Embed Size (px)
Citation preview

Prepared by Jessica White Senior Podiatrist, Sydney Local Health District
Access to High Risk Foot Care:
Who is referring and who is not?

Acknowledgements & Ethical approval
• This small quality audit did not require ethical approval based of Local Ethics Committee Policy

Background High Risk Foot Services are pivotal in the
management of diabetes-related ulceration2
Represent a key strategy for avoidance of unnecessary hospitalisation and amputation2
Evidenced based guidelines support a co-ordinated multidisciplinary service3
Specialised Multidisciplinary (MDT) High Risk Foot Services have been established in most major metropolitan hospitals1

International, National and State Guidelines
Figure 1. International Working Group on the Diabetic Foot
Figure 2. NHMRC Guidelines Figure 3. NSW State Guidelines

MDT Management & which patients are referred to a HRFS MDT management is of necessity in circumstances where:
Ulcers probe to tendon, joint or bone
Ulcers which fail to reduce in size after four weeks
Ischaemia
Ascending cellulitis
Limb or life threatening sepsis +/- critical limb ischaemia12

Diabetic Foot Ulcer Risk Factors
‘Treatment delay’ or ‘Wound duration’ have been identified as risk factors for:
Failure of wound healing and amputation6
Associated with increased wound size6
Poorer outcomes6
Wounds that present within an earlier time frame are “prognostically favourable”7
Figure 4. Clinical Risk Factors of DFU A Clinical Practice Guidelines Frykberg, R. (2006)_

‘Time to Presentation’ = ‘Ulcer Duration’
‘Time to Presentation’ i.e. ‘Ulcer Duration’ has been reinforced as a key performance indicator for HRFS1 and in grading systems
Local data has shown increased ulcer severity with delayed referral1
Diabetes Centre Royal Prince Alfred Hospital 2012-2013

Treatment Delay implications
Retrospective audit 75% of patients admitted to a major tertiary hospital with a diabetic foot infection had no contact with the MDT High Risk Foot Service9.
Lower extremity amputation increased five-fold when severe infection and no contact with the MDT High Risk Foot Service occurred in combination9.

Case Study
Wound Duration – 3 months
Wound Duration – 4 months

Case Study
Wound Duration 12 months 8 weeks post treatment

Audit Question/Aims What is the time to presentation at the Concord
Hospital High Risk Foot Service?
Who is the source of formal referral to the Concord Hospital High Risk Foot Service ?
What is the percentage of general practitioner referral to the service?

Methodology A retrospective study design was employed at the Concord
Hospital High Risk Foot Service
The source, category and percentage of referrals to the Concord Hospital High Risk Foot Service was captured for 84 patients from February 2014 using medical records
Percentage of referring GP’s was achieved by cross-referencing GP referrals with the number of GPs within the Foot service catchment areas
Time to presentation was measured from the patients recollection of ulcer presentation to first foot service visit

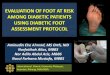
Results Source of referral % (n)
General Practitioner 36% (30)
Vascular Consultant 27% (23)
Private Podiatrist 18% (15)
District Nursing 6% (5)
Other Specialists 13% (11)
Total 84
Time to presentation days Mean 74

Discussion
Vascular Consultant referrals – high
General practitioner referrals - low

Discussion and next steps
Time to presentation is of concern
High Risk Foot Service must promulgate existence to referrers and provide accessible referral pathways
Strategies to overcome the issue must also focus on engaging with Primary Health Networks

Treatment Delay
Reasons for treatment delay most frequently is attributed to patient behaviour1
Some delay may be explained to health professional behaviours1
Eurodiale Study 27% of patients with DFU had been treated for 3 months before referral to a specialised MDT foot service8
50% had been treated by primary care physician8

References 1. Nube, V. et al. 2016. Hard to heal diabetes-related foot ulcers: current challenges and
future prospects. In Press
2. NHMRC. 2011. National Evidence-Based Guideline on Prevention, Identification, and Management of Foot Complications in Diabetes (Part of the Guidelines on Management of Type 2 Diabetes) [Online]. Melbourne: National Health and Medical Research Council. Available at: http://www.nhmrc.gov.au/_files_nhmrc/publications/attachments/diabetes_foot_full_guideline_23062011.pdf [Accessed: 3/3/2016].
3. IWGDF. 2007. Practical guidelines on the management and prevention of the diabetic foot [Online]. International Working Group on the Diabetic Foot Available at: http://www.iwgdf.org/index [Accessed: 2/3/2016].
4. ACI. 2014. High Risk Foot Service Guidelines. Available at: https://www.aci.health.nsw.gov.au/__data/assets/pdf_file/0004/248323/ACI_Standards_for_High_Risk_Foot_Services.pdf [Accessed: 2/3/2016].
5. Frykberg, R et al. 2006. A Clinical Practice Guideline. The Journal of Foot and Ankle. 45(5), pp.1-66

References 6. Prompers, L. et al. 2008. Prediction of Outcome in Individuals with Diabetic Foot Ulcers: focus on the differences between individuals with and without Peripheral Arterial Disease. The EURODIALE Study. Diabetologia. 51, pp. 747-55.
7. Margolis, D. et al. 2005. Healing diabetic neuropathic foot ulcers: are we getting better? Diabetic Medicine. 22(2), pp. 172-176.
8. Prompers, L. et al. 2008. Delivery of care top diabetic patients with foot ulcers in daily practice: results of The EURODIALE Study, a prospective cohort. Diabetes Medicine 25(6), pp. 700-707.
9. Plusch, D. et al. 2015. Primary care referral to multidisciplinary high risk foot services – too few, too late. Journal of Foot and Ankle Research. 8(62), pp. 1-13.
10. Sanders, A. Patient and professional delay in the referral trajectory of patients with diabetic foot ulcers. Diabetes Research and Clinical Practice. 102(2), pp.105-111.
11. Beckert, S. et al. 2009. M.A.I.D. A Prognostic Score Estimating Probablity of Healing in Chronic Lower Extremity Wounds. Annals of Surgery. 249(4), pp.677-681
12. Bergin, S. et al. 2012. Australian Diabetes Foot Network: management of diabetes-related foot ulceration – a clinical update. Med J Aust. 197(4), 226-229