Embed Size (px)
Citation preview
FROM THE ACADEMYStandards of Practice & Professional Performance
Academy of Nutrition and Dietetics: Revised 2012Standards of Practice in Nutrition Care andStandards of Professional Performance for DieteticTechnicians, Registered
The Academy Quality Management Committee and Scope of Practice Subcommittee of the Quality Management CommitteeDIETETIC TECHNICIANS, REGIS-tered (DTRs) are credentialedpractitioners specifically trai-ned and qualified to provide
nutrition and dietetics services and areaccountable and responsible for theirpractice and service. The Academy ofNutrition and Dietetics (Academy)leads the profession of nutrition and di-etetics by developing standards againstwhich the quality of practice and per-formance of DTRs can be evaluated. TheAcademy’s Scope of Practice in Nutri-tion and Dietetics,1 the 2012 Standardsof Practice (SOP) in Nutrition Care andStandards of Professional Performance(SOPP) for DTRs, along with the Code ofEthics2 and the 2012 Scope of Practicefor the DTR,3 guide the practice andperformance of DTRs in all settings.The standards and indicators found
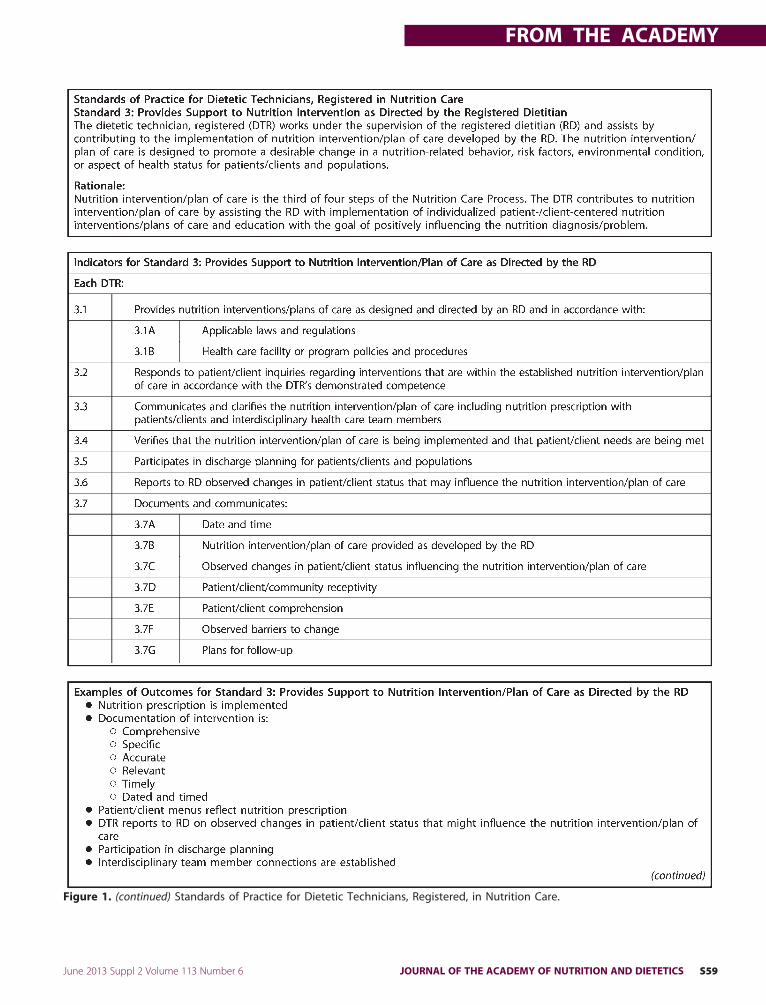
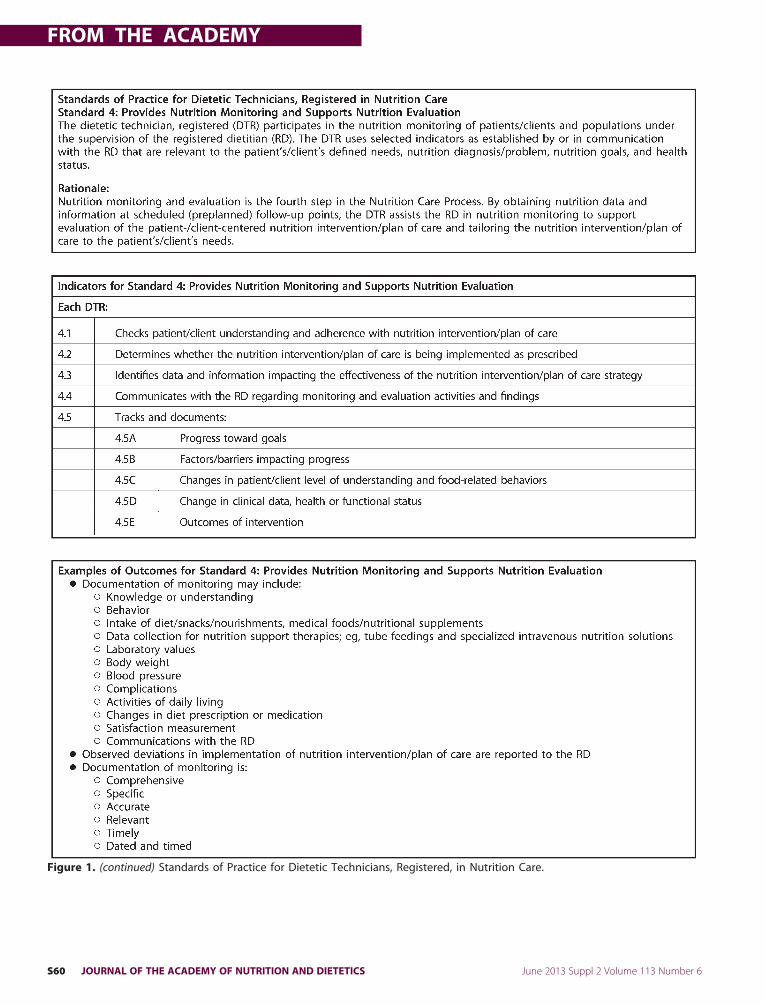
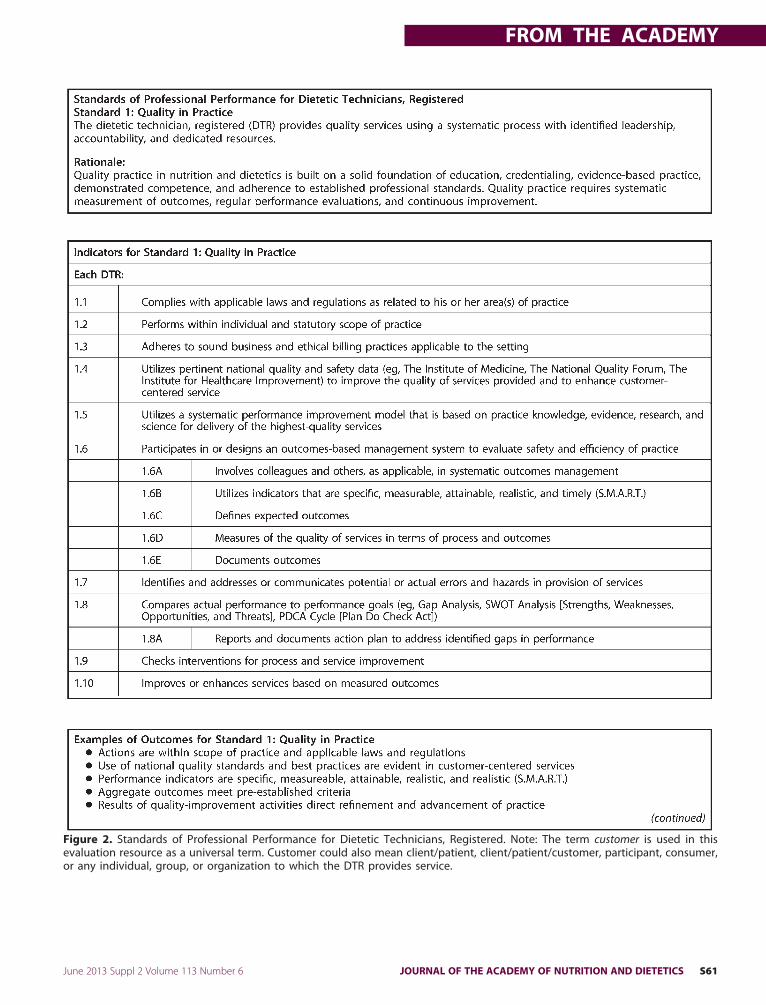
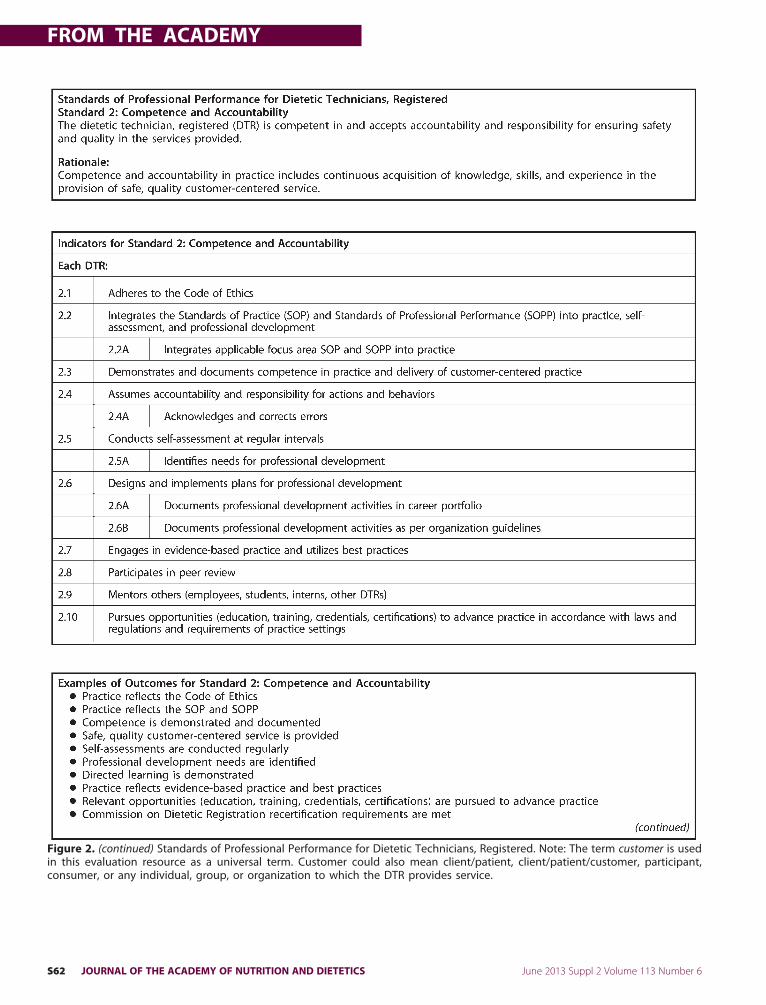
within the SOP and SOPP reflect theminimum competent level of nutritionand dietetics practice and professionalperformance for DTRs. The SOP in Nu-trition Care is composed of four stan-dards representing the four steps of theNutrition Care Process (NCP) as appliedto the care of patients/clients.4 TheSOPP for DTRs consists of standardsrepresenting six domains of profes-sionalism. This article represents the2012 update of the Academy’s SOPin Nutrition Care and SOPP for DTRs(Figures 1 and 2).
Statement of Potential Conflict of Interest:The authors have no potential conflict ofinterest to disclose.
2212-2672/$36.00doi: 10.1016/j.jand.2012.12.010
Available online 28 February 2013S56 JOURNAL OF THE ACADEMY OF NUTRITI
How Does the Academy’s Scopeof Practice in Nutrition andDietetics, Code of Ethics, and theScope of Practice for the DTRGuide the Practice andPerformance of DTRs in AllSettings?The Scopeof Practice inNutrition andDi-etetics is composedof statutory and indi-vidual components, including the Codeof Ethics, and encompasses the range ofroles, activities, and