Embed Size (px)
Citation preview

ACO Congress Using Analytics to Improve ACO PerformanceNovember 5, 2013

Propriety and Confidential. Do not distribute.
Introductions
2
General Manager, West RegionAccountable Care Solutions
Deb DavisOPTUM
National Lead, ACO ActuaryAccountable Care Solutions
Jay HazelrigsOPTUM
ACO Congress: Using Analytics to Improve ACO Performance 110513

Propriety and Confidential. Do not distribute. 3
Analytics for ACO’s
High Risk Claimants
Provider
Performance
ACO Congress: Using Analytics to Improve ACO Performance 110513

Propriety and Confidential. Do not distribute.
It may feel like you are scaling Mount Everest !
You need critical information to help make critical decisions
ACO Congress: Using Analytics to Improve ACO Performance 110513 4

Propriety and Confidential. Do not distribute.
The challenges in transitioning to value-based care
• “Which patients are at high risk?”
• “What conditions exist in my population?”
• “What’s happening to my patients outside of my four walls.”
• “Are my patients getting better?”
• “Who is managing the patient?”
• “What is the optimal treatment plan for the patient?”
• “Where am I on the quality standards?”
• “What is my bonus?”
• “How do I compare with my colleagues?”
ACO Congress: Using Analytics to Improve ACO Performance 110513 5

Propriety and Confidential. Do not distribute.
Electronic medical records are only the first step in the evolution, a technology for the fee-for-service model
Population Health Management
Prediction
Stratification
Analysis
Reporting
Monitoring
Health Status
Tech
nolo
gy
HighLow
Long
itudi
nal
Tran
sact
iona
l
Fee for value
Fee for service
6ACO Congress: Using Analytics to Improve ACO Performance 110513

Propriety and Confidential. Do not distribute.
Population Health Management
The next evolution is enabling technology that adds value to a fee- for-service and fee-for-value world
Prediction
Stratification
Analysis
Reporting
Monitoring
Health Status
Tech
nolo
gy
HighLow
Long
itudi
nal
Tran
sact
iona
l
Fee for value
Fee for service
7ACO Congress: Using Analytics to Improve ACO Performance 110513

Propriety and Confidential. Do not distribute. 8
Key Capabilities Needed
PCMH
P4P
Risk/Value-Based Contracts
Measure Reporting (ACO, PQRS, HEDIS, Etc.)
Physician Management
(Scorecards, Dashboards, etc.
Tasking and Alerting for Physicians in the
EMR
Patient Registries & Gaps-In-Care Management
Clinical Integration(HIE, Registries)
Basic Clinical Analytics (Clinical
Stratification)
Patient Relationship Management
Transition Management
Advanced Clinical Risk Prediction
Advanced Care Management
Cost/Risk Analytics
(Predicted Cost, Total Spend,
Leakage, Etc.)
HCC RAF/Risk Score
Optimization
Mobile Patient Education &
Remote Monitoring
ACO Congress: Using Analytics to Improve ACO Performance 110513

Population Segmentation

Propriety and Confidential. Do not distribute.
Population Segmentation – Commercial High Level Example
10ACO Congress: Using Analytics to Improve ACO Performance 110513

Propriety and Confidential. Do not distribute.
HCC Risk Score Stratification – by Beneficiary
11ACO Congress: Using Analytics to Improve ACO Performance 110513
Member Key Death Date
Attributed Physician
Paid 7/11 to 6/12
2012 Final Score
Total HCC Count HIV/ AIDS
Septicemia/ Shock
Opportunistic Infections
Metastatic Cancer and
Acute Leukemia
917 6/25/2012 Deceased $211,250 8.821 15 0 1 0 0
9854 JOHN DOE, MD $143,797 8.738 12 0 0 0 0
25174 11/14/2012 Deceased $171,693 8.607 13 0 1 0 0
4915 JOHN DOE, MD $182,737 8.347 15 0 1 1 0
11386 8/29/2012 Deceased $203,616 8.331 14 0 1 0 0
24530 JANE DOE, MD $231,594 8.117 14 0 1 0 0
19564 JANE DOE, MD $73,990 8.102 12 0 0 0 0
16662 JOHN DOE, MD $82,412 8.084 11 0 0 0 1
21446 JANE DOE, MD $100,917 7.989 11 0 1 0 1
7633 8/30/2012 Deceased $130,027 7.979 10 0 1 0 1

