Embed Size (px)
Citation preview

Accuracy of total bladder volume and residual urine measurements: Comparison between real-time ultrasonography and catheterization
Thomas C. Mainprize, MD, and Harold P. Drutz, MD
Toronto, Ontario, Canada
The practical value of ultrasonography as a rapid means to accurately determine total bladder volumes and residual urine volume was assessed. Transverse and sagittal bladder diameters were measured with real-time ultrasonography in 50 women: (1) before uroflowmetry, (2) before supine postvoiding catheterization, (3) before standing catheterization, and (4) after standing catheterization. Calculated bladder volumes, by use of the measured diameters, for each of eight formulas from the literature were compared with their correspondrng measured total urine volume, total residual volume, and standing residual volume. The lower limit of ultrasonographic visualization of urine in the bladder was approximately 42 m!. No correlation existed between calculated ultrasound bladder volumes and measured urine volumes for any of the eight formulas. Standing residual volumes were measured In 96% of cases. Ultrasonography cannot as yet rapidly measure bladder volumes accurately. Catheterization remains the best method of assessing postvold residuals: supine measurements, the gold standard, should be augmented by standing measurements when more accurate volumes are required. (AM J OSSTET GVNECOL 1989;160:1013-6.)
Key words: Real-time ultrasonography catheterization, standing residual urine, calculated bladder volume, measured urine volume
Ultrasonographic determination of bladder volumes is simple' and noninvasive.' e Even children are less distressed by an ultrasonographic assessment than by catheterization.' Obesity,' , dense pubic hair,' abdominal distention,' and irregular shape of the bladder' produce poor-quality results and have led to a search for an appropriate formula. Formulas that use sagittal and transverse bladder diameters \ '-7 and bladder arease " 'I have been used to calculate bladder volumes.
Calculated bladder volumes have been compared to fixed volumes of Huid infused into an empty bladder and to measured bladder volumes obtained by catheterization of the bladder. Ultrasonography has detected small residual urine volumes in the bladder that are missed by catheterization/ but catheterization remains the most accurate method' of determining residual urine volume. Catheterization is usually done in the supine position.
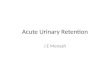
Fig. 1. Sagittal view of bladder showing height ( H) and depth (Ds) measurements.
This study was undertaken to assess the practical value of ultrasonography as a rapid means to accurately determine total bladder and residual urine volumes.
From the Gynecologlcal Urology and Urodyna/nlc Investigative Umt, Mount Smal Hospital, and the Department of ObstetriCs and Gynecology, Umverslly of Toronto.
Presented at the F ortyjourth Annual Meeting of The Society of Obstetrlcwus and Gynaecolo[!;lStl of Canada, Vancouver, Brltllh Co/umbw, Canada. June 21-25, 1988.
Repnnt requests: Dr. H. P Drutz, Sulfe 1221, Mount SmalHolpltal. 6()O UlilVer'\I(~ Ave .. Toronto. Ontarzo. Canada lH5G IX5.
Material and methods
Fifty female patients with chronic, persistent lower urinary tract symptoms were asked to participate in the study during routine visits to the Mount Sinai Hospital's Urodynamic Investigative Unit. An Aloka SSD-720 real-time scanner (Omnium Medical Devices of Canada, Richmond Hill, Ontario) with a 3 MHz transducer was used to measure sagittal height (H) and depth (Ds) (Fig. I) and transverse width (W) and depth (Dt)
1013

