Embed Size (px)
Citation preview
Dag 2
Ischemie en infarct
Mar$jn Meuwissen Academisch Medisch Centrum, Amsterdam
non‐profit / open access / physician moderated / up‐to‐date
Cursusoverzicht
• Dag 1: Basis, systema@sche beoordeling – Ivo van der Bilt
• Dag 2: Ischemie – Mar@jn Meuwissen
• Dag 3: Ritmestoornissen – Jonas de Jong
De cursus is interac,ef. Onderbreek gerust!
Cardionetworks
Auteurs:
• Jonas de Jong
• Ivo van der Bilt
• Mar@jn Meuwissen • Renée van den Brink
• Joris de Groot
Illustra@es:
• Rob Kreuger • Bart Duineveld
Met dank aan:
• Arthur Wilde
• Rudolph Koster
Boeken:
• Wellens: The ECG in Emergency Decision Making
• Garcia / Miller: Arrhythmia Recogni$on
• Braunwald Heart Disease
Agenda Ischemie en Infarct
• Achtergrond • Diagnos@ek • Infarct localisa@e • Complica@es
• Quiz
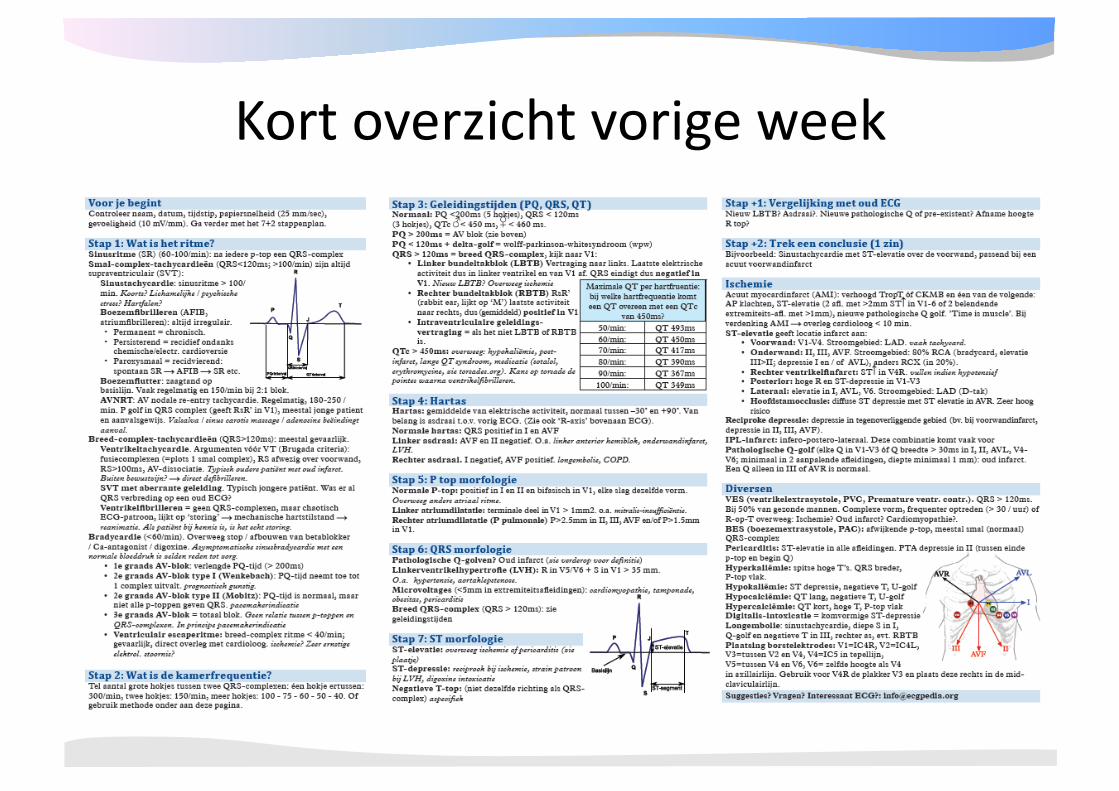
Kort overzicht vorige week
Pathofysiologie
• Oorzaak acuut coronair syndroom = acute afname of blokkade in coronaire doorbloeding
• Atherosclero@sche plaque • Thrombo@sche occlusie tgv plaque ruptuur
– Plaatjes aggrega@e – Vasoac@va > spasme – Thrombine > stollingsac@va@e > bevorderen aggrega@e
• Zelden: erosie/ embolie/ spasme/ anemie/ hypoxie
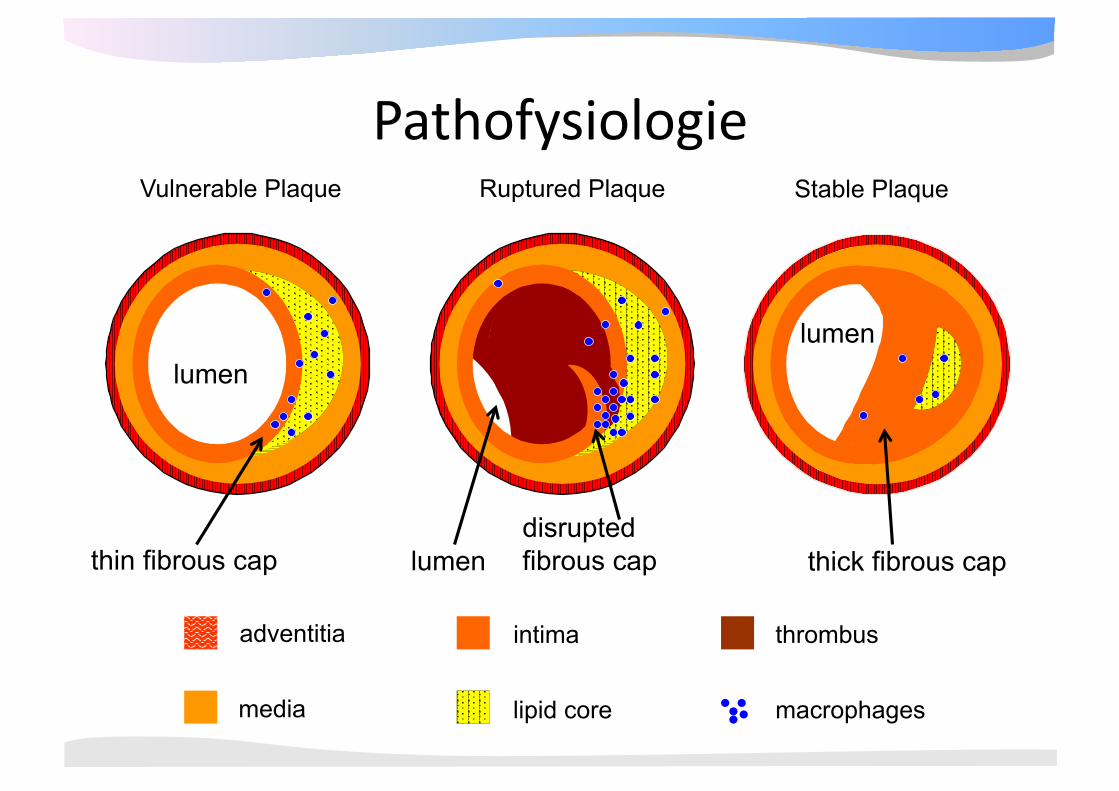
intima adventitia
media lipid core
thrombus
macrophages
Vulnerable Plaque
lumen
thin fibrous cap
Stable Plaque
thick fibrous cap disrupted fibrous cap lumen
Ruptured Plaque
Pathofysiologie
lumen
tijd
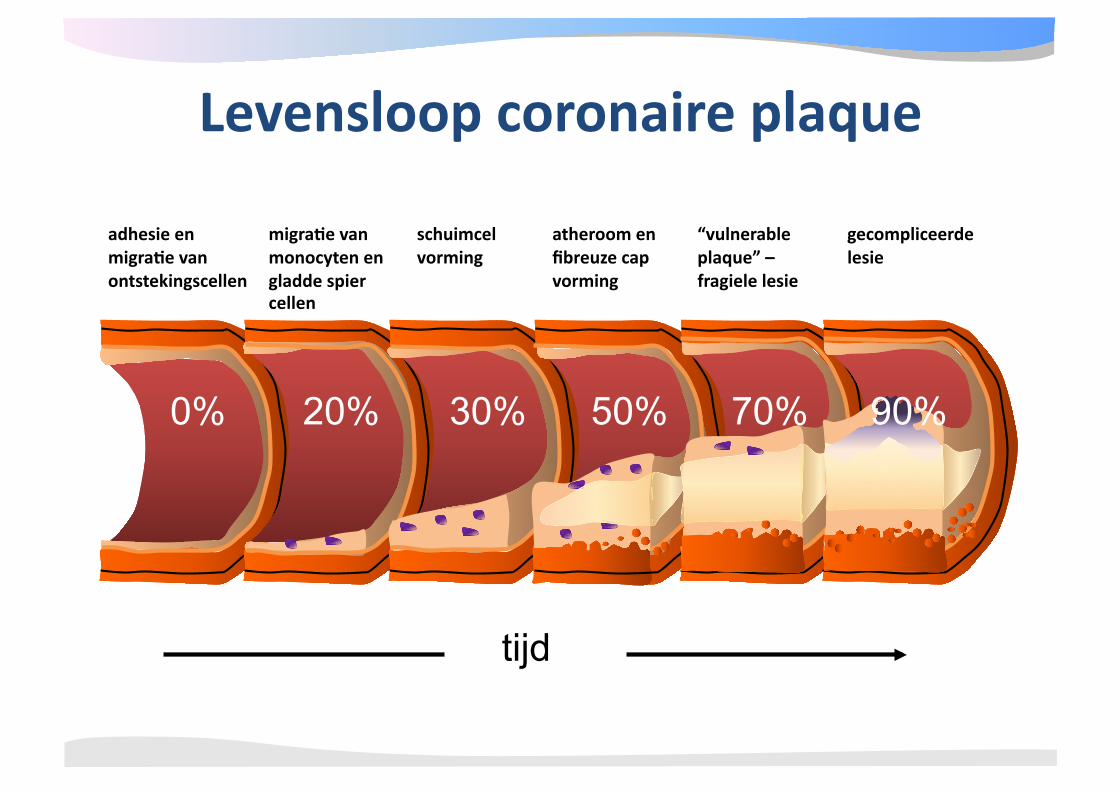
Levensloop coronaire plaque
adhesie en migra4e van ontstekingscellen
0%
migra4e van monocyten en gladde spier cellen
20%
schuimcel vorming
30%
atheroom en fibreuze cap vorming
50%
“vulnerable plaque” – fragiele lesie
70%
gecompliceerde lesie
90%
Pathofysiologie
• Acuut myocard infarct – Enzymen (troponines, CK-MB) + 1 of meer
van de volgende 1. Ischaemische symptomen 2. ECG afwijkingen passend bij ischaemie of
necrose: ontwikkeling van Q-golven, ST↑↓ 3. Pathologische kenmerken van AMI (echo)
Groo[e van infarct
Demand vs supply: – Supply: • plaats afsluiting (proximaal/ distaal) • duur afsluiting irreversibel na 20-30 min • collaterale doorbloeding • (Hb, PO2)
– Demand • zuurstof behoefte myocard • frequentie, RR, contractiliteit
Collateraal vorming
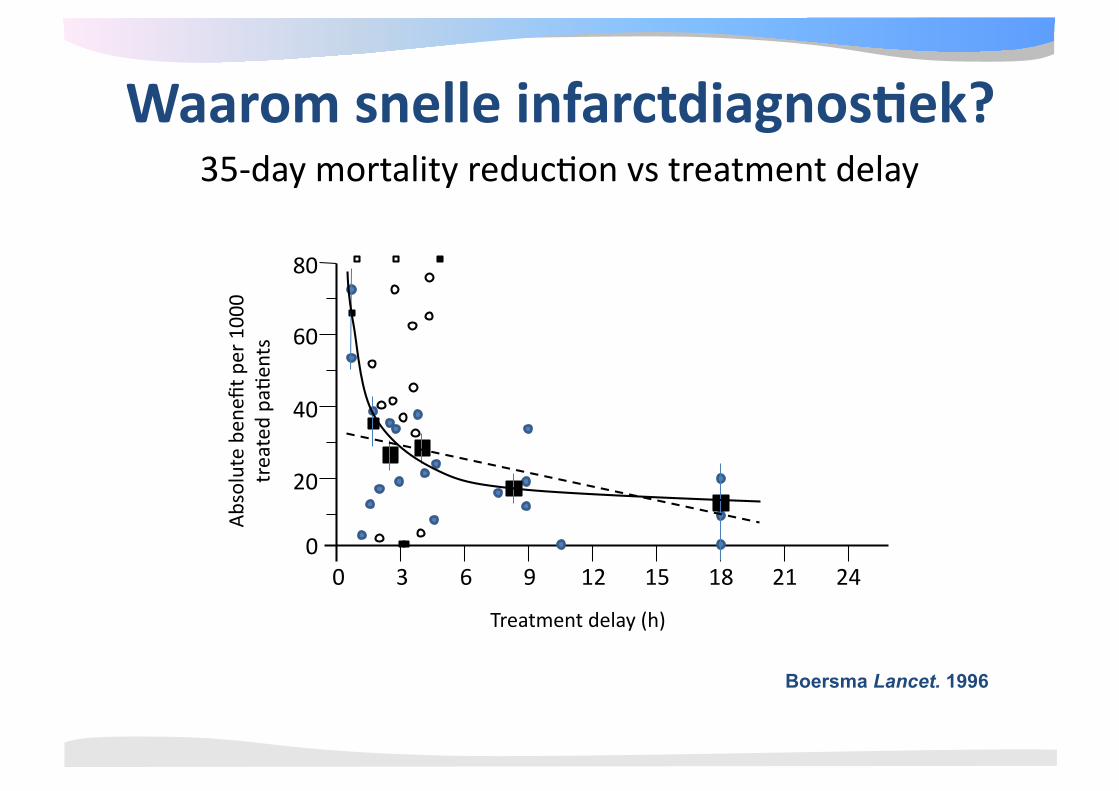
35‐day mortality reduc@on vs treatment delay
Boersma Lancet. 1996
0 3 6 9 12 15 18 21 24
80
60
40
20
0
Treatment delay (h)
Absolute be
nefit per 100
0 treated pa@e
nts
Waarom snelle infarctdiagnos4ek?
