Embed Size (px)
Citation preview

Achieving New Treatment Goals for LDL-C: Strategies for the Managed
Care Provider
Robert J. Chilton, DO, FACC
Associate Professor Department of Medicine, Division of Cardiology
The University of Texas Health Science Center at San Antonio
San Antonio, TX
Welcome to Achieving New Treatment Goals for LDL Cholesterol: Strategies for the Managed Care Provider. Dr. Robert Chilton is an Associate Professor in the Department of Medicine, Division of Cardiology at the University of Texas Health Science Center at San Antonio.

Accreditation and Educational Support
Educational support for this activity has been provided by Merck/Schering-Plough Pharmaceuticals
This activity is accredited by the Postgraduate Institute for Medicine. Educational support for this activity has been provided by Merck/Schering-Plough Pharmaceuticals.

Post test and Program Instructions
While viewing a presentation, you can control the slides and audio by using the PLAY, PAUSE, NEXT and PREVIOUS controls. You can also jump to a specific slide using the thumbnail images at the bottom of your screen. You can zoom into the slides by clicking the ENLARGE SLIDE button. Then, click the slide again to return it to its normal size.
After viewing the full, synchronized slide and audio presentation, you will have the opportunity to submit a post-test and evaluation form in order to receive CE credit. While viewing the presentation, you can control the slides and audio by using the Play, Pause, Next, and Previous controls. You can also jump to a specific slide using the thumbnail images at the bottom of your screen. You can zoom into the slides by clicking the Enlarge Slide button; then click the slide again to return it to its normal size.

Educational Objectives
Identify the effect of achieving the goals of lipid therapy on patient outcomesDescribe published algorithms and pathways used to improve patient outcomesReview the effect of lipid lowering on C Reactive Protein levelsExplain the role of coadministration therapy versus monotherapyDiscuss pharmacoeconomic aspects of lipid lowering therapies
The educational objectives for this program are: Identify the effect of achieving the goals of lipid therapy on patient outcomes; Describe published algorithms and pathways used to improve patient outcomes; Review the effect of lipid lowering on C Reactive Protein levels; Explain the role of coadministration therapy versus monotherapy; and Discuss pharmacoeconomic aspects of lipid lowering therapies

Welcome
Welcome to today’s conference, the title, Achieving New Treatment Goals for LDL Cholesterol: Strategies for the Managed Care Provider. I’m Dr. Robert Chilton from the University of Texas Health Science Center. Today we are going to discuss looking at commonly used things in the private practice setting for taking care of patients that have high cholesterol.
The overview of this conference today will entail the benefits of achieving LDL cholesterol on patient outcomes so to make sure that they work, algorithms and pathways to improve patient outcomes, looking at the safety and efficacy of current treatments for lipid modification and then coadministration of therapy versus the monotherapy of only one drug and then in closing, looking at the cost/benefit ratio of these different types of treatment.

According to the National Health and Nutrition Examination Survey (NHANES) III, approximately what percentage of the American population requires lipid lowering therapy to achieve ATP II cutpoints?
o A. 26%o B. 9%o C. 42% o D. 18%
According to the National Health and Nutrition Examination Survey (NHANES), approximately what percentage of the American population requires lipid-lowering therapy to achieve ATP-II cut points. The choices are:
A. 26%B. 9%C. 42% D. 18%.

Atherosclerosis Risk in Communities (ARIC) Study
141/146031/98403/1194959/283
110/146024/98189/1194935/283
05
101520253035
CV Deaths 12 1.5 24 7CV Events 20 3 31 9
Prior MIPrior MI
10-year F/UN=13790634 CV Events
Non-Diabetics Diabetics
NOPrior MI
NOPrior MI
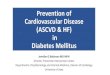
Lee CD, et al. Circulation. 2004;109:855-860.
% o
f Pat
ient
s
This next slide is one that probably each of us should be very proud of because this is a very large trial and in some respects I think this may be similar to the Framingham Heart Study as one that we can follow epidemiologically. This is the Atherosclerosis Risk in a Community study. Each of us in this room paid for this. These are the number of patients and they looked at the number of events and it gives us an idea over ten years what should you expect your chance if you have no risk factors of a cardiovascular death or event. And I’ve plotted it here on the slide so you can see it. If you took 13,000 people and you watched them over again ten years and you had no heart attack before and you’re healthy, you should have an event rate of around 1.5% in ten years. But, if you are a type 2 diabetic or a person that has diabetes and you’ve had no problems before and that’s all you have and you think you’re doing well, you’re event rate in ten years is 7%. That’s a lot higher than 1.5 and that means that you are a high-risk patient and that’s why in the actually NCEP guidelines, we consider a person that has diabetes to actually be equivalent to having heart disease. You can also see the tremendous increase in risk if you are a person that has diabetes and you actually have already had a heart attack, it’s 24% and that’s certainly higher than 1.5 at ten years.

ASA – Statin – ACEI
ASCOT-10 mg qdHPS- 40 mg qdHOPE-10 mg qdEUROPA- 8 mg qd
Fixed Dose
Hypertension115/75
135/80 HOT
HyperlipidemiaLDL 65-75 HPS
DiabetesHbA1c <5.5
FBS <85
Waist SizeMen <40”
Women <35”
Titrate to Desired Effect
10-year Risk of CV Event
20%-NCEP Treatment
1.5%-2%-Clean Living
10%-Lifestyle/Treat ?
Initiate Treatment Based on Baseline Risk for CHD
The next slide looks at initiating treatment based on baseline risk for coronary heart disease. And this is a slide that I’ve made up myself because I like evidence-based medicine. And in this slide, it basically shows you what you should look at as far as treatment risks. For example, the National Cholesterol Education Program considers at ten years a person who is greater than 20% risk of having a cardiovascular event should be treated obviously and if you are going to do that, then you need to look at drugs that are actually proven to decrease cardiovascular risk. For example, I think most folks, including my mom, would say that aspirin is a heart drug that is good. They would say that statins have been proven through a number of large trials to show benefit and certainly ACE inhibitors. And basically this slide shows you the targets that I myself have perceived by research looking at different independent studies that probably are ranges that we will be in the 21st century. And I think you can see from the numbers that they are much lower than many of the guidelines. This does not mean that these are the guidelines. These are my own personal opinions but I think this is the area that we are aiming and targeting and hopefully most of you are already in those areas without taking drugs but for those that are taking drugs, this is the areas that I think that you probably need to fit in.

Additive Effect of Cholesterol and Systolic BP on Risk of CHD Death
Neaton JD, et al. Arch Intern Med. 1992;152:56-64.
142+
125-131
<182182-202
203-220221-244
Cholesterol Quintile(mg/dL)
Systolic BP Quintile (mm Hg)<118
118-124
132-141
34
21
13
6
23
12
810
6
18
11
96
4
17
88
6
3
Deaths per 10,000 Patient-years
245+
14
56
3
12
17
n = 316,099
On this slide, it shows the additive effect of cholesterol and systolic blood pressure as a combined effect for risk for heart disease. For example, if you see in this slide nearly 300,000 patients were looked at and as the cholesterol goes up so does the deaths per 10,000 patient years. You will also notice that on the right-hand side that as the systolic blood pressure goes up so does the incidence of deaths. But if you combine them, they are synergistic and they are actually even worse. So the bottom line is global risk reduction and treatment of all the risk factors are more important than just treating one.

O’Keefe JH, et al. J Am Coll Cardiol. 2004;43:2142-2146.
TC <193(N=224)
TC >193(N=803)
n = 3277Healthy Adults
Lower Total Cholesterol Enhances Survival
In this slide, lower total cholesterol levels certainly show an enhanced survival. For example if 40 years ago, someone drew your cholesterol and you had a cholesterol that was less than 193, looking at this slide in healthy adults 40 years ago, you would find that you lived longer than the person who actually had a cholesterol greater than 193. And for most people in the audience, I would suspect you’re having a little chest pain because actually at 40 years ago if you think back, if you had your cholesterol done and it was greater than 193, which most of us would have thought was good, you thought you were okay but you’re really not. So total cholesterol does mean survival.

Anglo-Scandinavian Cardiac Outcomes Trial (ASCOT)
HTN Primary Prevention Trial5-year follow-upTC <250 mg/dL + 3 other risk factorsMostly men 40-79 yrsCCB + ACE vs. BB + Diuretic
Lipid lowering arm (n = 10,305)Atorvastatin 10 mg (no titration)
LDL-C 50 mg/dL in 1 yearPlacebo
LDL-C 42 mg/dL in 1 yearLipid arm of study stopped after 3.3 years
Survival benefits seen at 1 year
Diabetics: no benefits noted
Only 84 events noted Placebo
14% statin non-diabetic8% statins diabetic
No benefits noted in women
Only 36 events observed
Sever PS, et al. Lancet. 2003;361:1149-1158.Sever PS, et al. J Hyper. 2001;19:1139-1148.
This slide takes a look at the ASCOT trial, and in this trial, this is an important trial because it is a primary prevention trial done in hypertensive patients. These patients were followed up for five years but unfortunately due to the fact that it was so positive, this trial has actually been stopped early.

LDL-
C (m
mol
/L)
*33% reduction from baseline
*
0
1
2
3
4
AtorvastatinPlacebo
132 mg/dL 126 mg/dL
89 mg/dL
Moderate Risk
Lower LDL-C
↓ CV Events
3% Placebo
1.9% Treatment
Trial stopped at 3.3 years
ASCOT: Benefits of Reaching LDL-C Goal
ASCOT: Benefits of Reaching LDL-C Goal
BaselineBaseline 6 6 monthsmonths
I YrI Yr 2 Yr2 Yr 3 Yr3 Yr EndEnd
Sever PS, et al. Lancet. 2003;361:1149-1158.
n = 4669n = 4669n = 4627n = 4627
n = 4256n = 4256n = 4170 n = 4170
The benefits of the ASCOT trial can be seen in this slide. If you came into the ASCOT trial and you had high blood pressure but we measured your cholesterol and we looked at two groups and we treated you with 10 mg of atorvastatin, fixed dose not titrated, and we went from 126 LDL cholesterol down to 89, we took you from moderate risk to a lower LDL level, which would lower your risk. That meant that in this trial that was stopped at 3.3 years, the placebo group had 3% incidence of events and the treatment groups got 10 mg of atorvastatin, which is very low dosed, actually only had 1.9% events. It tells us that even a small drop in the cholesterol as you saw in this study actually significantly showed a change in the cardiovascular event rate.

