Embed Size (px)
Citation preview

ACID-BASE BALANCE, DENTINOGENESIS AND DENTAL CARIESExperimental studies in rats
TUULABÄCKMAN
Institute of Dentistry
1999

OULUN YLIOPISTO, OULU 1999
ACID-BASE BALANCE, DENTINOGENESIS AND DENTAL CARIES Experimental studies in rats
TUULA BÄCKMAN
Academic Dissertation to be presented with the assent of the Faculty of Medicine, University of Oulu, for public discussion in Auditorium 1 of the Institute of Dentistry (Aapistie 3), on September 24th, 1999, at 12 noon.

Copyright © 1999Oulu University Library, 1999
OULU UNIVERSITY LIBRARYOULU 1999
ALSO AVAILABLE IN PRINTED FORMAT
Manuscript received 1.9.1999Accepted 3.9.1999
Communicated by Professor (emer.) Heikki LuomaProfessor Gary M. Whitford
ISBN 951-42-5362-0(URL: http://herkules.oulu.fi/isbn9514253620/)
ISBN 951-42-5361-2ISSN 0355-3221

,ce
"
“We can lift ourselves out of ignorancewe can find ourselves as creatures of excellen
and intelligence and skill.We can be free! We can learn to fly!
Richard Bach


Bäckman, Tuula, Acid-base balance, dentinogenesis and dental caries. Experimen-tal studies in ratsInstitute of Dentistry, University of Oulu, FIN-90401 Oulu, Finland1999Oulu, Finland(Manuscript received 1.9.1999)
Abstract
High-sucrose diet and metabolic acidosis have some similar effects on bone and they both reducethe formation of dentine. This series of experiments was conducted in order to get informationabout the effects of acidosis and alkalosis on dentine during primary dentinogenesis and also toascertain if high-sucrose diet affects dentine formation via acidosis. Chronic metabolic acidosis(0.25 mol/L of NH4Cl in drinking water), chronic metabolic alkalosis (0.25 mol/L of NaHCO3 indrinking water) and chronic respiratory alkalosis (atmospheric pressure equivalent to an altitude of3000 m) were induced in the rats immediately after weaning for 6 and 7 weeks. One subgroup fromeach of the main groups was fed a high-sucrose (43%) diet and one astandard maintenance diet,each ad libitum. The control groups had the same diets, but normal drinking water and atmosphericpressure. Al l the rats were injected with tetracycline (to mark the onset of the experiment in den-tine) and inoculated orally with Streptococcus sobrinus. The acid-base status was verified by bloodgas analysis at the end of the experiments. After sacrifice, fissure caries was scored with Schiff rea-gent and the areas of dentinal lesions and tetracycline-marked new dentine were measured fromsagittally sectioned mandibular molars. The mineral elements (Ca, Mg, F, Na, P and total mineralcontents) of the dentine formed before and during the experiment were measured with an electronprobe microanalyzer.
With the high-sucrose diet, respiratory alkalosis and metabolic acidosis promoted the initiationand progression of caries while metabolic alkalosis slightly retarded it. With the standard diet, allthe experimental conditions slowed the rate of dentine formation and metabolic acidosis had themost pronounced effect. The mineral analysis revealed a totally different pattern of mineralizationwhen the rats with metabolic acidosis (increased calcium and total mineral content) were comparedto the previously reported rats with a high-sucrose diet (decreased calcium and total mineral con-tent). Besides this, metabolic alkalosis did not correct the effects of the dietary sucrose on dentineformation and blood gas analysis showed no acid-base disturbances in the sucrose diet group.Therefore, a high amount of sucrose in the diet slows the rate of dentine formation and reduces theability of teeth to resist caries attack by mechanisms different from those of metabolic acidosis.Nevertheless, metabolic acidosis was found to be the most harmful state of disturbance in acid-basebalance for the teeth of young rats, especially with a diet containing a high amount of sucrose.
Keywords: acidosis, alkalosis, cariogenic diet, tooth

tics,in-
ssorien-ed me
a,sal
holla
nen,jäder-ibu-End-
ithtoryi-
e ofn),tics
uca-ther,to
ande the
Acknowledgements
The work for this thesis was carried out in 1989-1998 in the Department of PedodonCariology and Endodontics at the Institute of Dentistry, University of Oulu, Oulu, Fland.
I wish to express my warmest gratitude to my mentor and supervisor, ProfeMarkku Larmas, D.D.S., Ph.D, who gave me the opportunity to enter the world of sctific research. His visions and ideas and his encouragement and support have helpto proceed on my scientific career ever since.
I am also grateful to the referees of this work, Professor Emeritus Heikki LuomD.D.S., Ph.D. and Professor Gary M. Whitford, D.M.D., Ph.D., for their critical appraiand valuable comments on the content and also the language of my manuscript.
I thank all the former and present faculty and staff at the Institute of Dentistry, whelped me to carry out this work, especially Sinikka Kortelainen, D.D.S., Ph.D., and UPajari, D.D.S., Ph.D., who first introduced me to the methods involved, Sisko HuumoD.D.S., Ph.D., who has helped and encouraged me throughout these years, Leo Thane, D.D.S., Ph.D., and Eeva-Liisa Hietala, D.D.S., Ph.D., for their valuable contrtions to this thesis and all the staff of the Department of Pedodontics, Cariology andodontics for their understanding attitude towards me and my research.
I owe very special thanks to Päivi Laukkanen, M.Sc. for her help and guidance wthe biostatistics. I am also grateful for the help I was given by the staff of the Laboraof the Institute of Dentistry (especially Mrs. Eeva-Maija Kiljander), the Laboratory Anmal Centre (especially Mrs. Päivi Moilanen), the Technical Department of the InstitutDentistry (especially Mr. Reijo Kettunen, Mr. Pasi Moilanen and Mr. Eino Kemppainethe Photography Laboratory (especially Mrs. Liisa Kärki), the Institute of Electron Opand the University Library.
I warmly thank my father Väinö Bäckman, who taught me to appreciate a good edtion and encouraged me to use my intelligence, and I cherish the memory of my moHilkka Bäckman, who taught me to conquer my limitations and fears. Finally, I wishthank my fellow skydivers, especially my team and my dear friends Hellevi PeltoketoRaimo Kemppainen for sharing so many moments of freedom and joy that gave mstrength to accomplish this work.

8
y, bySci-
This work was supported in part by a research grant from the Finnish Dental Societthe Medical Research Council of the Academy of Finland and by the Research andence Foundation of Farmos.
Oulu, September 1999 Tuula Bäckman

Abbreviations
A caries lesion in enamel (Schiff reaction)
ad lib. ad libitum
ATCC American type culture collection
B advanced dentinal caries lesion (Schiff reaction)
B.E. base excess
C cavitation (Schiff reaction)
COMPO back-scattered electron image
EPMA electron probe microanalyzer
H+ hydrogen ion
HCO3- bicarbonate
m-acid-stan metabolic acidosis and standard diet
m-acid-suc metabolic acidosis and sucrose diet
m-alk-stan metabolic alkalosis and standard diet
m-alk-suc metabolic alkalosis and sucrose diet
N no caries lesion (Schiff reaction)
n number of observations in groups
norm-suc control group with sucrose diet
norm-stan control group with standard diet
pCO2 carbon dioxide partial pressure
pO2 oxygen partial pressure
r-alk-stan respiratory alkalosis and standard diet
r-alk-suc respiratory alkalosis and sucrose diet
T initial dentinal caries lesion (Schiff reaction)

10

31515. 16161717171818181919
202122232526282*299
3131323232
33. 33
Contents
AbstractAcknowledgementsAbbreviations1. Introduction . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 12. Review of the literature . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
2.1. Acid-base balance . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .2.2. Causes of disturbances in acid-base balance . . . . . . . . . . . . . . . . . . . . . . . . . .
2.2.1. Causes of metabolic acidosis . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .2.2.2. Causes of metabolic alkalosis . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .2.2.3. Causes of respiratory acidosis . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .2.2.4. Causes of respiratory alkalosis . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
2.3. Maintaining of acid-base balance . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .2.3.1. Role of lungs in maintaining acid-base balance . . . . . . . . . . . . . . . . . .2.3.2. Role of buffers in maintaining acid-base balance . . . . . . . . . . . . . . . . .2.3.3. Role of kidneys in maintaining acid-base balance . . . . . . . . . . . . . . . . .
2.4. Acid-base balance and bone . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .2.4.1. Metabolic acidosis and bone . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .2.4.2. Respiratory acidosis and bone . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .2.4.3. Metabolic alkalosis and bone . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
2.5. Acid-base balance and teeth . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .2.6. High-sucrose diet and dentine . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .2.7. Dentinogenesis . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
3. Working hypothesis and aims of the study . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .4. Materials and methods . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
4.1. Maintenance of the rats . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .4.2. Diets . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 24.3. Conduct of the experiment . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
4.3.1. Induction of metabolic acidosis . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .4.3.2. Induction of metabolic alkalosis . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .4.3.3. Induction of respiratory alkalosis . . . . . . . . . . . . . . . . . . . . . . . . . . . . .4.3.4. Control rats (normalosis) . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
4.4. Anesthesia and blood samples . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .4.5. Preparation and analyses of the tooth samples . . . . . . . . . . . . . . . . . . . . . . . . .

345
36373838394041
42424343467
474750525253555556
5758596162
4.5.1. Quantification of dentine apposition . . . . . . . . . . . . . . . . . . . . . . . . . . .4.5.2. Mineral analysis (EPMA) . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 34.5.3. Caries scoring . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
4.6. Pilot studies . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .4.7. Statistical analyses . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
4.7.1. Statistics in blood gas analysis . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .4.7.2. Statistics in measuring dentine formation . . . . . . . . . . . . . . . . . . . . . . .4.7.3. Statistics in mineral analysis . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .4.7.4. Statistics in measuring caries . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
5. Results . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .5.1. Pilot studies . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .5.2. General health . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .5.3. Blood properties . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
5.3.1. Metabolic acidosis . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .5.3.2. Metabolic alkalosis . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 45.3.3. Respiratory alkalosis . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
5.4. Dentine formation . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .5.5. Dentine minerals . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .5.6. Caries . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
5.6.1. Areas of dentinal caries . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .5.6.2. Caries scoring . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
6. Discussion . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .6.1. General health . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .6.2. Acid-base balance . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .6.3. Dentine formation . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .6.4. Mineral analysis . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .6.5. Caries . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
7. Conclusions . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .8. References . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .

ledand
ario-oth-
se inecre-here
ent inpro-
eenrats
e (e.g.
et onro-
theand,
r min-one,
ido-arel-sdietof
1. Introduction
An attempt to distinguish the initiation of caries from its later progression in dentineto a development of a method in which the size of the carious lesion was calculatedcompared to the amount of dentine formed during the experiment (ie. during the cgenic challenge) (Larmas & Kortelainen 1989). From the beginning, the working hypesis was that because the secretion of dentine is the only known form of host responthis tissue, its rate should reflect the magnitude of the response. Thus, the rate of stion of dentine was supposed to be modulated by the rate of caries progression. Twere also reasons to assume, that the reactions of the odontoblast cells are differyoung compared to old teeth and also under active compared to arrested (or slowlygressing) caries lesions (Massler 1967).
In addition to its well-known caries inducing effect, a high-sucrose diet has bobserved to cause a reduction in the growth of dentine in the molar teeth of young(Kortelainen & Larmas 1990, Tjäderhaneet al. 1994, Bäckman & Larmas 1997, etc.) in adose-dependent manner (Huumonenet al. 1997). This was a surprising finding in thesense that caries has previously been reported to accelerate the formation of dentinMassler 1967, Silverstone & Mjör 1988).
A further question arose, of what causes the reducing effect of a high-sucrose didentine formation. This effect is powerful enough to overwhelm the (theoretical?) pmoting effect of caries on dentine formation. According to the literature, the wayhigh-sucrose diet affects dentine systemically is completely unknown. On the other hsome information has been reported on the effects of a high-sucrose diet on anotheeralized tissue, i.e. bone. It has been reported to cause loss of calcium from bdecrease in net renal tubular reabsorption of calcium (Lemannet al. 1970, Lennon &Piering 1970) and even osteoporosis (Saffaret al. 1981, Tamuraet al. 1983, de Tessieres& Saffar 1992). All the same effects have also been reported in chronic metabolic acsis (Barzel 1995, Green & Kleeman 1991). Collagen fibril formation and cross-linkinginhibited by glucosein vitro (Lien et al. 1984, 1992). Metabolic acidosis slows down colagen synthesis (Kriegeret al. 1992, Whiting & Draper 1981). Some of our pilot studieshowed slightly acidotic blood gas values in the rat groups fed on a high-sucrose(Bäckmanet al. 1996), which would suggest that one of the mediators of the reduction

14
o theisms
89,dietowl-dulat-entandrink-
staterose
iated
ealthanyeta-
son
nesislasts,mblelosise ingres-
se it
ther, in
ular
dentine formation might be the altered acid-base balance of the tissue. According tliterature, it still remains unknown whether or not there are any common mechanshared by these two states.
Bone and dentine have many similarities in composition and formation (Linde 19Linde & Goldberg 1993). Therefore, a question was set whether a high-sucrosecauses any reduction in the dentine formation via an acidotic state. Based on the knedge concerning bone, acid-base balance was thought to be one of the possible moing factors both in the dentine formation and dentinal caries progression. An experimwas planned to determine if acidosis would cause similar changes in dentine growthstructure as a high-sucrose diet does. Chronic metabolic acidosis was induced with ding water containing ammonium chloride.
In addition, the effects of chronic metabolic alkalosis were tested. As the oppositeto acidosis, it was hypothesized that alkalosis would correct the effects of a high-sucdiet on dentine growth and structure if the effects of a high-sucrose diet were medvia acidosis.
Also, the overall effects of the altered acid-base balance on the composition and hof the teeth were of interest. Acid-base imbalance is a common systemic disorder in mdiseases, in using certain drugs, in special diets, in high altitudes etc. Especially, mbolic acidosis in a mild form is quite common, it is detectable for example when a peris losing weight or consuming protein-rich diet. (Brewer 1990)
Assuming that the changes in acid-base balance during the primary dentinogewould cause changes in the calcium metabolism and collagen formation of odontoband thus in the growth (and probably the structure) of the dentine, of a kind that resethose in bone, we set out to analyze the effects of chronic metabolic acidosis and alkaand chronic respiratory alkalosis on dentine formation and mineral contents of dentinthe molar teeth of young rats and whether these conditions have any effect on the prosion of dentinal caries.
Chronic respiratory acidosis was not taken into this series of experiments becauhas little effect on bone (Lauet al. 1987, Bushinsky 1988, Bushinsky 1989, Chabalaet al.1991). Furthermore, it was impossible to maintain large enough groups of rats inhyperbaric chamber available. A pilot study with a small group was made, howevethe hyperbaric chamber (1.5 bar) containing 27% O2 and 0.03% CO2 in N2. The resultssuggest that respiratory acidosis may stimulate dentine formation in the mandibmolars of young rats.

disso-).
ationion of
Car-
vola-995)
rt onmanon-xtra-rate.alled
ding
ise.pH
2. Review of the literature
2.1. Acid-base balance
A substance that can release or donate hydrogen ions (H+) is called an acid and a sub-stance that combines with or accepts hydrogen ions is called a base. When an acidciates in a solution, it yields a free H+ and its conjugate base (with a negative chargeThe acid dissociation constant tells the strength of an acid: the higher the dissociconstant, the more an acid is ionized and the greater is its strength. The concentratH+ in a solution is usually given as pH, which is a negative logarithm of the H+ concen-tration when expressed as moles/L. (Rhoades & Tanner 1995)
Acids in the mammalian body fall into two groups: carbonic acid (H2CO3) and allother acids (so-called nonvolatile acids). All can be products of the metabolism.bonic acid is in equilibrium with the volatile gas CO2, which leaves the body via lungs,whereas the other acids in the body are not directly affected by breathing. The nontile acids are buffered in the body and excreted by the kidneys. (Rhoades & Tanner 1
Mammalian cells are very sensitive to intracellular changes in the H+ concentrationand also to that of the extracellular fluid, because the intracellular pH depends in pathe extracellular pH. Nevertheless, they are not identical. The normal pH of the huarterial blood is 7.40. In the venous blood it is slightly lower because of the higher ccentration of the carbon dioxide. Intracellular pH values are lower than those of the ecellular fluid and range from 6.8 to 7.3 depending on the tissue and its metabolicWhen arterial pH is below 7.40, the state is called acidosis and when above it, it is calkalosis. (Ganong 1981)
Acidosis and alkalosis are both classified as either metabolic or respiratory, depenon whether it is bicarbonate (HCO3
-) (metabolic) or carbon dioxide (pCO2) (respiratory)that primarily deviates from the normal range in blood (Martinet al. 1981). In metabolicacidosis HCO3
- and thus plasma pH (hydrogen concentration) fall, in alkalosis they rIn respiratory alkalosis pCO2 value and thus the carbonic acid concentration falls andrises (Martinet al.1981) and vice versa in respiratory acidosis.

