Embed Size (px)
Citation preview
ACQUIRED IMMUNODEFICIENCY SYNDROME / AIDS
Abhishek Jha
WHAT IS AIDS? Disease caused by the retrovirus human immunodeficiency
virus(HIV) and characterized by profound immunosuppression that leads to opportunistic infections, secondary neoplasm and neurologic manifestations.
Secondary(acquired) Immunodeficiencies
HIV is transmitted primarily via unprotected sexual intercourse, contaminated blood transfusions, hypodermic needles, and during pregnancy, delivery, or breastfeeding. Some bodily fluids, such as saliva and tears, do not transmit HIV
EPIDEMIOLOGY & STATISTICS Since its discovery in 1981, AIDS has increased
to epidemic proportions.According to the National Centers for Disease
Control and Prevention (CDC), 42 million people are estimated to be living with HIV/AIDS. Of these, 38.6 million are adults, 19.2 million are women, and 3.2 million are children under 15.
Genetic research indicates that HIV originated in west-central Africa during the late nineteenth or early twentieth century HIV/AIDS has had a great impact on society, both as an illness and as a source of discrimination.
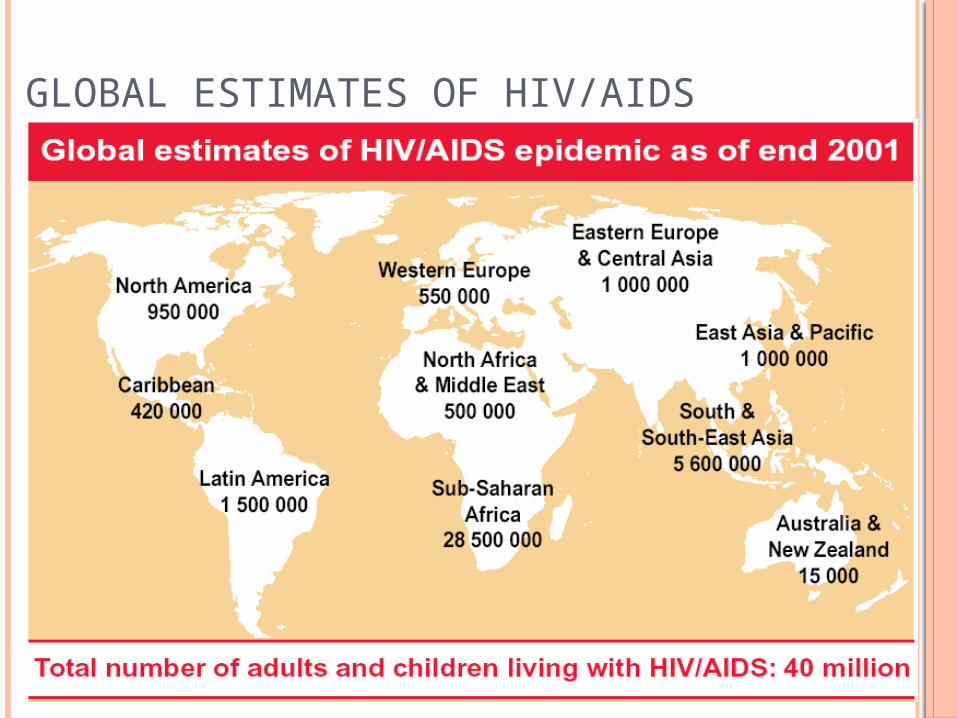
GLOBAL ESTIMATES OF HIV/AIDS
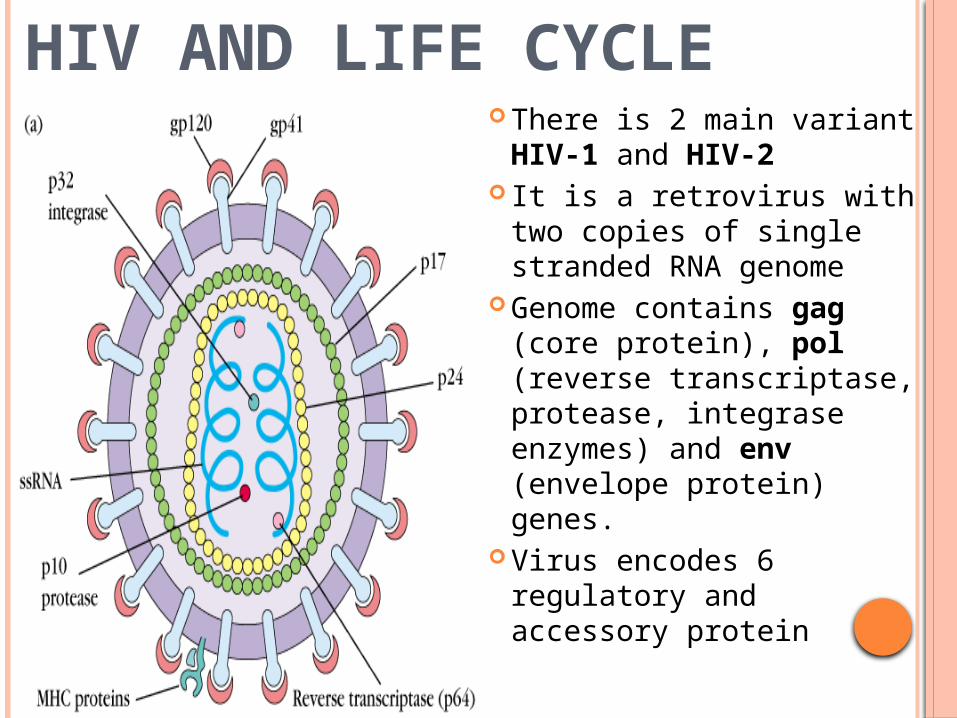
HIV AND LIFE CYCLE There is 2 main variant
HIV-1 and HIV-2 It is a retrovirus with two
copies of single stranded RNA genome
Genome contains gag (core protein), pol (reverse transcriptase, protease, integrase enzymes) and env (envelope protein) genes.
Virus encodes 6 regulatory and accessory protein
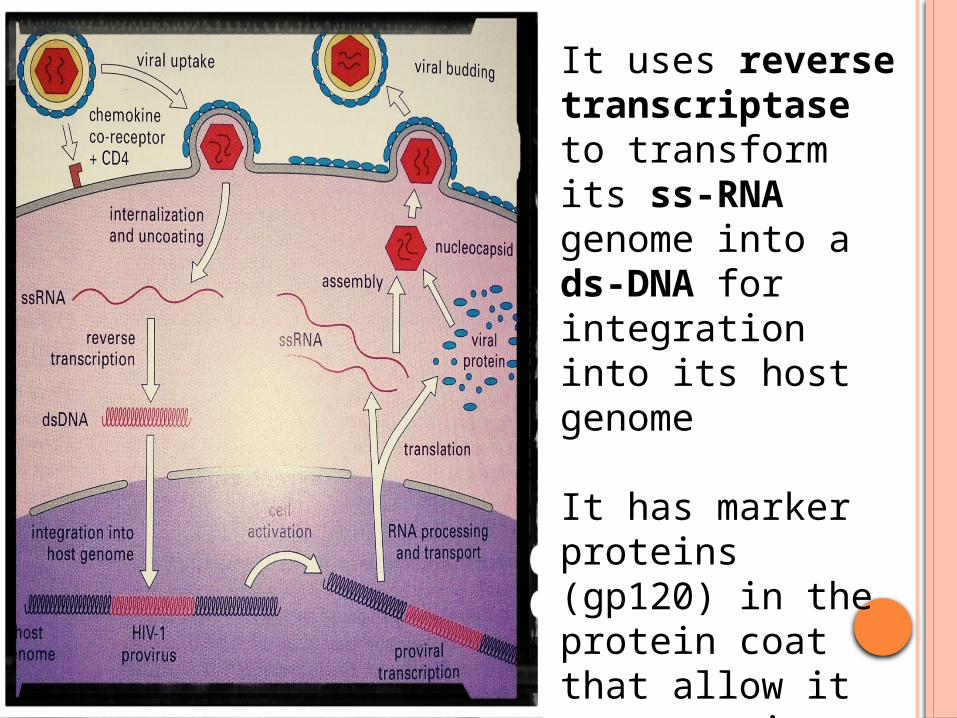
It uses reverse transcriptase to transform its ss-RNA genome into a ds-DNA for integration into its host genome