regulations withinwhich nutrition and dietetics practitio-ners perform. In states where a practiceactaddressesDTRs, state licensureactsorcertification statutes as well as otherstate statutes and regulations define theDTR’s statutory scope of practice andmay delineate the services theDTR is au-thorized to perform in that state.The DTR’s individual scope of practice
isdeterminedbyeducation, training, cre-dentialing, and demonstrated and docu-mented competence to practice. Individ-ual scope of practice in nutrition anddietetics has flexible boundaries to cap-ture the breadth of the individual’s pro-fessional practice. The Scope of PracticeDecisionTool,which isanonline, interac-tive tool, permitsaDTRtoansweraseriesof questions to determine if a particularactivity iswithin his or her scope of prac-tice. The tool is designed to allow for aDTR to critically evaluate his or herknowledge, skill anddemonstrated com-petence with criteria resources.
Why Were the Standards Revised?There is a scheduled5-year reviewprocessfor Academy documents. Regular reviewsare indicated to consider changes inhealthcare and other business segments, public
health initiatives,newresearchthatguidesON AND DIETETICS © 2
evidence-based practice and best prac-tices, consumer interests, technologi-cal advances, and emerging practiceenvironments. Questions from creden-tialed practitioners, federal and stateregulations, accreditation standards,and other factors necessitated reviewand revision of the 2008 “core” SOP inNutrition Care and SOPP for RegisteredDietitians andDTRs to assure safe, qual-ity, and competence in practice.5
How Were the Standards Revised?The members of the Quality Manage-ment Committee and its Scope of Prac-tice Subcommittee utilized collectiveexperience and consensus in reviewingstatements to support safe, qualitypractice, and desirable outcomes. Thereview focused on definition of terms,illustrative figures and tables, lists ofservices and activities in current prac-tice, and enhancements to support fu-ture practice and advancement. Thestandards, rationales, and indicators forthe 2012 standardswere updated usinginformation from questions receivedby the Academy’s Quality Manage-
Approved November 2012 by the QualityManagement Committee of the Academyof Nutrition and Dietetics (Academy) andthe Academy House of Delegates. Sched-uled review date: November 2017.
