Embed Size (px)
Citation preview

481EDUCATION EXHIBIT
Paul A. Sookur, MRCP • Ali M. Naraghi, FRCR • Robert R. Bleakney, FRCPC • Rosy Jalan, FRCR • Otto Chan, FRCR • Lawrence M. White, MD
A wide array of supernumerary and accessory musculature has been described in the anatomic, surgical, and radiology literature. In the vast majority of cases, accessory muscles are asymptomatic and represent incidental fi ndings at surgery or imaging. In some cases, however, accessory muscles may produce clinical symptoms. These symptoms may be related to a palpable swelling or may be the result of mass effect on neurovascular structures, typically in fi bro-osseous tunnels. In cases in which an obvious cause for such symptoms is not evident, recognition and careful evaluation of accessory muscles may aid in diagnosis and treatment.©RSNA, 2008
Accessory Muscles: Anatomy, Symptoms, and Radiologic Evaluation1
Abbreviations: ADM = abductor digiti minimi, AIN = anterior interosseous nerve, ECR = extensor carpi radialis, EDBM = extensor digitorum brevis manus, FCR = fl exor carpi radialis, FDAL = fl exor digitorum accessorius longus, FDS = fl exor digitorum superfi cialis, FHL = fl exor hal-lucis longus, FPL = fl exor pollicis longus, PAES = popliteal artery entrapment syndrome, PCI = peroneocalcaneus internus, TCI = tibiocalca-neus internus
RadioGraphics 2008; 28:481–499 • Published online 10.1148/rg.282075064 • Content Code: 1From the Department of Medical Imaging, Royal London Hospital, London, England (P.A.S., R.J.); Joint Department of Medical Imaging of University Health Network and Mount Sinai Hospital, Toronto Western Hospital, 399 Bathurst St, Toronto, ON, Canada M5T 2S8 (A.M.N., R.R.B., L.M.W.); and Department of Medical Imaging, London Independent Hospital, London, England (O.C.). Recipient of a Certifi cate of Merit award for an education exhibit at the 2006 RSNA Annual Meeting. Received April 4; revision requested June 26 and received August 14; accepted October 3. All authors have no fi nancial relationships to disclose. Address correspondence to A.M.N. (e-mail: [email protected]).
©RSNA, 2008
ONLINE-ONLYCME
See www.rsna.org/educaion/rg_cme.html
LEARNINGOBJECTIVESAfter reading this article and taking the test, the reader
will be able to:
Describe the ■
gross anatomy of the commonly occurring accessory muscles.
Identify the char- ■
acteristic imaging features of various accessory muscles.
Discuss the poten- ■
tial role of accessory muscles in symptom causation.
Note: This copy is for your personal, non-commercial use only. To order presentation-ready copies for distribution to your colleagues or clients, use the RadioGraphics Reprints form at the end of this article.
See last page
TEACHING POINTS

482 March-April 2008 RG ■ Volume 28 • Number 2
IntroductionMuscle anatomic variants are commonly encoun-tered. These variants may consist of absence of a muscle, supernumerary muscles, deviation from the normal course, or an anomalous origin or in-sertion. Accessory muscles are anatomic variants representing additional distinct muscles that are encountered along with the normal complement of muscles.
Historically, the majority of data regarding accessory musculature has been based on seren-dipitous fi ndings at surgery. However, with the advent of modern cross-sectional imaging tech-niques such as ultrasonography (US), computed tomography (CT), and magnetic resonance (MR) imaging, accessory muscles are regularly encountered and can be accurately identifi ed noninvasively.
Accessory muscles are commonly overlooked at imaging evaluation (1). Although they are typi-cally asymptomatic and encountered as incidental fi ndings, accessory muscles have been implicated as a potential source of clinical symptoms. Such symptoms are usually due to mass effect of the supernumerary muscle, with the patient present-ing with either a palpable swelling or second-ary compression of adjacent structures such as nerves, vessels, or tendons.
Cross-sectional imaging can accurately dem-onstrate accessory muscles and help differenti-ate them from other soft-tissue masses. In this article, we describe the gross anatomic and ra-diologic appearances of the normal musculature and the more commonly encountered accessory muscles in the shoulder, elbow, wrist, knee, and ankle, with emphasis on features that help distin-guish between normal and accessory muscles. In addition, we discuss and illustrate the patterns of clinical symptoms associated with specifi c acces-sory muscles.
Accessory Muscles of the ShoulderThe biceps brachii muscle has two heads: a long head, which arises from the supraglenoid tubercle within the capsule of the shoulder joint; and a short head, which lies medial to the long head and arises from the coracoid process. The two muscular bellies fuse, and a fl attened distal ten-
don attaches to the posterior margin of the radial tuberosity.
Additional heads of the biceps brachii result-ing in a three- or four-headed variant have been described. These variants are extremely rare, and the data are limited to case reports.
In a case report of a cadaveric dissection of a four-headed biceps (2), the fi rst supernumerary head arose from the humerus in the area between the lesser tuberosity and the coracobrachialis and brachialis muscles and joined the long head of the biceps at the level where the short head joined. The second supernumerary head origi-nated from the humerus at the site of insertion of the coracobrachialis and joined the biceps tendon at the bicipital aponeurosis in the distal third of the arm.
Other accessory heads have been described that originate from the intertubercular sulcus adjacent to the insertion of the pectoralis ma-jor muscle (3). A muscular slip may pass to the posterior fascia of the pronator teres muscle, forming a tunnel that encircles the median nerve and brachial artery. This entity is postulated as a potential cause of compression with ensuing symptoms.
Accessory Muscles of the Elbow
Accessory BrachialisThe brachialis arises from the anterior surface of the lower half of the shaft of the humerus and inserts into the tuberosity of the ulna and the ad-jacent surface of the coronoid process.
Figure 1. Drawing illus-trates the pos-terior surface of the elbow, with the anconeus epitrochlearis (arrow) extend-ing from the olecranon to the medial epicon-dyle superfi cial to the ulnar nerve (arrowhead).

RG ■ Volume 28 • Number 2 Sookur et al 483
An accessory brachialis originates from the medial midshaft of the humerus and the medial intermuscular septum, with a distal insertion into the common tendon of the antebrachial fl exor compartment muscles (4). The accessory bra-chialis runs medial to the elbow and crosses the median nerve and the brachial artery. The distal tendon has been observed to split and enclose the median nerve, which may result in symptoms of median nerve compression (4).
Anconeus Epitrochlearis MuscleThe anconeus epitrochlearis muscle takes the same course as the cubital tunnel retinaculum, running from the medial cortex of the olecranon to the inferior surface of the medial epicondyle (Fig 1). It runs superfi cial to the ulnar nerve and serves to keep the nerve in position. The cubital tunnel retinaculum is postulated to be the rem-nant of the anconeus epitrochlearis. The reported prevalence of the anconeus epitrochlearis from cadaveric studies is 11% (5). The anconeus epitrochlearis may be unilateral but was found to be bilateral in one of four patients with cubital tunnel syndrome in a study by Masear et al (6). The relationship to the ulnar nerve explains the association of the anconeus epitrochlearis with cubital tunnel syndrome (6,7). The anconeus epitrochlearis can be identifi ed at US (8) or, more accurately, at MR imaging (Fig 2) (7) and
needs to be distinguished from the ulnar head of the fl exor carpi ulnaris muscle, which occurs more distally and merges with the humeral head of that muscle.
Accessory Head of the Flexor Pollicis Longus MuscleThe fl exor pollicis longus (FPL) muscle arises from the anterior surface of the radius inferior to the anterior oblique line and superior to the pronator quadratus muscle, with additional fi bers arising from the interosseous membrane. At the wrist, the tendon passes deep to the fl exor reti-naculum to insert into the base of the distal pha-lanx of the thumb.
An accessory head of the FPL, or Gantzer muscle, is relatively common, with a prevalence from cadaveric studies of 45%–66% (9–11).
The origin of an accessory head of the FPL can be variable. Some studies have found the me-dial epicondyle to be the origin in 75%–85% of cases (9,11), whereas others have demonstrated the coronoid process as the most common origin (10). Other described origins of an accessory head of the FPL include the fl exor digitorum superfi cialis (FDS) muscle (11) and a dual origin from the medial humeral epicondyle and the cor-onoid process (Figs 3, 4) (9). An accessory head of the FPL inserts distally into the ulnar border of the FPL in 100% of cases (9,11) and is inner-vated by a branch of the AIN (9).
The relationship of the accessory head of the FPL to the median nerve and the AIN is impor-tant with respect to potential symptom causa-tion. There are confl icting reports in this regard, with some investigators fi nding the AIN typically coursing posterior to the muscular portion of the accessory head of the FPL (12) and others fi nd-ing the AIN coursing anterior (9). A study of 120 cadavers by Mahakkanukrauh et al (11) showed the AIN coursing anterior to the accessory head of the FPL in 13.4% of cases, lateral in 65.8%, posterior in 8.1%, and posterolateral in 12.8%. An accessory head of the FPL has been implicat-ed in compressive neuropathies of either the me-dian nerve or the AIN. Impingement on the AIN results in anterior interosseous nerve syndrome, particularly when the nerve runs deep to the muscle (11), whereas compression of the median nerve leads to pronator syndrome (9).
Figure 2. Axial T1-weighted MR im-age of the elbow shows the anconeus epi-trochlearis (arrow) extending across the cubital fossa from the medial cortex of the olecranon (∗) to the medial epicondyle (arrowhead).
TeachingPoint

