Embed Size (px)
Citation preview


Accreditation and Acknowledgement
▪ Forefront Collaborative designates this live activity for a maximum of 1.0 AMA
PRA Category 1 Credit™. Physicians should claim only the credit
commensurate with the extent of their participation in the activity.
▪ Forefront Collaborative is accredited by the Accreditation Council for Continuing
Medical Education (ACCME) to provide continuing medical education for
physicians.
▪ The activity is provided by Forefront Collaborative and supported by an
educational grant from Lilly.

Faculty Disclosures
▪ In compliance with ACCME and AMA guidelines, faculty disclosures will be
acknowledged prior to their slide presentation.
▪ When providing information, in whole or in part, related to non-FDA approved
uses for drug products and/or devices, the presenter will clearly acknowledge
the unlabeled indications or the investigative nature of their proposed uses to
the audience.
▪ Acknowledgement of unapproved uses or investigational nature of therapies is
noted within the slide presentation.

Planner Disclosures
Educational activities provided by Forefront Collaborative must demonstrate
balance, independence, and scientific rigor. All those in a position to control the
content of an activity must disclose all relevant financial relationship(s) with
commercial interest(s). For this educational activity, all conflicts of interest have
been resolved through peer review and revisions to ensure independence,
evidence base, fair balance, and absence of commercial bias. The reviewers of
this activity have no relevant financial relationships to disclose.
The following individuals have indicated that neither they nor their
spouses/partners have had, in the past 12 months, financial relationship(s) with
commercial interests relative to the content of this CME activity:
▪ Planner (Forefront Collaborative): Katie Detzler

Planner Disclosures (cont.)
The following individuals have disclosed that they and/or their spouse/partner has had a financial relationship in the past
12 months:
▪ Planner (Forefront Collaborative): Lily Zurkovsky, PhD, has personal stock in Teva Pharmaceutical Industries.
▪ Planner: Stewart J. Tepper, MD, has received salary from Dartmouth-Hitchcock Medical Center and from the American
Headache Society and royalties from Springer; he has been a consultant or on an advisory board for Acorda
Therapeutics, Alder BioPharmaceuticals, Alexza Pharmaceuticals, Allergan, AlphaSights, Amgen, Autonomic
Technologies, Axsome Therapeutics, Cefaly, Charleston Laboratories, DeepBench, Dr. Reddy’s Laboratories,
electroCore, Eli Lilly and Company, eNeura, GLG Pharma, Guidepoint Global, Magellan Rx Management, Neurolief,
Nordic BioTech, Novartis, Pfizer, Scion NeuroStim, Slingshot Insights, Supernus Pharmaceuticals, Teva Pharmaceutical
Industries, and Zosano Pharma Corporation; Dr. Tepper has contracted research for Alder BioPharmaceuticals,
Allergan, Amgen, Autonomic Technologies, Dr. Reddy’s Laboratories, electroCore, eNeura, Neurolief, Novartis, Scion
NeuroStim, Teva Pharmaceutical Industries, and Zosano Pharma Corporation; he has ownership interest in Autonomic
Technologies
▪ Reviewer: Lawrence Newman, MD, has contracted research for Alder BioPharmaceuticals, Allergan, Amgen, Eli Lilly
and Company, and Teva Pharmaceutical Industries
▪ Reviewer: Todd Schwedt, MD, has consulted or been on an advisory board for Alder BioPharmaceuticals, Allergan,
Amgen, Cipla, Eli Lilly and Company, Ipsen, Dr. Reddy’s Laboratories, Novartis, and Teva Pharmaceutical Industries;
Dr. Schwedt has contracted research for Amgen; he has ownership interest in Aural Analytics, Nocira, and Second
Opinion

How to Claim Credit
▪ To claim CME credit, you will have to complete the evaluation form located at
your seat and return the program staff at the end of this activity.
▪ The pre- and posttest are also located at your seat. If you have not completed
the pretest, please do so now. There will be some time at the end of the activity
for you to complete the posttest.

Slides and Question Cards
▪ The slides presented during this symposium can be downloaded at
forefrontcollabactivities.com/RethinkingMigraine.
▪ Question cards are in the center of your table. They will be collected throughout
the presentation; the question and answer session will begin following the last
presentation. Please hand the question cards to a staff member as they walk
around the room.
▪ As a courtesy to others, please silence your cell phones or set them to vibrate.