It has marker proteins (gp120) in the protein coat that allow it to recognize specific cells in the human body
The protein coat also contains MHC-I and MHC-II molecules
COMPLETE ACTIVATION OF HIV
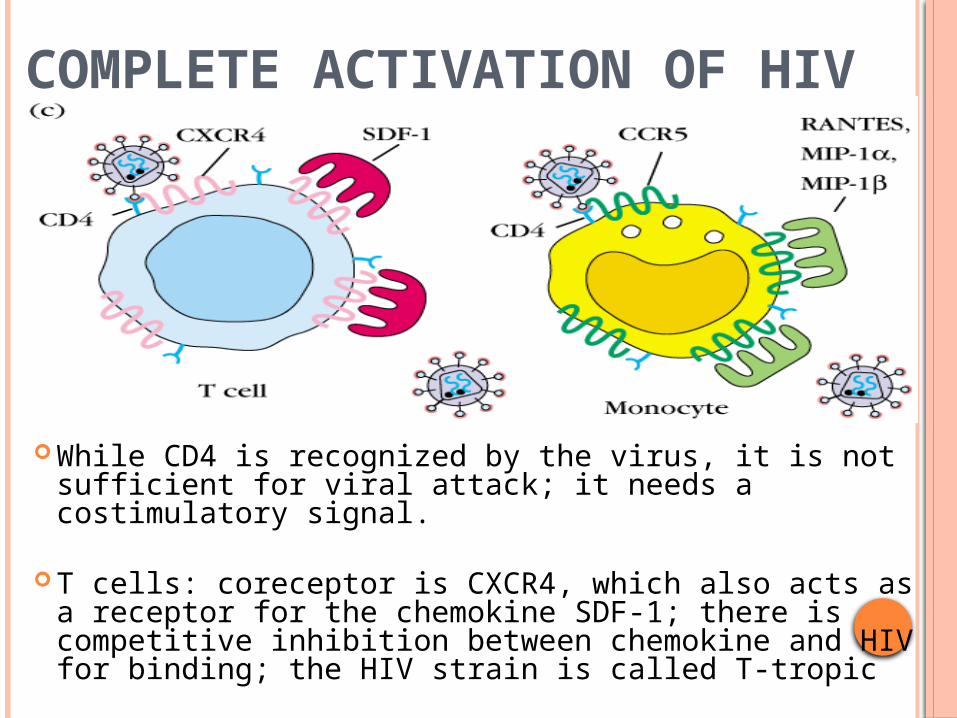
While CD4 is recognized by the virus, it is not sufficient for viral attack; it needs a costimulatory signal.
T cells: coreceptor is CXCR4, which also acts as a receptor for the chemokine SDF-1; there is competitive inhibition between chemokine and HIV for binding; the HIV strain is called T-tropic
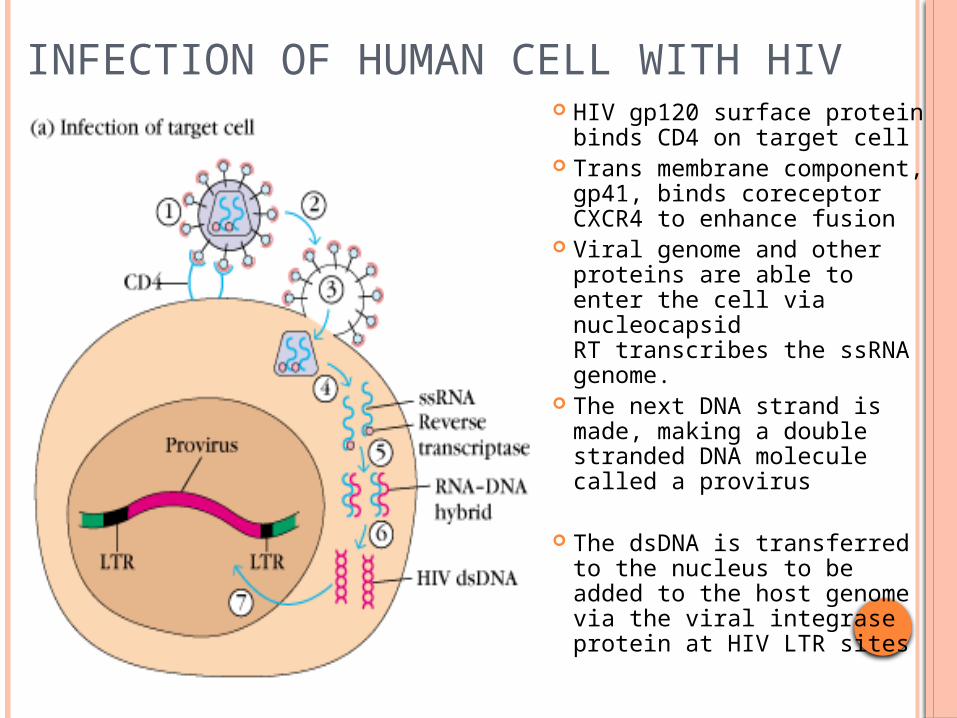
INFECTION OF HUMAN CELL WITH HIV HIV gp120 surface protein
binds CD4 on target cell Trans membrane
component, gp41, binds coreceptor CXCR4 to enhance fusion
Viral genome and other proteins are able to enter the cell via nucleocapsidRT transcribes the ssRNA genome.