484 March-April 2008 RG ■ Volume 28 • Number 2
Bifurcated Distal Biceps BrachiiThe distal insertion of the biceps brachii nor-mally consists of a tendinous insertion onto the radial tuberosity and the lacertus fi brosus, the lat-ter being an aponeurosis arising from the medial side of the tendon and continuing onto the deep fascia covering the common fl exor muscles of the forearm.
Anomalies of the insertion of the biceps brachii have been described, including a bifur-cated tendon inserting onto the radial tuberosity (13). The bifurcated distal tendon attaches via medial and lateral myotendinous units onto the radial tuberosity. Isolated complete tear of one of the myotendinous units clinically simulating a partial tear has been described (13).
Accessory Muscles of the Hand and Wrist
Volar Aspect
Accessory Flexor Digitorum Superfi cialis Indicis Muscle.—The FDS arises from humeral (common fl exor origin), ulnar, and radial heads. It extends through the forearm, dividing into su-perfi cial and deep planes, before passing through the carpal tunnel. The distal tendon to the index fi nger arises from the deep plane and inserts into the base of the middle phalanx.
An accessory FDS indicis muscle is a rare but well-described accessory muscle originating from the FDS tendon adjacent to the transverse carpal ligament and inserting into the index fi nger, typi-
cally in the region of the A1 pulley (14). Several variants of the accessory FDS indicis tendon have been reported in the literature, including a muscle belly located wholly within the palm and replacing the normal tendon. A second variant consists of a digastric muscular component with part of the muscle located in the forearm and part located in the palm. A third variant is char-acterized by a muscle belly that is located within the forearm and extends into but not beyond the carpal tunnel (15,16).
An accessory FDS with a muscular component in the palm may manifest clinically with a palpable soft-tissue mass. In cases involving a digastric component, more proximal extension of the accessory FDS can be associated with com-pression of the median nerve within the carpal tunnel (14). To our knowledge, there are no data regarding the prevalence of an accessory FDS indicis.
MR imaging has been successfully used to demonstrate an accessory FDS indicis. The anomalous muscle belly may be visualized in the palm, deep to the subcutaneous tissues and volar to the second metacarpal bone. The distal ten-don of the anomalous muscle belly may be seen extending into the fl exor tendon sheath as the superfi cial tendon (17). More proximal axial MR images through the carpal tunnel may help iden-tify the FDS tendon continuous with the muscle belly in the palm; alternatively, an additional, more proximal muscle belly may be evident in cases with digastric morphologic features (18).
Figure 4. Axial T1-weighted MR image of the proximal forearm demonstrates a prominent accessory head of the FPL (ar-row) deep to the pronator teres (∗) and medial to the anterior interosseous nerve (AIN) (arrowhead). Evaluating successive images makes it possible to distinguish an accessory muscle from the ulnar head of the pronator teres and the proximal fl exor digitorum profundus muscle.
Figure 3. Drawing illus-trates an acces-sory head of the FPL (arrow) with humeral and ul-nar origins and inserting into the ulnar border of the muscle (arrowhead).
TeachingPoint

RG ■ Volume 28 • Number 2 Sookur et al 485
Accessory Hypothenar Muscles.—The hy-pothenar eminence is composed of the abductor digiti minimi (ADM), fl exor digiti minimi, and opponens digiti minimi muscles; hence, acces-sory muscles of the hypothenar eminence will be described together. The ADM arises from the pisiform bone and fl exor carpi ulnaris and inserts into the ulnar side of the base of the proximal phalanx of the little fi nger. The fl exor digiti min-imi arises from the fl exor retinaculum and the hook of hamate. It inserts into the proximal pha-lanx with the abductor and acts to fl ex the fi fth metacarpophalangeal joint.
Of the accessory hypothenar muscles, the accessory ADM is the most common, with a prevalence of 24% (19). It originates from the antebrachial fascia, coursing anterior to the ul-nar neurovascular structures in the Guyon canal and inserting into the ADM or separately onto the ulnar aspect of the base of the proximal pha-lanx (Figs 5, 6) (20). Alternatively, the accessory muscle may originate from the palmaris longus tendon in the lower third of the forearm (19). At axial cross-sectional imaging, an accessory ADM is evident as a muscular structure anterior to the ulnar neurovascular bundle, on the radial aspect of the pisiform bone. In contrast, the ADM arises from the pisiform bone without extending ante-rior to the ulnar nerve at the level of the pisiform. Other muscles may be mistaken for an accessory ADM and include the palmaris brevis muscle,
which can be distinguished from the former ow-ing to its location distal to the pisiform bone and its insertion into the skin on the ulnar border of the palm.
An accessory fl exor digiti minimi is an ex-tremely rare variant that arises from the inter-compartmental septum on the ulnar aspect of the forearm just proximal to the wrist joint, with a distal insertion into either the proximal phalanx of the fi fth digit or the fl exor digiti minimi (21).
The relationship of these accessory muscles to the Guyon canal has been implicated in compres-sion neuropathy of the ulnar nerve at this level (20,22). An accessory ADM is still fl eshy as it crosses the Guyon canal, a characteristic that may contribute to compression of the ulnar nerve and helps identify the presence of an accessory mus-cle, since under normal circumstances no muscu-lar structures are visualized in this location.
Variations in Palmaris Longus Muscle Anatomy.—The palmaris longus muscle arises from the common fl exor origin and inserts into the palmar fascia. It consists of a short muscle proximally and a long tendon distally. The pal-maris longus is a vestigial fl exor of the wrist and is the most variable muscle in the forearm. It is com-monly used for the surgical repair of tendon tears.
The palmaris longus may have a variable ap-pearance in the forearm and wrist. It may be duplicated, digastric, entirely muscular, or ten-dinous proximally and muscular distally (reverse palmaris longus) (18). An accessory or epifascial palmaris longus is an extremely rare variant that arises from the subcutaneous fascia of the fore-arm, with a distal insertion into the superfi cial palmar aponeurosis. In an MR imaging study
Figure 5. Drawing illustrates the fl exor surface of the hand, with an accessory ADM (straight arrow) arising from the fl exor retinaculum (∗), coursing superfi cial to the ulnar nerve (arrowhead), and insert-ing into the base of the fi fth proximal pha-lanx with the ADM (curved arrow).
Figure 6. Axial T1-weighted MR image of the wrist shows an accessory ADM (ar-rowhead) superfi cial to the ulnar neurovas-cular bundle (arrow).

486 March-April 2008 RG ■ Volume 28 • Number 2
of 42 asymptomatic wrists, Zeiss and Guilliam-Haidet (19) reported a prevalence of 7% for a muscular palmaris longus, but no cases of an ac-cessory palmaris longus were identifi ed.
Palmaris longus variants may manifest clini-cally with a forearm soft-tissue mass or symptoms of compression of the median nerve (23) or ulnar nerve (24). Symptomatic cases of epifascial pal-maris longus have been successfully treated with surgical excision of the accessory muscle (25).
Epifascial palmaris longus, reverse palmaris longus, and the digastric and completely muscu-lar varieties of palmaris longus are characterized at axial cross-sectional imaging of the wrist by excess muscle tissue in the midline immediately superfi cial to the fl exor retinaculum. Imaging of the more proximal forearm may serve to fully de-lineate the morphologic features of the palmaris longus variant (18). Palmaris longus anomalies are commonly overlooked at MR imaging (25).
Flexor Carpi Radialis Brevis Vel Profundus Muscle.—There is very little literature on the rare short radiocarpal fl exor muscle known as the fl exor carpi radialis (FCR) brevis vel profundus muscle (26,27). This accessory muscle arises from the volar aspect of the distal radius, distal to the origin of the FPL. The muscle passes ante-rior to the pronator quadratus and crosses deep to the FCR. Distally, the tendon inserts onto the capitate bone and the base of the third and fourth metacarpals (Figs 7, 8). Although this rare accessory muscle has typically been described in cadaveric specimens, its position may potentially cause symptoms of carpal tunnel syndrome. To
our knowledge, there are no descriptions of the imaging characteristics of this muscle.
Dorsal Aspect
Extensor Digitorum Brevis Manus Muscle.—An extensor digitorum brevis manus (EDBM) muscle is a well-described accessory muscle that occurs on the dorsum of the hand. An EDBM is rare: In a recent study of 128 ca-davers by Rodriguez-Niedenfuhr et al (28), this accessory muscle was found in four limbs (1.6%). The muscle can be unilateral or bilateral.
The origin of an EDBM can vary, although the most common origin is the dorsal wrist
Figure 7. Drawing illus-trates the fl exor surface of the distal forearm, with an FCR bre-vis vel profundus (arrow) arising from the distal radius, traversing superfi cial to the pronator quadra-tus (∗), and pass-ing deep to the fl exor retinaculum (arrowhead).
Figure 8. FCR brevis vel profundus in a 22-year-old patient who presented with volar soft-tissue swelling. Axial T1-weighted MR image of the wrist shows no masses, but a prominent accessory muscle (straight arrow) is seen deep to the FCR (curved arrow) and superfi cial to the pronator quadratus (∗) on the radial aspect of the FPL (arrowhead).
Figure 9. Drawing illus-trates the dorsal aspect of the wrist, showing the course of the EDBM (arrow) of the index fi nger.

