Jeffrey Hayden (ACR staff), and Marie D. Zinninger (ACR staff).
Upon Dr Keelers retirement, Shawn
Etheridge was appointed to represent NEMA.
After reviewing substantial feedback from the field and
installed base, as well as changes that had
transpired throughout the MR industry in the interim, the panel
reconvened in 2002 and 2003 and agreed
to several modifications and updates to the original
document.
The following MR safe practice guidelines document, which
incorporates both prior papers, is intended to
be used as template for MR facilities to follow in the
development of an MR safety program. These MR
safe practice guidelines were developed to help guide MR
practitioners regarding these issues and to
provide a basis for them to develop and implement their own MR
policies and practices. It is intended that
these MR safe practice guidelines (and the policies and
procedures to which they give rise) be reviewed
and updated on a regular basis as the field of MR safety
continues to evolve.
This white paper does not attempt to deal with all aspects of MR
safety, but rather those that apply to an
already installed, active site, whether a clinical or research
facility. With the increasing advent and use of
3.0-T and higher strength magnets, users need to recognize that
one should never assume MR
compatibility or safety information about a device if it is not
clearly documented in writing. Decisions
based on published MR safety and compatibility claims should
recognize that all such claims apply only
to specifically tested conditions, such as static magnetic field
strengths, static gradient magnetic field
strengths and spatial distributions, and the strengths and rates
of change of gradient and radiofrequency
(RF) magnetic fields.
Finally, there is a whole host of other issues that should be
considered during the site-planning stages andthat is not dealt
with in this manuscript. These include, among many others, cryogen
emergency vent
locations and pathways, 5-G linesiting considerations, patient
access pathways, and considerations
regarding fringe field blooming that may result in the event
there is a failure of an actively shielded MRI
system. These issues, and many others, should be reviewed with
those experienced in MR site planning
and familiar with the patient safety and patient flow
considerations prior to committing construction to a
specific site design. In this regard, enlisting the assistance
of an architectural firm experienced in thisarea, and doing so
early in the design stages of the planning process, may prove most
valuable.
It remains the intent of the ACR that these MR safe practice
guidelines will prove helpful as the field of
MRI continues to evolve and mature, providing MR services that
are among the most powerful, yet safest,
of all diagnostic procedures to be developed in the history of
modern medicine.
1
-
8/12/2019 ACR Safety Guidelines 2004
2/24
ACR WHITE PAPER ON MAGNETIC RESONANCE (MR) SAFETYCombined Papers
of 2002 and 2004
ACR Magnetic Resonance Safe Practice Guidelines
Combined Papers of 2002 and 2004
A. Establish, Implement, and Maintain Current MR Safety Policies
and Procedures
1. All clinical and research MR sites should maintain MR safety
policies and procedures, which areto be established, implemented,
maintained, and routinely reviewed and updated, as appropriate.
The level of compliance by staff will be assessed and documented
annually. The policies and
procedures manual should be readily available to the MR
professionals on site at all times of
operation.
2. These policies and procedures should also be reviewed
concurrently with the introduction of any
significant changes in the safety parameters of the MR
environment of the site (eg, adding faster
or stronger gradient capabilities or higher RF duty cycle
studies) and updated as needed. In this
review process, national and international standards and
recommendations should be taken into
consideration prior to establishing local guidelines, policies,
and procedures.
3. Each site will name an MR medical director whose
responsibilities will include ensuring that
these MR safe practice guidelines are established and maintained
as current and appropriate forthe site. It is the responsibility of
the sites administration to ensure that the policies and
procedures that result from these MR safe practice guidelines
are implemented and adhered to at
all times by all of the sites personnel.
4. Procedures should be in place to ensure that any and all
adverse events, MR safety incidents, or
near incidents that occur in the MR site are reported to the
medical director in a timely fashion
(eg, within 24 hours, or 1 business day, of their occurrence)
and are used in continuous quality
improvement efforts.
B. Static Magnetic Field Issues: Site Access Restriction
1. Zoning:
The MR site is conceptually divided into 4 zones (see Figure 1
and Appendix 1):
a. Zone I: This region includes all areas that are freely
accessible to the general public. This area
is typically outside the MR environment itself and is the area
through which patients, health
care personnel, and other employees of the MR site access the MR
environment.
b. Zone II: This area is the interface between the publicly
accessible, uncontrolled Zone I and
the strictly controlled Zones III and IV. Typically, patients
are greeted in Zone II and are not
free to move throughout Zone II at will, but rather are under
the supervision of MR personnel
(see section B.2.b, below). It is in Zone II that the answers to
MR-screening questions, patient
histories, medical insurance questions, etc are typically
obtained.
c. Zone III: This area is the region in which free access by
unscreened non-MR personnel or
ferromagnetic objects or equipment can result in serious injury
or death as a result ofinteractions between the individuals or
equipment and the MR scanners particular
environment. These interactions include, but are not limited to,
those involving the MR
scanners static and time-varying magnetic fields. All access to
Zone III is to be strictly
restricted, with access to regions within it (including Zone IV,
see below) controlled by, and
entirely under the supervision of, MR personnel (see section
B.2.b, below). Specifically
identified MR personnel (typicallybut not necessarily onlythe MR
technologists) are to
be charged with ensuring that this MR safe practice guideline is
strictly adhered to for the
safety of the patients and other non-MR personnel, the health
care personnel, and the
2
-
8/12/2019 ACR Safety Guidelines 2004
3/24
ACR WHITE PAPER ON MAGNETIC RESONANCE (MR) SAFETYCombined Papers
of 2002 and 2004
equipment itself. This function of the MR personnel is directly
under the authority and
responsibility of the MR medical director or the level
2designated (see section B.2.b, below)
physician of the day for the MR site.
Zone III should be physically restricted from general public
access by, for example, key
locks, passkey locking systems, or any other reliable,
physically restricting method that can
differentiate between MR personnel and non-MR personnel. The use
of combination locks isdiscouraged as combinations often become
more widely distributed than initially intended,
resulting in site restriction violations being more likely with
these devices. Only MR
personnel shall be provided free access, such as the access keys
or passkeys, to Zone III.
There should be noexceptions to this guideline. Specifically,
this includes hospital or site
administration, physician, security, and other non-MR personnel
(see section B.2.c, below).
Non-MR personnel are not to be provided with independent Zone
III access until such time as
they undergo the proper education and training to become MR
personnel themselves. Zone
III, or at the very least the area within it wherein the static
magnetic fields strength exceeds 5
G, should be demarcated and clearly marked as being potentially
hazardous.
d. Zone IV: This area is synonymous with the MR scanner magnet
room itself, ie, the physical
confines of the room within which the MR scanner is located.
Zone IV, by definition, willalways be located within Zone III, as
it is the MR magnet and its associated magnetic field
that generates the existence of Zone III. Zone IV should also be
demarcated and clearly
marked as being potentially hazardous due to the presence of
very strong magnetic fields. As
part of the Zone IV site restriction, all MR installations
should provide for direct visual
observation by level 2 MR personnel to access pathways into Zone
IV. By means of
illustration only, the MR technologists would be able to
directly observe and control, via line
of site or via video monitors, the entrances or access corridors
to Zone IV from their normal
positions when stationed at their desks in the scan control
room.
Zone IV should be clearly marked with a red light and lighted
sign stating, the magnet is
on. Except for resistive systems, this red light and sign should
be illuminated at all times and
should be provided with a backup energy source to continue to
illuminate for at least 24 hours
in the event of a loss of power to the site.
In case of cardiac or respiratory arrest or other medical
emergency within Zone IV for which
emergent medical intervention or resuscitation is required,
appropriately trained and certified
MR personnel should immediately initiate basic life support or
CPR as required by the
situation whilethe patient is being emergently removed from Zone
IV to a predetermined,
magnetically safe location.Allpriorities should be focused on
stabilizing (eg, basic lifesupport with cardiac compressions and
manual ventilation) and then evacuating the patient as
rapidly and safely as possible from the magnetic environment
that might restrict safe
resuscitative efforts.