Propriety and Confidential. Do not distribute.
Hidden Risk/Low Utilizers
12ACO Congress: Using Analytics to Improve ACO Performance 110513
All Members Low Utilizers % of TotalLiving Beneficiaries 29,784 550 1.8%Gender Female 17,486 320 1.8%
Male 12,298 230 1.9%Race White 28,757 533 1.9%
Black 718 11 1.5%Asian 17 ‐ 0.0%Hispanic 50 ‐ 0.0%Native American 17 2 11.8%Unknown 81 1 1.2%Other 144 3 2.1%
Age Category <65 3,077 72 2.3%65‐69 5,472 51 0.9%70‐74 6,591 70 1.1%75‐79 5,659 73 1.3%80‐84 4,473 80 1.8%85‐89 2,896 105 3.6%90‐94 1,307 84 6.4%95+ 309 15 4.9%
Risk Score <1.00 21,088 ‐ 0.0%1.00 ‐ 1.15 1,752 248 14.2%1.15 ‐ 1.35 1,692 168 9.9%1.35 ‐ 1.65 1,685 76 4.5%1.65 ‐ 2.00 1,111 34 3.1%2.00 ‐ 2.25 526 9 1.7%2.25 ‐ 2.60 526 6 1.1%2.60 ‐ 3.10 509 7 1.4%3.10 ‐ 3.50 277 ‐ 0.0%3.50 ‐ 4.00 236 2 0.8%4.00+ 382 ‐ 0.0%
Low utilizers are defined as beneficiaries with a risk score
greater than 1.000 and less than $1,000 in claims
Identifies at risk populations by various categories
Beneficiary detail is also provided

Propriety and Confidential. Do not distribute.
Frequent Flyers – Emergency Room Visits
13ACO Congress: Using Analytics to Improve ACO Performance 110513
Similar report will be provided for frequent admissions/readmissions
People with Emergency Room Visits in November, 2012
Member
Key Death Date Primary Diagnosis (highest‐cost)
Paid 7/11
to 11/12 # ER Visits
16142 12/23/2012 5715 Cirrhosis of liver without mention of alcohol $42,231 6
12812 6824 Cellulitis and abscess of hand, except fingers and thumb $20,085 614762 7847 Epistaxis $4,176 6
28664 49121 Obstructive chronic bronchitis, with (acute) exacerbation $143,077 517239 30000 Anxiety state, unspecified $43,101 5
People with Multiple Emergency Room Visits in October and November, 2012
Member
Key Death Date Primary Diagnosis (highest‐cost)
Paid 7/11
to 11/12 # ER Visits
17239 34830 Encephalopathy, unspecified $43,101 1421613 490 Lymphocytic choriomeningitis $35,157 1213362 78659 Chest pain, other $42,973 922084 38014 Malignant otitis externa $13,686 8

Propriety and Confidential. Do not distribute.
Frequent Flyers – Monthly Summary
14ACO Congress: Using Analytics to Improve ACO Performance 110513
Similar reports provided for frequent admissions/readmissions
Member Key Primary Diagnosis
Total ER Visits
Diagnosis Specific ER Visits 11/1/12 10/1/12 9/1/12 8/1/12 7/1/12
21613 30000 Anxiety state, unspecified 62 10 2 1 2 4 1
2161334690
Migraine, unspecified without mention of intractable migraine without mention of status migrainosus 62 9 1 1 0 0 1
21613 78650 Chest pain, unspecified 62 4 0 1 0 0 0
21613 8479Sprain and strain of unspecified site of back 62 4 1 0 0 0 1
21613 920Early syphilis, latent, serological relapse after treatment 62 3 0 1 0 1 0
21613 8020 Nasal bones, closed fracture 62 2 0 0 0 0 021613 7242 Lumbago 62 2 0 0 0 0 121613 7840 Headache 62 2 0 0 1 0 021613 7245 Unspecified backache 62 2 0 0 0 0 121613 78605 Shortness of breath 62 2 0 0 0 0 021613 78900 Abdominal pain, unspecified site 62 2 0 0 1 0 021613 V681 Issue of repeat prescriptions 62 2 0 0 0 0 1
21613 78609Other dyspnea and respiratory abnormalities 62 1 0 0 0 0 0
21613 4739 Unspecified sinusitis (chronic) 62 1 0 0 0 0 0

