Embed Size (px)
DESCRIPTION
Advanced Cardiac Life Support
Citation preview

ACLS
Advanced Cardiac Life Support
RC 275

Defibrillation
External depolarization of the heart to stop Vfib or Vtach (that has not responded to other maneuvers)

Automated External Defibrillator
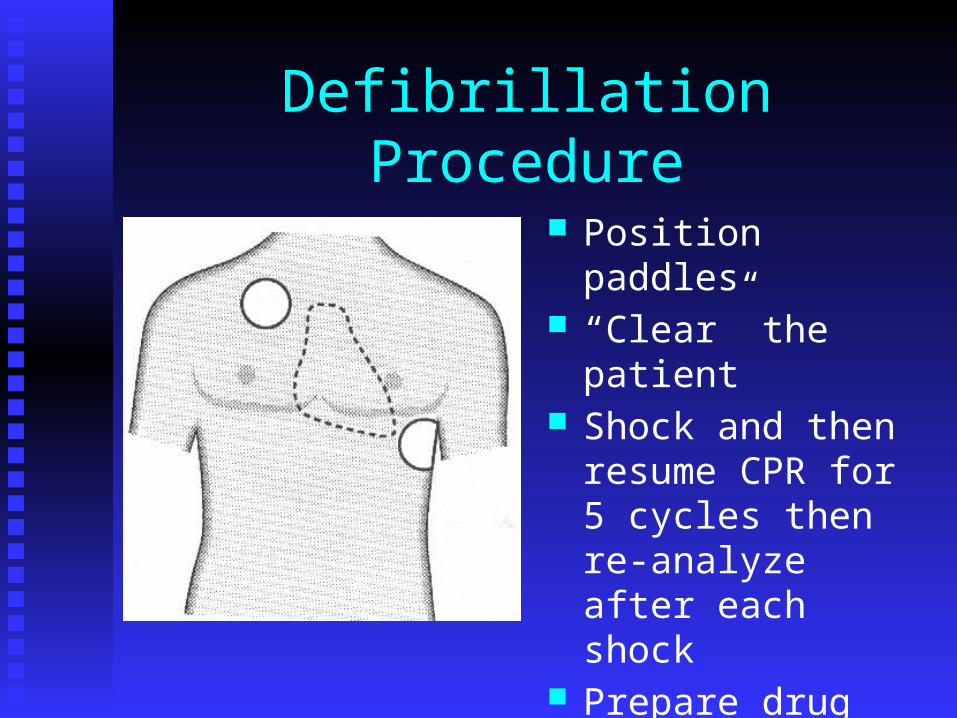
Defibrillation Procedure
Position paddles “Clear” the patient Shock and then
resume CPR for 5 cycles then re-analyze after each shock
Prepare drug therapy

ACLS Drug Therapy

Routes of Administration
Peripheral IV – easiest to insert during CPR Central IV – fast onset of action Intratracheally (down an ET tube) Intraosseous – alternative IV route in peds

Oxygen
FIO2 100% Assist Ventilation O2 Toxicity should not be a concern during
ACLS

IV Fluids
Volume Expanders – crystalloids , eg Ringer’s lactate, N/S, or colloids, eg Albumin or Hetastarch
TKO – D5W, N/S

Morphine Sulfate
Drug of choice for pain Also decreases pre-load IV dose – 2-4 mg as often as every 5
minutes Precautions
May cause respiratory depression

The Following Drugs Help to Control Heart Rate & Rhythm

Lidocaine
Indications: PVCs, Vtach, Vfib Can be toxic so no longer given
prophylactically IV dose :
1-1.5 mg/kg bolus then continuous infusion of 2-4 mg/min
Can be given down ET tube Signs of toxicity:
slurred speech, seizures, altered consciousness

Amiodarone (Cordarone) Indications:
Like Lidocaine – Vtach, Vfib IV Dose:
300 mg in 20-30 ml of N/S or D5W Supplemental dose of 150 mg in 20-30 ml of
N/S or D5W Followed with continuous infusion of 1
mg/min for 6 hours than .5mg/min to a maximum daily dose of 2 grams
Contraindications: Cardiogenic shock, profound Sinus
Bradycardia, and 2nd and 3rd degree blocks that do not have a pacemaker

Procainamide (Pronestyl)
Indications: Like lidocaine (is usually a second choice) Uncontrolled Afib or Atrial flutter if no signs of
heart failure Dose :
continuous IV infusion. Initially 20mg/min then titrated down to 1-4 mg/min
Side effects Hypotension Widening of the QRS

Atropine Indications:
Symptomatic sinus bradycardia Second Degree Heart Block Mobitz I May be tried in asystole Organophosphate poisoning
IV Dose: .5 – 1 mg every 3-5 minutes Max dose is .04mg/kg Can be given down ET tube
Side Effects: May worsen ischemia

Isoproterenol (Isuprel)
Indications:Temporary stimulant prior to pacemakerBradycardia refractory to atropineTorsades de Pointes refractory to
magnesium sulfate IV dose:
Continuous infusion of 2-10 micrograms/ml of infusion fluid