Questions regarding the Revised 2012 Stan-dards of Practice in Nutrition Care and Stan-dards of Professional Performance for Di-etetic Technicians, Registered may beaddressed to the Academy Quality Man-agement Staff: Karen Hui, RD, LDN, man-ager, Practice Standards; and SharonM. Mc-Cauley, MS, MBA, RD, LDN, FADA, director,Quality Management at [email protected]
ment Department, discussions with Di-
013 by the Academy of Nutrition and Dietetics.
FROM THE ACADEMY
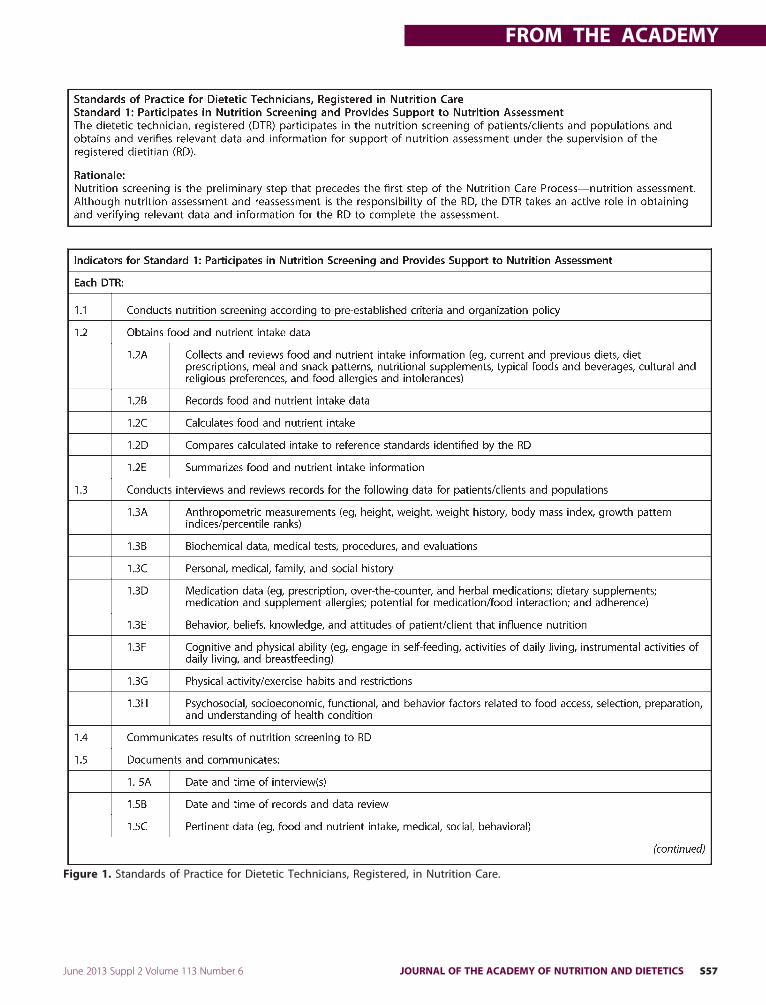
Figure 1. Standards of Practice for Dietetic Technicians, Registered, in Nutrition Care.
June 2013 Suppl 2 Volume 113 Number 6 JOURNAL OF THE ACADEMY OF NUTRITION AND DIETETICS S57
FROM THE ACADEMY
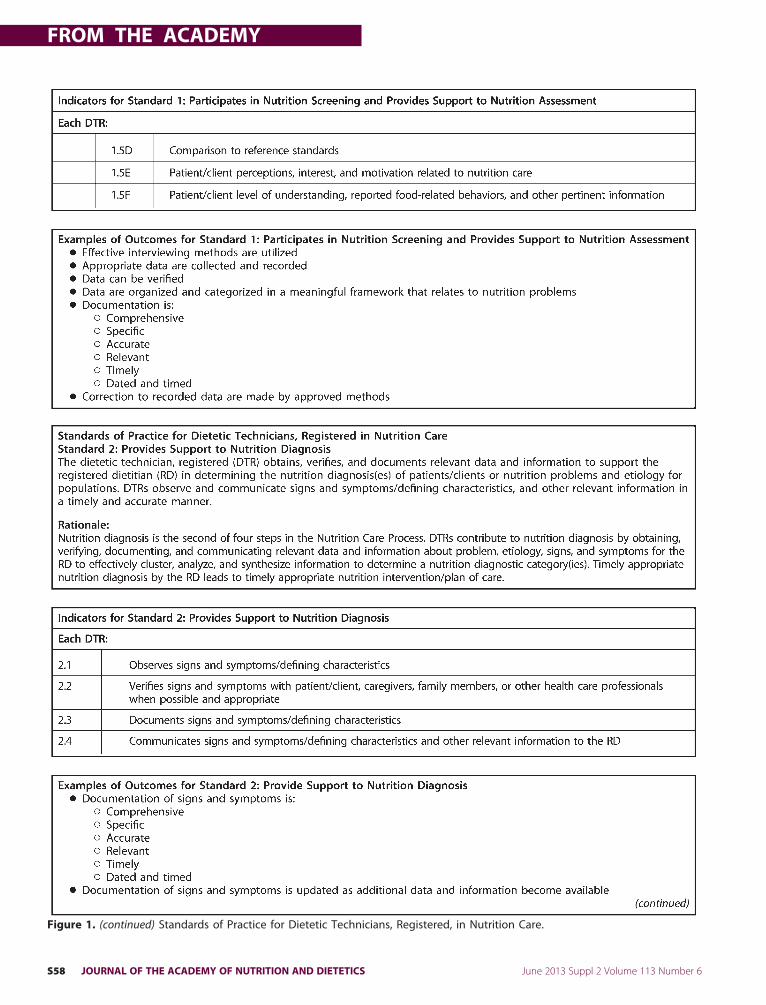
Figure 1. (continued) Standards of Practice for Dietetic Technicians, Registered, in Nutrition Care.
S58 JOURNAL OF THE ACADEMY OF NUTRITION AND DIETETICS June 2013 Suppl 2 Volume 113 Number 6
FROM THE ACADEMY
Figure 1. (continued) Standards of Practice for Dietetic Technicians, Registered, in Nutrition Care.
June 2013 Suppl 2 Volume 113 Number 6 JOURNAL OF THE ACADEMY OF NUTRITION AND DIETETICS S59
FROM THE ACADEMY
Figure 1. (continued) Standards of Practice for Dietetic Technicians, Registered, in Nutrition Care.