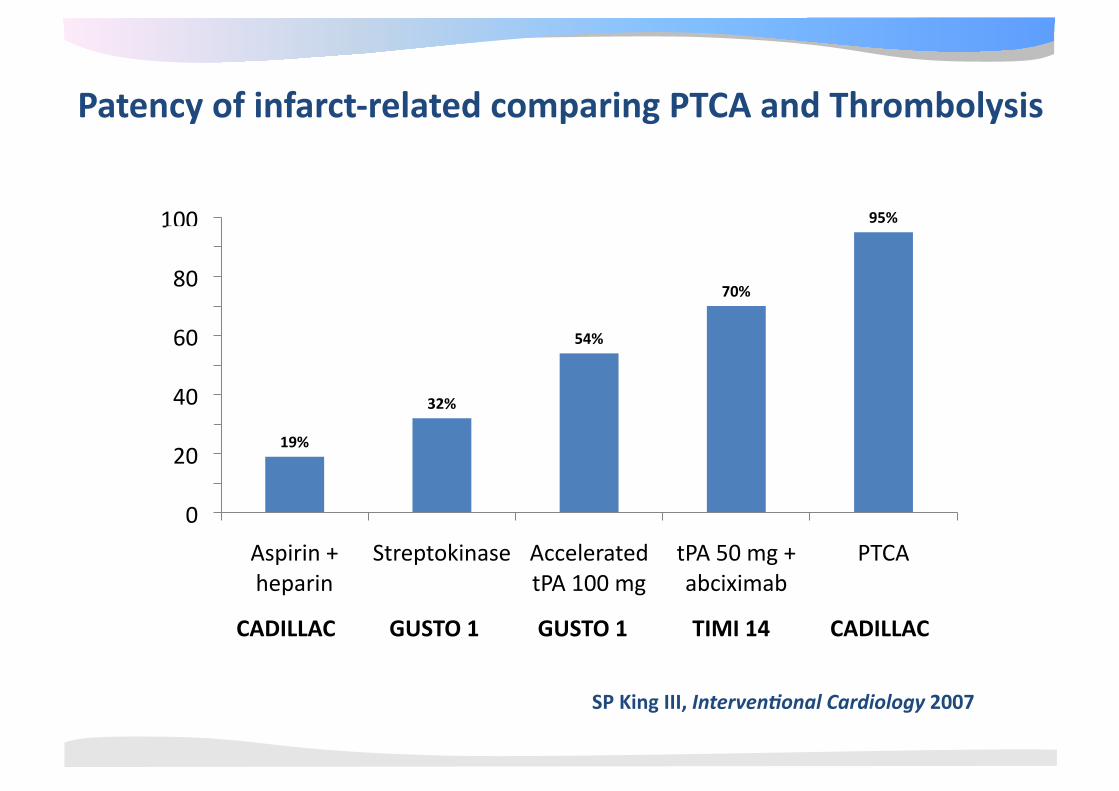
SP King III, Interven,onal Cardiology 2007
CADILLAC GUSTO 1 GUSTO 1 TIMI 14 CADILLAC
19%
32%
54%
70%
95%
0 10 20 30 40 50 60 70 80 90
100
Aspirin + heparin
Streptokinase Accelerated tPA 100 mg
tPA 50 mg + abciximab
PTCA
0
Patency of infarct‐related comparing PTCA and Thrombolysis
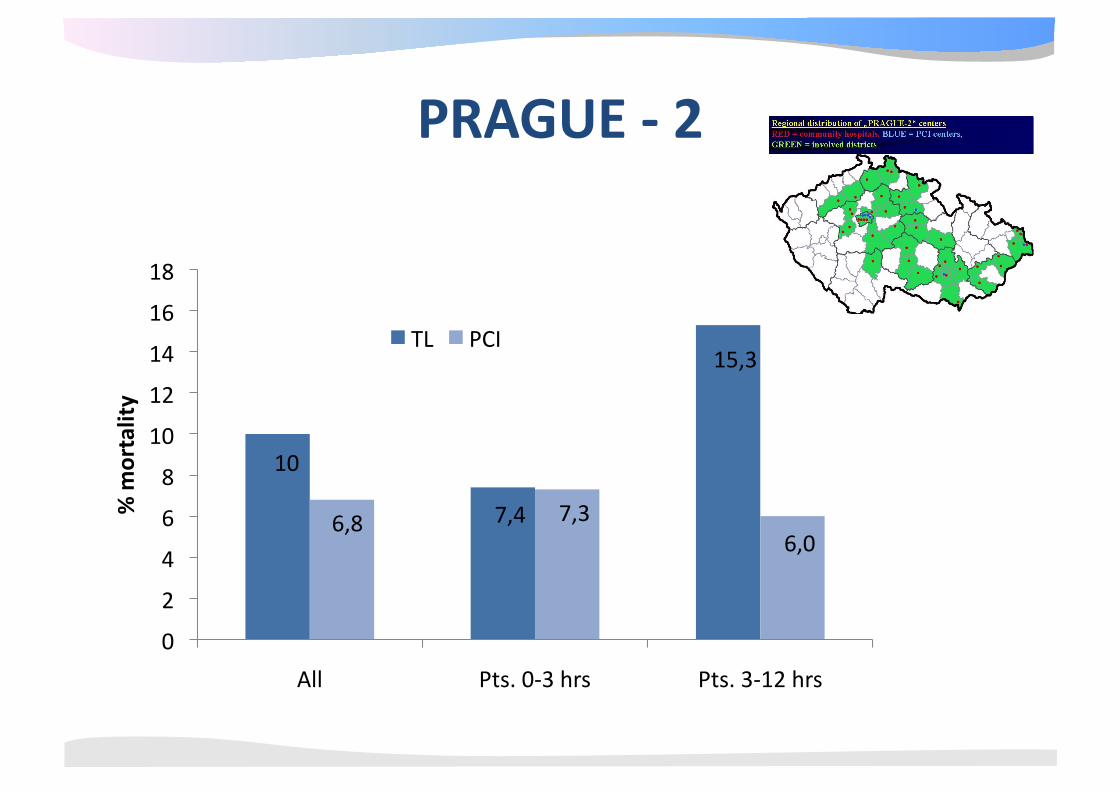
10
7,4
15,3
6,8 7,3 6,0
0
2
4
6
8
10
12
14
16
18
All Pts. 0‐3 hrs Pts. 3‐12 hrs
% m
ortality
TL PCI
PRAGUE ‐ 2
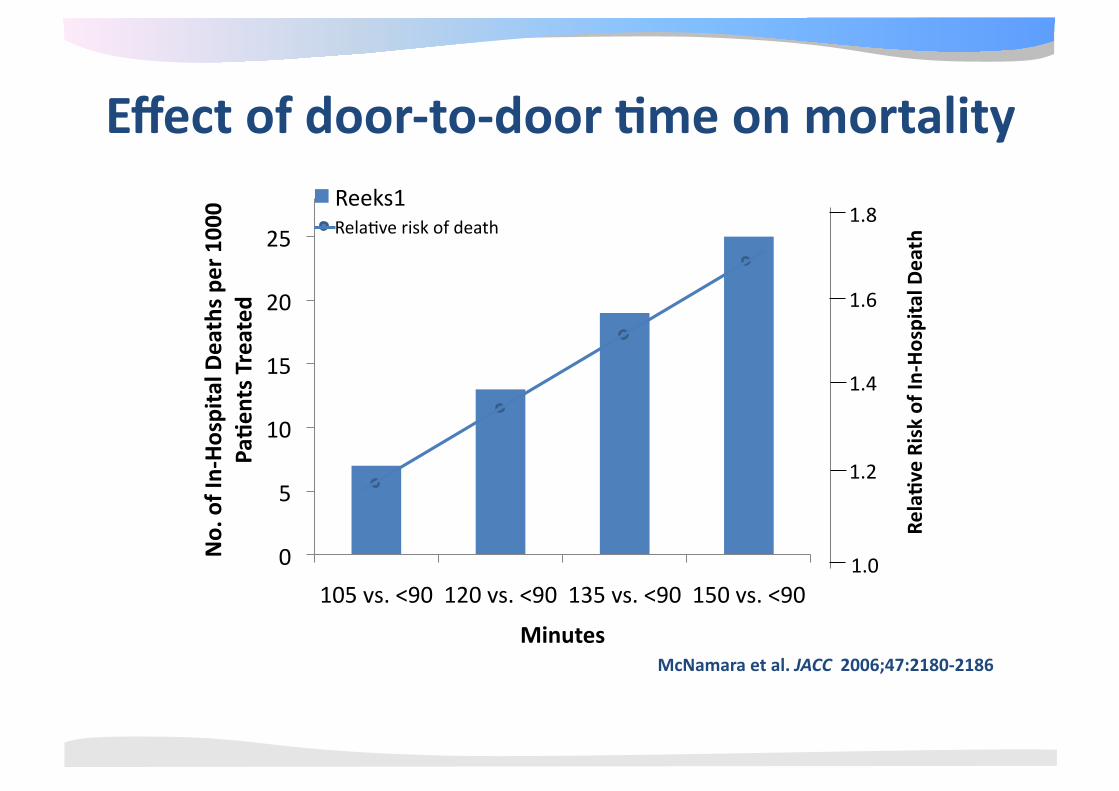
McNamara et al. JACC 2006;47:2180‐2186
0
5
10
15
20
25
105 vs. <90 120 vs. <90 135 vs. <90 150 vs. <90
No. of In‐Hospital D
eaths pe
r 10
00
Pa4en
ts Treated
Minutes
Reeks1 Rela@ve risk of death
1.2
1.4
1.6
1.8
Rela4ve Risk of In
‐Hospital D
eath
1.0
Effect of door‐to‐door 4me on mortality
Symptoms < 12 hrs
Time from “first medical contact” to start reperfusion therapy ≤ 90 min.
