Embed Size (px)
Citation preview

L
Asa
igdmiaarcapgmlApvtt
EpCl2e(pwlHHwabwfTpb6cpHBt
0d
Leukemia Research 35 (2011) e203– e205
Contents lists available at ScienceDirect
Leukemia Research
jo ur nal homep age: www.elsev ier .com/ locate / leukres
occur much earlier in MDS patients and does not such a nega-
etter to the Editor
cquired alpha thalassemia myelodyslastic/myeloproliferativeyndrome (ATMDS): Evolution on hypomethylating agent ther-py
Acquired alpha thalassemia myelodyslastic syndrome (ATMDS)s a rare syndrome associated with somatic point mutation in ATRXene in patients with myeloproliferative or myelodysplastic syn-rome. The ATRX protein is a chromatin associated protein whichay act as a transcriptional cofactor and plays an important role
n the epigenetic regulation of gene expression in particular onlpha globin gene [1]. A possible role of ATRX in carcinogeneis haslso been suggested, and altered ATRX expression levels have beeneported in gene expression profiling experiments using variousancer cells lines and a low expression of ATRX was correlated with
poor clinical outcome in de novo AML [2]. The majority of studiesublished about ATMDS focused on down regulation of alpha globinene, and there are few reports on the prognostic value of ATRXutation in the context of MDS. Moreover, up to now, hypomethy-
ating agent therapy has been reported in only one patient withTMDS and during a short period [3]. We described a patient whoresents a chronic myelomonocytic leukemia (CMML) occurringery lately after the presence of a non sens mutation in the 3′ exon ofhe ATRX gene, and we reported CMML evolution on 5 azacytidineherapy.
A 72-year-old man with no medical history and of northernuropean origin presented chronic fatigue in 2002. He was slightlyale. Physical examination was unremarkable (no splenomegaly).omplete blood count showed: Hb 10.2 g/dL, mean corpuscu-
ar volume (MCV) 67fl, mean corpuscular hemoglobin (MCH)0 pg, peripheral blood smear showed microcytic and hypochromicrythrocytes with marked aniso poikilocytosis and target cellsFig. 1A). Leucocytes count was 4810/�L, monocytes 600/�L, lym-hocytes 2700/�L, polynuclear neutrophil 1500/�L, platelet countas 105,000/�L. C reactive protein, fibrinogen, and serum ferritin
evel were normal. Reticulocytes count was 2.65% (130,000/�L).emoglobin electrophoresis showed a band consistent with Hb
comprising 7.3% of total Hb (Fig. 1D), the presence of Hb Has confirmed by isoelectric focusing. Despite the absence of
lpha thalassemia trait in the family and the presence of throm-ocytopenia, an erroneous diagnosis of hemoglobin H diseaseas made at this time. Three complete blood counts were per-
ormed during the 4-year follow up and were almost identical.hen the patient was lost to follow up for 3 years. In 2009 heresented again with a 3-month history of fatigue. The completelood count showed: Hb 9.4 g/dL, mean corpuscular volume (MCV)6fl, mean corpuscular hemoglobin (MCH) 21.8 pg. Leucocytesount was 14,500/�L, monocytes 3770/�L, lymphocytes 5220/�L,olynuclear neutrophil 5365/�L, platelet count was 124,000/�L.
