Embed Size (px)
Citation preview

638 IEEE TRANSACTIONS ON BIOMEDICAL ENGINEERING, VOL. 43, NO. 6, JUNE 1996
Accurate Measurement of Three-Dimensional Knee Replacement Kinematics Using
Single-Plane Fluoroscopy Scott A. Banks* and W. Andrew Hodge
Abstruct- A simple extension of a previously reported object recognition technique has been used to implement a six-degree- of-freedom positiodorientation estimator for the measurement of knee replacement motion from two-dimensional (2-D) flu- oroscopic images. Computer modeling studies and controlled mechanical tests were performed to assess the accuracy of the technique. The results indicate that knee rotations can be mea- sured with an accuracy of approximately one degree and that sagittal plane translations can be measured with an accuracy of approximately 0.5 mm. The measurement technique is uniquely well suited for performing dynamic kinematic measurements on individuals with knee replacements, and for performing com- parative studies among subjects with different designs of knee replacements.
I. INTRODUCTION PPROXIMATELY 177 000 total knee replacement A (TKR) operations were performed in the United States
in 1991, a 26% increase from the number implanted in 1990 [I]. For these operations, orthopaedic surgeons chose from greater than 20 different designs of knee replacements, with most designs supporting a large number of sizes and customizing options. This very large number of surgeries and available implant designs would seem to indicate that a fundamental understanding of the design, implantation, and in vivo performance of knee replacements had been achieved. Instead, there is almost no information on the detailed in vivo mechanical performance of knee replacements. Most designs are developed based on theory and mechanical simulation studies, and the majority of objective performance data is derived from implants retrieved after clinical failure. While it is true that TKR is already an extremely effective treatment for arthritic pain and functional disability, it is generally recognized that improvements in TKR design would result in greater device longevity, expanded indications for knee replacement, and enhanced patient function following TKR.
The knee is fundamentally a mechanical linkage that ex- hibits complex motions in response to applied loads. Accurate measurements of knee replacement kinematics during func- tional activities would provide the basis for assessing the
Manuscript received June 7, 1994; revised February 6, 1996. Asterisk indicates corresponding author.
*S. A. Banks is with the Orthopaedic Research Laboratory, Good Samaritan Medical Center, PO Box 3166, West Palm Beach, FL 33402 USA (e-mail: [email protected]).
W. A. Hodge is with the Orthopaedic Research Laboratory, Good Samaritan Medical Center, West Palm Beach, FL 33402 USA.
Publisher Item Identifier S 001 8-9294(96)03991-2.
performance of current designs and for objectively designing devices with improved kinematics. Many different techniques for measuring knee kinematics have been reported. Unfortu- nately, none of these techniques appear well suited for the precise measurement of TKR kinematics. The majority of reported techniques are unable to precisely measure TKR kinematics because they rely on skin-mounted markers or fixtures for the representation of bone motion [2]-[15]. Al- though some progress has been reported in quantifying the effects of soft tissue [I 11, it remains to be seen whether accurate measurements of bone motion can be obtained us- ing skin-mounted markers. Techniques which rely on direct attachment of markers to bone, although potentially quite accurate [16], [17], cannot be considered with TKR subjects for fear of infection. In vitro knee simulation techniques have the potential for very accurate measurements of knee kinematics, but doubt exists as to whether the results bear a true resemblance to in vivo kinematics given the limited degree to which the dynamic loading environment of, and muscle action on, the knee can be replicated [18]-[27]. Progress has been made in the application of high-speed computed tomography (CT) and magnetic resonance imaging (MRI) for motion measurement [28]-[3 11, however, the capacity does not yet exist to obtain full three-dimensional (3-D) scans of an entire joint at frame rates suitable for dynamic activities. Even when CT and MRI techniques are refined to allow full- motion kinematic measurements, they will still be very difficult to use with TKR subjects because of the deleterious effects of large metal objects on both modalities. Finally, accurate measurement techniques based on radiographically tracking small markers which are implanted in bone adjacent to the joint have been demonstrated [19], [32]. However, the requirement that markers be implanted when TKR is performed severely limits the existing (and future) population of subjects suitable for study, and the technique has not yet demonstrated frame rates adequate for analysis of dynamic motions.
The purpose of this investigation was to assess the feasibility of using an X-ray fluoroscopy based technique for the mea- surement of 3-D TKR kinematics during dynamic activities. The measurement approach is based on the concept that, given the imaging geometry of the fluoroscope and the surface geometry of the prosthetic components, a computer can create an image which matches any experimentally acquired image of the knee. Since the position and orientation of the prosthetic models are known for the synthesized images, these parameters
0018-9294/96$05.00 0 1996 IEEE

BANKS AND HODGE: ACCURATE MEASUREMENT OF THREE-DIMENSIONAL KNEE REPLACEMENT KINEMATICS 639
Lateral
z
X
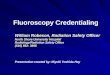
Fig. 1. spective projections.
Coordinate convention and intemal orientation parameters for per-
can be used as estimates of the physical components’ position and orientation. The direct implementation of a “model and match” technique, although quite simple, would require a tremendous amount of computational time and memory to perform the six-dimensional searches necessary to obtain 3-D kinematics. Instead, this paper reports on the extension of an efficient two-dimensional (2-D) object recognition technique into a full 3-D pose (position and orientation) estimation technique.
Section I1 of this paper presents in detail the computational and experimental methods used to implement and assess the accuracy of the positiodorientation estimation technique. Section I11 presents the accuracy results for computer model studies and for controlled in vitro studies. Section IV discusses the accuracy results and compares these results with previously reported kinematic measurement techniques.
11. METHODS
A. Overview
The kinematic measurement approach is based on imaging the knee joint as it moves, using X-ray fluoroscopy to obtain a sequence of images in which the prosthesis is projected as a 2-D perspective silhouette. These images are processed to extract the contours of the silhouette, which are compared with precomputed contours based on a precise geometric model of the prosthesis. The position and orientation of the TKR components are then estimated based on the known position and orientation of the computer model which generated the best matching contour. Since this process involves perspective projections, it is necessary to measure the imaging geometry of the fluoroscope in order to correctly generate the precom- puted contours. Fig. 1 shows the coordinate conventions for perspective imaging and defines the principal distance (Cpd), principal point, [Sz, S,], and the projection of object point ( X , Y, 2) as image point (X’ , Y’).
