Embed Size (px)
Citation preview

JCN 2017, Vol 31, No 2 25
WOUND CARE
With wound care currently calculated to cost the NHS £5.3 billion per year (Guest
et al, 2015), and the importance of carrying out comprehensive wound assessment should not be underestimated, as it is key to establishing a differential diagnosis and enables clinicians to set patient agreed goals of care. Community nurses should therefore be skilled and competent to complete wound assessments, which should not be performed in isolation, as many patient-related factors affect the healing process. These are grouped into intrinsic, extrinsic and environmental factors. Successful management relies on identification and management of these factors, alongside managing the wound, using a triumvirate approach as shown in Figure 1.
Accurate chronic wound assessment in the community setting
The acronym Heidi (Figure 2) provides a framework for structured assessment, diagnosis and management of wounds (Heinrichs et al, 2005). HISTORY-TAKING
It is important to step away from the wound and look at the person behind it. A complete medical history helps to establish comorbidities that have contributed to wound aetiology, and those that may affect healing. It is essential to establish the ‘healability’ before setting goals to ensure that these are achievable. As a minimum, community nurses should consider; Wound trigger — surgical,
trauma, pressure, infection, oedema, previous treatments
Medical background, e.g. cardiovascular disease or diabetes, as these factors may affect blood flow to the wound
Factors that may negatively impact ‘healability’, such as age, smoking, anaemia, concordance,
incontinence, immobility, pain Nutritional status — nutrition
has been linked to impaired wound healing (Australian Wound Management Association, 2009)
Socioeconomic status, including environmental factors, such as cluttered houses, pets, and inability to work leading to financial difficulties
Psychological status, cognitive impairment and stress.
Evaluation needs an accurate and appropriate baseline from which to measure. It is important to look at and listen to the patient, paying attention to the factors that affect wound healing. Family history may be significant in leg ulceration or suspected malignant wounds, or undiagnosed diabetes.
Successful outcomes depend on balancing knowledge of wound healing and matching product attributes and choices to expedite the natural healing process or correct imbalances that lead to chronicity.
Sometimes, for example in the case of pressure ulcers/diabetic foot wounds, it is also about engaging the patient with offloading.
EXAMINATION OF THE WOUND It is essential that wound documentation allows easy description of the wound in words. Assessment must include as a minimum; the wound location, size, shape, depth, tissue types in the wound and at the wound edge and in the periwound area, presence of any undermining, functional disturbance, odour, heat and exudate volume. It is important to ask if the history matches the wound. Failure to identify and treat
Jeanette Milne, clinical lead tissue viability, Northumbria Healthcare NHS Foundation Trust
The community nurse may come across a range of wounds in the community setting, particularly with the rise in comorbidities such as diabetes and cardiovascular disease due to unhealthy lifestyles and an ageing population. Accurate assessment is the key to identifying the most appropriate wound treatment programme; one that will promote healing and/or relieve symptoms associated with chronic wound healing. Product choice is secondary to getting the assessment process right and accurate assessment and methodical documentation not only help protect against legal challenges, but also aim to reduce waste, dressing change frequency (and thereby nurse time), and patient discomfort. The community nurse should always seek to match their wound-healing knowledge with what they see in the wound bed and the patient’s history, which in turn will enable the nurse to make informed therapy choices and provide expert patient advice.
KEYWORDS: Wounds Chronic wounds Assessment Diagnosis
Jeanette Milne
Wounds - Milne - read by ???.indd 25 23/03/2017 11:15
© 2017
Wou
nd C
are Peo
ple Lt
d