RG ■ Volume 28 • Number 2 Sookur et al 487
capsule deep to the extensor retinaculum (28). The muscle may also arise from the distal radius or the deep carpal fascia (29). It typically inserts onto the extensor hood of the index fi nger or middle fi nger (Fig 9) (28) but may also insert into the extensors of the fourth and fi fth fi ngers by way of either a tendon or a slip (29).
An EDBM can manifest clinically as a soft-tissue swelling on the dorsum of the hand that becomes fi rm on extension of the fi ngers. It is often clinically diagnosed as a ganglion, synovitis, or a carpal boss. An EDBM is usually painless but may occasionally be associated with exercise-induced pain or tenosynovitis of the extensor ten-dons. The EDBM tendon has been used in surgi-cal restoration of function of ruptured tendons.
At MR imaging, an EDBM typically appears as a masslike lesion with low T1 and T2 signal intensity, usually located between the second and third metacarpals, with the bulk of the muscle at the level of the carpometacarpal joints. Because of its low T1 and T2 signal intensity, the muscle may mimic a giant cell tumor of the tendon sheath (Fig 10) (30). US can be used to dem-onstrate the normal echotexture of the muscle as well as morphologic changes of the muscle upon fl exion and extension, resulting in dynamic contraction-induced protrusion of the muscle be-tween the extensor tendons (31).
Treatment of a symptomatic EDBM may in-clude extensor retinaculum release or excision of the muscle (32).
Accessory Extensor Carpi Radialis Muscle and Variations.—The extensor carpi radialis
(ECR) longus muscle originates from the distal lateral supracondylar ridge of the humerus and the lateral epicondyle and inserts into the dorsal surface of the base of the second metacarpal. The ECR brevis muscle originates from the lateral epicondyle of the humerus and the radial col-lateral ligament of the elbow and inserts into the dorsal surface of the base of the third metacarpal. The two tendons pass through the second exten-sor compartment at the wrist, located radial to the Lister tubercle.
A variety of accessory musculature related to ECR muscles has been reported in the literature, including accessory ECR brevis, ECR interme-dius, and ECR accessorius muscles.
An accessory ECR brevis arises from the medial aspect of the normal ECR brevis (33). The accessory tendon passes deep to the main tendon and enters the second extensor tunnel of the wrist. Variable insertions of the accessory ECR brevis have been described, including the base of the second metacarpal, the base of the third metacarpal, and the dorsal digital expan-sion of the index fi nger, and may occur bilaterally (33,34). An accessory ECR brevis may manifest clinically as a soft-tissue mass in the forearm that can be accurately distinguished from other masses at US and MR imaging (35). It may mimic a split tear of the ECR tendons in the sec-ond extensor tunnel, but more proximal images will demonstrate the presence of the anomalous muscle belly.
Figure 10. EDBM in a 25-year-old man who presented with a palpable swelling of the dorsal aspect of the wrist. (a, b) Sagittal T1-weighted (a) and axial T2-weighted (b) MR images of the wrist show a mass (arrowhead) that is isointense relative to muscle and cen-tered at the level of the carpometacarpal joint. (c) Longitudinal US image shows an EDBM with the characteristic muscle echotexture (arrowhead).

488 March-April 2008 RG ■ Volume 28 • Number 2
condyle. Similarly, the lateral head of the gastroc-nemius may have an aberrant origin, arising more medially from the posterior femur but maintain-ing its position lateral to the popliteal artery. An accessory slip of the medial head of the gastro-cnemius may arise from the intercondylar notch, passing between the popliteal artery and vein and inserting into the medial head of the muscle (Fig 13). An accessory slip of the lateral head of the gastrocnemius has also been described origi-nating from the posterior cortex of the distal fe-mur, medial to the lateral head. The slip courses anterolateral to the popliteal vessels, inserting into the lateral head of the gastrocnemius (Fig 14) (39,40).
An anomalous relationship between the popliteal artery and the proximal gastrocnemius may manifest clinically with PAES. PAES results
An ECR intermedius muscle originates be-tween the origins of the ECR longus and ECR brevis and inserts onto the base of the second or third metacarpal or the abductor pollicis longus muscle (Figs 11, 12). The reported prevalence of an ECR intermedius in cadaveric studies has ranged from 12% to 24%, with bilaterality in 59% of cases (36,37). When present, the tendon has been used successfully in tendon transfer pro-cedures (36,37).
The ECR accessorius muscle is an extremely rare accessory muscle that originates from the ECR longus and inserts into the abductor pollicis longus or abductor pollicis brevis muscle (38). When present, the ECR accessorius traverses the wrist through a separate fascial tunnel beneath the extensor retinaculum.
Accessory Muscles of the Knee
Accessory Slips of the Medial and Lateral Gastrocnemius MuscleThe gastrocnemius muscle has two bellies, which arise from the posterior surface of the femur just above the femoral condyles and from the adjacent capsule of the knee joint. The two bellies unite to form the Achilles tendon.
Reported variations of the origin of the medial and lateral heads of the gastrocnemius consist of anomalous origins and accessory slips. The medial head of the gastrocnemius may have an aberrant origin, arising from the region of the in-tercondylar notch rather than the medial femoral
Figure 11. Drawing illustrates an ECR in-termedius (arrow) origi-nating between the ECR brevis and ECR longus and inserting into the base of the second metacarpal.
Figure 12. Axial T1-weighted MR image of the wrist shows an incidental accessory ECR muscle (arrowhead) located between the ECR longus and ECR brevis tendons (arrows) in the second extensor compart-ment. The patient was completely asymp-tomatic in this area.
Figure 13. Drawing illus-trates the popliteal fossa, with an accessory slip of the medial head of the gas-trocnemius (ar-row) compressing the popliteal ar-tery (arrowhead).
TeachingPoint

RG ■ Volume 28 • Number 2 Sookur et al 489
around a normally situated medial head of the gastrocnemius. Type II anomaly is characterized by an anomalous medial head of the gastrocne-mius compressing the popliteal artery deep to it. In type III anomaly, the accessory slip of the medial head of the gastrocnemius forms a sling around the popliteal artery. In type IV anomaly, the popliteal artery courses deep to the popli-teus, whereas type V anomaly is characterized by concomitant involvement of the popliteal vein. Type VI involves a normally located artery that is entrapped by gastrocnemius hypertrophy. An anomalous lateral head of the gastrocnemius and an accessory slip of the lateral head have also been implicated in PAES (39).
An accessory slip of the medial head of the gastrocnemius has been found to occur in 21% of patients with PAES, and an accessory slip of the lateral head of the gastrocnemius was found in 30% of patients with PAES (39).
CT and MR imaging have been used to iden-tify such accessory slips, as well as an anomalous relationship of the popliteal vessels to the gastro-cnemius. MR angiography has proved effective in demonstrating popliteal artery occlusion and is useful in surgical planning (Fig 15) (39,40).
Tensor Fasciae Suralis MuscleA tensor fasciae suralis muscle is a very rare ac-cessory muscle. Although it may arise from the distal aspect of any of the hamstring muscles, in the majority of reported cases it originates from the distal semitendinosus muscle. It may insert into the posterior fascia of the leg, into the medial
from the occlusion of the popliteal artery upon active plantarfl exion or passive dorsifl exion of the ankle. This condition is typically encountered in young patients, who may present with symptoms of intermittent claudication following exercise. PAES has been classifi ed according to the rela-tionship of the popliteal vessels to the gastrocne-mius and popliteus muscles (41). In type I ano-maly, the popliteal artery takes a medial course
Figure 14. Popliteal artery entrapment syndrome (PAES) in a 33-year-old wom-an. Axial intermediate-weighted MR images of the knee demonstrate an accessory slip of the lateral head of the gastrocnemius (arrow) arising from the posterior aspect of the distal femur, crossing anterolateral to the popliteal vessels (arrowhead in a), and inserting into the lateral head of the gastrocnemius (∗ in b).
Figure 15. PAES caused by an anomalous ori-gin of the medial head of the gastrocnemius in a 35-year-old man. Maximum-intensity-projection MR angiographic image shows obliteration of the popliteal artery in the popliteal fossa (arrow).