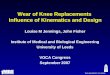
In theory, the use of a perspective imaging model has the advantage that it permits the determination of the translation of an object normal to the image plane (zooming or magnifica- tion), and in some cases permits unambiguous determination of object rotations about axes of geometric symmetry (because the projections of object features closer to the image plane appear smaller than those closer to the illumination source). However, silhouettes resulting from central projections are functions of object translations and rotations, which increases the dimensionality of the general matching problem from two degrees of freedom (DOF) for orthographic projections [33] to six DOF. By assuming that the objects’ translations normal to the image plane are limited to a small range, an approximation to perspective geometry can be made which permits full six DOF pose estimation, while requiring only two DOF shape matching. This simplifying assumption is equivalent to the assertion that the shape of an object’s silhouette is constant for a small range of translations normal to the image plane, even though the size of the silhouette will vary. Fig. 2 illustrates an example of this assumption and shows the silhouettes for an object at various distances from the image plane [Fig. 2(a)] as well as the normalized shapes of the contours [Fig. 2(b)].
Using this assumption, the development of a six-DOF model for pose estimation is straightforward. The first step is to estimate the out of plane (x- and y-axis) rotations by finding the best shape match between the unknown contour and a shape library of precomputed contours. The translations and in-plane rotations are then determined by bringing the best matched library contour into correspondence with the unknown contour.
B. Shape Representation
The 2-D object recognition technique presented by Wallace and Wintz [33] forms the basis for the shape representation and matching components of the pose estimation process. Contours are represented by normalized Fourier descriptors (NFD), where each contour is normalized for in-plane translation, in-plane rotation, and scale. NFD’s permit a very compact representation of shape information, which in turn permits fast shape comparisons and minimizes the amount of memory needed for shape libraries.
1 ) Normalized Fourier Descriptors: Given the 2-D coordi- nates of a closed contour in an image, it is possible to produce a periodic function by repeatedly tracing the contour (in the counter-clockwise direction) in equal-length increments. This periodic function can be represented by a Fourier series, the coefficients of which are called Fourier descriptors (FD’s). If the image is considered to lie in the complex plane (with the x and y coordinates representing the real and imaginary parts, respectively), then the contour can be considered a one-dimensional (1-D) complex sequence, and the FD is a 1-D complex sequence. The process of normalizing the FD effectively removes four DOF from the object silhouette, but has no effect on the shape of the contour. The normalization process used for this work is identical to that described by Wallace and Mitchell [35], and follows these steps.
a) Calculate the Fourier transform of the silhouette con- tour: Since the contour is described in terms of discrete

640 IEEE TRANSACTIONS ON BIOMEDICAL ENGINEERING, VOL. 43, NO. 6, JUNE 1996
(a) (b)
Fig. 2. component contours normalized for position and size.
(a) Femoral component model contours for object distances of 5.1, 7.6, 10.2, 12.7, and 15.2 cm from the image plane. (b) The same femoral
picture coordinates, the discrete Fourier transform (DFT) is used. The contour needs to be resampled in even length increments in order to obtain a proper Fourier transform. The contour is resampled into N = 2”(v = 1,2 ,3 , . . .) increments so that the fast Fourier transform (FFT) can be used. If s(n ) is the complex sequence representing the uniformly sampled
and the rotation property (via linearity)
s(n)ej ’ E 5 ~ ( k ) e j ’ ( 5 )
simultaneously, there are In - I1 normalizations which result in U = w = 0. The first normalization is found such that I351
silhouette contour and S ( k ) is its DFT, then [34] S( k) = S( k) e N k - K ) u + ( l -k).l/n- 1 )
N l 2 for - N / 2 + 1 L. k I N / 2 . ( 6 )
Each successive normalization is found by multiplying the previous sequence by e j ( 2 T ( k - 1 ) / l K - 1 1 ) . If n = 2, there is only one normalization. In order to compare the contour of an object at an unknown pose and a contour from the library, the contours must be normalized identically. This means that the same value of K must be used for both contours.
The only difference between the implementation for this
S ( k ) = s ( n ) e - j ( 2 W N )
n = - N / 2 + 1
for -N/2 + 1 5 k 5 N/2 N l 2
s(n) = - S ( ~ ) e j ( 2 “ ” / ” )
k = - N / 2 + 1 N
for -N/2 + 1 5 n 5 N/2. (2)
b) Normalize contour position: Set S(0) = 0. Since S(0) represents the geometric centroid of the contour, setting it to zero will give a consistent reference point independent of the position of the original contour. Save the original value of S(0) as the “position normalization constant” where the real part corresponds to the x image position, and the imaginary part the y image position.
c ) Normalize the object sizehcale:
for - N / 2 + 1 < k < N/2. (3)
This step normalizes the size of the contour, andlS(1)I is saved as the “magnitude normalization coefficient.” S( 1) is the coefficient of largest magnitude, since by definition the contour is traced in the counter-clockwise direction, and the contour is not self-intersecting [35].
d) Normalize the in-plane rotation and contour starting point: Find K such that S(n) is the coefficient of second greatest magnitude. Let U and w represent the phases of S( 1) and S(K) , respectively [35]. Using the starting point shift property of the Fourier transform
(4)
work, and that described by Wallace and Mitchell [35], is that the normalization coefficients (S(O), IS( 1) 1, and n, Onor,) are saved and used as inputs to the pose estimation process. (In order to simplify notation, S( k ) will be used in all subsequent sections to represent S( k),,,,, the contour NFD.)
2 ) Shape Library Generation: The pose estimation process is based on comparing the NFD of an input contour with the NFD of precomputed contours based on known positions and orientations of a geometric model of the prosthesis [33]. A library consists of the NFD for a particular object over a 2-D grid of viewing aspects (as if the object were at the center of a globe and each view corresponds to viewing the object along different lines of latitude and longitude). Since object position and in-plane rotation are normalized from the NFD, the library entries represent changes in the object’s rotation about axes parallel to the image plane (the x and y axes). Libraries for an object are constructed by rendering the geometric model at a fixed position and in-plane rotation, while varying the out-of- plane rotations in a systematic manner (the library is specific to particular values of the internal orientation parameters). The image containing the rendered object is processed to extract the contour of the silhouette and the NFD is determined for the contour. Each library entry includes the NFD and all of the normalization parameters for that specific contour. Since the normalization coefficient K of an input contour

BANKS AND HODGE ACCURATE MEASUREMENT OF THREE-DIMENSIONAL KNEE REPLACEMENT KINEMATICS
is not known a priori, libraries are created which contain the I K . - 11 normalizations of each contour (which satisfy U = ‘U = 0). This last point deviates from the approach of Wallace and Mitchell [35], but leads to a simpler, and possibly more robust, matching algorithm at the expense of increased memory requirements. For the femoral and tibial components used in this study, K is -1 and -2, respectively. Fig. 3 shows a small library of views for a femoral component, where each NFD was transformed back into the spatial domain for plotting (contours for K. = -1 are shown). Each contour is positioned so that its centroid is at the (z,y) location corresponding to the z and y rotations of the pose.