THE NEW ERA OF MIGRAINE TREATMENT
Deborah I. Friedman, MD, MPHProfessor of Neurology and Ophthalmology,
Department of Neurology and Neurotherapeutics
UT Southwestern Medical Center
Dallas, Texas

FACULTY DISCLOSURES
Consultant/advisory board: Alder BioPharmaceuticals, Allergan, Amgen, Biohaven Pharmaceuticals, electroCore, Promius, Supernus Pharmaceuticals, Teva Pharmaceutical Industries, and Zosano Pharma Corporation
Speaker: Allergan, Amgen, Autonomic Technologies, electroCore, Supernus, and Teva Pharmaceutical Industries
Received clinical trial grant support: Axon Optics, Autonomic Technologies, Eli Lilly and Company, Merck, and Zosano Pharma Corporation
Deborah I. Friedman, MD, MPH

OVERVIEW
The New Era of Migraine Treatment
▪ Recent advances in understanding migraine pathophysiology
▪ Impact of episodic and chronic migraine to quality of life
▪ Unmet patient needs
▪ New and emerging treatments in acute and preventive treatment of migraine
▪ Contrast to current standards of care
▪ Identify endpoints meaningful to clinical practice: how treatment success
and failure should be measured

PATHOPHYSIOLOGYAND THERAPEUTIC TARGETS

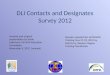
Migraine Pathophysiology
CGRP
CGRP=calcitonin gene-related peptide. TNC=trigeminal nucleus caudalis.
Adapted with permission from Goadsby PJ, et al. N Engl J Med. 2002;346:257–270.

Vesicle
I. SENSORY AXON
Neuropeptide
III. VASCULAR RECEPTOR INTERACTION
VASODILATION, PLASMAEXTRAVASATION,NEUROGENIC INFLAMMATION
II. NEUROPEPTIDERELEASE
Receptor
Smoothmuscle
Endothelium
IV.
Effects of Neuropeptide Release on Blood Vessels

Summary of Pathophysiology and Targets
4. 5-HT1F - Inhibit central pain transmission
5-HT1D—Inhibits
neuropeptide (CGRP) release
5-HT1B—
Vasoconstriction
5-HT1F—Inhibits central
pain transmission
5-HT1D—Decreases
pain signal
transmission
5-HT=5-hydroxytryptamine.
Adapted and updated from Hargreaves RJ, Shepheard SL. Can J Neurol Sci. 1999;26 (suppl3):S12–S19.

Pathophysiology and Treatments
▪ Migraine pain is modulated by release of CGRP and other neuropeptides with
resultant meningeal vasodilation and neurogenic inflammation
▪ Current migraine-specific acute treatments are serotonin (5-HT)1B/D agonists
that inhibit CGRP release, constrict CGRP-dilated vessels, and prevent
pain signals from returning to the brain; they are contraindicated with
vascular disease
▪ Oral preventive medications are centrally active, modulating central
migraine integration
▪ Targets to terminate or prevent migraine include 5-HT1B/D,F agonists (triptans,
ergots, lasmiditan) and CGRP antagonists (gepants and monoclonal antibodies)

Worldwide Migraine Impact
▪ In 2016, the World Health Organization
listed migraine #6 of the 10 greatest
causes of years lived with disability (YLDs)
▪ Migraine was 1 of the 2 leading causes of
YLDs in developed countries, and in the
top 5 worldwide
▪ “Migraine, including medication overuse
headache, a complication of chronic
migraine (CM), has become the second-
largest cause of disability in 2016”
GBD 2016 Disease and Injury Incidence and Prevalence Collaborators. Lancet. 2017;390(10100):1211-1259.

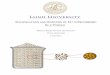
26
17
0
25
50
75
100
6 months 12 months
Adherence to Oral Migraine Preventives Is Poor▪ Retrospective claims database analysis: Insured patients with migraine and
≥15 headache days/month (N=8688)
Patients
Adhere
nt
to O
ral P
rophyla
xis
, %
discontinue preventive
treatment over the
course of 1 year83%
Hepp Z, et al. Cephalalgia. 2015;35:478-488.

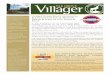
Reasons Patients Discontinue Prophylactic Medication: Unmet Need is High▪ International Burden of Migraine Study-II assessed preventive therapy patterns
in 1165 patients with migraine
0
5
10
15
20
25
30
35
40
45
50
Pa
tie
nts
, %
Satisfactory resolution Lack of efficacy Side effects Cost Other
Antidepressants (n=205)
Antiepileptics (n=125)
β-blockers (n=120)
Calcium channel blockers (n=59)
Lack of efficacy and/or medication side effects are the most common reasons for discontinuation of preventive medications.
Patient-Reported Reasons for Discontinuation of Prophylactic Medication
Blumenfeld AM, et al. Headache. 2013;53(4):644–655.