26 JCN 2017, Vol 31, No 2
WOUND CARE
the underlying cause is the main reason for failure of wounds to heal (Eagle, 2009).
Frameworks aid documentation by encouraging consistency. One example is the T.I.M.E (Shultz et al, 2003) acronym, which represents:
Tissue typeInfection or inflammationMoistureEdge or epidermal advancement.
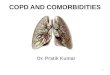
Advanced Wound Management (AWM) (Gray et al, 2005) is another method of wound assessment and documentation to help clinical decision-making, which uses three continuums related to wound parameters — tissue type, infection and exudate (see examples in Figures 3 and 4).
Whichever method of assessment is used, it is essential to differentiate between inflammation and infection. The inflammatory stage of wound healing lasts 3–5 days post wounding in acute wounds (Timmons, 2006). Neutrophil extravasation in the inflammatory phase of wound healing makes capillaries dilate to allow white cells to remove debris by phagocytosis. The permeability of capillaries produces exudate.
However, in normal circumstances this should start to reduce in numbers after about three days. Conversely, if bacterial counts are high, more white cell are needed which leads to more inflammation and more exudate. However, chronic wounds (those with an underlying pathophysiology) have high levels of unregulated
inflammatory mediators; which is linked with chronicity (Romanelli et al, 2016). Signs of infection to look out for include:
Redness (erythema) extending 2–3cm outside wound marginsHeat (+ or – swelling/oedema)OdourPainIncreasing exudate — change in colour, viscosity and typeDelayed healing or wound breakdownWound bed discolouration/granulation tissue which bleeds easilyPocketing at the base of the wound (World Union of Wound Healing Societies [WUWHS], 2008).
It is important to remember that different microorganisms can exist in polymicrobial communities and this is often the case within the margins of a wound. In relation to exudate, clear/straw-coloured exudate may be normal, but it could also be urine or lymph fluid. Gold-coloured exudate could indicate a Staphylococcus aureus colonisation or infection, while green/blue exudate can indicate Pseudomonas aeruginosaas the suspected pathogen (Romanelli et al, 2010).
Establishing wound size is also an important parameter on which success is measured — this should include width, length and depth of the wound and be recorded at initial presentation and each assessment thereafter. In addition, obtaining images of the wound with a camera following written consent can help to monitor progress.
INVESTIGATIONS
Any investigations should be proportionate to the past medical history and in keeping with clinical signs and symptoms, and should seek to inform and aid diagnosis. Depending on the type of wound, investigations may include:
Blood tests, full blood count (FBC) to exclude anaemia, international normalised ratio (INR) if bleeding, erythrocyte sedimentation rate (ESR), C-reactive protein
(CRP), electrolytes, lipids, haemoglobin A1c (HbA1c), mineral deficiencies and hypoalbuminemia can contribute to oedema formationWound swabs should only be taken if the patient is clinically symptomatic and the healthcare professional intends to treat the patient with antibiotics. Local symptoms of infection should be addressed with topical antimicrobial agents. If the wound fails to respond to antimicrobials, it can be helpful to consider looking for specific pathogens, as this can allow for a more targeted approach to specifically address the bioburden that is present in the wound and surrounding tissues. If there is any doubt about the type of specimen to send to the laboratory, contact the local microbiologist for advice. For example, in patients with repeated lower limb cellulitis, sending nail clippings to the laboratory to rule out fungal infection as the causative organism is often warrantedIf a patient’s wound is failing to progress or has a suspicious appearance, they should be referred to dermatology to obtain a tissue sample for histology to rule out malignancy and/or rarer immune diseases that lead to chronic wound development.
Figure 1.A triumvirate approach to wound assessment.
Figure 2.The acronym Heidi provides a framework for structured assessment, diagnosis and management (Heinrichs, 2005).
Formulatinga plan of
care
Diagnosis:establishing underlying
pathophysiology
Addressingpatient-centred
concerns
Identify reasonsfor non-healing
Interventions Examination
History
InvestigationsDiagnosis
Wounds - Milne - read by ???.indd 26 23/03/2017 11:15
© 2017
Wou
nd C
are Peo
ple Lt
d

E X I T
NOW AT THE HEART OF BSN MEDICAL’S INTEGRATED THERAPY SOLUTIONS
SAME TRUSTED QUALITYSAME CLINICALLY PROVEN EXCELLENCE
JUST A NEW NAME
For more information, please contact our Concierge Team on:Tel: 01482 670177 Email: [email protected]
Closing wounds. Together.
Cutimed® Sorbion®
BSN medical UK
PO Box 258 • WillerbyHull • HU10 6WT
www.bsnmedical.co.ukTel: 01482 670100 • Fax: 01482 670111E-mail: [email protected] 1968/317
170001175 - Cutimed Sorbion JCN Ad-v4.indd 1 28/03/2017 09:09
© 2017
Wou
nd C
are Peo
ple Lt
d

