-
7/29/2019 Acid-Base Disorders and the ABG
1/28
Acid-Base Disorders and the ABG
-
7/29/2019 Acid-Base Disorders and the ABG
2/28
Outline
1. Brief review of the acid-base physiology
2. Overview of systematic approach todiagnosing acid-base
disorders from the
ABG
3. Cases
-
7/29/2019 Acid-Base Disorders and the ABG
3/28
Overview of Acid-Base Physiology
-
7/29/2019 Acid-Base Disorders and the ABG
4/28
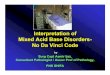
Henderson-Hasselbalch Equation
-
7/29/2019 Acid-Base Disorders and the ABG
5/28
Renal Regulation of Acid-Base
-
7/29/2019 Acid-Base Disorders and the ABG
6/28
Primary Acid-Base Disorders
As dictated by the Henderson-Hasselbalch equation,
disturbances in either the respiratory component (pCO2) or
metabolic component (HCO3-) can lead to alterations in pH.
Metabolic Acidosis
(Too little HCO3-)
Metabolic Alkalosis
(Too much HCO3-)
Respiratory Acidosis
(Too much CO2)
Respiratory Alkalosis
(Too little CO2)
-
7/29/2019 Acid-Base Disorders and the ABG
7/28
Compensation
When a primary acid-base disorder exists, the
body attempts to return the pH to normal via
the other half of acid base metabolism.
Primary metabolic disorder Respiratory compensation
Primary respiratory disorder Metabolic compensation
-
7/29/2019 Acid-Base Disorders and the ABG
8/28
Compensation (continued)
Primary Disorder Compensatory Mechanism
Metabolic acidosis Increased ventilation
Metabolic alkalosis Decreased ventilation
Respiratory acidosis Increased renal reabsorption of HCO3-
in the proximal tubule
Increased renal excretion of H in thedistal tubule
Respiratory alkalosis Decreased renal reabsorption of HCO3-
in the proximal tubule
Decreased renal excretion of H+ in the
distal tubule
-
7/29/2019 Acid-Base Disorders and the ABG
9/28
The Arterial Blood Gas (ABG)
pH, pCO2, pO
2 Measured directly
HCO3-, O2 saturation (usually) Calculated from pH, pCO2, and
pO2
-
7/29/2019 Acid-Base Disorders and the ABG
10/28
Practical Approach
1. Check the pH
If the pH < 7.35, acidemia (and at least 1 acidosis) is
present.
If the pH > 7.45, alkalemia (and at least 1 alkalosis) is
present.
-
7/29/2019 Acid-Base Disorders and the ABG
11/28
Practical Approach
2. Check the pCO2
pH < 7.35 and pCO2 < 40 metabolic acidosis
pH < 7.35 and pCO2 > 40 respiratory acidosis
pH > 7.45 and pCO2 < 40 respiratory alkalosis
pH > 7.45 and pCO2 > 40 metabolic acidosis
-
7/29/2019 Acid-Base Disorders and the ABG
12/28
Practical Approach
3. Choose the appropriate compensation formula
Most prominent
disorder
Compensation formula
Metabolic acidosis pCO2
1.5 [HCO3
-] + 8
Metabolic alkalosis pCO2 0.9 [HCO3-] + 16
Respiratory acidosis For every 10 in pCO2, pH decreases by:
0.08 (in acute resp. acidoses)
0.03 (in chronic resp. acidoses)
Respiratory alkalosis For every 10 in pCO2, pH increases by:
0.08 (in acute resp. alkaloses)
0.03 (in chronic resp. alkaloses)
-
7/29/2019 Acid-Base Disorders and the ABG
13/28
Practical Approach
4. Determine if the degree compensation is
appropriate
(If it isnt, a second acid-base disorder is likely present)
-
7/29/2019 Acid-Base Disorders and the ABG
14/28
Practical Approach
5. Calculate the anion gap
Anion gap = [Na+] ( [Cl-] + [HCO3-] )
If the anion gap is elevated, an elevated gap metabolic
acidosis is likely present.
-
7/29/2019 Acid-Base Disorders and the ABG
15/28
Practical Approach
6. If an elevated gap acidosis is present, calculate
the delta-delta ratio, to determine if a second
metabolic disorder is present.
DeltaDelta = Measured anion gap Normal anion gap
Normal [HCO3-] Measured [HCO3
-]
-
7/29/2019 Acid-Base Disorders and the ABG
16/28
Practical Approach
7. If a metabolic acidosis is present, check the urine
pH.