C. Matching/Pose Estimation Library matching is the process by which the input NFD is
compared with all of the similarly normalized library NFD’s in order to determine which library entries most closely resemble the input NFD. The measure of similarity between NFD’s is simply the Euclidean distance between the coefficient vectors. Once the closest matching library entries are identified, the pose estimation process is begun. As mentioned previously, the z and y object rotations can be taken to be those of the most similar library entry. However, this approach limits the resolution of the pose estimate to that of the library. Instead, determining the pose estimate by interpolating between several of the closest matching library entries results in a higher resolution and more accurate pose estimate without increasing the density of library views. Persoon and Fu [361 showed that “averaging the FD’s of two different shapes (frequency domain) yields a FD which will inverse transform to a shape which appears to be an “average” contour, intermediate in shape between the two original contours” [351.
The library interpolation scheme is the same as that de- scribed by Wallace and Wintz [33]. If the object viewing “space” is thought of as a Cartesian plane, with the library views representing a rectangular grid upon the plane (as in Fig. 3), then an arbitrarily oriented contour will generally fall on the plane between library entries. The goal of interpolation is to create the best matching NFD from a combination of three neighboring library entries. The first step of library
’ matching identifies the closest library entries (points on the grid) and the next step is to investigate the four triangular regions surrounding each of these entries using interpolation. Interpolation is simply a weighted average of the library NFD’s such that
3 3
S(k)est = a ,S , (k ) l ib subject t0 a, = 1 (7) i= l i=l
where
S(k)est = interpolated NFD Si (k ) l ib = library NFD
a, = positive weighting coefficient.
The goal is to find the set of positive coefficients (a’s) which minimize the differences between the input NFD, S(k) input , and the interpolated NFD, S(k),,, , given the three neighboring library entries. The optimum linear mean-square estimate of
~
641
’ the input NFD is obtained by solving the system of equations E331
M 2 M
fori={1,2}
with
D,( k ) = S, (k ) l ib -S3(k) l ib and a 3 = 1 --(Yz - a1
where M = number of NFD coefficients. An interpolated NFD estimate is obtained for all four
triangular neighborhoods surrounding the closest eight library entries. The same a’s are used to estimate z and y rotations by interpolating the (OZ, 0,) rotations of the library entries. Finally, a new set of normalization coefficients is determined by interpolation for each new NFD. The best matched contour is determined from the NFD which has the smallest Euclidean distance (fitting error) to the NFD of the unknown contour.
Library matching yields initial estimates of the z and y object rotations. The remaining translations and rotations can then be estimated by sequentially bringing the best fit NFD (and normalization coefficients) into correspondence with the input contour’s NFD using a simplified model of central projections. The sequence of pose estimates after library matching is: z-axis rotation (Oz-est), z-axis translation (Zest), z and y translation (Xest,Yest), and finally, z and y rotation correction The object in-plane rotation
can be estimated simply as the difference between the normalization angle of the best matching library contour and the normalization angle of the input contour
(9)
The z-axis translation (Zest) can be estimated by compar- ing the magnitude normalization coefficients with the simple relationship
Oz-est = oz-input - Qnorm.
where Zest Estimated z-axis position, Zlib Cpd Principal distance. Fig. 4 shows a geometric analog to (10) and the simple
relationship between the z-axis translation and the “zoom” factor of the contour.
Given the z rotation and the z translation, the z and y translations can be estimated by comparison of the position normalization coefficients and the relationship
z-axis position of object for library generation.
COS(0z-est) - sin(8z-est) sin(Qz,et) COS(Qz-est)
where Xest 3 Yest Estimated z- and y-axis translations

IEEE TRANSACTIONS ON BIOMEDICAL ENGINEERING. VOL. 43, NO. 6, JUNE 1996
-20 -10 0 10 20 X Axis Rotation (degrees)
Fig. 3. Spatial domain display of a library for a TKR femoral component. The views are over a range of f 16' about the I and y axes in 8' increments.
X i n p u t , Y&t Position normalization coefficients of in- put contour
Xinput = Re S(0) input
Knput = IWI i i S(0) input
x l i b 1 K i b Position normalization coefficients of li- brary contour
X l i b = Re s (0) lib , x i b = Im s(0) lib 0 0 Qz-est Estimated z-axis rotation. Fig. 5 shows the geometric analog to (11). The (z,y)
plane represents the image plane and the irregular figure represents the object silhouette. The measured silhouette is represented by the translated, rotated, and zoomed version of the irregular figure. The bracketed terms in (11) (from right to left) correspond to zooming the library figure into the same z-plane as the measured figure, the centroid of the library figure, rotating the library figure into alignment with the measured figure, and finally translating the library figure into correspondence with the centroid of the measured view.
Finally, the estimated 2 and y rotations need to be corrected for the effect z and y translations have on the object viewing aspect. Fig. 6 shows how translations parallel to the image plane alter the apparent angular orientation of the object (the figure shows the y-z plane, the same effect occurs in the z-z plane). The following relationship is used to correct for this effect:
- COS(Qz-est) sin(Qz-set) cos ( Qz -est ) sin ( Qz -set )
where Bz-est, Estimated z- and y-axis rotations.
Fig. 4. the relative magnitudes of the input and library contours.
Geometric equivalent of (10) for estimating object z translation from
6x-libi6y-lib Apparent z and y rotations from contour matching.
Rz-inc, Ry-inc Inclination of object with respect to princi- Dal axis. and
These simple approximations to the perspective projection allow the contour matching technique of Wallace and Wintz [33] to be applied to full six DOF pose estimation.
D. Image AcquisitiodProcessing
The video output of a fluoroscope (P1808, Precise Optics, Bay Shore, NY, 0.3 mm spot size) is recorded onto Hi-8 video tape. The video frames are digitized (752 x 480 x 24 bits) using a frame grabber board and a single frame controller. The images are converted to 8-bit gray scale and scaled to 640 x 480 square pixels.
Because timing fluctuations in tape transport can introduce image shifts, it is necessary to register sequences of images to a common reference point. This is accomplished by aligning the projections of registration markers fixed to the fluoroscope image intensifier. The position of the marker is determined for each image frame, and the average position for the sequence of images is taken to be the standard image reference position. Each image is then digitally shifted so that the marker is in the reference position.
