Embed Size (px)
Citation preview

Acquired isodisomy of chromosome 21 in an acute myeloid leukaemia (AML) patient as an incidental finding during routine chimaerism
analysis, and the introduction of a new RUNX1 screening service.
Joanne Mason, Registered Clinical Scientist
West Midlands Regional Genetics Laboratory,
Birmingham Women’s NHS Foundation Trust,

Joanne Mason, WMRGL Birmingham
Introduction• AML is a genetic disease
• Characterised by enhanced proliferation & differentiation block
• ~50% cases have cytogenetically visible aberrations
• The remaining cases have genetic aberrations which are only detectable at the molecular level
• These genetic lesions help to characterise the subtype of leukaemia, and can be used to guide therapeutic decisions and inform prognosis
• Molecularly-targeted therapy (e.g. Glivec in CML)

Joanne Mason, WMRGL Birmingham
Patient A
• Diagnosed with AML in May 2006• Karyotype analysis: trisomy 13 (47,XY,+13 [10])• Treated with chemotherapy on the MRC AML15
trial protocol
• Relapsed November 2007 (47,XY,+13)• Salvage chemotherapy, followed by stem cell
transplant (SCT) in March 2008

Joanne Mason, WMRGL Birmingham
Chimaerism monitoring post-SCT• Sex-matched SCT patients are monitored for levels of
donor and host DNA post-transplant using polymorphic microsatellite markers.
• A pre-requisite for chimaerism analysis is to find at least one informative marker that distinguishes donor from host.
CAGA CAGA 3-15 CAGA CAGA CAGA

Joanne Mason, WMRGL Birmingham
Multiplex microsatellite marker PCR and subsequent fragment analysis

Joanne Mason, WMRGL Birmingham
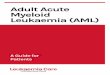
Chimaerism analysis
POST-TRANSPLANT
74% donor26% host
HOST PRE-TRANSPLANT
DONOR

Joanne Mason, WMRGL Birmingham
01000020000
30000400005000060000700008000090000
100000110000120000130000
100 150 200 250 300 350 400 450 500
Dy
e
Si
gn
al
Size (nt)
133.21134
D21S1437241.36
241D21S11
245.43246
D21S11
257.62258
D21S11
309.79310
D21S1270
311.85312
D21S1270
327.89328
D21S1270
398.40399
D13S634
415.55416
D13S634
490.06490
D18S535
494.22494
D18S535
0
5000
10000
15000
20000
25000
30000
35000
40000
45000
100 150 200 250 300 350 400 450 500
Dy
e
Si
gn
al
Size (nt)
160.95161
D18S391
246.01246
D13S742
268.35268
D13S742
289.26289
D13S742
379.82380
D18S386 443.85444
D13S305
451.61452
D13S305
0
2500
5000
7500
10000
12500
15000
17500
20000
100 150 200 250 300 350 400 450 500
Dy
e
Si
gn
al
Size (nt)
105.23105
AMEL
111.00111
AMEL
145.93146
D18S1371
150.04150
D18S1371
308.04307
D21S1411
462.61462
D13S628
464.57464
D13S628
Microsatellite results
• Pre-transplant DNA
13 13
13
0
10000
20000
30000
40000
50000
60000
70000
80000
90000
100000
110000
120000
130000
100 150 200 250 300 350 400 450 500
Dy
e
Si
gn
al
Size (nt)
241.36241
D21S11
245.43246
D21S11
257.62258
D21S11

Joanne Mason, WMRGL Birmingham
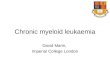
Chromosome 21 markers
Average ratio 4:1
D21S11
Penta D
D21S1411
D21S1270
Remission DNA
Relapse DNA

Joanne Mason, WMRGL Birmingham
• Possible explanations for the discrepancy:
– 1) Sub-microscopic deletion within chromosome 21 (unlikely as multiple deletions would be required)
– 2) A cryptic sub-clone with gain or loss of 21 in some cells, not detected by initial cytogenetic analysis (impossible with a microsatellite ratio of 4:1)
Ch 21 markers : copy number change?
Cytogenetics 2 normal copies Ch 21
– 3) Acquired isodisomy (aka acquired uniparental disomy, or copy number neutral loss of heterozygosity)

Joanne Mason, WMRGL Birmingham
Acquired isodisomy (AID)
• Common mechanism of oncogenesis
• Prognostic significance in AML?