Propriety and Confidential. Do not distribute.
High Cost Beneficiaries
15ACO Congress: Using Analytics to Improve ACO Performance 110513
Death Total Paid Total Paid Total PaidMember_KEY Age status Date Hospice? Highest‐Cost DRG or Condition IN 2011 in 2009 in 2010 in 2011
4624 44 Disabled Factor VIII Recombinant NOS $423,156 $558,483 $467,21528332 55 ESRD 0907 Other O.R. Procedures for Injuries with MCC 130,950 182,989 449,33424403 77 Aged 0003 ECMO or Tracheostomy with Mechanica l Venti la tion 96+ Hou 2,163 10,125 424,53213294 74 Aged 0003 ECMO or Tracheostomy with Mechanica l Venti la tion 96+ Hou 1,378 61,514 417,47029189 65 ESRD 0003 ECMO or Tracheostomy with Mechanica l Venti la tion 96+ Hou 62,689 73,977 372,02330613 68 Aged 0003 ECMO or Tracheostomy with Mechanica l Venti la tion 96+ Hou 34,267 84,167 366,05515840 60 ESRD 0329 Major Smal l and Large Bowel Procedures with MCC 132,201 284,447 354,9693801 82 Aged Oct‐11 0004 Tracheostomy with Mechanica l Venti lation 96+ Hours or Prin 6,666 2,145 343,70021451 80 ESRD Dec‐11 0166 Other Respira tory System O.R. Procedures with MCC 8,407 9,867 335,5751279 78 Aged 0003 ECMO or Tracheostomy with Mechanica l Venti la tion 96+ Hou 1,445 45,276 331,56520939 84 Aged 0003 ECMO or Tracheostomy with Mechanica l Venti la tion 96+ Hou 14,571 1,490 327,81225838 76 ESRD 0252 Other Vascular Procedures with MCC 19,567 18,211 327,43917944 67 Aged 0005 Liver Transplant with MCC or Intes tina l Transplant 7,802 13,788 323,523
8 70 Aged Jan‐12 0189 Pulmonary Edema and Respi ratory Fa i lure 11,924 30,378 322,75710914 71 Aged 0003 ECMO or Tracheostomy with Mechanica l Venti la tion 96+ Hou 7,239 350,037 322,5672659 57 Disabled 0003 ECMO or Tracheostomy with Mechanica l Venti la tion 96+ Hou 1,734 1,013 317,39432258 67 Aged 0001 Heart Transplant or Implant of Heart Ass is t System with MC 110,126 226,206 313,769589 78 ESRD 0239 Amputation for Circulatory System Disorders Except Upper Li 349,146 248,794 312,046
17730 46 Disabled 0003 ECMO or Tracheostomy with Mechanica l Venti la tion 96+ Hou 1,359 37,312 311,0896547 82 Aged Jan‐12 0356 Other Digestive System O.R. Procedures with MCC 22,899 20,449 304,91930017 84 Aged 0003 ECMO or Tracheostomy with Mechanica l Venti la tion 96+ Hou 1,385 103,248 303,498
Report will be provided using paid expenses and HCC risk scores as basis for high risk claimants