ASCOT: Clinical Event RatesASCOT: Clinical Event Rates
0
5
10
10 mg Atorvastatin
10 mg Atorva 1.9 7.5 3.4 3.6 1.4 1.7 0.8Placebo 3 9.5 4.8 4.1 1.6 2.4 0.7
MI/Fatal CHD
Total CV
Event/
Total Cor
Events
All Cause
CV Mortal
Stroke F/N MI F/N
Placebo
% Absolute Event Rates
NNT (3.3 years) 90 50 71 -- -- 142 --
Perc
ent
Primary & Secondary Endpoints
Sever PS, et al. Lancet. 2003;361:1149-1158.Sever PS, et al. J Hyper. 2001;19:1139-1148. Secondary endpoints
This slide is mainly for those who are more interested in details of this specific trial, and it just simply breaks out the primary and secondary end points of the ASCOT trial. The clinical event rates are listed below and it shows you the group that received atorvastatin 10 and also the placebo group, and you can see for the primary end point of MI – again fatal coronary heart disease at 1.9% and the placebo group actually had a 3% and then you can see it broken down into the secondary end points.

CV Event Rates in Clinical AtherosclerosisCV Event Rates in Clinical Atherosclerosis
3%ASCOT
5.5%TexCAPS
7.5%WOSCOPS
PlaceboTrial
3.3-5 years
NCEP III Goal - 20% Risk CV Event 10 yearsNew Zealand - 10% Risk CV Event 5 years
National Guidelines
10%Most Trials 5 years
Normal?1%
3%
5%
7%
9%
Ok to Treat
901.9%503.5%455.3%
NNTDrug
Event Rate
Event Rate
This next slide is a very interesting slide and basically takes a look at the primary prevention trials, which there was WOSCOPS initially and then in Texas we did TEXCAPS from San Antonio and Dallas and then the ASCOT trial, which was just recently discussed.
I think the point of this slide that makes it kind of interesting is that you take a look at the placebo event rate in each of these trials and notice that the WOSCOPS, which was done with Pravastatin, is 7.5% over about a five-year period - that’s if you did not get a statin in this trial.
The TEXCAPS study was done in San Antonio here and actually this is a population of people like most of us in the audience. They had relatively reasonable total cholesterols but their HDL’s were on the low side. And that placebo event rate was 5.5% in the placebo group at about five years. Now the ASCOT trial was a lower risk population even yet it’s only 3%. If you were in the placebo group, that was your event rate in roughly three to five years. Well, now if you took one of the statin drugs again you could see the benefit. We went from 7.5 with Pravastatin 40 all the way down to 5.3. You can see in the TEXCAPS with lovastatin we went from 5.5 to 3.5 again this is significant and in the ASCOT, we even got down to 1.9%. Well, 1.9% risk is pretty low and the other thing is too is that that tells us that probably the NCEP guidelines need to even be tighter than they are. I am personally not interested, and this is a primary prevention trial, and infracting first or having a stroke first, I would rather be treated a little earlier instead of waiting for these numbers to get lower. So I think this is an eye opener. I think you need to look at this but be sure that you look at it very carefully. Notice the placebo event rates. They are not the same in each of these three trials, which meant the highest risk group was the WOSCOPS. The lowest risk group is ASCOT.
In order to obtain statistical significance, it’s easier in a higher-risk population; it’s tougher in a very low-risk population. So it’s telling us that even in a low-risk population like in ASCOT, it’s telling us that statin drugs are very worthwhile in cardiovascular events.

4S Trial: Mean LDL-C Achieved4S Trial: Mean LDL-C Achieved
Pedersen TR, et al. Circulation. 1998;97:1453–1460.
0
100
150
200
250
mg/dL
1 2 3 4 50
3
4
5
6
Years
Mea
n LD
L-C
(mm
ol/L
)
2∆ -34% overmedian 5.4-yearfollow-up period
Placebo
Simvastatin
0
Benefits of Reaching GoalBenefits of Reaching Goal
High Risk
Lower LDL
N=4444
New NCEP LDL Goal- High Risk - 70 mg/dL- ATP III - <100 mg/dL
↓ CV Events
28% Placebo
19% Statin
The next slide takes a look at the 4S trial and it takes a look at the mean LDL cholesterol. The reason I picked the mean is because most of us know that that’s what most of us use to look at taking care of patients. We don’t use total. We look at the LDL cholesterol. The 4S trial is a very high-risk secondary prevention group. It’s famous. As a matter of fact I personally think if this trial had been negative, we would not use statin drugs today. This was a very high-risk group and we lowered their LDL cholesterol, you can see just down close to 100 but in current times that’s not good enough. It’s still above 100 LDL as a secondary prevention. But at that time, the placebo event rate was 28% at five years and if you will think back to the previous slide, we were talking in the 3 to 7% range – this is 28%. So this is nearly five times and in some respects higher, than what you saw before. Well with the use of simvastatin 40, they were able to drive this down to 19%, and this tells us since the marked reduction in cardiovascular events that statin drugs for secondary prevention is very worthwhile.

10-year Risk of CHD10-year Risk of CHD
NCEP & Framingham Risk of CHD
Per
cent
0
5
10
15
20
25
30
% 10-yr Risk 2 2 2 3 4 5 6 8 10 12 16 20 25 30
4 5 6 7 8 9 10 11 12 13 14 15 16 17
High Risk
1010--year Riskyear Risk
Points
4S Trial: Secondary Prevention
19.4%19.4%
55--year Riskyear Risk
28%28%
StatinBaselineRisk
Area For N
ew Treatm
ents
Pedersen TR, et al. Circulation. 1998;97:1453–1460.
The next slide is probably the more bothersome problem, and I think it has been brought up more in the last year or so that most of us really didn’t look at although it’s been talked about a lot. If you look at this slide, it shows on Framingham curve all the way up to the very high-risk group around 30% and you can see we treat at 10-year risk at the NCEP at 10 at about a 20% risk patient, this shows you the benefit of statins in the 4S trial. It went from 28% placebo event rate down to 19.4. Now if you take a look, that’s a very nice drop. I have a patient that got down to 19.4% at again five years but what about from 19 down to that 2% - that’s what I want to be at. I don’t want you to leave me at 19.4. That means that in the next five years that would be the event rate. Now you can’t exactly multiply that times two and make it ten year but I think what it tells us is that we know about one-third and these drugs do good for about one-third of the cardiovascular disease events. What I don’t know, and I think we need new drugs for, is the other 60 to 70% that’s not treated. That’s what’s missing in this equation. We certainly have focused on the fact that we have a statistical significant benefit of this class of drugs but I think even bigger than that, don’t forget that we only know probably bout 30% of the cause of cardiovascular disease in cardiovascular events. The other 70% is still not known.

Major Coronary Events Reduced in Proportion to LDL-C Achieved
Major Coronary Events Reduced in Proportion to LDL-C Achieved
Circulation. 1997;96:I-717 Abstract.
18.9
13.3
10.8
0
4
8
12
16
20
24
44-70%(58-104)
34-44%(105-126)
< 34%(127-266)
% LDL-C Reduction After 1 Year of Treatment
% M
ajor
Cor
onar
y Ev
ent R
ate
% LDL-C ReductionPost-treatment LDL-C (mg/dL)
4S
The next slide takes a look at the 4S as far as potential – how low do you take your cholesterol? A secondary prevention trial. Is lower particularly better? Is a lower cholesterol better than one that say gets under the M-100 or 99 as we say for the secondary prevention LDL number by NCEP. And this actual abstract that was published in Circulation kind of addresses that issue. It takes a look at people for major coronary event rate or cardiovascular events and the people who actually had the lower cholesterol in the 4S trial. And if you look, certainly you get a nice reduction in your cholesterol with the use, and you get between 127 post-LDL to 266 but notice that as you get down to 58 LDL, look at the marked reduction in events that occurred. So there is some data to support lower is better as many people have talked about for years.

Eligible patients presented with increased risk of CHD death due to prior disease
MI or other CHDOcclusive disease of non-coronary arteriesDiabetes mellitus or treated hypertension
Age: 40-80 yearsTotal cholesterol >3.5 mmol/L (>135mg/dL)n = 20,536Follow up: 5 yearsIntervention: simvastatin 40 mg QD
Heart Protection Study (HPS)Heart Protection Study (HPS)
Heart Protection Study Collaborative Group. Lancet. 2002;360:7-22.
This slide now moves on to a more new piece of data from the Heart Protection Study. This is currently the largest study for secondary prevention that we have. This to me was a spectacular study. This was done with simvastatin 40 in its fixed dose. Now if you think about it for a minute, I didn’t say titrated. They actually gave 40 mg of a drug called simvastatin and we looked at events. Most of you don’t measure things for aspirin; they really don’t do anything other than just give 40 mg of simvastatin. Now that doesn’t mean that we recommend that you only give the drug but if you are a hard purest, this is a study that was done with fixed dose. This is a study done in people who have again already had high risk of having heart problems. They’ve been diagnosed as having heart disease or equivalent to that with diabetes or treated hypertension, and again, you can see the age is between 40 and 80. That doesn’t address the people between 30 and 40, which we will get to that probably is an area that we really should consider targeting earlier than we do now. 20,000 patients. Kind of hard to beat that for a number. These are folks that were very nicely designed randomized trial and again followed for five years.