Further, for logistical safety reasons, the patient should
always be moved from Zone IV to the
prospectively identified location where full resuscitative
efforts are to continue.
Quenching the magnet (for superconducting systems only) is not
routinely advised for cardiac
or respiratory arrest or other medical emergency, since
quenching the magnet and having the
magnetic field dissipate could easily take more than a minute.
Furthermore, as quenching a
magnet can theoretically be hazardous, ideally one should
evacuate the magnet room, when
possible, for an intentional quench. One should rather use that
time wisely to initiate life
support measures while moving the patient from Zone IV to a
location where the strength of
the magnetic field is insufficient to be a medical concern.
Zones III and IV site access
3
-
8/12/2019 ACR Safety Guidelines 2004
4/24
ACR WHITE PAPER ON MAGNETIC RESONANCE (MR) SAFETYCombined Papers
of 2002 and 2004
restriction mustbe maintained during resuscitations and other
emergent situations for the
protection of all involved.
2. MR personnel and non-MR personnel (see Appendix 1):
a. All individuals working within at least Zone III of the MR
environment should be
documented as having successfully completed at least one of the
MR safety live lectures or
prerecorded presentations approved by the MR medical director.
Attendance should be
repeated at least annually, and appropriate documentation should
be provided to confirm
these ongoing educational efforts. These individuals shall be
referred to henceforth as MR
personnel.
b. There are 2 levels of MR personnel:
(1) Level 1 MR personnel: Those who have passed minimal safety
educational efforts to
ensure their own safety as they work within Zone III will be
referred to henceforth as
level 1 MR personnel.
(2) Level 2 MR personnel: Those who have been more extensively
trained and educated in
the broader aspects of MR safety issues, including, for example,
issues related to the
potential for thermal loading or burns and direct neuromuscular
excitation from rapidlychanging gradients, will be referred to
henceforth as level 2 MR personnel. It is the
responsibility of the MR medical director not only to identify
the necessary training, but
also to identify those individuals who qualify as level 2 MR
personnel. It is understood
that the medical director will have the necessary education and
experience in MR safety
to qualify as level 2 MR personnel.
c. All those not having successfully complied with these MR
safety instruction guidelines shall
be referred to henceforth as non-MR personnel. Specifically,
non-MR personnel will be the
terminology used to refer to any individual or group who has not
within the previous 12
months undergone the designated formal training in MR safety
issues defined by the MR
safety director of that installation.
3. Patient and non-MR personnel screening:
a. Allnon-MR personnel wishing to enter Zone III must first pass
an MR safetyscreening
process. Only MR personnel are authorized to perform an MR
safety screen prior to
permitting non-MR personnel into Zone III.
b. The screening process and screening forms for patients,
non-MR personnel, and MR
personnel should be essentially identical. Specifically, one
should not assume that non-MR
personnel, health care practitioners, or MR personnel will not
enter the bore of the MR
imager during the MRI process.
This might be the case if a pediatric patient cries for his
mother, who then leans into the bore,
or if the anesthetist leans into the bore to manually ventilate
a patient in the event of a
problem.
c. Metal detectors:
The usage of metal detectors in MR environments is
notrecommended. Reasons for this
recommendation include, among others:
(1) They have variedand variablesensitivity settings.
(2) The skills of the operators can vary.
4
-
8/12/2019 ACR Safety Guidelines 2004
5/24
ACR WHITE PAPER ON MAGNETIC RESONANCE (MR) SAFETYCombined Papers
of 2002 and 2004
(3) Todays metal detectors cannot detect, for example, a 23-mm,
potentially dangerous
ferromagnetic metal fragment in the orbit or near the spinal
cord or heart.
(4) Todays metal detectors do not differentiate between
ferromagnetic and
nonferromagnetic metallic objects, implants, or foreign
bodies.
(5) Metal detectors should not be necessary for the detection of
large metallic objects, such
as oxygen tanks on the gurney with the patients. These objects
are fully expected to be
detectedand physically excludedduring the routine
patient-screening process.
d. Non-MR personnel should be accompanied by, or under the
immediate supervision of and in
visual and verbal contact with, one specifically identified
level 2 MR person for the entirety
of their duration within Zone III or IV. However, it is
acceptable to have them in a changing
room or restroom in Zone III without visual contact as long as
the personnel and the patient
can communicate verbally with each other.
Level 1 MR personnel are permitted unaccompanied access
throughout Zones III and IV.
Level 1 MR personnel are also explicitly permitted to be
responsible for accompanying non-
MR personnel into and throughout Zone III, excluding Zone IV.
However, level 1 MR
personnel are notpermitted to directly admit, or be designated
responsible for, non-MRpersonnel in Zone IV.
In the event of a shift change, lunch break, etc, no level 2 MR
personnel shall relinquish their
responsibility to supervise non-MR personnel still within Zone
III or IV until such
supervision has been formally transferred to another of the
level 2 MR personnel.
e. Nonemergent patients should be MR safetyscreened on site by a
minimum of 2 separate
individuals. At least one of these individuals should be level 2
MR personnel. At least one of
these 2 screens should be performed verbally or
interactively.
Emergent patients and their accompanying non-MR personnel may be
screened only once,
provided the screening individual is level 2 MR personnel. There
should be no exceptions to
this.
f. Any individual undergoing an MR procedure must remove all
readily removable metallic
personal belongings and devices on or in them, eg, watches,
jewelry, pagers, cell phones,
body piercings (if removable), contraceptive diaphragms,
metallic drug-delivery patches (see
section I), cosmetics containing metallic particles (such as eye
makeup), and clothing items
that may contain metallic fasteners, hooks, zippers, loose
metallic components, or metallic
threads. It is therefore advisable to require patients or
research subjects to wear a site-
supplied gown with no metal fasteners during the MR procedure
when feasible. Inquiries
regarding drug-delivery patches or pads have led the panel to
review this issue and comment
as noted in section I, below.
g. All patients and non-MR personnel with a history of potential
ferromagnetic foreign object
penetration must undergo further investigation prior to being
permitted entrance to Zone III.Examples of acceptable methods of
screening include patient history, plain X-ray films, prior
CT or MR studies of the questioned anatomic area, or access to
written documentation of the
type of implant or foreign object that might be present. Once
positive identification has been
made as to the type of implant or foreign object that is within
a patient, best effort
assessments should be made to identify the MR compatibility or
MR safety of the implant or
object. Efforts at identification might include written testing
on the implant prior to
implantation (preferred), product labeling regarding the implant
or object, and peer-reviewed
publications regarding MR compatibility and MR safety testing of
the make, model, or type
5
-
8/12/2019 ACR Safety Guidelines 2004
6/24
ACR WHITE PAPER ON MAGNETIC RESONANCE (MR) SAFETYCombined Papers
of 2002 and 2004
of the object. MR safety testing would be of value only if the
object or device had not been
altered since such testing had been published.
All patients who have a history of orbit trauma by a potential
ferromagnetic foreign bodyfor
which they sought medical attentionare to have their orbits
cleared by either plain X-ray orbit
films10,11(2 views) or by a radiologists review and assessment
of contiguous cut prior CT or
MR images (obtained since the suspected traumatic event), if
available.
h. Conscious, nonemergent patients and research and volunteer
subjects are to complete written
MR safetyscreening questionnaires prior to their introduction to
Zone III. Family or
guardians of nonresponsive patients or of patients who cannot
reliably provide their own
medical histories are to complete a written MR safetyscreening
questionnaire prior to their
introduction to Zone III. These completed questionnaires are
then to be reviewed orally with
the patient, guardian, or research subject in their entirety
prior to permitting the patient or
research subject to be cleared into Zone III.