16
e of thes allecial-
ies isare
lismeenoss of
diet,
eeneavyunt of
ds inandneysorb
bularrewer
ar-rowthinfec-renal
ncon-CD-ewer
atecidosis
2.2. Causes of disturbances in acid-base balance
Various acute and chronic diseases cause severe changes in the acid-base balancbody. Reasons for small changes in the balance are still largely unknown, as well atheir consequences, but they are known to be common. Acid-base disorders are esply common in sick children (Brewer 1990).
2.2.1. Causes of metabolic acidosis
The most common imbalance in the acid-base balance in the industrialized countrmild chronic metabolic acidosis caused by the diet rich in the animal protein. Proteinsmetabolized to organic acids. The typical American diet produces after metaboapproximately 100 meq of acid every day (Barzel 1995). This kind of a diet has bproved to cause aciduria and calciuria as a consequence of acidosis and thus a ltotal calcium of the body (Breslauet al. 1988, Schuetteet al. 1980, Licataet al. 1981).Cola drinks that contain phosphoric acid are another acidosis-inducing ingredient ofespecially among young people (Barzel 1995).
In addition to the protein-rich diet, mild acute or chronic metabolic acidosis has breported in connection with diarrhoea (loss of bicarbonate), fasting (ketoacids) and hexercise. Strenous exercise, like all states causing tissue hypoxia, elevates the amothe lactic acid in the extracellular fluids. (Brewer 1990)
The metabolism of carbohydrates and fats produce lower amounts of organic aciblood than the metabolism of proteins. All these acids are normally rapidly bufferedexcreted, but sometimes they accumulate in the body (Ganong 1981). When the kidare not functioning normally they may fail to excrete the normal acid loads or reabsthe bicarbonate thus causing chronic metabolic acidosis. Renal failure and renal tudisorders, such as renal tubular acidosis, are known causes of metabolic acidosis (B1990). Kidney's ability to excrete acids also deteriorates with aging (Adleret al.1968).
The symptoms of type I (impaired hydrogen ion excretion) and type II (impaired bicbonate reabsorption) renal tubular acidosis are tiredness, loss of appetite, and gretardation in children. These diseases are usually a result of nephritis caused bytions or drugs. Also toxins and some congenital metabolic diseases may impair thefunction. (Jalanko & Holmberg 1998)
Examples of life-threatening diseases that cause chronic metabolic acidosis are utrolled diabetes mellitus (diabetic ketosis) (International Classification of Diseases: I10 code E14.1), starvation (ketoacidosis) (E12.1) and hypoaldosteronism (E27.4) (Br1990, Bicharaet al. 1990). Ingestion of acidifying salts (for instance NH4Cl or CaCl2),methanol or ethylene glycol (toxic metabolites formic acid and glycolic acid) or salicyloverdose are sometimes found to be a cause of a serious state of acute metabolic a(Brewer 1990).

17
mple21)
s the
artter. It is
ude
n
osis.[J45],tainravis
sly illper-raineralti-
g thexy-car-
1)
2.2.2. Causes of metabolic alkalosis
Metabolic alkalosis may also be caused by some serious medical problems, for exacongenital chloride diarrhoea (E87.8), prolonged vomiting, hyperparathyroidism (Eand various neoplasms (Brewer 1990, Bicharaet al. 1990). Also some diuretics, mineral-ocorticoid excess and ingestion of exogenous alkali are mentioned in the literature apossible causes for metabolic alkalosis (Brewer 1990).
Some renal diseases may also cause metabolic alkalosis. One example of this is Bsyndrome (E26.8), which is usually caused by mutations in the co-transport genesalso reported to induce hypercalcinuria. (Jalanko & Holmberg 1998)
Other causes of mild chronic metabolic alkalosis in industrialized countries inclbulimia (F50.2) (loss of gastric acids) (Mitchellet al. 1987), calcitonin administration forthe treatment of osteoporosis (Escaneroet al. 1991), a vitamin D excess or a vegetariadiet (alkaline metabolites) (Bicharaet al. 1990).
2.2.3. Causes of respiratory acidosis
Carbon dioxide formed by the tissue metabolism is in large part hydrated to H2CO3increasing the total hydrogen ion load until CO2 is excreted in the lungs. Thus, impaired(or suppressed) ventilation is the major cause of acute and chronic respiratory acidPossible reasons for the impared ventilation are lung diseases (for example asthmacystic fibrosis [E84], pneumonia or pulmonary edema), impared lung motion, or cerneuromuscular disorders (for example muscular dystrophy [G71], myasthenia g[G70], or drugs that depress central nervous system) (Brewer 1990).
2.2.4. Causes of respiratory alkalosis
Respiratory alkalosis is probably the most common acid-base disorder among serioupatients (Brewer 1990). Acute or chronic respiratory alkalosis is brought about by hyventilation caused for example by hysterical hyperventilation syndrome (F45.3), binjury (Martin et al. 1981), anxiety, stress (Magarian 1982), hyperthyroidism (E05), livfailure, fever (Brewer 1990), heart failure, anemia, pregnancy or a residence at hightude (Krapfet al. 1991).
Human and other mammals hyperventilate at high altitudes, both at rest and durinphysical activity. The hyperventilation partially compensates for the lower tension of ogen in the inhaled air. This leads to the lowered concentration of carbon dioxide (andbonic acid) in the blood resulting in higher pH and respiratory alkalosis. (Hurtado 197

18
s ins andpt toewer
theody,
pletenatemorethe
bynneratoryason
andeta-entra-
ric,-vol-es &
eseetingajor
2.3. Maintaining of acid-base balance
Normally pH remains relatively constant both outside and inside the cells. Alterationthe acid-base balance are resisted by extracellular and intracellular chemical bufferby respiratory and renal regulation. In the first place, kidneys and blood buffers attemcorrect metabolic disorders and lungs attempt to correct respiratory disorders. (Br1990)
Buffering in blood and extracellular fluid occurs in minutes. Acid or base added tobody enter cells and bone slowly, over hours (Rhoades & Tanner 1995). In human brespiratory compensation for a metabolic disorder begins within minutes and is comin 12-24 hours. Metabolic compensation for respiratory disorder (increase of bicarboin respiratory acidosis and decrease of bicarbonate in respiratory alkalosis) occursslowly: it begins in hours and requires 2-5 days for completion (Brewer 1990). Aftercompensations, the state of acid-base disturbance can be considered as chronic.
The change in pH in blood (produced when acid or base is added) is minimizedchemical buffers, but they do not entirely prevent the pH change (Rhoades & Ta1995). In fact, in a disturbance of the acid-base balance, neither buffers nor the respiror renal systems are completely successful in correcting pH until the underlying refor the disorder has been removed (Brewer 1990).
2.3.1. Role of lungs in maintaining acid-base balance
A normal adult produces about 300 liters of CO2 daily from the metabolism of food-stuffs. In the blood, CO2 reacts with water to form carbonic acid, which dissociates to H+
and HCO3-. In the lung capillaries they are converted back to CO2 and water and the CO2
is expired. (Rhoades & Tanner 1995).As a secondary respiratory compensation, the lungs react to metabolic acidosis
alkalosis. Metabolic acidosis stimulates breathing causing hyperventilation while mbolic alkalosis suppresses it. These are attempts to correct pH by changing the conction of carbon dioxide and carbonic acid in the blood. (Rhoades & Tanner 1995)
2.3.2. Role of buffers in maintaining acid-base balance
Oxidation of proteins and amino acids produces strong acids, like sulfuric, hydrochloand phosphoric acids, in the normal metabolism. These and other non-carbonic (nonatile) acids are buffered in the body and must then be excreted by the kidneys (RhoadTanner 1995).
The most important extracellular buffer is bicarbonate, which usually buffers thnon-volatile acids. The kidneys regenerate the bicarbonate used in buffering by excrhydrogen ions in the urine as ammonium and titratable acids (Brewer 1990). Other m

19
xtra-uid,
: toicar-l-10-o &
ule.bolictubu-
l parttoo.each
fluid,lly
lt isrine.98)can
tantbe
cer-
Ocon-
yap-out
ar inthen
chemical pH buffers in the body are inorganic phosphate and plasma proteins in the ecellular fluid, cell proteins, organic phosphates and bicarbonate in the intracellular fland mineral phosphates and mineral carbonates in bone (Rhoades & Tanner 1995).
2.3.3. Role of kidneys in maintaining acid-base balance
The kidneys have two important roles in the maintaining of the acid-base balancereabsorb bicarbonate from and to excrete hydrogen ions into urine. 4500 mmol of bbonate are filtered into the primary filtrate of urine daily, but only 2 mmol of it are finaly excreted. 70-80% of bicarbonate is reabsorbed in the first part of proximal tubule,20% in the loop of Henle and 5-10% in the distal tubule and collecting ducts. (JalankHolmberg 1998)
Carbonic anhydrase plays an important role in the reabsorption in the proximal tubDisturbance in the reabsorption of bicarbonate in the proximal tubule leads to metaacidosis, hyperchloremia and alkalotic urine. This disease is named as "type II renallar acidosis" (N25.8). (Jalanko & Holmberg 1998)
Renal tubules actively secrete hydrogen ions. Most of this takes place in the distaof the nephron, but active transport of hydrogen ions occurs in the proximal tubule,The H-ATPase of the apical cell membrane secretes hydrogen ions into urine. Forhydrogen ion secreted, one bicarbonate molecule is transported to the interstitialfrom there it diffuses into the bloodstream. Fifty mmol of hydrogen ions are normaexcreted daily. (Jalanko & Holmberg 1998)
If the hydrogen ions are not properly secreted into the collecting ducts, the resumetabolic acidosis, hypokalemia, hypocalcemia, nephrocalcinosis and an alkalotic uThis disease is called "type I renal tubular acidosis" (N25.8). (Jalanko & Holmberg 19
The maximal hydrogen ion gradient, against which the transport mechanismsecrete H+ ions, corresponds to a urine pH of 4.5 in humans. However, three impormolecules remove free hydrogen ions from the tubular fluid permitting more acid tosecreted: H+ is bound to ammonia, phosphate and bicarbonate to form NH4
+, H2PO4-,
CO2 and H2O. (Ganong 1991)The source of the hydrogen ions secreted by the tubular cells is not completely
tain. It is probably produced by dissociation of H2CO3. The acid-secreting cells containcarbonic anhydrase, which facilitates the rapid formation of H2CO3 from CO2 and water.The renal acid secretion is mainly regulated by the changes in the intracellular pC2,potassium concentration, carbonic anhydrase activity and adrenocortical hormonecentration. (Ganong 1991)
2.4. Acid-base balance and bone
The main constituents of bone are type I collagen in the organic matrix and hydroxatite in the inorganic matrix. The mineral in the skeleton is being turned over throughlife. Calcium in bone turns over at a rate of 100% per year in infants and 18% per yeadults. Osteoblasts produce bone by secreting collagen that forms the matrix which

20
e. Onew:
artialtheanareaage
n thescu-
ee-
boneainst
s, as
andcal-obi-toninapable
theaus-uff-95).
oadesone
lt iscal-
orp-
osisis
r and
calcifies. Osteoclasts are responsible of resorption: they erode and phagocytose bonturnover cycle, in which one cavity is resorbed and filled again, is relatively sloapproximately eight months. (Green & Kleeman 1991)
Inactive osteoblasts flatten out over the bone surfaces (Fig. 1). They make a pmembrane, which separates the so-called bone fluid (which is in contact withhydroxyapatites) from the extracellular fluid of the adjacent tissues (Green & Kleem1991). The fast regulation of serum calcium occurs across this quiescent surface(Parfitt 1987). Inside the bone canaliculi, osteocytes are involved in this process (Talm& Grubb 1977). The tiny hydroxyapatite crystals present an enormous surface area ibone (100-200 square meters per gram of bone). Also, the bone is relatively well valarized. This structure allows a rapid mobilization of the bone calcium. (Green & Klman 1991, Ganong 1991)
Acid-base balance has an effect on bone turnover, especially on the rates ofresorption and calcium mobilization. Bone mineral participates in the defense agacid-base disturbances, especially against metabolic acidosis (Lemannet al. 1966, Green& Kleeman 1991). The role of the bone mineral is important in the acid-base disorderno appreciable change in the intestinal calcium absorption occurs (Bicharaet al. 1990).
In the mammalian body, mainly three hormones regulate the calcium metabolismthe bone turnover. 1,25-dihydroxycholecalciferol (vitamin D derivative) increasescium absorption from the intestine and, indirectly, from bone. Parathyroid hormone mlizes calcium from the bone and increases the urinary phosphate excretion. Calciinhibits bone resorption (Ganong 1981). Used as drugs, these hormones are also cof inducing acid-base disorders. Calcitonin administration (Escaneroet al. 1991) and vita-min D excess (Bicharaet al. 1990) have been reported to cause metabolic alkalosis.
2.4.1. Metabolic acidosis and bone
In mammals, the endogenous metabolism produces acids, mostly originating fromproteins in the diet. The extracellular fluid bicarbonate buffers in part these acids, cing a decrease of bicarbonate in blood and thus a fall in systemic pH. Fall in pH is bered by other buffers in the body, including the mineral phases of bone (Bushinsky 19Bone contains large buffer stores, specifically salts of phosphate and carbonate (Rh& Tanner 1995). In the process of skeletal buffering, calcium is released from the bmineral (Bushinskyet al. 1983).
If the acids are produced in great amounts or their excretion is impaired, the resuthe loss of bone. The kidneys react to the additional calcium in plasma by increasingcium excretion (hypercalcinuria). As there is no change in the intestinal calcium abstion, the net result is a decrease in the amount of calcium in the body (Breslauet al.1988).
The change in the total mineral content of the bone is marked in severe acid(Lemann Jret al. 1966, Green & Kleeman 1991). The effect of acidosis on the bonemuch greater in young mammals than in adults (first described by Jaffeet al. 1932). Inadult subjects, there is less bone buffering due to the lower proportion of bone wate

21
lead
itivedjija
ility,mu-tion
ataseteo-re
y toses avefunc-
aci-has
s thestimu-
have
in then inCha-notring
are
is an
exchangable mineral surface (Burton 1992). However, even a mild acid loading mayover the years to osteoporosis (Sebastianet al. 1994). This kind of a mild acid loadingmay be caused by, for example, the high-protein diet.
In the bone the cell-mediated calcium release is the most important and sensmechanism of response to metabolic acidosis (Bushinsky 1989, Goldhaber & Raba1987). To a lesser extent, low pH also promotes physicochemical mineral solubwhich does not depend on the cells (Bushinsky & Lechleider 1987). In addition to stilating osteoclastic function, metabolic acidosis also inhibits osteoblastic bone formaby slowing down collagen synthesis (Kriegeret al. 1992, Whiting & Draper 1981).
In vitro, a decrease in the bone collagen synthesis and diminished alkaline phosphactivity occur in calvariae in metabolic acidosis, both indicating a suppression of osblastic function (Kriegeret al. 1992). The genes critical to osteoblastic function aaltered by pH. In a group of the immediate early response genes (c-fos, egr-1, junB, c-jun,junD), metabolic acidosis (pH 6.8) leads to a reduction inegr-1 stimulation, while meta-bolic alkalosis (pH 7.6) stimulates it. RNA for type 1 collagen reacts in the same waboth acidosis and alkalosis. Increasing or decreasing external pH by 0.2 units causignificant change in theegr-1 stimulation. Thus, small changes in systemic pH may haa significant effect on the expression of certain genes important for the osteoblastiction. (Fricket al.1997)
The activity of osteoclastic enzymes in cultured calvariae is enhanced in metabolicdosis (Kriegeret al. 1992). Stimulation of the osteoclastic beta-glucuronidase releasebeen reported (Bushinsky & Nilsson 1995).
Parathyroid hormone has similar effects as acidosis on the bone. It also inducecell-mediated bone resorption, suppresses the osteoblastic collagen synthesis andlates the osteoclastic beta-glucuronidase release.In vitro, additive effects of metabolicacidosis and hyperparatyroidism on the net calcium efflux and the bone cell functionbeen reported (Bushinsky & Nilsson 1995)
2.4.2. Respiratory acidosis and bone
Respiratory acidosis seems to cause mainly similar, but not as profound changescalcium metabolism as metabolic acidosis. Alterations in the surface ion compositiothe cultured bone in metabolic, but not in respiratory acidosis, have been reported (balaet al. 1991). There is proton influx into the bone during metabolic acidosis, butduring respiratory acidosis (Bushinsky 1988), and calcium efflux from the bone dumetabolic acidosis is greater than during respiratory acidosisin vitro (Bushinsky 1989).In the cultured bone, the alterations in the ion composition in respiratory acidosismuch less severe than in metabolic acidosis (Chabalaet al. 1991).In vivo, respiratory aci-dosis does not appreciably increase the urine calcium excretion, although thereincrease in the serum calcium concentration (Lauet al. 1987).