Adenosine Indication:
PSVT IV Dose:
6 mg bolus followed by 12 mg in 1-2 minutes if needed
Side Effects: Flushing Dyspnea Chest Pain Sinus Brady PVCs

Verapamil
Indications: Is a calcium channel blocker that may terminate
PSVT (is a backup to Adenosine) as well as atrial flutter and uncontrolled atrial fib
IV Dose: 2.5-5 mg over 2 minutes up to 20 mg
Side Effects: Hypotension N & V

Magnesium
Used for refractory Vfib or Vtach caused by hypomagnesemia and Torsades de Pointes
Dose:1-2 grams over 2 minutes
Side EffectsHypotensionAsystole!

Propranolol
Beta blocker that may be useful for Vfib and Vtach that has not responded to other therapiesVery useful for patients whose cardiac
emergency was precipitated by hypertension
Also used for Afib, Aflutter, & PSVT

The Following Drugs Improve Cardiac Output &Blood Pressure

Epinephrine Because of alpha, beta-1, and beta-2 stimulation, it
increases heart rate,stroke volume and blood pressure Helps convert fine vfib to coarse Vfib May help in asystole Also PEA and symptomatic bradycardia
IV Dose: 1 mg every 3-5 minutes Can be given down the ET tube Can also be given intracardiac May increase ischemia because of increased O2
demand by the heart
Vasopressin (ADH)
Similar effects to Epinephrine without as much cardiovascular side effects!
IV dose = 40 IU Can be given down ET tube May be better for asystole

Norepinephrine (Levarterenol)
Similar in effect to epinephrine Used for severe hypotension that is NOT due to
hypovolemia Cardiogenic shock Administered as a continuous infusion
Adult rate is usually 2-12 micrograms/min Range is .5-1 microgram up to 30!
Side effects: Like epinephrine, it may worsen ischemia Extravasation causes tissue necrosis

Dopamine
Used for hypotension (not due to hypovolemia) Usually tried before norepinephrine Has alpha, beta, and dopaminergic properties
Dopaminergic dilates renal and mesenteric arteries
Second choice for bradycardia (after Atropine) IV Dose:
1-20 micrograms/kg Side effects:
Ectopic beats N & V

Dobutamine
Actions similar to Dopamine Used for CHF with hypotension IV Dose:
2-20 micrograms/minute Side effects:
Tachycardia N & V Headache Tremors

Digitalis (Digoxin)
Slows conduction through A-V node and increases force of contraction
Used in CHF and chronic atrial fib/flutter Can be given orally or IV Side effects:
Arrhythmias N & V, diarrhea Agitation

Nitroglycerin
Vasodilator that helps relieve pain from angina pectoris
Can be given IV, sublingually, as an ointment or a slow release patch
Side effects: Headache Hypotension Syncope V/Q mismatch

Sodium Nitroprusside (Nipride)
Vasodilator used for hypertensive crisis IV dose:
Loading dose of 50 –100 mg followed by infusion of .5-8 micrograms/kg/min
Is light sensitive so IV bag must be wrapped in tin foil
Side effects: Hypotension so patient must have continuous
hemodynamic monitoring
Sodium Bicarbonate
Used for METABOLIC acidosis hyperkalemia H + HCO3 >H2CO3>H2O and CO2 Airway and ventilation have to be functional!
IV Dose: 1 mEq/kg If ABGs, [BE] x wt in kg/6
Side effects: Metabolic alkalosis Increased CO2 production

Thrombolytics
Used to improve coronary blood flow by lysing clots, ie coronary thrombosisBest if given within six hours of onset of
chest painExamples: TPA/Alteplase(Activase),
Streptokinase Side effects:
Bleeding
ACLS Scenario
You Run the Code!

A 62 year old female is admitted to the ER with chest pain, dyspnea, and moist, gurgling crackles. She appears in acute distress and is cyanotic. Vital signs are: P =110, R = 20, BP = 80/40.

Cardiac monitoring is initiated and the following EKG is observed:
What is the patients arrhythmia and probable medical problem?
What therapies should be done? Explain each one.

The EKG began to show:
What is occurring in the heart to cause this arrhythmia?
How is this treated? What other arrhythmias may occur now?

The patient suddenly becomes lifeless and the EKG shows:
Uh oh! What now?

The treatment(s) are unsuccessful and the following EKG appears:
What should be done now and why?

Finally, the following EKG is obtained. However, BP is 40/0
What needs to be done now?

You saved her! The course is complete!

Bretylium Tosylate (Bretylol)
Indications: Same as lidocaine and procainamide (usually
when condition doesn’t respond to these two) IV dose:
5-10mg/kg bolus followed by continuous infusion of 1-2 kg/min
Side Effects: N & V Hypotension

Amrinone
Similar to dobutamine Used for refractory CHF IV Dose:
2-15 micrograms/kg/min Side effects:
May worsen ischemia N & V Thrombocytopenia