Embed Size (px)
DESCRIPTION
Access to Controlled Medicines. Willem Scholten, PharmD, MPA Team Leader, Access to Controlled Medicines, World Health Organization, Geneva, Switzerland TECHNICAL BRIEFING SEMINAR Geneva, 29 October – 2 November 2012. Overview. The global pain management crisis Causes of the problem - PowerPoint PPT Presentation
Citation preview

Access to Controlled Medicines
Willem Scholten, PharmD, MPATeam Leader, Access to Controlled Medicines,World Health Organization, Geneva, Switzerland
TECHNICAL BRIEFING SEMINAR Geneva, 29 October – 2 November 2012

Access to Controlled Medicines | TECHNICAL BRIEFING SEMINAR Geneva, 31 Oct 2012 2 |
Overview
The global pain management crisis
Causes of the problem
Working methods for improvement– Including WHO Policy guidelines

Access to Controlled Medicines | TECHNICAL BRIEFING SEMINAR Geneva, 31 Oct 2012 3 |
Uses of Controlled Medicines
– Ergometrine and ephedrine:
emergency obstetrics
– Benzodiazepines: anxiolytics, hypnotics, antiepileptics
– Phenobarbital: antiepileptic
– Opioid analgesics: e. g. morphinemoderate and severe pain
– Long-acting opioid agonists:
methadone, buprenorphinetreatment of opioid dependence

Is there a crisis?

Access to Controlled Medicines | TECHNICAL BRIEFING SEMINAR Geneva, 31 Oct 2012 5 |
Inequality
93.8% of all (licit) morphine consumption by 21.8% of the world population (INCB 2010, Data for 2009)
4.7 billion people live in countries where medical opioid consumption is near to zero (on a total world population of 6.5 billion) (Seya et al. 2011, Data for 2006)

Access to Controlled Medicines | TECHNICAL BRIEFING SEMINAR Geneva, 31 Oct 2012 6 |
Other Controlled Medicines
Opioid analgesics best documented. Also access problems with other controlled medicines
Opioid agonist treatment of opioid dependence:– World-wide coverage: 8% of patients only
Phenobarbital– 80% of epilepsy patients in Africa have no access
Ketamine !!!!!!!!!!!– Upcoming surgery/anaesthesia crisis world-wide

Access to Controlled Medicines | TECHNICAL BRIEFING SEMINAR Geneva, 31 Oct 2012 7 |
Consumption increase
Global consumption of strong opioids rose from – 1.82 mg/capita of Morphine Equivalents (1980) to– 59.66 mg / capita (2009)(Pain & Policy Studies Group, University of Wisconsin)
Increase is faster since the introduction of the Three-Step Ladder of Cancer Pain Relief (WHO, 1986)
Most of increase in industrialized countries

Access to Controlled Medicines | TECHNICAL BRIEFING SEMINAR Geneva, 31 Oct 2012 8 |
Patients affected (world wide, annually)
Cancer pain patients untreated 5.4 million
HIV pain patients untreated 1 million
Lethal injuries 0.8 million
Surgery 8-40 million

Access to Controlled Medicines | TECHNICAL BRIEFING SEMINAR Geneva, 31 Oct 2012 9 |
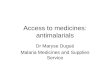
Adequacy Consumption of Opioid Analgesics (2007)
from: Seya MJ et al, J Pain & Pall Care Pharmacother 2011;25:6-18

Access to Controlled Medicines | TECHNICAL BRIEFING SEMINAR Geneva, 31 Oct 2012 10 |
Adequacy of Consumption Measure (ACM)
≥1 Adequate
0.3 – 1 Moderate
0.1 – 0.3 Low
0.03 – 0.1 Very Low
< 0.03 "No" consumption
Logarithmic scale!!!