The next DNA strand is made, making a double stranded DNA molecule called a provirus
The dsDNA is transferred to the nucleus to be added to the host genome via the viral integrase protein at HIV LTR sites
Co receptor facilitate the tight binding of the virus to the cell membrane and induce conformational change in the viral envelope glycoproteins .
Mostly helper T cells ( TH cells) and sometimes monocytes macrophages ,Nk cells, certain B cells and glial cells are target for HIVDuring infection , the virus infects TH cells within local mucosal surfaces infecting local lymphoid tissues.
The virus quickly disseminates systemically infecting remote lymphoid tissues as well as the glial cells . Then the virus quickly appears in genital secretions.
Within weeks of initial infection , virus specific cytotoxic T cells appear in the peripheral blood and lymphoid tissues.
After short period , neutralizing antibodies may be detected in the plasma and virus replication process is initiated in this process.
Hosts develop an adequate immune response to the virus . However reverse transcriptase makes very high replication error ( 1 in 10000 bases copied) .
So that HIV progeny virus mutates in each replication cycle ,thus HIV infected cells persists in lymph nodes.
Infected cells can be killed directly by virus replication or indirectly by virus specific effector mechanisms.
After several months of infection , a balance is established among virus replication , immune effector mechanisms and cells available for virus replication , and the infection enters its chronic phase during which the patient is generally asymptomatic.
Rapid viral replication is accompanied by a marked drop in the number of circulating CD4+ T cells
99 % virus replication occurs in CD4+ T cells in lymphoid organs and 1% virus replication occurs in monocytes and resting CD4+ T cells.
When CD4+ T cells decline below 200 cells/µl ,infections with variety of opportunistic microbes occur.
The risk of opportunistic infections ( OIs) and malignancies are high when CD4 T cells is below 50 cells/µl .
The rate of immunologic and clinical progression is directly related to the extent of virus replication and varies considerably from individual to individual
HIV INFECTED T-CELL
SIGN AND SYMPTOMS Brief flu-like illness two to four weeks after becoming infected.