The patient, guardian, or research subject as well as the
screening MR staff member must
both sign the completed form. This form should then become part
of the patients medical
record. No empty responses will be acceptedeach question mustbe
answered with a yes
or no, or specific further information must be provided as
requested. A sample pre-MRscreening form is provided (see Appendix
2). This is the minimum information to be
obtained; more may be added if the site so desires.
i. Screening of the patient or non-MR personnel with, or
suspected of having, an intracranial
aneurysm clip should be performed per the separate MR safe
practice guideline addressing
this particular topic (see section M, below).
j. Screening of patients for whom an MR examination is deemed
clinically indicated or
necessary but who are unconscious or unresponsive or who cannot
provide their own reliable
histories regarding prior possible exposure to surgery, trauma,
or metallic foreign objects and
for whom such histories cannot be reliably obtained from
others:
(1) If no reliable patient metal exposure history can be
obtained, and if the requested MRexamination cannot reasonably wait
until a reliable history might be obtained, it is
recommended that such patients be physically examined by level 2
MR personnel. All
areas of scars or deformities that might be anatomically
indicative of an implant, such as
on the chest or spine region, and whose origins are unknown and
which may have been
caused by ferromagnetic foreign bodies, implants, etc, should be
subject to plain-film
radiography (if recently obtained plain films or CT or MR
studies of such areas are not
already available). The investigation described above should be
made to ensure there are
no potentially harmful embedded or implanted metallic foreign
objects or devices. All
such patients should also undergo plain-film imaging of the
skull or orbits and chest to
exclude metallic foreign objects (if recently obtained
radiographic or MR information is
not already available).
(2) Monitoring patients in the MR scanner is sometimes
necessary. The potential for thermal
injury from excessive RF power deposition exists. Sedated,
anesthetized, or unconscious
patients may not be able to express symptoms of such injury.
This potential for injury is
greater on especially higher field whole-body scanners (eg, 1 T
and above). Much patient
monitoring information can be satisfactorily acquired via pulse
oximetry or other means
without the utilization of electrocardiographic tracing and its
inherent thermal injury
risks. Patients who require EKG monitoring and who are
unconscious, sedated, or
anesthetized should be examined after each imaging sequence with
potential
6
-
8/12/2019 ACR Safety Guidelines 2004
7/24
ACR WHITE PAPER ON MAGNETIC RESONANCE (MR) SAFETYCombined Papers
of 2002 and 2004
repositioning of the EKG leads and any other electrically
conductive material with which
the patient is in contact. Alternatively, cold compresses or ice
packs could be placed upon
all necessary electrically conductive material that touches the
patient during scanning.
k. Final determination of whether or not to scan any given
patient with any given implant,
foreign body, etc is to be made by the level 2designated,
attending MR radiologist, the MR
medical director, or specifically designated level 2 MR
personnel following criteria foracceptability predetermined by the
medical director.
l. All non-MR personnel (eg, patients, volunteers, and varied
site employees and professionals)
with implanted cardiac pacemakers, autodefibrillators,
diaphragmatic pacemakers, or other
electromechanically activated devices upon which the non-MR
personnel is dependent should
be precluded from Zone IV and physically restrained from the 5-G
line unless specifically
cleared in writing by a level 2designated attending radiologist
or the medical director of the
MR site. In such circumstances, specific defending risk-benefit
rationale should be provided
in writing and signed by the authorizing radiologist.
Should it be determined that non-MR personnel wishing to
accompany a patient into an MR
scan room require their orbits to be cleared by plain-film
radiography, a radiologist must first
discuss with the non-MR personnel that plain X-ray films of
their orbits are required prior topermitting them access to the MR
scan room. Should they still wish to proceed with access to
Zone IV or within the 5-G line, and should the attending
radiologist deem it medically
advisable that they do so (eg, for the care of their child about
to undergo an MR study),
written informed consent should be provided by these
accompanying non-MR personnel prior
to undergoing X-ray examination of their orbits.
m. MR scanning of patients, prisoners, or parolees with metallic
prisoner-restraining devices or
RF ID or tracking bracelets could lead to theoretical adverse
events, including: (1)
ferromagnetic attractive effects and resultant patient injury,
(2) possible ferromagnetic
attractive effects and potential damage to the device or its
battery pack, (3) RF interference
with the MRI study and secondary image artifact, (4) RF
interference with the functionality
of the device, (5) RF power deposition and heating of the
bracelet or tagging device or its
circuitry and secondary patient injury (if the bracelet would be
in the anatomic volume of the
RF transmitter coil being imaged). Therefore, in cases where
requested to scan a patient,
prisoner, or parolee wearing RF tagging bracelets or metallic
handcuffs or anklecuffs, request
that the patient be accompanied by the appropriate authorities
who can and will remove the
restraining device prior to the MR study and be charged with its
replacement following the
examination.
n. Firefighter, police, and security safety considerations: For
the safety of firefighters and other
emergent services responding to an emergent call at the MR site,
it is recommended that all
fire alarms, cardiac arrests, or other emergent service response
calls originating from or
located in the MR site should be forwarded simultaneously to a
specifically designated
individual from amongst the sites MR personnel. This individual
should, if possible, be on
site prior to the arrival of the firefighters or emergent
responders to ensure that they do nothave free access to Zone III
or IV. The site might consider assigning appropriately trained
security personnel, who have been trained and designated as MR
personnel, to respond to
such calls.
In any case, all MR sites should arrange to prospectively
educate their local fire marshals,
firefighter associations, and police or security personnel about
the potential hazards of
responding to emergencies in the MR suite.
7
-
8/12/2019 ACR Safety Guidelines 2004
8/24
ACR WHITE PAPER ON MAGNETIC RESONANCE (MR) SAFETYCombined Papers
of 2002 and 2004
It should be stressed that, even in the presence of a true fire
(or other emergency) in Zone III
or IV, the magnetic fields may be present and fully operational.
Therefore, free access to
Zone III or IV by firefighters or other non-MR personnel with
air tanks, axes, crowbars, other
firefighting equipment, guns, etc might prove catastrophic or
even lethal to those responding
or others in the vicinity.
As part of the Zones III and IV restrictions, all MR sites must
have readily accessible, clearlymarked, MR-compatible fire
extinguishing equipment physically stored within Zone III or
IV. All nonMR-compatible fire extinguishers and other
firefighting equipment should be
restricted from Zone III.
For superconducting magnets, the helium (and the nitrogen, as
well, in older magnets) is not
flammable and does not pose a fire hazard directly. However, the
liquid oxygen that can
result from the supercooled air in the vicinity of the released
gases might well increase the
fire hazard in this area. If there are appropriately trained and
knowledgeable MR personnel
available during an emergency to ensure emergency response
personnel are kept out of the
MR scanner or magnet room and 5-G line, quenching the magnet
during a response to an
emergency or fire should not be a requirement.
However,if the fire is in such a location that Zone III or IV
needs to be entered for whateverreason by firefighters or emergency
response personnel and their firefighting and emergent
equipment, such as air canisters, crowbars, axes, and
defibrillators, a decision to quench a
superconducting magnet should be veryseriously considered to
protect the health and lives of
the emergency response personnel. Should a quench be performed,
appropriately designated
MR personnel still need to ensure that allnon-MR personnel
(including and especially
emergency response personnel) continue to be restricted from
Zones III and IV until the
designated MR personnel has personally verified that the static
field is either no longer
detectable or at least sufficiently attenuated to no longer
present a potential hazard to one
moving by it with, for example, large ferromagnetic objects such
as oxygen tanks or axes.
For resistive systems, the magnetic field of the MR scanner
should be shut down as
completely as possible and verified as such prior to permitting
the emergency response
personnel access to Zone IV. For permanent, resistive, or hybrid
systems whose magnetic
fields cannot be completely shut down, MR personnel should be
available to warn the
emergency response personnel that a very powerful magnetic field
is still operational in the
magnet room.