Accurate comparisons between computer synthesized and experimentally measured contours can be made only if there is no systematic geometric distortion in the experimentally measured views. Common fluoroscope images have significant geometric distortion due to the system of phosphors and lenses employed to form the image. This distortion can be eliminated by determining the transformation between the known and measured coordinates of control points (also called reseau points), and by applying the transformation to the entire region bounded by the control points [37], [38]. The distortions are static; they only need to be measured once, and the same correction can be applied to all subsequent images. This is accomplished by imaging a rectangular grid of precisely placed markers, and by applying corrections to the resulting image so that the markers return to their known positions.
Bilinear interpolation is used for distortion correction. This approach has been used successfully for correcting distorted images from space satellites [37], [38] and medical images

BANKS AND HODGE ACCURATE MEASUREMENT OF THREE-DIMENSIONAL KNEE REPLACEMENT KINEMATICS
~
643
i Measured View
Fig. 5. pressed in (11).
Sketch representing the estimation of z and y translations as ex-
[39], [40]. The image is broken into contiguous quadrilateral regions, each bounded by four control points. The correction coefficients are determined for each sub-region, and then applied to that region, reconstructing the image in a square- by-square manner. Figs. 7 and 8 show “before” and “after” views of an image with a superimposed reseau grid.
Determination of the intemal orientation parameters is ac- complished by imaging a star shaped distribution of control points embedded in a plastic plate which is placed 30 cm from, and parallel to, the fluoroscope image intensifier. The relations between the marker positions, the image coordinates of the markers, and the internal orientation parameters are (Fig. 9)
(13)
where CP, Principal distance. b Distance between image intetlsifier and marker
plate. k Offset of principal point from coordinate origin. a,, a, Coordinates of markers on calibration grid. a;, U; Coordinates of markers in image plane. The internal orientation parameters are calculated for each
combination of markers visible in the image (typically 40 markers), and then averaged to obtain the final parameter esti- mates. A complete error analysis of the calibration procedure has been previously reported [40].
The task of extracting prosthesis boundaries from images is relatively simple since the radiopaque prostheses are normally the darkest and most well defined objects in the image (See Fig. 5). An interactive technique is used to identify and extract the boundaries of TKR silhouettes from the images. The TKR component is first identified by interactively placing (with a mouse) a bounding polygon around the entire component. A gray scale transformation is applied to the image within the polygon, such that all pixels below a certain intensity level are set to 255, and all pixels above the threshold are set to zero. The contour is identified by applying an edge detector (unsharp masking) to the binarized subimage [41]. A simple contour following routine is used to determine the sequence of (z, y) contour coordinates in the image. The threshold intensity for the gray scale transformation is adjusted interactively to
CPd
Fig. 6. object orientation, and the relationship to the true orie y-z plane).
Sketch representing the effect z and y translations have on apparent
obtain the best fitting contour around the si1 threshold intensity was used in processing all of the images for this study.
The contour described by the sequence of (z,y) image coordinates is parameterized by arc length and resampled into 128 points using tension splines [42]. The resulting contour is used for library matching and pose estimation.
E. Computer Model Studies
Computer model studies were conducted to assess the accuracy of the pose estimation technique under ideal con- ditions. A total of 100 views each were computer generated for the femoral and tibial components of a typical knee replacement (Omnifit 7000, Osteonics Corp., Allendale, NJ.). The component positions and orientations were randomly generated from a uniform distribution over the ranges
-2.5 cm < x translation < 2.5 cm -2.5 cm < y translation < 2.5 cm
7.5 cm < x translation < 12.5 cm -16.0 deg < x rotation < 16.0 deg -16.0 deg < y rotation < 16.0 deg -90.0 deg < z rotation < 90.0 deg.
The intemal orientation parameters were the same as those determined from the in vitro studies (Section 11-F). The same set of random poses was used for each object model. Pose estimates were generated using shape libraries of 21 x 21 views in 2” increments (same libraries used for in vitro matching, Section 11-F). Student’s t test was used to determine if the mean errors were significantly different from zero (Ho: E = 0; Ha: E > 0 or E < 0, where t is mean estimation error). Linear regression between object pose and estimation error was performed to determine if significant systematic error was introduced by the simplified perspective model ( g o ; = 0; Ha:,& > 0 or PI < 0, where PI is regression slope).
F. In Vitro Studies
The femoral and tibial components from a knee replacement (Omnifit 7000, Osteonics Corp., Allendale, NJ.) were installed

644 IEEE TRANSACTIONS ON BIOMEDICAL ENGINEERING, VOL. 43, NO. 6, JUNE 1996
I I 1 1 I I
I I I I I Fig 7 Raw fluoroscope image showing geometnc distortion. Image contains projections of the femoral (top) and tibial (bottom) knee components, and the reseau grid is superimposed
in artificial bones and the “joint” was rigidly fixed. The speci- men was mounted to the actuator of a two axis servohydraulic system (model 8521, Instron Corp., Canton, MA) which was calibrated to ASTM standards E74 and E4 [43], with linear accuracy of 0.5 mm and rotary accuracy of 1 .O”. The specimen was rotated about the y axis of the actuator (corresponding to internal/external rotation of the knee) over a range of f 1 6 ” in 2” increments. The specimen was also translated along the y axis of the actuator over a range of f 1 0 mm in 5-mm
position. Fluoroscope images were acquired and processed as explained above, and pose estimates were generated using
Fig. 8. Geometry corrected image with corrected reseau grid superimposed.
increments, and the sequence of rotations were repeated at each I J origin
shape libraries of 21 21 views in 20 increments (f20 degree Fig. 9. geometry for a sing1e pair Of InarkerS.
range for both rotations). An accurately measured frame of reference was not avail-
able for the position and orientation of the hydraulic actuator relative to the fluoroscope, or for the components relative to the actuator. This required estimation of the relative posi- tiodorientation of the rotational axis and the fluoroscope, and the components relative to the actuator, in order to assess the accuracy of the prosthesis pose estimates. The transformation of coordinate frames from the fluoroscope to the prosthesis can be modeled as
globalA - global *machine prosthesis - Amachine Aaxis
(15)
where each A is a 4 x 4 homogeneous transformation matrix and
globalA =transformation from global coordinate system to prosthesis coordinate system. These are the rotations and translations that are estimated by the contour matching system (dependent variables).
= transformation from the global coordinate system to the lineadrotary axis of the hydraulic actuator (estimated).
*axis Aprost hesis
globalA
machine Aaxis = transformation representing rotations and translations of the actuator relative to the fixed machine frame of reference. This transformation consists of a pure rotation about, and a pure translation along, the y axis of the actuator. These rotations and translations are the independent variables for the experiments.
axis Aprosthesis = transformation from the actuator to the prosthesis. The “knee” was approximately aligned with the machine axes, but devi- ations of several degrees from a neutral alignment can be reasonably expected.