Access to Controlled Medicines | TECHNICAL BRIEFING SEMINAR Geneva, 31 Oct 2012 11 |
Adequacy as a function of development
-5.00
-4.00
-3.00
-2.00
-1.00
0.00
1.00
0.0 0.1 0.2 0.3 0.4 0.5 0.6 0.7 0.8 0.9 1.0
HDI
log
(AC
M)
Data for 2006

Access to Controlled Medicines | TECHNICAL BRIEFING SEMINAR Geneva, 31 Oct 2012 12 |
Method for ACM
Based on– Consumption of all strong opioids (INCB statistics 2006)– Morbidity (HIV, cancer, lethal injuries)– Benchmark: average of Top-20 Human Develop Index
Method for calculating long term needs Long term targets for countries
– Unsuitable for accurate calculation of short term needs
A first comparison between the consumption of and the need for opioid analgesics at country, regional and global levels
Seya MJ et al, J Pain and Pall Care Pharmacother, 2011;25:6-18

Access to Controlled Medicines | TECHNICAL BRIEFING SEMINAR Geneva, 31 Oct 2012 13 |
ACM Benchmark
No generally accepted Good per Capita Consumption Level
Assumption: most developed countries are near to "good"
Average of " Top–x " from Human Development Index (HDI) can be used as benchmark
– Choice of x is arbitrary – but major impact on outcome!
-5.00
-4.00
-3.00
-2.00
-1.00
0.00
1.00
0.0 0.1 0.2 0.3 0.4 0.5 0.6 0.7 0.8 0.9 1.0
HDIlo
g (A
CM)

Access to Controlled Medicines | TECHNICAL BRIEFING SEMINAR Geneva, 31 Oct 2012 14 |
Adequacy of opioid consumption(x million people)*
World WPRO SEARO EURO EMRO AMRO AFRO
464 0 0 129 0 335 0 Adequate
252 25 0 228 0 0 0 Moderate
255 128 0 127 0 0 0 Low
457 79 0 94 77 206 1 Very low
4718 151 172 283 400 304 503 No cons.
433 22 2 26 64 49 270 No data6580 1763 1721 887 540 895 774 Total
*Number of people living in countries where opioid consumption is…

Access to Controlled Medicines | TECHNICAL BRIEFING SEMINAR Geneva, 31 Oct 2012 15 |
Global need to treat all pain
Current global consumption of strong opioids:
213 000 kg morphine equivalents (2006)
Needed to treat all pain adequately:
1 292 000 kg morphine equivalents
Seya MJ et al., J of Pain and Palliative CarePharmacotherapy; 2011;25:6-18

Access to Controlled Medicines | TECHNICAL BRIEFING SEMINAR Geneva, 31 Oct 2012 16 |
Validation?
For the Netherlands:
ACM: 51 % (Seya et al.)
43% of chronic non-cancer pain patients report not to receive pain treatment
79% of patients believe their pain is inadequately treatedBekkering GE et al, Epidemiology of chronic pain and its treatment in the Netherlands. The Netherlands J of Med. 2011; 69(3): 141 – 152 (Systematic review)
Studies for other European countries on their way; this will allow validation of ACM-method

Treatment of opioid dependence

Access to Controlled Medicines | TECHNICAL BRIEFING SEMINAR Geneva, 31 Oct 2012 18 |
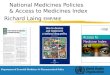
Availability of MMT/BMT

Access to Controlled Medicines | TECHNICAL BRIEFING SEMINAR Geneva, 31 Oct 2012 19 |
References
BM Mathers, Degenhardt L, Ali H et al,. HIV Prevention, treatment, and care services for people who inject drugs; a systematic revie of global, regional, and national coverage.The Lancet 2010; 375: 1014 – 28.
BM Mathers, Degenhardt L, Phillips B et al. Global epidemiology of injecting drug use and HIV among people who inject drugs: a systematic review. The Lancet (www.thelancet.com) Published online September 24, 2008 DOI:10.1016/S0140-6736(08)61311-2

Why do people do this one to another?

Access to Controlled Medicines | TECHNICAL BRIEFING SEMINAR Geneva, 31 Oct 2012 21 |
Because they have…
Excessive fear for dependence
Excessive fear for diversion
Neglected and ignored medical needs

Access to Controlled Medicines | TECHNICAL BRIEFING SEMINAR Geneva, 31 Oct 2012 22 |
Why do these barriers exist and what are they?
One century of drug control– 23 January 1912, The Hague: first Opium Convention
Focus has been on prevention of – abuse, – dependence and – crime related to trafficking
Medical and scientific supply "forgotten"