Experienced team, high volume center
AHC / AHA Guidelines
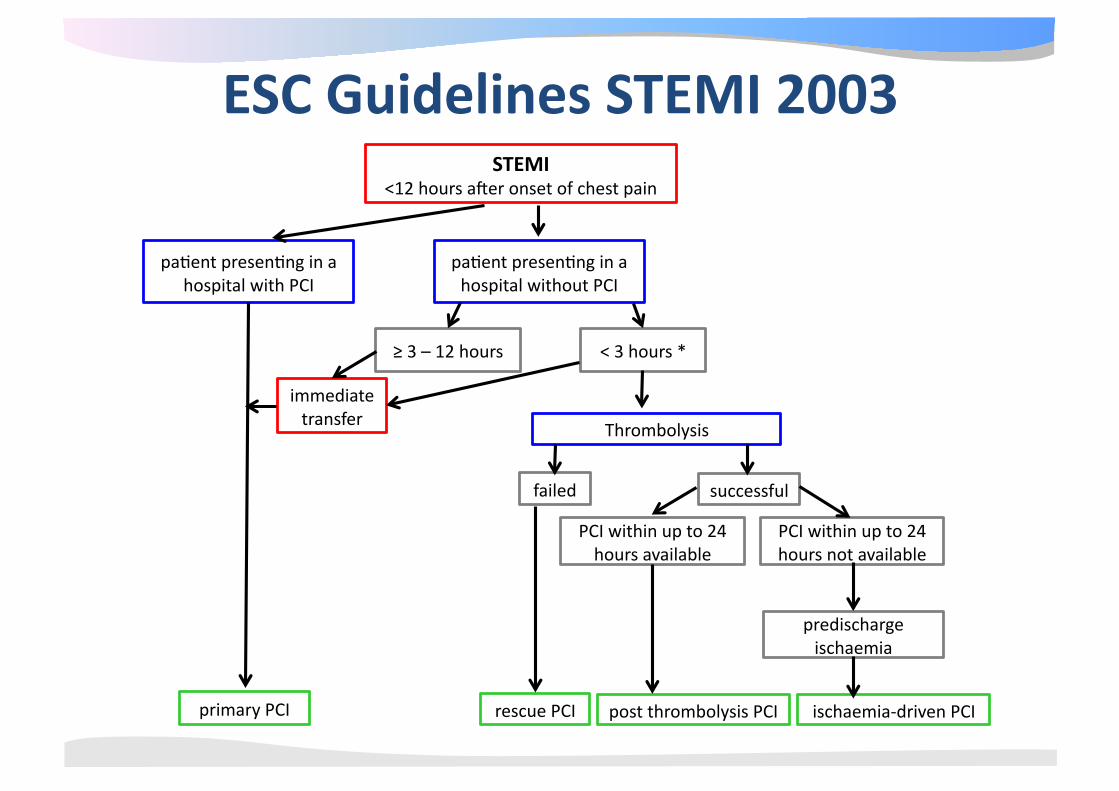
STEMI <12 hours aker onset of chest pain
pa@ent presen@ng in a hospital with PCI
pa@ent presen@ng in a hospital without PCI
immediate transfer
Thrombolysis
≥ 3 – 12 hours < 3 hours *
failed successful
PCI within up to 24 hours available
PCI within up to 24 hours not available
predischarge ischaemia
primary PCI rescue PCI post thrombolysis PCI ischaemia‐driven PCI
ESC Guidelines STEMI 2003
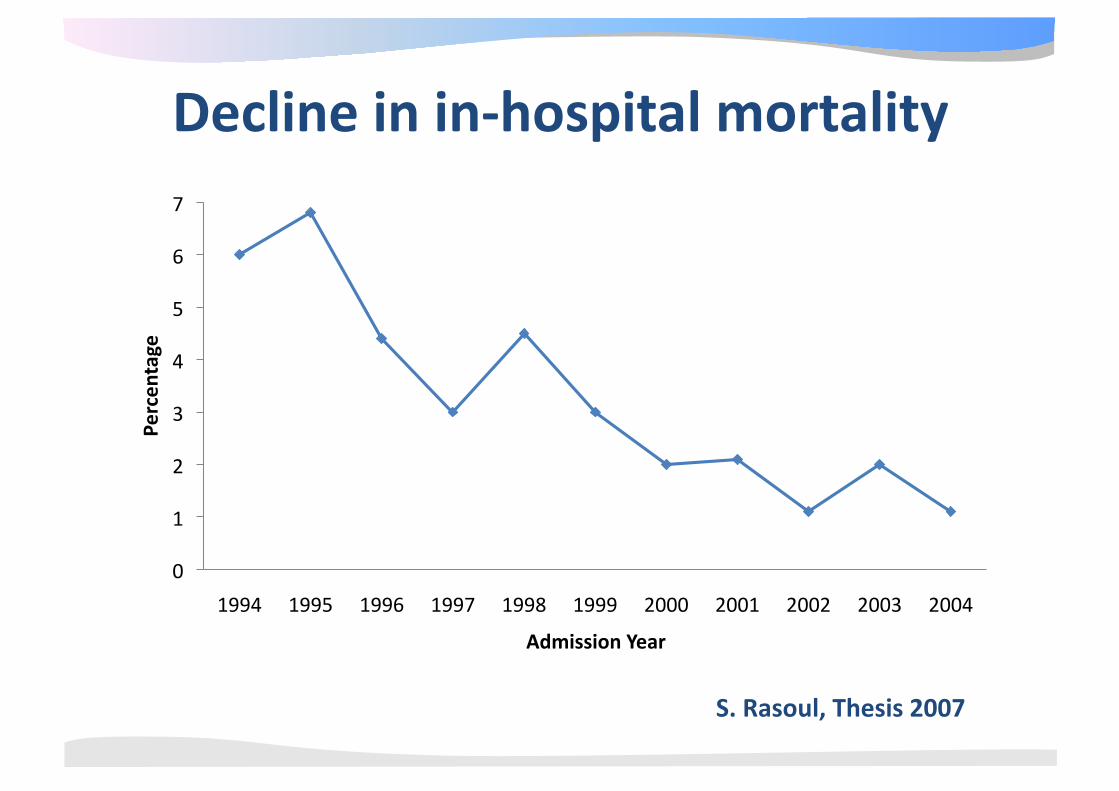
S. Rasoul, Thesis 2007
0
1
2
3
4
5
6
7
1994 1995 1996 1997 1998 1999 2000 2001 2002 2003 2004
Percen
tage
Admission Year
Decline in in‐hospital mortality
Algemene Infarct Diagnos@ek
• Anamnese – Drukkende retrosternale POB, dyspnoe, radia@e, angst, vegeta@ef, (geen) reac@e op NTG, collaps , risicofactoren
• Lichamelijk onderzoek – Vegeta@eve verschijnselen, pols, bloeddruk, decompensa@o cordis, shock
• ECG – ST devia@e, Q’s, ritme‐/ geleidingsstoornissen (LBTB)
• Lab – troponine, CKMB etc
Algemene Diagnos@ek
• Mogelijke gevolgen van AMI – Dyspneu: backward failure (MI?)
– Shock: forward failure (ruptuur?) – Duizelig/collaps: ritme‐/ geleidingsstoornissen