HPS: Benefits of Achieving LDL-C Treatment Goal
HPS: Benefits of Achieving LDL-C Treatment Goal
↓ All Cause MortalityP<0.001
14.7% Placebo
12.9% Statin
↓ CV DeathsP<0.002
6.9% Placebo
5.7% Statin0
20
40
60
80
100
120
140
LDL-C 126 126 89
Control Treatment Treatment
LDL-
C (m
g/dL
)
Heart Protection Study Collaborative Group. Lancet. 2002;360:7-22.
This slide looks at the benefits of achieving LDL goal in the Heart Protection Study. From this slide, you can see the actual LDL treatment goal for the control – the treatment in the control group – and also in the treatment arm where they started from – both about 126 LDL. And if you think about it, that’s probably what most folks around here have. Now notice that with treatment with simvastatin, you got down to 89 – clearly under the NCEP guidelines of under 100. And then you can see over on the right-hand side the 14% placebo event rate and you can take a look at again the benefit of the statin clear down to 7.7%, which is a highly significant reduction in not only cardiovascular deaths but in all cause mortality. This tells us clearly that statin drugs are absolutely part of the cardiovascular armormarterium, especially in people that are secondary prevention.

116 mg/dL
77 mg/dL
≈25% ReductionVascular Dx Risk
Vascular Events
LDL-
C (m
g/dL
)
0
50
100
Placebo Statin
97
65
N=3500
Entry LDL-C
Special Interest Group-Low Baseline LDLSimilar Reduction in Risk as Higher LDL Group
CHDx, CVA, or Revascularization
Risk Reduction in HPS
Heart Protection Study Collaborative Group. Lancet. 2002;360:7-22.
This slide is probably most interesting to me. I’m sure many of you in the audience wonder – well, what if these guys decide to take folks who have an LDL cholesterol under 100 that entered the study, you’d think, if it’s under 100, there’s no reason to treat that guy because his cholesterol is clearly on a LDL less than 100 not worth treating – just leave him alone. Well, that’s not what they found. As matter of fact, there are 3,500 patients in this very large study that showed that if you came in and you had a 97 LDL and I lowered you with a statin, simvastatin in this study 40 mg, they got the same benefit as the guys who had a higher LDL cholesterol. So it tells us that there potentially is a thing called a pleiotrophic effect of statins that far exceed the benefits of just the number LDL cholesterol. Certainly the reduction of LDL cholesterol is proven in atherogenic models and in cardiovascular events to be important but there is also tons of scientific data to support the fact that pleotrophic activity of these type of drugs are certainly decreasing cardiovascular events and stabilizing plaque.

Clinical Outcome ResearchDrugs Proven to Reduce CV EventsClinical Outcome Research
Drugs Proven to Reduce CV Events
N=26513 N=20536 N=9297
5 yrs5 yrs
Secondary Prevention Trials
N=9014 N=4159
LIPID CARE
8.36.4
13.210.2
Pravastatin 40 mg
335290261830NNT1.91.1 33.85.53.3ARR
ARR-absolute risk reduction
0
10
20
30
TreatmentPlacebo
Treatment 11.5 19.9 14Placebo 14.8 25.4 17.8
ASA 325qd
Simva 40qd
Ramp 10qd
N=10305
1.93
Atorva 10qd
3.3 yrs
10 Prevention TrialR
isk
Red
uctio
n (%
)
This slide looks at the clinical outcomes research that I put together for some house staff that sometimes it’s hard to read all the papers and kind of get an idea of what’s going on. So the way for the Board Examinations for Internal Medicine, I looked at the actual drugs proven to reduce cardiovascular events. For example, aspirin. That’s a pretty easy one to look at for secondary prevention and you can see the treatment number of 11% and the placebo group had 14%. Clearly a benefit shown here. Then if you actually looked at the absolute risk reduction, which was a 3% difference, that translates into only 30 people having to be treated to decrease one cardiovascular event.
So it’s highly worthwhile to use an aspirin. You can see the next one for the Heart Protection Study, which was a statin that I just discussed. You can also see now the effects of ACE inhibitor from the HOPE trial. Need to only treat 26 people in there for five years to show a benefit from a fixed dose of ramipril, which is an ACE inhibitor. It wasn’t titrated and it wasn’t specifically a high blood pressure study. And then you can see the ASCOT trial, which was the primary prevention study. I already showed you and you only have to treat 90 people again for a short time to show a benefit. Now you can see that you’ve got to treat a lot more people but remember the atorvastatin study, ASCOT, was primary prevention – it wasn’t people who already had cardiovascular disease.

AgeYears Points20-34 -935-39 -440-44 045-49 350-54 655-59 860-64 1065-69 1170-74 1275-79 13
CHD RiskPoints 10-y
Risk (%)<0 <10 11 12 13 14 15 26 27 38 49 5
10 611 812 1013 1214 1615 2016 25≥17 ≥30
Systolic Blood PressureUntreated Treated
<120 0 0120-129 0 1130-139 1 2140-159 1 2≥160 2 3
HDL-C (mg/dL)Points
>60 -150-59 040-49 1<40 2
Score = 2110-y Risk >
30%
LDL-C goal:<100 mg/dL
Total Age (years)Cholesterol(mg/dL) 20-39 40-49 50-59 60-69 70-79 <160 0 0 0 0 0160-199 4 3 2 1 0200-239 7 5 3 1 0240-279 9 6 4 2 1≥280 11 8 5 3 1
Cigarette SmokingNonsmoker 0 0 0 0 0
8 5 1 1
Framingham Risk Calculation
3Smoker
National Cholesterol Education Program Expert Panel. JAMA. 2001;285:2486-2497.
Now the next slide takes a look at the Framingham point score estimates. There are certainly one for women but men are somewhat more fun to look at because they usually are higher risk. They don’t have the advantage of estrogen or at least most men that I know. And if you take a look, you can see the age – it goes from 20 to 79. Now that means that before 20, I guess there’s no risk and after 80, you don’t have to worry either. Probably now some people would consider middle age someplace around 65 or 70 because many people, even the ones that we put stents in in the cardiovascular labs are around 90 and are very active and travel around the world. So you need to look here at this graph and see well – let’s see, age does add risk points and you look across, it looks like to me that age has the most points. So if I had to say your biggest risk factor as you get older is your age.
Now if you also look, you’ll also notice that cholesterol has an age-related number. That means that when you’re young, you get the most points for your cholesterol. But if you take a look at a person who is only middle aged, 60 to 70, notice they get very few points for cholesterol. That doesn’t mean that cholesterol is not important but if you look at the Framingham risk for having a cardiovascular event, when you’re older you are much more likely to have already had your event. And you can see here, in the older folks, they don’t give them as many points for risk. But if you’re young and your cholesterol is high, that’s the guy to go after as far as looking at treatment because you can make a big difference in his risk stratification since he gets so many points when he is young for high cholesterol. You can also take a look and notice that smoking is age related. But as you get to be 70, you only get one point for smoking but when you are young, if you quit smoking, you can certainly reduce even more impressively your risk because you get 8 points for it if you are between 20 and 40.

Risk Factors @ CHD EventsPercent by AgeRisk Factors @ CHD EventsPercent by Age
Age 40
39%
38%
15%0% 8%
20%
20%
13%
40%
7%
Age 50
7% 7%
13%66%7%
Age 60
SmokingTC>200HDL<40AgeSBP>130
Age
Age
Risk factors for coronary heart disease events are shown on this slide and it basically shows you a break down of the percent of each risk factor at different ages. You will be able to see on the slide that the main risk factor when you’re over 60 is age but you can see that when you’re young, around 40, smoking and again the cholesterol are major players along with high blood pressure. So I think it's important to know the age of the patient and what you are trying to treat.

10-year Risk of CHD
%
0
5
10
15
20
25
30
% 10-yr Risk 2 2 2 3 4 5 6 8 10 12 16 20 25 30
4 5 6 7 8 9 10 11 12 13 14 15 16 17
NCEP & Framingham Risk of CHD
8 Points8 Points
TChol >200=5 pointsHDL <40=2 pointsBP >140=1 pointSmoking=5 points
Age 45
13 points Total13 points Total
NCEP
High Risk45 y/o Baseline Risk (3)-No RF
The ten-year risk of coronary heart disease at age 45 is shown on this slide to illustrate the previous slide’s principles. If you see, I have listed each of the four major risk factors from Framingham – the total cholesterol, the HDL, the blood pressure and the smoking. If you start at the top and you had all those factors and you are 45, I can bring your risk all the way down to the very low point of around 3 or 4% because I have 13 points to take off of your total.

10-year Risk of CHD
0
5
10
15
20
25
30
% 10-yr Risk 2 2 2 3 4 5 6 8 10 12 16 20 25 30
4 5 6 7 8 9 10 11 12 13 14 15 16 17
NCEP & Framingham Risk of CHD
8 Points8 Points
TChol >200=1 pointsHDL <40=2 pointsBP >140=1 pointSmoking=1 points
Age 60
5 points Total5 points Total
NCEP
High Risk60 y/o Baseline Risk (1010)-No RF%
But if you were a person who was much older as you can see on the next slide at 60, even the very best I can do, I can only get you down to around a 6% ten-year event rate because at that point in time your age is the most important risk factor. It’s not the other additive risk factors you can see comparing again the previous slide at age 45 with the current slide at age 60 – you can see there’s a big difference in the points that I have given you and also the maximum points that you can reduce.

CRPMore than a Marker for CHD
Marker of CHD RiskMarker of Inflammation
AtherosclerosisEndothelial Dysfunction
Proinflammatory
Stable CADAcute coronary syndrome
Stroke, PVDxPost MI
Metabolic syndromePCI
DiabetesHypertension
CRP levels 1 mg/L (low risk)1 to 3 mg/L (intermediate)
>3 mg/L (high risk)Circulation. 2004;109:1914 –1917
WBC Adhesion
Endothelial ActivationCytokine Stimulation
AtherosclerosisProgression
CRP (monomeric)
This slide shows CRP, which is an inflammatory marker. Now this is really important because in recent days we’ve noticed the White Paper from Circulation July 13 from Dr. Grundy representing the National Cholesterol Education Program has discussed more in depth information about the inflammatory marker. And I think many of us now are noticing that certainly it is a marker for inflammation throughout the body or an inflamed endothelium but now we are starting to see research from scientific areas that are actually showing us that C reactive protein is more than a marker and may be in itself atherogenic and this slide simply depicts and lets you see some of the effects that occur other than just being a marker.