Both globalAmachine and axis Aprosthesis were estimated to establish a standard for comparison with the contour matching based pose estimates. globalAmachine was approximated by determining the global orientation of the average finite helical axis for the estimated object positions/orientations [44]. The rotations in axisAprost~es~s were approximated by comparing the results of the model (15) with the contour matching based results and by iteratively varying the three static rotations until the average difference was zero for all three rotations. The radial offsets of the components relative to the axis of rotation

BANKS AND HODGE ACCURATE MEASUREMENT OF THREE-DIMENSIONAL KNEE REPLACEMENT KINEMATICS
X translation error (mm) Y translation emor (mm) Z translation error (mm)
X rotation emr (deg)
2 rotation error (deg) Y rotation emr (deg)
-
645
(99 view) (sskews) -0.073 f 0.136' -0.072 f 0.1281 -0.036 f 0.122' -0.050 i 0.1 15' 0.021 f 1.395 0.870 1.552l -0.033 f 0.230 0.024 0.394
0.023 f 0.343 0.015 f 0.333 0.006 f 0.251 -0.040 0.313 - ~ _ _ . - ~ - - . _ _
TABLE I AVERAGE ESTIMATION ERRORS FOR COMPUTER MODEL STUDIES OF Two KNEE PROSTHESIS COMPONENTS
(IhDICATES THAT MEAN ERROR IS SIGNIFICANTLY D m m r FROM ZERO WITH P = 0.005)
I I Femoral component model I Tibial cornwnent model 1
were estimated first by assuming that the arc length traveled by the components from frame to frame was constant, and then these estimates were iteratively refined until the average differences between the pose estimates and the model (15) were zero. This estimation procedure assumes that the errors in pose estimation are unbiased.
Comparing the modeled orientations with the contour matching estimates will result in conservative error estimates. Any errors in estimating either globalAmachine or axisAprosthesis will result in a less accurate model, causing the error estimates to increase relative to their actual values. This process of determining the accuracy of the estimated pose relative to a modeled pose forces mean errors to zero, so that the measure of the average deviation between experiment. and model is the standard deviation of the error, hereafter referred to as the standard error.
111. RESULTS
A. Computer Model Studies
The results for the computer model studies are summarized in Table I. The data in Table I reflect estimation results for 99 of the randomly generated femoral views and 98 of the tibial views. One of the femoral pose estimates and two of the tibial pose estimates had large angle and position errors, and indicated clear blunders in library matching. Fig. 10 shows the normalized tibial contour with the best matching results [Fig. 10 (a)], as well as the three normalized contours with the worst matching results [Fig. tO(b)-(d)]. The estimates for contour [Fig. 10(b)] were in error by 2.1" and 2.36 cm for the z-axis translation. The estimates for contour Fig. 1O(c) were in error by 28.4' for the y-axis rotation (17.0' estimated, -11.4' actual) and 2.42 cm for the z-axis translation. The estimates for contour [Fig. 10(d)] were in error by 8.3' for the z-axis rotation (-2.6' estimated, 5.7' actual) and 1.94 cm for the z- axis translation. These three contours [Fig. 10(b)-(d)] had the largest contour fitting errors for the 100 trials with each model. This magnitude of error would presumably be detected in any data set and the estimates discarded for that frame of data.
The average errors in angular estimates were not signif- icantly different from zero ( p = 0.1). The average errors for 2- and y-axis positions were significantly different from zero ( p = 0.005) with an average bias of -55 pm. The average errors for z-axis position estimates were unbiased for the femoral component, but had a bias of 0.87 mm for the tibial component ( p = 0.005).
Fig. 10. Computer generated contours (solid line) with contours from library matching (dashed line). A well matched tibial contour is shown in (a). Matching blunders are shown in (b), (c), and (d).
Regression analysis revealed no significant relationships between femoral component position and estimation error ( p = 0.l), while the tibial component z position error was signifi- cantly related to the component II: position ( p = 0.01). There were also significant relationships between object orientation and estimation error for both components. Table I1 shows the slope of the linear regression line relating object pose and estimation error for cases where a significant relationship exists. In general, errors in the estimated z and y positions were significantly related to the object z-axis rotation, with a ratio of position error to z rotation of approximately 0.1%.
B. In Vitro Studies
Pose estimation errors for the in vitro studies are based on the average deviations of the experimental data from the model of (15). One frame of tibial data and one frame of femoral data exhibited clear blunders in pose estimation and were replaced by linearly interpolating from the two adjacent frames of data. Table 111 gives the standard errors for pose estimation based on comparison with the model for 85 frames of data.
The two components of the knee replacement were fixed with respect to each other and moved as a single unit through- out the tests. An alternative method for assessing the accuracy

646 IEEE TRANSACTIONS ON BIOMEDICAL ENGINEERING, VOL. 43, NO. 6, JUNE 1996
TABLE I1 SLOPES OF REGRESSION LINES RELATING OBJECT POSITION AND ORIENTATION WITH POSE ESTIMATION ERRORS. (TWO-TAILED STUDENTS &TEST AGAINST THE
NULL HYPOTHESIS THAT THE REGRESSION SLOPES WERE ZERO, p = 0.01. NS INDICATES NOT STATISTICALLY SIGNIFICANT WITH p = 0.01)
TABLE 111 STANDARD ERRORS FOR IN VITRO STUDIES OF Two KNEE PROSTHESIS COMFQNENTS (COLUMNS 1-3). COLUMN 4 SHOWS THE AVERAGE RESULTS FROM T
of the estimation technique is to consider any relative motions measured between the two components as estimation error. The third column of Table 111 shows the standard deviation (error) of relative motions between the two components.
IV. DISCUSSION The results of both the computer modeling and in vitro
studies are consistent with an intuitive understanding of per- spective projections. Object motions parallel to the image plane are effectively magnified by the object’s position relative to the illumination source, while object motions perpendicular to the image plane are manifest primarily as changes in silhouette size. Measurements of motion parallel to the image plane should be more accurate than measurements of motion perpendicular to the image plane, and the study results show standard errors approximately ten times smaller for motion parallel to the image plane. Similarly, accuracy in angular measurements should be best when the amount of silhouette shape change per unit rotation is greatest. In-plane (z-axis) rotations have a direct effect on the silhouette orientation and should be measured quite accurately, although there will be a decrement in accuracy with objects whose silhouettes change dramatically with out of plane rotations. Out-of-plane (x- and y-axis) rotations are manifest as changes in silhouette shape, so that measurement accuracy is strongly affected by the shape of the object. For both computer modeling and in vitro studies, the standard errors for out-of-plane rotations were smaller for the femoral component, while the standard errors for in-plane rotations were smaller for the tibial component.