S60 JOURNAL OF THE ACADEMY OF NUTRITION AND DIETETICS June 2013 Suppl 2 Volume 113 Number 6
FROM THE ACADEMY
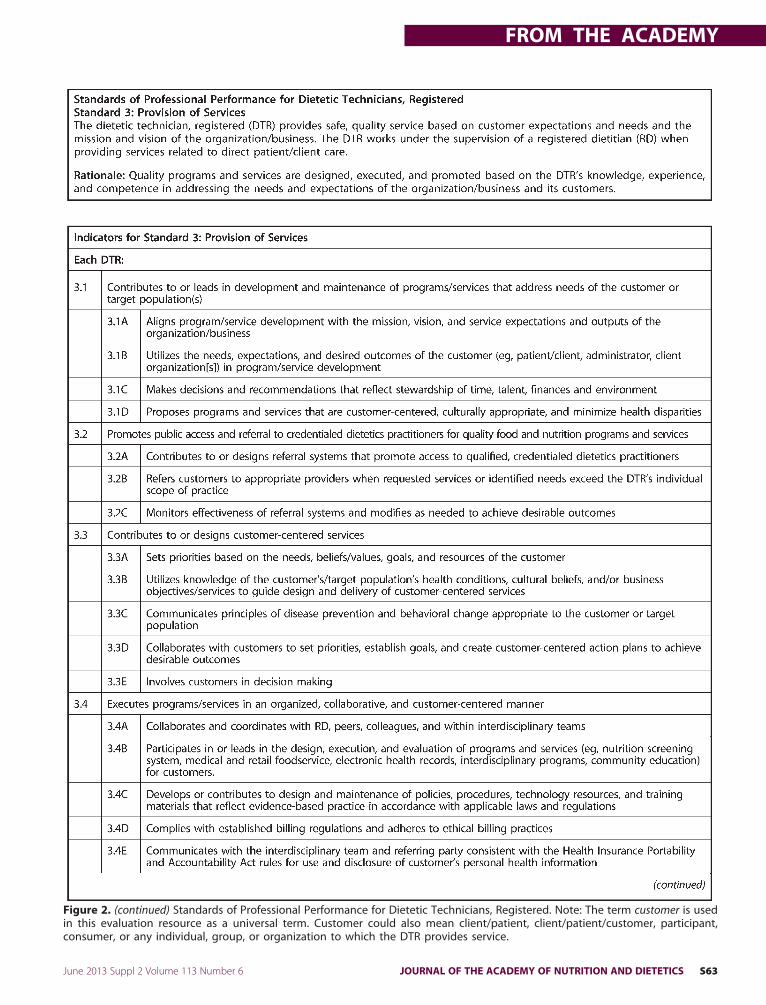
Figure 2. Standards of Professional Performance for Dietetic Technicians, Registered. Note: The term customer is used in thisevaluation resource as a universal term. Customer could also mean client/patient, client/patient/customer, participant, consumer,
or any individual, group, or organization to which the DTR provides service.June 2013 Suppl 2 Volume 113 Number 6 JOURNAL OF THE ACADEMY OF NUTRITION AND DIETETICS S61
FROM THE ACADEMY
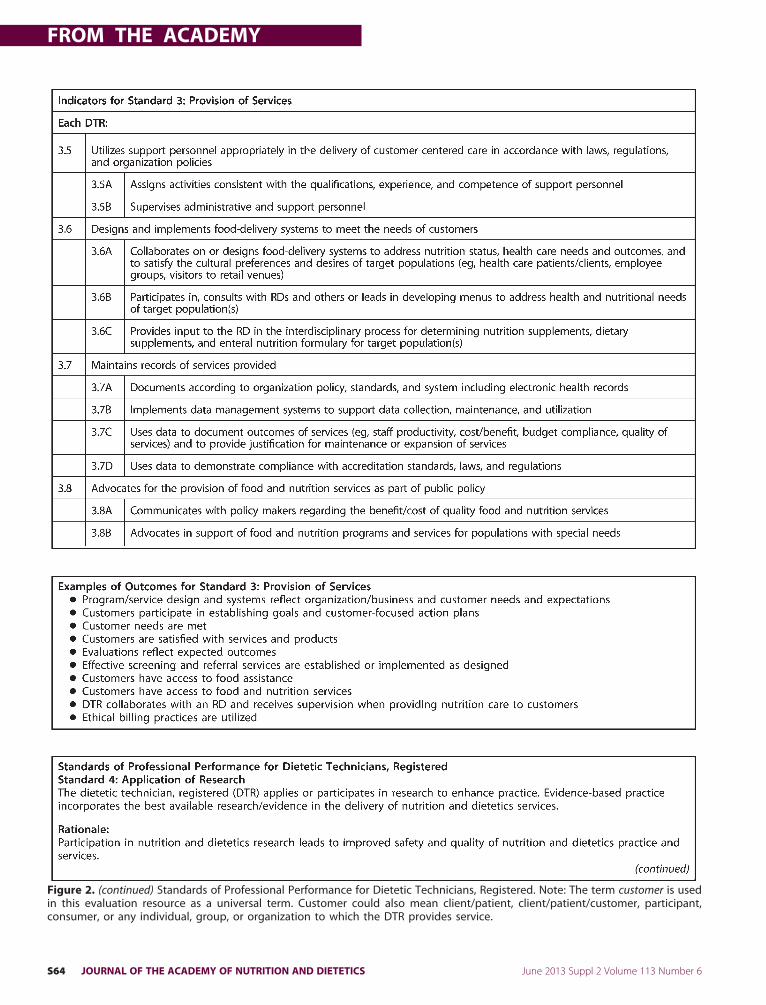
Figure 2. (continued) Standards of Professional Performance for Dietetic Technicians, Registered. Note: The term customer is usedin this evaluation resource as a universal term. Customer could also mean client/patient, client/patient/customer, participant,
consumer, or any individual, group, or organization to which the DTR provides service.S62 JOURNAL OF THE ACADEMY OF NUTRITION AND DIETETICS June 2013 Suppl 2 Volume 113 Number 6
FROM THE ACADEMY
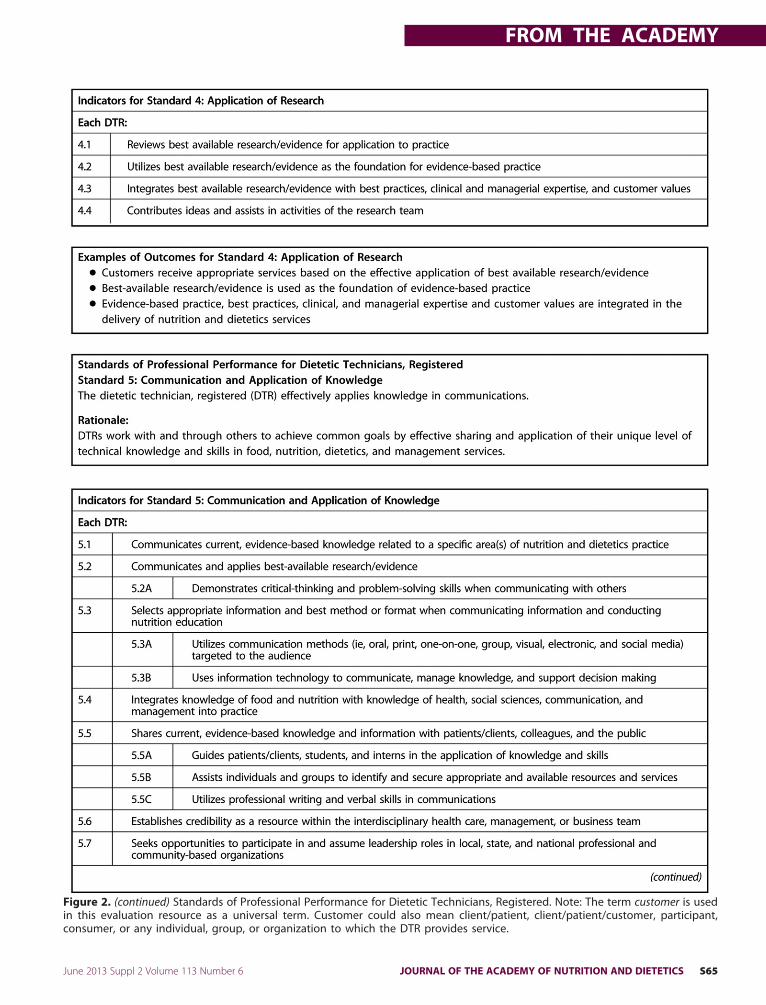
Figure 2. (continued) Standards of Professional Performance for Dietetic Technicians, Registered. Note: The term customer is usedin this evaluation resource as a universal term. Customer could also mean client/patient, client/patient/customer, participant,
consumer, or any individual, group, or organization to which the DTR provides service.June 2013 Suppl 2 Volume 113 Number 6 JOURNAL OF THE ACADEMY OF NUTRITION AND DIETETICS S63
FROM THE ACADEMY
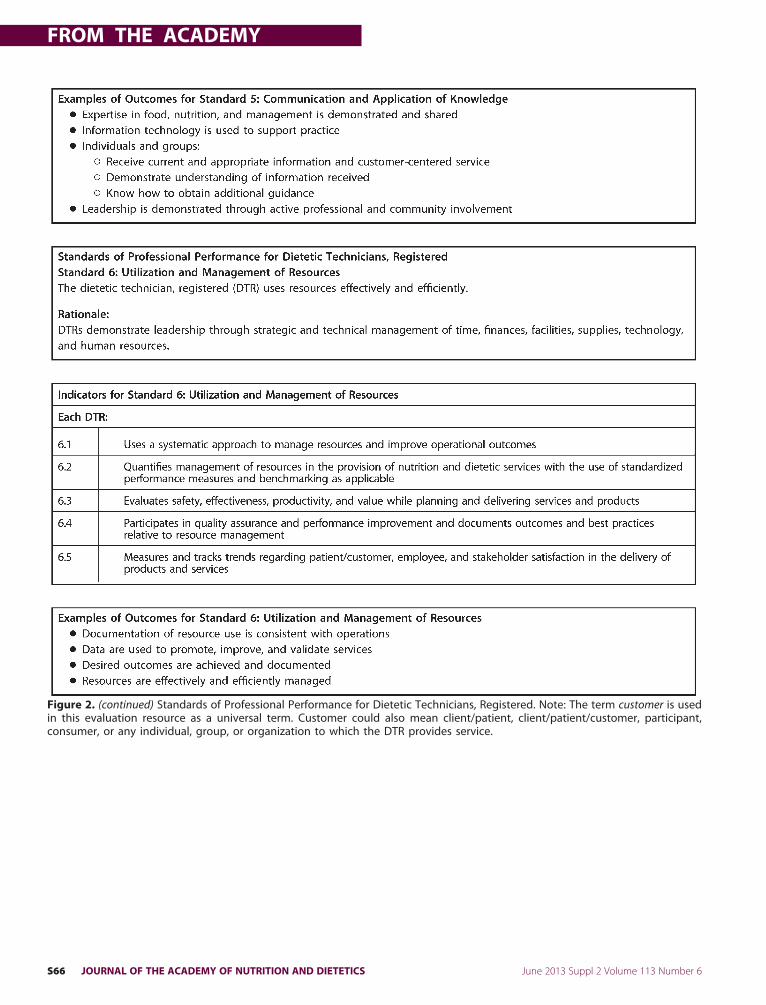
Figure 2. (continued) Standards of Professional Performance for Dietetic Technicians, Registered. Note: The term customer is usedin this evaluation resource as a universal term. Customer could also mean client/patient, client/patient/customer, participant,
consumer, or any individual, group, or organization to which the DTR provides service.S64 JOURNAL OF THE ACADEMY OF NUTRITION AND DIETETICS June 2013 Suppl 2 Volume 113 Number 6
FROM THE ACADEMY
Figure 2. (continued) Standards of Professional Performance for Dietetic Technicians, Registered. Note: The term customer is usedin this evaluation resource as a universal term. Customer could also mean client/patient, client/patient/customer, participant,
consumer, or any individual, group, or organization to which the DTR provides service.June 2013 Suppl 2 Volume 113 Number 6 JOURNAL OF THE ACADEMY OF NUTRITION AND DIETETICS S65
FROM THE ACADEMY