Interventions Using Analytics

Propriety and Confidential. Do not distribute.
Ambulatory Care Sensitive Conditions
17ACO Congress: Using Analytics to Improve ACO Performance 110513
Potentially avoidable admissions or ambulatory care sensitive conditions defined by the Agency for Health Research and Quality. The metrics are based on admissions for conditions that may be avoided through well-managed, coordinated primary care.
Additional detail based on attributed provider, servicing provider and facility can be used to identify opportunities to reduce admissions.
Potentially avoidable admissions or ambulatory care sensitive conditions defined by the Agency for Health Research and Quality. The metrics are based on admissions for conditions that may be avoided through well-managed, coordinated primary care.
Additional detail based on attributed provider, servicing provider and facility can be used to identify opportunities to reduce admissions.
Data
Conditions Number of Admissions Percent of Admits Rate/1000 MembersAsthma 114 3.33% 3.19CHF (non-Htn) 838 24.47% 23.45COPD 681 19.89% 19.06DiabMel no c 27 0.79% 0.76DiabMel w/cm 192 5.61% 5.37Epilepsy/cnv 132 3.86% 3.69Gastroent 63 1.84% 1.76HTN 60 1.75% 1.68PID 4 0.12% 0.11Pneumonia 724 21.14% 20.26Tuberculosis 3 0.09% 0.08UTI 586 17.11% 16.40Grand Total 3,424 100.00% 95.84
Potentially Avoidable AdmissionsPotentially Avoidable Admissions

Propriety and Confidential. Do not distribute.
Preference-Sensitive Conditions: Admissions
18ACO Congress: Using Analytics to Improve ACO Performance 110513
Acute Inpatient AdmitsMedicare Paid PMPM Admits per 1,000
unique Admits Paid (for admits State Percentiles of FFS Medicarepeople per 1,000 per Admit with the condition) Min 20th 40th 60th 80th
Hip fracture surgical repair 198 5.8 $15,064 $7.28 3.9 5.2 5.6 6.1 6.5Total hip replacement 192 5.5 $17,549 $8.11 3.5 5.6 6.1 6.5 7.2Total knee replacement 256 7.7 $15,344 $9.85 4.2 7.6 8.9 9.9 11.6Total shoulder replacement 12 0.4 $13,771 $0.45 0.0 0.7 0.8 1.0 1.1
CABG 90 2.5 $48,287 $10.15 1.3 2.1 2.5 3.0 3.4Back Surgery 70 2.0 $18,251 $3.03 0.3 2.0 2.2 2.8 3.4Carotid endarterectomy 86 2.8 $15,760 $3.68 0.8 1.8 2.1 2.4 2.7Lower Extremity Bypass 39 1.3 $24,586 $2.58 0.0 0.7 0.9 1.1 1.3
Angiography 188 5.8 $24,421 $11.75 1.5 4.7 6.0 7.0 7.8Mastectomy 21 0.6 $5,949 $0.29 0.0 0.3 0.5 0.5 0.7PCI/PTCA 202 5.9 $21,628 $10.71 2.8 5.5 6.6 7.5 8.6Colectomy 77 2.3 $28,046 $5.37 1.4 2.0 2.2 2.4 2.6
Cholecystectomy 108 3.0 $17,589 $4.44 0.9 2.7 3.1 3.4 3.9Prostatectomy 11 0.3 $11,272 $0.29 0.0 0.4 0.6 0.7 0.9
• Carotid Endarterectomy, Lower Extremity Bypass, and Mastectomy each appear to have relatively high admit rates, as compared to state percentiles of FFS Medicare
• Carotid Endarterectomy, Lower Extremity Bypass, and Mastectomy each appear to have relatively high admit rates, as compared to state percentiles of FFS Medicare