(VF familieanamnese!)
– CVA: LV thrombus/ AFib
• NB: frequent geen (duidelijke) klachten → ouderen, diabe$ci!!
Differen@aal diagnos@ek • Cardiaal
– (pericardi@s, mechanische complica@e (s@l) AMI, takotsubo)
• Vasculair – Type A (B) dissec@e, aneurysma
• Pulmonaal – longembolie
• Gastro‐oesophageaal – spasme
• Bewegingsapparaat – Tietze
ECG Diagnos@ek 1. Acute coronair occlusie
– ST eleva@e, (reciproke) depressie – Q‐vorming
– T‐top inversie – Geleiding: Nieuw linker‐ / rechter bundeltak blok
– As‐draai – QT verlenging
– Ritmestoornissen (VF/ AIVR/ AF/ totaal AVB)
2. Instabiele angina pectoris – Persisterende of voorbijgaande ST depressie – T golf veranderingen (vlak / inversie / pseudo‐normalisa@e)
– Niet‐specifiek / normaal ECG
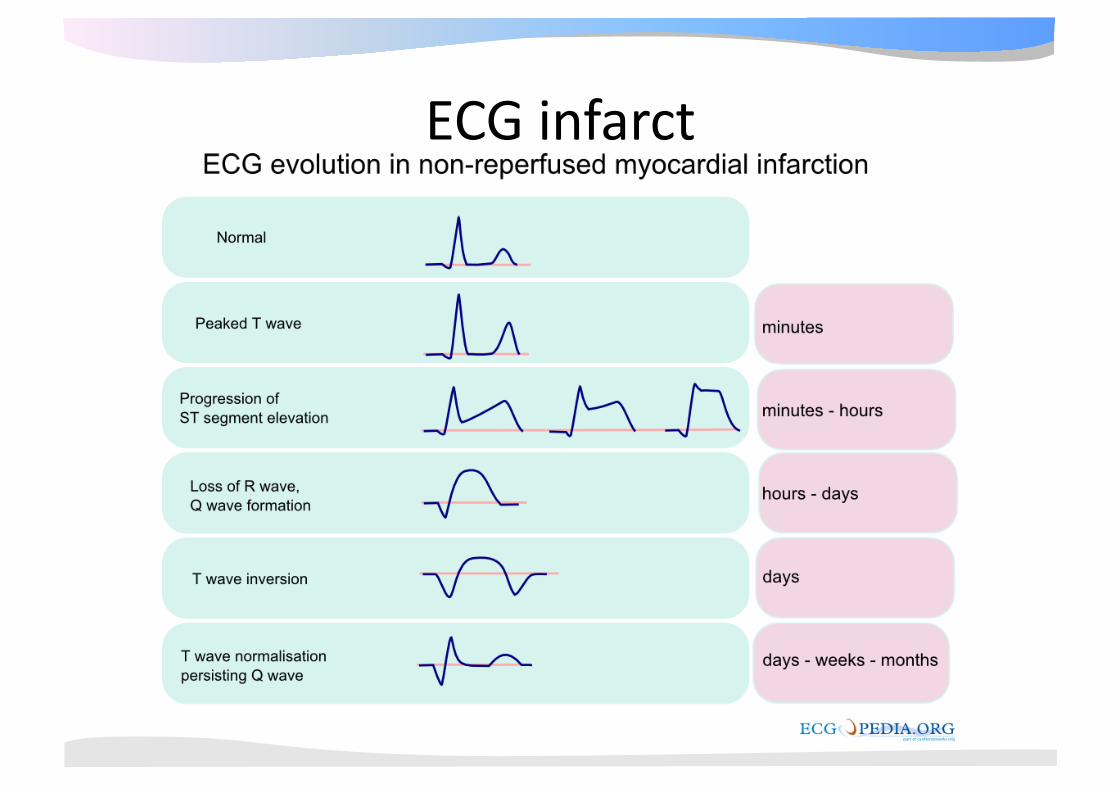
ECG infarct
ECG Diagnos@ek
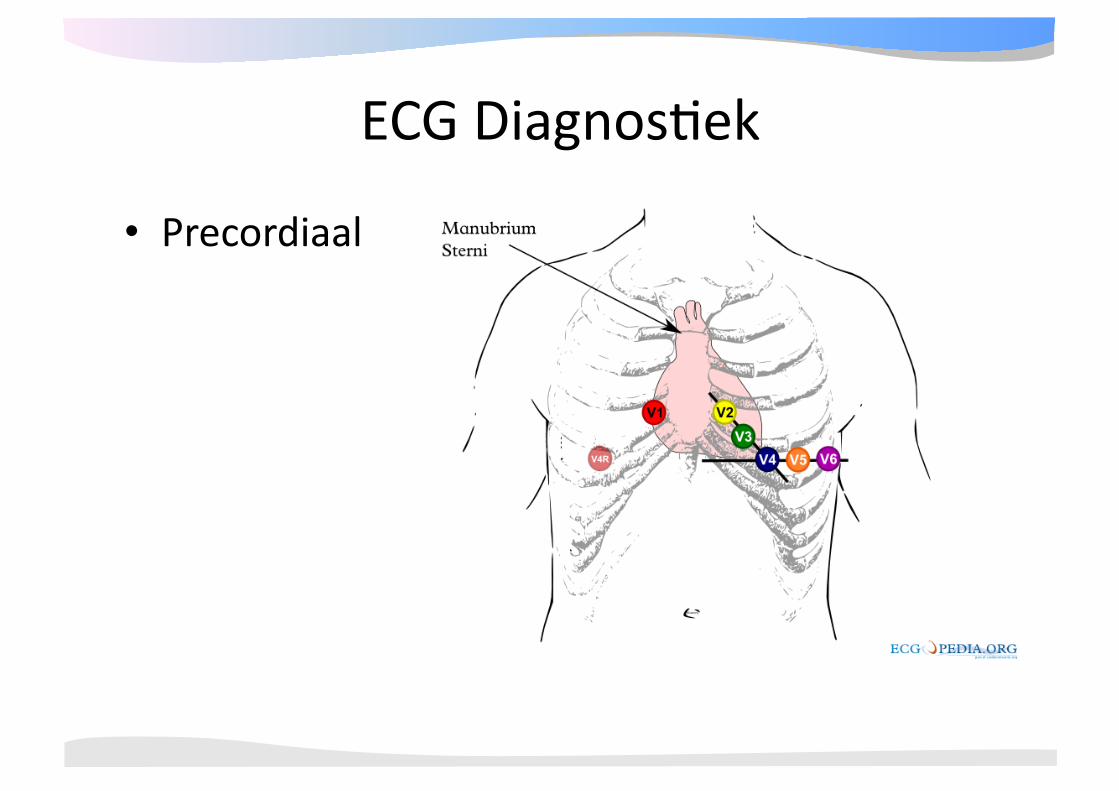
• Precordiaal
ECG Diagnos@ek
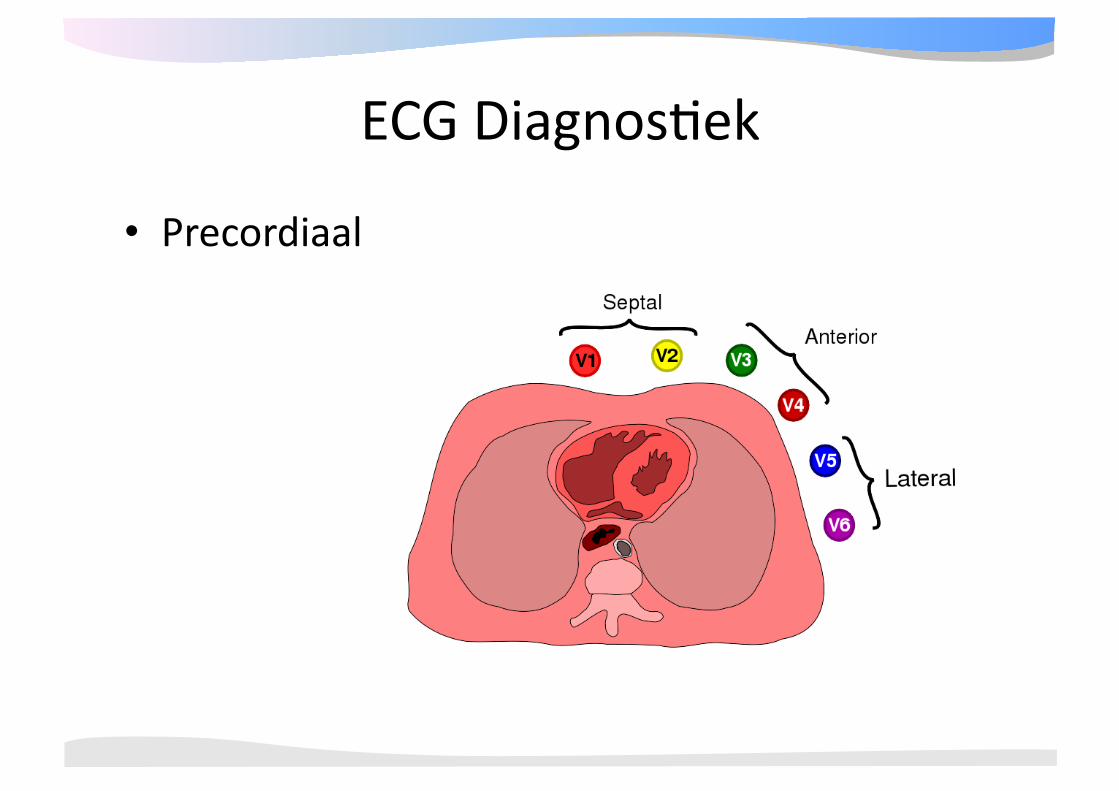
• Precordiaal
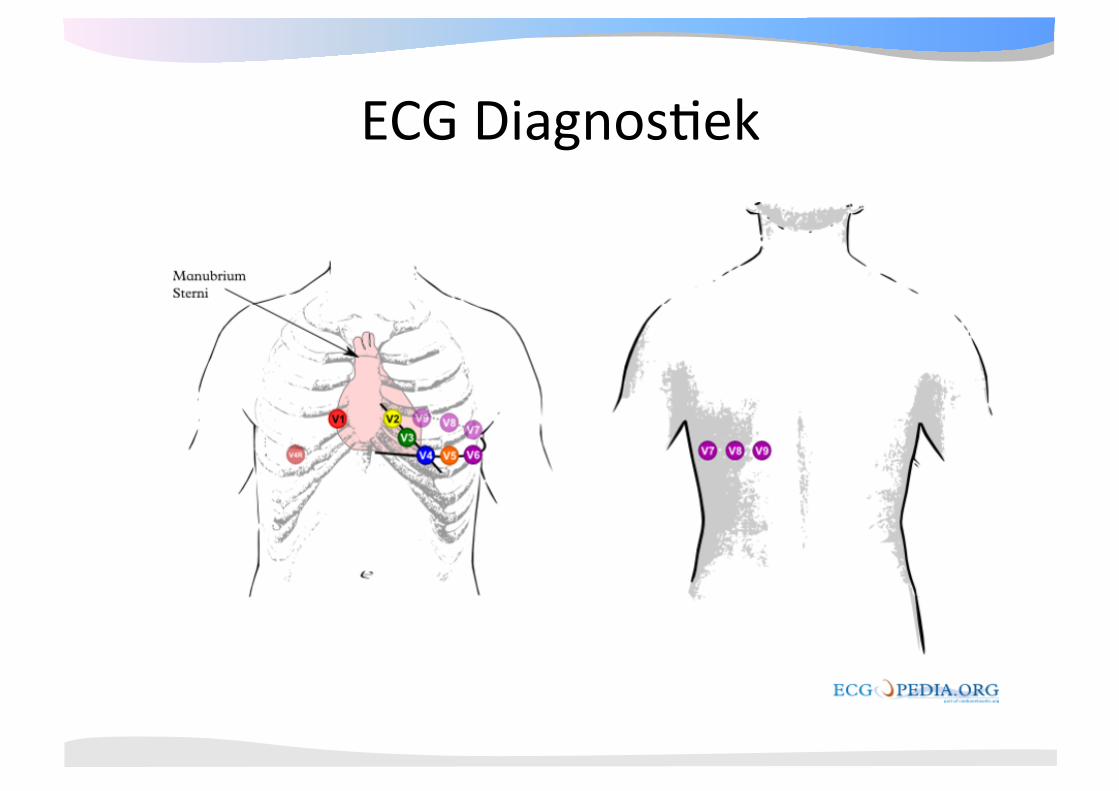
ECG Diagnos@ek
ECG Diagnos@ek
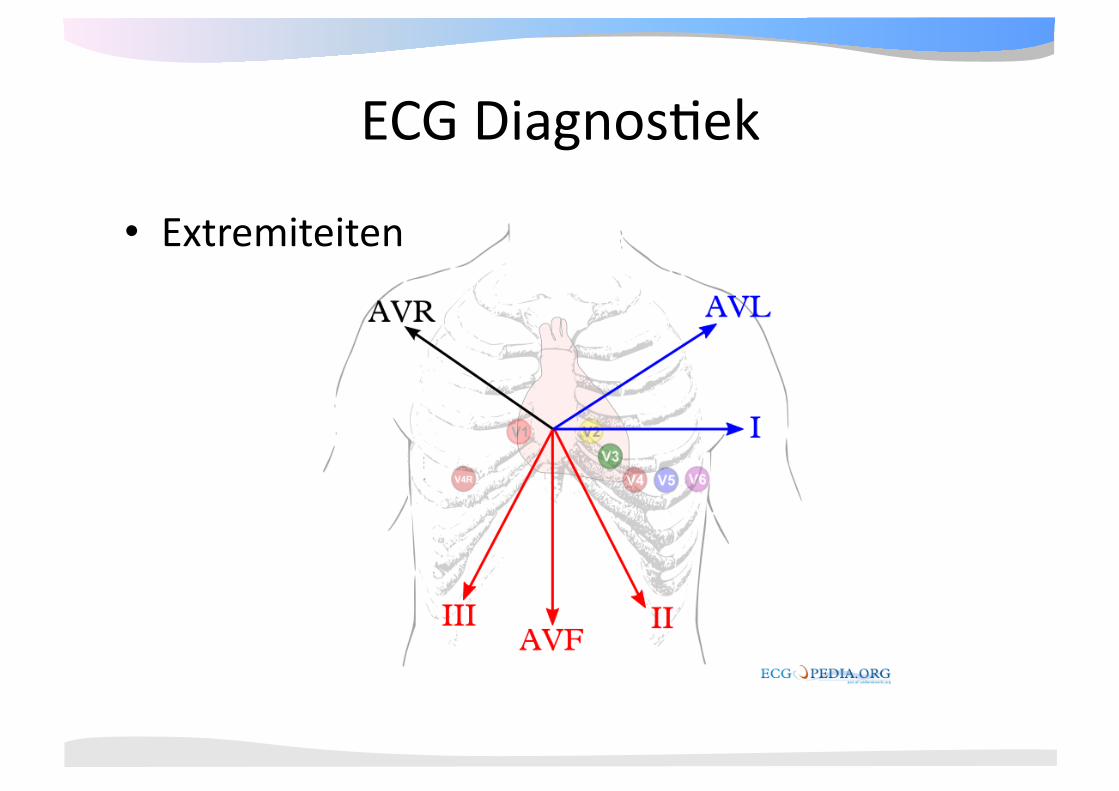
• Extremiteiten
Systema@sche beoordeling • Algemene kenmerken 1. Ritme 2. Frequen@e 3. Geleidings@jden 4. Hartas 5. P top morfologie 6. QRS morfologie 7. ST morfologie