490 March-April 2008 RG ■ Volume 28 • Number 2
the posteromedial capsule. MR imaging demon-strates an accessory muscle located between the popliteal vessels and the posterior knee capsule and coursing obliquely through the popliteal fossa (Fig 17). Although in this reported case the accessory muscle was asymptomatic, the authors postulated that the proximity of the muscle to the neurovascular bundle might result in compressive symptoms (46).
Accessory Muscles of the Ankle
Lateral Aspect: Ac-cessory Peroneal MusclesThe peroneus longus muscle (arising from the proximal fi bula) and the peroneus brevis muscle (arising from the lower two-thirds of the fi bula) contribute tendons, which pass behind the lateral malleolus. The peroneus brevis tendon lies more anterior and separates the peroneus longus from the peroneal groove of the distal fi bula. More distally, the peroneus longus and peroneus brevis tendons are typically separated by the peroneal tubercle of the calcaneus.
A third peroneal tendon, the peroneus tertius tendon, is encountered in 83%–95% of cases in cadaveric studies (47). The tendon and muscle are located in the anterior compartment of the leg and arise from the anterior surface of the dis-tal fi bula and the extensor digitorum longus mus-cle. The tendon passes deep to the inferior exten-sor retinaculum, either in the same compartment as the extensor digitorum longus or in a different compartment. The peroneus tertius inserts onto the base and the dorsal surface of the shaft of the
head of the gastrocnemius, or via a long thin tendon onto the superfi cial aspect of the Achilles tendon (42). A tensor fasciae suralis is located superfi cially in the popliteal fossa, between the semitendinosus and semimembranosus muscles medially and the biceps femoris muscle laterally. It is an unusual cause of a popliteal soft-tissue swelling or mass (43) and is innervated by the tibial nerve (42).
A tensor fasciae suralis can be accurately iden-tifi ed with US or MR imaging, which delineate an accessory muscle in the popliteal fossa, lat-eral to the semitendinosus tendon and posterior to the semimembranosus (Fig 16) (43,44). A muscle similar in location but arising from the semimembranosus has also been described (ac-cessory semimembranosus) (45). In practice, differentiating between these entities may be dif-fi cult, especially if the full extent of the muscle is not imaged.
Accessory PopliteusThe popliteus arises via a short tendon from the groove along the lateral cortex of the lateral femoral condyle and inserts into the postero-medial surface of the proximal tibia, above the popliteal line.
An accessory muscle termed the accessory popliteus has also been described in the radiology literature (46). This variant has a common origin with the lateral gastrocnemius and extends infero-medially deep within the popliteal fossa, passing anterior to the popliteal vessels and inserting into
Figure 16. Tensor fascia suralis in a 30-year-old man. Axial proton-density–weighted MR images show a popliteal swelling caused by an accessory muscle (straight arrow) posterior to the semimembranosus (∗ in a) and lateral to the semi-tendinosus (arrowhead in a). More inferiorly, a tensor fascia suralis is seen superfi -cial to the medial head of the gastrocnemius (curved arrow in b).

RG ■ Volume 28 • Number 2 Sookur et al 491
ranging from 13% to 26% (50,51). Radiologic studies demonstrate a similar range of prevalence, with 10% in an ankle MR imaging study (52) and 22% in a US study (53). Peroneus quartus muscles are frequently bilateral and are more commonly seen in men (52,54).
In the majority of cases, a peroneus quartus originates from the peroneus brevis. Other ori-gins that have been described include the poste-rior surface of the fi bula and the peroneus longus (54). The peroneus quartus descends medial and posterior to the other peroneal tendons (Fig 18) (52). The distal insertion of peroneus quartus tendons varies and has been classifi ed into several types (51). Insertion into the calcaneus is known as peroneocalcaneus externum and represents the most common type (54). The calcaneal at-tachment may be onto the peroneal tubercle (50) or the retrotrochlear eminence posterior to the peroneal tubercle (52). Insertion of the tendon onto the retrotrochlear eminence may lead to sig-nifi cant hypertrophy of the latter structure (52). However, other studies have found no difference in the size of the retrotrochlear eminence in per-sons with a peroneus quartus and those without (55). A peroneus quartus may also rarely insert onto the cuboid (peroneocuboideus) (50,54), the peroneus longus (peroneoperoneolongus), or the inferior peroneal retinaculum adjacent to the ret-rotrochlear eminence (54).
The peroneus digiti minimi arises from the peroneus brevis to insert via two tendons into the base and head of the fi fth metatarsal and the base of the proximal phalanx (50,52). The peroneus
fi fth metatarsal and may cause snapping over the lateral dome of the talus (48).
A large number of other accessory peroneal muscles have been described, including peroneus quartus, peroneus accessorius, peroneocalcaneus externum, and peroneus digiti minimi muscles (49). Occasionally, the term peroneus quartus is used to refer to several or even all of the ac-cessory peroneal muscles (1,50). The reported prevalence of peroneus quartus muscles varies widely, partly due to the variety of terminology used. Cadaveric studies demonstrate a prevalence
Figure 17. Accessory popliteus in a 43-year-old man who was being evaluated for an anterior cruciate ligament tear. Axial (a), sagittal (b), and coronal (c) proton-density–weighted MR images of the knee demonstrate an acces-sory popliteus (straight arrow) coursing obliquely across the popliteal fossa deep to the popliteal vessels (arrowhead). The accessory muscle courses parallel to the normal popliteus in the coronal plane (curved arrow in c).
Figure 18. Drawing illustrates the peroneocalcaneus externum type of peroneus quartus (arrowhead) aris-ing from the peroneus brevis (arrow) and inserting into the retrotrochlear eminence (∗).

492 March-April 2008 RG ■ Volume 28 • Number 2
ferentiated from a split tear by evaluating the more proximal images, which will demonstrate
an anomalous muscle a peroneus quartus may vary in size, and the
myotendinous junction may extend distally to a variable extent. In the retromalleolar region, the myotendinous unit may range from completely tendinous to completely muscular (53).
Medial Aspect
Flexor Digitorum Accessorius Longus.—The fl exor digitorum longus arises from the shaft of the tibia below the soleal line. Its tendon passes behind the medial malleolus and, in the sole, splits into four slips to insert into the distal pha-langes of the second through fi fth toes.
A fl exor digitorum accessorius longus (FDAL) originates either from the medial margin of the tibia (60) and the fascia of the deep posterior compartment, or, with equal frequency, from the lateral margin of the fi bula distal to the origin of the fl exor hallucis longus (FHL) (61). However, an FDAL can vary widely in origin, arising from any structure in the posterior compartment, in-cluding adjacent muscles such as the FHL (62).
The FDAL tendon descends posterior and su-perfi cial to the tibial nerve (63), courses beneath the fl exor retinaculum through the tarsal tunnel, and is intimately related to the posterior tibial artery and tibial nerve (61). Within the tarsal tunnel, it may contain fl eshy fi bers (62), a factor that helps identify an FDAL at MR imaging. The distal tendon inserts into the quadratus plantae
accessorius has been reported to arise from the muscular portion of the peroneus brevis, insert-ing onto the peroneus longus (56).
Similar to the other peroneal muscles, a pero-neus quartus acts predominantly as a pronator of the foot. It is commonly encountered as an asymptomatic variant but may cause lateral ankle pain or ankle instability, particularly in athletes (54). Hypertrophy of the bone attachments has been implicated in peroneal tenosynovitis (50). The presence of an extra tendon may result in crowding of tendons deep to the peroneal reti-naculum, leading to anterior subluxation, me-chanical attrition, or longitudinal tears of the peroneal tendons (50,57). In some cases, surgical excision has provided symptomatic relief (54). Peroneus quartus tendons have been used suc-cessfully for surgical repair of superior and infe-rior peroneal retinacular injuries (58).
US can help identify a peroneus quartus and its calcaneal insertion (53), but the muscle is op-timally delineated at MR imaging (59). On axial MR images, a peroneus quartus is visualized pos-teromedial or medial to the peroneus brevis and is separated from it by a fat plane (Fig 19) (52,53). The accessory tendon may be mistaken for a longitudinal split tear of the peroneal tendons. However, the accessory tendon can be dif-
Figure 19. Axial T1-weighted MR image of the ankle above the level of the tibiotalar joint shows a peroneus quartus (arrow-head) posteromedial to the peroneus lon-gus (straight arrow) and peroneus brevis (curved arrow) and separated from them by a subtle fat plane.
Figure 20. Drawing illustrates an FDAL (arrows) inserting into the quadratus plantae (arrowhead).
an anomalous muscle belly. The muscle belly
TeachingPoint

RG ■ Volume 28 • Number 2 Sookur et al 493
sory muscles within the tarsal tunnel, such as peroneocalcaneus internus (PCI) and tibiocalca-neus internus (TCI) muscles, which insert onto the calcaneus. However, demonstration of the insertion of an FDAL onto the fl exor digitorum longus may be diffi cult in some cases. MR imag-ing may also exclude other causes of tarsal tunnel syndrome, including ganglia, tumors, varicosities, and FHL tenosynovitis (Fig 22).
Peroneocalcaneus Internus.—The largest se-ries describing the MR imaging characteristics of a PCI showed the muscle to originate at the inner aspect of the lower fi bula, below the origin of the FHL, with interdigitation between these two muscles (66). A PCI descends posterior and lateral to the FHL and displaces it anteriorly
muscle or the fl exor digitorum longus tendon (Fig 20) (61,63).
An FDAL has a prevalence of 6%–8%, is more common in males, and is infrequently bilateral (61,62).
Because of the close relationship of the tendon in the tarsal tunnel to the neurovascular bundle, it is not surprising that the presence of an FDAL is associated with tarsal tunnel syndrome (63,64). An FDAL has a prevalence of up to 12.2% in patients with tarsal tunnel syndrome (65) and has also been associated with tenosynovitis of the FHL tendon (60).
An FDAL can be optimally identifi ed on axial MR images (62), which demonstrate the muscle within the tarsal tunnel, typically superfi cial to the neurovascular bundle (Fig 21). Attachment onto the fl exor digitorum longus or quadratus plantae allows differentiation from other acces-
Figure 21. Axial (a) and coronal (b) intermediate-weighted MR im-ages of the ankle show a fl eshy FDAL (straight arrow) medial to the FHL (curved arrow in a) and deep to the fl exor retinaculum (arrowhead in a). The insertion of the FDAL onto the quadratus plantae (∗ in b) is well vi-sualized in the coronal plane.
Figure 22. Axial intermediate-weighted MR images obtained in a 40-year-old patient with tarsal tunnel syndrome show an FDAL (arrowhead in a), along with fatty infi ltration of the FHL (straight ar-row in b) and soleus muscle (curved arrow in b).