Joanne Mason, WMRGL Birmingham
Mitotic Recombination
21 21
AID 21

Joanne Mason, WMRGL Birmingham
Acquired isodisomy (AID)
• AID is a mechanism by which homozygosity for a mutation can be achieved without detrimental loss or gain of contiguous chromosome material
• It is cytogenetically invisible (both chromosomes look the same) and therefore very difficult to detect unless you specifically look for it.
• DNA microarrays – sub-microscopic & cryptic changes

Joanne Mason, WMRGL Birmingham
AID21: What genes might be affected?
• RUNX1 21q22.3• Transcription factor• Most frequent target for chromosomal
translocation in leukaemia
• Point mutations – in sporadic AML – In familial platelet disorder/AML (FPD/AML)

Joanne Mason, WMRGL Birmingham
RUNX1 point mutations in sporadic AML
• 1.2% of all AML
• Highly associated with
– AML FAB M0
– trisomy 21
– trisomy 13 (80-100%) [Patient AS 47,XY,+13]
• RUNX1 mutation associated with a poor prognosis in MDS (prognosis in AML not yet known)
• Discovery of mutations has implications for – Risk adapted therapy– Molecularly targeted therapy

Joanne Mason, WMRGL Birmingham
Familial Platelet Disorder with Predisposition to Acute Myeloid Leukaemia (FPD/AML)
• Rare autosomal dominant disorder• Characterised by inherited thrombocytopenia,
platelet function defect and a lifelong risk of myelodysplastic syndrome (MDS) and AML
• Caused by heterozygous germline mutations in RUNX1
• Worldwide, only fifteen pedigrees have been reported to date.
• In November 2008, request for ?FPD/AML in a West Midlands AML patient.

Joanne Mason, WMRGL Birmingham
RUNX1 Point Mutations
• RUNX1 mutation screening service– AID21 patient – AML cases with a strong association with
RUNX1 mutations (FAB M0, +13)– FPD/AML patient
• Sequencing of the entire coding region

Joanne Mason, WMRGL Birmingham
RUNX1 mutation screening service
• cDNA template• PCR under same conditions (‘touchdown PCR’)• M13 tag to facilitate high-throughput sequencing
a
b
c
d
Primer sequences courtesy of Dicker et al, Leukemia 2007

Joanne Mason, WMRGL Birmingham
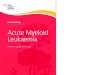
RUNX1 sequencing results.....so far
• Patient A: p.Asp171Gly (D171G, homozygous)• DNA binding domain
• Previously reported in two AML patients
• 26% of mutations in RUNX1 are homozygous (wild-type RUNX1 is lost)
Wild-type
Patient AS

Joanne Mason, WMRGL Birmingham
• SNP-based DNA microarrays to investigate cytogenetically cryptic areas of somatically acquired homozygosity (AID)
• Postulated that such regions contain homozygous mutations in genes known to be mutational targets in leukaemia.
• In 7 of 13 cases with acquired isodisomy, homozygous mutations were identified at four distinct loci (WT1, FLT3, CEBPA, and RUNX1)
• The mutation precedes mitotic recombination, which acts as a "second hit" responsible for removal of the remaining wild-type allele.

Joanne Mason, WMRGL Birmingham
RUNX1 sequencing results.....so far
• ?FPD/AML patient and three AML patients with trisomy 13 (i.e. highly likely to have RUNX1 mutations)
• Patient B AML 47,XX +13– p.Val137_Gly138insThr
wt
B
wt
C
• Patient C AML 50,XY +8,+9,+13,+21– p.Met25Lys– p.Arg135Lys
• All de novo, but two other mutations involving arginine 135 have been reported before

Joanne Mason, WMRGL Birmingham
Further work
• Complete the sequence analysis of all four fragments comprising the coding region of RUNX1
• Effect of mutations?
– Inheritance pattern in familial cases
– Confirm RUNX1 mutations are acquired and not constitutional by sequencing stored remission DNA

Joanne Mason, WMRGL Birmingham
Summary
Unexpected microsatellite pattern in pre-transplantDNA taken at relapse
Molecular data + cytogenetic data = acquired isodisomy 21
Candidate gene = RUNX1
RUNX1 mutation D171G
Sequencing service for other sporadic AML patients,and for suspected FPD/AML referrals.

Joanne Mason, WMRGL Birmingham
Acknowledgements
• Birmingham, WMRGL:– Val Davison– Mike Griffiths– Fiona Macdonald– Susanna Akiki– Paula White– Natalie Morrell– Charlene Crosby
• Birmingham Clinicians:– Dr Prem Mahendra– Prof Charlie Craddock
Thank you for your attention