Apoptosis as Link Between Inflammationand AtherothrombosisApoptosis as Link Between Inflammationand Atherothrombosis
Lipid Rich Plaques
Macrophages undergo apoptosis
Expression of TF and active caspase-3
Human AtheromaN=15 carotidsN=6 coronaries
CD-68 Immunostaining
Caspase-3Immunostaining
Tissue FactorImmunostaining
Fib-Fibrous areaLIP-lipid core Circulation April 27, 2004;109:2001-2008
Again a link that has been very difficult for many people to actually connect is the connection between again inflammation and atherothrombosis or a blood vessel that simply closes off – it thromboses off. This study that was done in Circulation within the last six months shows us an area that are taken from humans from the carotids and coronary arteries and now for the very first time links macrophages, which again are general purpose antibodies that suck up cholesterol and are their own little chemistry factories that actually produce compounds that brake down the cap that makes you rupture. It is now shown that each of these three little slides show you the actual same staining location that connects macrophages to tissue factor which when you cut your hand you clot, which is thrombotic, with actually death pathways, which means that endothelial lining cells die of a process called apatosis or programmed cell death. Many of us wonder how do you link inflammation with atherothrombosis? Well this is the same cut specimen in the same patient that shows staining of all three areas at the same time. That tells us that the plaque has a lot going on than just lipid itself. It shows an activation again of the tissue factor, which is clotting and at the same time activation of endothelial cell death, which means cells are dying and when they die, again it makes it more thrombotic and more like Velcro where things stick down and cause atherosclerotic problems.

Relationship Between C-Reactive Protein and CV EventsRelationship Between C-Reactive Protein and CV EventsPravastatin or Atorvastatin Evaluation and Infection Therapy–
Thrombolysis in Myocardial Infarction 22 (PROVE IT–TIMI 22) Investigators
3745 patientswith ACS
Copyright © 2005 Massachusetts Medical Society. All Rights Reserved.Ridker PM, et al. N Engl J Med. 2005;352:20-8.
In a recent paper that was published in the New England Journal of Medicine this year in 2005 by Dr. Ridker, he takes a look at some breakdowns showing inflammation added to cholesterol and whether or not it would actually change the risk of recurrent myocardial infarctions in this acute coronary syndrome population of 3,000 patients.
Now the importance is to point out, as we talked earlier, that inflammation measured by C reactive protein is important. And I think this study with acute coronary syndrome patients makes the point. For example, in the PROVE-IT trial or the TIMI-22, the people who had again the lowest risk of having a cardiovascular – another recurrent infarction, were the guys that had LDL cholesterol’s of less than 70 as you can see from the slide and a CRP less than 2 mg/liter compared to the guys with an LDL greater than 70 and a CRP greater than 2. So it tells you it’s LDL cholesterol and it’s also inflammation that really does play a role in these cardiovascular events.

Influence of C-Reactive Protein on Atheroma VolumeInfluence of C-Reactive Protein on Atheroma Volume
REVERSAL
Copyright © 2005 Massachusetts Medical Society. All Rights ReservedNissen SE, et al. N Engl J Med. 2005;352:29-38.
In another very provocative paper published in the New England Journal in the same issue as Dr. Ridker’s, Dr. Steve Nissen from the Cleveland Clinic from the REVERSAL trial which is stable angina patients with intravascular ultrasound correlates the total atheroma volume with C reactive protein and as you can see in the folks who were treated with atorvastatin 80, there is a marked regression below the line and you can see the little dash lines or the 95% confidence intervals. If you were able to change your CRP down to a –6 to a –10 mg/dL, you can see a marked improvement in the actual total volume regression as you get further away from baseline and the actual treatment with a statin drug. So I think it’s telling us for the very first time we can show you not only stabilization of plaque, reduction in cardiovascular events, how about regressing atherosclerosis in the human body. This is the first decade and first century we’ve actually seen that. So it’s an exciting time.

≥160 mg/dL
≥130 mg/dL
≥130 mg/dL
≥100 mg/dL
Initiate TLC
190 mg/dL (160-189 mg/dL:
LDL-lowering drug optional)
160 mg/dL
130 mg/dL (100-129 mg/dL: consider drug
options)
100 mg/dL (<100 mg/dL: consider drug
options)
Consider Drug Therapy
<160 mg/dL
<130 mg/dL
<130 mg/dL
<100 mg/dL (proposed
optional goal: <70 mg/dL)
LDL-C GoalRisk Category
Lower risk:0-1 risk factor
Moderate risk:2+ risk factors (10-year risk <10%)
Moderately high risk:2+ risk factors (10-year risk 10% to 20%)
High risk:CHD or CHD risk equivalents (10-year risk >20%)
ATP III LDL-C Goals and Cutpoints for Lipid-Lowering Interventions
Grundy, S. et al. Circulation. 2004;110:227-239.
The ATP LDL cholesterol goals have been recently published again and this is referenced on your slide and you may want to get this for your office for your clinical nurse specialty folks and your paramedical people to help take care of patients, but notice only one thing I want to point out. Everything on here is pretty much the same except for the high-risk patient. If you’ll take a look, the proposed optimal goal is a LDL cholesterol of less than 70 and that’s pretty tough to get. So I think it’s telling us that the cholesterol goal of under 100 was great atone time, but I think our data is now starting to support lower is better and it looks like the goal they are looking at for the new guidelines looks like it is less than 70 – certainly for people who are at high risk. That means somebody that has diabetes that has not had a heart attack yet. A person who has peripheral vascular disease or maybe a person who has an abdominal aortic aneurysm that is talked about. We don’t normally think about those things but in the cath lab we do because we have to go through those aortas and we do have to go through those legs and they are certainly loaded with atherosclerosis. I think this is a reasonable and prudent idea and I think if the cholesterol level is less than 70, I think that’s great for the people certainly that are high risk.

Coronary Heart Disease Risk Equivalents
Coronary Heart Disease Risk Equivalents
Clinical forms of atherosclerotic disease
Peripheral artery diseaseAbdominal aortic aneurysmSymptomatic carotid artery disease
DiabetesMultiple risk factors that confer a 10-year risk of CHD >20%
National Cholesterol Education Program Expert Panel. JAMA. 2001;285:2486-97.
As previously discussed in the previous slide and comments, you can see on this slide, I have just taken a one photo inset from a case of ours here, and I think you can see there is a gap in the artery as it comes down from the leg. This is an example of a patient who has no chest pain, actually came because he was wanting to take Viagra for some impotency problems. He was subsequently put on the treadmill and was not able to go very far. When he got ready for his heart cath, we could not get up this gentleman’s leg. So I think it tells us that certainly even if you do not have a heart attack or something like that or diabetes, if you have peripheral vascular disease, it still counts and your risk is considered high.

Therapeutic Lifestyle Changes (TLC) in LDL-C Lowering Therapy
Therapeutic Lifestyle Changes (TLC) in LDL-C Lowering Therapy
Major Features
TLC dietReduced intake of cholesterol-raising nutrients (same as previous Step II Diet)
Saturated fats <7% of total caloriesDietary cholesterol <200 mg per day
Options for LDL-C lowering Plant stanols/sterols (2 g per day)Viscous (soluble) fiber (10–25 g per day)
Weight reduction Increased physical activity
National Cholesterol Education Program Expert Panel. JAMA. 2001;285:2486-2497.
Therapeutic lifestyle changes or what we call TLC has many different abbreviations and names in lowering your cholesterol I think is important. As a person who is very interested in healthy ways to treat things other than drugs, I would definitely consider this. I personally think that it’s important that you start with your diet and exercise. Which is more important to a person who needs to lose weight since that seems to be the epidemic or pandemic of the world currently. Would it be for you to say to the person, “you need to exercise more” or would you say to the person, “you need to cut your calories more”. One of them accounts for 80% of the benefit. You might want to think –which one would you recommend? Well if you ask 250 medical students, the answer is pretty much split 50/50. Half the group would say, “shoot, they need to exercise more and eat whatever they want” and the other group would say, “no, they need to cut their calories and they don’t care if they exercise or not”. The answer is – cut the calories, it accounts for 80% of weight loss. It’s not the exercise that’s the major player here. So even if a person that is overweight says that “you know, I can’t really exercise because I have a bum leg”. That’s okay, you can still cut your calories because that accounts for 80% of your weight loss. And most of the people that I see that have high cholesterols, I doubt seriously that if most of us couldn’t lose a few pounds. And if you only add a pound on for every year past high school, you can see why you are 40 pounds over – most of the time. So cutting calories is the major player.

Steps to Achieve Therapeutic Lifestyle Changes
Steps to Achieve Therapeutic Lifestyle Changes
• Reinforce reductionin saturated fat andcholesterol
• Consider addingplant stanols/sterols
• Increase fiber intake• Consider referral to
a dietitian
• Initiate Tx forMetabolicSyndrome
• Intensify weightmanagement &physical activity
• Consider referral to a dietitian
6 wks 6 wks Q 4-6 mo
• Emphasizereduction insaturated fat &cholesterol
• Encouragemoderate physicalactivity
• Consider referral toa dietitian
Visit IBegin Lifestyle
Therapies
Visit 2Evaluate LDL-C
responseIf not at goal,
intensifyLDL-C Lowering Tx
Visit 3Evaluate LDL-C
responseIf not at goal,
consider drug Tx
MonitorAdherence
to TLC
Visit N
Third Report of the National Cholesterol Education Program (NCEP) Expert Panel on Detection, Evaluation, and Treatment of High Blood Cholesterol in Adults (Adult Treatment Panel III) Executive Summary. NIH Publication No. 01-3670, May 2001.JAMA. 2001;285:2486-2497.
Now for those who don’t want to be careful – and we certainly have plenty of stents – and you want to keep your weight high, this is probably the better way to go about it. First of all you need to start with this algorithm and basically this is straight out of the National Cholesterol Education Program. I think you can read this for yourself. It’s pretty straightforward.