EMERGING ACUTE TREATMENT CLASSES

DITAN: 5-HT1F AGONIST

Lasmiditan, Phase 3 Data inAcute Migraine Treatment
▪ 2-hour pain freedom is 32.2% (placebo 15.3%)
▪ Treatment emergent adverse events after the first dose: 200 mg (42.7%),
100 mg (36.3%), placebo (16.4%)▪ Most common were dizziness, paresthesia, and somnolence
▪ The lasmiditan adverse events are likely due to activation of the 5-HT1F
receptors, which are mostly central
▪ 5-HT1F receptors do not cause vasoconstriction; so, unlike triptans,
this new class should be safe in the presence of vascular disease
1. Kuca B, et al. Neurology. 2018;91(24):e2222-e2232. 2. Wietecha LA, et al. Abstract PO-02-180 presented at IHC 2017; Vancouver.

TREATMENTSTARGETING CGRP

CGRP
▪ Neuropeptide belonging to calcitonin family
▪ Calcitonin
▪ Amylin
▪ Adrenomedullin
▪ Intermedin
adenylylcyclase
Gs
RCP
CGRP
RA
MP
1
CLR
cAMP
▪ Receptors that bind or are activated by
CGRP are present throughout the body,
including the gut
▪ Present at all migraine pathogenesis sites
in the trigeminovascular system
▪ Plasma level increases in migraine;
decreases with treatment
RAMP1=receptor activity modifying protein 1. cAMP=cyclic adenosine monophosphate. CLR=calcitonin receptor-like receptor. RCP=receptor component protein. NS=nervous system.
VMpo=ventromedial posterior nucleus. VPpc=ventral posterior parietal cortex. elPB=external pontine lateral parabrachial nucleus. emPB=external medial parabrachial nucleus.
1. Naot D, Cornish J. Bone. 2008;43(5):813-818. 2. Benarroch EE. Neurology. 2011;77:281-287. 3. Walker CS, Hay DL. Br J Pharmacol. 2013;170(7):1293-1307. 4Holzer P, Farzi A. Adv Exp Med Biol.
2014;817:195-219.

GEPANTS: SMALL-MOLECULE CGRP RECEPTOR ANTAGONISTS

The Small Molecule CGRP Receptor Antagonists: Gepant Summary
Acute Treatment of Episodic Migraine (EM)
▪ There have been 6 gepants tested which demonstrated efficacy in acute
migraine treatment: olcegepant, BI 44370 TA, telcagepant, MK-3207,
rimegepant, and ubrogepant
▪ BI 44370 TA, telcagepant, and MK-3207 are all reportedly liver toxic
▪ Ubrogepant and rimegepant have reported out positive regulatory trials
and will likely be submitted to the FDA for acute treatment of migraine over
the next year
▪ 2-hour pain freedom ≈ 20% in phase 3 trials
▪ They do not cause vasoconstriction; unlike triptans, should be safe with
vascular disease
1. Tfelt-Hansen P. Headache. 2011;51:118-123. 2. Tfelt-Hansen P, Do TP. Abstract PO-01-48 presented at IHC 2017; Vancouver. 3. Allergan press release. February 6, 2018.
https://www.allergan.com/news/news/thomson-reuters/allergan-announces-positive-top-line-phase-3-resul. Accessed April 26, 2018. 4. Biohaven press release. March 26, 2018. http://biohavenpharma.com/biohaven-
announces-successful-achievement-of-both-co-primary-regulatory-endpoints-in-two-pivotal-phase-3-trials-of-rimegepant-an-oral-cgrp-receptor-antagonist-for-the-acute-treatment-of-migraine/. Accessed April 26, 2018.

The Small Molecule CGRP Receptor Antagonists: Gepant Summary (cont.)
Preventive Treatment of EM
▪ Atogepant vs placebo reported positive phase 2 trial data in 2018 and showed
drops in mean monthly migraine days for EM; will proceed to phase 3 trials
▪ No signal of liver toxicity
▪ Rimegepant will be tested for prevention in phase 2
1. Tfelt-Hansen P. Headache. 2011;51:118-123. 2. Tfelt-Hansen P, Do TP. Abstract PO-01-48 presented at IHC 2017; Vancouver. 3. Allergan press release. February 6, 2018.
https://www.allergan.com/news/news/thomson-reuters/allergan-announces-positive-top-line-phase-3-resul. Accessed April 26, 2018. 4. Biohaven press release. March 26, 2018. http://biohavenpharma.com/biohaven-
announces-successful-achievement-of-both-co-primary-regulatory-endpoints-in-two-pivotal-phase-3-trials-of-rimegepant-an-oral-cgrp-receptor-antagonist-for-the-acute-treatment-of-migraine/. Accessed April 26, 2018.