Figure 2. (continued) Standards of Professional Performance for Dietetic Technicians, Registered. Note: The term customer is usedin this evaluation resource as a universal term. Customer could also mean client/patient, client/patient/customer, participant,
consumer, or any individual, group, or organization to which the DTR provides service.S66 JOURNAL OF THE ACADEMY OF NUTRITION AND DIETETICS June 2013 Suppl 2 Volume 113 Number 6

FROM THE ACADEMY
etetic Practice Groups, Member Inter-est Groups, and member commentsthrough focus area SOPandSOPPdevel-opment.This document was presented to and
reviewedbytheAcademy’sHouseofDel-egates LeadershipTeamand theHouseofDelegates (includes representation fromstate affiliates and Dietetic PracticeGroups). Thisprovidedopportunity tore-fine the document and gain consensusfrom members representing diversepractice and geographic perspectives.Comments received were considered bytheQualityManagementCommittee andits Scope of Practice Subcommittee. Therevised draft document was reviewedand approved by the House of Delegatesin November 2012.
What Are the Standards ofPractice in Nutrition Care?The SOP in Nutrition Care:
• incorporate the NCP as a methodto manage nutrition care activi-ties;
• apply to DTRswho provide directcare to individual patients/cli-ents in acute and extendedhealth care settings, as well as inpublic health, home-based andcommunity services, and ambu-latory care settings;
• are formatted according to thefour steps of the NCP (ie, nutri-tion assessment, nutrition diag-nosis, nutrition intervention, andnutritionmonitoring and evalua-tion); and
• reflect the training, responsibil-ity, and accountability of theDTR.
What Are the Standards ofProfessional Performance?The SOPP:
• apply to DTRs in all practice set-tings;
• are formatted according to sixdomains of professional behavior(ie, quality in practice, compe-tence and accountability, provi-sion of services, application ofresearch, communication andapplication of knowledge, andutilization and management ofresources); and
• reflect the training, responsibil-ity, and accountability of the
DTR.June 2013 Suppl 2 Volume 113 Number 6
The SOP and SOPP comprehensivelydepict the minimum expectation forcompetent care of the patient/client orother customer and professional be-havior for theDTR. The term customer isused in this evaluation resource as auniversal term. Customer could alsomean client/patient, client/patient/customer, participant, consumer, orany individual, group, or organizationto which the DTR provides service.