• Vergelijking met oud ECG
• Conclusie
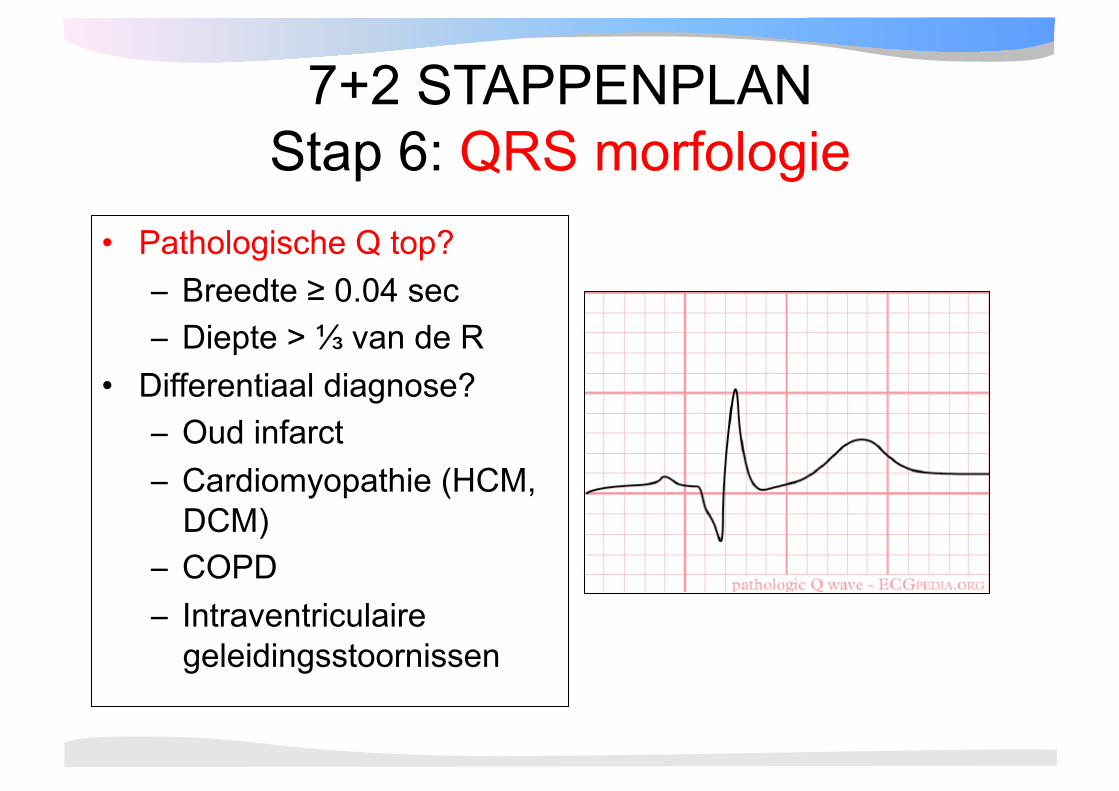
7+2 STAPPENPLAN Stap 6: QRS morfologie
• Pathologische Q top? – Breedte ≥ 0.04 sec – Diepte > ⅓ van de R
• Differentiaal diagnose? – Oud infarct – Cardiomyopathie (HCM,
DCM) – COPD – Intraventriculaire
geleidingsstoornissen
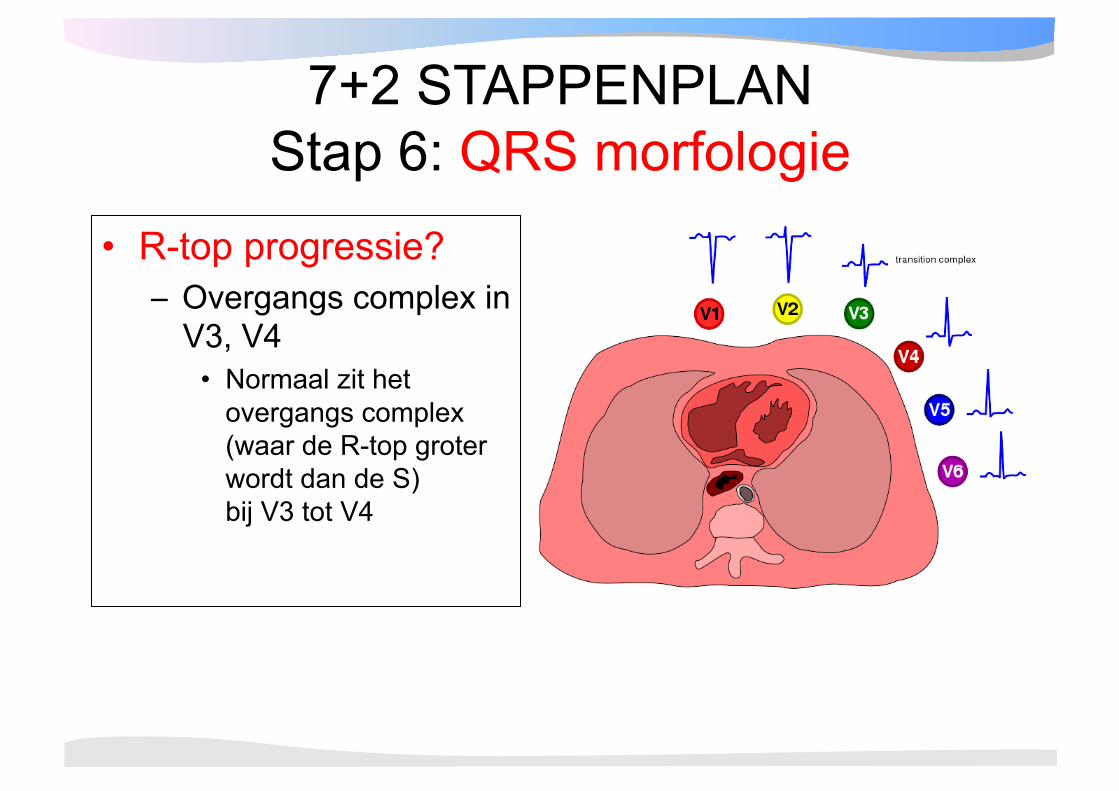
7+2 STAPPENPLAN Stap 6: QRS morfologie
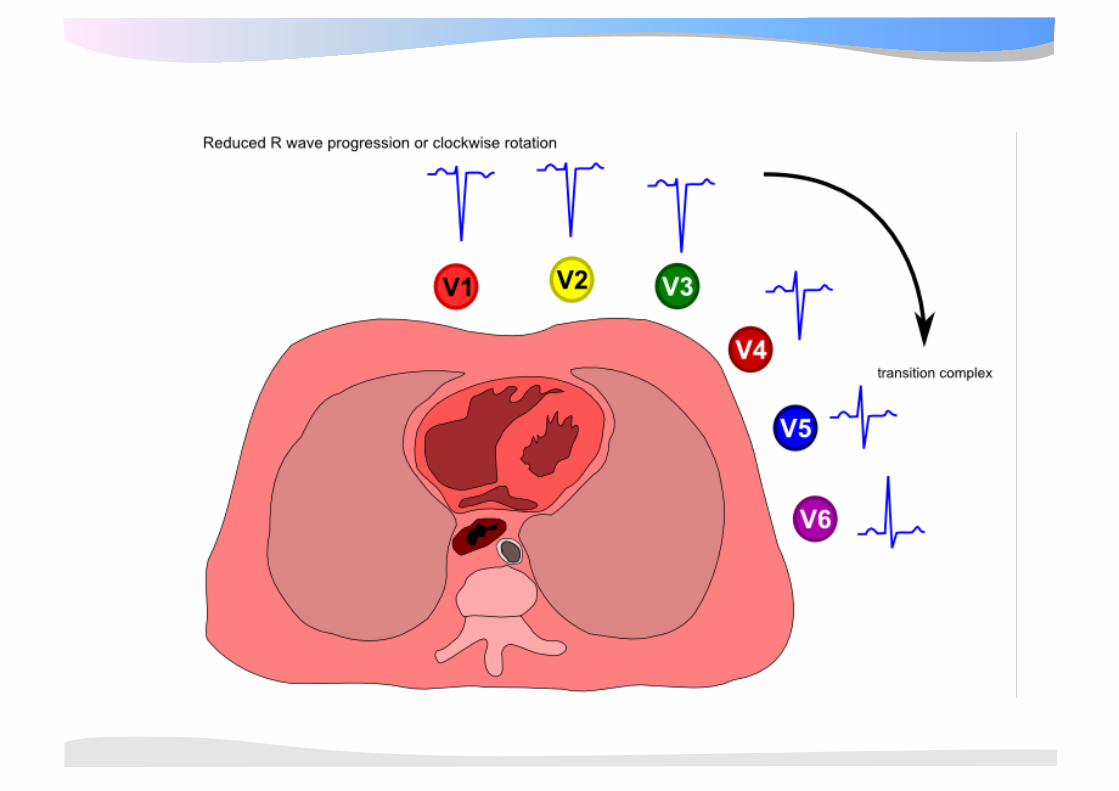
• R-top progressie? – Overgangs complex in
V3, V4 • Normaal zit het
overgangs complex (waar de R-top groter wordt dan de S) bij V3 tot V4
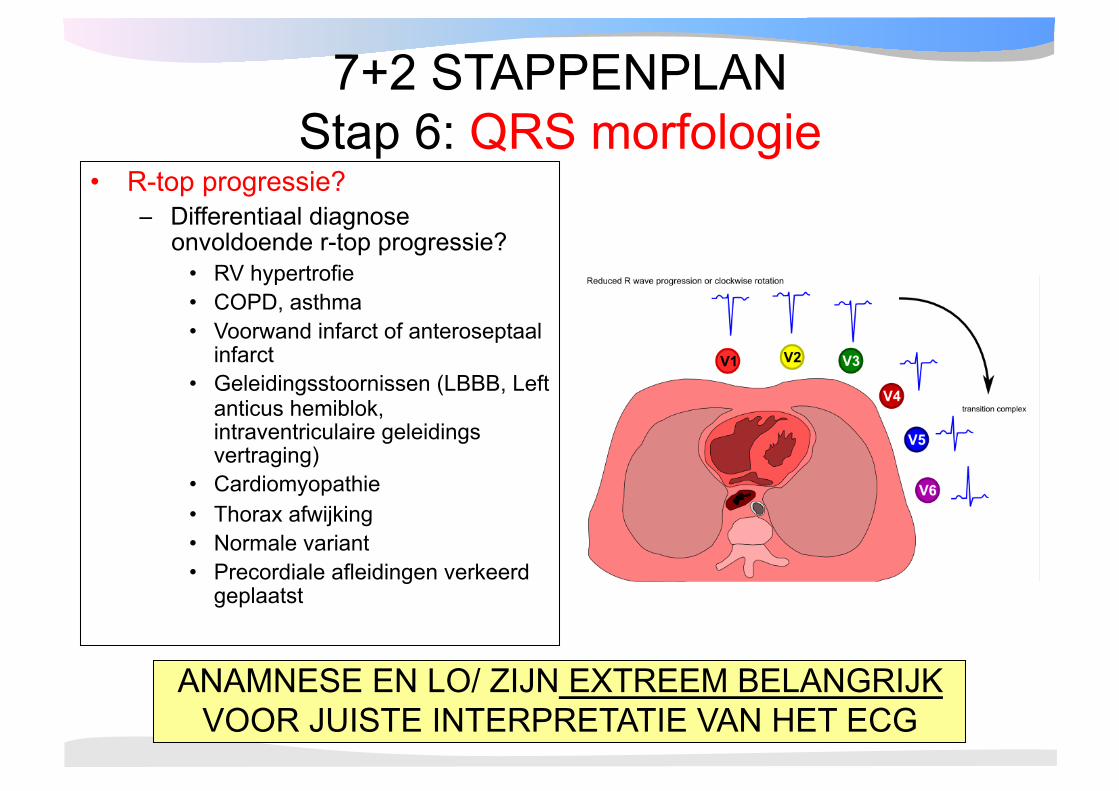
7+2 STAPPENPLAN Stap 6: QRS morfologie
• R-top progressie? – Differentiaal diagnose
onvoldoende r-top progressie? • RV hypertrofie • COPD, asthma • Voorwand infarct of anteroseptaal
infarct • Geleidingsstoornissen (LBBB, Left
anticus hemiblok, intraventriculaire geleidings vertraging)
• Cardiomyopathie • Thorax afwijking • Normale variant • Precordiale afleidingen verkeerd
geplaatst
ANAMNESE EN LO/ ZIJN EXTREEM BELANGRIJK VOOR JUISTE INTERPRETATIE VAN HET ECG
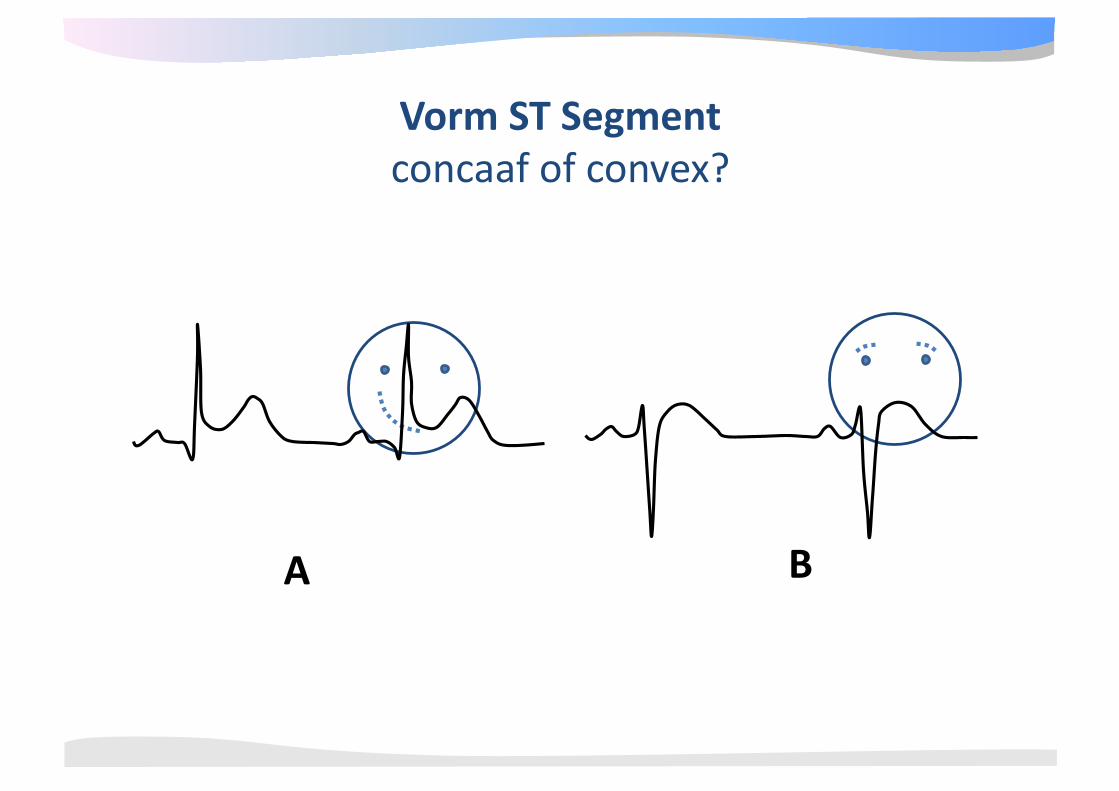
A B
Vorm ST Segment concaaf of convex?