1014 Mainprize and Drutz
A
TRANSVERSE PLANE
Fig. 2. Transverse view of bladder showing width (W) and depth (DI) measurements.
(Fig. 2). Scans were repeated until maximum values were obtained.
When the women experienced a strong sensation to void, the first of four sets of ultrasonographic measurements was made. Uroflowmetry and perianal electromyography, with surface electrodes, were performed with a DISA 2100 uroflow system (DISA Elektronik A/S, DK-2740 Skovlunde, Denmark). The voided volume recorded by the DISA 2100 system was confirmed by measuring the volume with a 250 ml graduated cylinder. A second set of ultrasonographic diameters was measured to assess the residual bladder volume.
With a sterile technique, an Fr. 10 Foley catheter was inserted, and the bladder was drained into a 250 ml graduated cylinder to measure the supine bladder residual. A sample of urine was sent for culture. When no further urine was returned through the catheter, the catheter bulb was inflated with 5 ml of normal saline solution in the bladder and the catheter was clamped. A third set of ultrasonographic diameters of the bladder was taken. The patient was asked to stand, the catheter bulb was deflated, and the catheter unclamped. The urine was collected in the graduated cylinder as the catheter was withdrawn and the standing residual urine volume was measured. The last of four
April 1989 Am J Obstet Gynecol
Table I. Uroflowmetry results (N = 50)
Voided volume (ml) Peak flow (mil sec) Mean flow (ml/sec) Voiding time (sec) Residual (ml) Time to peak flow (sec)
Mean ± SD
319 ± 167 19.8 ± 10.3 8.1 ± 6.4
89.5 ± 86.0 156 ± 115 II ± 14
Range
69 -774 3.5 - 48.8 1.0 - 32.1
9 - 399 13 - 567
1 - 85
Pattern: continuous, n = 35; intermittent, n = 15.
ultrasonograms was obtained with the patient supine to confirm that the bladder was empty.
The bladder diameters measured with ultrasonography were used to calculate three bladder volumes (total bladder capacity, total residual volume, and standing residual volume). These were calculated from each of eight formulas taken from the literature:
H x Ds X W7 (1)
W x Ds x H x TI"
6 (2) H X Ds x W - 3.14"
2.17 ( 3) H X Ds x W X 0.7 1l1 ( 4)
H x Ds X W X 0.625' ( 5)
H x W X (Ds + Dt)" 2 (6)
H X Ds X 6.6' (7)
W x H X 12.56" ( 8)
Accuracy was calculated by the method reported by Griffiths et al.": Volume calculated .;- Volume measured. Percent error was determined by the formula: (Volume calculated - Volume measured) x 100 .;- Volume measured.
Results
The average age was 53.8 years (range 20 to 78). Four patients had positive urine cultures: Escherichia coli (n = 2), Proteus mirabilis (n = 1), and group B streptococci (n = 1). Uroflowmetry results are recorded in Table I. Perianal electromyographic activity was reported as normal in 27 and increased in 23 cases.
Six women had empty bladders by ultrasonography after uroflowmetry; supine residual volumes measured 13 to 28 ml. Ten women had empty bladders on ultrasonography after supine catheterization, but only two women had no standing residual volume. Forty-eight (96%) patients had standing residual urine volumes and 36% had residuals >30 ml.
A total of 104 sets of ultra so no graphic measurements were recorded; 68 of these sets were associated with measured bladder volumes> 150 ml. The average accuracy and percent error for each formula are shown

Volume 160 Number 4
Bladder volume- Ultrasonography versus catheterization 1015
Table II. Accuracy and percent error for each formula with all calculated formulas (N = 104) and measured urine volumes> ISO ml (n = 68)
Accuracy % Error
All formula> Volume> 150 ml All formulas Volume> 150 ml (N = 10-1) (n = 68) (N = 104) (n = 68)
Formula No. (mean ± SD) (mean ± SD) (//lean ± SD) (mean ± SD)
1 0.76 ± 0.54 0.95 ± 0.54 49 ± 32 41 ± 34 2 0.40 ± 0.28 0.50 ± 0.28 62 ± 24 53 ± 23 3 0.35 ± 0.25 0.43 ± 0.25 67 ± 24 58 ± 23 4 0.54 ± 0.38 0.68 ± o.:n 53 ± 27 44 ± 25 5 0.48 ± 0.33 0.59 ± 0.34 57 ± 26 47 ± 23 6 0.75 ± 0.51 0.92 ± 0.50 47 ± 32 39 ± 32 7 0.66 ± 0.31 0.71 ± 0.33 41 ± 22 38 ± 21 8 1.41 ± 0.69 1.40 ± 0.60 59 ± 54 53 ± 49
in Table II. The number of times each formula gave a calculated volume closest to the measured volume was as follows: (I) 13,* (2) 3, (3) 4, (4) 8, (5) 0, (6) 18,* (7) 20, t and (8) 41. No bladder volume ;:,,42 ml was missed by ultrasonography; five of 50 measured urine volumes <42 ml were identified by ultrasonography.
Comment
As a simple, noninvasive test, ultrasonography would appear to be perfect for assessing bladder volumes. The many formulas in the literature attest to the difficulty in finding one formula to fit irregular geometric bladder configurations.' Bladder volumes have been calculated by means of measurements of bladder diameter and surface area. No clear consensus as to which is better has been reached; surface area has been reported as being better than diameter' and vice versa. 7
The use of transverse or sagittal diameters or both is the most commonly reported method and is quicker to perf()rm than serial area measurements. In the search for a rapid method for office use, we chose to explore the approach with transverse and sagittal diameter measurements. Of the eight formulas taken from the literature, the greatest accuracy was achieved by multiplying as follows: Sagittal height x Sagittal depth x Transverse width. 7 The lowest percent error was achieved with the formula: Sagittal height x Sagittal depth x 6.6." The formula producing the largest number of calculated volumes closest to the measured volumes was: Sagittal height x Transverse width x 12.56." No one formula proved to be better for quantitative assessment of bladder volumes.
To provide a truly objective assessment of the ultrasonography technique to replace catheterization, we
*On two occasions more than one formula gave the same result.
tOn one occasion more than one formula gave the same result.
felt that all calculated volumes should be included. The inclusion of cases where measurements were hindered because of obesity or where more than the usual suprapubic pressure was necessary to identify the bladder contributed to the poor results. Unfortunately, these situations occur commonly and need to be included in the objective assessment.
The qualitative assessment of bladder volume had a limit of approximately 42 ml. All 99 measured volumes ;:,,42 ml were visualized by ultrasonography, but only five of 50 (10%) volumes <42 ml were identified.
If the normal upper limit of 50 ml for residual urine volume is used, then ultrasonography is an excellent technique qualitatively. Our investigative unit uses 30 ml as the upper limit for residual urine volume and we urge patients to strive for this goal. Qualitative assessment of bladder volumes has not yet replaced catheterization in our unit.
Even catheterization, the gold standard for assessing residual urine volumes, has its limitations. Hakenberg et a!." reported identifying residual urine with ultrasonography after catheterization. Ninety-six percent of our patients had additional residual urine volumes with standing measurements after supine catheterization for residual volumes was completed. Of the 48 patients, 17 (36%) had volumes >30 ml. Studies that relied on ultrasonography alone' x to confirm bladder emptiness may be misleading in their assessment of true bladder capacity.
Catheterization remains the most accurate method of assessing residual bladder volumes, especially if augmented by standing residual urine measurements. Ultrasonography is poor for quantitative assessment of bladder volumes, particularly at the low residual volumes. Although ultrasonography provides good qualitative assessment of bladder volumes, it fails for low bladder volumes. Ultrasonography is useful where the risks of an accurate measurement outweigh the benefits of a less accurate assessment, as in children. I The use

