Embed Size (px)
Citation preview

Journal of Clinical Lipidology (2009) 3, 393–397
Case Studies
Acquired severe hypercholesterolemia andhypoalphalipoproteinemia
Zuhier Awan, MD, Dana Bailey, MSc, Anouar Hafiane, MSc, Jacques Genest, MD*
Cardiovascular Research Laboratories, McGill University Health Center Research Institute, McGill University, RoyalVictoria Hospital, 687 Pine Avenue West, Room M4.72, Montreal, Quebec, Canada H3A 1A1
Case report
A 51-year-old woman of French-Canadian descent withobesity (body mass index 37 kg/m2), hypertension, elevatedcholesterol, and type 2 diabetes was admitted to the hospi-tal with altered mental state, jaundice, and diarrhea. Shehad evidence of microvascular complications, includingcataracts, peripheral neuropathy, and diabetic nephropathy.There was a significant family history of premature coro-nary artery disease. Her mother had a myocardial infarctionat age 55, and her father underwent coronary bypass sur-gery at age 60. She was a habitual smoker (one pack/dayfor 35 years), led a sedentary lifestyle, consumed a westerndiet, and had poor compliance to medical therapy.
Physical examination revealed an obese lady withplethoric face and tanned skin. The cardiorespiratoryexamination was normal. Abdominal examination revealedmarked distension with shifting dullness and ascites; liverand spleen size were difficult to assess. Her extremitieswere warm, and peripheral pulses were slightly diminished.The right big toe was amputated after osteomyelitis asso-ciated with diabetes.
Laboratory examinations revealed the following values:decreased hemoglobin (91 g/L), normal red blood cell indi-ces. The initial plasma glucose level was 14 mmol/L, andHbA1c was increased (0.09 mmol/L; normal range,0.04 2 0.06 mmol/L). During her admission, plasma glu-cose levels ranged between 7 and 14 mmol/L; an insulinsliding scale was used to normalize glucose levels. Therewas a considerable hyponatremia (Na 128 mmol/L), normal
* Corresponding author.
E-mail address: [email protected]
Submitted July 8, 2009. Accepted for publication October 1, 2009.
1933-2874/$ -see front matter � 2009 National Lipid Association. All rights
doi:10.1016/j.jacl.2009.10.001
potassium, increased alkaline phosphatase (659 U/L; nor-mal range, 25 2 200 U/L), increased g-glutamyltransferase(308 U/L; normal range, 0 2 40 U/L), normal alanine ami-notransferase (43 U/L; normal range, 6 2 45 U/L), in-creased serum bilirubin (22 mmol/L; normal range,2 2 19 mmol/L), decreased albumin (18 g/L; normal range,38 2 50 g/L), decreased total protein (42 g/L; normalrange, 60 2 80 g/L), elevated high-sensitivity C-reactiveprotein (32 mg/L; normal range, ,2 mg/L), normal thyroidstimulating hormone (3.07 mU/L; normal range, 0.4 2 4.4mU/L), elevated CA9-9 (2736 kU/L), and elevated alphafetoprotein (3 mg/L). Serology for hepatitis B, C, and Ewere negative. During admission, renal function deterio-rated significantly (urea creatinine, 22 mmol/L; normalrange, 2.1 2 7.5 mmol/L; plasma creatinine 162 mmol/L;normal range, 40 2 90 mmol/L), and the estimated glomer-ular filtration rate decreased to 31 mL/min/1.73 m2 (normalrange, 52 2 134 mL/min/1.73 m2). A 24-h urine collectionrevealed proteinurea (3.6 g/24 h), and urinalysis revealedproteinuria and hyaline and granular casts.