The computer modeling results demonstrated that, under ideal conditions, extremely accurate estimates of position and orientation can be obtained (Table I). The standard errors for translations parallel to the image plane averaged approximately 0.2 mm or 0.4% of the range of translations studied. The standard errors for translations perpendicular to the image
plane averaged approximately 2.0 mm or 2.0% of the range of translations studied (0.2% of the principal distance). The translation results for both components were similar, indicating that object shape does not have a significant effect on position measurement accuracy.
The measurement bias for translations parallel to the image arises from the approximate nature of the perspective model. A more accurate measurement could be obtained by taking the initial pose estimate, creating a small library of views for incremental rotations from that pose, and then matching the unknown contour with the new library. Given the small magnitude of the bias (55 pm), it is not clear that the additional computational time and complexity of this approach is warranted. Similarly, the correlations between object pose and estimation error result from the approximate nature of the perspective model. It is somewhat surprising that the magnitude of the relations are only 0.1%-1.0%!
The standard errors for x- and y-axis rotations were smaller for the femoral component than the tibial component, while the standard error for z-axis rotations were smaller for the tibial component. These results are consistent with the shapes of the respective components; the femoral component has a much more complex shape so small out of plane rotations result in large changes of the shape of the projected silhouette. The tibial component has a simpler shape, which is symmetric with respect to its mid x-y (sagittal) plane, and out-of-plane rotations have a much more subtle effect on the projected silhouette. The fact that out-of-plane tibial rotations have a smaller effect on the projected silhouette results in smaller errors for in-plane rotation estimates.
One of the femoral and two of the tibial estimates for the computer model studies, and one frame each for the in vitro studies exhibited obvious blunders in pose estimation. In these instances the magnitude of angular error was greater than several degrees, and the z-axis position errors and contour fitting errors were large. Two distinct types of blunders were

BANKS AND HODGE ACCURATE MEASUREMENT OF THREE-DIMENSIONAL KNEE REPLACEMENT KINEMATICS 641
TABLE IV TABLE COMPARING AVERAGE ACCURACY FIGURES FROM COMPUTER MODELJNG AND IN VITRO !;TUDES WITH .4CcuRACY FIGURES REPORTED IN THE LITERATURE
FOR KINEMATIC MEASLIREMENT SYSTEMS. ONLY THE IMAGE-BASED POSE ESTIMATES AND THE X-RAY sTEREOPHOTOGRAMMETRIC MEASUREMENTS
FIXTURE MOTION; THEREFORE THE ACCURACY FIGURES ARE LOWER BOUNDS FOR THE MEASUREMENT ERROR OF BONEPROSTHESIS MOTION PROVIDE A DIRECT MEASUREMENT OF BO~WFROSTHESIS MOTION. ALL OTHER LISTED TECHNIQUES DETECT SKIN-MOUNTED MARKER OR
observed. First, for the blunders observed in vitro, in Fig. 10(b) and in Fig. 1O(c), the object was in neutral rotation about the object’s z axis, while having a large rotation about the y axis. This type of orientation results in relatively ambiguous silhouettes when the objects are symmetric with respect to the z-y (sagittal) plane, such that rotations of (0,e) about the z and y axes can generate silhouettes very similar to those arising from rotations of (0, -6). The second type of blunder, as shown in Fig. 10(d), occurred when the object in-plane rotation was near 90’. In this case the simplified perspective model is inadequate to account for the perspective distortions resulting from in-plane translations and rotations (it is interesting to note that the eighth best library match would have resulted in an accurate pose estimate). In practice, blunders are easily detected from large fitting errors and discontinuities in the frame-to-frame parameter estimates.
The standard errors for the in vitro studies were an average of three times greater than the standard errors for the com- puter modeling studies. Possible sources contributing to the increased errors include: errors in the servo-hydraulic position- ing system, residual geometric distortions, errors in identifying the silhouette boundaries in the images, errors in the internal orientation parameters, and errors in estimating the parameters of the reference model (15). The rotational accuracy of the servo hydraulic system was verified against a manual precision rotational stage (Model 30008-P, Daedal Inc., Harrison City, PA) and was found to exhibit standard errors of 0.16’ over the range from f61” . Based on the 9 x 9 reseau grid and bilinear correction, the average residual geometric distortion in the image is approximately two pixels or roughly 1% of the size of the projected silhouettes [40]. There is an almost linear relationship between errors in the internal orientation parameters and the average errors in position and orientation estimates, i.e., the measures become biased [40]. However, for the average errors in estimating the internal orientation parameters the resulting bias in orientation estimates will be approximately 0.1 O . The position measurement bias introduced
by errors in the internal orientation parameters will directly affect the estimated position of the prosthetic components, but will have a very small effect on the measurement of relative motions between the two components of a knee replacement. Errors in estimating the parameters of the reference model (15) will also have a direct effect on the assessed accuracy of the measurement technique, resulting in error estimates which are conservative.
The in vitro results show errors in z-axis rotations to be smaller than the errors for y-axis rotations, while the computer simulation studies showed similar errors for both rotations. This is almost certainly due to the fact that only y-axis rotations were investigated for the in vitro studies, and that the range of resulting z-axis rotations was very small. It is reasonable to assume that the errors for z-axis rotations will be larger when a larger range of z-axis rotations occurs, and that the errors should be similar to those found for the y-axis rotations.
The accuracy of measuring z-axis translations is poor rela- tive to the accuracy in measuring z - and y-axis translations. Fortunately, this does not present a major problem for the measurement of knee motions because the ligaments of the knee and the design of the articular surfaces of knee re- placements significantly constrain motions along the z axis (mediaVlateral), limiting them to very small translations. By assuming that z-axis translations between the femoral and tibial components are zero, the resulting “measurement” errors will be in the range of several millimeters, and will be smaller than the errors resulting from the image-based estimate of relative motions.
The standard errors for relative motions between the two components were smaller than the sum of the individual errors in locating each component. This implies that the errors are correlated, indicating some systematic measurement error. Since knee kinematic measurements are always performed by relating one component (or bone) to another, these systematic effects can be negated to a certain extent. Thus the sum of

648 IEEE TRANSACTIONS ON BIOMEDICAL ENGINEERING, VOL. 43, NO. 6, JUNE 1996
errors in locating the individual components can serve as a reasonable upper bound for the errors in measuring the relative motion between the components.