TREATMENTSTARGETING CGRP

PREVENTION: MABs

MABs to CGRP or the CGRP Receptor for Migraine Prevention
▪ How are they different than previous oral
migraine prevention?
▪ MABs are big molecules that cross the
blood brain barrier to a very small extent1,2
▪ MABs are eliminated by the reticuloendothelial
system, so no risk for hepatotoxicity—so far,
MABs are safe1
▪ Efficacy data suggest that peripheral,
not central, anti-CGRP action is sufficient
to block migraine in some patients
Small Molecule
~0.2-1 kDa
lgG1 Monoclonal Antibody
~150 kDa
1. Yu YJ, Watts RJ. Neurotherapeutics. 2013;10(3):459-472. 2. Lipton RB, et al. US Neurology. 2018;14 (suppl4):S3-S10.
3. Tepper SJ. Headache 2018;58 (suppl3):238-275. 4. Tepper SJ. Headache 2018;58 (suppl3):276-290.

MABs to CGRP or the CGRP Receptor for Migraine Prevention (cont.)
▪ Are they an improvement?3,4 All 4
▪ Work to prevent EM, CM, and decrease the number of acute
medications taken in patients with medication-overuse headache
▪ Have quick onset, separating from placebo within 1 week in
post hoc analysis
▪ Show clinically meaningful response by 1 month
▪ Have responder rates for ≥75% and higher
▪ Have safety and tolerability similar to placebo
▪ Decrease acute medication use days, impact, and disability,
and improve quality of life in clinical trials
1. Yu YJ, Watts RJ. Neurotherapeutics. 2013;10(3):459-472. 2. Lipton RB, et al. US Neurology. 2018;14 (suppl4):S3-S10.
3. Tepper SJ. Headache 2018;58 (suppl3):238-275. 4. Tepper SJ. Headache 2018;58 (suppl3):276-290.

4 Injectable MABs to CGRP or Its Receptor:3 Now FDA Approved and Available
Erenumab-aooe
(fully human)
Fremanezumab-vfrm
(fully humanized)
Galcanezumab-gnlm
(humanized)
Eptinezumab
(humanized)
Studied for EM, CM EM, CM, eCH EM, CM, eCH EM, CM
Route and
dosing
Monthly SC
70, 140 mg
Monthly or quarterly SC;
225 mg monthly, or
675 mg Q3 months
Monthly SC; 240 mg loading
dose, then 120 mg SC
monthly thereafter
Q3 months IV
Target CGRP receptor CGRP peptide or ligand CGRP peptide or ligand CGRP peptide or ligand
Regulatory
status
FDA-approved
5/17/18 for migraine
prevention
FDA-approved
9/14/18 for migraine
prevention
FDA-approved
9/26/18 for migraine
prevention
In development;
presented (+) phase
3 EM and CM RCTs
Terms: n=neurologic; umab=fully human; zumab=humanized; human=100%; humanized=90-95%
eCH= episodic cluster headache. RCTs=randomized clinical trials.
1. Tepper SJ. Headache. 2018;58 (suppl3):238–275. 2. Tepper SJ. Headache. 2018;58 (suppl3):276–290. 3. Edvinsson L. Headache. 2018;58 (suppl1):33-47.

3 Major MAB Questions
Are they safe?Are they different
than what we have now?
Are they an improvement?
1 2 3

Clinical Utility of the 4 MABs
MAGNITUDE OF EFFECT
▪ In CM, erenumab showed a 6.5 day reduction in monthly migraine days from
baseline through weeks 9-12 in the pivotal RCT
▪ At 1 year in the open-label erenumab study, mean monthly migraine days
dropped 10.5 days from baseline
▪ 4 new months of no migraine compared with baseline
▪ Eptinezumab showed an 8 day reduction from baseline at 12 weeks
ONSET OF EFFECT
▪ In post hoc analysis, MABs separate from placebo in less than a week
▪ Show meaningful clinical benefit in the first month
1. Tepper SJ. Headache 2018;58 (suppl3):238-275. 2. Tepper SJ. Headache 2018;58 (suppl3):276-290.

Other Clinical Advantages
▪ Safety and tolerability: comparable to placebo
▪ Acute migraine medication use decreased, including triptans and all acute
meds (erenumab, fremanezumab, galcanezumab)
▪ Effectiveness with comorbid illnesses such as depression and anxiety
(erenumab, fremanezumab, galcanezumab)
▪ Patient reported outcomes: disability, impact, and satisfaction all improved
▪ CV safety (erenumab, fremanezumab, galcanezumab)
1. Tepper SJ. Headache 2018;58 (suppl3):238-275. 2. Tepper SJ. Headache 2018;58 (suppl3):276-290.