Methods
Lipoproteins were separated by high-performance liquidchromatography (HPLC) on a Superose 6 column (GEHealthcare, Madison, WI). Cholesterol was determinedenzymatically by the use of a commercial kit (Thermo-Electron, Waltham, MA). High-density lipoprotein (HDL)subparticles were analyzed by two-dimensional polyacry-lamide gradient gel electrophoresis (2D-PAGGE) beforeand after treatment as previously described.1 Lecithin-cholesterol acyltransferase (LCAT) activity was assayedby the use of an artificial proteoliposome substrate of
reserved.

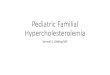
Figure 1 (A) and (B) are core liver biopsy; I, Masson-Trichromestaining highlighting the bridging fibrous septa seen in cirrhosis;II, hematoxylin and eosin staining demonstrating bile-stained he-patocytes; III, inflammatory cells predominantly neutrophilic; IV,expanded portal tract with prominent bile ductular proliferation.(C) and (D) are the kidney biopsy; V, diabetic glomerulosclerosiswith increased mesangial matrix and Kimmelstiel-Wilson noduleformation; VI, hyaline arteriosclerosis.
394 Journal of Clinical Lipidology, Vol 3, No 6, December 2009
apolipoprotein (apo)A-I: [3H]-cholesterol:lecithin, as previ-ously described.2 LCAT activity was determined as theamount of cholesteryl esters incorporated into apoA-I-containing proteoliposomes.
Results
Chest X-ray was normal, and ultrasonography confirmedthe presence of ascitic fluid and an enlarged liver. Cardiacechocardiography showed a normal left ventricular ejectionfraction of 70% with moderate diastolic dysfunction. Anendoscopic retrograde cholangiopancreatography (ERCP)revealed a stricture at ampulla of Vater as causative of theobstructive jaundice. Biopsies taken from the intra-ampullaryportion of the bile duct showed no primary biliary cirrhosis.Trans-hepatic liver biopsies performed via the jugular veinshowed stage 3 2 4 cirrhosis (Fig. 1A and 1B). A renal bi-opsy confirmed the presence of diabetic nephropathy(Fig. 1C and 1D). A radionuclide (Tc99 m-DTPA) renalscan showed a mild decreased flow and function with a pro-longed bilateral parenchymal transit time, which may be re-lated to hepatorenal syndrome. The effective renal plasmaflow was 420 mL/min. The corrected glomerular filtrationrate was 49 mL/min/1.73 m2. Ascites were drained by para-centesis, and the obstructive jaundice was relieved byERCP-mediated dilation of the ampulla of Vater. Intravenousinsulin was given to normalize serum glucose, and diureticsand electrolytes were given to correct fluid homeostasis. Agradual improvement was noted in the patient’s condition, in-cluding a 50% reduction in proteinurea from 3.6 to 1.82 g/24 h, and she was discharged after 13 days.
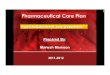
The lipid profile was monitored over the course of thepatient’s follow-up (Fig. 2A). The HPLC profile revealedan absence of HDL-cholesterol (HDL-C) and a marked in-crease in cholesterol-containing lipoproteins in the very lowdensity lipoprotein and low-density lipoprotein (LDL)ranges, with a distinct peak characteristic of lipoprotein(x),ie, Lp-(x) (Fig. 2B). The increase in LDL-sized particles islikely attributable to both increased LDL particles and het-erogeneous Lp-(x). One year before admission, the patient’sserum total cholesterol (TC) was 6.5 mmol/L (254 mg/dL),and HDL-C was 0.97 mmol/L (38 mg/dL). Upon presenta-tion with extrahepatic biliary obstruction and proteinuria,TC increased to 37 mmol/L (1443 mg/dL), triglyceridesto 2.4 mmol/L (218 mg/dL), and HDL-C decreased to,0.13 mmol/L (,5 mg/dL). Total apoB was 2.02 g/L,and apoA-I was 0.71 g/L, confirming the HPLC profile. Al-though the calculated LDL-cholesterol (LDL-C) would be36 mmol/L (1365 mg/dL), this value reflects the sum ofcholesterol contained within LDL particles plus Lp(x),The apoE genotype was E2/E3. Total Lp(a) was 55 mg/L.After treatment, the HPLC profile showed a modest in-crease in HDL-C and a marked resolution of the Lp-(x)and LDL-peaks (Fig. 2B).