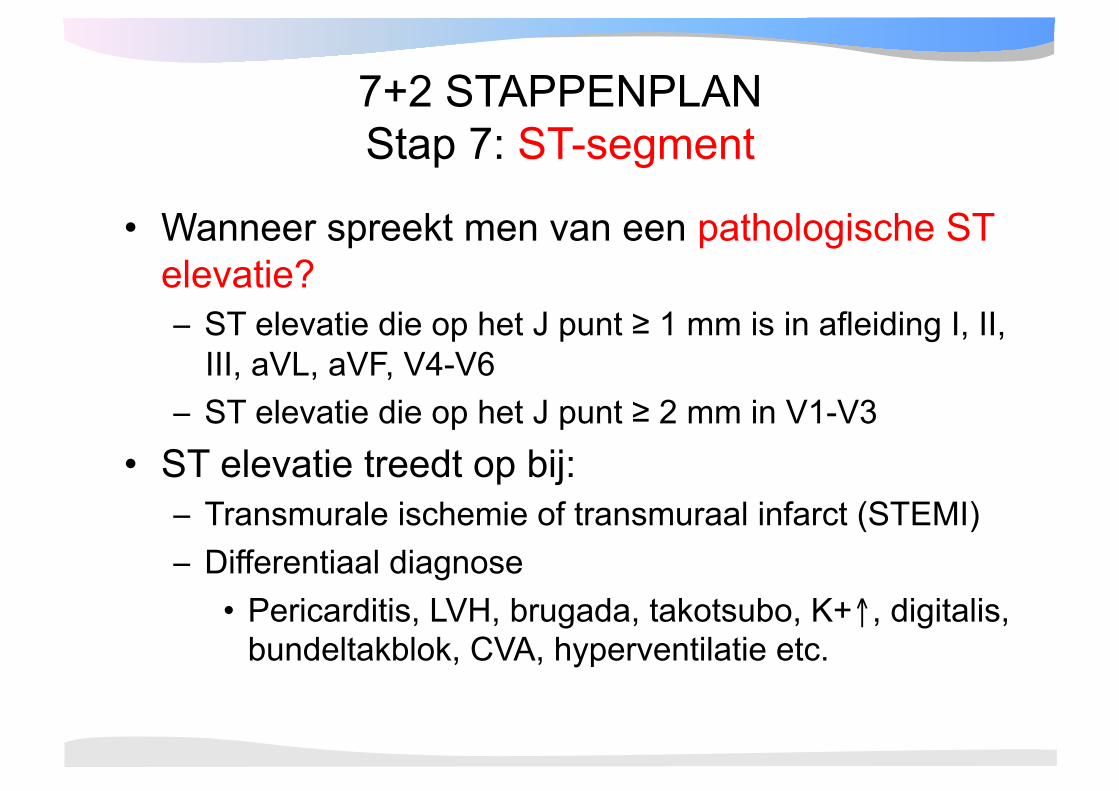
7+2 STAPPENPLAN Stap 7: ST-segment
• Wanneer spreekt men van een pathologische ST elevatie? – ST elevatie die op het J punt ≥ 1 mm is in afleiding I, II,
III, aVL, aVF, V4-V6 – ST elevatie die op het J punt ≥ 2 mm in V1-V3
• ST elevatie treedt op bij: – Transmurale ischemie of transmuraal infarct (STEMI) – Differentiaal diagnose • Pericarditis, LVH, brugada, takotsubo, K+↑, digitalis,
bundeltakblok, CVA, hyperventilatie etc.
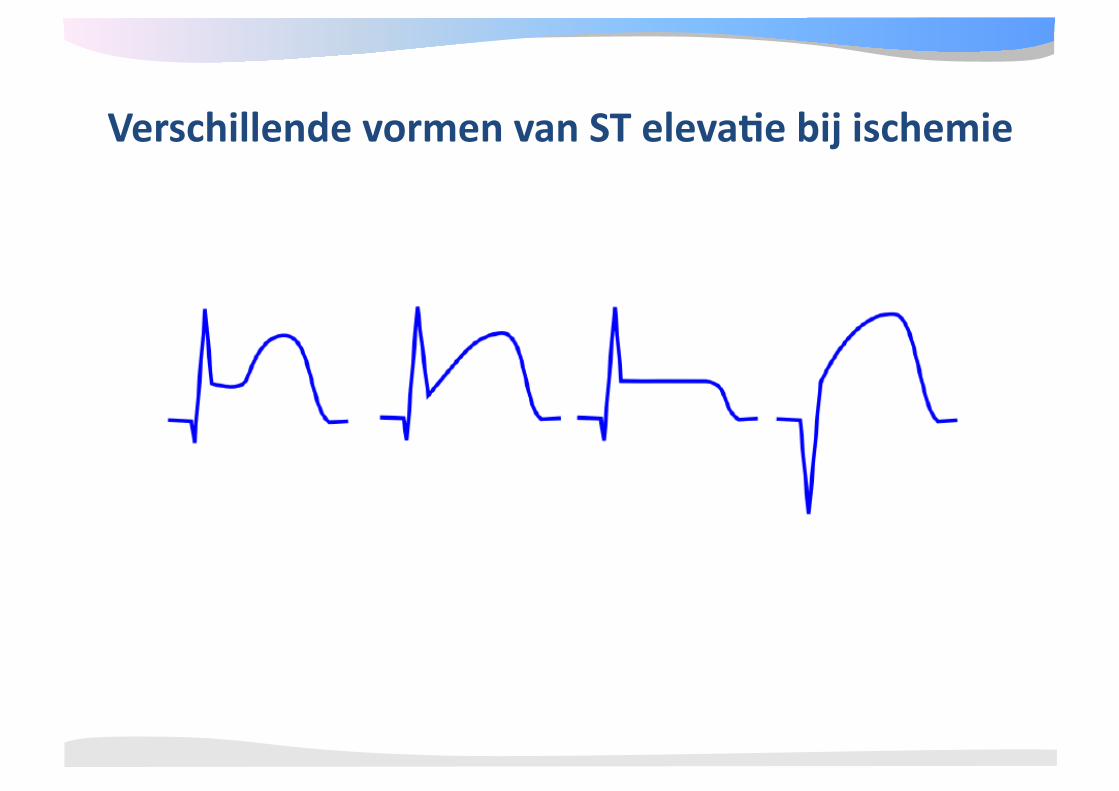
Verschillende vormen van ST eleva4e bij ischemie
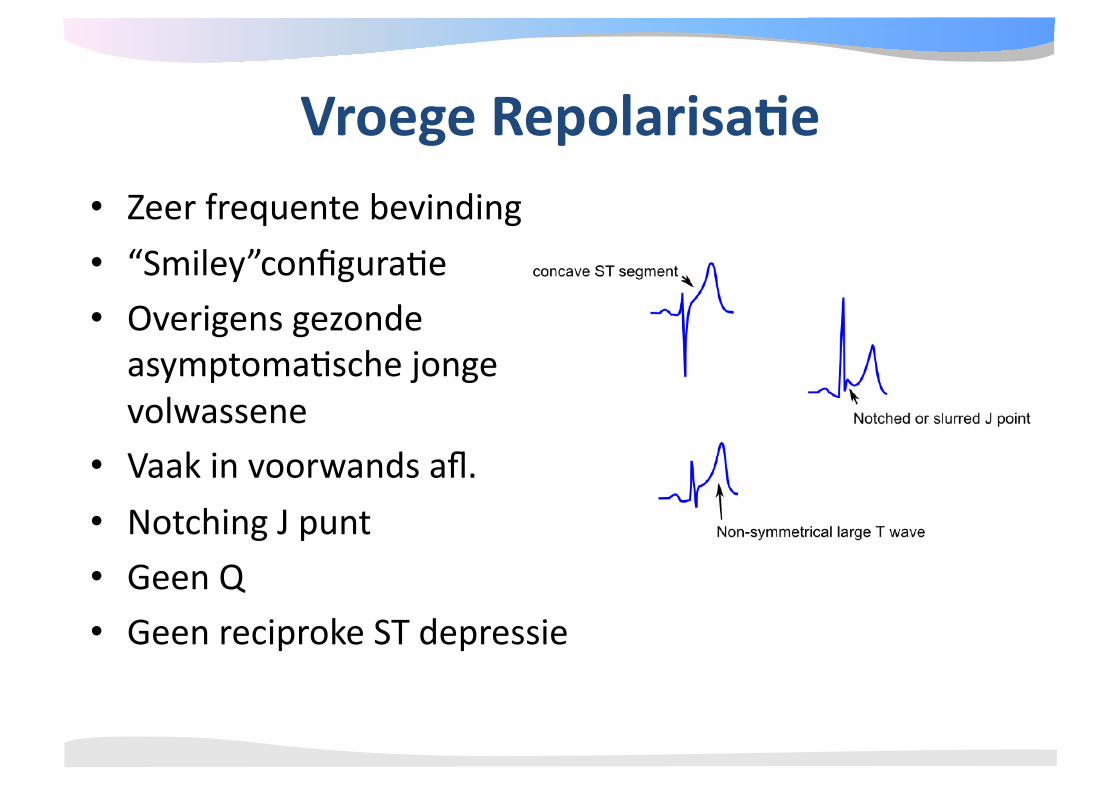
• Zeer frequente bevinding • “Smiley”configura@e • Overigens gezonde asymptoma@sche jonge volwassene
• Vaak in voorwands afl. • Notching J punt • Geen Q • Geen reciproke ST depressie
Vroege Repolarisa4e
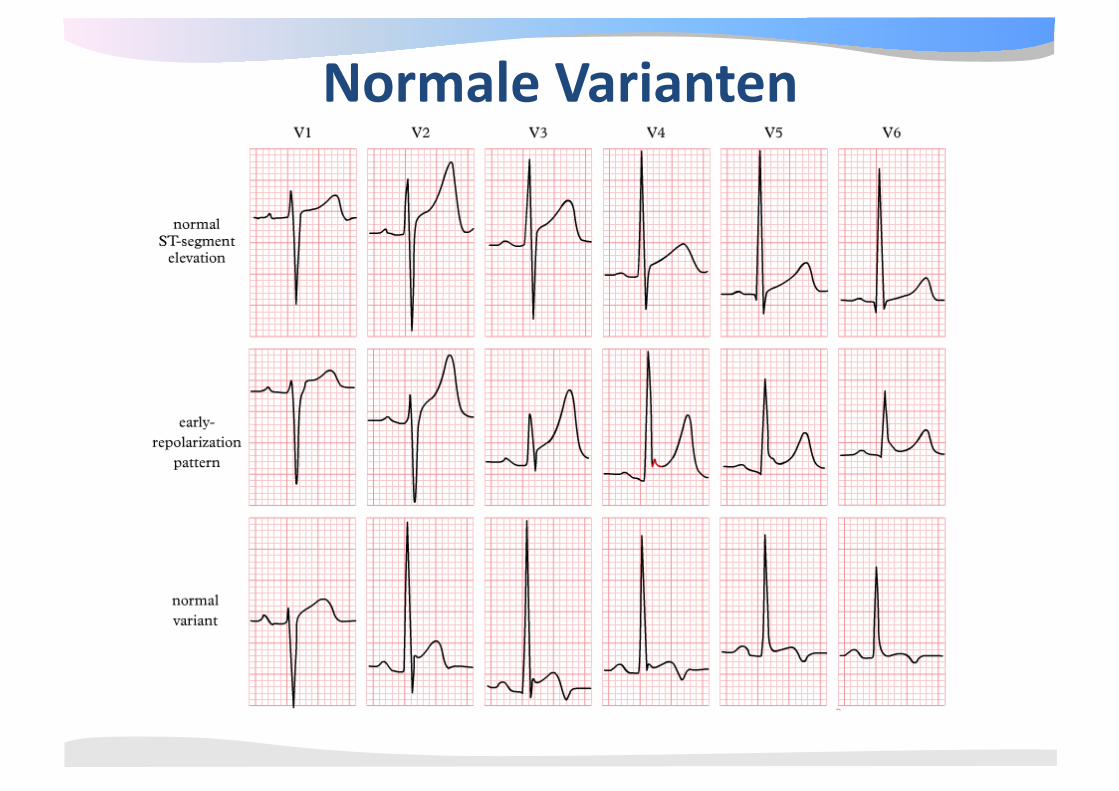
Normale Varianten
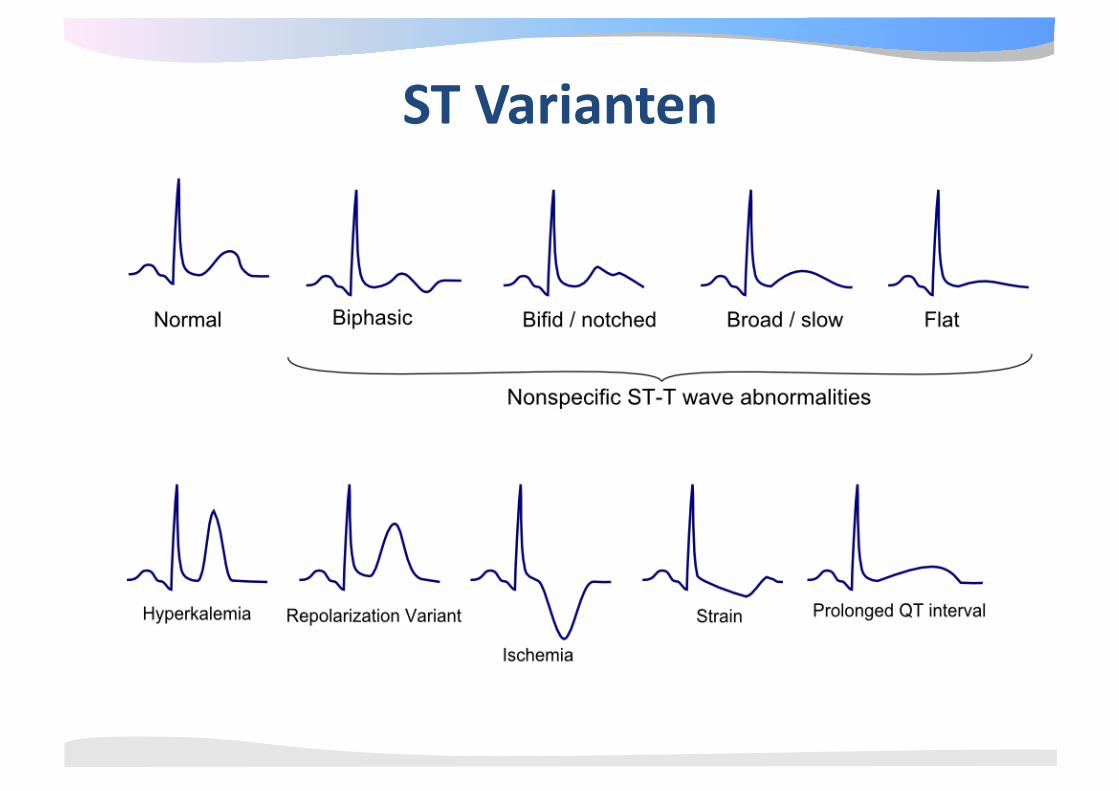
ST Varianten
7+2 STAPPENPLAN Stap 7+1: Vergelijk met oud ECG
• Verandering ritme? – Nieuw boezemfibrilleren?