4. MR personnel screening:
All MR personnel are to undergo an MR-screening process as part
of their employment interview
process to ensure their safety in the MR environment. For their
own protection, and for the
protection of the non-MR personnel under their supervision, all
MR personnel must immediately
report to the MR medical director any trauma, procedure, or
surgery they experience or undergo
where a ferromagnetic metallic object or device may have been
introduced within or on them.
This will permit appropriate screening to be performed on the
employee to determine the safetyof permitting that MR
personneldesignated employee into Zone III.
5. Device and object screening:
As part of the Zone III site restriction and equipment testing
and clearing responsibilities, all sites
should have ready access to a strong handheld magnet (1000 G).
This will enable the site to test
external, and even some superficial internal, devices or
implants for the presence of grossly
detectable ferromagnetic attractive forces.
8
-
8/12/2019 ACR Safety Guidelines 2004
9/24
-
8/12/2019 ACR Safety Guidelines 2004
10/24
ACR WHITE PAPER ON MAGNETIC RESONANCE (MR) SAFETYCombined Papers
of 2002 and 2004
C. MR Technologist
1. MR technologists should be ARRT registered technologists
(RTs). Furthermore, all MR
technologists must be trained as level 2 MR personnel during
their orientation, prior to being
permitted free access to Zone III.
2. All MR technologists will maintain current certification in
American Heart Association basic life
support at the health care provider level.
3. Except for emergent coverage, there will be a minimum of 2 MR
technologists or one MR
technologist and one other individual with the designation of MR
personnel in the immediate
Zone II through Zone IV environment. For emergent coverage, the
MR technologist can scan
with no other individuals in their Zone II through Zone IV
environment as long as there is in-
house, ready emergent coverage by designated department of
radiology MR personnel (eg,
radiology house staff or radiology attendings).
D. Pregnancy-Related Issues
1. Health care practitioner pregnancies:
Pregnant health care practitioners are permitted to work in and
around the MR environmentthroughout all stages of their
pregnancy.12Acceptable activities include, but are not limited
to,
positioning patients, scanning, archiving, injecting contrast,
and entering the MR scan room in
response to an emergency. Although permitted to work in and
around the MR environment,
pregnant health care practitioners are requested not to remain
within the MR scanner bore or
Zone IV during actual data acquisition or scanning.
2. Patient pregnancies:
a. Pregnant patients can be accepted to undergo MR scans at any
stage of pregnancy if, in the
determination of a level 2 MR personneldesignated attending
radiologist, the risk-benefit
ratio for the patient warrants that the study be performed. The
radiologist should confer with
the referring physician and document the following in the
radiology report or the patients
medical record:
(1) The information requested from the MR study cannot be
acquired via nonionizing means
(eg, ultrasonography).
(2) The data is needed to potentially affect the care of the
patient or fetus duringthe
pregnancy.
(3) The referring physician does not feel it is prudent to wait
until the patient is no longer
pregnant to obtain this data.
b. MR contrast agents should notbe routinely provided to
pregnant patients. This decision, too,
is one that must be made on a case-by-case basis by the covering
level 2 MR personnel
designated attending radiologist who will assess the
risk-benefit ratio for the particular
patient.
c. It is recommended that pregnant patients undergoing an MR
examination provide written
informed consent to document that they understand the risks and
benefits of the MR
procedure to be performed, are aware of the alternative
diagnostic options available to them
(if any), and wish to proceed.
10
-
8/12/2019 ACR Safety Guidelines 2004
11/24
ACR WHITE PAPER ON MAGNETIC RESONANCE (MR) SAFETYCombined Papers
of 2002 and 2004
E. Pediatric MR Safety Concerns
1. Sedation and monitoring issues:
Children form the largest group requiring sedation for MRI,
largely because of their inability to
remain motionless during scans. Sedation protocols may vary from
institution to institution
according to the procedures performed (diagnostic vs
interventional), the complexity of the
patient population (healthy preschoolers vs premature infants),
the method of sedation (mild
sedation vs general anesthesia), and the qualifications of the
sedation provider.
Adherence to standards of care mandates following the sedation
guidelines developed by the
American Academy of Pediatrics,13,14the American Society of
Anesthesiologists,15and the Joint
Commission on Accreditation of Healthcare Organizations.16In
addition, sedation providers must
comply with the protocols established by the individual state
and the practicing institution. These
guidelines require the following provisions:
a. Preprocedural medical history and examination for each
patient
b. Fasting guidelines appropriate for age
c. Uniform training and credentialing for sedation providers
d. Intraprocedural and postprocedural monitors with adapters
appropriately sized for children
(compatible with the magnetic field)
e. Method of patient observation (window, camera)
f. Resuscitation equipment, including oxygen delivery and
suction
g. Uniform system of record keeping and charting (with
continuous assessment and recording of
vital signs)
h. Location and protocol for recovery and discharge
i. Quality assurance program that tracks complications and
morbidityFor the neonatal and the young pediatric population,
special attention is needed in monitoring
body temperature in addition to other vital signs. Temperature
monitoring equipment that is
approved for use in the MR suite is becoming more readily
available. Commercially available,
MR-approved neonatal isolation transport units and other warming
devices are also available for
use during MR scans.
2. Pediatric screening issues:
Children may not be reliable historians and, especially for
older children and teenagers, should be
questioned both in the presence of parents or guardians and
separately to maximize the possibility
that all potential dangers are disclosed. Therefore, it is
recommended that they be gowned before
entering Zone IV to help ensure no metallic objects, toys, etc
inadvertently find their way into
Zone IV. Pillows, stuffed animals, and other comfort items
brought from home represent real
risks and should be discouraged from entering Zone IV. If
unavoidable, each should be carefully
checked with the powerful handheld magnet and perhaps again in
the MR scanner prior topermitting the patient to enter Zone IV in
order to ensure they do not contain any objectionable
metallic components.
11
-
8/12/2019 ACR Safety Guidelines 2004
12/24
ACR WHITE PAPER ON MAGNETIC RESONANCE (MR) SAFETYCombined Papers
of 2002 and 2004
3. MR safety of accompanying family and personnel:
Although any age patient might request that others accompany
them for their MR examination,
this is far more common in the pediatric population. Those
accompanying or remaining with the
patient should be screened using the same criteria as anyone
else entering Zone IV.
In general, it would be prudent to limit accompanying adults to
a single individual. Only a
qualified, responsible MR physician should make screening
criteria exceptions.
Hearing protection and MR-compatible chairs or stools are
recommended for accompanying
family members within the MR scan room.
4. Fetal MR contrast agent safety concerns:
The decision to administer a gadolinium-based MR contrast agent
to pregnant patients should be
accompanied by a well-documented and thoughtful risk-benefit
analysis. This analysis should be
able to defend a decision to administer the contrast agent based
on overwhelming potential
benefit to the patient or fetus outweighing the theoretical but
potentially real risks of the long-
term exposure of the developing fetus to free gadolinium
ions.
Studies have demonstrated that gadolinium-based MR contrast
agents pass through the placentalbarrier and enter the fetal
circulation. From here, they are filtered in the fetal kidneys and
then
excreted into the amniotic fluid. In this location, the
gadolinium-chelate molecules are in a
relatively protected space and may remain in the amniotic fluid
for an indeterminate amount of
time before finally being reabsorbed and eliminated. As with any
equilibrium situation involving
any dissociation constant, the longer the chelate molecule
remains in this space, the greater the
potential for dissociation of the potentially toxic gadolinium
ion from its chelate molecule. It is
unclear what impact such free gadolinium ions might have if they
were to be released in any
quantity in the amniotic fluid. Certainly, deposition into the
developing fetus would raise
concerns of possible secondary adverse effects.