Balancing Safety with Efficacy
LDL-CLower Better ?
DosageLower Better?
Fewer CV Events?
Fewer Side Effects?≅Total 72 patients
≅30,000 patients
Pedersen TR, et al. Arch Int Med. 1996;156:2085-92.Lipid Study Group. N Engl J Med. 1998;339:1349-57.Sacks FM, et al. N Engl J Med. 1996;335:1001-1009.
Downs JR, et al. JAMA. 1998;279:1615-1622.Shepherd J, et al. N Engl J Med. 1995;333:1301-07.Pasternak RC, et al. Circulation. 2002;106:1024-28.
Balancing safety and efficacy. This is always a real teeter-totter kind of problem, and I’m sure many of you say well gosh you know drugs have side effects and I’m concerned. But if you tried to get aspirin approved currently by the FDA, I doubt if anyone would approve it but yet it saves a significant amount of lives – like it’s something like 42% reduction in cardiovascular events.
So I think if you take a look at balancing the risk ratio versus the benefit, statin drugs that we currently use are one of the safest compounds that we have ever seen. There’s hardly anything that has been proven in all the different types of statins to be as safe. Certainly we did have trouble with cerivastatin, it was more toxic than we expected but for the other compounds that have been on the market, they have been extremely safe.

Placing Safety of Statins in PerspectivePlacing Safety of Statins in Perspective12,500,000 Americans taking statins
>50,000 individuals studied in statin clinical trials averaging 5.4 yearsNo serious morbidity or increase in mortality observed in drug treatment groups
Elevated ALT/AST generally occur in 0.5%-2.0% of cases and are dose-dependentReported myopathy in statin trials: ~5%Severe myopathy reported: 0.08%Myopathy occurs more frequently with certaincombination therapies such as statins and fibratesFDA report: Fatal rhabdomyolysis extremely rare(<1 death/million prescriptions)
Pasternak RC, et al. Circulation. 2002;106:1024-1028.
Placing safety of statins in perspective and I have listed here basically six things. I think most of you can read these on your own. They are pretty straightforward. But 12 million people have taken these drugs and probably worldwide, it’s much more than that. Certainly, there are concerns that all of us as clinicians and paramedical people need to watch and ask patients about the myopathies or weakness in the arms and stuff are ones that many of us talk about but again a very low percentage of people have trouble. The FDA report for fatalrhabdomyelosis is extremely rare. For example, less than one death per million prescriptions. I can’t think of a drug that is that safe. I am not even sure if you eat sugar every day it’s that safe. So I think these drugs have really proven out to be a very safe class.

Muscle Disorders That Can Occur With Statin Use
MyopathyGeneral term referring to any disease of muscles; myopathies can be acquired or inherited and can occur at birth or later in life
MyalgiaMuscle ache or weakness without CK elevation
MyositisMuscle symptoms with increased CK levels
RhabdomyolysisMuscle symptoms with marked CK elevation (greater than 10x the upper limit of normal [ULN]) and creatinine elevation (usually with brown urine and urinary myoglobin)
Pasternak RC, et al. Circulation. 2002;106:1024-1028.
Muscle disorders – I put this slide in. I’m not going to really spend any time on it but you can see the different definitions. I think it’s important when you look at your patients and you chart things to make sure that you have these properly put together. Sometimes these myositis, myalgias and myopathies get kind of confused.

Pharmacokinetic Interactions Between Statins and Fibrates
Pharmacokinetic Interactions Between Statins and Fibrates
Gemfibrozil Fenofibrate
Atorvastatin Not available Not available
Pravastatin Significant increase in C-max No effect
Fluvastatin No effect Not available
Simvastatin Increased C-max by 112% No effect
Cerivastatin Increased C-max by 2- to 3-fold No effect
Rosuvastatin Increased C-max by 2-fold No effect
Pharmacokinetic interactions between statins and fibrates are very important and I have listed here some interactions that are very important if you use gemfibrozil. Currently, I probably would say to most of the young docs that I train, I would not use gemfibrozil with a statin. If I have to, I would rather use phenofibrates. And the reason is shown there on the right hand side. As far as interactions, you don’t see as many as you do with gemfibrozil. I think we noticed that gemfibrozil has some difficulties with metabolism with some of the statins so currently I do not recommend its combination use. If you want to lower triglycerides in a patient that has Type 2 diabetes, I would suggest that you use a phenofibrate drug for fibric acid instead of gemfibrozil. I think at one time it was the only drug that we had. We now have safer drugs that are quite good and I think it is a better choice for most people.

Increased Muscle Enzymes Observed in Major Statin Trials
Increased Muscle Enzymes Observed in Major Statin Trials
0
0.1
0.2
0.3
0.4
0.5
0.6
0.7
WOSCOPS AFCAPS CARE 4S LIPID HPS
TreatmentPlacebo ACC/AHA Advisory on Statins
Severe myopathyLovastatin 0.8%Simvastatin 0.8%
CK >x10 normalPravastatin 0.9%
Pasternak RC, et al. J Am Coll Cardiol. 2002;40:567-572.
% P
atie
nts
with
CPK
> 1
0x
ULN
The next slide just simply looks at again the increased muscle enzymes observed with major statin trials. I put this in her for your own information, and I think again you can see all the trials. Now I would point out one thing. Any time a new class of drugs comes to market and this example being AFCAPS – that’s lovastatin, we all targeted for safety. So a lot of the cases that we are looking at here are excellent reporting when it first comes out. But as certainly drugs get used more and more, I think we are less likely to report them because we are expecting certain types of effects that we’ve known. So be careful with the interpretation of this and even if you look at the AFCAPS trial, you can see that it’s still not very high incidence of elevated CPK’s above ten times normal but you can see the other trials have much lower reporting. I think again, it’s improvement in the knowledge base in the reporting that’s done at first.

Risk Factors for Statin-Associated Myopathy
Risk Factors for Statin-Associated Myopathy
Concomitant medications or consumption of:
Fibrates (especially gemfibrozil)Nicotinic acid (rarely)CyclosporineAzole antifungals (ketoconazole)Macrolide antibiotics (erythromycin, clarithromycin)HIV protease inhibitorsNefazodone (antidepressant)VerapamilAmiodarone>1 qt/day grapefruit juiceAlcohol abuse
Advanced age (especially>80 yr; women > men)Small body frame, frailtyMultisystem disease (eg, chronic renal insufficiency, especially due to diabetes)Multiple medicationsPerioperative periods
Pasternak RC, et al. Circulation. 2002;106:1024-1028.
This slide probably deserves a little attention. You need to look – anytime you talk about use of statin drugs –risk factors that might be associated with myopathies or again muscle toxicity and you can see there are a list of things and you might want to look down through there. Drug interactions are important. It almost requires a computer with a pharmacy expert to keep track of some of these drugs and as you know, I don’t know many people who are 60 years of age or older that don’t take at least two or three drugs. So it is very easy to get into trouble with these combined agents. So look across there and see if there are any of the ones that you happen to particularly like to use.
Now down in Texas, we have grapefruit juice a lot and in Florida and so if somebody wants to inhale a lot, like a quart a day, you might want to rethink some of their enzymes in the liver like the P450 system. But by and large other than that, I think you’ll find that these are not too much of a problem. I would point out that women who are older seem to have a little bit more risk for statin myopathies - smaller framed person, more frail as pointed out here.

Guideline RecommendationsGuideline RecommendationsEvaluate muscle symptoms and CK before starting therapy. Evaluate muscle symptoms 6 to 12 weeks after starting therapy and at each follow-up visit. Obtain a CK measurement when patients have muscle soreness, tenderness, or pain.Discontinue statin therapy (or statin and niacin or fibrate if the patient is on combination therapy) when a CK greater than 10 times the ULN is encountered in a patient with muscle soreness, tenderness, or pain.Hypothyroidism predisposes to myopathy, a TSH levelshould also be obtained in any patient with muscle symptoms.If the patient experiences muscle soreness, tenderness, or pain with either no CK elevation or a moderate elevation (3-10X ULN), follow the patient’s symptoms and CK levels weekly until there is no longer any medical concern.
Pasternak RC, et al. Circulation. 2002;106:1024-1028.
This is a very nice paper that was done by Dr. Pasternaki. I would urge you to look at it if you are interested in this area. It is a well-written paper and very well done.
Guideline recommendations I have also listed on this slide and it goes through basically how to evaluate it. The most important thing to me on this slide is that if you are going to put this person on a statin drug, for sure pull a set of enzymes for CPK to start with and then if they come back in two weeks and say, “you know, I’ve got aches and cough and chills or whatever”, you can secondarily look at their enzymes if there is a concern about a myopathy. Maybe all it is, is a viral illness and there is no change in their actual CPK so it is very helpful to get a baseline set of liver function tests and again CPK levels. It is also important to look at anybody that might have thyroid risk. A lot of older people have hypothyroidism and that is a secondary cause of elevated lipids.

o A. Rosuvastatin 10 mgo B. Niacin 1000 mg and lovastatin 40 mg o C. Simvastatin 10 mg and ezetimibe 10 mgo D. All of the above can lower LDL-C by >40%
Which of the following lipid lowering drug regimens can lower LDL-C by >40%?
The next slide is a question for you in the audience. Which of the following lipid-lowering drug regimens can lower the LDL cholesterol greater than 40%?
A. Rosuvastatin 10 mg B. Niacin 1,000 mg and lovastatin 40 mg C. Simvastatin 10 mg and ezetimibe 10 mg D. All of the above can lower the LDL cholesterol greater than 40%.