• Verandering frequentie? – Bradycardie (SB, AV blok→medicatie effect?) of tachycardie ([S]VT)
• Verandering geleidingstijden? – PQ tijd ↑ (medicatie?); QRS↑ (ischemie, medicatie?) QT tijd↑ (medicatie?)
• Verandering hartas? – Verandering geleiding, infarct doorgemaakt?
• Nieuwe pathologische Q’s – Verandering geleiding, infarct doorgemaakt, plaatsing elektroden?
• Verandering R top progressie precordiaal? – Afname R (infarct, tamponade, plaatsing elektroden?) – Toename R top (LVH, RVH, verandering geleiding intraventriculair)
• Verandering ST segment? • Verandering T-top?
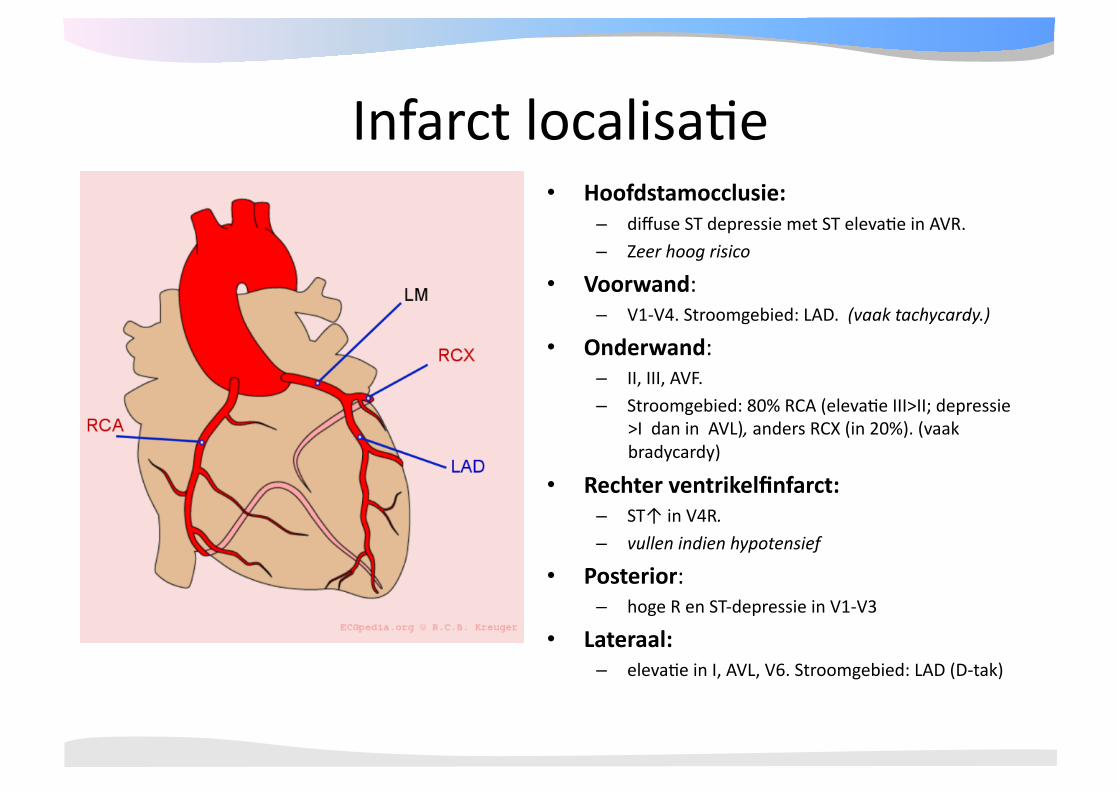
Infarct localisa@e • Hoofdstamocclusie:
– diffuse ST depressie met ST eleva@e in AVR. – Zeer hoog risico
• Voorwand: – V1‐V4. Stroomgebied: LAD. (vaak tachycardy.)
• Onderwand: – II, III, AVF. – Stroomgebied: 80% RCA (eleva@e III>II; depressie
>I dan in AVL), anders RCX (in 20%). (vaak bradycardy)
• Rechter ventrikelfinfarct: – ST↑ in V4R. – vullen indien hypotensief
• Posterior: – hoge R en ST‐depressie in V1‐V3
• Lateraal: – eleva@e in I, AVL, V6. Stroomgebied: LAD (D‐tak)
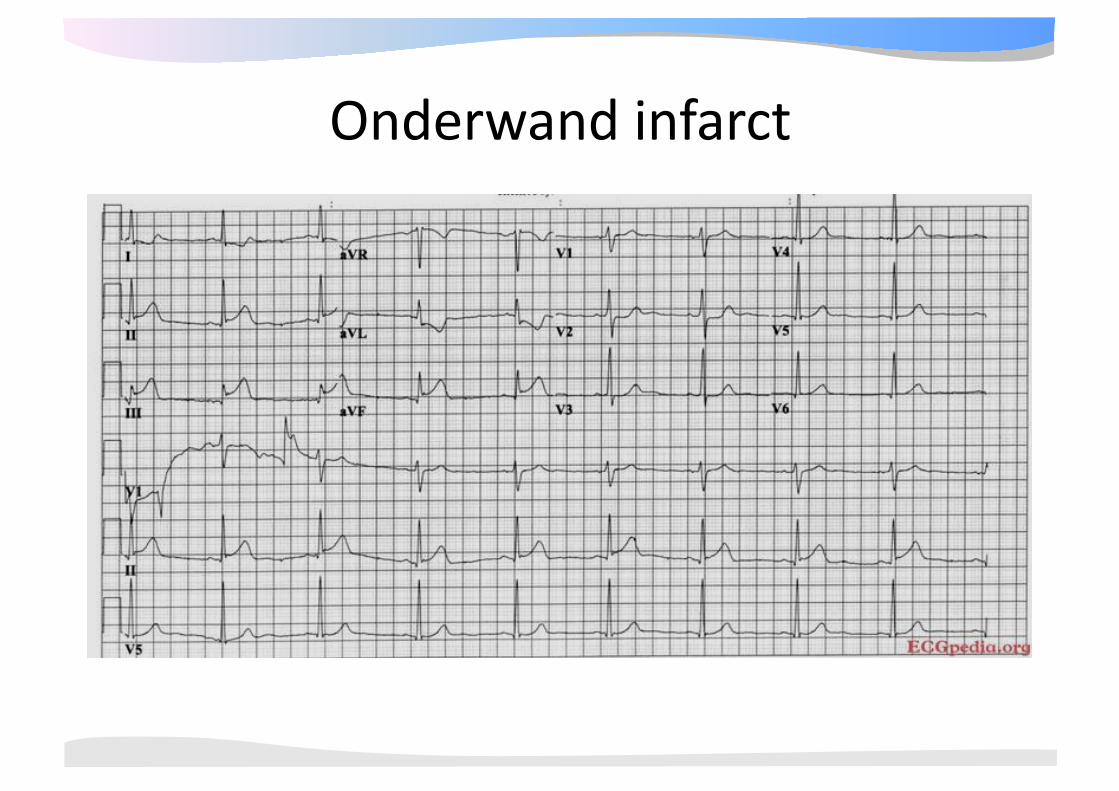
Onderwand infarct
Onderwandinfarct RCA of RCx?