New Outcome Measures to Evaluate Migraine Treatment Effectiveness
1. Tepper SJ. Headache 2018;58 (suppl3):238-275. 2. Tepper SJ. Headache 2018;58 (suppl3):276-290. 3. Lipton RB et al. Headache. 2018;58 (suppl2):162-163.
Conversion of chronic to EM (erenumab,
fremanezumab, galcanezumab)
Conversion of acute medication overuse to no overuse (erenumab)

▪ Effectiveness in patients with lack of response to previous
preventive medications
▪ Prospective placebo-controlled randomized clinical trials of 2-4 previous
preventives (erenumab LIBERTY trial and fremanezumab FOCUS study)
▪ Subanalyses (erenumab, fremanezumab, galcanezumab)
▪ Specific exposures: fremanezumab and patients with a lack of success
with onabotulinumtoxinA and topiramate
Clinically Meaningful Outcome Measures
1. Tepper SJ. Headache 2018;58 (suppl3):238-275. 2. Tepper SJ. Headache 2018;58 (suppl3):276-290. 3. https://www.tevapharm.com/news/teva_announces_positive_topline_phase_iiib_results_with
_fremanezumab_in_adults_with_migraine_who_did_not_respond_to_multiple_classes_of_preventive_treatments_12_18.aspx. Accessed December 24, 2018. Ï

▪ Overall responder rates
▪ 41% of patients showed ≥75% responder rates of reduction in mean
monthly migraine days at 1 year in the erenumab open-label extension trial
▪ 54% showed ≥75% responder rates of reduction in mean monthly migraine
days at 1 year in the eptinezumab placebo-controlled RCT
▪ The ≥75% responder rates are linked to marked drops in disability and
impact and improvements in quality of life in clinical trial data
1. Tepper SJ. Headache 2018;58 (suppl3):238-275. 2. Tepper SJ. Headache 2018;58 (suppl3):276-290. 3. https://www.tevapharm.com/news/teva_announces_positive_topline_phase_iiib_results_with
_fremanezumab_in_adults_with_migraine_who_did_not_respond_to_multiple_classes_of_preventive_treatments_12_18.aspx. Accessed December 24, 2018. Ï
Clinically Meaningful Outcome Measures (cont.)

How Are They Given?
▪ Erenumab and galcanezumab: Self-inject monthly
▪ Fremanezumab: Self-inject monthly or every 3 months
▪ Eptinezumab: Receive an IV infusion every 3 months
Erenumab With AutoinjectorAlso used for etanercept for rheumatoid arthritis,
and one of the generic sumatriptan injection products
Top
Teal injection button
Lock ring
Lock/unlock symbols
Medicine
Clear base
Base cap
Galcanezumab With Autoinjector
Also used for dulaglutide for DM2
and ixekizumab for psoriasis
or prefilled syringe
Fremanezumab
With Prefilled Syringe
DM2=diabetes mellitus type 2.

Summary
▪ Pathophysiology has led to pharmacology, which is
translational research made real
▪ Migraine is one of the most disabling disorders
in the world
▪ Unmet need is high, with patients discontinuing current
oral preventive medications more than 80% of the time
by the end of a year
▪ New designer classes of acute medication are
in development
▪ Gepants, serotonin (5-HT1F) agonist
▪ New classes of preventive medication are available and
in development
▪ Gepants
▪ Anti-CGRP or CGRP receptor MABs
▪ New measures of effectiveness suggest marked
improvements in outcomes with the new MABs
Future so bright, we gotta wear shades

Q&A

Stacy V. Smith, MDNeurologist,
Houston Methodist Neurological Institute
Assistant Professor,
Houston Methodist Institute of Academic Medicine and Weill Cornell Medicine
Houston, Texas
CASES IN EPISODICAND CHRONICMIGRAINE

FACULTY DISCLOSURES
Speaker: Eli Lilly and Company and Teva Pharmaceutical Industries
Stacy V. Smith, MD

CASE 1

Case 1
▪ Ms S. is a 25-year-old woman with
depression, anxiety, Raynaud’s disease,
and headaches since childhood
▪ The attacks occur weekly and are generally
2 days in duration
▪ They are often triggered by stress, fatigue,
and menses
▪ Headaches are preceded by a prodrome of
1 day of cognitive fuzziness and malaise
but no true aura
VS=vital signs. BP=blood pressure. P=pulse. R=respiratory rate.

Case 1 (cont.)
▪ Each headache day is accompanied by
throbbing, bilateral moderate to severe pain,
photo- and phonophobia, and nausea with
frequent disability and work loss
▪ VS: BP 120/70, P 72, R 12; complete medical
and neurologic exams are normal
▪ Acutely, she gets relief with sumatriptan 100 mg
PO but usually has recurrence that requires
retreatment
▪ For prevention, she has tried amitriptyline,
which caused excessive sedation, and
topiramate, which caused word-finding difficulty
VS=vital signs. BP=blood pressure. P=pulse. R=respiratory rate.