When to Consider Coadministration Therapy
Some patients require coadministration therapy to reach their ATP III treatment goalsCoadministration therapy may be needed to
Gain an additional LDL-C reductionAchieve a non-HDL-C goalRaise HDL-CTreat elevated triglycerides
Coadministration is also effective for patients whoCannot tolerate or do not respond to other lipid lowering drugsHave dose-related side effects to monotherapy with other agents
Third Report of the National Cholesterol Education Program (NCEP) Expert Panel on Detection, Evaluation, and Treatment of High Blood Cholesterol in Adults (Adult Treatment Panel III). NIH Publication No. 02-5215, 2001.
When do you consider lipid combining two agents – for example coadministration of therapy? Some patients can require, as you’ve seen in the ATP III goals the combination of two different types of drugs to attain the lipid reduction that you need and certainly coadministration may be needed especially in the patients that have diabetes. Another group of people that I see a lot are people that have already had a heart attack that still are not under the 99 goal for the LDL are considered high risk which now optimally is around 70 or less, which means it is a lot tougher. So these type of patients would potentially benefit from coadministration from a combination drug that would actually lower their LDL cholesterol.
This slide takes a look at considering coadministration therapy. Some patients do require coadministration to reach their ATP III target. There are actually other groups of people who actually coadministration may be needed to gain additional LDL reduction because they didn’t get to goal, achieve a non-HDL cholesterol goal and that simply calculated by the total minus the HDL and the goal should be less than 130 or to raise the HDL cholesterol sometimes coadministration is beneficial. Other folks are to treat elevated triglycerides. Also it is effective for those that cannot tolerate the very high dose of statin drugs and there are some patients that you probably can think of where you wouldn’t want to raise the dose because of concern of toxicity or they had myopathies but if you combined it, you might be able to get by with the coadministration. So again, there are a number of people that might benefit from coadministration therapy.

Rule of 6: Doubling Statin Dose Elicits Additional 6% Decrease in LDL-C
% Reduction in LDL-C
One-Step Coadministration
Three-Step Statin Titration
10 20 30 40 50 600
- 6% - 6%
Statin 10 mg 20 mg
40 mg
80 mg
- 6%
Statin 10 mg + Ezetimibe 10 mg
The next slide takes a look at the rule of six. I would like to attribute this to my good friend Bill Robertson in Dallas because I think he was the one that spends a lot of time explaining how these drugs work but I think what it tells you is when you first give a statin drug you get the major effect and then for each additional increase in the dose, you only get another 6% drop and it simply shows in this slide that example. At the same time, if you look at the one below it, it shows the coadministration of 10 mg of a statin with a new type of GI blocking drug called ezetimibe. And you notice that you end up with a very similar reduction in the LDL cholesterol.

Atorvastatin10/20/40/80 mg
211 mg/dL*
Simvastatin10/20/40 mg†219 mg/dL*
Mea
n %
Cha
nge
in L
DL-
C F
rom
Bas
e lin
e
LDL-C Lowering Greatest at Lowest Statin Doses
Jones P, et al. Am J Cardiol. 1998;81:582-587.
*Mean baseline LDL-C.†At the time of this study, the maximum dose for simvastatin was 40 mg.
Daily Statin Dose
10 mg
20 mg
40 mg
80 mg16% reduction in LDL-C with 3 titrations
13% reduction in LDL-C with 2 titrations
38%
46%
54%
28%
35%
-60%
-50%
-40%
-30%
-20%
-10%
0%
38%
46%51%
28%
35%41%
This slide shows a very similar benefit from again taking a look at how you combine drugs. It shows a lowering of the greatest at the lowest statin dose and you can see very similar to the previous slide – if you take a look at the first effect of the drug, you get your greatest benefit and if you compare the two different compounds here, you can see in this study that was done by Peter Jones, the actual drop in the actual LDL reduction, and you can see that it can down to a fairly good reduction. But even though you see this slide and it looks great, to get to 70 in a patient who has heart disease even with these very powerful drugs, we still struggle.

EASE Trial: Achieving NCEP GoalUnderlying baseline of statins6-week randomized, blinded, placebo-controlledPrimary endpoint
% LDL-C change from baseline% achieving NCEP ATP III goal
Baseline LDL-C 129 mg/dLSpecial populations
CAD patients: LDL-C at baseline = 123 mg/dLMultiple risk factors 147 mg/dL<2 risk factors 167 mg/dL
SafetyALT>3X ULN
Ezetimide 0.4%Placebo 0.2% (p=NS)
PPlaceboEzetimibemg/dL
0.001-0.81.3HDL-C
0.001-1.6-12.8TG
0.001-1.1-25.1 LDL-C
% A
chie
ving
NC
EP
Goa
l
71
20.6
01020304050607080
Ezetimibe Placebo
n = 3030
Pearson T, et al. Abstract presented at: Annual Scientific Sessions of the American College of Cardiology; March 7–10, 2004; New Orleans, LA.
The next slide is the EASE trial, and everybody likes new information that’s not even published yet. Well this was presented at the American College of Cardiology in March 2004 by Dr. Tom Pearson. This is a very neat trial and what this does. It lets us take a look at the addition of using again ezetimibe in having people achieve their NCEP goal. And if you see the slide, you can very easily find that in the population studied – in again, a six-week randomized trial, they were able to achieve goal in 71% versus if they were in the placebo group, they only were able to achieve it with 24 and 6%. It’s not a small study. It’s 3,000 patients and you can see the benefit of LDL reduction with this compound compared to placebo.

Rational Coadministration OptionsStatins + bile acid sequestrants
Lower LDL-C, raise HDL-C, variable effect on TGUse associated with significant GI distress
Statins + fibratesEffect on LDL-C is variable; lower TG; raise HDL-CMonitor for myopathy and symptoms of muscle pain
Statins + nicotinic acidLower LDL-C and TG; increase HDL-CMonitor closely for myopathy and flushing
Statins + cholesterol absorption inhibitor (ezetimibe)Lower LDL-C and TG, raise HDL-CMonitor liver enzymes as recommended in statin labeling
Third Report of the National Cholesterol Education Program (NCEP) Expert Panel on Detection, Evaluation, and Treatment of High Blood Cholesterol in Adults (Adult Treatment Panel III). NIH Publication No. 02-5215, 2001. Feldman T, et al. Am J Cardiol. 2004;93:1481-1486.
Looking at rational coadministration options – and again, I think all of us here already know this but to go through it – statins can be certainly combined as we did many years ago with bile acid sequestrants. Unfortunately most of us don’t use those because they’ve got too much GI side effects. No one would take them. I think most patients I know use them as a doorstop to actually hold their doors open.
The next one that came along was actually gemfibrozil, which was a blockbuster with looking at the VA HIT trial and showed benefit. Well if you combine the fibrates, which help decrease the triglycerides a lot – and certainly diabetes fit into that category – or diabetic patients – the addition of a statin to that gave us a little difficulty with some side effects and risks. So that’s another concern and option but one that we’ve probably…phenofibrates are a better choice.
And now I think from the recent publication in the Archives of Internal Medicine, Dr. Whitney, a very nice paper looking at the combination with the nicotinic acid type drugs and the statins, it gives you the benefit of potentially lowering your LDL and raise your HDL significantly. But again, those are folks that you need to monitor very carefully and certainly stay on the same type of niacin-type drug if you are going to use it. Probably again, some of the newer slower released drugs are better tolerated by some patients. And then the newest area that we’ve talked about is the actually addition of ezetimibe to statins which I’ll have to say totally changed many of our directions. It is a drug that is very, very easy to take and has been very helpful. I think that these type of compounds in the future – this being one of the very first type – are going to be important because they do not increase in a lot of ways, our side effect profile. Although you do have to watch for a mild increase in liver function tests as which has been reported by the FDA.

Fewer Patients Administered Coadministration Therapy Required
Increased Statin Dose
Feldman T, et al. Am J Cardiol. 2004;93:1481-1486.
Patie
nts
Req
uirin
g Si
mva
stat
in
Dos
e In
crea
se (%
)
0
10
20
30
40
50
60
70
80
simvastatin20 mg
EZE 10 +simva 10
EZE 10 +simva 20
EZE 10 +simva 40
68%
33%*
22%*
12%*
*P <0.001 vs. simvastatin 20 mg
EZE = ezetimibe
Looking at again coadministrations and required for increased statin dosing, you can see from this study from Dr. Feldman, that if you are looking at patients requiring simvastatin dose increases – if you use just a standard dose of simvastatin 20, you can see 68% but if you were to then add even one-half the dose and just use 10 of simva plus ezetimibe 10, notice now you went from nearly 70% requiring again dose increases to only 33%. And you can see further down the slide as you increase the dose of the statin, you even had less and less people requiring increased statin dosing. So I think it’s telling us that the use of a drug like ezetimibe really does add to the therapy that we use now.

Insull W, et al. Arch Intern Med. 2004;164:1121-1127.
Lipid-Modifying Effects of Extended Release Niacin and Lovastatin
29
27
21
11
N/A
N/A
-24
-9
-3825-46-392000
N/A24-43-351500
-2918-38-321000
N/A7-35-29500
ER Niacin Dose
mg/day
Lovastatin Dose, mg/day
20 40 20 40 20 40
% ∆ LDL-C % ∆ HDL-C % ∆ TG
n = 34 for lovastatin 20 mg + ER niacinn = 32 for lovastatin 40 mg + ER niacin20-week dose titration study with sequential 4-week treatment periods.
Lipid modifying effects of extended released niacin and lovastatin have been looked at in this slide. This is from Insullin the Archives of Internal Medicine and basically goes through an extended released niacin form and then takes a look at the actual reduction in the LDL cholesterol. I think most of you can read this on your own very easily but you can see the benefit of adding niacin to a statin drug.