Signs and symptoms may include: Fever, Headache, Sore throat, Swollen lymph glands, Rash,
Diarrhea , Weight loss The development of an opportunistic infection — an
infection that occurs when your immune system is impaired — such as Pneumocystis carinii pneumonia (PCP)
A CD4 lymphocyte count of 200 or less — a normal count ranges from 800 to 1,200 which causes
Soaking night sweats , Dry cough and shortness of breath
Shaking chills or fever higher than 100 F (38 C) for several weeks
Persistent white spots or unusual lesions on tongue or in face
Persistent headaches, Blurred and distorted vision ,Persistent fatigue , Swelling of lymph nodes for more than three months
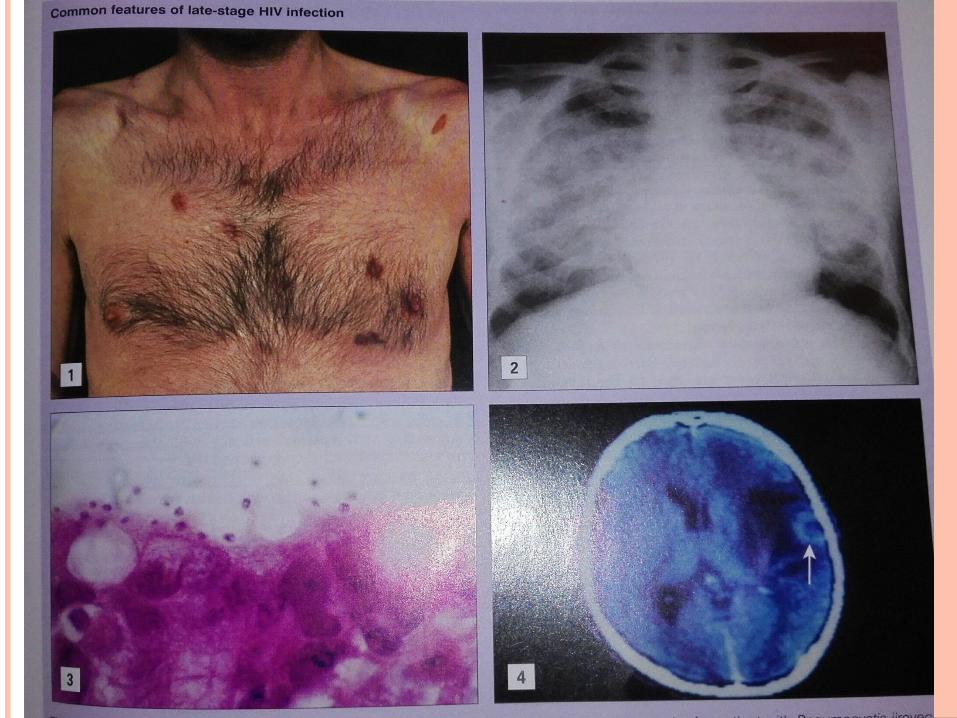
There is more likely to develop certain cancers, especially Kaposi's sarcoma, cervical cancer and lymphoma
Symptoms of HIV in children :Children who are HIV-positive may experience:
Difficulty gaining weight Difficulty growing normally Problems walking ,Delayed mental development Severe forms of common childhood illnesses such as
ear infections (otitis media), pneumonia and tonsillitis
TESTING FOR HIV Enzyme-linked immunosorbent assay (ELISA). This
screening test is usually the first test used to detect infection with HIV. If antibodies to HIV are present (positive result), the test is usually repeated.
Western blot. This test requires high technical skills. It is more difficult than the ELISA to perform and interpret accurately, but it is less likely to give a false-positive result because it can distinguish HIV antibodies from other antibodies that may react to the ELISA. A Western blot is usually done to confirm the results of two positive ELISA tests.
Indirect fluorescent antibody (IFA). This test also detects antibodies made to fight an HIV infection. Like a Western blot test, it is used to confirm the results of an ELISA.
Polymerase Chain Reaction (PCR). This test detects the RNA of HIV, rather than detecting antibodies to HIV. Therefore, PCR can reveal an HIV infection before antibodies can be detected. PCR can also accurately determine whether a baby born to an infected mother has HIV.
TREATMENTHAART: Highly Affective Anti-Retro Viral Therapy: Physicians consider 200 to 350 CD4 cells/mm3 as the range to consider . HAART combines two types of antiretroviral drugs
RTI’s (Reverse Transcriptase Inhibitors): Type 1: NRTI’s – nucleoside drugs provide faulty DNA building blocks, stopping the DNA chain the virus uses to make copies of itself.
Type 2: NNRTI’s- non-nucleoside RT inhibitors bind RT so the virus cannot carry out its copying function
NNRTI’s (Non-Nucleoside RTI’S) : Delavirdine, Nevirapine, Efavirenz
Protease Inhibitors: Indinavir, Ritonavir
WHAT DOES THE FUTURE HOLD? Scientists are working on more potent protease
inhibitors, less toxic RT inhibitors, as well as 2 new classes of drugs:
*Fusion Inhibitors- Drugs which act to block HIV before it enters the human immune cell. This class of drugs works to stop HIV replication at an earlier stage.
*Integrase Inhibitors- Aim to block the integration of the virus’s DNA into the cell’s chromosome. 2 different integrase inhibitors are currently in human trials.