22
t as
no
tionbeennate
res-rre-romhas
andh theone
ear.idase,
blas-haveeto-e
llagen
s andthe
, thes the
Thisclast-fectscal-
Klee-been
2.4.3. Metabolic alkalosis and bone
Metabolic alkalosis causes an influx of calcium into the bone, but the effect is nostrong as the opposite effect of metabolic acidosis (Bushinskyet al. 1983). Also, metabol-ic alkalosis results in hypocalcinuria and thus a retention of calcium, while there ischange in the intestinal calcium absorption (Bicharaet al. 1990).Neutralization of the daily metabolic acid load with base decreases calcium excre(Bushinsky 1996). In clinical studies, patients with a negative calcium balance havetreated successfully with sodium bicarbonate (Lutz 1984) and potassium bicarbo(Sebastianet al.1994).
In vitro, both mild (pH 7.5) and severe (pH 7.6) metabolic alkalosis cause a progsive decrease in the calcium efflux from the bone. The calcium efflux is inversely colated with medium pH: the higher the medium bicarbonate, the less calcium efflux fthe bone (Bushinsky 1996). Also in several clinical studies metabolic alkalosisdecreased bone resorption and even increased bone formation (Breslauet al. 1988, Licataet al. 1981, Schuetteet al.1980).
Metabolic alkalosis decreases bone calcium efflux by stimulating the osteoblastssuppressing the osteoclasts (Bushinsky 1996). Alkalosis may alter the function of botosteoblasts and the osteoclasts to a similar degree or it may modify the function ofcell type which then alters the function of the other. These mechanisms are not yet cl
Alkalosis causes a decrease in the release of osteoclastic enzyme beta-glucuronwhich has an important role in the bone resorption (Bushinsky 1996). Also, the osteotic collagen synthesis is induced. The genes important for the osteoblastic functionbeen found to react in metabolic alkalosis.In vitro, the osteoblastic early response genegr-1 and RNA for the type 1 collagen are stimulated resulting in induction of the odonblast collagen synthesis (Fricket al. 1997). There is an inverse correlation between theffects of metabolic alkalosis on osteoclastic enzyme release and osteoblastic cosynthesis (Bushinsky 1996).
In the process of resorption, the osteoclasts secrete protons between themselvethe bone mineral. To prevent intracellular alkalinity, the osteoclasts must excretebicarbonate generated for every hydrogen ion secreted. In metabolic alkalosisincreased concentration of the bicarbonate in the extracellular fluid may suppresosteoclastic hydrogen ion secretion. (Bushinsky 1996)
If the osteoclastic activity is inhibited by calcitonin, the influx and efflux of calciumare still, although in lesser extent, correlated with the concentration of bicarbonate.indicates that the alterations in the bicarbonate concentration have also a non-osteomediated effect on the bone. It remains unknown whether metabolic alkalosis also afthe physicochemical mineral dissolution in addition to its effects on the cell-mediatedcium flux. (Bushinsky 1996)Data relating to the alkali loads and the respiratory changes are scarce (Green andman 1991). No reports concerning respiratory alkalosis and the bone seem to havepublished.

23
princi-at noan-ction
.
blastsare
ges ined, inte of
, resultenitalanentand
dosis
2.5. Acid-base balance and teeth
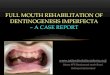
There are numerous similarities between the osteoblasts and the odontoblasts. Thepal difference between the osteogenesis and the odontogenesis lies in the fact thremodelling nor osteoclast-like cells exist in the dentine (Fig. 1). However, microorgisms seem to be capable of destroying enamel and dentine structure by a direct aresembling osteoclasts dissolving bone (Brännströmet al.1980, Luomaet al.1984).
Fig. 1. Schematic drawing of the dentine (left) and the bone (right). Gray area = mineralizedtissue. Striped gray area = unmineralized new dentine (predentine) / bone (osteoid). Left:carious dentine and cariogenic bacteriae up, odontoblast cells (pulp) down. Odontoblastprocesses in tubules. Right: Active (round) and passive (flat) osteoblasts surround the boneOsteocytes are located inside the bone. They are communicating via the bone canaliculi witheach other and with the osteoblasts. In left upper corner, multinucleated osteoclast resorbs thebone.
The odontoblasts are partly under the same metabolic regulation as the osteo(Linde & Goldberg 1993), and therefore the formation of the bone and the dentineprobably regulated by similar factors. Thus there is a reason to assume that the chanacid-base balance have effects on dentine metabolism as they do on the bone. Indeprevious studies we have found that chronic metabolic acidosis slowed down the radentine formation and the general body growth in the young rats (Bäckmanet al.1996).
In humans, several congenital chronic diseases, causing acid-base disturbancesinto changes in dental health and development and the structure of the teeth. Congpersistent proximal type renal tubular acidosis causes enamel defects of the permteeth (Winsneset al. 1979). Also, missing and peg-shaped teeth, enamel hypoplasiasexcessive caries in carbonic anhydrase II deficiency syndrome with renal tubular acihave been reported (Ohlssonet al. 1986).

24
oundis of
wereromwas 3
.8],n-
rtederma-
was
fluo-hleyosis
with
alsoord
it-
ithisoruseandadio-
een
ups.front
h isthe
ride.ride.
thead, it
Severe symmetrically distributed enamel hypoplasia in the permanent teeth was fin a patient with chronic metabolic acidosis (congenital persistent renal tubular acidosproximal type, capillary blood pH 7.07-7.15) (Koppanget al. 1984). Delayed sheddingand eruption, agenesia of a few permanent teeth and retarded tooth developmentalso reported. The primary teeth were normal except for an extremely thin enamel. Fa 10-year old boy, several teeth had been extracted due to caries. His skeletal ageyears and dental age 2 years delayed.
Both chronic metabolic alkalosis (children with congenital chloride diarrhoea [E87Myllärniemi & Holmberg 1975) and chronic respiratory alkalosis (children with acyaotic congenital atrial septal defect in heart [Q21.1], Bäckmanet al. 1990) have beenobserved to increase caries resistance. Myllärniemi & Holmberg (1975) also repoenamel defects and hypoplasias of varying severity in both the deciduous and the pnent teeth. The timing of the deciduous and permanent teeth formation and eruptionnormal.
Acid-base balance also affects the fluoride metabolism. The absorption rate ofride from the stomach is dependent on the pH of the gastric contents (Whitford & Pas1984). Plasma clearance of fluoride by the kidneys is related to urinary pH: acidinduces reduction in the renal clearance of fluoride (Whitfordet al. 1976). High concen-trations of fluoride and magnesium are found in the bone and the enamel associatedthe acidotic state (Angmar-Månsson & Whitford 1995).
Mineralization defects in the enamel of rats and dogs, resembling fluorosis, havebeen found in acidosis without an exposure to fluoride (Angmar-Månsson & Whitf1990). Both chronic metabolic acidosis (exposure to NH4Cl) and chronic respiratory aci-dosis (exposure to 10% CO2) result in major disturbances in the rat incisor enamel (Whford & Angmar-Månsson 1995).
In an experiment with young pups, chronic metabolic acidosis was induced wNH4Cl (Angmar-Månsson & Whitford 1986, Angmar-Månsson & Whitford 1990). Thresulted in an increase in the amount of fluoride in teeth with no change in the phosphconcentration. Also in NH4Cl -induced acidosis with no fluoride supplementation, thmineralization of enamel was severely disturbed with alternating layers of hyper-hypomineralization, having in some cases even cystic appearance in the microrgraphic analyses. Chronic metabolic alkalosis (induced with NaHCO3) caused only minorchanges in the mineralization pattern. The ratios of Ca/P or Ca/Na did not differ betwthese groups or compared to the controls.
With similar experimental setting, Driessenset al. (1987) found no differences in theCa/P or Ca/Na ratios in the molar dentine between acidotic, alkalotic and control pAlso, there was not a clear trend in these ratios as a function of the distance from theof the mineralization.
Metabolic alkalosis enhances the excretion rate of fluoride by the kidneys, whicreflected in reduced fluoride levels in both soft and hard tissues. The disturbance inenamel mineralization associated with alkalosis is additive to that produced by fluoIn acidosis, the defective mineralization is attenuated by a supplementation with fluo(Angmar-Månsson & Whitford 1990)
Calcium phosphate supplementation of the diet did not mitigate the defects inenamel mineralization associated with the chronic acid-base disturbances. Insteworsened them, especially in chronic acidosis. (Angmar-Månsson & Whitford 1990)

25
490cisoraphi-rousntra-
igh-
tit-
y thes was
tion oreans
rerfacemay
amel
pro-sug-
osition
ationrose,
ofitical
n indtheice
ourotein.
Chronic respiratory alkalosis, caused by living in low pressure corresponding 5meters above sea level, also results in disturbances in the mineralization of the rat inenamel. The enamel is severely damaged both macroscopically and microradiogrcally and uniformly bleached to the color of chalk. The incisor dentine contains numesmall lacunae. Like in metabolic acidosis, hard and soft tissues have a higher concetion of fluoride. (Angmar-Månssonet al.1984, Angmar-Månsson & Whitford 1990)
2.6. High-sucrose diet and dentine
Reduction in the growth of dentine in the molar teeth of young rats caused by a hsucrose diet has been observed in numerous studies (Larmaset al.1992, Tjäderhaneet al.1995, Huumonenet al.1997, etc.). This effect is independent on the other dietary consuents as well as on the severity of caries (Tjäderhaneet al. 1994).
The results also indicate that the reduction of dentine apposition is not caused bcaries, but by the systemic effects of a high-sucrose diet, because dentinogenesislowed down even under the intact fissures (Huumonenet al. 1997). And vice versa:slower dentinogenesis has not been found to increase (or decrease) the caries initiaprogression. This result has been obtained by reducing the dentine formation by mother than sucrose during the primary dentinogenesis (Huumonenet al. 1996).
Concerning molar fissures, it is difficult to confirm if microbial effects on dentine atotally avoided or not. The bacteria seem to be able to invade the enamel through sumicrodefects. A cross-section reveals only one plane of enamel and the defectsremain unobserved (Seppä 1984, Seppäet al. 1989). Also, dentine may be infectedthrough an incipient enamel lesion, even when no cavitation has occurred on the ensurface. This has been reported both in rats (Luoma A-R.et al. 1984, Luoma H.et al.1987, Seppäet al. 1989) and in humans (Brännströmet al.1980, Seppä 1984, Seppäet al.1985).
During secondary dentinogenesis, the rate of the dentine formation and the cariesgression both are less than 1/10 of that during the the primary dentinogenesis. Thisgests that there is a connection between the rate of caries progression and the depof the dentine. (Hietala & Larmas 1992, Kortelainen & Larmas 1994)
The concentration of sucrose in the diet must be high to reduce the dentine formin the rats. When young rats were fed on a diet containing 15%, 30% or 43% of sucsignificant reduction in the dentinogenesis was only seen in the animals with 43%sucrose in the diet. The rats were not inoculated with cariogenic bacteria. The cramount of sucrose seemed to be between 30 and 40 g/ 100 g. (Huumonenet al.1997)
All kinds of high-sucrose diets seem to have the same effect on dentine formatiothe young rats. Autioet al. (1997) reported only a slightly stronger reduction in rats feon the modified Stephan-Harris diet (43% of sucrose, Table 1) than in those fed onR36 diet (special diet for growing rats and mice, Brood Stock Feed for Rats and MR36, Finnewos Aqua Oy, Turku, Finland), in which most of the barley and wheat flwere replaced by sucrose (41%) and casein was added to compensate the loss of pr

26
ntinf
beendiet
rats
ungifiedodi-rch)total
trond Zn,
ifferhichlts to
causeet.ent inve-at thein theentine
one
diet.resses
ighlyrough-s/ight
apa-
Theden-ited
the
Both of the sucrose diets mentioned above slightly increased the width of predecompared with the control diet (R36) (Autioet al. 1997). In this respect, the effects oboth sucrose diets were equal. The same effect, but more pronounced, has alsoreported in the study of Hietala et al. (1997), in which the modified Stephan-Harriswas used. The increased width of predentin indicates disturbed mineralization in thefed on the high-sucrose diets (Butler 1995).
Also quantitative changes in the amounts of mineral elements of dentine of the yorats' molars has been observed in connection with the high-sucrose diet (the modStephan-Harris diet) compared to the standard diet (Ewos R3, Table 1) and to the mfied Stephan-Harris diet in which sucrose has been replaced with potato flour (sta(Tjäderhane 1996). Calcium, phosphorus, fluoride, sodium, magnesium, zinc and thecontent of minerals in dentine were determined with SEM equipped with an elecprobe microanalyzer (EPMA). Reduction in all the elements measured, except F anwas found in the sucrose group.
In the study referred to above (Tjäderhane 1996), the dentinal Ca/P ratios did not dbefore or during the experiment or between the groups. A Stephan-Harris diet in wsucrose had been replaced with complex carbohydrate (starch) gave identical resuthe Ewos R3 standard diet, which suggests that nutritional deficiences were not theof the changes in the mineral contents in the dentine of the rats fed on the sucrose di
The high-sucrose diet has also been reported to suppress the rate of fluid movemthe molar dentine of young rats (Steinman & Leonora 1971). The rate of the fluid moment was inversely related to the incidence of dental caries. The authors assume thproducts of metabolism (lactic acid) accumulate and the nutrient uptake decreasesdentine as a consequence of the suppressed fluid movement. Unlike the bone, the dis avascular and thus more dependent on the fluid transport system.
The dentinal fluid movement has been found to be regulated by parotid horm(”parotin”) in rat (Leonoraet al. 1992) and in pig (Tiecheet al. 1994). Parotidectomizedrats had a suppressed fluid movement in the dentine regardless of the quality of theA high sucrose-diet reduces the secretion of the parotid hormone and thereby suppthe rate of the dentinal fluid movement in both the rats and the pigs (Leonoraet al. 1992,Tiecheet al.1994).
2.7. Dentinogenesis
The odontoblasts lining the pulp chamber produce the dentine. The dentine is a hpermeable tissue, because densely packed dentinal tubules radiate from the pulp thout all the layers. 15000 tubules/mm2 are present in the outer dentine and 55000 tubulemm2 near the pulp. The dentine contains more minerals than the bone: 70% of weconsists of the minerals. Type I collagen is predominate in the organic and hydroxytite in the inorganic portion. (Linde & Goldberg 1993)
The dentine may be divided into intertubular dentine and peritubular dentine.former is the main product of the odontoblasts constituting the largest volume of thetine. The intertubular dentine consists of a fibrous network of collagen with deposmineral crystals. The peritubular dentine forms a highly mineralized sheath around

27
allyulp
junc-is 5-reerg
ture,g thetoblica-
llytooth
andlattercturemary
Toothe thedion,rationfullyed of
erg
d theis
old-
med.erent
tino-ames
g the
dentinal tubule (0.5-1 micrometers thick in humans). The peritubular dentine gradu(partly or completely) fills up the dentinal tubules at some distance away from the pchamber. (Linde & Goldberg 1993)
The first stage of the dentinogenesis forms mantle dentine on the dentine-enameltion during the early stages of the tooth development. In human, the mantle dentine30 micrometers thick (Linde & Goldberg 1993). It is rich in proteoglycans and moirregular and less mineralized than the following layers. (Jenkins 1978, Linde & Goldb1993).
The second stage, forming the next layer and consisting the most of the tooth strucis called primary dentinogenesis. Some confusion exists in the literature concerninending time of this stage (Coxet al. 1992). The primary dentinogenesis is consideredbe finished and secondary dentinogenesis started at different phases in different putions, such as when the crown is fully formed, when the tooth erupts (Coxet al. 1992),when the tooth becomes functional (Linde & Goldberg 1993) or when the root is fuformed (Torneck 1994). The latter seems most reasonable, because (in humans) themetabolism becomes slower after the root apex is formed.
In rat molars, the dentine formation slows down gradually during both the primarythe secondary dentinogenesis with no apparent transition from the former to the(Johannessen 1961, Hietala & Larmas 1992, Kortelainen & Larmas 1994). The struof the secondary dentine is supposed to be slightly more irregular than that of the pridentine (Torneck 1994).
The next stage, tertiary dentinogenesis, occurs as a tooth response to irritations.preparation made by a dentist, dentinal caries, attrition, abrasion and/or erosion armost common irritating factors (Coxet al. 1992). The tertiary dentine may also be nameaccording to the quality of the irritation: The dentine formed as a response to attritabrasion or erosion is called "reactional dentine" to separate it from caries and prepainduced "reparative dentine". The tertiary dentinogenesis may be absent even in amatured tooth. The quality of the tertiary dentine seems to be dependent on the speits formation: the faster it is formed, the more irregular it appears (Linde & Goldb1993, Torneck 1994).
Predentine is the innermost layer of the dentine, right next to the odontoblasts anpulp. It is a thin layer of unmineralized organic matrix, mostly collagen. This layerpresent also in an old tooth, in which the dentinogenesis is slowed down. (Linde & Gberg 1993)
During all the stages of the dentinogenesis, permanent layers of dentine are forThus, a disturbance in any stage leaves persisting marks in the structure. This is difffrom the bone, in which constant turnover exists.
Because of the confusing terminology concerning the different stages of the dengenesis and the lack of apparent zones of transition from one stage to another, the nof the stages are partly ignored in this study. Considering the age of the rats durinexperiments (3-10 weeks), however, the dentine formed was mostly primary.