Propriety and Confidential. Do not distribute.
ACO System Care Retention by Member, Physician and Hospital
19ACO Congress: Using Analytics to Improve ACO Performance 110513
Who has attributed patients seeking care within the delivery system?
NPI NameAttributed Members Total Inpatient Outpatient
Physician - PCP
Physician - SPEC DME
Deceased Deceased 804 26% 31% 20% 67% 4% 48%1234567890 JOHN SCOTT MD 431 11% 0% 5% 77% 1% 26%1234567891 JOHN BECKNER MD 415 8% 3% 1% 68% 1% 35%1234567892 JOHN MANLEY MD 410 34% 42% 44% 90% 1% 44%1234567893 JANE LEAHY MD 407 44% 61% 50% 88% 3% 65%1234567894 JANE AUSTIN MD 401 8% 1% 1% 66% 1% 54%1234567895 JOHN REESE MD 382 18% 14% 19% 87% 6% 31%1234567896 JANE AUSTIN MD 338 9% 2% 1% 70% 1% 45%1234567897 JOHN BRAKEBILL MD 338 35% 52% 36% 89% 4% 56%1234567898 JOHN THOMAS MD 333 44% 65% 69% 86% 4% 66%
1234567899 JANE MONTGOMERY MD 326 38% 51% 48% 88% 5% 57%
Beneficiaries of the largest attributed
physician have no in- network inpatient admits
Beneficiaries of the largest attributed
physician have no in- network inpatient admits
This attributed physician has lowest PCP care
retention – potential loss of beneficiaries from CMS
attribution
This attributed physician has lowest PCP care
retention – potential loss of beneficiaries from CMS
attributionACO may have additional opportunities to manage care by expanding their
network, formally or informally, to include
specialists
ACO may have additional opportunities to manage care by expanding their
network, formally or informally, to include
specialists

Propriety and Confidential. Do not distribute.
Provider Detail Tool Provider Summaries
20ACO Congress: Using Analytics to Improve ACO Performance 110513
Provider NPI/Site Number 1234567895 ACO AverageAttributed Members 401 101 Attributed Member Months 7,217 223,475 Average HCC Risk Score 1.0208 0.9456 Average PMPY $ 7,904.14 $ 7,614.22 Average PMPM $ 658.68 $ 634.52
Member Utilization ACO AverageNo. of Low Utilizers 8 1.6 No. of Top 100 Frequent Flyer ER Members 0 0.3 No. of Top 100 Frequent Flyer IP Members 1 0.3 No. of High Cost Beneficiary Members 11 2.5 No. of Readmits 32 5.5 No. of Avoidable Admits 20 4.7 No. of Preference Sensitive Conditions 72 18.3 IP Admits/1,000 359.2 276.5 ER Visits/1,000 396.6 405.2
Chronic Conditions Member Count % of Total ACO AverageDiabetics 121 30.2% 27.5%CHF 48 12.0% 8.8%COPD 44 11.0% 11.4%CAD 39 9.7% 6.0%AMI 5 1.2% 1.0%Vascular Disease 43 10.7% 9.2%Dialysis or Renal Failure 33 8.2% 9.9%Mental Health/Psych 5 1.2% 4.1%
Provides comparison for ACO average or ACO- provided benchmarks
Provides comparison for ACO average or ACO- provided benchmarks

Propriety and Confidential. Do not distribute.
Provider Detail Tool Assigned Beneficiaries’ Characteristics
21ACO Congress: Using Analytics to Improve ACO Performance 110513
Member Summary
Attributed Member KeyACO Assigned Record
Number Risk Score Paid
12590 64565 6.658 $ 185,754 1336 456456 2.903 $ 105,392 2613 654645 4.824 $ 84,632 26326 789746 2.437 $ 80,273 1303 969877 5.167 $ 74,069 29126 459094 3.464 $ 70,957 5154 459465 4.111 $ 68,292
Utilization Summary ‐
By Member Key
Low Utilizers ER Frequent Flier IP Frequent Flier High Cost Beneficiary4016 29126 133610102 515417189 715917580 1063518649 1259020025 1536120068 2109126092 23749
2543325684
Report also includes detailed claims of attributed beneficiariesReport also includes detailed claims of attributed beneficiaries