494 March-April 2008 RG ■ Volume 28 • Number 2
Figure 25. Drawing illustrates an ac-cessory soleus (arrow) arising from the tibia anterior to the soleus (black ∗) and gastrocnemius (white ∗) and inserting onto the superior surface of the calca-neus anteromedial to the Achilles tendon (arrowhead).
accessory muscle relative to the neurovascular bundle may also help differentiate between an FDAL and a PCI. The latter is typically located posterior and lateral to the neurovascular bundle and separated from it by the FHL (Fig 24); in contrast, an FDAL lies immediately superfi cial to
and medially, which may cause encroachment on the neurovascular bundle as the tendons pass through the tarsal tunnel (67). Both tendons pass inferior to the sustentaculum tali, with the PCI tendon inserting onto a small tubercle on the medial aspect of the calcaneus below the susten-taculum (Fig 23).
In a study of asymptomatic volunteers, a PCI was seen in 1% of cases, with bilaterality in 75% (66).
A PCI is usually asymptomatic, since it is not directly related to the neurovascular bundle and typically becomes tendinous 2–3 cm above the tibiotalar joint. However, cases of ankle pain and limitation of movement have been described (66,67), although the exact causative mechanism is unclear. A PCI has been demonstrated in the clinical setting of posterior ankle impingement and FHL tenosynovitis (67).
MR imaging can accurately delineate the origin and insertion of a PCI. At imaging, a PCI may be diffi cult to differentiate from an FDAL, with both tendons taking a similar course through the ankle and hindfoot. Distinctive features of a PCI include insertion onto the cal-caneus, with a fat plane between the PCI and quadratus plantae. In contrast, an FDAL inserts into the fl exor digitorum longus tendon or the quadratus plantae itself. The calcaneal insertion of a PCI may be optimally evaluated on coro-nal oblique images (66). The relationship of the
Figure 23. Drawing illustrates a PCI (arrow) located posterior to the FHL (arrowhead) and inserting onto the medial surface of the calcaneus, anterior and infe-rior to the sustentaculum tali.
Figure 24. PCI in a 38-year-old man with prior lateral ligamentous reconstruc-tion. Axial intermediate-weighted MR image of the ankle shows a PCI (arrow) coursing deep to the fl exor retinacu-lum and posterolateral to the FHL (arrowhead).

RG ■ Volume 28 • Number 2 Sookur et al 495
An accessory soleus may manifest clinically as a soft-tissue mass in the posteromedial aspect of the ankle. Clinically evident accessory soleus muscles have a male predilection and commonly manifest in the 2nd and 3rd decades of life (69), a fact that may be attributable to the increase in muscle mass and activity during this period. There may be associated pain, which is typically exertional, with a higher prevalence in athletes (69,71). There are various explanations for pain associated with an accessory soleus, including development of a localized compartment syn-drome due to an increase in intrafascial pressure (71,73) or an inadequate blood supply from the posterior tibial artery (69). Alternatively, acces-sory soleus hypertrophy may cause compression of the adjacent posterior tibial nerve. Although an accessory soleus lies outside the tarsal tunnel, it has been implicated in tarsal tunnel syndrome in cases in which the muscle attaches to the medial aspect of the calcaneus (65). Symptomatic cases have been successfully treated with fasciotomy, tendon release, excision, or debulking (69,74). In a case report of an accessory soleus with congeni-tal clubfoot, Chotigavanichaya et al (72) found the talipes equinus and talipes varus deformities resistant to percutaneous Achilles tenotomy, ne-cessitating concomitant release of the accessory soleus.
An accessory soleus may be visualized at conventional radiography (Fig 26) (68), CT (Fig 27) (68,73), US (73), and MR imaging (69,71,74–76). At conventional radiography, the normal triangular appearance of the Kager fat pad anterior to the Achilles tendon is obscured
the neurovascular bundle. Occasionally, the FHL may demonstrate two tendinous slips, which may be mistaken for a PCI tendon (66).
Accessory Soleus.—The soleus lies deep to the gastrocnemius and arises from (a) the posterior aspect of the head and upper shaft of the fi bula, (b) the soleal line of the tibia, (c) the middle third of the medial border of the tibia, and (d) a fi brous band bridging its fi bular and tibial origins. The fi bers converge on a short tendon, which normally joins the deep surface of the Achilles tendon.
An accessory soleus arises from the anterior (deep) surface of the soleus or from the fi bula and soleal line of the tibia (68–70). From its ori-gin, the muscle descends anterior or anterome-dial to the Achilles tendon (Fig 25) (68,70).
Five types of accessory soleus have been de-scribed on the basis of insertion characteristics. Insertion points include the Achilles tendon, the upper surface of the calcaneus with a fl eshy muscular insertion, the superior surface of the calcaneus with a tendinous insertion, the medial aspect of the calcaneus with a fl eshy muscular insertion, and fi nally, the medial aspect of the calcaneus with a tendinous insertion (68,70,71). When the accessory muscle inserts separately into the superior surface of the calcaneus, the insertion is anterior and medial to the calcaneal insertion of the Achilles tendon (70,72). The ac-cessory soleus is innervated by the posterior tibial nerve, and the blood supply is via the posterior tibial artery (69,71).
According to cadaveric studies, an accessory soleus has a prevalence of 0.7%–5.5%, with the muscle most commonly seen as a unilateral fi nd-ing (69).
Figures 26, 27. (26) Accessory soleus in a 29-year-old man. Lateral radiograph of the ankle shows partial obliteration of the Kager fat pad. An accessory soleus (∗) is seen anterior to the Achilles tendon (arrowhead) and posterior to the FHL (arrow). (27) Coronal reformatted image of the ankle from CT data obtained with a soft-tissue algorithm shows an acces-sory soleus (∗) inferomedial to the normal soleus (arrow) with a muscular insertion onto the medial surface of the calcaneus.
TeachingPoint

496 March-April 2008 RG ■ Volume 28 • Number 2
the fl exor digitorum longus or quadratus plantae may be used as a distinguishing feature.
To our knowledge, there are no radiology re-ports on the TCI. Given its location within the tarsal tunnel and its similarities to the accessory soleus and FDAL, the TCI may be associated with tarsal tunnel syndrome.
or obliterated by a well-defi ned area of increased soft-tissue density. Cross-sectional imaging is more sensitive and specifi c in the identifi cation of an accessory soleus. The accessory muscle is demonstrated anterior to the Achilles tendon and superfi cial to the fl exor retinaculum, typically ex-tending medially to the area between the medial edge of the Achilles tendon and the medial mal-leolus (Fig 28). In some cases, MR imaging may demonstrate abnormal signal intensity, a fi nding that refl ects the presence of trauma, ischemia, or atrophy (Fig 29).
Tibiocalcaneus Internus.—There is scant literature concerning the TCI (77,78), a rare accessory muscle that arises from the medial crest of the tibia and descends deep to the fl exor retinaculum and posterior to the neurovascular structures. A TCI inserts distally onto the medial surface of the calcaneus approximately 1–2 cm anterior to the Achilles tendon insertion. The ori-gin and insertion of a TCI is similar to the type of accessory soleus that inserts onto the medial cor-tex of the calcaneus. However, the two accessory muscles can be distinguished on the basis of their location relative to the fl exor retinaculum. A TCI passes deep to the fl exor retinaculum, whereas an accessory soleus is located superfi cial to the fl exor retinaculum (Fig 30). The location of a TCI (within the tarsal tunnel and superfi cial to the neurovascular bundle) may resemble that of an FDAL. The distal insertion of an FDAL onto
Figures 28, 29. (28) Axial intermediate-weighted MR image obtained slightly cranial to the tibiotalar joint shows an accessory soleus (∗) anteromedial to the Achilles tendon (arrow) and superfi cial to the tarsal tunnel and fl exor retinaculum (arrowhead). (29) Accessory soleus in a 45-year-old woman. (a) Sagittal short inversion time inversion-recovery image of the ankle shows a tear of the Achilles tendon (arrow). (b) Axial intermediate-weighted MR image of the ankle shows an accessory soleus (arrowhead) with tendinopathy and low-grade partial tearing.
Figure 30. TCI in a 30-year-old patient with tarsal tunnel syndrome. Axial inter-mediate-weighted MR image of the ankle shows a TCI (arrow), which resembles an accessory soleus in that it is located antero-medial to the Achilles tendon and inserts onto the medial surface of the calcaneus (not shown). However, it differs from an accessory soleus in that it is located deep to the fl exor retinaculum (arrowheads). Its insertion onto the medial surface of the cal-caneus helps distinguish it from an FDAL.