8%
- 23%
9%
- 26%
2.4%0.9%
- 1.3%
- 44% - 44%
-60
-50
-40
-30
-20
-10
0
10
20
Reprinted from Journal of the American College of Cardiology, V40(12), Davidson MH, et al, EzetimibeCoadministration with Simvastatin in patients with primary hypercholesterolemia: 2125-2138, Copyright © 2002, with permission from the American College of Cardiology Foundation.
Lipid Modification With Low Doses of Ezetimibe and Simvastatin
LDL-C HDL-C TGR
educ
tion
From
Bas
elin
e at
Wee
k 12
(%)
Placebosimvastatin 80 mgezetimibe 10 mg + simvastatin 10 mg
The next slide is from Michael Davidson and is a very nice paper that took a look at the combination of the high dose of simvastatin versus if I was just to use a low dose plus again, ezetimibe 10 mg. I think you can appreciate from the slide if you look at the LDL, they are both 44% down. Now that means that in some people’s thoughts, you could use a high dose of a single monotherapy or you could use a low dose plus ezetimibe and get the same drop. So I think again depending upon the physician’s choice of what he would like to do, you can also notice the nice improvement in HDL that’s around 9% although to me that’s not enough for a guide – you need a lot more than that but probably the best that we currently have. The triglyceride fall is also equally as good as the high dose of simvastatin 80.
Davidson M, McGarry T, Bettis R, et al. Ezetimibe co-administered with simvastatin in 668 patients with primaryhypercholesterolemia. J Am Coll Cardiol. 2002;39(suppl A):Abstract 1084-90.

Reduction of CrP by Simvastatin and Ezetimibe
Sager PT, et al. Atherosclerosis. 2005;179:361-7.
-50-45-40-35-30-25-20-15-10-50
simvastatin (mg)ezetimibe +
simvastatin (mg)
10 20 40 80 10/10 10/20 10/40 10/80M
edia
n C
hang
e (%
) -4.4-8.3
-26.9
-20.0
-26.3-31.8
-35.9
-44.4
*
*
*
**
*p <0.01; ** p = 0.03 coadministration vs. simvastatin alone
The reduction in C reactive protein by simvastatin and ezetimibe is an important issue because I think you are now seeing that many of us think that inflammatory signals are worth measuring in especially people who are borderline. You can’t decide whether to treat them or not but maybe they are high risk. So you pull a CRP if its high, you may choose to treat because you feel like that is the thing to do because it may be representing vascular inflammation. Here you can see the benefit of adding again ezetimibe to simvastatin for each dose and the marked reduction in the actual CRP level. I think this tells us that again, not only with this drug, but also with a study done by Christy Balletime who looked at atorvastatin with ezetimibe also, there are marked reductions in these type – by adding these two compounds together to reduce C reactive protein. I think this could be a big deal because if you have a person that would potentially would have acute coronary syndrome that has – and is well known from other studies – very high C reactive protein, this might be a way to bring it down very quickly in an acute patient although that has not been tested or studied at this time.

HPS: Dollars and CentsHPS: Dollars and Cents
305452
210 324
0
200
400
600
PCI CABG
Statin
Placebo
305
452P
atie
nts
Cost ( $ ) 950,000 3,840,000
20,536/5 yrs
P<0.0001
P<0.0001
95128
PCI= $10,000CABG= $30,000
Heart Protection Study Collaborative Group. Lancet. 2002;360:7-22.
The next slide is one of mine I put together because people always ask how much it costs dollars and cents, if you say, take a statin or you don’t take a statin. So I thought I would do it in Wal-Mart pricing.
A PCI – I’ll give you a special price of about $10,000 a crack. Just a rough estimate. Certainly now that eachstent costs $3,500, it’s probably going to be more than that but we’ll do the cheapest one we have. CABG, a turn key for around $30,000. Don’t know many people who do that but if you estimate it. Now if you take a look at the Heart Protection Study and you look at the number of patients and you can multiply them yourself and see, you save a lot of money using statin drugs to keep people from having to have interventional procedures and CABG’s. And you can see again, depending on whether the patients get PCI’s or whether they get CABG, in 20,000 patients over five years, you would have saved nearly $4 million bucks. So it is cost effective.

Cost Effectiveness of Simvastatin Treatment for 5 Years in Patients With
LDL-C >261 mg/dL
5,1001,60010,5005,400Cost per year ($)
0.160.280.160.28Years of life gained
8094591,6851,524Net
–1,601–1,783–725–718Associated morbidity
2,4102,2422,4102,242Intervention
Costs ($)
WomenMenWomenMenVariable
Direct + Indirect CostsDirect Costs
Johannesson M, et al. N Engl J Med. 1997;336:332–336.
Another important study that was done in the New England Journal of Medicine that was done a few years back was the cost effectiveness of using simvastatin treatment for five years in patients that have cholesterol LDL’s greater than 261 mg/dL. This is not a low number. I don’t think many of us in this audience see folks that have this high of cholesterol levels. But if you look at the cost per year, direct and indirect cost, it is certainly very important and saves a lot of dollars if you treat these people. Of course as I say, the 261 LDL level is certainly higher than people that I see and these are really sort of borderline on being familial hypercholesterolemic heterozygotes.

Cost per Year of Life Gained in Patients With CHD Who Received Simvastatin
for 5 Years
6,2003,8003,2001,200SavingsSavings3098,5004,7004,9001,600SavingsSavings261
13,3006,2008,6002,100SavingsSavings213Direct + indirect costs
6,2003,8007,1004,20013,2006,7003098,5004,70010,3005,50018,8008,800261
13,3006,20016,4007,00027,40011,400213
Direct costsWomenMenWomenMenWomenMen
Age 70Age 59Age 35TC before treatment (mg/dL)
Copyright © 1997 Massachusetts Medical Society. All Rights Reserved.Johannesson M, et al. N Engl J Med. 1997;336:332–336.
The next slide takes a look at the cost per year of life gained in patients with heart disease (that’s secondary prevention) who have received simvastatin for five years. As you look across the direct cost and look at the age, whether it’s a man or a woman, you can see again the benefit of treatment when you treat these people to lower their cholesterol levels with a statin drug. And again, the indirect and direct cost added together, you can see even more savings.

Cost of LDL-Lowering Drugs Impacts Cost Effectiveness of Lipid Treatment ATP III
Lipid Goal
25,00050,000100,000200,0005
12,50025,00050,000100,00010
625012,50025,00050,00015
3125625012,50025,00025
12502500500010,00035
Ten-Year Risk(%)
Annual Cost of LDL-Lowering Therapy
Cost per Quality-Adjusted Life Years
$1000/Yr $500/Yr $250/Yr $125/Yr
Third Report of the National Cholesterol Education Program (NCEP) Expert Panel on Detection, Evaluation, and Treatment of High Blood Cholesterol in Adults (Adult Treatment Panel III). NIH Publication No. 02-5215, 2001.
The next slide is an important one because it comes from the National Cholesterol Education expert Panel. This was published in JAMA in 2001. Again, this looks at a ten-year risk – again 25, 35, 15, 10 or five and it breaks it down to the actual annual cost of LDL-lowering therapy. Now at the time these drugs came out, they were certainly more expensive than they were now and so many of us had concerns about how much it costs. But if you look at it long term over a period again, a ten-year risk, it is very cost effective to lower their cholesterols and bring them under control.

Which of the following statement(s) is/are TRUE regarding generic lovastatin?
o A. 40 mg dose provides ~30% LDL reductiono B. Dosage is available in 10 mg, 20 mg and
40 mg tabletso C. Maximum therapeutic response is usually
seen within 4-6 weekso D. All of the above
This question is asking us, which of the following statements is or are true regarding generic lovastatin?
A. 40 mg dose provides around a 30% LDL reductionB. Dosage is available in 10, 20 and 40 mg tabletsC. Maximum therapeutic response is usually seen within four to six weeksD. All of the above.

Clinical and Cost Outcomes for Lovastatin + Niacin ER for
Each ATP III Lipid Goal
61663.7< 100 mg/dL
40085.6< 130 mg/dL
33389< 160 mg/dL
Lovastatin + Niacin ER Cost
($)
Lovastatin + Niacin ER
Success Rate* (%)
Goal LDL-C + HDL-C
> 40 mg/dL
Armstrong E, et al. J Manag Care Pharm. 2004;10:251-258.
*Success rate defined as a patient achieving LDL-C and HDL-C goals and not experiencing a significant adverse event.Data derived from a decision analytic model; all drug costs at AWP.
The clinical and the cost outcomes for lovastatin plus niacin, again, for extended release in ATP lipid goals are shown on this slide and again from Dr. Armstrong’s very nice paper, you can see again, the combination and success rates are shown very nicely in the ones that are less than 100 mg/dL for LDL and an HDL that has a goal greater than 40. If you look at the actual cost, again, it is very worthwhile of pointing out the pharmacoeconomics of good therapy in taking care of patients.

Steps to Improve Cost Effectiveness of Lipid-Modifying Treatment
Identify high-risk patientsScreen patients for CHD, CHD risk equivalents, and multiple risk factors
Increase effectiveness of treatmentAggressively lower LDL-C to revised ATP III target goals Educate patients
Reduce treatment costsMaximize Therapeutic Lifestyle Changes (TLC)Maximize adherenceUse safe and effective drugs
Steps to improve cost effectiveness of lipid-modified types of treatment identifies high-risk patients and then really screen them. So what you would like to do is that if you have high-risk people – like if their mother or father had heart disease. Now we did not talk about in her about genetic predisposition, but if you look at the Framingham Heart Study and you look at the offspring data from their research – if you have heart disease in your mom or dad before they are around 55 or 60, that probably triples your risk and it just again, makes all of the risk factors even more important. So a high-risk group would be one that would be cost effective to look at.Certainly, somebody that has aggressive lipid lowering because of – showing that increased treatment is better is a very cost-effective way to look at it. Educating your patients is important to reduce the treatment cost by maximizing therapy. For example, if your patients are in the hospital, to let them leave the hospital without being on again statin drugs if they have heart disease unless there is a good reason at a dose that brings them in within range is probably not a good idea because to come back for another intervention or for a CABG is a lot more expensive than to give them a low-cost drug that’s followed - that is a drug that is very safe to use. So again, I would urge you to really look at your patients before they leave the hospital. You have their undivided attention while they are there to make sure their cholesterol is under control.