28 JCN 2017, Vol 31, No 2
Figure 2
WOUND CARE
Health economic burden that wounds impose on the national health service in the UK. BMJ Open 5(12): e009283. Available online: http://bmjopen.bmj.com/content/5/12/e009283.full
Heinrichs EL, Llewellyn M, Harding K (2005) Assessment of a patient with a wound. In: Gray D, Cooper P, eds. Wound Healing; a systematic approach to advanced wound healing and management. Wounds UK Aberdeen: 1–27
Romanelli M, Dowsett C, Doughty D, et al (2016) Position document: Advances in wound care: the triangle of wound assessment. Wounds International.
Romanelli M, Vowden K, Weir D (2010) Exudate Management Made Easy. Wounds Int 1(2). Available online: www.woundsinternational.com
Schultz G, Sibbald G, Falanga V, et al (2003) Wound bed preparation: a systematic approach to wound management. Wound Repair Regen 11: 1–28
Timmons J (2006) Skin function and wound healing physiology. Wound Essentials 1:8–17
World Union of Wound Healing Societies (2008) Principles of best practice: Wound infection in clinical practice. An international consensus. MEP Ltd, London
overall health, while evaluating if the chosen treatment is achieving the desired outcome.
CONCLUSION
Accurate assessment is key to identifying the most appropriate treatment to expedite healing and/or to palliate symptoms associated with chronic wound healing. Product choice is secondary to getting the assessment process right. In the author’s clinical experience, good assessment and methodical contemporaneous documentation not only help to protect against legal challenges, but also aim to reduce waste, dressing frequency, nurse time, and patient discomfort.
REFERENCES
Australian wound management association (2009) Expert Guide for Healthcare Professionals: Nutrition and Wound Healing. Available online: www.awma.com.au/publications/2009_vic_expert_guide_nutrition_wound_healing.pdf (accessed June, 2016)
Eagle M (2009) Wound assessment: the patient and the wound. Wound Essentials4: 14–24
Gray D, et al (2005) Understanding applied wound management. Wounds UK 1(1):62–8
Guest JF, Ayoub N, Mcilwraith T, et al (2015)
In addition to the tests listed above, blood flow — ankle brachial pressure index (ABPI), oxygenation and neurological investigations should be sought if the patient’s wound is on their lower limb.
DIAGNOSIS
Accurate diagnosis is dependent on the results of the patient history taken, the findings of wound assessment, and the interpretation of the findings from examination and requested investigations. It is imperative that an onward referral is made if there is any doubt as to the cause of the wound and/or it is failing to progress towards healing after four weeks of appropriate treatment.
INTERVENTIONS AND INDICATORS
Interventions should reflect best practice recommendations for the type of wound and marry with the expected outcome and patient’s expectations of treatment.
The community nurse’s goal of care acts as a gauge of success to assess if the treatment plan is appropriate. For example, wound healing may be an appropriate goal in a non-complicated acute surgical wound in a patient that is fit and healthy. However, in a more complex chronic wound, such as a painful venous leg ulcer, it is reasonable to initially aim to manage the patient’s pain effectively before using compression.
Assessment is an ongoing process, which monitors changes in both the wound and the patient’s
Figure 3.The AWM exudate continuum (Gray et al, 2005).
Figure 4.The AWM tissue type continuum, ranging from necrosis (black), to granulation tissue (pink/red) (Gray et al, 2005).
VOLUME HIGH 5 MEDIUM 3 LOW 1
HIGH 5
MEDIUM 3
LOW 1
KEY POINTS Wound healing is initiated after injury and, at a cellular level, is a complex set of interactions between cells which result in closure of the defect.
For acute wounds, for example surgical incisions that are closed, the process is ordered and occurs in a timely and sequential fashion and could be described as predictable.
Unfortunately, the combination of underlying disease processes and an ageing population with multiple comorbidities can lead to chronicity.
Wounds - Milne - read by ???.indd 28 23/03/2017 11:16
© 2017
Wou
nd C
are Peo
ple Lt
d