Access to Controlled Medicines | TECHNICAL BRIEFING SEMINAR Geneva, 31 Oct 2012 23 |
Preamble Single Convention
Single Convention on Narcotic Drugs (1961; as amended)
Recognizing that the medical use of narcotic drugs continues to be indispensable for the relief of pain and suffering and that adequate provision must be made to ensure the availability of narcotic drugs for such purposes …

Barriers frequently encountered

Access to Controlled Medicines | TECHNICAL BRIEFING SEMINAR Geneva, 31 Oct 2012 25 |
Categories of barriers
Legislation and Policy
Knowledge
Attitudes – Health-Care Professionals– General Public
Economic

Access to Controlled Medicines | TECHNICAL BRIEFING SEMINAR Geneva, 31 Oct 2012 26 |
Legislative barriers
Inappropriate laws and regulations– Rules often not preventing abuse, dependence and diversion– Rules often a barrier for medical access
Limitations on prescriptions and administration– Duration– Maximum dosage– Administration of medicines restricted
Special prescription forms
Limitation of outlets
Limitations on who is allowed to prescribe– Special licensing in spite of medical degree

Access to Controlled Medicines | TECHNICAL BRIEFING SEMINAR Geneva, 31 Oct 2012 27 |
Policy barriers
Access to controlled medicines not included in national policy plans
– National Pharmaceutical Policy Plan– National Cancer Control Plan– National HIV/AIDS Plan
Investigation/prosecution of prescribers– Investigation of those who subscribe at an adequate level
Too much red tape– Speed of licensing procedures

Access to Controlled Medicines | TECHNICAL BRIEFING SEMINAR Geneva, 31 Oct 2012 28 |
Knowledge barriers
Medical Schools– Many do not teach opioid analgesia
Physicians– Fear for dependence– Unfamiliarity with prescribing and dosing– Prescribing obsolete medicines (pethidine=meperidine still in
use)– Unfamiliarity with pain assessment– Learned "not to treat symptoms, but disease"

Access to Controlled Medicines | TECHNICAL BRIEFING SEMINAR Geneva, 31 Oct 2012 29 |
Attitude barriers
Patient and family– Association morphine impending death– Conviction that suffering chastens
Health-care and other professionals– Continuing use of obsolete or counter-productive terminology– Seniors not allowing juniors to introduce new techniques

Access to Controlled Medicines | TECHNICAL BRIEFING SEMINAR Geneva, 31 Oct 2012 30 |
Economical and procurementbarriers
General issues as for other medicines e.g.– Insurance and affordability– Distribution problems
In some countriesSeparate distribution systems for controlled medicines

How to Beat the Global Pain Management Crisis?

Access to Controlled Medicines | TECHNICAL BRIEFING SEMINAR Geneva, 31 Oct 2012 32 |
Improving access
Suggested steps
Policy analysis
Legal analysis (external lawyer, trained on the issue)
National policy on improving access
National one-day symposia for awareness raising

Access to Controlled Medicines | TECHNICAL BRIEFING SEMINAR Geneva, 31 Oct 2012 33 |
Working methods (1)
Preferrably: working group that includes– authorities– representatives of relevant health-care professionals
• Pharmacists, GPs, PC, oncology, surgery…. (pain everywhere!)
• Treatment of opioid dependence• Veterinarians?
– patient representatives

Access to Controlled Medicines | TECHNICAL BRIEFING SEMINAR Geneva, 31 Oct 2012 34 |
Working methods (2)
Full analysis of barriers
Policy planning– Priority setting
Implementation
Evaluate, set new priorities and adjust policy plan
etc…

Access to Controlled Medicines | TECHNICAL BRIEFING SEMINAR Geneva, 31 Oct 2012 35 |
Tools
WHO Policy guidelines
WHO Guidelines on the Pharmacological Treatment of Persisting Pain in Children with Medical Illness
Published 2012 on-line (free) and in print
Other WHO pain guidelines to follow– Persisting Pain in Adults– Acute Pain

WHO Policy Guidelines

Access to Controlled Medicines | TECHNICAL BRIEFING SEMINAR Geneva, 31 Oct 2012 37 |
WHO Policy Guidelines
English, French and Spanish in print form
In print form: US$ 25.– (US$ 17.50 for developing countries)
On-line: 15 languages available free of charge online
http://www.who.int/medicines/areas/quality_safety/guide_nocp_sanend/en/index.html
Ensuring Balance in National Policies on Controlled Substances, Guidance for accessibility and availability of controlled medicines (Geneva 2011)