What Is the Relationship of theDTR and RD?In direct patient/client care, the RD andDTR work as a team utilizing the NCP4
and Standardized Language,6 a struc-turedmethod for guiding nutrition careactivities and providing consistency indocumentation,monitoring, and evalu-ating progress.7 The RD develops andoversees the system for delivery of nu-trition care activities, often with the in-put of others, including the DTR. Com-ponents of the nutrition-care deliverysystem might include the following:policies and procedures, standards ofcare, forms, documentation standards,and roles and responsibilities of sup-port and technical personnel partici-pating in theNCP. The RD is responsiblefor completing the nutrition assess-ment, determining the nutrition diag-nosis(es), implementing the nutritionintervention, and evaluating the pa-tient’s/client’s response.6 The RD su-pervises the activities of support, ad-ministrative, and technical personnel(ie, DTR assisting with the patient’s/cli-ent’s care).The DTR is an integral contributor to
the nutrition care of patients/clients.The DTR is often the first staff from thenutrition team that a patient or clientmeets; serves as a conduit of nutritioncare information to RDs, nurses, andothers at meetings and care conferenc-es; and contributes to the continuumofcare by facilitating communication be-tween staff providing nutrition careand staff providing nursing care.The RD assigns duties to the DTR that
are consistentwith theDTR’s individualscope of practice. For example, the DTRmay initiate standard procedures, suchas completing and following up on nu-trition screening for assigned units/pa-tients; performing routine activitiesbased on diet order and protocol, poli-cies, and procedures; completing the
intake process for a new clinic client;JOURNAL OF THE ACADE
and reporting to the RD when a pa-tient’s/client’s data suggest the need fora nutrition assessment. The DTR ac-tively participates in nutrition care bycontributing information and observa-tions, guiding patients/clients in menuselections, providing nutrition educa-tion on prescribed diets, and reportingto the RD on the patient’s/client’s re-sponse, including documenting out-comes or providing evidence signifyingthe need to adjust the nutrition careplan.The RD is responsible for supervising
anypatient/client careactivities assignedto other staff, including the DTR, and canbeheldaccountable to thepatient/clientsand others for services rendered. The fol-lowing resources provide additional in-formation regarding the roles and prac-tice of DTRs: Scope of Practice for theDTR,8 theSOPandSOPP forRDs,9 PracticeTips: The RD/DTR Team,10 and PracticeTips: What Is Meant by “Under the Su-pervision of the RD”?11
What Is Meant by “Under theSupervision of an RD”?To comply with laws, regulations, andaccreditation standards, the Academyevaluated the requirement for RD su-pervision of the DTR and other support,administrative, and technical person-nel involved in the direct nutrition careof patients/clients.The Academy describes supervision
of nutrition care delivered to patients/clients as follows:
• The RD is accountable for the nu-trition care of patients/clients invarious health care settings (eg,hospitals, nursing homes, homehealth agencies, end-stage renalfacilities), social services pro-grams (eg, Special SupplementalNutrition Program for Women,Infants, and Children), and nutri-tion services provided by theOlder Americans Act (throughprovision of dailymeals providedin congregate and home-deliv-ered settings). DTRs may be su-pervised by RDs in any of thesesettings in which direct patient/client care is provided.
• In many health care settings, aDTR and other staff may be avail-able to assist the RD and carrythrough with routine food andnutrition services delivered to
the patient/client/customer. AnMY OF NUTRITION AND DIETETICS S67
FROM THE ACADEMY
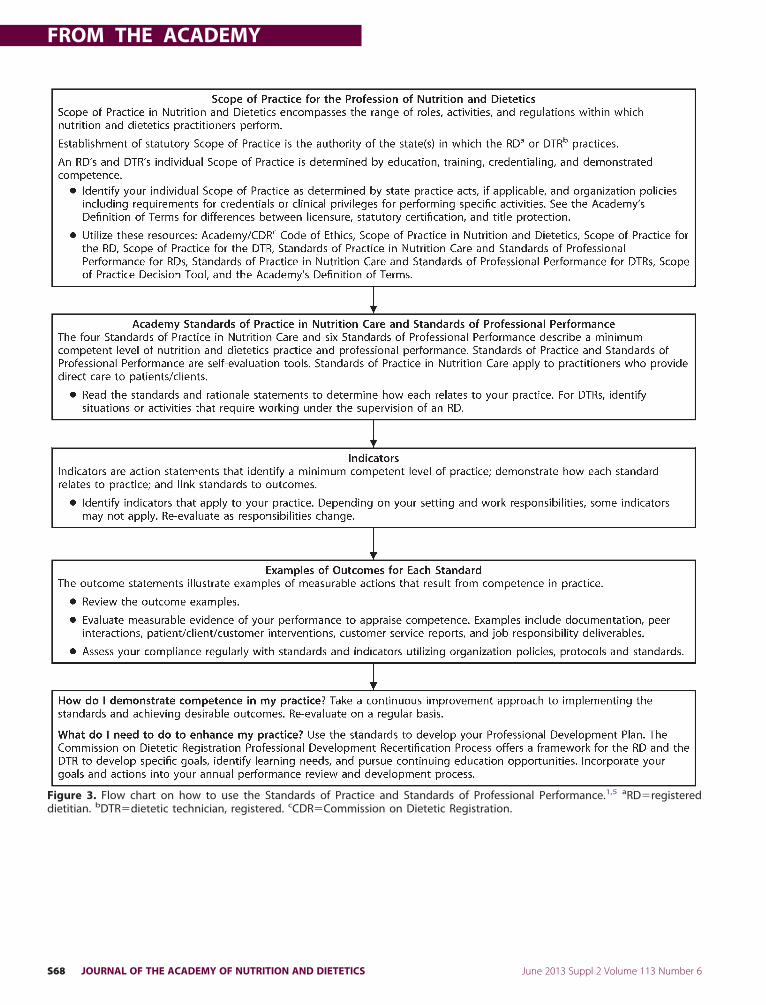
Figure 3. Flow chart on how to use the Standards of Practice and Standards of Professional Performance.1,5 aRD�registered
dietitian. bDTR�dietetic technician, registered. cCDR�Commission on Dietetic Registration.S68 JOURNAL OF THE ACADEMY OF NUTRITION AND DIETETICS June 2013 Suppl 2 Volume 113 Number 6
FROM THE ACADEMY
RD in these settings may assignactivities to the DTR and othersupport personnel consistentwith the individual’s qualifica-tions and competence. The RD isresponsible for overseeing dutiesassigned to others and must an-swer to patients/clients, employ-ers, and boards of dietetics licen-sure if care is compromised.
• The RD may assign certain tasksfor the purpose of attainingneeded information (eg, screen-ing data, diet history) or commu-nicating with and educating pa-tients. An RD may assign to DTRsinterventions within their scopeof practice and demonstratedcompetence, such as nutritioneducation,monitoring consump-tion of meals and medical foodsupplements, and referring pa-tients/clients to communityagencies and programs. The DTRand other support, administra-tive, and technical staff can con-tribute valuable information andobservations to the RD that sup-ports quality patient/client-cen-tered care.