Recovery of HDL particles was confirmed by 2D-PAGGE analysis (Fig. 3A and 3B). Before treatment, thesubject was deficient in larger, a-migrating HDL-particles,
characteristic of LCAT deficiency. After treatment, therewas an increase in these mature HDL particles (a1-LpAI,corresponding to HDL2 particles). To confirm LCAT defi-ciency, LCAT activity was measured by the use of a proteo-liposome substrate. Before treatment, the patient had amarked reduction in LCAT activity (16% of control), whichimproved significantly after relief of extrahepatic biliaryobstruction (w40% of control; Fig. 4).
Discussion
Severe dyslipoproteinemia is usually attributable tomonogenic disorders of key genes involved in lipoproteinmetabolism. Marked elevations in serum levels of LDL-C,characteristic of familial hypercholesterolemia, may becaused by mutations in the LDL-receptor (LDL-R) gene,its ligand apoB, proprotein convertase subtilisin/kexin 9(PCSK9), or the adaptor protein autosomal-recessive hyper-cholesterolemia (ARH).3,4 Carriers of these mutations typi-cally have an LDL-C level .95th percentile for age- andsex-matched subjects, whereas homozygotes (or compound

Figure 2 (A) Graphical presentation demonstrating TC and HDL-C level as a function of time during follow-up. Arrows indicate theperiod during which the patient was admitted to hospital with extreme hypercholesterolemia and HDL deficiency. (B) HPLC analysisof serum lipoprotein: I, Solid line represents pretreatment cholesterol levels, showing a high peek at VLDL position, reflecting Lp-(x)and a marked increase in LDL-C; II, broken line represents post-treatment normalized lipoprotein profile; III, dotted line represents serumpooled from control healthy, young female subjects.
Awan et al Acquired severe hypercholesterolemia and hypoalphalipoproteinemia 395
heterozygotes) have marked and severe elevations in serumlevels of LDL-C, often .15 mmol/L (580 mg/dL). Genesthat affect the metabolism of HDL also may cause markeddecreases in HDL-C. The most common genetic cause ofHDL-C deficiency is mutations in the ATP binding cassetteA1 (ABCA1). Other genes, such as APOA1, which codes forthe main structural lipoprotein of HDL, and several HDL-processing enzymes, may also cause HDL-C deficiency.5
In addition to genetic causes of dyslipoproteinemia, ac-quired forms are commonly encountered clinically. In Westernsociety, the most frequent form of dyslipidemia is associatedwith lifestyle, diet, obesity, and insulin resistance and isclustered in the components of the metabolic syndrome.6
Other metabolic disorders, especially hypothyroidism, maycause elevations in LDL-C. Several classes of medicationscan also cause lipoprotein disorders.7
This case demonstrates the multifactor etiology to acomplex lipoprotein disorder, highlighting the dramaticdyslipidemia that can result from combined hepatic andrenal disease. The presence of obesity and type 2 diabetes isassociated with mild-to-moderate hypertriglyceridemia andlow HDL-C. The concomitant presence of extrahepaticbiliary obstruction jaundice, hepatic cirrhosis, and thenephrotic syndrome caused an extreme phenotype of mas-sive hypercholesterolemia, characterized by elevations inboth Lp-(x) and LDL-C, and severe HDL-C deficiency(Fig. 2B).