Access to Controlled Medicines | TECHNICAL BRIEFING SEMINAR Geneva, 31 Oct 2012 38 |
Policy principle
Based on Principle of Balance: Obligation of governments to establish a system of drug
control that – ensures the adequate availability of controlled
substances for medical and scientific purposes
– while simultaneously preventing abuse, diversion and trafficking
21 Guidelines and Country Check List

Access to Controlled Medicines | TECHNICAL BRIEFING SEMINAR Geneva, 31 Oct 2012 39 |
21 Guidelines
Topics
Content of drug control legislation and policy (2 GLs)
Authorities and their role in the system (4 GLs)
Policy planning for availability and accessibility (4 GLs)
Healthcare professionals (4 GLs)
Estimates and statistics (3 GLs)
Procurement (3 GLs)
Other (1 GL)

WHO Pain Treatment Guidelines

Access to Controlled Medicines | TECHNICAL BRIEFING SEMINAR Geneva, 31 Oct 2012 41 |
Ground breaking guidelines
Cancer Pain Relief (1986)– 2nd Edition: 1996
WHO Cancer Pain and Palliative Care in Children (1998)

Access to Controlled Medicines | TECHNICAL BRIEFING SEMINAR Geneva, 31 Oct 2012 42 |
Cancer Pain Relief (in children)
Systematic approach:– "By the ladder"– "By the clock"– "By the appropriate route"– "By the individual"
Three Step Analgesic Ladder No maximum dose on morphine
– "The right dose is the dose that works"
Obsolete now for some recommended opioids– E.g. levorphanol, pethidine
Not evidence-based / no transparency

Access to Controlled Medicines | TECHNICAL BRIEFING SEMINAR Geneva, 31 Oct 2012 43 |
WHO Pain Treatment Guidelines Series
WHO Treatment Guidelines on Persisting Pain in Children with Medical Illnesses
– On-line since February 2012– In print: next week!
Persisting Pain in Adults (in progress)– Scoping document online available
Acute Pain (Planned)

Access to Controlled Medicines | TECHNICAL BRIEFING SEMINAR Geneva, 31 Oct 2012 44 |
Persisting Pain in Children Package

Access to Controlled Medicines | TECHNICAL BRIEFING SEMINAR Geneva, 31 Oct 2012 45 |
Persisting Pain in Children Package
Printed version will be available as a package:
Guidelines and brochures
Wall chart
Dosage card
2 Pain measurement schales (FPS-R and VAS)

Access to Controlled Medicines | TECHNICAL BRIEFING SEMINAR Geneva, 31 Oct 2012 46 |
Contents (1)
Principles – All moderate and severe pain in children should always be
addressed.
19 clinical recommendations– Two-step approach
4 health system recommendations
Most evidence levels assessed "low" and "very low"
Research agenda – Evidence Based Child Health 6: 1017-1020 (2011)

Access to Controlled Medicines | TECHNICAL BRIEFING SEMINAR Geneva, 31 Oct 2012 47 |
Contents (2)
Chapter 1. Introduction.
Chapter 2. Classification of pain in children
Chapter 3. Evaluation of persisting pain in the paediatric population
Chapter 4. Pharmacological treatment strategies
Chapter 5. Improving access to pain relief in health systems

Access to Controlled Medicines | TECHNICAL BRIEFING SEMINAR Geneva, 31 Oct 2012 48 |
Contents (3)
Annex 1. Clinical recommendations
Annex 2. Evidence retrieval and appraisal
Annex 3. Research agenda
Annex 4. Health system interventions recommendation
Annex 5. Opioid analgesics and international conventions

Conclusion

Access to Controlled Medicines | TECHNICAL BRIEFING SEMINAR Geneva, 31 Oct 2012 50 |
Conclusion
Potentially 4.7 billion people affected
Medical opioid consumption needs to go up 6 times
Policies needed to identify and overcome barriers
Concerted action by health-care professionals of all specialties and policy makers required
Tools include WHO policy and treatment guidelines

Willem Scholten, PharmD, MPATeam Leader, Access to Controlled Medicines,World Health Organization, Geneva, Switzerland
wk.scholten@ bluewin.ch
Access to Controlled Medicines