Table IV compares the accuracy results for the image-based measurement technique with a variety of other systems for measuring knee kinematics. In general the accuracy results for the image-based technique are in the range of reported accuracies for the other techniques. The key advantage to the image-based technique is that it is a direct measurement of dynamic prosthetic motion, while the other techniques all involve an indirect measurement. All of the techniques in Table IV, except the image-based technique and the X-ray stereophotogrammetric technique, are based on measuring the motions of a fixture or set of markers which are externally mounted to the leg. These techniques very accurately measure the motions of the fixture or markers, but cannot eliminate errors caused by relative motion between the markers and bone, or the errors introduced in transforming marker kinemat- ics into bone kinematics. When these issues are considered, the actual accuracy of these techniques for measuring bone or prosthesis motion is much poorer, and the image-based technique has superior accuracy. X-ray stereophoto-grammetry can be used to perform extremely accurate measurements of joint position, but has not yet been used to perform truly dynamic measurements of knee motion.
The image-based measurement technique appears uniquely well suited for performing accurate measurements of knee prosthesis kinematics during dynamic activities. The infor- mation gained from the study of prosthetic kinematics will dramatically increase the understanding of how these devices are functioning in vivo, and will permit quantitative functional comparisons between different prosthetic designs. Quantitative comparison data will permit the design of improved devices based on positive performance and measured mechanics, rather than design based on compensation for observed clinical failures.
ACKNOWLEDGMENT
The authors would like to acknowledge the research support of The Biomotion Foundation and Good Samaritan Medical Center, and Osteonics Corporation for providing the surface models of the prosthetic components.
REFERENCES
[ 11 National Hospital Discharge Survey, National Center for Health Statis- tics, 1991.
[2] K. N. An, M. C. Jacobsen, L. J. Berglund, and E. Y. S. Chao, “Application of magnetic tracking device to kinesiologic studies,” J. Biomech., vol. 21, pp. 613-620, 1988.
[3] T. P. Andriacchi, J. Galante, and A. W. Fermier, “The influence of total knee-replacement design on walking and stair-climbing,” J. Bone Joint Surg., vol. 64A, pp. 1328-1335, 1982.
[4] E. K. Antonsson and R. W. Mann, “Automatic 6-DOF kinematic trajectory acquisition and analysis,” J. Dyn. Sys. Meas. Cont., vol. 1 1 I , pp. 31-39, 1989.
(51 E. Y. S. Chao, “Justification of triaxial goniometer for the measurement of joint rotation,” J. Biomech., vol. 13, pp. 989-1006, 1980.
[6] R. A. Hart, C. D. Mote, and H. B. Skinner, “3-D description of the motion of human knee using the finite helical axis,” Trans. Orrhop. Res. Soc., pp. 200, 1989.
171 J. Isacson, L. Gransberg, and E. Knutsson, “Three-dimensional electro- goniometric gait recording,” J. Biomech., vol. 19, pp. 627-635, 1986.
[8] M. P. Kadaba, H. K. Ramakrishnan, M. E. Wootten, J. Gainey, J. Gorton, and G. V. B. Cochran, “Repeatability of kinematic, kinetic, and electromyographic data in normal adult gait,” J. Orthop. Res., vol. 7, pp. 849-860, 1989.
[9] M. P. Kadaba, H. K. Ramakrishnan, and M. E. Wootten, “Measurement of lower extremity kinematics during level walking,” J. Orthop. Res.,
[lo] 2. Ladin and G. E. Wu, “Combining position and acceleration measure- ments for joint force estimation,” J. Biomech., vol. 24, pp. 1173-1 187, 1991.
[ l l ] B. El Nahass, M. M. Madson, and P. S. Walker, “Motion of the knee after condylar resurfacing-An in vivo study,” J. Biomech., vol. 24, pp. 1107-1117, 1991.
[I21 P. 0. Riley, R. W. Mann, and W. A. Hodge, “Modeling of the hiome- chanics of posture and balance,” J. Biomech., vol. 23, pp. 503-506, 1990.
[13] A. Stein, B. Fleming, M. H. Pope, and J. G. Howe, “Total knee arthroplasty kinematics: An in vivo evaluation of four different designs,” J. Arthroplasty, vol. 21, pp. 31-36, 1988.
141 W. J. Suntay, E. S. Grood, M. S. Hetzy, D. L. Butler, and F. R. Noyes, “Error analysis of a system for measuring three-dimensional joint motion,” J. Biomech. Eng., vol. 105, pp. 127-135, 1983.
151 M. C. Verstraete and R. W. Soutas-Little, “A method for computing the three-dimensional angular velocity and acceleration of a body segment from three-dimensional position data,” J. Biomech. Eng., vol. 112, pp. 114-118, 1990.
161 M. A. Lafortune and P. R. Cavanagh, “The measurement of normal knee joint motion during walking using intracortical pins,” in Biomechanical Measurements in Orthopaedic Practice, M. Whittle, D. Harris, ed. Oxford, U.K.: Clarendon, 1985, pp. 234-243.
[17] M. C. Murphy, B. Zarins, M. Jasty, and R. W. Mann, “In vivo measurement of the three dimensional skeletal motion at the normal knee,” Trans. Orthop. Res. Soc., pp. 142, 1985.
[I81 T. P. Andriacchi, T. S. Stanwyck, and J. 0. Galante, “Knee biomechan- ics and total knee replacement,” J. Arthroplasty, vol. 1, pp. 21 1-219, 1986.
[19] L. Blankevoort, R. Huiskes, and A. DeLange, “The envelope of passive knee joint motion,” J. Biomech., vol. 21, pp. 705-720, 1988.
[20] S. S. Blick, D. M. Daniel, J. Davis, L. Fochte, and K. Foreman, “Kinematics of the quadriceps stabilized anterior cruciate disrupted knee,” Trans. Orthop. Res. Soc., pp. 25, 1989.
[21] A. E. Engin and M. S. Korde, “Biomechanics of normal and abnormal knee joint,” J. Biomech., vol. 7, pp. 325-334, 1974.
[22] E. S. Grood, S. F. Stowers, and F. R. Noyes, “Limits of movement in the human knee,” J. Bone Joint Surg., vol. 70A, pp. 88-97, 1988.
[23] R. L. Horwood, E. N. Biden, and L. M. Focht, “The role of the posterior cruciate ligament in the kinematics of total knee arthroplasty,” Trans. Orthop. Res. Soc., pp. 360, 1988.
[24] I. M. Levy, P. A. Torzilli, J. D. Gould, and R. F. Warren, “The effect of lateral menisectomy on motion of the knee,” J. Bone and Joint Surg., vol. 71A, pp. 401-406, 1989.