Cholestatic jaundice is associated with the formation ofan abnormal lipoprotein, Lp-(x), that is characterized by ahigh content of phospholipids (w60 2 70% by weight) andunesterified cholesterol (w20 2 25%), a marked reductionin cholesteryl esters (,5%), and a low protein content

Figure 3 2D-PAGGE of serum, detecting apoA-I containing HDL species by anti-apoA-I iodinated antibody. (A) left panel: control sub-ject; right panel: patient serum sampled pretreatment when the serum cholesterol was 37 mmol/L and HDL-C was 0.13 mmol/L. A markedreduction in mature HDL species (a1-LpA-I) is noted, compared with control, characteristic of LCAT enzyme deficiency. A molecularweight ladder with particles ranging in size from 7.1 to 17 nm is shown. (B) Samples were separated as in (A). Patient serum was sampledafter treatment when the serum cholesterol was 5 mmol/L and HDL-C was 1.10 mmol/L. The after-treatment serum shows a marked in-crease in (a1-LpA-I) particles, consistent with recovery of LCAT function.
396 Journal of Clinical Lipidology, Vol 3, No 6, December 2009
(w5 2 10%).8–10 The association of Lp-(x) formation withcholestatic jaundice suggests an important role for bileacids in the formation of this abnormal lipoprotein. It hasbeen suggested that the reflux of bile into the plasma com-partment causes the formation of Lp-(x) in cholestasis as aresult of physicochemical process.9 Similarly; cirrhosis andextrahepatic biliary obstruction acted in concert in our pa-tient to produce Lp-(x).
Cirrhosis is associated with deficiency in LCAT activityand marked HDL deficiency.11 In turn, LCAT deficiency, as
Figure 4 LCAT assay; I, LCAT activity in serum pooled from normal cis used as a negative-control; III, LCAT activity in the patient pre-treatmthe patient after treatment; V, serum obtained from two subjects with genbackground activity.
seen here, is also associated with formation of Lp-(x) similarin structure to those observed in cholestatic jaundice.12
LCAT transfers an acyl chain from the R2 position of phos-phatidylcholine to the 30-hydroxyl residue of cholesterol, re-sulting in the formation of a cholesteryl ester. The markedHDL-C deficiency in the present case is attributed to partial,and reversible, LCAT deficiency (Fig. 4). A lack of formationof cholesteryl esters prevents the formation of mature HDLparticles (Fig. 3A and 3B), leading to rapid clearance of ‘‘im-mature’’ HDL-C in the kidneys. Furthermore, LCAT
ontrol subjects; II, in vitro inhibition of LCAT activity when DTNBent showing LCAT activity of 16% of control; IV, LCAT activity inetic LCAT deficiency; VI, negative control (no serum) to determine

Awan et al Acquired severe hypercholesterolemia and hypoalphalipoproteinemia 397
deficiency and subsequent accumulation of plasma Lp-(x) isassociated with spontaneous glomerulopathy.13
The association between nephrotic syndrome, hyperlip-idemia, and low HDL-C has been known for some time.14–16
The major lipoprotein abnormality in the nephrotic syn-drome is a marked, but reversible, elevation of LDL-C, whichmay approach levels observed in familial hypercholesterole-mia. The pathogenesis involves hepatic overproduction ofapoB-containing lipoproteins.14
The medical management of the dyslipidemia in circum-stances such as this one is a matter of debate. Because of therarity of such cases, it is nearly impossible to quantify thecardiovascular risk in these patients. There are data suggest-ing that Lp-(x) may not contribute to atherosclerosis.12 Thecardiovascular risk attributable to the increase in serumcholesterol is a function of the time of exposure and the sever-ity of the lipoprotein disorder. The use of lipid-loweringagents in this setting remains controversial. The presence ofliver enzyme abnormalities, coupled with deteriorating renalfunction, is a contraindication to the use of statins, fibrates,selective inhibitors of intestinal cholesterol absorption, andniacin. Bile acid binding resins are probably safe in thissetting but are of uncertain value as the etiology of the dysli-pidemia is predominantly secondary to hepatic production ofLp-(x) and LDL. Relief of biliary obstruction by papillotomyduring ERCP, stabilization of the electrolyte disorders and hy-perglycemia upon admission, and correction of the fluid statusled to dramatic improvements in renal function, a markeddecrease in proteinuria, and reversal of the extreme dyslipide-mia, returning lipid values to baseline (Fig. 2A). Therefore,the best approach in such cases of acquired metabolic dyslipi-demia remains the treatment of the underlying disorder(s).