Propriety and Confidential. Do not distribute.
Provider Detail Tool Chronic Disease Registries
22ACO Congress: Using Analytics to Improve ACO Performance 110513
NPI: 1234567890Provider: JOHN DOE, MD
Beneficiaries: 401
Members with Specific Chronic Condition ‐
by Member Key
Diabetics CHF COPD CAD AMIVascular
Disease
Dialysis or
Renal Failure
Mental
Health/Psych
121 48 44 39 5 43 33 5 257 121 121 121 121 1303 1303 4120807 416 1505 257 3826 1336 2613 7040
1356 2198 2613 596 15274 1750 3826 115101505 2279 3320 2005 27132 2613 5154 138461520 2613 3490 2538 27984 2794 5851 210911750 3826 3555 2613 3555 59491775 4718 3826 2831 3951 70361952 5154 6366 3826 4807 7159
Over 30% of this physician’s beneficiaries
have diabetes
Over 30% of this physician’s beneficiaries
have diabetes
Shows members with multiple chronic
conditions
Shows members with multiple chronic
conditions

Propriety and Confidential. Do not distribute.
Provider Detail Tool Physician Performance
23ACO Congress: Using Analytics to Improve ACO Performance 110513
Avoidable Admits Preference Sensitive ConditionsSummary Summary
Avoidable Admits Count Paid Preference Sensitive Condition Count PaidBacterial pneumonia 10 $ 39,045 ER visit for abdominal pain 12 $ 4,647 Cellulitis 1 3,352 ER visit for acute bronchitis 3 1,035 CHF 3 21,328 ER visit for asthma 2 730 COPD 2 10,465 ER visit for back pain 4 1,036 Diabetes 3 11,588 ER visit for fever 1 637 Kidney/urinary infection 1 3,047 ER visit for head ache 4 909
ER visit for nausea/vomiting 3 1,021 ER visit for UTI 16 9,325 ER visit pharyngitis 1 44 IP visit for Angiography 4 65,569 IP visit for Back Surgery 2 9,246 IP visit for CABG 1 35,390
Indicates opportunity for physician education to
increase savings
Indicates opportunity for physician education to
increase savingsIndicates opportunity for
physicians to educate beneficiaries on
appropriate healthcare choices
Indicates opportunity for physicians to educate
beneficiaries on appropriate healthcare
choices
Report also includes detail of which beneficiaries are having avoidable or preference sensitive admits
Report also includes detail of which beneficiaries are having avoidable or preference sensitive admits

Propriety and Confidential. Do not distribute.
Project Potential Impact of Interventions
24ACO Congress: Using Analytics to Improve ACO Performance 110513

Operational and Programmatic Strategies

Propriety and Confidential. Do not distribute.
Care Management Programs
26ACO Congress: Using Analytics to Improve ACO Performance 110513
•Eme rgency Room
•Home
•Specialty Care Clinic
•Primary Care Clinic
•Patient
•Inpatient Hospital
•Avoid revenue losses as a result of non-payment for readmissions
within 30 days
•Readmission Prevention
•Avoid costly delivery of services in the ER that are more
appropriately delivered by PCP
•Emergency Department Redirection
•Avoid revenue losses as a result of patient
engagement outside the health system
•Referral Management
•Drive quality compliance with EBM, improve patient outcomes and generate medical cost savings to improve pay for performance or risk
bearing opportunities
•Complex & Chronic Patient Management
•Reduce medical costs driven by redundant or inappropriate
utilization
•Care Access Services
•Avoid the cost, time and risk to develop, design and delivery population health management services independently
•Care Management Deployment Services

Propriety and Confidential. Do not distribute.
Steward Health Care Network
Client Overview: Steward Health Care Network (SHCN) is the second largest physician network in Massachusetts with over 1,100 member physicians comprised of both primary care physicians and a full range of specialists. Steward participates in the CMS Pioneer ACO Program where they are responsible for managing the health their attributed Medicare fee for service beneficiaries.
27
Case Study – Steward Health Care Network
ACO Congress: Using Analytics to Improve ACO Performance 110513