As indicated before, but repeated for added emphasis, a
documented, in-depth analysis of the
potential risks and benefits to the patient and her fetus is
necessary in order to arrive at a
reasonable conclusion as to the clinical advisability of
administering a gadolinium-based MR
contrast agent to any pregnant patient.
F. Time-Varying Gradient Magnetic FieldRelated Issues: Induced
Voltages
Types of patients needing extra caution:
Patients with implanted or retained wires in anatomically or
functionally sensitive areas (eg,
myocardium or epicardium, implanted electrodes in the brain)
should be considered at higher
risk, especially from faster MRI sequences, such as echo planar
imaging (which may be used in
such sequences as diffusion-weighted imaging, functional
imaging, perfusion-weighted imaging,
MR angiographic imaging, etc). The decision to limit the dB/dt
(rate of magnetic field change)
and maximum strength of the magnetic field of the gradient
subsystems during the imaging of
such patients should be reviewed by the level 2 MR
personneldesignated attending radiologistsupervising the case or
patient.
G. Time-Varying Gradient Magnetic FieldRelated Issues: Auditory
Considerations
1. All patients and volunteers should be offered and encouraged
to use hearing protection prior to
undergoing any imaging in the MR scanners.
2. All patients or volunteers in whom research sequences are to
be performed (ie, MR scan
sequences that have not yet been approved by the Food and Drug
Administration) are to have
12
-
8/12/2019 ACR Safety Guidelines 2004
13/24
ACR WHITE PAPER ON MAGNETIC RESONANCE (MR) SAFETYCombined Papers
of 2002 and 2004
hearing protective devices in placeprior to initiating any MR
sequences. Without hearing
protection in place, MRI sequences that are not FDA approved
should not be performed on
patients or volunteers.
H. Time-Varying Radiofrequency Magnetic FieldRelated Issues:
Thermal
1. All unnecessary or unused electrically conductive materials
should be removed from the MR
system before the onset of imaging. It is not sufficient merely
to unplug or disconnect unused,
unnecessary electrically conductive material and leave it within
the MR scanner with the patient
during imaging. All electrical connections, such as on-surface
coil leads or monitoring devices,
must be visually checked by the scanning MR technologist prior
to each scan to ensure the
integrity of the thermal and electrical insulation.
2. Electrical voltages and currents can be induced within
electrically conductive materials that are
within the bore of the MR imager during the MR imaging process.
This might result in the
heating of this material by resistive losses. This heat might be
of a caliber sufficient to cause
injury to human tissue. Among the variables that determine the
amount of induced voltage or
current is the consideration that the larger the diameter of the
conductive loop the greater the
potential induced voltages or currents and, thus, the greater
the potential for resultant thermal
injury to adjacent or contiguous patient tissue.
Therefore, when electrically conductive materials (wires, leads,
implants, etc) are required to
remain within the bore of the MR scanner with the patient during
imaging, care should be taken
to ensure no large-caliber, electrically conductive loops
(including patient tissue; see section H.5,
below) are formed within the MR scanner during imaging.
Furthermore, it is possible, with the
appropriate configuration, lead length, static magnetic field
strength, and other settings, to
introduce resonant circuitry between the transmitted RF power
and the lead. This could result in
very rapid and clinically significant lead heating, especially
at the lead tips, in a matter of seconds
to a magnitude sufficient to result in tissue thermal injury or
burns. This can also theoretically
occur with implanted leads or wires even when they are not
connected to any other device at
either end. Thus, exposure of electrically conductive leads or
wires to the RF-transmitted power
during MR scanning should only be performed with caution and
with appropriate steps taken to
ensure significant lead or tissue heating does not result (see
section H.9, below).
3. When electrically conductive materials are required to be
within the bore of the MR scanner with
the patient during imaging, care should be taken to place
thermal insulation (including air, pads,
etc) between the patient and the electrically conductive
material while simultaneously attempting
to (as much as feasible) keep the electrical conductor from
directly contacting the patient during
imaging. It is also appropriate to try to position the leads or
wires as far as possible from the innerwalls of the MR scanner if
the body coil is being used for RF transmission. When it is
necessary
that electrically conductive leads directly contact the patient
during imaging, consideration should
be given to prophylactic application of cold compresses or ice
packs to such areas.
4. Depending on specific magnet designs, care may be needed to
ensure that the patients tissues do
not directly come into contact with the inner bore of the MR
imager during the MRI process. Thiscare is especially important for
several higher-field MR scanners. The manufacturers of these
devices provide pads and other insulating devices for this
purpose, and manufacturer guidelines
should be strictly adhered to for these units.
5. It is important to ensure the patients tissues do not form
large conductive loops. Therefore, care
should be taken to ensure the patients arms or legs are not
positioned in such a way as to form a
large caliber loop within the bore of the MR imager during the
imaging process. For this reason,
it is preferable that patients be instructed not to cross their
arms or legs in the MR scanner.
13
-
8/12/2019 ACR Safety Guidelines 2004
14/24
ACR WHITE PAPER ON MAGNETIC RESONANCE (MR) SAFETYCombined Papers
of 2002 and 2004
6. Skin staples and superficial metallic sutures: Patients
requested to undergo MR studies in whom
there are skin staples or superficial metallic sutures (SMS) may
be permitted to undergo the MR
examination if the skin staples or SMS are not ferromagnetic and
are not in the anatomic volume
of RF power deposition for the study to be performed. If the
nonferromagnetic skin staples or
SMS are within the volume to be RF irradiated for the requested
MR study, several precautions
are recommended:
a. Warn the patient and make sure they are especially aware of
the possibility that they may
experience warmth or even burning along the skin staple or SMS
distribution. The patient
should be instructed to report immediately if they experience
warmth or burning sensations
during the study (and not, for example, to wait until the end of
the knocking noise).
b. It is recommended that a cold compress or ice pack be placed
along the skin staples or SMS if
this can be safely clinically accomplished during the MRI
examination. This will help to
serve as a heat sink for any focal power deposition that may
occur, thus decreasing the
likelihood of a clinically significant thermal injury or burn to
adjacent tissue.
7. For patients with extensive or dark tattoos, including
tattooed eyeliner, in order to decrease the
potential for RF heating of the tattooed tissue, it is
recommended that cold compresses or ice
packs be placed on the tattooed areas and kept in place
throughout the MRI process if thesetattoos are within the volume in
which the body coil is being used for RF transmission. This
approach is especially appropriate if fast spin echo (or other
high-RF-duty cycle) MRI sequences
are anticipated in the study. If another coil is being used for
RF transmission, a decision must be
made if high RF-transmitted power is to be anticipated by the
study protocol design. If so, then
the above precautions should be followed. Additionally, patients
with tattoos that have been
placed within 48 hours prior to the pending MR examination
should be advised of the potential
for smearing or smudging of the edges of the freshly placed
tattoo.
8. The unconscious or unresponsive patient should have all
attached leads covered with a cold
compress or ice pack at the lead attachment site for the
duration of the MR study prior to the
initiation of scanning.
9. As noted above, it has been demonstrated that resonant
circuitry can be established during MRIbetween the RF energies
being transmitted and specific lengths of long, electrically
conductive
wires or leads, which can thus act as efficient antennae. This
can result in heating of the tips of
these wires or leads to temperatures in excess of 90C in a few
seconds. Therefore, patients in
whom there are long, electrically conductive leads, such as
Swan-Ganz thermodilution cardiac
outputcapable catheters or Foley catheters with electrically
conductive leads, should be
considered at risk for MR studies if the body coil is to be used
for RF transmission over theregion of the electrically conductive
lead. This is especially true for higher-field systems and for
imaging protocols utilizing fast spin echo or other high-RF-duty
cycle MRI sequences. Each such
patient should be reviewed and cleared by an attending level 2
radiologist, and a risk-benefit ratio
assessment should be performed prior to permitting them access
to the MR scanner.