• Whether the supervision is di-rect (RD is on premises and im-mediately available) or indirect(RD is immediately available bytelephone or other electronicmeans) is determined by regula-tory and organization policiesand procedures.
• Additional considerations includeregulation, state dietitian/nutri-tionist licensure statutes, andrules that may include definitionsof supervision and scope of prac-tice specifications for technicalandother support andadministra-tive staff. Federal and state rulesand regulations for health care fa-cilities, dialysis centers, and for so-cial service programs specify thequalified dietitian.
• Organization accreditation mustalso be considered. Standardsverify compliance with federaland state regulatory require-ments and may specify addi-tional requirements for an RD.
This description of supervision as itrelates to the RD/DTR teams is not syn-onymous with managerial supervisionor oversight, clinical supervision (eg, peer-
to-peer), supervision of provisional li-June 2013 Suppl 2 Volume 113 Number 6
censees, and/or supervision of dieteticsinterns andstudents. Clinical supervisionis used in medicine and the mentalhealth fields for the purposes of case re-view and professional development.5,11
In What Other Settings Do DTRsProvide Services?
Although many DTRs work in clinicalsettings, career opportunities forDTRs are broader than clinical set-tings. The role for a DTR in providingfood and nutrition services in non-clinical settings where an RD may notbe directly involved in the program/activity is guided by the DTR’s indi-vidual scope of practice and require-ments contained in regulations,employer or organizational policiesand procedures, and state practiceacts. These settings include commu-nity nutrition programs, fitness cen-ters, school nutrition, child nutritionprograms, and foodservice systemsmanagement outside of health caresettings. The SOPP and the Scope ofPractice for the DTR6 clearly delineateexpanded roles and opportunities forDTRs.
Why Are the Standards Importantfor DTRs?The standards promote:
• safe, effective, and efficient food,nutrition, dietetics, and relatedservices;
• evidence-basedpractice andbestpractices;
• improved health-related outcomesand cost-reductionmethods;
• quality assurance and performanceimprovement;
• ethical business and billing prac-tices12,13;
• practitioner competence and qua-lification verification because statedepartments of health and federalregulatory agencies, such as theCenters for Medicare and MedicaidServices looktoprofessionalorgani-zations to createandmaintain stan-dards of practice14,15;
• adherence to the rules and regula-tions of state departments of healthand federal regulatory agencies,such as Centers for Medicare andMedicaid Services, which state thattechnical personnel demonstratecompetence though education, ex-
perience, and specialized trainingJOURNAL OF THE ACADE
with appropriate credentials as re-quired to perform task(s) as-signed14,15;
• consistency in practice and perfor-mance;
• dietetics research, innovation, andpractice development; and
• individual advancement.
The standards provide:• minimum competent levels of
practice and performance;• common indicators for self-eval-
uation;• activities for which DTRs are ac-
countable;• a description of the role of nutri-
tion and dietetics and the uniqueservices that DTRs offer withinthe health care team and in prac-tice settings outside of healthcare; and
• guidance for policies and proce-dures, job descriptions, compe-tence assessment tools, and aca-demic objectives for educationprograms.
How Are the StandardsStructured?A standard is a brief description of thecompetent level of nutrition anddietet-ics practice. A rationale is a descriptionof the intent, purpose, and importanceof the standard. An indicator is an ac-tion statement illustrating how eachstandard may be applied in practice.Examples of outcomes are also in-cluded that depict measurable resultsthat relate indicators to practice.Each standard is equal in relevance
and importance. The content for stan-dard, rationale, and indicator descrip-tions in the SOP in nutrition care areadapted from the Academy’s Interna-tional Dietetics & Nutrition TerminologyReference Manual: Standardized Lan-guage for the Nutrition Care Process.6
How Can I Use the Standards toEvaluate and Advance MyPractice and Performance?The standards can be used as part of theCommission on Dietetic RegistrationProfessional Development Portfolioprocess16 to develop goals and focuscontinuing education efforts. The Pro-fessional Development Portfolio en-courages DTRs to engage in reflection,
self-assessment, and goal setting,MY OF NUTRITION AND DIETETICS S69

FROM THE ACADEMY
which are the critical components ofCommission on Dietetic Registrationrecertification. Figure 3 presents a flowchart for applying the 2012 SOP in Nu-trition Care and the SOPP into a DTR’spractice. Self-assessment using the SOPand SOPP can identify learning needsand opportunities for advancement forindividual practitioners.DTRs may not apply every indicator
and achieve every outcome all at once;DTRs are not limited to the indicatorsand examples of outcomes provided;and all indicatorsmay not be applicableto all DTRs. The standards arewritten inbroad terms to allow for individualpractitioner’s handling of nonroutinesituations. The standards are geared to-ward typical situations and towardpractitioners with the DTR credential.Strictly adhering to standards does notin and of itself constitute best care andservice. It is the responsibility of indi-vidual practitioners to recognize andinterpret situations, and to know whatstandards apply and in what ways theyapply.17
SummaryDTRs face complex situations everyday. Competently addressing theunique needs of each situation and ap-plying standards appropriately is es-sential to providing safe, timely, per-son-centered quality care and service.All DTRs are advised to conduct theirpractice based on the most recent edi-tion of the Academy’s Code of Ethics2
and the Scope of Practice in Nutrition
These standards have been formulated tobe used for individual self-evaluation andthe development of practice guidelines,but not for institutional credentialing orfor adverse or exclusionary decisions re-garding privileging, employment oppor-tunities or benefits, disciplinary actions,or determinations of negligence or mis-conduct. These standards do not consti-tute medical or other professional advice,and should not be taken as such. Theinformation presented in these standardsis not a substitute for the exercise ofprofessional judgment by the health careprofessional. The use of the standards forany other purpose than that for whichthey were formulated must be under-taken with the sole authority and discre-tion of the user.
and Dietetics,1 the Scope of Practice for
S70 JOURNAL OF THE ACADEMY OF NUTRITI
the DTR,3 the 2012 Standards of Prac-tice in Nutrition Care and Standards ofProfessional Performance for DTRs.These resources provide minimumstandards and tools for demonstratingcompetence and safe practice, and areused collectively to gauge and guide aDTR’s performance in nutrition and di-etetics practice. The SOP and SOPP forthe DTR are self-evaluation tools thatpromote quality assurance and perfor-mance improvement. Self-assessmentprovides opportunities to identify areasfor enhancement, new learning andskill development, and to encourageprogression of career growth.All DTRs are advised to have in their
personal libraries the most recent copyof the Academy’s Scope of Practice inNutrition and Dietetics1 and its compo-nents: The 2012 Academy Standards ofPractice in Nutrition Care and Stan-dards of Professional Performance forDTRs; the Code of Ethics2; and theScope of Practice for the DTR.3
To ensure that credentialed dieteticspractitioners always have access to themost current materials, each resourceis maintained on the Academy’s web-site. The documents will continue to bereviewed and updated as new trends inthe profession of nutrition and dieteticsand external influences emerge.