1016 Mainprize and Drutz
of a vaginal or rectal probe may provide better qualitative assessment, but this has yet to be proved; the problem of quantitative assessment because of irregular bladder configuration is unlikely to be improved with a vaginal or rectal probe. In a future study we intend to compare the accuracy of these various methods of ultrasonographic measurement of bladder volumes.
REFERENCES
1. Harrison NW, Parks C, Sherwood T. Ultrasound assessment of residual urine in children. Br] UroI1976;47:805-14.
2. Rageth ]C, Langer K. Ultrasonic assessment of residual urine volume. Urol Res 1982;10:57-60.
3. Hakenberg OW, Ryall RL, Langlois SL, Marshall YR. The estimation of bladder volume by sonocystography] Urol 1983; 130:249-51.
4. Ravichandran G, Fellows GJ. The accuracy of a hand-held real time ultrasound scanner for estimating bladder volume. Br] UroI1983;55:25-7.
Bound volumes available to subscribers
April 1989 Am J Obstet Gynecol
5. Poston GJ, Joseph AEA, Riddle PRo The accuracy of ultrasound in the measurement of changes in bladder volume. Br J Urol 1983;55;361-3.
6. McLean GK, Edell SL. Determination of bladder volumes by gray scale ultrasonography. Radiology 1978; 128: 181-2.
7. Pederson JF. Bartrum ~. Grytter C. Residual urine determination by ultrasonic scanning. Am ] Roentgenol 1975;125;474-8.
8. Griffiths CJ, Murray A, Ramsden PD. Accuracy of and repeatability of bladder volume measurement using ultrasound imaging.] UroI1986;136:808-12.
9. Doust BD, Baum ]K, Maklad NF, Baum RF. Determination of organ volume by means of ultrasonic B-mode scanning. ]CU 1974;2(2): 127-30.
10. Kiely EA, Hartnell GG, Gibson RN, Williams G. Measurement of bladder volume by real-time ultrasound. Br ] Urol 1987;60:30-5.
11. Orgaz RE, Gomez AZ, Ramirez CT, Torres JLM. Applications of bladder ultrasonography. I. Bladder content and residue.] Urol 1981; 125: 174-6.
Bound volumes of the AMERICAN JOURNAL OF OBSTETRICS AND GYNECOLOGY are available to subscribers (only) for the 1989 issues from the Publisher, at a cost of $56.00 ($79.00 international) for Vo!' 160 (January-June) and Vo!' 161 (July-December). Shipping charges are included. Each bound volume contains a subject and author index and all advertising is removed. Copies are shipped within 60 days after publication of the last issue in the volume. The binding is durable buckram with the JOURNAL name, volume number, and year stamped in gold on the spine. Payment must accompany all orders. Contact The C.V. Mosby Company, Circulation Department, 11830 Westline Industrial Drive, St. Louis, Missouri 63146-3318, USA; phone (800) 325-4177, ext. 351.
Subscriptions must be in force to qualify. Bound volumes are not available in place of a regular JOURNAL subscription.


![Intestinal metaplasia of the bladder in 89 patients: a ...Oct 10, 2015 · bladder extrophy, long-term catheterization, bladder calculi and neurogenic bladder [1]. The presence of](https://img.pdfslide.us/doc/110x75/60b92038f4dd374d6469d737/intestinal-metaplasia-of-the-bladder-in-89-patients-a-oct-10-2015-bladder.jpg)