Propriety and Confidential. Do not distribute.
Local Chapter by Month by
Covered Lives
2013 Pioneer Jan
2013 Pioneer Feb
2013 Pioneer Mar
2013 Pioneer
April
2013 Pioneer
May
2013 Pioneer
JuneCape Cod 10 10 10 10 10
Greater Boston West 5,320 5,268 5,223 5,195 5,149
Greater Brockton 11,136 11,085 11,040 11,001 10,945
Greater Dorchester 2,316 2,303 2,291 2,276 2,267
Greater Fall River 3,124 3,096 3,078 3,064 3,044
Greater Haverhill 107 107 107 107 107
Greater Methuen 5,712 5,681 5,663 5,634 5,605
Greater Nashoba 2,489 2,475 2,466 2,449 2,442
Greater Norwood 4,386 4,353 4,339 4,321 4,296
Greater Quincy 2,010 1,996 1,986 1,973 1,964
Greater Taunton 8,270 8,229 8,196 8,165 8,131
Out of Area 20 20 20 20 20
Data Opt-Outs* 2,261 2,261 2,261 2,261 2,261 2,261
Total 47,161 46,884 46,680 46,476 46,241 46,002
ACO Congress: Using Analytics to Improve ACO Performance 110513 28
2013 Pioneer Covered Lives

Propriety and Confidential. Do not distribute.
Develop Interventions: Complex & Chronic Patient Management
29ACO Congress: Using Analytics to Improve ACO Performance 110513
•Value Proposition: 1-2% cost savings for the managed population with primary drivers of admit reduction and ER visit reduction
•Targeted Population: High Cost = Healthcare cost >/= $10,000; High Risk = No PCP/multiple physicians, 4 or more ER visits in 12 months, 2 or more unscheduled inpatient admissions in 6 months, Inpatient length of stay >/= 10 days, Readmission within 30 days, Coordination of multiple services (PT, OT, ST, HH, and high risk DME), Poly Pharmacy >/= 10 prescriptions, Co-morbid mental health condition, and multiple trauma
•Focused Interventions:– Medication reconciliation– Compliance with EBM and treatment plan– Reduction in total cost of care for targeted population
•Method of Engagement: Local telephonic RN’s aligned to System Provider organizations with optional face to face engagement in home/physician office
•Assumptions:– Savings valid for Optum defined program with no variation to
targeted population, method of engagement, focused interventions, staffing or workflow/processes
– Physician communication, engagement and participation in support of program and patient participation is expected and should be facilitated by client
– IP admit and ER visit reductions serve as a prospective proxy for the achievement of 1 – 2 % cost savings for the managed population
– Retrospective measurement of program effectiveness is calculated by comparing medical costs across 2 time periods – prior to program implementation (baseline group) and after the program is initiated (intervention group). A “24-12” identification approach is used, whereby individuals are identified for the baseline and intervention periods using 24 months of data but claim costs are calculated using the most recent 12 months of experience (with 3 months of claim run out)
Value/Savings Model: Complex and Chronic Patient
Management: 2% Assumptions ValueOverall Membership 26,000 Outreach 2% 520 Engagement 70% 364
Driver #1 ‐
ER ReductionER visits per 1,000 897 327 ER Visit Reduction of Engaged 20% 65 Average cost per ER visit for CCPM
patients $ 1,000 Driver #1 Savings $ 65,302
Driver #2 ‐
Admit ReductionAdmits per 1,000 1,440 524 Admit Reduction of engaged 30% 157.25 Average cost per admit for CCPM
patients $ 15,000 Driver 2 Savings $ 2,358,720
Total Gross Savings $ 2,424,022 Utilization Adjustment Factor 15% $ (363,603)Net Savings $ 2,060,418 % Gain Sharing to System 50% $ 1,030,209
CCPM 2% Total $ 1,030,209

Propriety and Confidential. Do not distribute.
Steward Program Components Complex & Chronic Patient Management
30ACO Congress: Using Analytics to Improve ACO Performance 110513
• Covers 6 provider organizations— approximately 100 PCPs
• Includes 9 Optum nurses with varied clinical backgrounds and 1 nurse with psychiatric nursing subspecialty; meets language needs of beneficiaries (Russian and Portuguese)
• Community-based program with geographical considerations in beneficiary/provider organization assignment allows for home- and office-based contract
• Beneficiary identification and stratification uses a combination of predictive modeling and real-time data
• Physician community makes direct referrals