Financial disclosures
Sources of financial support: Canadian Institutes ofHealth Research (CIHR) grant MOP 15042.
Acknowledgment
The authors would like to acknowledge and thankDr. Ramila Amre, FRCP(C), and Dr. Khurram Sher, MD,
of the Division of Anatomical Pathology at the McGillUniversity Health Center for their expertise.
References
1. Krimbou L, Marcil M, Davignon J, Genest J. Interaction of lecithin:-
cholesterol acyltransferase (LCAT)-alpha 2-macroglobulin complex
with low density lipoprotein receptor-related protein (LRP). Evidence
for an alpha 2-macroglobulin/LRP receptor-mediated system partici-
pating in LCAT clearance. J Biol Chem. 2001;276:33241–33248.
2. Chen CH, Albers JJ. Characterization of proteoliposomes containing ap-
oprotein A-I: a new substrate for the measurement of lecithin:cholesterol
acyltransferase activity. J Lipid Res. 1982;23:680–691.
3. Marais A. Familial hypercholesterolaemia. Clin Biochem Rev. 2004;
25:49–68.
4. Horton J, Cohen J, Hobbs H. Molecular biology of PCSK9: its role in
LDL metabolism. Trends Biochem Sci. 2007;32:71–77.
5. Miller M, Zhan M. Genetic determinants of low high-density lipoprotein
cholesterol. Curr Opin Cardiol. 2004;19:380–384.
6. Brien S, Katzmarzyk P. Physical activity and the metabolic syndrome
in Canada. Appl Physiol Nutr Metab. 2006;31:40–47.
7. Alwaili K, Alrasadi K, Awan Z, Genest J. Approach to the diagnosis
and management of lipoprotein disordersq. Curr Opin Endocrinol
Diabetes Obes. 2009;16:132–140.
8. Miller J. Dyslipoproteinaemia of liver disease. Baillieres Clin Endocrinol
Metab. 1990;4:807–832.
9. Soros P, Bottcher J, Maschek H, Selberg O, Muller M. Lipoprotein-X
in patients with cirrhosis: its relationship to cholestasis and hypercho-
lesterolemia. Hepatology. 1998;28:1199–1205.
10. Seidel D, Alaupovic P, Furman R. A lipoprotein characterizing
obstructive jaundice. I. Method for quantitative separation and identi-
fication of lipoproteins in jaundiced subjects. J Clin Invest. 1969;48:
1211–1223.
11. DeMartiis M, Barlattani A, Parenzi A, Sebastiani F. Pattern of lecithin-
cholesterol-acyltransferase (L-CAT) activity in the course of liver
cirrhosis. J Intern Med Res. 1983;11:232–238.
12. Sorokin A, Brown J, Thompson P. Primary biliary cirrhosis, hyperlip-
idemia, and atherosclerotic risk: a systematic review. Atherosclerosis.
2007;194:293–299.
13. Zhu X, Herzenberg A, Eskandarian M, et al. A acyltransferase
(LCAT)-deficient mouse expressing predominatly LpX is associated
with spontaneous glomerulopathy. Am J Pathol. 2004;165:1269–1278.
14. Kronenberg F. Dyslipidemia and nephrotic syndrome: recent advances.J Ren Nutr. 2005;15:195–203.
15. Vaziri N, Liang K, Parks J. Acquired lecithin-cholesterol acyltransfer-
ase deficiency in nephrotic syndrome. Am J Physiol Renal Physiol.
2001;280:F823–F828.
16. Joven J, Villabona C, Vilella E, Masana L, Alberti R, Valles M.
Abnormalities of lipoprotein metabolism in patients with nephrotic
syndrome. N Engl J Med. 1990;323:579–584.