Embed Size (px)
Citation preview

Acquired Esotropia in Acquired Esotropia in a middle aged female a middle aged female
myopemyope
NOSA 2004NOSA 2004
Mark Donaldson &Lionel Kowal, Mark Donaldson &Lionel Kowal, Ocular Motility Clinic, RVEEHOcular Motility Clinic, RVEEH
Jenni Sorraghan, Optometrist, Jenni Sorraghan, Optometrist, Shepparton Shepparton

Case ReportCase Report
51 yo WCF
6 y progressive esotropia and hypotropia
POHx - Left anisomyopic amblyopia
- no known neurological / orbital disease
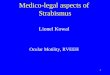
Examination findingsExamination findings
VA. R = 6/12 L = HMRefr R = -0.50-1.00 x 175 L = - 40 (ret)
EOM 27 L ET12 L hypotropia
Reduced Abduction & Elevation LE
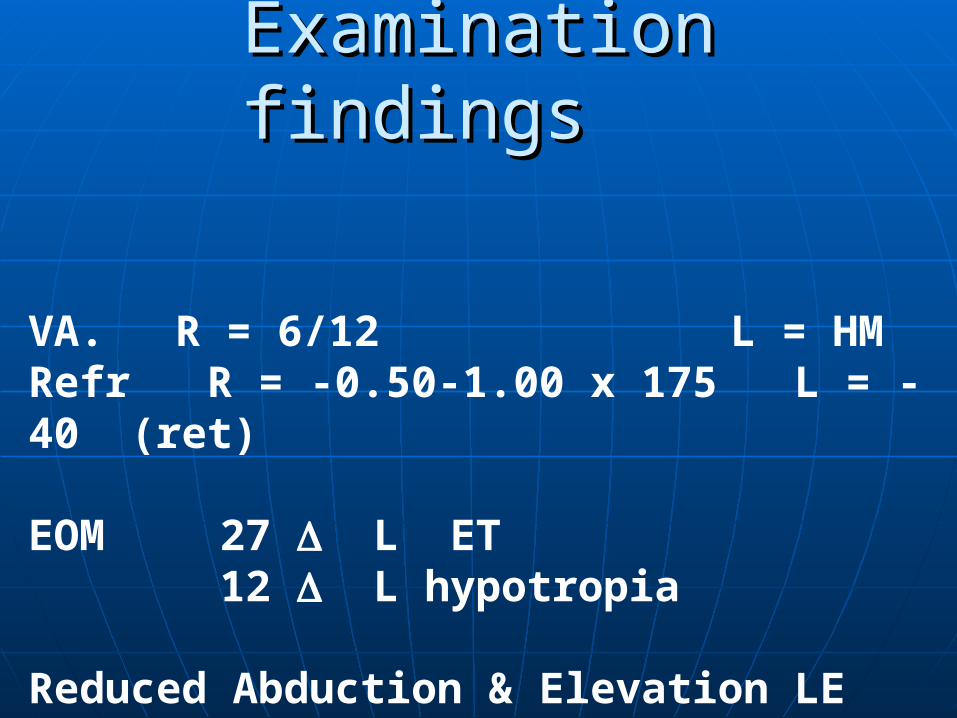
Pre-op PhotosPre-op Photos
Poor elevation
L ET & hypo

For neurologists onlyFor neurologists only
What now?What now?

Axial length L 35 mm
Normal LLR
No intracranial path
Inf displacement LLR
Nasal displacement LSR
SR/LR angle = 135 deg

For Ophthalmologists and For Ophthalmologists and neurologistsneurologists
What is this?What is this?