What Is Her Diagnosis?
International Classification of Headache Disorders (ICHD-3)
Diagnostic Criteria for Episodic Migraine Without Aura
A. At least five attacks fulfilling criteria B-D
B. Headache attacks lasting 4-72 hours (when untreated or unsuccessfully treated)
C. Headache has at least 2 of the following 4 characteristics:
1. Unilateral location
2. Pulsating quality
3. Moderate or severe pain intensity
4. Aggravation by or causing avoidance of routine physical activity (eg, walking or climbing stairs)
D. During headache at least 1 of the following:
1. Nausea and/or vomiting
2. Photophobia and phonophobia
E. Not better accounted for by another ICHD-3 diagnosis
Cephalalgia. 2018;38(1):1-211.

Options: Classification of Migraine Preventive Therapies AAN AHS Guidelines, 2012
*FDA-approved for migraine prevention.
ƗNew evidence puts candesartan Level A or B.
VPA=valproate. MRM=menstrually-related migraine. ACE=angiotensin converting enzyme. ARBs=angiotensin receptor blockers. CBZ=carbamazepine. SSRIs=selective serotonin reuptake inhibitors. AEDs=antiepileptic drugs.
GBP=gabapentin. CCB=calcium channel blocker. LTG=lamotrigine. TCAs=tricyclic antidepressants. OXCB=oxcarbazepine. BZD=benzodiazepine. NSAIDs=nonsteroidal anti-inflammatory drugs.
Silberstein SD, et al. Neurology. 2012;78(17):1337-1345.
Level A (≥2 Class I trials)
Antiepileptic drugs
VPA*
Topiramate*
β-blockers
Metoprolol
Propranolol*
Timolol*
All of the MABs have
Level A as of 2018:
Erenumab,
Fremanezumab,
Galcanezumab
Level B: Probably effective (1 class I or 2 class II studies)
Antidepressants
Amitriptyline
Venlafaxine
β-blockers
Atenolol
Nadolol
Level C: Possibly effective (1 class II study)
ACE inhibitors
Lisinopril
β-blockers
Nebivolol
Pindolol
ARBs
CandesartanƗ
Antihistamines
Cyproheptadine
Old data/meds
Clonidine, Guanfacine,
CBZ
Level U: Inadequate or conflicting data to support or refute use
Carbonic inhibitors—acetazolamide
Antithrombotics—warfarin
SSRIs—fluoxetine, fluvoxamine
β-blockers—bisoprolol
TCAs—protriptyline
AEDs—GBP
CCBs
Verapamil, nicardipine, nimodipine,
nifedipine
Muscle relaxants—cyclandelate
Possibly or probably ineffective
Established as not effective
AEDs—LTG
Probably not effective
TCAs—clomipramine
Possibly not effective
AEDs—OXCB
BZDs—clonazepam
β-blockers—acebutolol
NSAIDs—nabumetone
ARBs—telmisartan

What Are Your Considerations in Picking Medication Options for Her? ▪ There are 3 major categories of preventive medications for EM prevention:
▪ Antidepressants (none FDA-approved)
▪ Antihypertensives (propranolol and timolol FDA-approved)
▪ AEDs (divalproex and topiramate FDA-approved)
▪ Her blood pressure is on the low side, but not prohibitively so
▪ Depression and Raynaud’s disease mitigate against β-blockers
▪ There is now excellent evidence for effectiveness of candesartan 16 mg in EM prevention
▪ We started her on candesartan 8 mg PO QHS week 1, then increased to 16 mg PO QHS week
2 for a 3-month trial
QHS=every night at bedtime.
1. Tronvik E, et al. JAMA. 2003;289(1):65-69. 2. Stovner LJ, et al. Cephalalgia. 2014;34(7):523-532.

Candesartan Made Her Light-Headed and Was Not Tolerated. Now What? ▪ Keeping in mind the 3 major categories of preventive medications for EM:
▪ Antihypertensives (propranolol and timolol FDA-approved); she can’t take the beta blockers
and can’t tolerate the candesartan; verapamil has very low evidence for effectiveness, so this category will not be our
next step
▪ AEDs (divalproex and topiramate FDA-approved); both out
▪ Divalproex/valproate is contraindicated in pregnancy due to risk of polycystic ovaries and birth defects; discuss plans to conceive
and use of birth control
▪ Antidepressants (none FDA-approved); amitriptyline out
▪ The combination of depression and anxiety would allow for an SNRI; there is level B evidence for venlafaxine
▪ There is level C evidence for ACE inhibitors
▪ What about the problem of recurrence with the sumatriptan?
▪ Ask about dose, formulation, and timing
▪ Addition of an NSAID with the triptan can reduce recurrence and give greater likelihood of a sustained
pain-free response
SNRI=serotonin norepinephrine reuptake inhibitor.
1. Bulut S, et al. Clin Neurol Neurosurg. 2004;107(1):44-48. 2. Ozyalcin SN, et al. Headache. 2005;45(2):144-152..