3. Working hypothesis and aims of the study
Among dentists, dental caries is thought to merely imply the dissolution of the tooth min-erals by bacterial functions. In fact, this is principally the case in the enamel, and undeni-ably also in dentine, although perhaps less exclusively.
In the dentine, the vital processes are principally regulated by the cells of the pulp/den-tine complex in a way that makes dentinal caries a process notably resembling the boneresorption. Thus, the function of the cariogenic bacteria in the dentine may be comparableto the function of the osteoclasts in the bone.
The rate of the destruction in dentinal caries seems to be associated with the rate of thedentinogenesis. Caries proceed faster in the teeth of the young animals with rapid growthof the dentine than in the teeth of the older animals (Hietala & Larmas 1992, Kortelainen& Larmas 1994). On the other hand, a high-sucrose diet and metabolic acidosis slowdown the rate of the dentinogenesis and induce caries (Kortelainen & Larmas 1990,Tjäderhaneet al. 1994, Bäckmanet al.1996).
The aim of this work was to find out whether the high-sucrose diet and the acid-baseimbalance of the body have the same kind of systemic effects on caries (on cariogenicbacteria) and on the odontoblasts in the dentine as they have on the osteoclasts, osteo-blasts and osteocytes in the bone and whether these processes are connected. The slowerrate of formation, as such, of the dentine is thought to be analogous to bone resorption, asno resorption by tissue cells occurs in the normal dentine.
The tested central hypotheses were:1. Sucrose affects odontoblasts causing reduction in dentine formation and acceleration
in caries progression at least partly via metabolic acidosis.2. Metabolic alkalosis eliminates most of the effects of sucrose, if the hypothesis num-
ber one is correct.

ther,ni-
weredis-ed by
spensamemancageoughcages
roseAB,ted infor
72).
4. Materials and methods
4.1. Maintenance of the rats
All the experimental animals were Wistar rats (Wistar Hannover), 96 animals altogeand they were bred in the Department of Laboratory Animals, Institute of Dentistry, Uversity of Oulu. Their maintainance and care and all the experimental proceduresperformed by persons licenced to that work. The animals did not suffer from pain oreases of any kind during the experiments. The experimental protocols were acceptthe Experiment Animal Committee of the Medical Faculty, University of Oulu.
The animals were housed 2 or 3 to a cage (Macrolon III) on a bed of European ashavings at a temperature of 21°C and humidity of 40%-60%, and subjected to thelighting regimen (12 hours light and 12 hours dark) and the same frequency of huhandling. The rats were weighed once a week. The food and water consumption perwere recorded at intervals of three days throughout the experiment. These were restimations, because no metabolic cages or feeding machines were used (individualare not found to be suitable for caries experiments in rats, Bakeret al. 1979).
4.2. Diets
A modified Stephan-Harris diet was mixed in our laboratory and used as the high-sucdiet and a commercial Ewos R3 diet (Brood Stock Feed for Rats and Mice R3, EwosSödertälje, Sweden) as the standard one. The compositions of the diets are presenTable 1 and the nutritional values in Table 2. The diets are nutritionally acceptablegrowing rats according to the recommendation of National Research Council (19Both diets were supplied in a powdered form and providedad lib.

30
Table 1. Compositions of the diets.
Table 2. The nutritional values of the diets.
Diet Ingredient Amount (wt%)
Modified Stephan-Harris diet Sucrose 43
(sucrose diet) Wheat flour 22
Skimmed milk powder 32
Liver powder 2
Vegetable oil 1
Ewos R3 diet Oat flour 28
(standard diet) Wheat products 50
Soya meal 7
Fish powder 7
Fodder yeast 3
Minerals 3
Animal and vegetable fat 1
Vitamins and trace elements <1
Abbreviations: wt% = weight (g) per 100 g.
ComponentUnit / kg diet
Modified Stephan-Harris diet(sucrose diet)
Ewos R3 diet(standard diet)
RDA
Energy, kJ 15560 12600 18420Protein, g 143 210 133Fat, g 21.6 50 55Linoleic acid, g 0.8 1.5 2.4Calcium, g 5.9 9.9 5.6Phosphate, g 3.9 6.5 4.4Sodium chloride, g 3.8 7 6Magnesium, g 0.47 2 0.4Potassium, g 6 8 20Ferric, mg 18 190 38.9Copper, mg 5.3 30 5.6Retinol, mg 0.85 0.36 0.67dl - α - tocopherol acetate, mg 7.6 63 35Thiamin hydrochloride, mg 2.5 3.3 1.5Riboflavin, mg 7.1 12 2.8Pyridoxine hydrochloride, mg 1.8 4 7.8Vitamin B12,µg 7.6 20 5.6Calcium pantothenate, mg 17.2 10 8.9Free fluoride, ppm 0.00 0.05 0.00
Abbreviations: RDA = recommended daily allowance, National Research Council (1972).

31
s 5-8e ratsed toghed,/kgas
reshfameupsistur-
lim-ome
ntslongperi-
d6;
86).e thendard
ink-tersame
on-
4.3. Conduct of the experiment
The rats were 3 weeks old at the beginning of the experiments. Groups 1-4, groupand groups 9-11 were run at the same time. Inside the groups 1-4, 5-8 and 9-11, thwere taken from the same litters. The same number of rats from each litter was placeach of the groups. Each rat was randomly chosen for its group. The rats were weimarked and given an intraperitoneal injection of oxytetracycline hydrochloride (30 mgTerramycin®, Pfizer Corp., Brussels, Belgium) to mark the onset of dentine appositiona line visible in UV-light (Larmas & Kortelainen 1989, Hietalaet al. 1993).
In order to induce dental caries, the mouths of the animals were inoculated with a fsuspension ofStreptococcus sobrinus(ATCC 27531 K 1 Fitzgerald) on days 2 and 3 othe experiment and then weekly. The repeated inoculation of all the rats with the sbacteria also ensured the relative equality of the oral microbial flora in all the grothroughout the experiment. In order to avoid large dentinal carious lesions (and the dbances in odontoblastic metabolism induced by deep caries), the experiments wereited to six weeks' duration in the groups with the high-sucrose diet. Nevertheless, sbacterial invasion may have been progressing deep in the dentine (Luoma H.et al. 1987,Seppäet al. 1989) also disturbing odontoblast function. The duration of the experimewas based on pilot studies. The cariogenic challenge was adjusted to be sufficientlyfor both the initial and advanced carious lesions to be present at the end of the exments.
4.3.1. Induction of metabolic acidosis
The rats, referred to as acidotic, were divided into three groups and they all receiveadlib. distilled drinking water supplemented with 0.25 mol/L ammonium chloride (pH 5.0PHM62 Standard pH meter, Radiometer, Denmark; Angmar-Månsson & Whitford 19The sucrose diet was given to one acidotic group (6 week experiment, group 1), whilother two groups (6 and 7 week experiments, groups 2 and 9) were fed on the stadiet (Table 3).
Distilled water was used (instead of the tap water) to ensure the similarity of the dring water in every group throughout the experiments. The quality of the drinking wawas not an essential matter in these experiments, since all the groups consumed thekind of water (part of them supplemented with ammonium chloride or sodium bicarbate).

32
ng-eksoth-
nt torose
illed
er viaimen-ent
ardions.n the
4.3.2. Induction of metabolic alkalosis
Three alkalotic groups receivedad lib. distilled water supplemented with 0.25 mol/Lsodium bicarbonate (pH 8.3; PHM62 Standard pH meter, Radiometer, Denmark; Amar-Månsson & Whitford 1986). One group was fed on the sucrose diet for six we(group 3), while two groups received the standard diet, one for six (group 4) and theer for seven weeks (group 10) (Table 3).
4.3.3. Induction of respiratory alkalosis
Two groups were kept in a hypobaric chamber with an atmospheric pressure equivalean altitude of 3000 m (69,7 kPa) for 6 weeks. One group (group 5) was fed on the sucdiet and the other (group 6) on the standard diet (Table 3). They all received distdrinking water (pH 6.10; PHM62 Standard pH meter, Radiometer, Denmark).
The people taking care of the animals entered and passed the hypobaric chambairlock, so that the pressure remained constant in the chamber throughout the expertal period. Also, the blood samples from the tails of the rats at the end of the experimwere taken inside the hypobaric chamber to ensure the correct blood gas values.
4.3.4. Control rats (normalosis)
The remaining three groups received distilled drinking water (pH 6.10; PHM62 StandpH meter, Radiometer, Denmark) and were kept under normal atmospheric conditOne group was fed on the sucrose diet for 6 weeks (group 7) and the other two ostandard diet for 6 and 7 weeks (groups 8 and 11) (Table 3).
Table 3. Grouping and treatment of the rats in the experiments.
Group Male Female Diet Acid-base status Group abbreviationn n
6 weeks1 4 2 sucrose metabolic acidosis m-acid-suc 6wk2 5 1 standard metabolic acidosis m-acid-stan 6wk3 3 6 sucrose metabolic alkalosis m-alk-suc 6wk4 3 6 standard metabolic alkalosis m-alk-stan 6wk5 3 8 sucrose respiratory alkalosis r-alk-suc 6wk6 3 7 standard respiratory alkalosis r-alk-stan 6wk7 3 6 sucrose normalosis norm-suc 6wk8 3 6 standard normalosis norm-stan 6 wk
7weeks9 3 5 standard metabolic acidosis m-acid-stan 7 wk10 4 6 standard metabolic alkalosis m-alk-stan 7 wk11 5 4 standard normalosis norm-stan 7wk

33
sup-
rilerebes
A.)..
car-weresaw
4.4. Anesthesia and blood samples
At the end of the experiment the rats were anaesthetized by a minimum respiratorypression using a mixture of midazolam (Dormicum®; Roche, Basel, Switzerland), flu-anisone-fentanyl (Hypnorm®; Janssen Pharmaceutica, Brussels, Belgium) and stewater 1:1:2 0.2 mL/100 g of rat weight, given intraperitoneally. While the rats weunconscious, blood samples were taken from the cut tips of their tails into capillary tucontaining heparin and an "iron flea" for stirring (review: Beetham, 1982).
The blood samples were used for the measurement of pH, bicarbonate (HCO3-), base
excess (B.E.), and oxygen and carbon dioxide partial pressures (pCO2 and pO2), with ablood gas analyzer (Corning 168 pH/Blood Gas Analyzer, Corning Medical, U.S.After this, when still unconsious, the animals were killed in a carbon dioxide chamber
4.5. Preparation and analyses of the tooth samples
The mandibular molars were prepared for the analysis of dentine formation, dentinalies and mineral analysis using a method described by Keyes (1958). The mandiblesdissected, defleshed and sectioned sagittally by using a 0.1 mm thick diamond diskand water cooling, in an oblique parasagittal plane (Fig. 2).

34
rans-thirdin
to-tion
Fig. 2. Sectioning of the rat mandible.
4.5.1. Quantification of dentine apposition
From the lingual halves of the jaws and teeth, the areas of dentine under the middle tverse fissure of the first molar, the mesial one of the second molar and that of themolar (Fig. 3) were photographed on Kodak Ektachrome daylight film, 400 ASA,ultraviolet light (460 nm, C2 200W/4 mercury vapor lamp, Philips, Belgium). Phographing was done under an Orthoplan Ploemopak microscope with 16x magnifica(Leitz, Wetzlar, Germany; subsidiary, Midland, ON, Canada).

35
mea-the
an)Inc.,
res-andples,
EOLobeed.
a),ents
stan-werefirstamele andtine
The areas of dentine surrounded by a tetracycline-line and the pulp (Fig. 3) weresured planimetrically from video images by circumscribing them as they appeared onmonitor (Salora 445 A RGB, Salo, Finland; camera: Hitachi VKM 96 E, Tokyo, Japwith a serial "mouse" connected to a PCVision Frame Grabber (Imaging Technology,Woburn, MA., U.S.A.) (Larmas & Kortelainen 1989).
Fig. 3. Schematic drawing of sagittally sectioned mandibular molars of rat. Wide black line =enamel. Grey area = dentine apposition measured. Dotted line = tetracycline-marked onset ofdentine formation during the experiment.
4.5.2. Mineral analysis (EPMA)
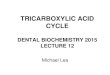
One of the two lingual halfs of the each sectioned mandible was embedded in epoxyin as a bulk sample to eliminate the influence of the sample thickness, then polishedcoated with carbon. For analyses of dentine mineral element contents from the saman electron microscope equipped with an electron probe microanalyzer (EPMA) (JJSM-35 Scanning Microscope with JEOL JCXA-733 Super Probe electron prmicroanalyzer with a ZAF-correction program; JEOL Ltd., Tokyo, Japan) was usExamination spot diameter was 10 micrometers, beam current 15 nA.
With EPMA, the amounts of calcium (Ca), phosphorus (P), fluoride (F), sodium (Nmagnesium (Mg) and total mineral contents were determined. These mineral elemwere given in oxides (CaO, P2O5, Na2O, MgO and ZnO) with the exception of fluoride.The actual weight percentages were calculated.
The analyses were made for the groups 2, 4, 6 and 8 (6 week's groups with thedard diet) because they did not include dentinal caries lesions. The measurementsperformed in two areas under the second (main) fissure of the first molars and the(main) fissure of the second molars: the first three spots between the dentino-enjunction and the tetracycline line, the second three spots between the tetracycline linthe pulp (Fig. 4). The third molar was excluded because of the small amount of denformed before the start of the experiment.
1st 2nd 3rd

36
sameed in
Fig. 4. Back-scattered electron image (COMPO) of rat's first and second mandibular molarshowing the spots from where the mineral elements were measured with EPMA.
4.5.3. Caries scoring
The areas of dentinal caries were measured from the same photographs under thefissures with the same method as the dentine apposition (Fig. 5). Method is describdetail in Larmas & Kortelainen (1989) and Hietalaet al. (1993).

37
vealroups-
lassi-ne
sixthreeigh-
kalo-is forbar)
tur-
Fig. 5. Photomicrograph of the crown of the third molar. The dentinal caries lesion is seen as afluorescent area (surrounded by dotted line). Fluorescent tetracycline line shows the onset ofdentine apposition during the experiment.
All the sectioned molars and fissures were also stained with Schiff reagent to rethe caries lesions in the dentine and enamel. The dye reacts with the aldehyde goriginating from proteolyses (Königet al. 1958). The lesions in each fissure (three fissures in the first, two in the second and one in the third molars) were examined and cfied into one of the following grades: N = no lesion, A = enamel lesion, T = initial dentilesion, B = advanced dentine lesion or C = cavitation (scoring system of Königet al.1958). (Hietalaet al. 1993).
4.6. Pilot studies
Before running the experiments described above, six pilot groups were made withcorresponding control groups. These animals were Long Evans rats and they wereweeks old at the beginning of the experiments. All these groups were fed on the hsucrose diet. Metabolic acidosis was induced for three and five weeks, metabolic alsis for seven and nine weeks, respiratory alkalosis for seven and respiratory acidossix weeks. The rats with respiratory acidosis were kept in a hyperbaric chamber (1.5containing 27% of oxygen and 0.03% of carbon dioxide in nitrogen. The other disbances in acid-base balance were created the same way as above.

38
e, butstrain,ges ofred tousing
peri-
d inan-
eas ofe per-n per-help-pro-
aly-skal-dentU --way
comecept-
thewereffect
paredwithvs. 7,the+10,hit-
t dif-
The dentine formation was measured basically the same way as mentioned beforolder equipments were used. Because of that, and also because of the different ratthe results can not be compared to those of the experimental groups. Thus, percentathe increase or decrease in weight gain, dentine formation and dentinal caries compathe corresponding control groups were calculated. Dentinal caries was explored bySchiff reagent. No statistical analyses were performed for the pilot groups.
4.7. Statistical analyses
Inter-examiner variations in determining the areas of dentine formed during the exment (Larmas & Kortelainen 1989) and carious lesions (Hietalaet al. 1993) by the abovemethods were insignificant. Nevertheless, minimum number of persons were involvehandling of the material. All blood samples were taken and all the sectionings of the mdibles were made by the author. The areas of dentinal caries (the author) and the ardentine apposition (another researcher trained by the author) were measured by onson. Schiff staining and analyses were made by the author. One laboratory techniciaformed the EPMA analyses. The statistical analyses were made by the author, withand guidance of the biostatistician. The analyses were performed by using SPSSgram (releases 6.1.3 and 7.5).
4.7.1. Statistics in blood gas analysis
According to the Shapiro-Wilks normality tests, the observations of the blood gas ansis were not normally distributed and therefore non-parametric tests were used. KruWallis -test was utilized to declare the need of comparisons of each two indepengroups. The Kruskal-Wallis statistics is a direct generalization of the Mann-Whitneytest for more than two independent groups. It is an analogous procedure to the oneanalysis of variance, but does not require making assumptions of observations tofrom normally distributed populations. Because the groups were small, p<0.1 was aced as a significant difference. (Glantz 1989)
When values of some groups were different according to the Kruskal-Wallis -test,Mann-Whitney U -test was used to determine which differences of each two groupssignificant. The Mann-Whitney U -test tests the hypothesis that a treatment had no ewhen observations are in two independent groups (Glantz 1989). Groups were comin multiple pairs: Each group with metabolic acid-base disturbance was comparedthe corresponding group with the normal acid-base balance and the same diet (12+9 vs. 8+11, 3 vs. 7, 4+10 vs. 8+11, 5 vs. 7 and 6 vs. 8+11). Also, the groups withsame treatment, but different dietary compositions were compared (1 vs. 2+9, 3 vs. 45 vs. 6 and 7 vs. 8+11). Because the multiple comparisons are ignored by the Mann-Wney U -tests, the two tailed p-values of p=0.02 or less were considered as significanference (instead of p=0.05).