Large Angle Esotropia with High Large Angle Esotropia with High Myopia Myopia Heavy Eye SyndromeHeavy Eye Syndrome
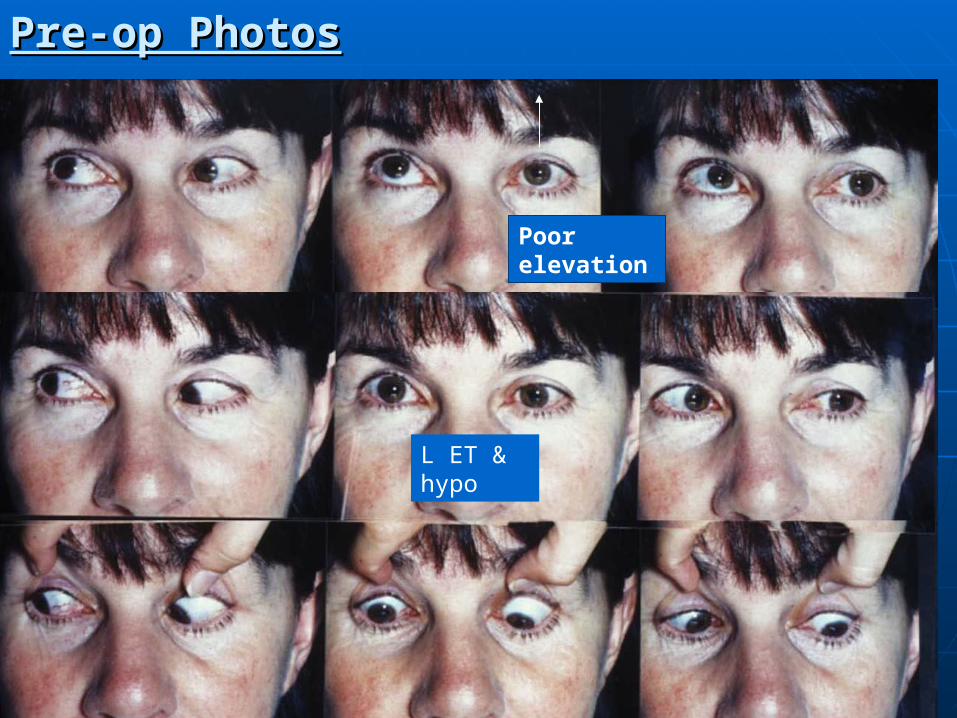
Progressive enlargement of myopic globe after orbital growth has finished
Globe appears to prolapse / herniate between superior and lateral recti ?orbital septum weakest here
Abnormal LR/SR position abnormal function
Result: Large angle esotropia with hypotropia
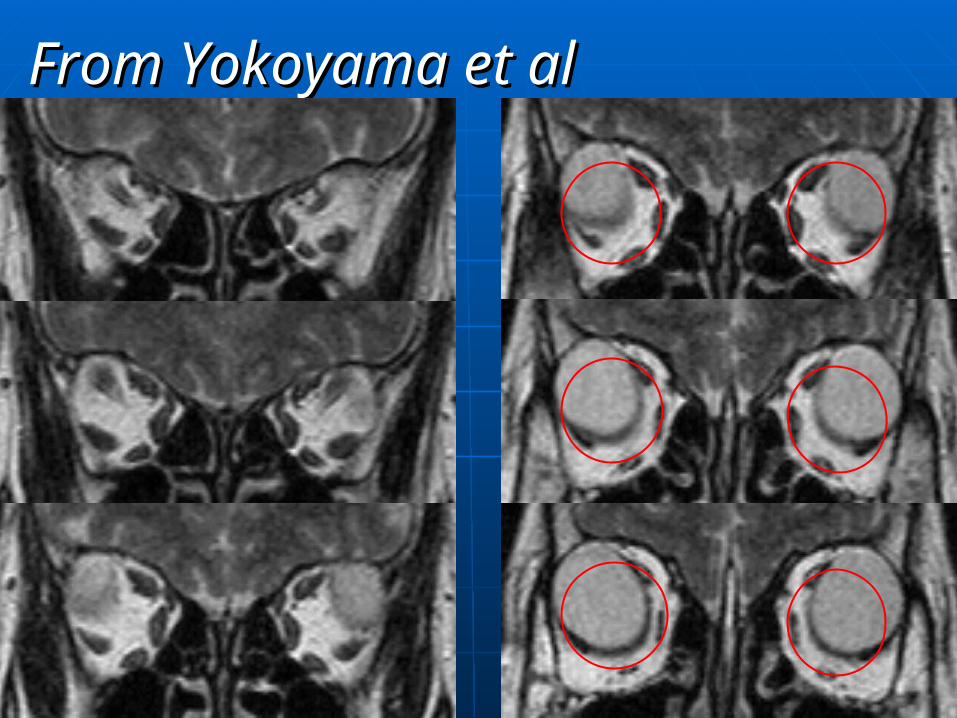
From Yokoyama et alFrom Yokoyama et al