Propriety and Confidential. Do not distribute.
Complex and Chronic Patient Management - ER visits declined 16% All Chapters
31ACO Congress: Using Analytics to Improve ACO Performance 110513
Total Member Population
Engagement Summary since Program Inception (July 23 2012) Count % Target
Total High Risk Prospect in CCPM Program Identified High Risk through Algorithm Other Referral
Total Member Population Outreached Enrolled (currently enrolled or discharged)
Members: 378 798 2,500

Propriety and Confidential. Do not distribute.
Steward Program Components Readmission Prevention Program
32ACO Congress: Using Analytics to Improve ACO Performance 110513
• Deployed at SNF level of care (versus IP acute)
• Provides coverage for 7 markets (aligned with major IP acute care facilities) consisting of 43 SNFs
• Jointly staffed with 6 Steward nurses and 2 Optum nurses
• Makes initial contact face-to-face while beneficiary is in SNF
• Conducts post-discharge follow- up care via phone call

Propriety and Confidential. Do not distribute.
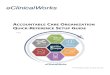
Readmission Prevention (RAP)- Readmission rates declined 25% All Chapters
33ACO Congress: Using Analytics to Improve ACO Performance 110513
Total Members Discharged From Steward
Hospital to SNF (Estimated for Period Nov
2012 ‐
Mar 2013)1,237
Engagement Summary Since November 2012
Count %Patients referred to RAP (from Pioneer
Patient Tracker)468 38%
1
Readmissions for beneficiaries with an acute discharge to a SNF
N=964 N=
676 N=370
N=702
N=491
N=250

Financial Analysis

Propriety and Confidential. Do not distribute. 35ACO Congress: Using Analytics to Improve ACO Performance 110513
Updated Benchmark/Performance
Year Targets
Gross
Shared
Savings
Are we making any money?
Basic Business Model Historic Benchmarks, Performance Year Targets and Actual Expenditures

Propriety and Confidential. Do not distribute.
Financial Modeling Considerations
36ACO Congress: Using Analytics to Improve ACO Performance 110513
One step at a time…..need to understand and quantify
• Medicare Benefit Cost Sharing Impacts• ACO Program Definition Impacts (i.e. paid through dates, interim billing, etc.)• Duplicate Claims• IBNR / Speed of Payments• Truncation• Local and National Trends by Eligibility Type• Medicare Unit Cost Fee Schedule Changes – Local and National (i.e. AWI & GPCI)• Excluded Beneficiaries and Medical Expense Impact• Opt-out Beneficiary Claims• Substance Abuse Claims• Beneficiary Churn• Risk Adjustment Impacts

Propriety and Confidential. Do not distribute.
ACO Average Claims Cost Projection vs. Updated Benchmark
37ACO Congress: Using Analytics to Improve ACO Performance 110513
Updated Benchmark /
Target = $10,300
• Base projection almost 3% below updated benchmark• ACO claims net increase 3.7% from base projection once all
adjustments considered • Initial estimate showed ACO revenues, final projection does not
• Base projection almost 3% below updated benchmark• ACO claims net increase 3.7% from base projection once all
adjustments considered• Initial estimate showed ACO revenues, final projection does not

Conclusions

Propriety and Confidential. Do not distribute.
Conclusions
39ACO Congress: Using Analytics to Improve ACO Performance 110513
• Segment Population: • Leverage Payer Data• Understand Your Risk - Strong Actuarial Analysis
• Quantify Interventions:• By Condition• By Physicians• Care Network Location
• Develop Care Management Programs:• Condition-Based• Use Dynamic Registries• Measure Impacts
• Maintain Financial Discipline:• Understand Your Contracts and Targets• Understand & Update Financial Results…Constantly

Contact Information
Deb Davis Jay Hazelrigs 970.560.3027 303.619.2442 [email protected] [email protected]