Next Steps
▪ Desvenlafaxine 50 mg PO QAM was initiated for prevention▪ Venlafaxine is a Level B agent
▪ Desvenlafaxine has fewer side effects
▪ Sumatriptan-naproxen sodium combination tablet was started for acute treatment
▪ The acute treatment increased the likelihood of pain freedom rather than just relief, and
reduced duration of migraine attacks to one day about 2/3 of the time, a big improvement
▪ The desvenlafaxine reduced migraine frequency by ≥50% and helped both depression and
anxiety—optimal!
▪ Some scenarios for which the provider should be prepared:
▪ The combination sumatriptan-naproxen sodium does not achieve sustained pain freedom in ≥50%
of attacks—now what?
▪ The desvenlafaxine causes sexual dysfunction and insomnia—now what?
QAM=every morning.

Considerations for Next Steps
Options for EM prevention
▪ The anti-CGRP receptor monoclonal antibody erenumab and the anti-CGRP
monoclonal antibodies fremanezumab and galcanezumab are approved for
migraine prevention, both episodic and chronic
▪ They are appropriate for use in patients with a lack of success with the 2-4
categories of preventive medication and significant disability
▪ The neuromodulation devices providing external trigeminal nerve stimulation
(eTNS) and single pulse transcranial magnetic stimulation (sTMS) are both
FDA-approved for prevention of migraine and for acute treatment of
migraine and could work for both problems

Considerations for Next Steps (cont.)
Options for acute treatment of EM
▪ Sometimes other triptans such as naratriptan or frovatriptan can be effective
with or without a concomitant NSAID at achieving reduced recurrence rates
▪ DHE by self-injection or nasal spray has superior sustained benefit and
might address the issue of recurrence
▪ Weigh the risk/benefit
▪ The 2 neuromodulation devices mentioned above, plus the noninvasive
vagal nerve stimulator (nVNS) are all FDA-approved for acute treatment
of migraine

CASE 2

Case 2
▪ Ms Y. is a 45-year-old woman with depression, anxiety,
headaches since childhood, and accelerating frequency
so that she has had headache ≥15 days per month for
≥4 hours per day for ≥10 years
▪ She has migraine and associated features ≥8 days per
month, that is days of moderate to severe bilateral
throbbing pain, photo- and phonophobia, nausea, and
sometimes vomiting
▪ She is using triptans and/or OTC combination
analgesics for ≥15 days per month
MRI=magnetic resonance imaging. MRA=magnetic resonance angiogram. MRV=magnetic resonance venography. TFTs=thyroid function tests.

Case 2 (cont.)
▪ She has a history of a bleeding gastric ulcer but
is still using the aspirin-acetaminophen-caffeine
(AAC) combination tablets up to 6 per day with or
without triptans
▪ She recently took a temporary leave from work, no longer
able to focus or function on many days per month
▪ VS: BP 135/78, P 72, R 12, and the rest of her complete
medical and neurologic exam is normal
▪ MRI without contrast, MRA, MRV, TFTs, Lyme titers,
inflammatory markers all normal
MRI=magnetic resonance imaging. MRA=magnetic resonance angiogram. MRV=magnetic resonance venography. TFTs=thyroid function tests.

Case 2 (cont.)
▪ She has unsuccessfully tried at least 30 different medications
▪ Prevention trials included:
▪ Tricyclics
1. Amitriptyline
2. Nortriptyline
▪ SNRIs
3. Venlafaxine
4. Duloxetine
▪ Beta blockers
5. Propranolol
6. Metoprolol
▪ Calcium channel blockers
7. Verapamil
8. Amlodipine
▪ ACE inhibitors
9. Lisinopril
▪ ARBs
10. Candesartan
▪ AEDs
11. Topiramate
12. Zonisamide
13. Divalproex
14. Gabapentin
15. Pregabalin

Case 2 (cont.)
▪ She has unsuccessfully tried at least 30 different medications
▪ Acute trials included:
▪ Triptans
1. Sumatriptan
2. Zolmitriptan
3. Rizatriptan
4. Eletriptan
5. Naratriptan
▪ NSAIDs
6. Ibuprofen
7. Aspirin alone and AAC
8. Naproxen sodium
9. Solubilized diclofenac
10. Ketorolac
11. Meloxicam
12. Celecoxib
▪ Ergots
13. DHE nasal spray
▪ Miscellaneous
14. Tizanidine
15. Metoclopramide

What Is Her Diagnosis?
ICHD-3 Diagnostic Criteria for Chronic Migraine Without Aura
A. Headache (migraine-like or tension-type-like) on ≥15 days/month for >3 months, and
fulfilling criteria B and C
B. Occurring in a patient who has had at least 5 attacks fulfilling criteria for migraine
without aura and/or criteria for migraine with aura
C. On ≥8 days/month for >3 months, fulfilling any of the following:
1. Criteria for migraine without aura
2. Criteria for migraine with aura
3. Believed by the patient to be migraine at onset and relieved by a triptan or ergot derivative
D. Not better accounted for by another ICHD-3 diagnosis
1. Cephalalgia 2018;38(1): 1–211. 2. Bigal ME, et al. Headache. 2008;48(8):1157-1168.