From Yokoyama et alFrom Yokoyama et al
normal
New abnormal SR vector - elevates less well& adducts
New abnormalLR vector & ANTI- ELEVATOR
Normal SR vector

Large Angle ET + High Myopia Large Angle ET + High Myopia
Heavy Eye SyndromeHeavy Eye Syndrome[not really heavy][not really heavy]
Inferior displacement of lateral rectus
i) Reduced abducting force of the lateral rectus
ii) LR restricts elevation

Surgical managementSurgical management
‘Yokoyama procedure’
Join LR & SR 15mm behind limbus with permanent suture
Elevates the LRAbducts the SR
Makes their function more normal
Post operative Post operative photosphotos
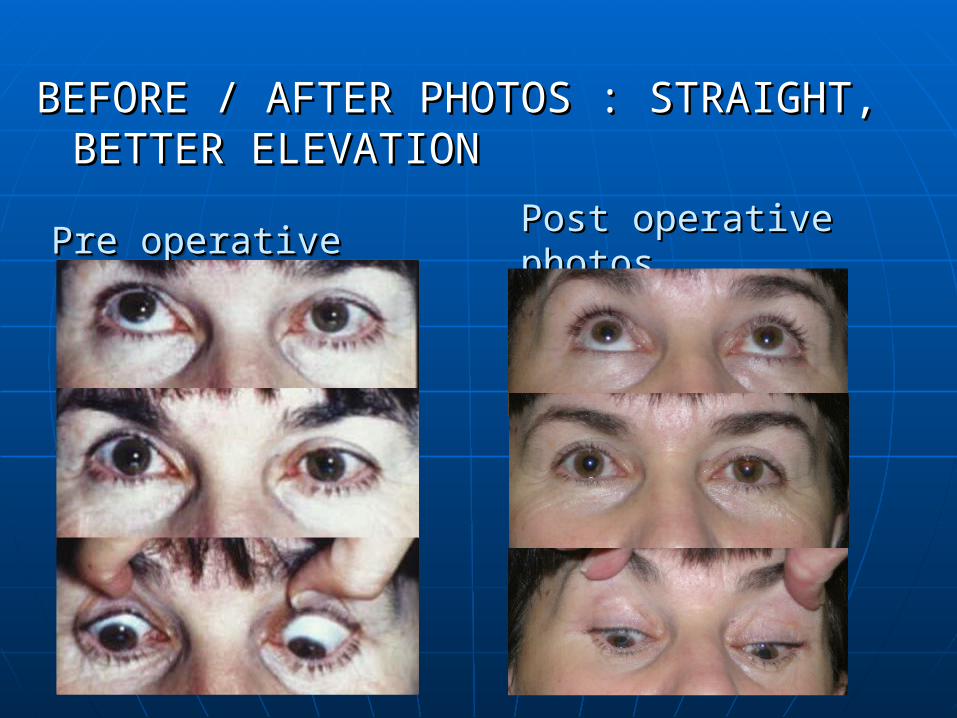
BEFORE / AFTER PHOTOS : STRAIGHT, BEFORE / AFTER PHOTOS : STRAIGHT, BETTER ELEVATIONBETTER ELEVATION
Pre operative Pre operative Pre operative Pre operative

Post operative photosPost operative photos

Conclusions:Conclusions: Large Angle Esotropia with High Myopia Large Angle Esotropia with High Myopia(Heavy Eye Syndrome)(Heavy Eye Syndrome)
Unusual mechanism of acquired esotropia [with hypo] in a uni- or bi- lateral myope : acquired change in orbital anatomy and muscle mechanics
Distinctive pathophysiology which dictates a logical and [usually] effective treatment

Conclusions:Conclusions: Large Angle Esotropia with High Myopia Large Angle Esotropia with High Myopia(Heavy Eye Syndrome)(Heavy Eye Syndrome)
Thank you