RG ■ Volume 28 • Number 2 Sookur et al 497
tion to anterior interosseous nerve in Thai popula-tion. Clin Anat 2004;17:631–635.
12. Shirali S, Hanson M, Branovacki G, Gonzalez M. The fl exor pollicis longus and its relation to the anterior and posterior interosseous nerves. J Hand Surg [Br] 1998;23:170–172.
13. Sassmannshausen G, Mair SD, Blazar PE. Rupture of a bifurcated distal biceps tendon: a case report. J Bone Joint Surg Am 2004;86-A:2737–2740.
14. Elias LS, Schulter-Ellis FP. Anomalous fl exor su-perfi cialis indicis: two case reports and literature review. J Hand Surg [Am] 1985;10:296–299.
15. Probst CE, Hunter JM. A digastric fl exor digitorum superfi cialis. Bull Hosp Joint Dis 1975;36:52–57.
16. Christensen S. Anomalous muscle belly of the fl ex-or digitorum superfi cialis in two generations. Hand 1977;9:162–164.
17. Sanger JR, Krasniak CL, Matloub HS, Yousif NJ, Kneeland JB. Diagnosis of an anomalous superfi -cialis muscle in the palm by magnetic resonance imaging. J Hand Surg [Am] 1991;16:98–101.
18. Timins ME. Muscular anatomic variants of the wrist and hand: fi ndings on MR imaging. AJR Am J Roentgenol 1999;172:1397–1401.
19. Zeiss J, Guilliam-Haidet L. MR demonstration of anomalous muscles about the volar aspect of the wrist and forearm. Clin Imaging 1996;20:219–221.
20. Spiess AM, Gursel E. Entrapment of the ulnar nerve at Guyon’s canal by an accessory abductor digiti minimi muscle. Plast Reconstr Surg 2006; 117:1060–1061.
21. Wahba MY, Singh GD, Lozanoff S. An anomalous accessory fl exor digiti minimi profundus muscle: a case study. Clin Anat 1998;11:55–59.
22. Al-Qattan MM. Ulnar nerve compression at the wrist by the accessory abductor digiti minimi mus-cle: wrist trauma as a precipitating factor. Hand Surg 2004;9:79–82.
23. Tiengo C, Macchi V, Stecco C, Bassetto F, De Caro R. Epifascial accessory palmaris longus mus-cle. Clin Anat 2006;19:554–557.
24. Bozkurt MC, Tagil SM, Ersoy M, Tekdemir I. Muscle variations and abnormal branching and course of the ulnar nerve in the forearm and hand. Clin Anat 2004;17:64–66.
25. Schuurman AH, van Gils AP. Reversed palmaris longus muscle on MRI: report of four cases. Eur Radiol 2000;10:1242–1244.
26. Carleton A. Flexor carpi radialis brevis vel profun-dus. J Anat 1935;69:292–293.
27. Nakahashi T, Izumi R. Anomalous interconnection between fl exor and extensor carpi radialis brevis tendons. Anat Rec 1987;218:94–97.
28. Rodriguez-Niedenfuhr M, Vazquez T, Golano P, Parkin I, Sanudo JR. Extensor digitorum brevis manus: anatomical, radiological and clinical rele-vance—a review. Clin Anat 2002;15:286–292.
29. Cavdar S, Dogan T, Bayramicli M, Sehirli U, Yuk-sel M. An unusual variation of extensor digitorum brevis manus: a case report and literature review. J Hand Surg [Am] 1998;23:173–177.
30. Anderson MW, Benedetti P, Walter J, Steinberg DR. MR appearance of the extensor digitorum manus brevis muscle: a pseudotumor of the hand. AJR Am J Roentgenol 1995;164:1477–1479.
ConclusionsA large number of accessory muscles have been described in the surgical and radiology literature, primarily in limited case reports. The vast major-ity of these accessory muscles are asymptomatic and tend to represent incidental fi ndings at sur-gery or imaging. However, accessory muscles may result in symptoms in some cases. Symptoms may be related to a palpable swelling, and the dif-ferential diagnosis of an accessory muscle should be borne in mind when an obvious mass is not detected at imaging. Furthermore, accessory muscles may result in compression neuropathies, especially in relation to the cubital tunnel, carpal tunnel, Guyon canal, and tarsal tunnel. Careful evaluation of fi bro-osseous tunnels for an acces-sory muscle may help identify such a muscle as a causative factor, which can easily be overlooked unless accessory muscles are specifi cally sought out during the review process.
References 1. Zammit J, Singh D. The peroneus quartus muscle:
anatomy and clinical relevance. J Bone Joint Surg Br 2003;85:1134–1137.
2. Vazquez T, Rodriguez-Niedenfuhr M, Parkin I, Sanudo JR. A rare case of a four-headed biceps brachii muscle with a double piercing by the musculocutaneous nerve. Surg Radiol Anat 2003; 25:462–464.
3. Nakatani T, Tanaka S, Mizukami S. Bilateral four-headed biceps brachii muscles: the median nerve and brachial artery passing through a tunnel formed by a muscle slip from the accessory head. Clin Anat 1998;11:209–212.
4. Loukas M, Louis RG Jr, South G, Alsheik E, Christopherson C. A case of an accessory brachia-lis muscle. Clin Anat 2006;19:550–553.
5. Dellon AL. Musculotendinous variations about the medial humeral epicondyle. J Hand Surg [Br] 1986;11:175–181.
6. Masear VR, Hill JJ Jr, Cohen SM. Ulnar com-pression neuropathy secondary to the anconeus epitrochlearis muscle. J Hand Surg [Am] 1988;13: 720–724.
7. Jeon IH, Fairbairn KJ, Neumann L, Wallace WA. MR imaging of edematous anconeus epitrochlearis: another cause of medial elbow pain? Skeletal Ra-diol 2005;34:103–107.
8. Okamoto M, Abe M, Shirai H, Ueda N. Diagnos-tic ultrasonography of the ulnar nerve in cubital tunnel syndrome. J Hand Surg [Br] 2000;25: 499–502.
9. al-Qattan MM. Gantzer’s muscle: an anatomical study of the accessory head of the fl exor pollicis lon-gus muscle. J Hand Surg [Br] 1996;21:269–270.
10. Oh CS, Chung IH, Koh KS. Anatomical study of the accessory head of the fl exor pollicis longus and the anterior interosseous nerve in Asians. Clin Anat 2000;13:434–438.
11. Mahakkanukrauh P, Surin P, Ongkana N, Setha-davit M, Vaidhayakarn P. Prevalence of accessory head of fl exor pollicis longus muscle and its rela-