emoglobin electrophoresis showed Hb H band comprising 5.4%.rilliant cresyl blue supra vital stain of the peripheral blood showedhat 20% of the red cells contained Hb H inclusions (Fig. 1C).145-2126/$ – see front matter. Crown Copyright © 2011 Published by Elsevier Ltd. All rioi:10.1016/j.leukres.2011.07.010
Molecular studies done to find out a mutation in alpha globincluster included the search for the most frequent deletions orpoint mutations using: (i) a specific reverse dot blot p kit (Vien-nalab �-Globin Strip AssayTM, Vienna, Austria) and (ii) the directsequencing of �1 and �2 genes to screen for rare � non dele-tional �-thal traits. An in-depth study of the �-locus to searchfor rare deletions was done using Multiplex Ligation-dependentProbe Amplification (MLPA) methods (MRC-Holland Salsa MLPA p-140B kit Hb A, Amsterdam, The Netherland). No rearrangement ofthe alpha globin cluster and no point mutations were detected bythis procedure. Denaturing high performance liquid chromatog-raphy of the entire coding region of the ATRX gene performedon PMB cell showed an abnormal pattern in exon 36 and thesequence analysis of bone marrow DNA cells identified a C to Ttransition in codon 2407 (Fig. 1E). No mutation was seen usingthe same technique on non hematopoietic cells (cells of hair fol-licle). Bone marrow aspiration showed a hyper cellular marrow(95%) with left-shifted granulopoiesis, erythroid hyperplasia withnormoblastic maturation and an inverted myeloid: erythroid ratio,monocytosis (confirmed by esterase staining, immunochemistrywith CD68), dys-megakaryocytopoiesis and excess in undifferenti-ated myeloblasts evaluated 10% (Fig. 1B). Ringed sideroblasts werenot observed. The diagnosis was consistent with WHO-definedCMML, subtype II (10–20% blasts); karyotype was normal 46, XYin 20 cells. The patient also exhibited a mutation in ASLX genein exon 12 (dupG + deletion of 23 bp → G646WfsX12 + E635RfsX15)(Fig. 1F) and a mutation in TET2 gene in exon 3 (mutation Q1030X)codon stop and two SNP (G355D, P363L) (Fig. 1G). There were nomutations in AML1, FTL3, N and K RAS, CBL genes. In December2009, because the patient exhibited anaemia (Hb8,9) and hyperleu-cocytosis (leucocytes count was 23,800/�L, monocytes 7300/�L),hypomethylating agents therapy with 5 azacytidine 75 mg/kg/d(for 5 days for patient convenience) every 21 days was started. Evo-lution on therapy of Hemoglobin level, mean corpuscular volume,leukocytes, monocytes and platelets count and bone marrow blastcount are reported in Table 1 and shows a stability of disease over12 months. Molecular analysis showed the persistence of ATRX,TET2, ASLX mutations after 6 cycles. The transfusion requirementwas stable on therapy 8 PRBBC every six months. The patient diedin November 2010 on therapy of an unrelated cause.
1. Discussion
We could reasonably argue that ATRX mutation had beenpresent since 2002 given the red cell phenotype and the presenceof Hb H, and that CMML appeared secondary (from at least four toseven years later). Our case illustrates that ATRX mutation could
tive prognosis value as previously suggested. This case could alsosuggested that the role of mutated ATRX gene in the epigenetic reg-ulation of genes expression seems to be more pronounced or faster
ghts reserved.

e204 Letter to the Editor / Leukemia Research 35 (2011) e203– e205
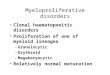
Figure 1. (A) Patient’s peripheral blood smear (May-Grünwald Giemsa Staining, 1000×) demonstrating aniso poikylocytosis, hypochromic and targets cells. (B) Bone marrowaspirate (May-Grûnwald Giemsa 1000×) showing global dysmyelopoiesis with excess of blasts. (C) Supra vital staining with brilliant cresyl blue method, showing Hb H “golfball” inclusions in about 20% of erythrocytes. (D) Chromatogram of Hb H determined by HPLC �-thal Short Program (Variant I BIORAD). (E) ATRX exon 36 sequencing: lane(a): DNA from blood cells and lane (b): DNA from bone marrow cells: C to T transition in codon 2407; lane (c): DNA form hair root cells: no mutation. (F) ASXL1 mutation:E635RfsX15. (G) TET2 mutation: Q1030X.
Table 1Evolution on 5 azacytidine therapy of main hematological parameters.
2002 M1 december 09 start therapy M3 M6 M9 M12 death
Hb(g/dL) 10.2 8.9 10.4 10.1 8.1 10.9MCV (fl) 69.3 67 69 72 68 74Hb H (%) 5.3 3.73 3.1 3.5Leucocytes (�L) 4000 23,800 17,300 7810 19,400 34,400
olii[iictiktTmThoso
F
[
[
Monocytes (�L) 500 7300
Platelets (�L) 150,000 300,000
BM blasts (%) ND 10
n alpha globin genes than on other potential genes involved ineukemogenesis. This point could be correlated to the fact that in thenherited ATR-X syndrome there is no evidence of genomic instabil-ty and no increased incidence of MDS or hematologic malignancies4]. In inherited ATR-X syndrome, the alteration of gene expressions mediated by binding to G rich tandem repeats, and the sever-ty seems to be independent of the specific ATRX mutation andorrelates with the number of G-rich tandem repeats [5]. In con-rast, our patient exhibited others mutation (TET2, ASLX) possiblynvolved in the regulation of epigenetic factors and according to thenown prognostic value of these mutations, we could speculatehat they arise secondarily, although no study was done in 2002.his report shows that TET2, ASXL1, and ATRX mutations are notutually exclusive, unless they were present in different clones.