39
auseof thelues.
iationd of
fewmilar). The02)
pH
ndenties ofd as
. Theplace
r ofpartlye line.epa-f thed as
nsid-oups1,
3.48).pre-
ed,en theseven
d onlye sixeek's
The logarithmic scale in the pH values did not affect the statistical analyses, becnon-parametric tests were used. In the non-parametric tests, ranks are given to eachnumerical values and the test is made by using these ranks, not the original vaBecause the data were not normally distributed, median (referenced by md) and varof measures (mainly presented by range from minimum to maximum) are given insteamean and standard deviation.
As metabolic and respiratory alkalosis and acidosis obtain the chronic stage in adays after the beginning of an experiment (Brewer 1990), the groups that had the sitreatments for 6 or 7 weeks were combined (groups 2 and 9, 4 and 10, and 8 and 11only values that differed significantly between the combined groups, were pH (p=0.0and pCO2 (p=0.002) in groups 8 and 11 (Mann-Whitney U -test). In group 8 the md ofwas 7.34 (range 7.25 to 7.42) and pCO2 7.33 kPa (5.69 to 9.28). In group 11 the md of pHwas 7.41 (7.35 to 7.45) and pCO2 5.76 kPa (5.03 to 6.49).
4.7.2. Statistics in measuring dentine formation
In these experiments, the molars in the right and left side were regarded as indepesamples when the dentine growth was measured. Because of the genetic similaritthe rats in this study, the molars in the right and left side of one rat can be considereequally dependent (or independent) on each other than the molars of different ratsgenetics of the rats which are from the same laboratory rat strain, bred in the sameand originate from the same litters are very similar.
Another reason for the combination of the right and left side was the small numbethe samples in each group. This was partly caused by the small number of the rats,for discarding of the samples judged unacceptable for the analyses (the tetracyclinwas not visible in 93 teeth and sectioning was not of acceptable accuracy in 17 teeth)
The dentine formation during the experiment was measured from each molar srately. Thus, 33 individual groups were formed of the results. The measured areas odentine were normally distributed in 31 groups out of 33, when p>0.09 was regardenormally distributed in Shapiro-Wilks -test and skewness and kurtosis were also coered. (Shapiro-Wilks normality test is appropriate when the groups are small.) The grnot meeting the criteria for normality were as follows: group 11, first molar (p=0.0skewness -1.16 and kurtosis 0.79) and group 11, second molar (p=0.05, 1.22 andConsidering the small number of samples in each group, these two groups did notvent the use of the parametric tests.
Global testing between all the groups (F-test: one-way-ANOVA) was not needbecause all possible pairwise comparisons were not appropriate. Comparison betwegroups was made the same way as in the blood gases, except that groups with theweek's experimental period (groups 9, 10 and 11) were kept separated and compareto each other (9 vs. 11 and 10 vs. 11). As obvious, less dentine was formed during ththan the seven week's experiments preventing the combining of the six and seven wgroups.

40
les t-vari-
-tests,of the
ine,t. Withaticlyreli-
tribut-
ereperi-ringosened t-
sub-
andas thexperi-werea dif-o, insec-
y the
thesure-
ars ofr than
itneyulti-
an in
Comparisons of the two groups at a time was performed with independent samptest. Equality of variances were determined by using Levene's test (when p<0.09, theances were unequal) and an appropriate version of the t-test was used. In the tp=0.01 (or less) was considered as a significant difference, because of multiple usegroups in comparisons.
4.7.3. Statistics in mineral analysis
Because of the great variability, which is typical for EPMA measurements in the dentmedian of the three measurements in each spot was chosen to represent that pointhis method, the unacceptable values (the very high and very low values) are automexcluded. Limits for acceptable values are not given which makes the method moreable compared to the use of mean values. The chosen values were not normally dised in any of the groups. Thus, non-parametric tests were used in comparisons.
Global test (Kruskal-Wallis) was used to show the differences (no differences wfound) between the groups in the mineral elements of dentine formed before the exment. Wilcoxon signed-rank test (Wilcoxon matched pairs test) was used in compathe dentine formed before to that formed after the start of the experiment (the pre-chsignificance level was 0.05). The Wilcoxon signed-rank test is analogous to the pairtest, testing that the treatment had no effect when observations are from the samejects (like before and after treatment) (Glantz 1989).
Each group was compared to the control group (group 8) and also to the groups 24 were compared to each other (Mann-Whitney U -test). In these tests, each value wcalculated difference between the measurement before and after the start of the ement. The tendencies of both molars in the results of the comparing of the groupsanalyzed and found quite similar, except that in fluoride and phosphorus, there wasference between the groups 6 and 8 in the first molar but not in the second one. Alssodium, there was a difference between the groups 4 and 8 in the first but not in theond molar. This was thought to be caused by the small number of the samples or bslightly different stage of development in the first and second molar.
Based on the results above, the genetic similarities of the rats in this study andnearly same developmental stage of the first and second molar, the mineral meaments of the first and second molars were combined. Thus, the first and second molthe same rat were considered as equally dependent (or independent) on each othethe molars of different rats. Then, the groups were compared by using the Mann-WhU -test. p=0.03 (or less) was considered as a significant difference, because of the mple use of the groups in comparisons. Here, the number of the groups is smaller thcomparing blood-gas values, thus the significance level is p=0.03 instead of p=0.02.

41
cari-suressults
clud-
d byionsd asystemooth,e rigt
raty U-
4.7.4. Statistics in measuring caries
In calculating the areas of dentinal caries lesions, based on the fluorescence of theous dentine observed under the fluorescent light, such a large number of intact fiswere present, that rational statistical analysis was not appropriate. As such, the resupplement the other findings concerning caries. Groups with standard diet were exed from this data because of the very small number of carious lesions.
The results of the Schiff staining were compared by using a method describeKönig et al. 1958. In this method, intact fissures (N) are scored as 0 and enamel les(A) as 1. Initial (T) and advanced (B) dentinal lesions and cavitations (C) are all score7 to emphasize the difference between enamel and dentinal lesions. (This scoring shas been previously used for example in comparing dysfunction indexes.) In every tthe scores of each fissure were summarized (3 fissures from left side and 3 from thside in the first, 2 from both sides in the second and 1 from both sides in the thirdmolar). These sum scores were used in compairing the groups by using Mann-Whitnetest (non-parametric data). Pre-chosen significance level was set at p<0.05.

ps inup 3)oupnot
ed as
aci-le as
lkalo-also
pira-en-
losis.and
the
5. Results
5.1. Pilot studies
The results of the pilot studies are given in percentages compared to the control grouTable 4. Two experimental groups, which had the same treatments (group 1 and groare included. All the pilot groups were fed on the high-sucrose diet. One control grwith normalosis and high-sucrose diet was run for each of the pilot groups (datashown). Caries was scored with Schiff reagent and T, B and C lesions were regarddentinal lesions.
The numbers of the rats in pilot groups with respiratory alkalosis and respiratorydosis were small and standard deviations were high. The results were not as reliabthose presented in Table 4 and therefore they are not presented in it. In respiratory asis the weight gain was higher in the males, dentine formation was decreased anddentinal caries was slightly decreased (the control group had plenty of caries). In restory acidosis, weight gain was slightly and dentine formation apparently increased. Dtinal caries were increased in the first and decreased in the third molars.
Table 4. Results of the pilot studies on the effects of metabolic acidosis and alkaIncrease (+) or decrease (-) of the weight gain of the rats, and dentine formationdentinal caries in the 1st, 2nd and 3rd molars given in percentages compared tocontrols. All the groups were fed the high-sucrose diet (see Table 1).
Group nWeight Dentine formation Dentinal caries
Male Female 1st 2nd 3 rd 1st 2nd 3 rd
m-acid-sucpilot 3 wkpilot 5wkexp. 6 wk
1066
-27-23-11
-24-28-9
-25-15-9
-35-29-13
-4-9-3
+18+32+47
+29+50+33
+6+39+56
m-alk-sucexp. 6 wkpilot 7 wkpilot 9 wk
988
+4+28
-5+32
+4+20+16
-1+8+23
+4+8-3
-11-13-8
-42-10-23
-6+1-48
Abbreviations: exp. = experimental group, n = number of the rats.

43
wk)wasotic
con-with
anal-small. Theales
dardiffer-weight
tal
roupsheseeforeental
5.2. General health
Two rats died during the ordinary experiment: one rat from the group 1 (m-acid-suc 6and one from the group 9 (m-acid-stan 7 wk). Thus, the mortality of the animalswithin the usual limits, even though both of the rats that died were from the acidgroups.
No significant differences in general appearance and behaviour or food and watersumption were seen between the groups. The weight gain of the acidotic animalsboth diets (groups 1, 2 and 9), was lower than that of the others (Table 5). Statisticalyses concerning the weight differences were not appropriate because of the verynumber of rats in the groups, when the groups were divided into males and femalesmale rats with the high-sucrose diet seemed to gain slightly less weight than the mwith the standard diet with the exception of the rats with metabolic acidosis and standiet (group 2). In females, the order was the reverse (except in the group 2) and the dences between the groups were smaller. As expected, the female rats gained lessthan the males.
Table 5. Mean weight gain (in grams) during the periods of the ordinary experimenstudies. The groups are arranged according to the weight of the males.
5.3. Blood properties
Blood pH, base excess, bicarbonate, carbon dioxide and oxygen values of the rat gat the end of the experiment are given in Figures 6-10. No significant differences in tvalues were found between the male and the female rats in any of the groups. Therthe values of the sexes were combined. Also, the groups that had the same experim
GroupWeight gain
Male Female
6 weeks
2 (m-acid-stan) 144 99
1 (m-acid-suc) 166 118
5 (r-alk-suc) 178 117
7 (norm-suc) 186 130
3 (m-alk-suc) 193 123
8 (norm-stan) 201 118
6 (r-alk-stan) 205 111
4 (m-alk-stan) 208 134
7 weeks
9 (m-acid-stan) 191 110
10 (m-alk-stan) 239 138
11 (norm-stan) 250 136

44
dura-been
settings for 6 or 7 weeks were combined, because the one week's difference in thetion does not make any difference in the blood gas values since the chronic stage hasobtained in a couple of days after the onset of the experiments (Brewer 1990).
Fig. 6. Blood pH in the experimental groups. Each 7-week group is included in thecorresponding 6-week group: m-acid-stan (groups 2 and 9), m-alk-stan (4 and 10) and norm-stan groups (8 and 11) are combined. In box plots the box presents 1st and 3rd (upper andlower) quartiles with the median value inbetween. The whiskers give the lowest and highestvalues. Extreme values are marked as circles. n = number of blood samples.
Fig. 7. Blood base excess (B.E.) in each group given in mEq/L. For groups and box plotpresentation: see Fig. 6.
1: m-acid-suc (n=6)
2+9: m-acid-stan (n=13)
3: m-alk-suc (n=9)
4+10: m-alk-stan (n=16)
5: r-alk-suc (n=9)
6: r-alk-stan (n=8)
7: norm-suc (n=9)
8+11: norm-stan (n=18)
6,9 7,57,1 7,3
1: m-acid-suc (n=6)
2+9: m-acid-stan (n=13)
3: m-alk-suc (n=9)
4+10: m-alk-stan (n=16)
5: r-alk-suc (n=9)
6: r-alk-stan (n=8)
7: norm-suc (n=9)
8+11: norm-stan (n=18)
-20 20-10 0 10

45
Fig. 8. Blood bicarbonate (HCO3-) given in mmol/L. For groups and box plot presentation: see
Fig. 6.
Fig. 9. Blood carbon dioxide partial pressure (pCO2) given in kPa. For groups and box plotpresentation: see Fig. 6.
1: m-acid-suc (n=6)
2+9: m-acid-stan (n=13)
3: m-alk-suc (n=9)
4+10: m-alk-stan (n=16)
5: r-alk-suc (n=9)
6: r-alk-stan (n=8)
7: norm-suc (n=9)
8+11: norm-stan (n=18)
10 5020 30 40
1: m-acid-suc (n=6)
2+9: m-acid-stan (n=13)
3: m-alk-suc (n=9)
4+10: m-alk-stan (n=17)
5: r-alk-suc (n=9)
6: r-alk-stan (n=8)
7: norm-suc (n=9)
2 124 6 8 10
8+11: norm-stan (n=18)

46
om-fer-nd 6).
.ere
th the8, 3
epple-lyallyacuteheand
heirdiet
Fig. 10. Blood oxygen partial pressure (pO2) given in kPa. For groups and box plotpresentation: see Fig. 6.
The groups with the same drinking water and pressure, but different diet, were cpared (group 1 vs. group 2+9, 3 vs. 4+10, 5 vs. 6 and 7 vs. 8+11). No significant difences were found except between the groups with respiratory alkalosis (groups 5 aIn group 5 (r-alk-suc) the concentration of bicarbonate (HCO3
-) (p=0.01) and the partialpressure of carbon dioxide (pCO2) (p=0.004) were lower than in group 6 (r-alk-stan) (Fig8 and 9) (Mann-Whitney U-test). In the following are presented the results, which wobtained when each group with metabolic acid-base disturbance was compared wicorresponding control group (norm-suc or norm-stan) (group 1 vs. group 7, 2+9 vs.vs. 7, 4+10 vs. 8, 5 vs. 7 and 6 vs. 8).
5.3.1. Metabolic acidosis
When blood pH, B.E. and HCO3- are all considered, the animals were acidotic in th
groups (m-acid-suc and m-acid-stan, groups 1 and 2+9) receiving drinking water sumented with NH4Cl (Fig. 6, 7 and 8). pH was lowered in both diet groups, significantso with the standard diet (group 2+9, p=0.001) (Mann-Whitney U-test). In chronicaltered acid-base balance pH is buffered and thus closer to the normal value than instage, thus B.E. and HCO3
- reveal the disturbances more clearly. B.E. (p=0.002 with thigh-sucrose diet in group 1 and p=0.0001 with the standard diet in groups 2+9)HCO3
- (p=0.001 and p=0.009 respectively) were significantly lowered compared to tcontrols with normalosis and high-sucrose diet (group 7) or normalosis and standard(group .8+11).
1: m-acid-suc (n=6)
2+9: m-acid-stan (n=13)
3: m-alk-suc (n=9)
4+10: m-alk-stan (n=17)
5: r-alk-suc (n=9)
6: r-alk-stan (n=8)
7: norm-suc (n=9)
4 128 16
8+11: norm-stan (n=18)

47
drink-on-
gh-d to. 7)p 7
oup
toryas
andup 8
tion,ithup 6by
d inbodynifi-
vs.
f sta-pari-
ig. 11
5.3.2. Metabolic alkalosis
pH, base excess and bicarbonate values were elevated in the groups with alkaloticing water (m-alk-suc and m-alk-stan, groups 3 and 4+10) (Fig. 6, 7 and 8), which cfirmed the alkalotic effect of the sodium bicarbonate containing water. With the hisucrose diet (group 3, Fig. 6), the elevation of pH was significant (p=0.008) comparethe group 7 with normalosis and high-sucrose diet (Mann-Whitney U-test). B.E. (Figwas higher with both diets (p=0.0003 with the high-sucrose diet in group 3 vs. grouand p=0.005 with the standard diet in groups 4+10 vs. group 8+11). Also HCO3
- was sig-nificantly elevated by metabolic alkalosis (p=0.0004 group 3 vs. 7 and p=0.0004 gr4+10 vs. 8+11, respectively).
5.3.3. Respiratory alkalosis
The measured blood values (Fig. 6, 7, 8, 9 and 10) were typical to chronic respiraalkalosis in the groups 5 and 6 (r-alk-suc and r-alk-stan). Significantly alkalotic pH wfound only when the high-sucrose diet (group 5, p=0.0007, Mann-Whitney U-test)the standard diet groups (group 6 vs, p=0.01) were compared to the original gro(norm-stan 6 wk).
Here respiratory alkalosis is caused by the lack of oxygen leading to hyperventilawhich lowers the concentration of carbon dioxide (visible with both diets: p=0.0003 wthe high-sucrose diet in group 5 vs. group 7 and p=0.002 with the standard diet in grovs. group 8+11). Hyperventilation did not fully correct the lack of oxygen inducedhypobaric conditions. With the standard diet in group 6, pO2 was significantly lowered(p=0.0003) compared to the control group 8+11.
Lower concentration of carbon dioxide (and thus of carbonic acid), is compensatea chronic stage by reducing the amount of bases in blood. This way a mammaliantends to return pH towards normal. Thus B.E. was lower in the groups 5 and 6 (sigcantly so in the group 6 with the standard diet vs. group 8+11, p=0.0008). HCO3
- wasreduced significantly with both diets (p=0.0003 with the high-sucrose diet in group 5group 7 and p=0.0001 with the standard diet in group 6 vs. group 8+11).
5.4. Dentine formation
The amounts of the dentine formed during the experimental periods and the results otistical comparison (independent samples t-test) are given in Table 6. For easier comson, dentine formation in the second molars (as an example) is also presented in Fand 12.