I. Drug-Delivery Patches and Pads
Some drug-delivery patches contain metallic foil. Scanning the
region of the metallic foil may result
in thermal injury.17Since removal or repositioning can result in
altering the patients dose,
consultation with the patients prescribing physician would be
indicated in assessing how best to
manage the patient. If the metallic foil of the patch delivery
system is positioned on the patient so that
it is in the volume of excitation of the transmitting RF coil,
the case should be specifically reviewed
with the radiologist or physician covering the case. Alternative
options may include placing an ice
pack directly on the patch. This solution may still
substantially alter the rate of delivery or absorption
14
-
8/12/2019 ACR Safety Guidelines 2004
15/24
ACR WHITE PAPER ON MAGNETIC RESONANCE (MR) SAFETYCombined Papers
of 2002 and 2004
of the medication to the patient (and be less comfortable to the
patient, as well). This ramification
should therefore not be treated lightly, and a decision to
proceed in this manner should only be made
by a knowledgeable radiologist attending the patient and with
the concurrence of the referring
physician, as well.
If the patch is removed, a specific staff member should be given
responsibility for ensuring that it is
replaced or repositioned.
J. Cryogen-Related Issues
1. For superconducting systems, in the event of a system quench,
it is imperative that all personnel
and patients be evacuated from the MR scan room as quickly and
as safely feasible and that the
site access be immediately restricted to all individuals until
the arrival of the MR equipment
service personnel. This is especially so if cryogenic gases are
observed to have vented partially or
completely into the scan room, as evidenced in part by the
sudden appearance of white clouds
or fog around or above the MR scanner. As noted in section B.3.n
above, it is especially
important to ensure all police and fire response personnel are
restricted from entering the MR
scan room with their equipment (axes, air canisters, guns, etc)
until it can be confirmed that the
magnetic field has been successfully dissipated, as there may
still be considerable static magnetic
field present despite a quench or partial quench of the
magnet.
2. It should be pointed out that room oxygen monitoring was
discussed by the MR Blue Ribbon
Panel and rejected at this time because the present
oxygen-monitoring technology was considered
by industry experts not to be sufficiently reliable to allow for
continued operation during
situations of power outages, etc.
K. Claustrophobia, Anxiety, Sedation, Analgesia, and
Anesthesia
Adult and pediatric patient anxiolysis, sedation, analgesia, and
anesthesia for any reason should
follow established ACR,18,19American Society of
Anesthesiologists,15,20-22and JCAHO standards.23
L. Contrast Agent Safety
1. Contrast agent administration issues:
No patient is to be administered prescription MR contrast agents
without orders from a duly
licensed physician. Intravenous injectionqualified MR
technologists may start and attend to
peripheral IV access lines if they have undergone the requisite
site-specified training in peripheral
IV access and have demonstrated and documented appropriate
proficiency in this area. IV-qualified MR technologists may
administer FDA-approved gadolinium-based MR contrast agents
via peripheral IV routes as a bolus or as a slow or continuous
injection, as directed by the orders
of a duly licensed site physician.
a. Administration of these agents is to be performed as per the
ACR policy: The ACR approves
of the injection of contrast material and diagnostic levels of
radiopharamceuticals by certified
and/or licensed radiologic technologists and radiologic nurses
under the direction of a
radiologist or his or her physician designee who is personally
and immediately available, ifthe practice is in compliance with
institutional and state regulations. There must also be prior
written approval by the medical director of the radiology
department /service of such
individuals; such approval process having followed established
policies and procedures, and
the radiologic technologists and nurses who have been so
approved maintain documentation
of continuing medical education related to materials injected
and to the procedures being
performed. (Res 1-H, 1987, 1997)
15
-
8/12/2019 ACR Safety Guidelines 2004
16/24
ACR WHITE PAPER ON MAGNETIC RESONANCE (MR) SAFETYCombined Papers
of 2002 and 2004
2. Prior contrast agent reaction issues:
a. According to the ACRManual on Contrast Media,Adverse events
after intravenous
injection of gadolinium seem to be more common in patients who
had previous reactions to
an MR contrast agent. In one study, 16 (21%) of 75 patients who
had previous adverse
reactions to MR contrast agents reacted to subsequent injections
of gadolinium. Patients with
asthma also seem to be more likely to have an adverse reaction
to gadolinium. Patients withallergies also seemed to be at
increased risk (~2.0-3.7 times, compared with patients without
allergies). Patients who have had adverse reactions to iodinated
contrast media are more than
twice as likely to have an adverse reaction to gadolinium (6.3%
of 857 patients).
b. At present there are no well-defined policies for patients
who are considered to be at
increased risk for having adverse reaction to MR contrast
agents; however, the following
recommendations are suggested: patients who have previously
reacted to one MR agent can
be injected with another agent, if they are restudied, and
at-risk patients can be pre-medicated
with corticosteroids and, occasionally, antihistamines.24
c. All patients with asthma, allergic respiratory histories,
prior iodinated or gadolinium-based
contrast reactions, etc should be followed more closely as they
are at a demonstrably higher
risk of adverse reaction.
M. Patients in Whom There Are or May Be Intracranial Aneurysm
Clips
1. In the event it is unclear whether a patient does or does not
have an aneurysm clip in place, plain
films should be obtained. Alternatively, if available, any
cranial plain-film, CT, or MR
examination that may have been taken in the recent past (ie,
subsequent to the suspected surgical
date) should be reviewed to assess for a possible intracranial
aneurysm clip.
2. In the event that a patient is identified to have an
intracranial aneurysm clip in place, the MR
examination should not be performed until it can be documented
that the type of aneurysm clip
within that patient is MR safe or compatible. All documentation
of types of implanted clips,dates, etc mustbe in writing and signed
by a licensed physician. Phone or verbal histories and
histories provided by a nonphysician are not acceptable. Faxed
copies of operative reports,physician statements, etc are
acceptable as long as a legible physician signature accompanies
the
requisite documentation. A written history of the clip having
been appropriately tested for
ferromagnetic properties (and a description of the testing
methodology used) prior to implantation
by the operating surgeon is also considered acceptable if the
testing follows the deflection test
methodology established by the American Society of Testing and
Materials.
3. All implanted intracranial aneurysm clips that are documented
in writing to be composed of
titanium (either the commercially pure or the titanium alloy
types) can be accepted for scanning
without any other testing.
4. All nontitanium intracranial aneurysm clips manufactured 1995
or later for which the
manufacturers product labeling continues to claim MR
compatibility may be accepted for MR
scanning without further testing.
5. Clips manufactured prior to 1995 require either pretesting
(per the American Society of Testing
and Materials deflection test methodology) prior to implantation
or the individual review of a
previous MRI of the clip or brain in that particular case, if
available. By assessing the size of the
artifact associated with the clip relative to the static field
strength on which it was studied, the
sequence type, and the MRI parameters selected, an opinion may
be issued by one of the sites
level 2 MR attending radiologists as to whether the clip
demonstrates significant ferromagnetic
properties or not. Access to the MR scanner would then be based
on that opinion.
16
-
8/12/2019 ACR Safety Guidelines 2004
17/24
ACR WHITE PAPER ON MAGNETIC RESONANCE (MR) SAFETYCombined Papers
of 2002 and 2004
6. A patient with an aneurysm clip (or other implant) may have
safely undergone a prior MR
examination at any given static magnetic field strength. This
fact in and of itself isnot sufficient
evidence of the implants MR safety or compatibility and should
notsolely be relied upon to
determine the MR safety or compatibility status of the aneurysm
clip (or other implant).
Variations in static magnetic field strength, static magnetic
field spatial gradient, orientation of
the aneurysm clip (or other implant) to the static magnetic
field or static field gradient, rate ofmotion through the spatial
static field gradient, etc are all variables that are virtually
impossible to
control or reproduce. These variables may not have resulted in
adverse events in one
circumstance but may result in significant injury or death on a
subsequent exposure. For example,
a patient who went blind from interactions between the metallic
foreign body in his retina and thespatial static fields of the MR
scanner entered the magnet and underwent the entire MR
examination without difficulty; he went blind upon exiting the
MR scanner at the completion of
the examination.