498 March-April 2008 RG ■ Volume 28 • Number 2
42. Tubbs RS, Salter EG, Oakes WJ. Dissection of a rare accessory muscle of the leg: the tensor fasciae suralis muscle. Clin Anat 2006;19:571–572.
43. Montet X, Sandoz A, Mauget D, Martinoli C, Bianchi S. Sonographic and MRI appearance of tensor fasciae suralis muscle, an uncommon cause of popliteal swelling. Skeletal Radiol 2002;31: 536–538.
44. Chason DP, Schultz SM, Fleckenstein JL. Tensor fasciae suralis: depiction on MR images. AJR Am J Roentgenol 1995;165:1220–1221.
45. Stoane JM, Gordon DH. MRI of an accessory semimembranosus muscle. J Comput Assist To-mogr 1995;19:161–162.
46. Duc SR, Wentz KU, Kach KP, Zollikofer CL. First report of an accessory popliteal muscle: detection with MRI. Skeletal Radiol 2004;33:429–431.
47. Witvrouw E, Borre KV, Willems TM, Huysmans J, Broos E, De Clercq D. The signifi cance of per-oneus tertius muscle in ankle injuries: a prospective study. Am J Sports Med 2006;34:1159–1163.
48. Sammarco GJ, Henning C. Peroneus tertius mus-cle as a cause of snapping and ankle pain: a case report. Am J Sports Med 2007;35:1377–1379.
49. Best A, Giza E, Linklater J, Sullivan M. Posterior impingement of the ankle caused by anomalous muscles: a report of four cases. J Bone Joint Surg Am 2005;87:2075–2079.
50. Sobel M, Levy ME, Bohne WH. Congenital varia-tions of the peroneus quartus muscle: an anatomic study. Foot Ankle 1990;11:81–89.
51. Hecker P. Study on the peroneus of the tarsus. Anat Rec 1923;26:79–82.
52. Cheung YY, Rosenberg ZS, Ramsinghani R, Bel-tran J, Jahss MH. Peroneus quartus muscle: MR imaging features. Radiology 1997;202:745–750.
53. Chepuri NB, Jacobson JA, Fessell DP, Hayes CW. Sonographic appearance of the peroneus quartus muscle: correlation with MR imaging appearance in seven patients. Radiology 2001;218:415–419.
54. Donley BG, Leyes M. Peroneus quartus muscle: a rare cause of chronic lateral ankle pain. Am J Sports Med 2001;29:373–375.
31. Ouellette H, Thomas BJ, Torriani M. Using dy-namic sonography to diagnose extensor digitorum brevis manus. AJR Am J Roentgenol 2003;181: 1224–1226.
32. Gama C. Extensor digitorum brevis manus: a re-port on 38 cases and a review of the literature. J Hand Surg [Am] 1983;8:578–582.
33. Gumusalan Y, Kalaycioglu A, Yazar F, Arifoglu Y, Sinav A. Accessory extensor carpi radialis muscle and interconnecting muscular bundle. Acta Anat (Basel) 1997;159:57–60.
34. Khaledpour C, Schindelmeiser J. Atypical course of the rare accessory extensor carpi radialis muscle. J Anat 1994;184(pt 1):161–163.
35. Vessal S, Rai SB. Accessory extensor carpi radialis brevis muscle, a pseudomass of the distal forearm: ultrasound and MR appearances—case report and literature review. Clin Radiol 2006;61:442–445.
36. Albright JA, Linburg RM. Common variations of the radial wrist extensors. J Hand Surg [Am] 1978;3:134–138.
37. Wood VE. The extensor carpi radialis intermedius tendon. J Hand Surg [Am] 1988;13:242–245.
38. Hong Michael K-Y, Hong Matthew K-H. An un-common form of the rare extensor carpi radialis accessorius. Ann Anat 2005;187:89–92.
39. Kim HK, Shin MJ, Kim SM, Lee SH, Hong HJ. Popliteal artery entrapment syndrome: morpho-logical classifi cation utilizing MR imaging. Skeletal Radiol 2006;35:648–658.
40. Elias DA, White LM, Rubenstein JD, Christakis M, Merchant N. Clinical evaluation and MR imaging features of popliteal artery entrapment and cystic adventitial disease. AJR Am J Roentgenol 2003; 180:627–632.
41. Rich NM, Collins GJ Jr, McDonald PT, Kozloff L, Clagett GP, Collins JT. Popliteal vascular entrap-ment: its increasing interest. Arch Surg 1979;114: 1377–1384.

RG ■ Volume 28 • Number 2 Sookur et al 499
67. Seipel R, Linklater J, Pitsis G, Sullivan M. The peroneocalcaneus internus muscle: an unusual cause of posterior ankle impingement. Foot Ankle Int 2005;26:890–893.
68. Lorentzon R, Wirell S. Anatomic variations of the accessory soleus muscle. Acta Radiol 1987; 28:627–629.
69. Brodie JT, Dormans JP, Gregg JR, Davidson RS. Accessory soleus muscle: a report of 4 cases and review of literature. Clin Orthop Relat Res 1997;337:180–186.
70. Kendi TK, Erakar A, Oktay O, Yildiz HY, Saglik Y. Accessory soleus muscle. J Am Podiatr Med Assoc 2004;94:587–589.
71. Yu JS, Resnick D. MR imaging of the accessory so-leus muscle appearance in six patients and a review of the literature. Skeletal Radiol 1994;23:525–528.
72. Chotigavanichaya C, Scaduto AA, Jadhav A, Ot-suka NY. Accessory soleus muscle as a cause of resistance to correction in congenital club foot: a case report. Foot Ankle Int 2000;21:948–950.
73. Bianchi S, Abdelwahab IF, Oliveri M, Mazzola CG, Rettagliata P. Sonographic diagnosis of acces-sory soleus muscle mimicking a soft tissue tumor. J Ultrasound Med 1995;14:707–709.
74. Featherstone T. MRI diagnosis of accessory soleus muscle strain. Br J Sports Med 1995;29:277–278.
75. Ekstrom JE, Shuman WP, Mack LA. MR imaging of accessory soleus muscle. J Comput Assist To-mogr 1990;14:239–242.
76. Buschmann WR, Cheung Y, Jahss MH. Magnetic resonance imaging of anomalous leg muscles: ac-cessory soleus, peroneus quartus and the fl exor digitorum longus accessorius. Foot Ankle 1991;12: 109–116.
77. Sarrafi an S. Anatomy of the foot and ankle. Phila-delphia, Pa: Lippincott, 1983; 221–223.
78. Hecker P. Etude sur le peronier du tarse: variations des peroniers lateraux. Arch Anat Histol Embryol 1924;3:327–359.
55. Saupe N, Mengiardi B, Pfi rrmann CW, Vienne P, Seifert B, Zanetti M. Anatomic variants associated with peroneal tendon disorders: MR imaging fi nd-ings in volunteers with asymptomatic ankles. Radi-ology 2007;242:509–517.
56. Buschmann WR. Congenital variations of the peroneus quartus muscle: an anatomical study by Sobel et al. Foot Ankle 1991;11:342.
57. Trono M, Tueche S, Quintart C, Libotte M, Bail-lon J. Peroneus quartus muscle: a case report and review of the literature. Foot Ankle Int 1999;20: 659–662.
58. Mick CA, Lynch F. Reconstruction of the peroneal retinaculum using the peroneus quartus: a case re-port. J Bone Joint Surg Am 1987;69:296–297.
59. Wang XT, Rosenberg ZS, Mechlin MB, Schweit-zer ME. Normal variants and diseases of the peroneal tendons and superior peroneal retinacu-lum: MR imaging features. RadioGraphics 2005; 25:587–602.
60. Eberle CF, Moran B, Gleason T. The accessory fl exor digitorum longus as a cause of fl exor hallucis syndrome. Foot Ankle Int 2002;23:51–55.
61. Peterson DA, Stinson W, Lairmore JR. The long accessory fl exor muscle: an anatomical study. Foot Ankle Int 1995;16:637–640.
62. Cheung YY, Rosenberg ZS, Colon E, Jahss M. MR imaging of fl exor digitorum accessorius longus. Skeletal Radiol 1999;28:130–137.
63. Gumusalan Y, Kalaycioglu A. Bilateral accessory fl exor digitorum longus muscle in man. Ann Anat 2000;182:573–576.
64. Ho VW, Peterfy C, Helms CA. Tarsal tunnel syn-drome caused by strain of an anomalous muscle: an MRI-specifi c diagnosis. J Comput Assist To-mogr 1993;17:822–823.
65. Kinoshita M, Okuda R, Morikawa J, Abe M. Tar-sal tunnel syndrome associated with an accessory muscle. Foot Ankle Int 2003;24:132–136.
66. Mellado JM, Rosenberg ZS, Beltran J, Colon E. The peroneocalcaneus internus muscle: MR im-aging features. AJR Am J Roentgenol 1997;169: 585–588.
This article meets the criteria for 1.0 AMA PRA Category 1 CreditTM. To obtain credit, see www.rsna.org/education/rg_cme.html.

RG Volume 28 • Volume 2 • March-April 2008 Sookur et al
Accessory Muscles: Anatomy, Symptoms, and Radiologic Evaluation
Paul A. Sookur, MRCP, et al
Page 483 The relationship to the ulnar nerve explains the association of the anconeus epitrochlearis with cubital tunnel syndrome (6,7). Page 484 In cases involving a digastric component, more proximal extension of the accessory FDS can be associated with compression of the median nerve within the carpal tunnel (14). Page 488 An anomalous relationship between the popliteal artery and the proximal gastrocnemius may manifest clinically with PAES. Page 492 The accessory tendon may be mistaken for a longitudinal split tear of the peroneal tendons. However, the accessory tendon can be differentiated from a split tear by evaluating the more proximal images, which will demonstrate an anomalous muscle belly. Page 495 Occasionally, the FHL may demonstrate two tendinous slips, which may be mistaken for a PCI tendon (66).
RadioGraphics 2008; 28:481–499 • Published online 10.1148/rg.282075064 • Content Code:

RadioGraphics 2008 This is your reprint order form or pro forma invoice
(Please keep a copy of this document for your records.)
Author Name _______________________________________________________________________________________________ Title of Article _______________________________________________________________________________________________ Issue of Journal_______________________________ Reprint # _____________ Publication Date ________________ Number of Pages_______________________________ KB # _____________ Symbol RadioGraphics Color in Article? Yes / No (Please Circle) Please include the journal name and reprint number or manuscript number on your purchase order or other correspondence. Order and Shipping Information Reprint Costs (Please see page 2 of 2 for reprint costs/fees.) ________ Number of reprints ordered $_________ ________ Number of color reprints ordered $_________ ________ Number of covers ordered $_________ Subtotal $_________ Taxes $_________ (Add appropriate sales tax for Virginia, Maryland, Pennsylvania, and the District of Columbia or Canadian GST to the reprints if your order is to be shipped to these locations.) First address included, add $32 for each additional shipping address $_________
TOTAL $_________
Shipping Address (cannot ship to a P.O. Box) Please Print Clearly Name ___________________________________________ Institution _________________________________________ Street ___________________________________________ City ____________________ State _____ Zip ___________ Country ___________________________________________ Quantity___________________ Fax ___________________ Phone: Day _________________ Evening _______________ E-mail Address _____________________________________ Additional Shipping Address* (cannot ship to a P.O. Box) Name ___________________________________________ Institution _________________________________________ Street ___________________________________________ City ________________ State ______ Zip ___________
Country _________________________________________ Quantity __________________ Fax __________________ Phone: Day ________________ Evening ______________ E-mail Address ____________________________________ * Add $32 for each additional shipping address
Payment and Credit Card Details Enclosed: Personal Check ___________ Credit Card Payment Details _________ Checks must be paid in U.S. dollars and drawn on a U.S. Bank. Credit Card: __ VISA __ Am. Exp. __ MasterCard Card Number __________________________________ Expiration Date_________________________________ Signature: _____________________________________ Please send your order form and prepayment made payable to: Cadmus Reprints P.O. Box 751903 Charlotte, NC 28275-1903 Note: Do not send express packages to this location, PO Box.
FEIN #:541274108
Invoice or Credit Card Information Invoice Address Please Print Clearly Please complete Invoice address as it appears on credit card statement Name ____________________________________________ Institution ________________________________________ Department _______________________________________ Street ____________________________________________ City ________________________ State _____ Zip _______ Country ___________________________________________ Phone _____________________ Fax _________________ E-mail Address _____________________________________ Cadmus will process credit cards and Cadmus Journal
Services will appear on the credit card statement. If you don’t mail your order form, you may fax it to 410-820-9765 with
your credit card information. Signature __________________________________________ Date _______________________________________ Signature is required. By signing this form, the author agrees to accept the responsibility for the payment of reprints and/or all charges described in this document.
Reprint order forms and purchase orders or prepayments must be received 72 hours after receipt of form either by mail or by fax at 410-820-9765. It is the policy of Cadmus Reprints to issue one invoice per order.
Please print clearly.
Page 1 of 2 RB-9/26/07
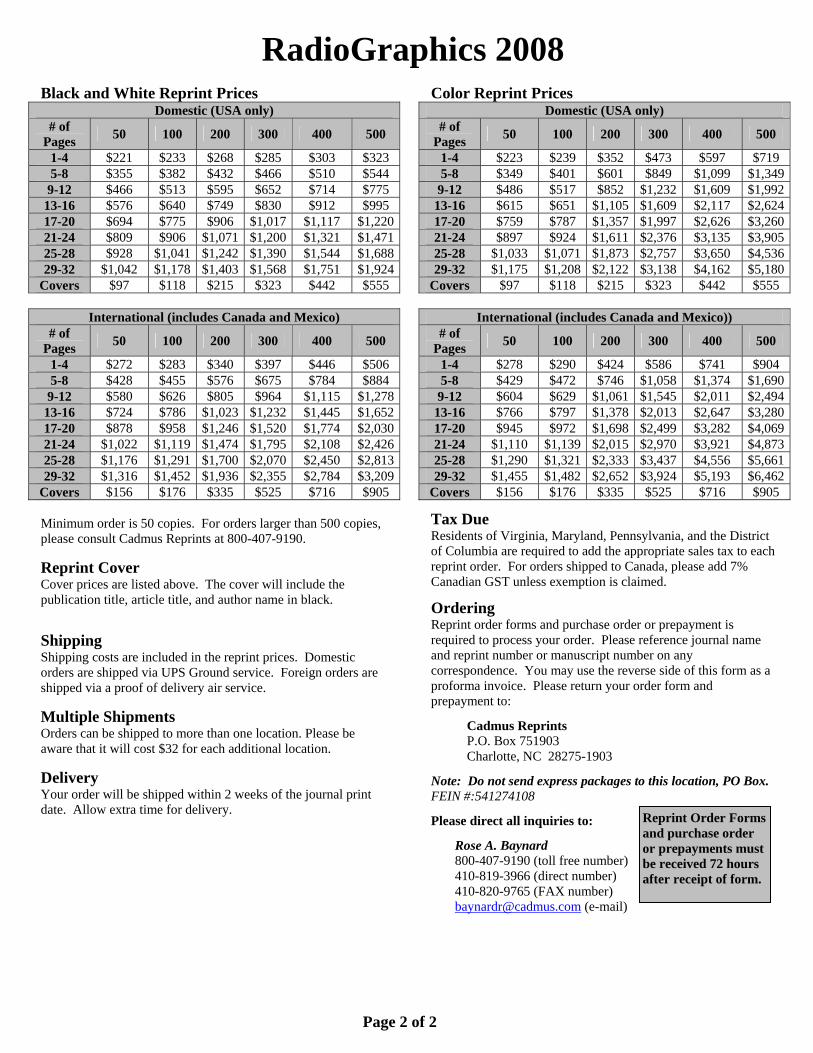
RadioGraphics 2008 Black and White Reprint Prices
Domestic (USA only) # of
Pages 50 100 200 300 400 500
1-4 $221 $233 $268 $285 $303 $323 5-8 $355 $382 $432 $466 $510 $544 9-12 $466 $513 $595 $652 $714 $775
13-16 $576 $640 $749 $830 $912 $995 17-20 $694 $775 $906 $1,017 $1,117 $1,22021-24 $809 $906 $1,071 $1,200 $1,321 $1,47125-28 $928 $1,041 $1,242 $1,390 $1,544 $1,68829-32 $1,042 $1,178 $1,403 $1,568 $1,751 $1,924
Covers $97 $118 $215 $323 $442 $555
International (includes Canada and Mexico) # of
Pages 50 100 200 300 400 500
1-4 $272 $283 $340 $397 $446 $506 5-8 $428 $455 $576 $675 $784 $884 9-12 $580 $626 $805 $964 $1,115 $1,278
13-16 $724 $786 $1,023 $1,232 $1,445 $1,65217-20 $878 $958 $1,246 $1,520 $1,774 $2,03021-24 $1,022 $1,119 $1,474 $1,795 $2,108 $2,42625-28 $1,176 $1,291 $1,700 $2,070 $2,450 $2,81329-32 $1,316 $1,452 $1,936 $2,355 $2,784 $3,209
Covers $156 $176 $335 $525 $716 $905 Minimum order is 50 copies. For orders larger than 500 copies, please consult Cadmus Reprints at 800-407-9190. Reprint Cover Cover prices are listed above. The cover will include the publication title, article title, and author name in black. Shipping Shipping costs are included in the reprint prices. Domestic orders are shipped via UPS Ground service. Foreign orders are shipped via a proof of delivery air service. Multiple Shipments Orders can be shipped to more than one location. Please be aware that it will cost $32 for each additional location. Delivery Your order will be shipped within 2 weeks of the journal print date. Allow extra time for delivery.
Color Reprint Prices
Domestic (USA only) # of
Pages 50 100 200 300 400 500
1-4 $223 $239 $352 $473 $597 $719 5-8 $349 $401 $601 $849 $1,099 $1,3499-12 $486 $517 $852 $1,232 $1,609 $1,992
13-16 $615 $651 $1,105 $1,609 $2,117 $2,62417-20 $759 $787 $1,357 $1,997 $2,626 $3,26021-24 $897 $924 $1,611 $2,376 $3,135 $3,90525-28 $1,033 $1,071 $1,873 $2,757 $3,650 $4,53629-32 $1,175 $1,208 $2,122 $3,138 $4,162 $5,180
Covers $97 $118 $215 $323 $442 $555
International (includes Canada and Mexico)) # of
Pages 50 100 200 300 400 500
1-4 $278 $290 $424 $586 $741 $904 5-8 $429 $472 $746 $1,058 $1,374 $1,6909-12 $604 $629 $1,061 $1,545 $2,011 $2,494
13-16 $766 $797 $1,378 $2,013 $2,647 $3,28017-20 $945 $972 $1,698 $2,499 $3,282 $4,06921-24 $1,110 $1,139 $2,015 $2,970 $3,921 $4,87325-28 $1,290 $1,321 $2,333 $3,437 $4,556 $5,66129-32 $1,455 $1,482 $2,652 $3,924 $5,193 $6,462
Covers $156 $176 $335 $525 $716 $905 Tax Due Residents of Virginia, Maryland, Pennsylvania, and the District of Columbia are required to add the appropriate sales tax to each reprint order. For orders shipped to Canada, please add 7% Canadian GST unless exemption is claimed. Ordering Reprint order forms and purchase order or prepayment is required to process your order. Please reference journal name and reprint number or manuscript number on any correspondence. You may use the reverse side of this form as a proforma invoice. Please return your order form and prepayment to: Cadmus Reprints P.O. Box 751903 Charlotte, NC 28275-1903 Note: Do not send express packages to this location, PO Box. FEIN #:541274108 Please direct all inquiries to:
Rose A. Baynard 800-407-9190 (toll free number) 410-819-3966 (direct number) 410-820-9765 (FAX number)
[email protected] (e-mail)
Reprint Order Forms and purchase order or prepayments must be received 72 hours after receipt of form.
Page 2 of 2





