48
thes 8 and
high-parately)
Table 6. Mean dentine formation in three molars in square micrometers x103 during theexperimental period.
Fig. 11. Dentine formation in square micrometers in the second molars in the six week'sexperiments. The box presents the 1st and 3rd (upper and lower) quartiles with the medianvalue inbetween. The whiskers give the lowest and highest values. n = number of the teeth.
Group1st Molar 2nd Molar 3rd Molar
n Mean SD n Mean SD n Mean SD
6 weeks
1 (m-acid-suc) 10 180 25 10 148 32 8 341 34
2 (m-acid-stan) 10 209* 42 11 181* 33 12 349* 22
3 (m-alk-suc) 13 206# 28 14 168# 19 13 368 36
4 (m-alk-stan) 16 260 34 15 207* 23 16 391 34
5 (r-alk-suc) 14 176# 34 14 153# 25 13 342 25
6 (r-alk-stan) 18 243 21 18 204* 22 16 357* 34
7 (norm-suc) 16 197# 44 16 170# 34 15 353# 24
8 (norm-stan) 13 262 24 13 242 27 12 398 27
7 weeks
9 (m-acid-stan) 14 210* 27 11 163* 21 12 322* 45
10 (m-alk-stan) 18 249* 21 18 200* 20 155 380 42
11 (norm-stan) 17 292 20 17 238 22 168 387 36
Abbreviations: n = number, SD = standard deviation, * = significant difference (connected by ]) betweenexperimental and corresponding control group (groups 1, 3 and 5 versus group 7, groups 2, 4 and 6 versugroups 9 and 10 versus 11, each molar separately). # = significant difference (connected by <) betweensucrose and standard diet group (group 1 versus 2, 3 versus 4, 5 versus 6 and 7 versus 8, each molar se(p = 0.01 or less in independent samples t-test).
1: m-acid-suc (n=10)
2: m-acid-stan (n=11)
3: m-alk-suc (n=14)
4: m-alk-stan (n=15)
5: r-alk-suc (n=17)
6: r-alk-stan (n=18)
7: norm-suc (n=16)
8: norm-stan (n=13)
100 000 150 000 200 000 250 000 300 000

49
theps 1,3 vs.t-test)the
weres. 7,fol-
high-
, these ind 3rd
tion)riodek'ssec-
spi-rats
Fig. 12. Dentine formation in square micrometers in the second molars in the seven weeks'sexperiments. For box plot presentation: see Fig. 11.
According to Table 6, the reducing effect of the high-sucrose diet, as compared tostandard diet on dentine apposition, was visible in all the high-sucrose groups (grou3, 5 and 7). In the first and second molars it was more apparent (p<0.001 in groupgroup 4, 5 vs. 6, and 7 vs. 8 in both first and second molars, independent samplesthan in the third molars. In the third molars, the difference was significant betweengroups 7 and 8 (p<0.001).
When the rat groups with an acid-base disturbance and the high-sucrose dietcompared to the controls with the high-sucrose diet (group 1 vs. 7, 3 vs. 7 and 5 veach molar separately), no significant differences were found, although the resultslowed the same patterns as in the groups with the standard diet. The effect of thesucrose diet seemed to be independent of the acid-base disturbance.
In the groups with metabolic acidosis and the standard diet (groups 2 and 10)amount of dentine apposition was reduced in all the molars when compared to thothe control groups (groups 8 and 11) (6 weeks: 1st molar p=0.003, 2nd p<0.001 anp<0.001, 7 weeks: p<0.001 in all the molars.)
In metabolic alkalosis and the standard diet (groups 4 and 11), a difference (reducwas found in the second molar (p=0.001) in the group with 6-week's experimental pe(group 4), when compared to the controls with the standard diet (group 8). In the 7-weexperiment (group 10), the amount of dentine was reduced in the first (p<0.001) andond (p<0.001) molar compared to the controls (group 11).
Statistically significant reduction in the dentine formation was also observed in reratory alkalosis (group 6) in the second (p<0.001) and third (p=0.002) molars in thefed the standard diet for 6 weeks, as compared to the group 8.
9:m-acid-stan (n=11)
10:m-alk-stan (n=18)
11:norm-stan (n=17)
100 000 150 000 200 000 250 000 300 000

50
theCa/P
r theps in
thatido-is)tentsnt of
iner-
tinethoseCa,er,
olicMgthe
5.5. Dentine minerals
Only groups fed on the standard diet (the 6 week's experiments) were included inmineral element analyses in order to avoid caries induced demineralization zones.ratio was the same (1.8) in all the groups in dentine formed both before and afteonset of the experimental period. Also, no differences were found between the grouany of the measured mineral elements of dentine formed before the experiment.
The amount of calcium in dentine formed before the experiment was higher thanformed during the experiment in all the groups, except in the group 2 (metabolic acsis), in which it was lower (Table 7). In addition to this, in group 4 (metabolic alkalosthe amount of fluoride increased and the amount of phosphorus and total mineral condecreased during the experiment. In the group 6 (respiratory alkalosis) the amoumagnesium decreased and in the group 8 (controls) sodium, phosphorus and total mals decreased during the experiment.
When the change in mineral values (dentine formed during the experiment - denformed before the experiment) of the groups 2, 4 and 6 were compared (Table 7) toof the control group 8, the group 2 (metabolic acidosis) differed most: the values ofMg, Na and total minerals were higher in the group 2. The amount of fluoride was lowbut not significantly. When the "opposite" groups 2 (metabolic acidosis) and 4 (metabalkalosis) were compared, the amounts of Ca (p=0.008, Mann-Whitney U -test),(p=0.03), P (p=0.005) and total minerals (p=0.007) were higher in group 2, butamount of fluoride was lower (p=0.027).

51
(b)m oftheental
anksr less,
Table 7. Median (md) dentine mineral contents in dentine formed before (a) and duringthe experimental period, given in weight percentages. Minimum, median and maximuthe difference between mineral contents in dentine formed during and beforeexperiment. P-values for comparisons between b versus a and between the experimgroups (2, 4, 6) versus the control group (8).
MineralGroup
Beforemd. a
Duringmd. b
Difference Diff. b-ap-value
Comp. to controlp-valueMin. Median Max.
Calcium2 (m-acid-stan) 30.89 32.05 -0.06 0.60 2.05 0.021* 0.008#4 (m-alk-stan) 32.35 30.52 -7.92 -1.70 5.98 0.034* 0.6076 (r-alk-stan) 31.79 30.24 -5.77 -1.20 2.87 0.036* 0.9838 (norm-stan) 31.69 30.69 -8.14 -0.83 1.78 0.036*
Magnesium2 (m-acid-stan) 0.37 0.35 -0.10 0.04 0.11 0.203 0.017#4 (m-alk-stan) 0.28 0.27 -0.18 -0.01 0.10 0.121 0.8436 (r-alk-stan) 0.46 0.31 -0.23 -0.07 0.06 0.015* 0.3518 (norm-stan) 0.35 0.33 -0.22 -0.03 0.05 0.078
Fluoride2 (m-acid-stan) 0.58 0.49 -0.33 -0.05 0.40 0.114 0.0314 (m-alk-stan) 0.38 0.55 -0.25 0.16 0.86 0.030* 0.3046 (r-alk-stan) 0.47 0.41 -0.43 -0.04 0.54 0.363 0.0788 (norm-stan) 0.47 0.50 -0.24 0.07 0.44 0.061
Sodium2 (m-acid-stan) 0.55 0.54 -0.06 -0.02 0.05 0.203 0.023#4 (m-alk-stan) 0.48 0.46 -0.18 -0.03 0.29 0.171 0.1056 (r-alk-stan) 0.55 0.43 -0.15 -0.02 0.11 0.256 0.0368 (norm-stan) 0.60 0.52 -0.32 -0.09 0.09 0.006*
Phosphorus2 (m-acid-stan) 17.48 18.50 -1.00 0.36 2.02 0.241 0.0314 (m-alk-stan) 17.30 16.89 -4.70 -0.58 0.45 0.003* 0.9376 (r-alk-stan) 16.38 17.01 -1.80 0.12 2.83 0.496 0.0718 (norm-stan) 17.89 17.45 -7.83 -0.41 1.74 0.041*
Total2 (m-acid-stan) 84.24 89.62 -10.55 2.82 7.43 0.203 0.017#4 (m-alk-stan) 83.48 81.96 -14.48 -3.35 2.00 0.008* 0.9686 (r-alk-stan) 82.78 84.86 -11.01 -0.86 6.74 0.363 0.3308 (norm-stan) 87.28 84.02 -32.25 -3.67 3.89 0.031*
* = significant difference between b versus a values inside the groups (p = 0.05 or less, Wilcoxon Signed RTest). # = significant difference between b-a values in the experimental versus control groups (p = 0.03 oMann-Whitney U -test).

52
havetheresidethe
) andan oftheand
sis)suressis)
meta-mer-3. Ins are
5.6. Caries
5.6.1. Areas of dentinal caries
In Table 8, the areas of caries lesions were calculated only from the fissures, whichdentinal caries. Only the groups with the high-sucrose diet were included, becausewere no dentinal caries lesions in the groups with the standard diet. The right and leftdid not differ markedly and they are combined. Also there was no difference betweenmale and the female rats, thus their data are combined, too.
Table 8. Areas of dentinal caries lesions. Total numbers of the fissures examined (npercentages of the fissures with dentinal caries lesions. Minimum, maximum and methe lesion area in each group, given in square micrometers (calculated only fromfissures with lesion). The experimental groups are arranged according to the numberthe mean size of the lesion.
In the first molars, the carious lesions were smallest in groups 3 (metabolic alkaloand 7 (controls). In both of those groups, there were also the greatest number of fiswith no dentinal caries. In the groups 1 (metabolic acidosis) and 5 (respiratory alkalothe lesions were the largest and more numerous.
In the second molars, there were the least caries and fewest lesions in group 3 (bolic alkalosis). Lesions were equally large in the groups 1, 5 and 7, and the most nuous in the group 5. For easier comparison, a box plot presentation is given in Fig. 1the figure, the right and left side are also combined and the fissures with no carieincluded.
Molar GroupFissures Lesions Area
n % Min Max Mean
first 5 (r-alk-suc) 21 81 800 13330 4810
1 (m-acid-suc) 12 67 440 9240 3980
3 (m-alk-suc) 18 11 490 5380 2940
7 (norm-suc) 18 44 40 7080 3420
second 5 (r-alk-suc) 22 91 640 9460 4580
1 (m-acid-suc) 12 50 680 8330 4630
3 (m-alk-suc) 18 22 210 1730 1057
7 (norm-suc) 18 56 930 12260 4470
third 5 (r-alk-suc) 19 100 5510 39350 16900
1 (m-acid-suc) 9 100 3140 25060 14760
3 (m-alk-suc) 18 78 1040 16830 7190
7 (norm-suc) 15 87 2140 16560 6500

53
.:
firstroup 5h no
dietIn alle rest
ion,sione cat-
Fig. 13. Areas of dentinal caries in the second molars of the rats in the groups 1, 3, 5 and 7Extreme values are marked as circles and outline values as asterisks. For box plot presentationsee Fig. 11.
In the third molars, lesions were generally larger and more numerous than in theand second molars. Lesions were smallest in the groups 3 and 7 and largest in the g(not much difference between the groups 1 and 5). There was only a few teeth witdentinal caries, most of them existed in the group 3 (metabolic alkalosis).
5.6.2. Caries scoring
Schiff reagent revealed same amounts of caries in the groups with the standard(groups 2, 4, 6, 8, 9, 10, 11 were compared to each other in pairs) (data not shown).those groups, less than half of the fissures were affected by enamel lesions only, thwere intact.
The results of Schiff staining are given in Table 9. According to the dye penetrateach fissure was classified as healthy (N), enamel lesion only (A), initial dentinal le(T), more advanced dentinal lesion (B) or cavitation (C). Percentages of each of thesegories are given separately.
1:m-acid-suc (n=12)
3:m-alk-suc (n=18)
5:r-alk-suc (n=22)
7:norm-suc (n=18)
-2000 2000 6000 10000 14000

54
f theare
pari-Table
eachand
ntinal
ced
=
Table 9. Results of Schiff staining of the caries lesions. Percentages are given ofissures with no caries (N) and lesions of different depths (A, T, B, C). The groupsarranged according to Table 8.
Lesions were scored and the dentinal lesions (T, B and C) were combined for comson of the groups. The results of this scoring (see: 4.7.4. Statistics) are presented in10. The sides were combined.
Table 10. Minimum, median and maximum of the sum scores of the caries lesions ingroup (Schiff staining). Healthy fissures (N) were scored as 0, enamel lesions (A) as 1dentinal lesions (T, B, C) as 7 to emphasize the difference between enamel and delesions. The groups arranged according to Tables 8 and 9.
Molar Group n N A T B C
first 5 (r-alk-suc) 66 1,5 25,8 15,2 40,8 16,7
1 (m-acid-suc) 36 2,8 16,6 27,8 27,8 25,0
3 (m-alk-suc) 54 13,0 64,7 16,7 5,6 0,0
7 (norm-suc) 54 3,7 63,0 5,6 25,9 1,8
second 5 (r-alk-suc) 44 0,0 2,3 20,4 63,7 13,6
1 (m-acid-suc) 24 0,0 16,7 16,7 50,0 16,6
3 (m-alk-suc) 36 25,0 66,6 5,6 2,8 0,0
7 (norm-suc) 36 5,6 44,4 25,0 22,2 2,8
third 5 (r-alk-suc) 22 0,0 22,7 18,2 45,5 13,6
1 (m-acid-suc) 12 0,0 16,7 25,0 50,0 8,3
3 (m-alk-suc) 18 5,6 72,1 16,7 5,6 0,0
7 (norm-suc) 18 5,6 66,6 5,6 22,2 0,0
Abbreviations: n = number of fissures, N = no lesion, A = enamel lesion, T = initial dentinal lesion, B = advandentinal lesion, C = cavitation.
Molar Group n Min Md Maxfirst 5 (r-alk-suc) 66 8 15 21
1 (m-acid-suc) 36 8 21 213 (m-alk-suc) 54 1 3 217 (norm-suc) 54 3 9 15
second 5 (r-alk-suc) 44 8 14 141 (m-acid-suc) 24 8 14 143 (m-alk-suc) 36 1 2 87 (norm-suc) 36 1 8 14
third 5 (r-alk-suc) 22 1 7 71 (m-acid-suc) 12 1 7 73 (m-alk-suc) 18 0 1 77 (norm-suc) 18 0 1 7
Abbreviations: n = number of fissures, N = no lesion, A = enamel lesion, T = initial dentinal lesion, Badvanced dentinal lesion, C = cavitation.

eri-ndi-ver,not
n the, butas-ergy
ation
nalomenger
stab-bal-
ce ofrowtht the
ani-
in the
therom
6. Discussion
6.1. General health
The growth of the animals, with the exception of metabolic acidosis, during the expment indicated that the animals were growing normally and that the experimental cotions did not endanger their health. The animals with metabolic acidosis, howeappeared healthy. Thus the effects of the experimental conditions evidently werereflections of severe problems in the general health.
The rats fed on the high-sucrose diet gained slightly less weight than those fed ostandard diet. The modified Stephan-Harris and Ewos R3 diets differ in many aspectstheir effect on the general health of rats has been shown previously to be equal (Larmetal. 1992, Tjäderhaneet al. 1994, Autioet al. 1997). The diets are slightly under the recommended energy level (Table 2). Rats are known to regulate food intake to meet enneed (National Research Council 1972) and food was freely available, thus no deprivof energy resulted.
Both diets are nutritionally acceptable for growing rats, although according to NatioResearch Council (1972), the amount of fat is too low in high-sucrose diet. Also sminor deficiences in vitamins and minerals exist in both diets, but they do not endathe health of the animals (Huumonenet al. 1997). Control groups of both diets (group 7fed on modified Stephan-Harris diet and groups 8 and 11 on Ewos R3 diet) were elished to allow a comparison of each of the experimental groups with an acid-base imance to the corresponding control group with the same diet.
The reduced weight gain in the acidotic animals has been found to be a consequendisturbances in the bone calcium and muscle protein metabolism, causing retarded g(May et al. 1986). The same mechanisms that affect the bone are also likely to affecdentine, and our results do indeed indicate reduced dentine formation in the acidoticmals.
Metabolic alkalosis has been thought to cause corresponding anabolic changesbone and muscle growth (Bushinskyet al. 1989). We found only a hint of the anaboliceffects: the rats gained a little more weight in the group with metabolic alkalosis andstandard diet. Also one pilot group supported this finding (no weights were available fthe other pilot group).

56
theillary79),otic
ilddingbyndsg ofon &peri-
selypen-
astur-Kacz-thus
ass-.ortedplander tosem-
for
ere),in the
lularonto-
auseore toed by
um-
6.2. Acid-base balance
Rats have slightly more alkaline blood than humans. Koppanget al. (1984) reported nor-mal range in capillary blood of humans to be pH 7.38-7.44. The technique of takingblood sample from the cut tails resembles the measuring of blood gases from a capblood sample in humans (Beetham 1982). In the study of Whitford & Pashley (197.46 was the blood pH of the control rats. However, lower pH values for the normalrats have also been given (pH 7.41-7.45, Whitford & Reynolds 1979).
Whitford & Pashley (1979) considered blood pH 7.41 to be an evidence of a mchronic metabolic acidosis in rat. In their experiment, acidosis was induced by adNH4Cl (0.25M) to the drinking water. Mild chronic metabolic alkalosis was induced0.15M NaHCO3, respectively, and the blood pH was 7.53. Blood pH apparently depeon the site from which the sample is taken, the device for measuring pH, the handlinthe blood samples and the condition of the animals (stress, anesthesia etc.) (UptMorgan 1975). Thus, pH values are not entirely comparable between different exments.
Our results concerning the blood-gas values in the normalotic groups followed clothose taken from rats with cannula implanted in the aortic arch under anesthesia withtobarbital or inactine (Brun-Pascaudet al. 1982). The acid-base balance was what hbeen considered normal in the control groups without metabolic or respiratory disbances (groups 7, 8 and 11), except that pCO2 -value was higher in several cases (marczyk & Reinhardt 1975). Anesthesia tends to cause ventilatory depression andraise the pCO2 values (Bar-Ilan & Marder 1980, Brun-Pascaudet al. 1982). Probablybecause of that, pCO2 values in our experiments were above normal and the variation whigh within the groups. pH and HCO3
- parameters are regulated by slower metabolic sytems and can thus be considered more reliable when measuring the acid-base status
The metabolic acidosis induced here was moderate relative to the previously repblood gas values for rats (Kaczmarczyk & Reinhardt 1975) and humans (Pesce & Ka1987). The aim was to keep the changes in the acid-base balance moderate in ormaintain the good health of the animals and to obtain a physiological stage (i.e. rebling diet-induced acid-base disturbance in humans). The B.E. and HCO3
- valuesrevealed the differences better than did the pH, indicating the involvement of bufferscorrection of the pH values. This confirmed the chronic state (Pesce & Kaplan 1987).
In these series of experiments (unlike in one of the pilot groups, not presented hthe high-sucrose diet itself was not seen to cause acidosis or any other distubancesacid-base balance. Blood pH is very well buffered, while the changes in the intracelpH are yet possible. The acid-base conditions and buffer mechanisms inside the odblast cells are extremely difficult (if not impossible) to measure.
The use of ammonium chloride for inducing acidosis has been under review becsome investigators have suspected that its effects on the bone may be attributable mthe chloride ion than to the hydrogen ion and acidosis as such. This has been refuttesting the effect of various concentrations of nitric acid on the bonein vitro, whereuponthe results approximated those obtained with an addition of HCl when equivalent nbers of protons had been added (Goldhaber & Rabadjija 1987).