[25] J. J. O’Connor, J. W. Goodfellow, and J. A. Bradley, “Quadriceps forces following meniscal knee arthroplasty-An in vitro study,” Trans. Orrhop. Res. Soc., pp. 357, 1988.
[26] R. L. Piziali, J. Rastegar, D. A. Nagel, and D. J. Schurman, “The contri- bution of the cruciate ligaments to the load-displacement characteristics of the human knee joint,” J. Biomech. Eng., vol. 102, pp. 277-283, 1980.
[27] J. A. Sidles, R. V. Larson, J. L. Garbini, and D. J. Downey, F. A. Matsen, “Ligament length relationships in the moving knee,” J. Orthop. Res., vol. 6, pp. 593-610, 1988.
[28] S. F. Dye, L. G. Shapero, M. J. Lipton, and E. G. Glavin, “Quantitative assessment of functional knee morphology by means of cine computed tomography,” Trans. Orthop. Res. Soc., pp. 201, 1987.
[29] M. K. Stehling, R. Turner, and P. Mansfield, “Echo-Planar imaging: Magnetic resonance imagine. in a fraction of a second.” Sci.. vol. 254.
vol. 8, pp. 383-392, 1990.
pp.43-49, 1991. 1301 W. 0. Thomuson. F. L. Thaete. F. H. Fu. and S. F. Dve. “Tibial meniscal < . - .
dynamics using three-dimensional reconstruction of magnetic resonance images,” Am. J. Sporrs Med., vol. 19, pp. 21C216, 1991.
[31] H. J. Woltring, P. V. Roy, M. Hebbelinck, M. Osteaux, and L. Ver- bruggen, “3-D knee joint kinematics by magnetic resonance imaging,” J. Biomech., vol. 23, pp. 384, 1990.
[32] K. G. Nilsson, J. Karrholm, and L. Ekelund, “Knee motion in total knee arthroplasty,” Clin. Orthop., vol. 256, pp. 147-161, 1990.
[33] T. P. Wallace and P. A. Wintz, “An efficient three-dimensional aircraft recongnition algorithm using normalized Fourier descriptors,” Comput. Graphics Image Processing, vol. 13, pp. 99-126, 1980.

649 BANKS AND HODGE ACCURATE MEASUREMENT OF THREE-DIMENSIONAL KNEE EPLACBMENT KINEMATICS
A, V. Oppenheim and A. S. Willsky, Signals and Systems. Englewood Cliffs, NJ: Prentice-Hall, Inc., 1983. T. P. Wallace and 0. R. Mitchell, “Analysis of three-dimensional movement using Fourier descriptors,” ZEEE Trans. Pat. Anal. Mach. Intel., vol. PAMI-2, pp. 583-588, 1980. E. Persoon and K. S. Fu, “Sequential decision procedures with prespec- ified error probabilities and their applications,” Sch. Elect. Eng., Purdue Univ., Tech. Rep. TR-EE 74-30, 1974. W. B. Green, Digital Image Processing: A Systems Approach. New York Van Nostrand Reinhold, 1989. D. A. O’Handlev and W. B. Green, “Recent developments in digital - - image processing at the image processing laboratory at the Jet Propulsion Laboratory,” Proc. IEEE, vol. 60, pp. 821-828, 1972.
[39] C. K. Cheng, N. K. Yao, and H. C. Liu, “Computer surgery simulation and its biomechanical evaluation of the anterior displacement of the tibial tubercle,” Trans. Orthop. Res. Soc., pp. 476, 1992.
[40] S. A. Banks, “Model based 3-D kinematic estimation from 2-D per- spective silhouettes: application with total knee prostheses,” Ph.D. dissertation, Massachusetts Institute of Technology, Cambridge, MA, 1992.
[41] J. S. Lim, Two-Dimensional Signal and Image Processing. Englewood Cliffs, NJ: Prentice-Hall, Inc., 1990.
1421 PV-WAVE v4.0 Command Language Reference, Precision Visuals, Inc., . . - - Boulder, Colorado, 1992.
[43] Annual Book of ASTM Standards. Philadelphia: Am. Soc. Testing and Materials, 1992, vol. 3.01.
1441 P. 0. Rilev. R. S. Fiian. W. A. Hodge, and R. W. Mann, “Determination . - I
of joint centers for posture studies,” in Biomechanics of Normal and Prosthetic Gait, J. L. Stein, Ed. Boston: ASME Press, 1987, pp. 131-136.
Scott A. Banks received the BSc. and M.Sc. de- grees in biomedical engineering from Case Western Reserve University, Cleveland, OH, and the Ph.D. in mechanical engineering from MIT, Cambridge, MA.
Since 1992, he has been the Technical Director of the Orthopaedic Research Laboratory, Good Samar- itan Medical Center, West Palm Beach, FL. Hls research interests are in the biomechanics of human motion, evaluation and design of joint replacements, injury mechanisms in sports, and applications of
image analysis for motion measurement. Dr. Banks is a member of the American Society for Biomechanics, the
American Society for Testing and Materials, the Society for Biomaterials, and Sigma Xi.
W. Andrew Hodge received the BSc. degree in aeronautical engineering from the University of Illinois, Urbana, and the M.D. degree from Rush Medical College, Chicago, IL.
He trained in orthopaedic surgery at Rush- Presbyterian-St. Luke’s Medical Center, Chicago, IL, and completed a clinical fellowship in joint replacement surgery at Haward’s Massachusetts General Hospital, Boston, MA, and a research fellowship in orthopaedic biomechanics at MIT. While in Boston, he served as co-director of the
HarvardMIT Rehabilitation Engineering Center, and as Medical Director of the Biomotion Laboratory at Massachusetts General Hospital. He is currently the Medical Director of the Orthopaedic Research Laboratory, Good Samaritan Medical Center, West Palm Beach, FL. His research interests concentrate on developing new surgical techniques and improving joint implant design and function.
Dr. Hodge serves on the Committee on Bioengineering of the American Academy of Orthopaedic Surgery, is a fellow in both the American College of Surgeons and the American Academy of Orthopaedic Surgery, and is a member of lhe Associatlon of Bone and Joint Surgeons, the Orthopaedic Research Society, and the American Society of Biomechanics.








![The Kinematic Alignment 16 Technique for Total Knee ... · 177 non-physiological knee ligament laxities and residual instability [11, 15] and abnormal 10, knee kinematics [1316, ,](https://img.pdfslide.us/doc/110x75/60bbb243c19342776239ee29/the-kinematic-alignment-16-technique-for-total-knee-177-non-physiological-knee.jpg)