References1. Academy of Nutrition and Dietetics Qual-
ity Management Committee and Scope ofPractice Subcommittee of the QualityManagement Committee. Academy of Nu-trition and Dietetics: Scope of Practice inNutrition and Dietetics. J Acad Nutr Diet.2013;113(6 suppl 2):S11-S16.
2. American Dietetic Association. AmericanDietetic Association/Commission on Di-etetic Registration. Code of ethics for theprofession of dietetics and process forconsideration of ethical issues. J Am DietAssoc. 2009;109(8):1461-1467.
3. Academy of Nutrition and Dietetics Qual-ity Management Committee and Scope ofPractice Subcommittee of the QualityManagement Committee. Academy of Nu-trition and Dietetics: Scope of Practice forthe Dietetic Technician, Registered. J AcadNutr Diet. 2013;113(6 suppl 2):S46-S55.
4. Writing Group of the Nutrition Care Pro-cess/Standardized Language Committee.Nutrition care process and model part I:The 2008 update. J Am Diet Assoc. 2008;108(7):1113-1117.
5. American Dietetic Association QualityManagement Committee. American Di-etetic Association Revised 2008 Standards
of Practice for Registered Dietitians in Nu-trition Care; Standards of ProfessionalON AND DIETETICS
Performance for Registered Dietitians;Standards of Practice for DieteticTechnicians, Registered, in Nutrition Care;and Standards of Professional Perfor-mance for Dietetic Technicians, Regis-tered. J Am Diet Assoc. 2008;108(9):1538-1542e9.
6. Academy of Nutrition and Dietetics. Interna-tional Dietetics & Nutrition Terminology Refer-ence Manual: Standardized Language for theNutrition Care Process. 4th ed. Chicago, IL:AcademyofNutrition andDietetics; 2012.
7. Academy of Nutrition and Dietetics. Prac-tice Tips: DTR Scope of Practice & the Nu-trition Care Process. http://www.eatright.org/scope/. Accessed March 12, 2012.
8. Academy of Nutrition and Dietetics Qual-ity Management Committee and Scope ofPractice Subcommittee of the QualityManagement Committee. Academy of Nu-trition and Dietetics: Scope of Practice forthe Registered Dietitian. J Acad Nutr Diet.2013;113(6 suppl 2):S17-S28.
9. Academy of Nutrition and Dietetics Qual-ity Management Committee and Scope ofPractice Subcommittee of the QualityManagement Committee. Academy of Nu-trition and Dietetics: Revised 2012 Stan-dards of Practice in Nutrition Care andStandards of Professional Performance forRegistered Dietitians. J Acad Nutr Diet.2013;113(6 suppl 2):S29-S45.
10. Academy of Nutrition and Dietetics. Prac-tice Tips: RD/DTR Team. http://www.eatright.org/scope/. Accessed March 12,2012.
11. Academy of Nutrition and Dietetics. Prac-tice Tips:What IsMeant by “Under the Su-pervision of the RD.” http://www.eatright.org/scope/. Accessed March 12, 2012.
12. Hodorowicz MA, White JV. Ethics in ac-tion. Elements of ethical billing for nutri-tion professionals. J Acad Nutr Diet. 2012;112(3):432-435.
13. Grandgenett R, Derelian D. Ethics in ac-tion. Ethics in business practice. J Am DietAssoc. 2010;110(7):1103-1104.
14. US Department of Health and Human Ser-vices, Centers for Medicare and MedicaidServices. State Operations Manual. Ap-pendix A�Survey Protocol, Regulationsand Interpretive Guidelines for Hospitals(Rev. 37, 10-17-08); Section 482.28 Foodand Dietetic Services (pp 287-294). http://www.cms.hhs.gov/manuals/downloads/som107ap_a_hospitals.pdf. AccessedMarch 14, 2012.
15. US Department of Health and Human Ser-vices, Centers for Medicare and MedicaidServices. State Operations Manual. Ap-pendix PP�Guidance to Surveyors forLong Term Care Facilities (Rev. 26, 08-17-07); Section 483.35 Dietary Servi-ces. http://www.cms.gov/CFCsAndCoPs/Downloads/som107ap_pp_guidelines_ltcf.pdf. Accessed March 14, 2012.
16. Weddle DO. The professional develop-ment portfolio process: Setting goals forcredentialing. J Am Diet Assoc. 2002;102(10):1439-1444.
17. Gates G. Ethics opinion: Dietetics profes-sionals are ethically obliged to maintain
personal competencies in practice. J AmDiet Assoc. 2003;103(5):633-635.June 2013 Suppl 2 Volume 113 Number 6

FROM THE ACADEMY
AUTHOR INFORMATIONMembers of the Academy Quality Management Committee 2010-2011, 2011-2012, 2012-2013 and Scope of Practice Subcommittee of theQuality Management Committee 2010-2011, 2011-2012, 2012-2013: Joyce A. Price, MS, RD, LDN–Chair 2010-2011; Sue Kent, MS, RD, LD–Chair2011-2012; Marsha R. Stieber, MSA, RD–Chair 2012-2013; Valaree M. Williams, MS, RD, LDN–Vice Chair 2012-2013; Joanne B. Shearer, MS, RD,LN; Charlotte B. Oakley, PhD, RD, FADA; Sharon A. Cox, MA, RD, LD; Mary J. Marian, MS, RD, CSO; Elise A. Smith, MA, RD, LD; Pamela Charney,PhD, RD; M. Patricia Fuhrman, MS, RD, LD, FADA; Isabel M. Parraga, PhD, RD, LD; Doris V. Derelian, JD, PhD, RD, FADA; Terry L. Brown, MPH, RD,CNSC, LD; Susan L. Smith, MBA, RD; Barbara J. Kamp, MS, RD; Gretchen Y. Robinson, MS, RD, LD, FADA; Margaret J. Tate, MS, RD; Carol J. Gilmore,MS, RD, LD, FADA; Patricia L. Steinmuller, MS, RD, CSSD, LN; Jean A. Anderson, MS, RD; Lois J. Hill, MS, RD, CSR, LD; Sandra J. McNeil, MA, RD,CDN, FADA; Bethany L. Daugherty, MS, RD, CD; Pauline Williams, PhD, MPA, RD, CD; Melissa N. Church, MS, RD, LD; Karen Hui, RD, LDN; andSharon M. McCauley, MS, MBA, RD, LDN, FADA.
ACKNOWLEDGEMENTSThe Academy Quality Management Committee and its Scope of Practice Subcommittee thank the following Academy members for theirassistance with manuscript preparation: COL George A. Dilly, PhD, RD, LD, US Army; LTC Dianne T. Helinski, MHPE, RD, LD, US Army; MartinYadrick, MBA, MS, RD, FADA; Elaine Ayres, MS, RD, FAC-PPM; Christina Ferroli, PhD, RD; Connie Mueller, MS, RD, SNS; Diane Duncan-Goldsmith,MS, RD, LD; Angie Tagtow, MS, RD, LD; Deborah Canter, PhD, RD, LD; Glenna McCollum, DMOL, MPH, RD; and Lindsay Hoggle, MS, RD, PMP.
June 2013 Suppl 2 Volume 113 Number 6 JOURNAL OF THE ACADEMY OF NUTRITION AND DIETETICS S71