57
natewas).is anence
ildby a
sis:uffersatedse ofnt of
rats,maseeni-asts.du-
an
the
ss.roups
t leastacid-e pilotrentlyoupss oftine
rats,asng
The results obtained in the blood gas analysis of the groups given sodium bicarboin drinking water (groups 3, 4 and 10) indicated that the chronic metabolic alkalosismild (Brun-Pascaudet al.1982, Kaczmarczyk & Reinhardt 1975, Pesce & Kaplan 1987There has been discussion about whether orally administered sodium bicarbonateappropriate tool for creating metabolic alkalosis in the rat because it causes a differof less than 3 meq in serum bicarbonate values (Atkins & Burg 1985, Knepperet al.1985, Gallaet al. 1991). In our experiments the alkalosis was intentionally kept at a mlevel in order to keep the animals healthy. Alkalosis is less tolerated than acidosismammalian body.
Metabolic compensation was clearly visible in the groups with respiratory alkalothe amounts of bases and especially that of bicarbonate were lowered in order to bpH closer to normalosis. In theory, metabolic alkalosis and acidosis are also compenby respiratory changes. However, this was not visible in our results, probably becauthe mildness of the metabolic acid-base disturbances or of the relatively small amouthe rats in each group.
6.3. Dentine formation
The high-sucrose diet reduced the rate of dentine formation significantly in youngwhich has also been found previously (Larmas & Tjäderhane 1992, Hietala & Lar1994, Autioet al. 1997, etc.). A reduced bone growth with a high-sucrose diet has breported in adult hamsters (Safferet al. 1981) and rats (Hietala 1993). This lends addtional support to the idea of the similarities between the odontoblasts and the osteobl
Microbial invasion in dentine may occur even in incipient caries and possibly molate the dentine development. Early invasion of oral microbes into white spot of humenamel (Brännströmet al. 1980, Seppä 1984, Seppäet al.1985) and invasion of twostrains of Streptococcus mutans into enamel of rat and further into dentine, whileenamel surface apparently had not yet collapsed (Luoma A-R.et al. 1984, Luoma H.etal. 1987, Seppäet al. 1989) suggest their early involvement in dentinal caries proceThis may be one of the reasons for the reduced dentine formation especially in the gwith the high-sucrose diet.
One of the hypotheses tested in this work was that sucrose affects odontoblasts apartly via metabolic acidosis. Since the high-sucrose diet as such did not shift thebase status towards the more acidic end of the scale (as it seemed to do in one of thstudies), the mechanism by which the sucrose effect on dentine is mediated is appanot via the acidotic state. Other evidence against this hypothesis is visible in the grwith metabolic alkalosis: Although the alkalotic drinking water changed the pH statuthe blood, it did not correct the reducing effect of the high-sucrose diet on the denapposition.
No differences in dentine growth were found between the male and femalealthough their body weights differed significantly. Thus, (primary) dentine formation wnot connected to body growth and weight gain, confirming previous findings in you

58
n in
ungfind-lism,
imin-
ain-lso
thersteeth
canhtly
tineperi-der-tinu-n istion
pro-
or-wereeta-is in
om-ignifi-.04,
hit-cido-
alsntine.in theden-
rats (Kortelainen & Larmas 1990, Tjäderhaneet al. 1995, Bäckman & Larmas 1997).Therefore, it is unlikely that the lower weight gain per se affected the dentine formatiothe groups with metabolic acidosis, as the animals otherwise appeared healthy.
The main new finding here was the strong reduction in the dentine formation in yorats associated with chronic metabolic acidosis. Both the pilot groups supported thising. Acidotic animals and humans have disturbances in calcium and protein metabocausing retarded growth and even protein catabolism (Mayet al. 1986). In our study,chronic metabolic acidosis was indeed accompanied by reduced body weight and dished dentine apposition.
Mild chronic metabolic acidosis is common among people with modern diet conting plenty of animal protein and cola drinks (Barzel 1995). The diet of young people acontains a lot of sugar. If acidosis and high amounts of sugar potentiate each oeffects in young humans, like they seem to do in young rats, the development of theof numerous children may be affected.
When the primary dentinogenesis is still going on in the weanling rats (Bakeret al.1980) and the teeth are producing dentine at maximum efficiency, any disturbanceprobably cause a reduction in the dentine formation. This would explain the sligslower dentine apposition in metabolic and respiratory alkalosis.
6.4. Mineral analysis
The amount of mineral elements (except fluoride) seemed to be lower in the denformed during the experiment than in the dentine formed before the onset of the exmental period (Table 7). The same pattern of mineralization has been found by Tjähane (1996) and by Huumonen & Larmas (in press). This is presumably due to a conous mineralization inside the dentine, not only at the border of the pulp. Mineralizatioprobably in a more advanced state in the dentine formed earlier. This kind of maturaprocess may be typical for young teeth, in which the primary dentinogenesis is stillceeding.
The mineralization in the group with metabolic alkalosis followed closely to this "nmal" trend. Differences between dentine formed before and during the experimentnot as apparent in respiratory alkalosis and the "normal" trend disappared totally in mbolic acidosis. The weight percentage of calcium was even higher in metabolic acidosthe dentine formed during the experiment.
When the percentages of calcium in dentine formed during the experiment were cpared between the groups, the result remained the same: calcium content was scantly higher in the group with metabolic acidosis compared to the control group (p=0Mann-Whitney U -test) and to the group with metabolic alkalosis (p=0.01, Mann-Wney U -test). Surprisingly, the bone has been reported to lose calcium in metabolic asis (Green & Kleeman 1991, Bushinsky 1995).
One explanation for increased amounts of calcium in the dentine of acidotic animmay be the absence of resorption by the osteoclasts or corresponding cells in the deMetabolic acidosis probably decreases the collagen synthesis by the odontoblastssame way it decreases it in the osteoblasts. This would result in slower apposition of

59
nor-cent-the
ense
ultedring
k-oldf theork-
et on
alsodur-waskins,y ofnot
es innor-withriesain-and
sec-t theatelyer
in alln thatfter
elaquecepti-
tine. But, as resorption does not occur in the dentine, the mineralization proceedsmally. Two possible explanation are suggested to explain the higher than normal perage of calcium: the increased amount of calcium available in the blood due toincreased bone resorption, or more thorough mineralization of the dentine (more dstructure) due to the slower rate of formation.
Tjäderhane (1996) found that the sucrose diet (modified Stephan-Harris diet) resin half the amounts of the total mineral contents in the dentine formed before and duthe experiment, compared to the controls. (The experiment was started with 3-weerats and lasted for five weeks.) Thus, compared to metabolic acidosis, the effect ohigh-sucrose diet was completely different. This gives more evidence (against our wing hypothesis) that the reducing effect of metabolic acidosis and a high-sucrose dithe growth of dentine are mediated through different mechanisms.
In the study of Tjäderhane (1996) the amounts of calcium and phosphorus werelower, but the Ca/P ratio remained unaffected in the dentine formed both before anding the experiment in the high-sucrose and the control groups. In our study, the ratio1.8 in all the groups, which has been reported as a normal ratio in the dentine (Jen1978). The acid-base status did not affect this ratio in our study in rats nor in the studDriessenset al. (1987) in dogs. This may suggest that the mineralization processes areeasily disturbed in the dentine.
6.5. Caries
In the groups with the sucrose diet, there was the smallest quantity of dentinal carimetabolic alkalosis. There was also markedly less caries in the control group withmalosis and high-sucrose diet than in metabolic acidosis and respiratory alkalosisthe same diet. The group with respiratory alkalosis was slightly more affected by cathan the group with metabolic acidosis. These results were confirmed with Schiff sting. (The pilot studies supported the findings in the groups with metabolic acidosisalkalosis.)
The occurrence and severity of dentinal caries were quite similar in the first andond molars, but different in the third ones. The first and second molars erupt almost asame time, the first one 1-2 days before the second. Their eruption time is approximthe 16-18th day after birth (3-5 days before the beginning of the experiments) (Baketal. 1980).
The caries lesions were most advanced and most numerous in the third molarsthe groups, even though the eruption of the 3rd molar occurs about 16 days later thaof the 1st and 2nd molars. The eruption time of the third molar is the 32-34th day abirth (11-13th day of the experiments) (Bakeret al.1980). The developmental stage of ththird molars and, perhaps, the elevated amount of cariogenic micro-organisms in pat the time of eruption due to prolonged sucrose ingestion may make them more susble to caries.

60
alsoolar.
in the
ink-d via
d tormen-
ratslso
t onlosisrsa),ira-also
losis.the
rents to be
e car-insmallnto-ary
ido-ts onffectdedent of
th offorstatuss hass:tionsters'
Maturation of the enamel is incomplete at the time of eruption in all teeth, and thisincreases the amount of caries in the molars in young rats, especially in the 3rd mFurthermore, the progression of dentinal caries has been found to be much slowerteeth of adult rats than those of young ones (Kortelainen & Larmas 1994).
Metabolic alkalosis or acidosis were induced by using the alkalized or acidified dring water. Thus, some of the effects of those waters on caries were probably mediatethe pH of the oral fluid locally. Bicarbonate-phosphate combinations (pH 7.4) addesucrose has been demonstrated to reinforce oral natural buffers and lessen plaque fetative pH fall in vitro (Luoma & Luoma 1967, 1968, Luomaet al. 1970) andin vivo(Luoma & Luoma 1968). With this method, caries prevention was observed in(Luoma et al. 1968). Although blood was not studied, the additive effect probably areinforced the blood buffering.
In our study, respiratory alkalosis surprisingly had the strongest activating effeccaries, in spite of the fact that no local effect on mouth was present. Respiratory alkais compensated in mammalian body by creating mild metabolic acidosis (and vice vealthough pH is never fully corrected (Brewer 1990). Metabolic compensation for resptory alkalosis might be strong enough to enhance caries, but more likely there areother, yet unknown effects, which accelerate caries progression in respiratory alkaThe changes in the dentinal growth and mineral contents were different betweengroups with respiratory alkalosis and metabolic acidosis, which suggests that diffemechanisms were involved in these states. These aspects need more experimentsolved.
Previous research has demonstrated that chronic metabolic alkalosis increases thies resistance of children's teeth (Myllärniemi & Holmberg 1975), a finding which gasupport from the present experiment with young rats' molar teeth. In spite of the sreduction in the dentine formation in the groups with metabolic alkalosis, the odoblasts may build dentine of better quality, which, together with a possible rise in salivpH, might increase the caries resistance.
Our results pointed to the harmful effect of the opposite state, chronic metabolic acsis, on teeth. The results give reason to believe that, (in addition to the probable effecsaliva, which were not studied here), metabolic acidosis has a systemic impairing eon the ability of pulp/dentine complex to resist caries attack, probably via the retargrowth, the altered structure and/or some other changes in the growth and developmdentine.
These factors are worth remembering in the treatment and prophylaxis of the teechronically ill patients, especially of such children. Also, if no other reason is foundan exceptionally bad caries status, it seems to be worth while to check the acid-baseof the patient. This may sometimes help in finding an undiagnosed general disease, ahappened in our clinic (Bäckmanet al.1990). Furthermore, an interesting question arisewhat are the effects of acidosis inducing high-protein diet and cola-drinks, in connecwith candies and other sweet food, on the development and caries status of the yougteeth?

7. Conclusions
In the blood gas analysis, the experimental methods were proved adequate: moderatechronic metabolic acidosis and mild metabolic alkalosis and respiratory alkalosis wereconfirmed.
As expected, chronic metabolic acidosis resulted in reduced weight gain. Also, thedentine formation in the molar teeth was slowed down significantly. The primary dentino-genesis is probably easily disturbed: a slight reduction in the growth of dentine was seenin most of the experimental groups.
The high-sucrose diet also markedly reduced the growth of dentine, but apparently bya different mechanism than metabolic acidosis. Firstly, the high-sucrose diet did notinduce acidosis in the blood gas analysis. Secondly, alkalosis did not eliminate the reduc-ing effect of the high-sucrose diet on dentine formation. Thirdly, the effects of metabolicacidosis on the mineralization of the dentine in molars were completely different from thepreviously reported effects of the high-sucrose diet.
Chronic metabolic acidosis increased the weight percentage of calcium and total min-eral content in the dentine formed during the experiment. This is different from the resultsreported in bone and probably due to the lack of resorption and remodelling in dentine.
Metabolic acidosis and respiratory alkalosis promoted the initiation and progression ofthe dentinal caries. This was only seen in the rats with the high-sucrose diet. The thirdmolars were most affected, which implies higher caries susceptibility of erupting teethwith ongoing maturation process, when compared to the erupted ones with moreadvanced stage of dentinal development, as found earlier. Metabolic alkalosis slightlyprotected the teeth from caries.
Metabolic acidosis and the high-sucrose diet potentiated each others effects in promot-ing caries and reducing the growth of dentine in the teeth of young animals. Respiratoryalkalosis seemed to be harmful mostly concerning caries and metabolic alkalosis provedto be even slightly beneficial to the teeth.
Answers to the tested hypotheses are:1. Sucrose affects odontoblasts causing reduction in dentine formation and acceleration
in caries progression via processes other than metabolic acidosis.2. Metabolic alkalosis did not eliminate the effects of sucrose on dentine formation,
which supports the finding mentioned above.

uri-
ing
en-
d
m J
nd
n in
cy-51-54.. In:lish-
ons.
e im-
3.ircu-rat. J
ome
y
-base
8. References
Adler S, Lindeman RD, Yiengst MJ & Beard ES (1968) The effect of acute acid loading on thenary excretion of acid by the aging human kidney. J Lab Clin Med 72: 278-282.
Angmar-Månsson B & Whitford GM (1986) Effects of acid-base status and fluoride on developcanine enamel (abstract). Caries Res 20: 159.
Angmar-Månsson B & Whitford GM (1990) Environmental and physiological factors affecting dtal fluorosis. J Dent Res 69 (special issue): 706-713.
Angmar-Månsson B, Whitford GM, Allison NB, Devine JA & Mahler JT (1984) Effects of simulatealtitude on fluoride retention and enamel quality (abstract). Caries Res 18: 165.
Atkins JL & Burg MB (1985) Bicarbonate transport by isolated perfused rat collecting ducts. APhysiol 249F: 485-489.
Autio J, Hietala E-L & Larmas M (1997) The effect of two sucrose diets on formation of dentin apredentin in growing rats. Acta Odontol Scand 55: 292-295.
Bäckman T & Larmas M (1997) Chronic metabolic alkalosis, sucrose diet and dentine formatioyoung rats. Archs Oral Biol 42: 299-304.
Bäckman TK, Larmas MA, Käär M-L & Paavilainen T (1990) Caries incidence in children with aanotic congenital heart diseases before and after the heart operation. J Clin Pediatr Dent 15:
Bäckman T, Pajari U & Larmas M (1996) Effect of metabolic acidosis on dentinogenesis in ratShimano M, Maeda T, Suda H & Takahashi K (eds) Dentin/Pulp Complex. Quintessence Pubing Co, Ltd, Tokyo, p 291-292.
Baker HJ, Lindsey JR & Weisbroth SH (1980) The laboratory rat. Volume II: Research applicatiAcademic Press, London, p 59-74.
Barzel US (1995) The skeleton as an ion exchange system: Implications for the role of acid-basbalance in the genesis of osteoporosis. J Bone Miner Res 10: 1431-1436.
Beetham R (1982) A review of blood pH and blood-gas analysis. Ann Clin Biochem 19: 198-21Bichara M, Mercier O, Borensztein P & Paillard M (1990) Acute metabolic acidosis enhances c
lating parathyroid hormone, which contributes to the renal response against acidosis in theClin Invest 86: 430-443.
Brännström M, Gola G, Nordenvall KJ & Torstenson B (1980) Invasion of microorganisms and sstructural changes in incipient enamel caries. Caries Res 14: 276-284.
Breslau NA, Brinkley L, Hill K & Pak CYC (1988) Relationship of animal protein-rich diet to kidnestone formation and calcium metabolism. J Clin Endocrinol Metab 66: 140-146.
Brewer DE (1990) Disorders of acid-base balance. Pediatr Clin North Am 37: 429-447.Brun-Pascaud M, Gaudebout C, Blayo MC & Pocidalo JJ (1982) Arterial blood gases and acid
status in awake rats. Respir Physiol 48: 45-57.