Supporting healthcare professionals for over 150 years ™Trademark of Smith & Nephew ©January 2017 Smith & Nephew 81173
Together let’s keep an ambitious objective in mind: ZERO.Zero delay in wound healing.
Zero chronic wound recurrence.
Zero wound-related readmissions.
Zero waste of healthcare resources.
Zero diabetic amputations.
CLOSERTO ZERO
“Together lets reduce delays in wound healing”
PICO™ Single-Use Negative Pressure Wound Therapy
“Together lets reduce unnecessary dressing changes”
ALLEVYN™ wound dressings
“Together lets reduce prolonged wound infection”
ACTICOAT™ antimicrobial barrier dressings
www.twoweekchallenge.co.ukwww.celebratewithpico.co.ukwww.allevynbetterways.com
© 2017
Wou
nd C
are Peo
ple Lt
d

Sessions focused on• Debridement/debulking of full thickness
necrosis.• Removal of wound debris and biofilm using
curette.• Removal of wound debris using different
debridement tools and techniques.
Course tutorsProfessor David Gray, Professor Steve Jeffrey,Professor Jackie Stephen-Haynes and Associate Lecturer Pam Cooper.
Feedback from previous courses100 per cent said it was excellent or very good.
Who should attendPractitioners from the field of woundhealing/management seeking to develop their practical skills and understanding of the most advanced clinical practice.
Cost £150, includes lunch and refreshments.
�������������������������������������������������������������������������������������������������������������������
Thursday 1 June 2017 and Wednesday 29 November 2017, 8.45am – 4.30pmSeacole Building, City South Campus, B15 3TN
For more information contactClaire Pickerill at [email protected] orT: 0121 300 4282
��������������������������������������������
Birmingham City University
�D�e�b�r�i�d�e�m�e�n�t� �T�e�c�h�n�i�q�u�e�s� �i�n�P�r�a�c�t�i�c�e� �W�o�r�k�s�h�o�p�s
�T�h�e�s�e� �o�n�g�o�i�n�g� �e�v�e�n�t�s� �w�i�l�l� �b�e� �p�r�i�m�a�r�i�l�y� �h�a�n�d�s� �o�n� �e�x�p�e�r�i�e�n�c�e� �w�o�r�k�i�n�g� �u�n�d�e�r� �d�i�r�e�c�t� �s�u�p�e�r�v�i�s�i�o�n� �o�f� �e�x�p�e�r�t� �p�r�a�c�t�i�t�i�o�n�e�r�s�.
birminham uni2.indd 1 3/23/17 4:55 PM
© 2017
Wou
nd C
are Peo
ple Lt
d

Patients with infected wounds don’t need to endure embarrassing smells as well. CliniSorb is an activated charcoal dressing that effectively adsorbs the volatile molecules that cause malodour. It’s also convenient as you can cut it to any shape, and it doesn’t cost the earth either.
CliniSorb – the great choice to cut out odour and activate confi dence.
Cut out odour Activate confi dence
I understand that this request will be handled by CliniMed Limited. I would like my details to be kept on fi le, so that I can be kept up to date with information about relevant new products and services.
CliniMed® and CliniSorb® are registered trademarks of CliniMed (Holdings) Ltd. Cavell House, Knaves Beech Way, Loudwater, High Wycombe, Bucks. HP10 9QY. ©2007 CliniMed Ltd. 943/0308
For a free sample of CliniSorb®, please complete the coupon and return it to: CliniMed Ltd., FREEPOST HY241, High Wycombe, Bucks. HP10 8BR (NO STAMP REQUIRED), call our free confi dential care-line 0800 036 0100 or visit www.clinimed.co.uk.Mr/Mrs/Ms: Initials: Surname: Address:
Postcode:
Tel. No.: E-mail:
0946 CliniSorb A4 AD.indd 1 13/3/08 15:43:06
© 2017
Wou
nd C
are Peo
ple Lt
d