7. Barring availability of either pretesting or prior MRI data
of the clip in question, a risk-benefit
assessment and review must be performed in each case
individually. Further, for patients with
intracranial clips with no available ferromagnetic or imaging
data, should the risk-benefit ratio
favor the performance of the MR study, the patient or guardian
should provide written informed
consent that includes death as a potential risk of the MRI
procedure prior to permitting that
patient to undergo an MR examination.
N. Patients in Whom There Are or May Be Cardiac Pacemakers or
Implantable Cardioverter
Defibrillators
It is recommended that the presence of implanted cardiac
pacemakers or implanted cardioverter
defibrillators (ICDs) be considered contraindicated for routine
MRI. Should an exception be
considered, it should be done on a case-by-case and site-by-site
basis and only if the site is manned
with individuals with the appropriate radiology and cardiology
knowledge and expertise on hand.
Ideally, the nonemergent patient should be apprised of the risks
associated with the procedure and
should provide prospective written informed consent prior to its
initiation. Further, should any MRI
examination be contemplated for a patient with an implanted
pacing device, it is recommended that
radiology and cardiology personnel and a fully stocked crash
cart and defibrillator be on hand
throughout the procedure in case a significant arrhythmia
develops during the examination and for
whatever reason does not terminate with the cessation of the MR
study. All such patients should be
actively monitored for cardiac and respiratory function
throughout the examination. At the conclusion
of the examination, the cardiologist or electrophysiologist
should interrogate the pacemaker to
confirm that the function is consistent with the pre-examination
state. The panel is unaware at this
time of any ICD devices that are designed to be safely exposed
to intentional MR scanning. In fact,
there have been reports of ICD device malfunction after
inadvertent exposure to MR scanning.
There have been numerous reports of patients with pacemakers who
have undergone MR
examinations, both intentionally as well as inadvertently,
without difficulty or apparent injury. There
have also been several patients who were inadvertently exposed
to MR studies who have died during
the examination or very shortly thereafter. There is an
increasing body of evidence documenting theability of the MRI
process to produce, in specific cases and under certain
circumstances, direct
cardiac stimulation and arrhythmias. It is theorized that such
arrhythmogenesis and its severe
hypotensive sequelae were the cause of death in at least several
of these patients, some of whom were
not pacemaker dependent prior to the MR examination. It is also
becoming more apparent that the
primary cause of such arrhythmias seems to result from
interactions between the pacemakers lead
circuitry and the RF power transmitted during the MRI
process.
17
-
8/12/2019 ACR Safety Guidelines 2004
18/24
ACR WHITE PAPER ON MAGNETIC RESONANCE (MR) SAFETYCombined Papers
of 2002 and 2004
Some have suggested that it might be possible to perform MRI
examinations on patients with
implanted cardiac pacemakers as long as rigid guidelines were
carefully defined and adhered to
throughout the imaging process. These include recommendations,
among others, that ensure no
pacemaker-dependent patient is scanned, that the RF power
transmitted during the MRI process is not
deposited over the volume that contains the pacemaker or its
leads, etc. This guideline makes no
attempt to judge the scientific veracity of these observations
or claims. However, it clearly recognizes
that, even if it is possible to safely perform MRI examinations
on cardiac pacemaker patients, theexpertise necessary to safely do
so is exceedingly rare throughout MR industry today.
The entire field of MR scanning of pacemaker patients is one
that is exhibiting tremendous activity,
research, and growth of late. Fiber-optic pacemaker devices,
coated or shielded leads and pacingdevices, and various other
designs and configurations of MR pacing devices and leads are
being
actively investigated in an to attempt to devise MR-safe cardiac
pacemakers. It is therefore another
area within MR safety that bears close observation and frequent
updates over the next few months
and years as progress continues to be made toward developing
avenues that will enable pacemaker,
and eventually perhaps even ICD, patients to have safe access to
the powerful diagnostic modality
that is MRI.
REFERENCES:
1. Chaljub G, Kramer LA, Johnson RF III, Johnson RF Jr, Singh H,
Crow WN. Projectile cylinder
accidents resulting from the presence of ferromagnetic nitrous
oxide or oxygen tanks in the MR suite.
AJR Am J Roentgenol.2001;177:27-30.
2. ECRI hazard report: patient death illustrates the importance
of adhering to safety precautions in
magnetic resonance environments.Health
Devices.2001;30:311-314.
3. Kanal E, Borgstede JP, Barkovich AJ, et al. American College
of Radiology white paper on MR
safety.AJR Am J Roentgenol.2002;178:1335-1347.
4. Kanal E, Borgstede JP, Barkovich AJ, et al. American College
of Radiology white paper on MR
safety: 2004 update and revisions.AJR Am J
Roentgenol.2004;182:1111-1114.
5. Shellock FG, Kanal E. Policies, guidelines, and
recommendations for MR imaging safety and patient
management. The SMRI Safety Committee.J Magn Reson
Imaging.1991;1:97-101.
6. Kanal E, Shellock FG. Policies, guidelines and
recommendations for MR imaging safety and patient
management. The SMRI Safety Committee.J Magn Reson
Imaging.1992;2:247-248.
7. Shellock FG, Kanal E. Guidelines and recommendations for MR
imaging safety and patient
management. III. Questionnaire for screening patients before MR
procedures. The SMRI Safety
Committee.J Magn Reson Imaging.1994;4:749-751.
8. Magnetic resonance imaging monograph: safety and
sedation.Practice Guidelines and Technical
Standards.Reston, Va: American of College Radiology; 1996.
9. ACR standard for performing and interpreting magnetic
resonance imaging (MRI).PracticeGuidelines and Technical
Standards.Reston, Va: American of College Radiology; 2000.
10. Jarvik JG, Ramsey S. Radiographic screening for orbital
foreign bodies prior to MR imaging: is it
worth it?Am J Neuroradiol.2000;21:245-247.
11. Seidenwurm DJ, McDonnell CH III, Raghaven N, Breslau J. Cost
utility analysis of radiographic
screening for an orbital foreign body before MR imaging.Am J
Neuroradiol.2000;21:426-433.
18
-
8/12/2019 ACR Safety Guidelines 2004
19/24
ACR WHITE PAPER ON MAGNETIC RESONANCE (MR) SAFETYCombined Papers
of 2002 and 2004
12. Kanal E, Gillen J, Evans JA, Savitz DA, Shellock FG. Survey
of reproductive health among female
MR workers.Radiology.1993;187(2): 395-399.
13. American Academy of Pediatrics Committee on Drugs.
Guidelines for monitoring and management
of pediatric patients during and after sedation for diagnostic
and therapeutic procedures.Pediatrics.
1992;89:1110-1115.
14. American Academy of Pediatrics Committee on Drugs.
Guidelines for monitoring and management
of pediatric patients during and after sedation for diagnostic
and therapeutic procedures: addendum.
Pediatrics.2002;110:836-838.
15. Updated Practice Guidelines for Sedation and Analgesia by
Non-anesthesiologists.Park Ridge, Ill:
American Society of Anesthesiologists; August 2001.
16. Standards and intents for sedation and anesthesia care.
Comprehensive Accreditation Manual for
Hospitals.Chicago, Ill: Joint Commission on Accreditation of
Healthcare Organizations; 2002.
Report No. TX 2-2.
17. Shellock FG.Pocket Guide to MR Procedures and Metallic
Objects: Update 2001.Philadelphia, Pa:
Lippincott Williams and Wilkins; 2001:147-148.
18. ACR standard for adult sedation/analgesia.Practice
Guidelines and Technical Standards.Reston, Va:
American of College Radiology; 2000.