What Is Her Diagnosis?
ICHD-3 Diagnostic Criteria for Medication Overuse Headache
A. Headache occurring on 15 days/month in a patient with a pre-existing headache disorder
B. Regular overuse for >3 months of one or more drugs that can be taken for acute and/or
symptomatic treatment of headache
C. Not better accounted for by another ICHD-3 diagnosis
ICHD-3 amounts
▪ Triptans, opioids, combination analgesics: ≥10 days of use per month
▪ Nonopioid analgesics, NSAIDs, acetaminophen, ergots: ≥15 days of use per month
Also known
▪ Butalbital at ≥4 days of use per month
1. Cephalalgia 2018;38(1): 1–211. 2. Bigal ME, et al. Headache. 2008;48(8):1157-1168.

What Is the Evidence for Efficacy of Chronic Migraine Prevention?▪ There are 2 RCTs of topiramate for CM prevention; she has already tried it unsuccessfully
1. Diener HC et al. Cephalalgia. 2007;27(7):814-823. 2. Silberstein SD, et al. Headache. 2007;47(2):170-180. 3. Starling AJ, et al. Cephalalgia. 2018;38(6):1038-1048. 4. Schoenen J, et al. Neurology. 2013;80(8):697-704.
FDA-approved medications
for CM
▪ OnabotulinumtoxinA
▪ Erenumab
▪ Fremanezumab
▪ Galcanezumab
FDA-approved neuromodulation
devices tested in CM
▪ sTMS
▪ (eTNS only tested in EM)

What Might Work Here?
▪ OnabotulinumtoxinA is effective and FDA-approved for CM prevention
▪ sTMS was effective in patients with 4-25 headache days per month, but not explicitly tried for
medication overuse headache
▪ The MABs work in CM prevention and lowered all acute medication use
▪ The MABs were effective in patients with 2-4 previous preventive medication trials which,
although fewer trials than this patient tried, may be a good choice here
1. Diener HC, et al. Cephalalgia. 2010;30(7):804-814. 2. Aurora SK, et al. Cephalalgia. 2010;30(7):793-803. 3. Starling AJ, et al. Cephalalgia. 2018;38(6):1038-1048. 4. Tepper SJ. Headache 2018;58 (suppl3):238-275.
5. Tepper SJ. Headache 2018;58 (suppl3):276-290.

What About a Taper?
▪ It would be better from a health standpoint for this patient to lower her acute medication intake,
especially given her gastrointestinal risk from the AACs
▪ Neither the onabotulinumtoxinA nor the MAB pivotal trials included a formal taper of the
overused medications, and triptan use fell in both; analgesic use also decreased in the MAB
studies
▪ Nonetheless, a clear taper of the triptans and AACs should be written out for this patient when
the MAB starts lowering headache frequency, which is often within 1 month

What About Acute Medication for This Patient?
▪ First and foremost, no NSAIDs or aspirin-containing compounds for acute treatment
▪ As a general rule, try to avoid prescribing medication classes that the patient is overusing
▪ Probably also best to avoid triptans as she is in sumatriptan overuse
▪ Longer-acting triptans are less likely to cause overuse headache
▪ A retry with DHE, this time with self-injection, may be in her best interest, not more than 2 days
per week, as her PRN medication
▪ eTNS, sTMS, or nVNS could be used for acute treatment and won’t cause an overuse
syndrome or the consequences of overuse
▪ The acute migraine US treatment guidelines are in
Marmura MJ, et al. Headache. 2015;55:3-20
PRN=as needed.

Conclusions on the Cases
▪ 3 classes of oral preventive medications are widely used first for prevention of EM:
antidepressants, antihypertensives, and AEDs
▪ Only valproate, topiramate, propranolol, and timolol are FDA-approved for prevention of EM
▪ Only topiramate has randomized controlled data for use in CM, and its efficacy in CM is modest
▪ OnabotulinumtoxinA, erenumab, fremanezumab, and galcanezumab have efficacy in
preventing CM, but onabotulinumtoxinA is not FDA-approved for preventing EM, while the
MABs are FDA-approved for either EM or CM
▪ eTNS and sTMS are FDA-approved for both acute and preventive treatment of migraine;
nVNS is FDA-approved for acute treatment of migraine

Q&A