he response to hypomethlating agents in the context of ATMDSas never been reported on the long term and seems without effectn the red cell penotype and on Hb H level in our case. It alsoeems to induce the stability of CMML only, and no hematologicalr molecular response.
unding source
No financial support for this study.
[
3600 1000 5200 11,000102,000 163,000 125,000 285,000
5 5
Conflict of interest
All authors have no conflict of interest to declare.
Acknowledgements
None.Contribution: C.R. wrote the paper, clinical management of the
patient; C.H. provided patient’s care; M.F. and A.C. provided thecytological analysis and the figures; O.N., A.R. and C.P. providedthe ASLX, TET2, AML1, FTL3, N and K RAS, CBL genes analysis andreviewed the paper; S.P. provided the alpha globin gene analysisand C.B. provided the molecular analysis of ATRX gene.
References
1] Steensma DP, Higgs DR, Fisher CA, Gibbons RJ. Acquired somatic ATRX muta-tions in myelodysplastic syndrome associated with alpha thalassemia (ATMDS)convey a more severe hematologic phenotype than germline ATRX mutations.Blood 2004;103(6):2019–26.
2] Serrano E, Lasa A, Perea G, Carnicer MJ, Brunet S, Aventin A, et al. Acute myeloid
leukemia subgroups identified by pathway-restricted gene expression signa-tures. Acta Haematol 2006;116(2):77–89.3] Costa DB, Fisher CA, Miller KB, Pihan GA, Steensma DP, Gibbons RJ, et al. Anovel mutation in the last exon of ATRX in a patient with alpha-thalassemiamyelodysplastic syndrome. Eur J Haematol 2006;76(5):432–5.

ia Res
[
[
Letter to the Editor / Leukem
4] Gibbons RJ, Pellagatti A, Garrick D, Wood WG, Malik N, Ayyub H, et al. Identifica-tion of acquired somatic mutations in the gene encoding chromatin-remodelingfactor ATRX in the alpha-thalassemia myelodysplasia syndrome (ATMDS). NatGenet 2003;34(4):446–9.
5] Law MJ, Lower KM, Voon HP, Hughes JR, Garrick D, Viprakasit V, et al. ATR-X syn-drome protein targets tandem repeats and influences allele-specific expressionin a size-dependent manner. Cell 2010;143(3):367–78.
Christian Rose ∗
Service d’onco hématologie, Hôpital Saint Vincent dePaul, Boulevard de Belfort, UC Lille, Univ Nord de
France, F-59000 Lille, France
Martine FournierOlivier Nibourel
Centre de Biologie-Pathologie, CHRU Lille, Univ Nordde France, Lille, France
Charles Herbaux
Agnes CharpentierService d’onco hématologie, Hôpital Saint Vincent dePaul, Boulevard de Belfort, UC Lille, Univ Nord de
France, F-59000 Lille, France
earch 35 (2011) e203– e205 e205
Aline RennevilleCentre de Biologie-Pathologie, CHRU Lille, Univ Nord
de France, Lille, France
Serge PissardService de Génétique et de Biochimie, CHU Hôpital
Henri Mondor, Université Paris 12 Créteil, France
Catherine BadensCatherine BADENS, Laboratoire de Génétique
Moléculaire Hôpital d’enfants de la Timone, MarseilleCedex 5, France
Claude PreudhommeCentre de Biologie-Pathologie, CHRU Lille, Univ Nord
de France, Lille, France
∗ Corresponding author. Tel.: +33 3 20 87 45 32;fax: +33 3 30 87 45 85.
E-mail address: [email protected] (C. Rose)
12 May 2011Available online 9 August 2011