Case StudyPatient: 51-year-old male; smoker (1/2 pack/day
reduced from 4 packs/day), construction worker
Physical Findings: SBP 135DBP 90Waist (in) 35BMI (kg/m2) 32
Laboratory Measures: TC (mg/dL) 254LDL-C (mg/dL) 178HDL-C (mg/dL) 32Triglycerides (mg/dL) 195Non-HDL-C (mg/dL) 222Fasting Glucose (mg/dL) 115
This is the case study – and I present here a classic case – one that probably most of you see daily. A 51-year-old male that smokes only one-half pack per day reduced from four packs to day, which to me, he needs to quit completely because that’s one of his major risk factors and is a construction worker. A guy who works really at a tough job. You can also see his physical findings. His blood pressure is 135 and diastolic is 90. Waist in inches is 35 and a BMI of 32, which means this man is not liked. If you take a look at his laboratory measures, his total cholesterol is 254, which makes him quite high risk. LDL of 178, which puts him up almost - just really a very high-risk guy. His HDL is classic for most American Anglo men in the 30’s, which is unfortunately not one you want. The triglycerides show you again probably in effect of a person who is overweight and again the triglycerides are elevated in my books and the non-HDL cholesterol of 222. That should be less than 130. And a fasting glucose of 115, which is tending towards again having diabetes. As you can see on his risk factor assessment, his positive family history with the father having a fatal infarction in his late 40’s makes him high-risk to me.

Risk Factor Assessment
Framingham Risk Factor AssessmentPositive family history
Father with fatal MI in late 40’sElevated TC and low HDL-C
Metabolic SyndromeIncreased waist circumferenceElevated TG and low HDL-CHypertensionImpaired fasting glucose
Risk factor assessment – The Framingham Risk Factor Assessment with a positive family history is important. You can see his father had fatal MI in his late 40’s. The total elevated cholesterol that’s real high and the low HDL puts him at very high risk. And then probably more important than anything is the metabolic syndrome. Now you think a diabetic is high risk, you can just double the risk here because metabolic syndrome if you have that, again, the increased waist circumference, the guy with the elevated triglycerides and low HDL, the hypertension and empiric fasting glucose, this man is very high-risk and probably would be visiting the cath lab in his area.

<40 mg/dL<50 mg/dL
MenWomen
>40 in>35 in
MenWomen
≥110 mg/dLFasting glucose
≥130/≥85 mm HgBlood pressure
HDL-C
≥150 mg/dLTG
Abdominal obesity*
(Waist circumference†)
Defining LevelRisk Factor
ATP III: The Metabolic Syndrome(Diagnosis is established when ≥3 risk factors are present)
ATP III. JAMA. 2001;285:2486-2497
Now if you forgot what the definition of a metabolic syndrome is, I have pulled it from the ATP III guidelines. You only need three. Pick any three you like. There is the abdominal obesity – men and women. The triglycerides greater than 150. The HDL you can see is a little different for men and women. The blood pressure and the fasting glucose.

AgeYears Points20-34 -935-39 -440-44 045-49 350-54 655-59 860-64 1065-69 1170-74 1275-79 13
CHD RiskPoints 10-y
Risk (%)<0 <10 11 12 13 14 15 26 27 38 49 5
10 611 812 1013 1214 1615 2016 25≥17 ≥30
Systolic Blood PressureUntreated Treated
<120 0 0120-129 0 1130-139 1 2140-159 1 2≥160 2 3
HDL-C (mg/dL)Points
>60 -150-59 040-49 1<40 2
Score = 2110 y Risk >
30%
LDL-C goal:<100 mg/dL
Total Age (years)Cholesterol(mg/dL) 20-39 40-49 50-59 60-69 70-79 <160 0 0 0 0 0160-199 4 3 2 1 0200-239 7 5 3 1 0240-279 9 6 4 2 1≥280 11 8 5 3 1
Cigarette SmokingNonsmoker 0 0 0 0 0
8 5 3 1 1
Framingham Risk Calculation
3Smoker
Third Report of the National Cholesterol Education Program (NCEP) Expert Panel on Detection, Evaluation, and Treatment of High Blood Cholesterol in Adults (Adult Treatment Panel III). NIH Publication No. 02-5215, 2001.
You can see from the Framingham Risk calculation. I have simply outlined each for the variables in this patient’s case. Notice that his age falls, he gets six points. Notice his cholesterol total gets nine points. Blood pressure one. HDL he gets two. And when he’s finished in ten years, his chance of a cardiovascular event isgreater than 30%. That’s pretty high. He needs to come down – remember in the ARC trial, at the first of the conference; I’d like around a 2% for mine, not 30. So we have a long ways to go here.

Treatment Strategy
What is the initial treatment strategy to achieve an LDL-C of <100 mg/dL and reduce the 10-year-risk of CHD (43% LDL-C reduction)?
TLCImmediate drug therapy?
Which drug(s) at what dose?How long before reevaluation of drug and dose?
For treatment strategy, what is the initial treatment strategy to achieve an LDL less than 100 and reduce the ten-year risk of his coronary heart disease. Again, the tender loving care or total life style modification is important. That means he needs an exercise program, needs to lower his cholesterol levels and certainly eat less. I think probably if I had to pick one thing, I would see if this man would lose weight – with weight loss in somebody with a BMI of 30+, he will lower his blood pressure. He will lower his cholesterol, his lipids. He will be much more active and he is more likely to live a lot better life than he currently has. So weight reduction alone gets rid of the diabetes by 75%, hypertension about 70% and his cholesterol in probably 60 to 70% of people. So of all the pills I’d say, the toughest one to swallow is the most important one and that’s again, changing your lifestyle.
And in addition, the immediate drug therapy – which drugs, in which dose and what drug dose would you like – how long before reevaluation of the drug and the dose? For example, would you wait for this guy to have an event before you start him on drug therapy or would you say, you need to do lifestyle modification for six weeks and then come back, or would you say, would you like to lose ten pounds?

3 Month Follow-Up
Patient started on simvastatin 20 mgPatient lost 10 poundsLaboratory measures
TC 220 mg/dL (i13%)LDL-C 116 mg/dL (i35%)HDL-C 34 mg/dL (h6%)TG 175 mg/dL (i10%)
At the three month followup, the patient had been started on simvastatin 20. I think that’s a good idea because he is so high risk. The patient had lost ten pounds. I think that at the beginning that I’d spend a lot more time talking to this guy because if not, he will be visiting the lab. We’ll put a stent in here and there but it’s not going to take care of his entire body. This disease process of atherosclerosis in this man is largely driven by food toxicity and this guy needs to lose weight.
The laboratory measures as you can see on the slide – the total cholesterol is 220. You can see his LDL is 116. You can see his HDL is 34 and his triglycerides are 175. I am personally not happy with his LDL and I’m not happy with his HDL or his triglycerides. I think these need to be even tighter. This guy is very high risk and this guy is the one that you would see. Another thing that’s interesting, as just an anecdotal point, most cath lab tables in the United States break at about 285 pounds. This man probably would not be able to have an emergency heart catheterization if he had a heart attack.

Titration of Drug Therapy
Patient has high 10-year risk of CHD eventLDL-C goal should be between 100 mg/dL and 130 mg/dL
Recently proposed modifications to ATP III suggest treating this patient to LDL-C <100 mg/dL is a therapeutic option
Consideration should be given to coadministration therapy due to multiple lipid abnormalities
Low HDL-C Elevated LDL-CElevated TG
Titration of drug therapy. The patient has a high ten-year risk of coronary heart disease. The LDL should be less than 100 or between 100 and 130. Recently proposed modifications from ATP III suggest this patient be considered for something less than 100. Consideration should be given to a coadministration due to the again multiple lipid abnormalities he’s got. A low HDL, a high LDL, and a high triglyceride.

Case Study: Summary
Statin + EzetimibeGreatest reductions in LDL-C, TG, non-HDL-CBlood glucose reduction equal to that achieved with increased statin dose or statin + fibric acid
Statin + NiacinGreatest reduction in TG and increase in HDL-CClinical and angiographic outcomes data
Main objective is to target LDL-Cuntil goal is achieved
In case study, the statin plus ezetimibe, the greatest reduction in LDL and triglycerides and non-HDL would be seen in this patient. Certainly you can use other choices but this would be a strong consideration. Blood glucose reductions equal to that achieved with again, starting the fibrate or the statin dose would be important and again, the greater reduction in triglyceride with an increase in HDL would be seen with a statin plus niacin. Niacin certainly increases the HDL more than any other compound that we have for drugs and again, we do have clinical and angiographic outcome studies. These are probably some of the best ones done – were done by Greg Brown in the FATS trial that was published years ago but again it does tell us that we need to get to target.

http://www.nzgg.org.nz/guidelines/0035/CVD_Risk_Chart.pdf
5-year Cardiovascular Disease Risk
This last slide is not from the United States but I like it. And the reason I like it is because it gives you an understanding very quickly from an eye’s view of what’s important to decrease your cardiovascular global risk. You can take a look, for example, at a 50-year-old man. If he is a diabetic, in order to get him to the lowest category, he is going to have to be a nondiabetic. He’s going to have to lower his cholesterol and his blood pressure but you will not find that any one risk factor alone will give you as great a benefit as if you lower the global risk factors for this entire patient. That means lose weight, become a nondiabetic if possible, stop smoking, lower your cholesterol and lower your blood pressure. That probably is the bottom line. Global risk reduction will beat any one risk factor by itself.