63
ase
Am
ory
16-
clasts
et-
cal-
ium
use
ed
af-
f-l and
onin
te-
08-
J
4-
ure.
torial
dult
inal
ult
ma-
res-
Burton RF (1992) The roles of intracellular buffers and bone mineral in the regulation of acid-bbalance in mammals. Comp Biochem Physiol 102A: 425-432.
Bushinsky DA (1988) Net proton influx into bone during metabolic, but not respiratory acidosis.J Physiol 254F: 306-310.
Bushinsky DA (1989) Net calcium efflux from live bone during chronic metabolic but not respiratacidosis. Am J Physiol 256F: 836-842.
Bushinsky DA (1995) The contribution of acidosis to renal osteodystrophy. Kidney Int 47: 181832.
Bushinsky DA (1996) Metabolic alkalosis decreases bone calcium efflux by suppressing osteoand stimulating osteoblasts. Am J Physiol 271F: 216-222.
Bushinsky DA, Kittaka MK, Weisinger JR, Langman GB & Favus MJ (1989) Effects of chronic mabolic alkalosis on Ca2+, PTH and 1,25(OH)2D3 in the rat. Am J Physiol 257E: 578-582.
Bushinsky DA, Krieger NS, Geisser DI, Grossman EB & Coe FL (1983) Effects of pH on bonecium and proton fluxesin vitro. Am J Physiol 245F: 204-209.
Bushinsky DA & Lechleider RJ (1987) Mechanism of proton-induced bone calcium release: calccarbonate dissolution. Am J Physiol 253F: 998-1005.
Bushinsky DA & Nilsson EL (1995) Additive effects of acidosis and parathyroid hormone on moosteoblastic and osteoclastic function. Am J Physiol 269C: 1364-1370.
Butler W (1995) Dentin matrix proteins and dentinogenesis. Conn Tiss Res 33: 59-65.Chabala JM, Levi-Setti R & Bushinsky DA (1991) Alteration in surface ion composition of cultur
bone during metabolic, but not respiratory, acidosis. Am J Physiol 261F: 76-84.Cox CF, White KC, Ramus DL, Farmer JB & Milner Snuggs H (1992) Reparative dentin: factors
fecting its deposition. Quintessence Int 23: 257-270.Driessens FCM, Angmar-Månsson B, Heijligers HJM, Whitford GM & Verbeeck RMH (1987) E
fects of acid-base status and fluoride on the composition of the mineral in developing enamedentine in the dog. J Biol Buccale 15: 225-228.
Escanero JF, Elosegui LM, Cordova A, Pecondon A, Asin JJ, Beltran J & Otero W (1991) Calcitand metabolic alkalosis. Biomed & Pharmacoter 45: 307-309.
Frick KK, Jiang L & Bushinsky DA (1997) Acute metabolic acidosis inhibits the induction of osoblasticegr-1 and type 1 collagen. Am J Physiol 272C: 1450-1456.
Ganong WF (1981) Review of medical physiology. LANGE Medical Publications, Los Altos, p 3583.
Galla JH, Gifford JD, Luke RG & Rome L (1991) Adaptations to chloride-depletion alkalosis. AmPhysiol 261R: 771-781.
Glantz SA (1989) Primer of biostatistics, 2nd ed. McGraw-Hill Book Company, New York, p 29310.
Goldhaber P & Rabadjija L (1987) H+ stimulation of cell mediated bone resorption in tissue cultAm J Physiol 253E: 90-98.
Green J & Kleeman CR (1991) Role of bone in regulation of systemic acid-base balance. Edireview. Kidney Int 39: 9-26.
Hietala E-L (1993) The effect of ovariectomy on periosteal bone apposition and resorption in aanimals. Bone and Mineral 20: 57-66.
Hietala E-L, Autio J & Larmas M (1997) The effect of early weaning on dentin formation and dentcaries in rats. Acta Odontol Scand 55: 201-205.
Hietala E-L & Larmas M (1992) The effect of ovariectomy on dentin formation and caries in adrats. Acta Odontol Scand 50: 337-343.
Hietala E-L & Larmas M (1994) The effect of ovariectomy and high-sucrose diet on dentine fortion and caries in growing rats. Archs Oral Biol 39: 973-978.
Hietala E-L, Tjäderhane L & Larmas M (1993) Dentin caries recording with Schiff's reagent, fluocence, and back-scattered electron image. J Dent Res 72: 1588-1592.

64
ghLon-
in-
eases2230.cor--286.byd 56:
14:
the
Oral
istar
ing
a-
ea-: 489-
and
pro-
us-94-
teo-
den-
ula-
ng-
e to09:
rthersis. J
Hurtado A (1971) The influence of high altitude on physiology. In: Porter R & Knight J (eds) Hialtitude physiology: cardiac and respiratory aspects. Churchill Livingstone, Edinburgh anddon, p 3-8.
Huumonen S & Larmas M (in press) An electron probe x-ray microanalytical study on dentine merals in sucrose fed or clucocorticoid medicated rats. Calcif Tissue Int.
Huumonen S, Tjäderhane L & Larmas M (1997) Greater concentration of dietary sucrose decrdentin formation and increases the area of dentinal caries in growing rats. J Nutr 127: 2226-
Huumonen S, Pajari U, Bäckman T, Tjäderhane L & Larmas M (1996) Effect of low-dose glucoticoid treatment on dentin formation and dentinal caries in rats. Acta Odontol Scand 54: 282
Jaffe HL, Bodansky A & Chandler JP (1932) Ammonium chloride decalcification, as modifiedcalcium intake: The relation between generalized osteoporosis and ostitis fibrosa. J Exp Me823-834.
Jalanko H & Holmberg C (1998) Munuaisten toiminta II: Tubulus ja kokoojaputki. Duodecim 1153-161.
Jenkins GN (1978) Chemical composition of teeth. In: The physiology and biochemistry ofmouth. Blackwell Scientific Publications, Oxford, p. 54-112.
Johannessen LB (1961) Dentine apposition in the mandibular first molars of albino rats. ArchBiol 5: 81-91.
Kaczmarczyk G & Reinhardt HW (1975) Arterial blood gas tension and acid-base status of Wrats during thiopental and halotane anesthesia. Lab Anim Sci 25: 184-190.
Keyes PH (1958) Dental caries in the molar teeth of rats. J Dent Res 37: 1088-1099.Knepper MA, Good DW & Burg MB (1985) Ammonia and bicarbonate transport by rat collect
ducts perfusedin vitro. Am J Physiol 249F: 870-877.König KG, Marthaler TM & Mühlemann HR (1958) Methodik der Kurzfristig Erzeugten Rattenk
ries. Dt Zahn-, Mund- u Kieferheilk 29: 99-127.Koppang HS, Stene T, Solheim T, Larheim TA, Wisnes A, Monn E & Stokke O (1984) Dental f
tures in congenital persistent renal tubular acidosis of proximal type. Scand J Dent Res 92495.
Kortelainen S & Larmas M (1990) Effects of low and high fluoride levels on rat dentinal cariessimultaneous dentine apposition. Archs Oral Biol 35: 229-234.
Kortelainen S & Larmas M (1994) Effect of fluoride on the rate of dentin apposition and cariesgression in young and old Wistar rats. Scand J Dent Res 102: 30-33.
Krapf R, Beeler I, Hertner D & Hulter HN (1991) Chronic respiratory alkalosis. The effect of stained hyperventilation on renal regulation of acid-base equilibrium. N Engl J Med 324: 131401.
Krieger NS, Sessler NE & Bushinsky DA (1992) Acidosis inhibits osteoblastic and stimulates osclastic activity in vitro. Am J Physiol 262F: 442-448.
Larmas M & Kortelainen S (1989) Quantification of the areas of dentinal lesions and secondarytin on fissures of rat molars. Caries Res 23: 32-35.
Larmas M, Kortelainen S, Bäckman T, Hietala E-L & Pajari U (1992) Odontoblast-mediated regtion of the progression of dentinal caries. Proc Finn Dent Soc 88 (Suppl. I): 313-320.
Larmas M & Tjäderhane L (1992) The effect of phenytoin medication on dentin apposition, root leht and caries progression in rat molars. Acta Odont Scan 50: 345-350.
Lau K, Rodriguez-Nichols F & Tannen RL (1987) Renal excretion of divalent ions in responschronic acidosis: evidence that systemic pH is not the controlling variable. J Lab Clin Med 127-33.
Lemann Jr J, Lennon EJ & Letzow JR (1966) The effects of chronic acid loads in normal man; fuevidence for the participation of bone mineral in the defense against chronic metabolic acidoClin Invest 45: 1608-1614.

65
stion578-
pen-
bo-
d
lism.
ec
rates 92:
bo-al cal-
ate-
ad-
intake
ns of
b-
us-
ge-
iar-
n an-ce,
e:: 371-
Lemann J, Lennon EJ, Piering WR, Prien EL & Ricanati ES (1970) Evidence that glucose ingeinhibits net renal tubular reabsorption of calcium and magnesium in man. J Lab Clin Med 75:585.
Lennon EJ & Piering WF (1970) A comparison of the effects of glucose ingestion and NH4Cl acidosison urinary calcium and magnesium excretion in man. J Clin Invest 49: 1458-1465.
Leonora J, Tieche JM & Steinman RR (1992) The effect of dietary factors on intradentinal dyeetration in the rat. Arch Oral Biol 37: 733-741.
Licata AA, Bou E, Bartter FC & West F (1981) Acute effects of dietary protein on calcium metalism in patients with osteoporosis. J Gerontol 36: 14-19.
Lien Y-H, Stern R, Fu JCC & Siegel RC (1984) Inhibition of collagen fibril formation in vitro ansubsequent cross-linking by glucose. Science 255: 1489-1491.
Lien Y-H, Tseng MM & Stern M (1992) Glucose and glucose analogs modulate collagen metaboExp Mol Pathol 57: 215-221.
Linde A (1989) Dentin matrix proteins: composition and possible functions in calcification. Anat R24: 154-166.
Linde A & Goldberg M (1993) Dentinogenesis. Crit Rev Oral Biol Med 4: 679-728.Luoma A-R, Luoma H & Pelttari A (1984) Microbial invasion and subsurface colonization of
enamel in early fissure caries observed by scanning electron microscopy. Scand J Dent R120-126.
Luoma H, Antoniades K, Turtola LO & Kuokka MA (1970) The effects of phosphate and bicarnate-phosphate additions to dietary sugar on caries and on the formation of renal and dentculus in rats. Caries Res 4: 332-347.
Luoma H & Luoma A-R (1967) Influences of sucrose and buffer additives on plaque and32P of theenamel. J Dent Res 46: 1392-1399.
Luoma H & Luoma A-R (1968) Modification of the pH of human plaque by sucrose and bicarbonphosphate additives. Caries Res 2: 27-37.
Luoma H, Niska K & Turtola L (1968) Reduction of caries in rats through bicarbonate-phosphateditions to dietary sucrose. Archs oral Biol 13: 1343-1354.
Luoma H, Seppä L, Spets-Happonen S, Tulla M & Pelkonen K (1987) Early penetration ofStrepto-coccus mutansinto fissure enamel of gnotobiotic rats. Oral Microbiol Immunol 2: 30-34.
Lutz J (1984) Calcium balance and acid-base status of women as affected by increased proteinand by sodium bicarbonate ingestion. Am J Clin Nutr 39: 281-288.
Magarian GJ (1982) Hyperventilation syndromes: infrequently recognized common expressioanxiety and stress. Medicine 61: 219-236.
Martin DW, Mayes PA & Rodwell VW (1981) Harper's review of biochemistry. Lange Medical Pulications, Los Altos, p 524.
Massler M (1967) Pulpal reactions to dental caries. International Dental Journal 17: 441-460.May RC, Kelly RA & Mitch WE (1986) Metabolic acidosis stimulates protein degradation in rat m
cle by a glucocorticoid-dependent mechanism. J Clin Invest 77: 614-621.Mitchell JE, Seim HC, Colon E & Pomeroy C (1987) Medical complications and medical mana
ment of bulimia. Ann Intern Med 107: 71-77.Myllärniemi S & Holmberg PC (1975) Caries resistance in children with congenital chloride d
rhoea. Archs Oral Biol 20: 239-240.National Research Council (1972) Nutrient requirements of the laboratory rats. In: Committee o
imal nutrition (ed) Nutrient Requirements of Laboratory Animals. National Academy of ScienWashington DC., p 56-93.
Ohlsson A, Cumming WA, Paul A & Sly WS (1986) Carbonic anhydrase II deficiency syndromrecessive osteopetrosis with renal tubular acidosis and cerebral calcification. Pediatrics 77381.
Parfitt AM (1987) Bone and plasma calcium homeostasis. Bone 8 (supp. 1): S1-S8.

66
uis,
, p
drate
hy-
andJ Med
ion of
en-
on of-
n
nce
ol of
s in-
openia
den-
probei K
tion
y a
ruc-
dno-
is-
ent.
one
Pesce AJ & Kaplan LA (1987) Methods in clinical chemistry. The C. V. Mosby Company, St. Lop 62.
Rhoades RA & Tanner GA (1995) Medical physiology. Little, Brown and Company, New York465-469.
Saffar JL, Sagroun B, de Tessieres C & Makris G (1981) Osteoporotic effect of a high-carbohydiet (Keyes 2000) in golden hamsters. Archs Oral Biol 26: 393-397.
Schuette SA, Zemel MB & Linksweiler HM (1980) Studies on the mechanism of protein-inducedpercalciuria in older men and women. J Nutrition 110: 305-315.
Sebastian A, Harris ST, Ottaway JH, Todd KM & Morris Jr RC (1994) Improved mineral balanceskeletal metabolism in postmenopausal women treated with potassium bicarbonate. N Engl330: 1776-1781.
Seppä L (1984) A scanning electron microscopic study of early subsurface bacterial penetrathuman molar-fissure enamel. Archs Oral Biol 29: 503-506.
Seppä L, Alakuijala P & Karvonen I (1985) A scanning electron microscopic study of bacterial petration of human enamel in incipient caries. Archs Oral Biol 30: 595-598.
Seppä L, Luoma H, Forss H, Spets-Happonen S, Markkanen S & Pelkonen K (1989) InvasiStreptococcus mutansandLactobacillus salivariusin early caries lesions of gnotobiotic rats. Caries Res 23: 371-374.
Silverstone LM & Mjör IA (1988) Dental Caries. In: Hörsted-Bindslev P & Mjör IA (eds) ModerConcepts in Operative Dentistry. Munksgaard, Copenhagen, p 16-58.
Steinman RR & Leonora J (1971) Relationship of fluid transport through the dentin to the incideof dental caries. J Dent Res 50: 1536-1543.
Talmage RV & Grubb SA (1977) A laboratory model demonstrating osteocyteosteoblast contrplasma calcium concentrations. Clin Orthoop 122: 299-306.
Tamura T, Fujii A, Kobayashi S & Kuboyama N (1983) Relationship between prolonged excestake of sucrose and Ca balance (abstract). J Dent Res 62: 653.
de Tessieres C & Saffar JL (1992) Spontaneous recovery from growth disturbances and osteinduced by a high carbohydrate diet in hamsters. J Biol Buccale 20: 117-120.
Tieche JM, Leonora J & Steinman RR (1994) High-sucrose diet inhibits basal secretion of intratinal dye penetration-stimulating parotid hormone in pigs. J Appl Physiol 76: 218-222.
Tjäderhane L (1996) The effect of high sucrose diet on dentin minerals measured by electronmicroanalyzer (EPMA) in growing rat molars. In: Shimano M, Maeda T, Suda H & Takahash(eds) Dentin/Pulp Complex. Quintessence Publishing Co, Ltd, Tokyo, p 293-296.
Tjäderhane L, Bäckman T & Larmas M (1995) Effect of sucrose and xylitol diets on dentin formaand caries in rat molars. Eur J Oral Sci 103: 166-171.
Tjäderhane L, Hietala E-L & Larmas M (1994) Reduction in dentine apposition in rat molars bhigh-sucrose diet. Archs Oral Biol 39: 491-495.
Torneck CD (1994) Dentin-pulp complex. In: Ten Cate AR (ed) Oral Histology. Development, stture and function. Mosby Co, St Louis, p 169-217.
Whitford GM & Angmar-Månsson B (1995) Fluorosis-like effects of acidosis, but not NH4+, on ratincisor enamel. Caries Res 29: 20-25.
Whitford GM & Pashley DH (1979) The effect of body fluid pH on fluoride distribution, toxity anrenal clearance. In: Continuing evaluation of the use of fluorides. Am Assoc Advan Sci Mograph, Selected symposium 11: 187-221.
Whitford GM & Pashley DH (1984) Fluoride absorption: The influence of gastric acidity. Calcif Tsue Int 36: 302-307.
Whitford GM, Pashley DH & Stringer GI (1976) Fluoride renal clearance: A pH-dependent evAm J Physiol 230: 527-532.
Whiting SJ & Draper HH (1981) Effect of a chronic acid load as sulfate or sulfur amino acids on bmetabolism in adult rats. J Nutrit 111: 1721-1726.

67
ular
Winsnes A, Monn E, Stokke O & Feyling T (1979) Congenital persistent proximal type renal tubacidosis in two brothers. Acta Paediatr Scand 68: 861-868.