19. ACR standard for pediatric sedation/analgesia.Practice
Guidelines and Technical Standards.Reston,
Va: American of College Radiology; 1998.
20. Guidelines for Non-operating Room Anesthetizing
Locations.Park Ridge, Ill: American Society of
Anesthesiologists; 1994.
21. Standards for Basic Anesthetic Monitoring.Park Ridge, Ill:
American Society of Anesthesiologists;
1986,1998.
22. Standards for Post Anesthesia Care.Park Ridge, Ill: American
Society of Anesthesiologists;
1988,1994.
23. Standards and intents for sedation and anesthesia care.
Comprehensive Accreditation Manual for
Hospitals.Chicago, Ill: Joint Commission on Accreditation of
Healthcare Organizations; 2001.
Report No. TX 2-2.4.1.
24. American College of Radiology Committee on Drugs and
Contrast Media.Manual on Contrast
Media.4.1 ed. Reston, Va: American College of Radiology;
1998.
19
-
8/12/2019 ACR Safety Guidelines 2004
20/24
ACR WHITE PAPER ON MAGNETIC RESONANCE (MR) SAFETYCombined Papers
of 2002 and 2004
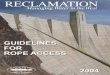
Figure 1
Model MR Facility Zone Configuration
This figure is meant to represent an idealized sample floor
plan, illustrating site access restriction
considerations. Other potential MR safety issues, such as magnet
site planning related to fringe magnetic
field considerations, are not meant to be included herein.
See Appendix 1 for personnel and zone definitions.
Note: In any zone of the facility, there should be compliance
with HIPAA regulations in regard to privacy
of patient information. However, in Zone III, there should be a
privacy barrier so that unauthorized
persons cannot view the control panels.
20
-
8/12/2019 ACR Safety Guidelines 2004
21/24
ACR WHITE PAPER ON MAGNETIC RESONANCE (MR) SAFETYCombined Papers
of 2002 and 2004
Appendix 1
PERSONNEL DEFINITIONS
Non-MR Personnel
Patients, visitors, or facility staff who do not meet the
criteria of level 1 or 2 MR personnel will be
referred to as non-MR personnel. Specifically, non-MR personnel
will be the terminology used to refer to
any individual or group who has not within the previous 12
months undergone the designated formaltraining in MR safety issues
defined by the MR safety director of that installation.
Level 1 MR Personnel
Individuals who have passed minimal safety educational efforts
to ensure their own safety as they work
within Zone III will be referred to as level 1 MR personnel (eg,
MRI department office staff, patient
aides).
Level 2 MR Personnel
Individuals who have been more extensively trained and educated
in the broader aspects of MR safety
issues, including, for example, issues related to the potential
for thermal loading or burns and direct
neuromuscular excitation from rapidly changing gradients, will
be referred to as level 2 MR personnel
(eg, MR technologists, radiologists, radiology department
nursing staff).
ZONE DEFINITIONS
Zone I
This region includes all areas that are freely accessible to the
general public. This area is typically outside
the MR environment itself and is the area through which
patients, health care personnel, and other
employees of the MR site access the MR environment.
Zone II
This area is the interface between the publicly accessible,
uncontrolled Zone I and the strictly controlled
Zone III (see below). Typically, patients are greeted in Zone II
and are not free to move throughout Zone
II at will, but rather are under the supervision of MR personnel
.It is in Zone II that the answers to MR-
screening questions, patient histories, medical insurance
questions, etc are typically obtained.
Zone III
This area is the region in which free access by unscreened
non-MR personnel or ferromagnetic objects or
equipment can result in serious injury or death as a result of
interactions between the individuals or
equipment and the MR scanners particular environment. These
interactions include, but are not limited
to, those involving the MR scanners static and time-varying
magnetic fields. All access to Zone III is to
be strictly restricted, with access to regions within it
(including Zone IV, see below) controlled by, and
entirely under the supervision of, MR personnel.
Zone IV
This area is synonymous with the MR scanner magnet room itself.
Zone IV, by definition, will always be
located within Zone III, as it is the MR magnet and its
associated magnetic field, which generates the
existence of Zone III.
Non-MR personnel should be accompanied by, or under the
immediate supervision of and visual contact
with, one specifically identified level 2 MR person for the
entirety of their duration within Zone III or IV.
Level 1 and 2 MR personnel may move freely about all zones.
21
-
8/12/2019 ACR Safety Guidelines 2004
22/24
ACR WHITE PAPER ON MAGNETIC RESONANCE (MR) SAFETYCombined Papers
of 2002 and 2004
Appendix 2
Safety Screening Form
for
Magnetic Resonance (MR) Procedures
Date: _______________ Name (first middle last):
Female [ ] Male [ ] Age: _____ Date of birth: ___________
Height: _______ Weight:
Why are you having this examination (medical problem)?
Yes No
Have you ever had an MRI examination before and had a problem?
____ ____
If yes, please describe:
Have you ever had a surgical operation or procedure of any kind?
____ ____
If yes, list all prior surgeries and approximate dates:
Have you ever been injured by a metal object or foreign body
(eg, bullet, BB, shrapnel)? ____ ____
If yes, please describe:
Have you ever had an injury from a metal object in your eye
(metal slivers, metal
shavings, other metal object)?
____ ____
If yes, did you seek medical attention? ____ ____
If yes, describe what was found:
Do you have a history of kidney disease, asthma, or other
allergic respiratory disease? ____ ____
Do you have any drug allergies? ____ ____
If yes, please list drugs:
Have you ever received a contrast agent or X-ray dye used for
MRI, CT, or other X-ray
or study?
____ ____
Have you ever had an X-ray dye or magnetic resonance imaging
(MRI) contrast agent
allergic reaction?
____ ____
If yes, please describe:
Are you pregnant or do you suspect you may be pregnant? ____
____
Are you breast-feeding? ____ ____
Date of last menstrual period: _______________ Are you
postmenopausal? ____ ____
22
-
8/12/2019 ACR Safety Guidelines 2004
23/24
-
8/12/2019 ACR Safety Guidelines 2004
24/24
ACR WHITE PAPER ON MAGNETIC RESONANCE (MR) SAFETYCombined Papers
of 2002 and 2004
____ ____ Radiation seeds (eg, cancer treatment)
____ ____ Any implanted items (eg, pins, rods, screws, nails,
plates, wires)
____ ____ Any hair accessories (eg, bobby pins, barrettes,
clips)
____ ____ Jewelry
____ ____ Any other type of implanted item
Type:
Instructions for the Patient
1. You are urged to use the earplugs or headphones we supply
during your MRI examination since some
patients may find the noise levels unacceptable, and the noise
levels may affect your hearing.
2. Remove all jewelry (eg, necklaces, pins, rings).
3. Remove all hairpins, bobby pins, barrettes, clips, etc.
4. Remove all dentures, false teeth, and partial dental
plates.
5. Remove hearing aides.
6. Remove eyeglasses.
7. Remove your watch, pager, cell phone, credit cards,
bankcards, and all other cards with a magnetic
strip.
8. Remove body piercing objects.9. Use gown, if provided, or
remove all clothing with metal fasteners, zippers, etc.
I attest that the above information is correct to the best of my
knowledge. I have read and understand theentire contents of this
form, and I have had the opportunity to ask questions regarding the
information on
this form.
Patient signature:
MD/RN/RT signature: Date:
Print name of MD/RN/RT:
For MRI Office Use Only
Patient name:
Patient ID number: _______________ Referring physician:
Procedure: _________________________ Diagnosis:
Clinical History:
Hazard Checklist for MRI Personnel
Yes No
____ ____ Endotracheal tube
____ ____ Swan-ganz catheter
____ ____ Extra ventricular device
____ ____ Arterial line transducer
____ ____ Foley catheter with temperature sensor and/or metal
clamp
____ ____ Rectal probe
____ ____ Esophageal probe
____ ____ Tracheotomy tube
____ ____ Guidewires