Urine pH > 6.0 in the setting of an acidosis Suggests RTA
-
7/29/2019 Acid-Base Disorders and the ABG
17/28
Practical Approach
8. Generate a differential diagnosis
If multiple disorders are present, they may be:
All related to the same process
All independent of one another
-
7/29/2019 Acid-Base Disorders and the ABG
18/28
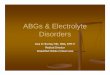
Overview of Biochemical Homeostasis
-
7/29/2019 Acid-Base Disorders and the ABG
19/28
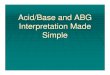
Differential Diagonsis for Acid-Base Disorders
-
7/29/2019 Acid-Base Disorders and the ABG
20/28
Summary of the Approach to ABGs
1. Check the pH
2. Check the pCO2
3. Select the appropriate compensation formula
4. Determine if compensation is appropriate
5. Check the anion gap
6. If the anion gap is elevated, check the delta-delta
7. If a metabolic acidosis is present, check urine pH
8. Generate a differential diagnosis
-
7/29/2019 Acid-Base Disorders and the ABG
21/28
Case 1
A 26 year old man with unknown past medical history
is brought in to the ER by ambulance, after friends
found him unresponsive in his apartment. He had last
been seen at a party four hours prior.
ABG: pH 7.25 Chem 7: Na+ 137
PCO2 60 K+ 4.5
HCO3- 26 Cl- 100
PO2 55 HCO3- 25
-
7/29/2019 Acid-Base Disorders and the ABG
22/28
Case 2
A 67 year old man with diabetes and early diabeticnephropathy
(without overt renal failure) presents for aroutine clinic visit.
He is currently asymptomatic.Because of some abnormalities on his
routine blood
chemistries, you elect to send him for an ABG.
ABG: pH 7.35 Chem 7: Na+ 135
PCO2 34 K+ 5.1
HCO3- 18 Cl- 110PO2 92 HCO3
- 16
Cr 1.4
Urine pH: 5.0
-
7/29/2019 Acid-Base Disorders and the ABG
23/28
Case 3
A 68 year old woman with metastatic colon cancerpresents to the
ER with 1 hour of chest pain andshortness of breath. She has no
known previouscardiac or pulmonary problems.
ABG: pH 7.49 Chem 7: Na+ 133
PCO2 28 K+ 3.9
HCO3-
21 Cl-
102PO2 52 HCO3
- 22
-
7/29/2019 Acid-Base Disorders and the ABG
24/28
Case 4
A 6 year old girl with severe gastroenteritis is admittedto the
hospital for fluid rehydration, and is noted tohave a high
[HCO3
-] on hospital day #2. An ABG isordered:
ABG: pH 7.47 Chem 7: Na+ 130
PCO2 46 K+ 3.2
HCO3-
32 Cl-
86PO2 96 HCO3
- 33
Urine pH: 5.8
-
7/29/2019 Acid-Base Disorders and the ABG
25/28
Case 5
A 75 year old man with morbid obesity is sent to theER by his
skilled nursing facility after he developed afever of 103 and
rigors 2 hours ago. In the ER he islucid and states that he feels
terrible, but offers nolocalizing symptoms. His ER vitals include a
heart rateof 115, and a blood pressure of 84/46.
ABG: pH 7.12 Chem 7: Na+ 138
PCO2 50 K+
4.2HCO3
- 13 Cl- 99
PO2 52 HCO3- 15
Urine pH: 5.0
-
7/29/2019 Acid-Base Disorders and the ABG
26/28
Case 6
A 25 year old man with type I diabetes presents to theER with 24
hours of severe nausea, vomiting, andabdominal pain.
ABG: pH 7.15 Chem 7: Na+ 138
PCO2 30 K+ 5.6
HCO3- 10 Cl- 88
PO2 88 HCO3- 11Cr 1.1
Urine pH: 5.0
-
7/29/2019 Acid-Base Disorders and the ABG
27/28
Case 7
A 62 year old woman with severe COPD comes to theER complaining
of increased cough and shortness ofbreath for the past 12 hours.
There are no baselineABGs to compare to, however, her HCO3
- measuredduring a routine clinic visit 3 months ago was 34
mEq/L.
ABG: pH 7.21 Chem 7: Na+ 135
PCO2 85 K+ 4.0
HCO3- 33 Cl- 90PO2 47 HCO3
- 34
Urine pH 5.5
-
7/29/2019 Acid-Base Disorders and the ABG
28/28
Case 8
A 36 year old man with a history of alcoholism isbrought to the
ER after being found on the floor of hisapartment unresponsive,
soiled with vomit, and with anempty pill bottle nearby.
ABG: pH 7.03 Chem 7: Na+ 134
PCO2 75 K+ 5.2
HCO3-
19 Cl-
90PO2 48 HCO3
- 20
Urine pH 5.0