• RCA occlusie – ST eleva@e III > II – ST depressie in aVL > I – V4R isoelectrisch of geëleveerd – RV infarct mogelijk – S:R in aVL > 3
• RCX occlusie: – ST eleva@e II > III – V4R nega@eve T – S:R in aVL < 3
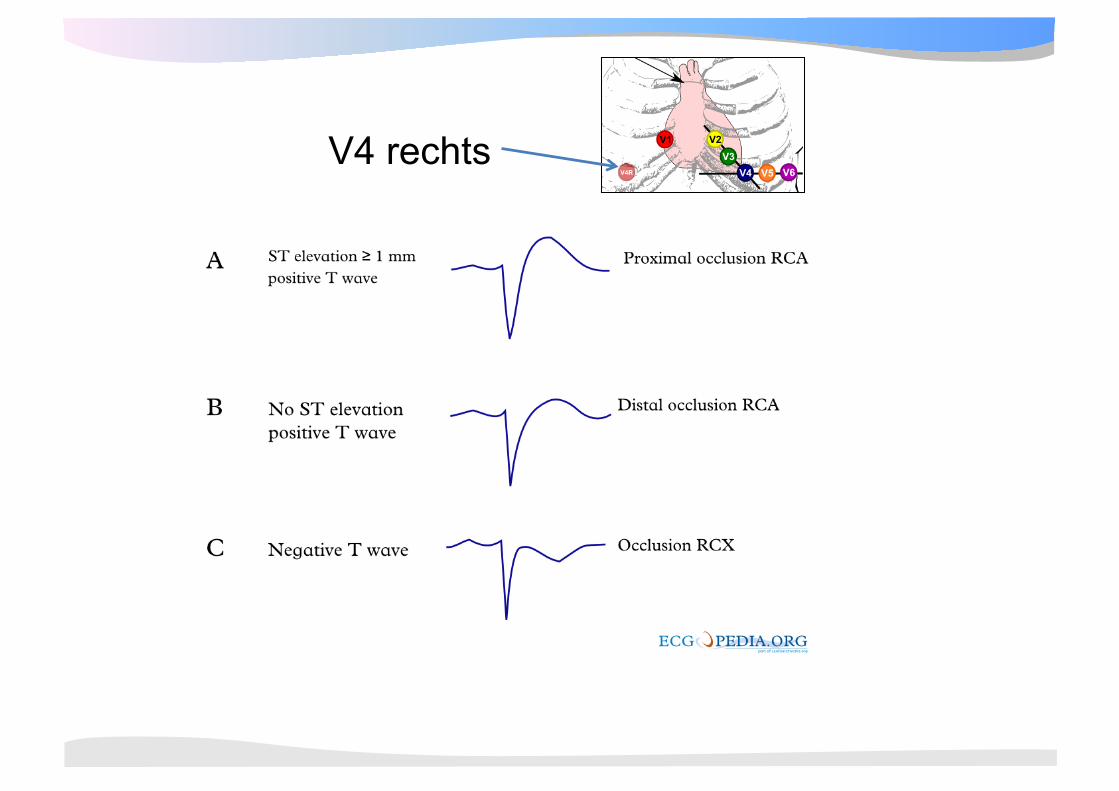
V4 rechts
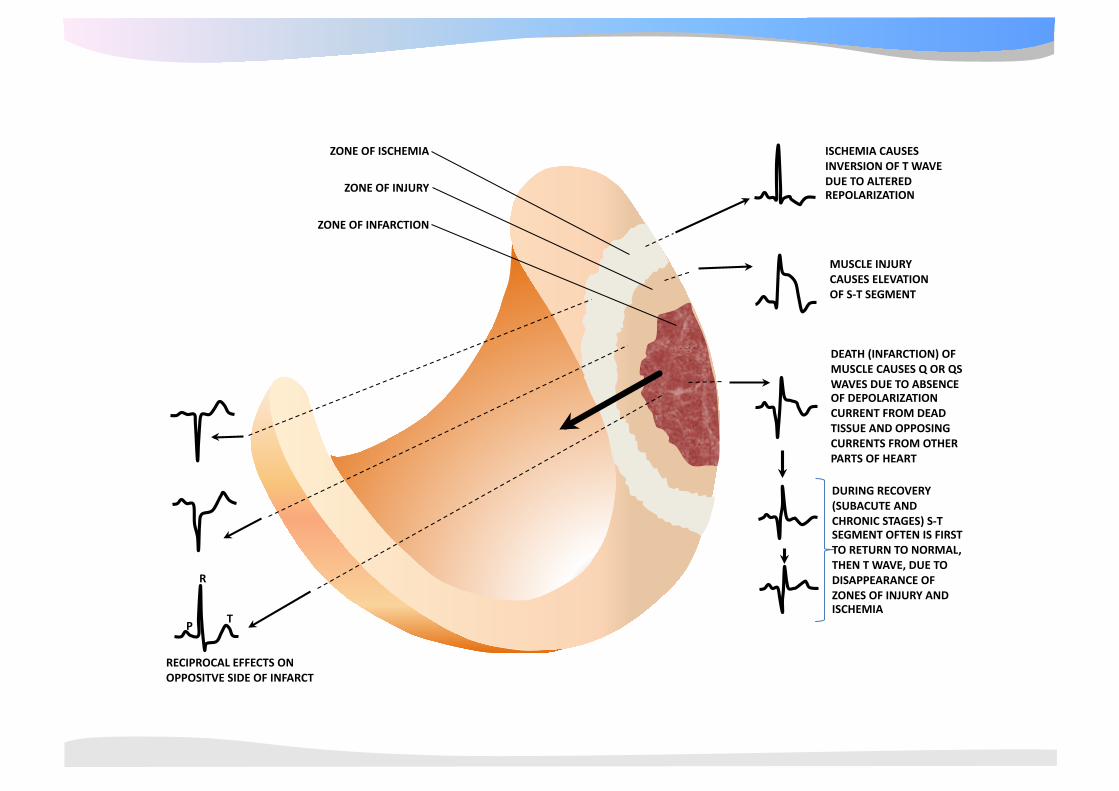
RECIPROCAL EFFECTS ON OPPOSITVE SIDE OF INFARCT
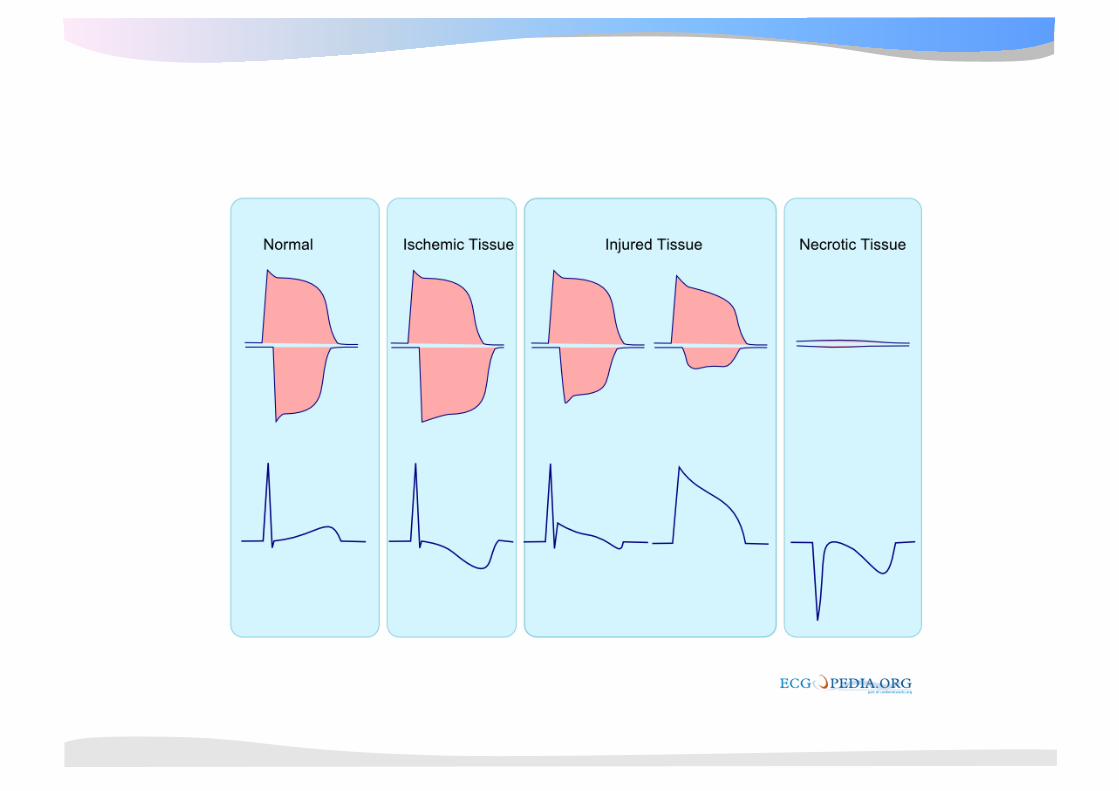
R
TP
ZONE OF ISCHEMIA
ZONE OF INJURY
ZONE OF INFARCTION
ISCHEMIA CAUSES INVERSION OF T WAVE DUE TO ALTERED REPOLARIZATION
MUSCLE INJURY CAUSES ELEVATION OF S‐T SEGMENT
DURING RECOVERY (SUBACUTE AND CHRONIC STAGES) S‐T SEGMENT OFTEN IS FIRST TO RETURN TO NORMAL, THEN T WAVE, DUE TO DISAPPEARANCE OF ZONES OF INJURY AND ISCHEMIA
DEATH (INFARCTION) OF MUSCLE CAUSES Q OR QS WAVES DUE TO ABSENCE OF DEPOLARIZATION CURRENT FROM DEAD TISSUE AND OPPOSING CURRENTS FROM OTHER PARTS OF HEART
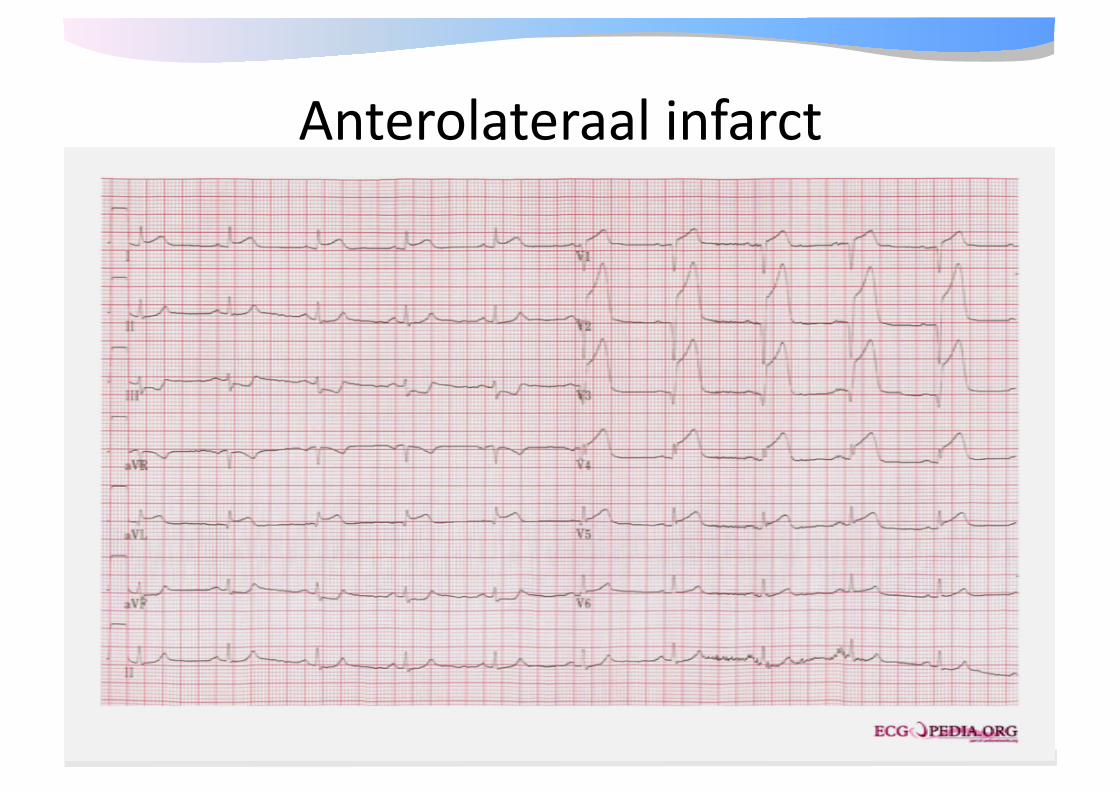
Anterolateraal infarct
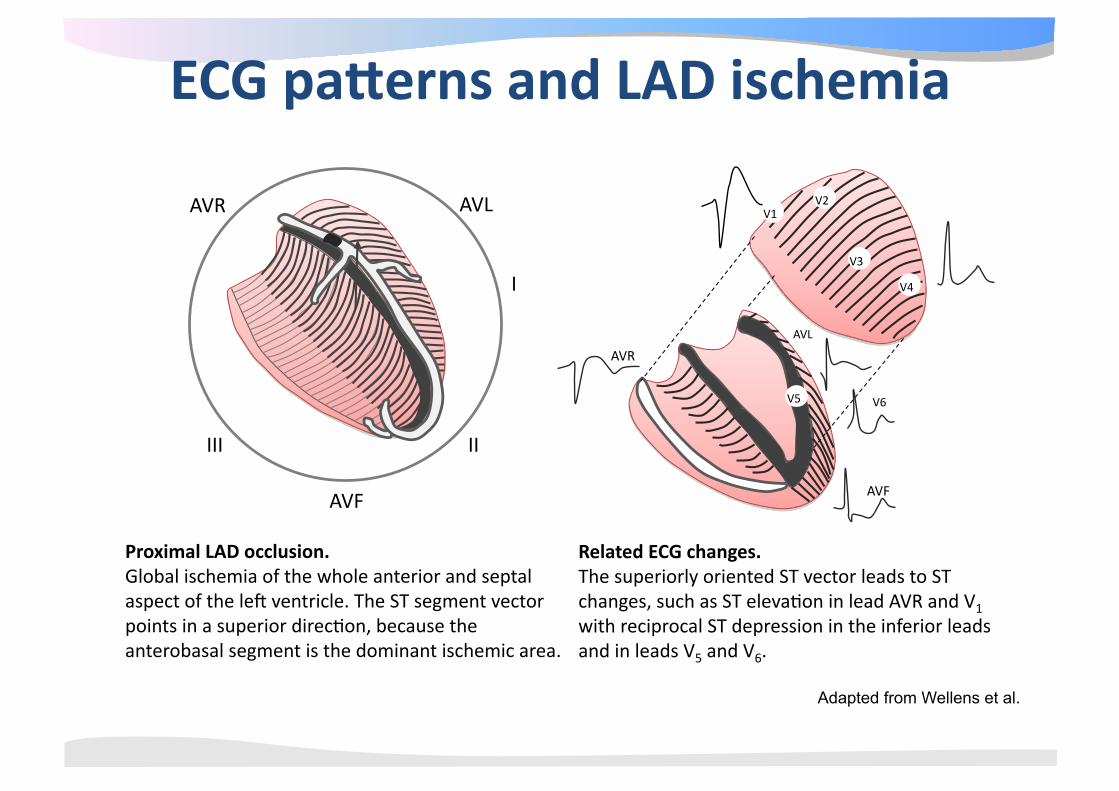
Related ECG changes. The superiorly oriented ST vector leads to ST changes, such as ST eleva@on in lead AVR and V1 with reciprocal ST depression in the inferior leads and in leads V5 and V6.
AVR AVL
I
II
AVF
III
V5
AVF
AVR
V6
AVL
V3
V4
V2 V1
ECG panerns and LAD ischemia
Proximal LAD occlusion. Global ischemia of the whole anterior and septal aspect of the lek ventricle. The ST segment vector points in a superior direc@on, because the anterobasal segment is the dominant ischemic area.
Adapted from Wellens et al.
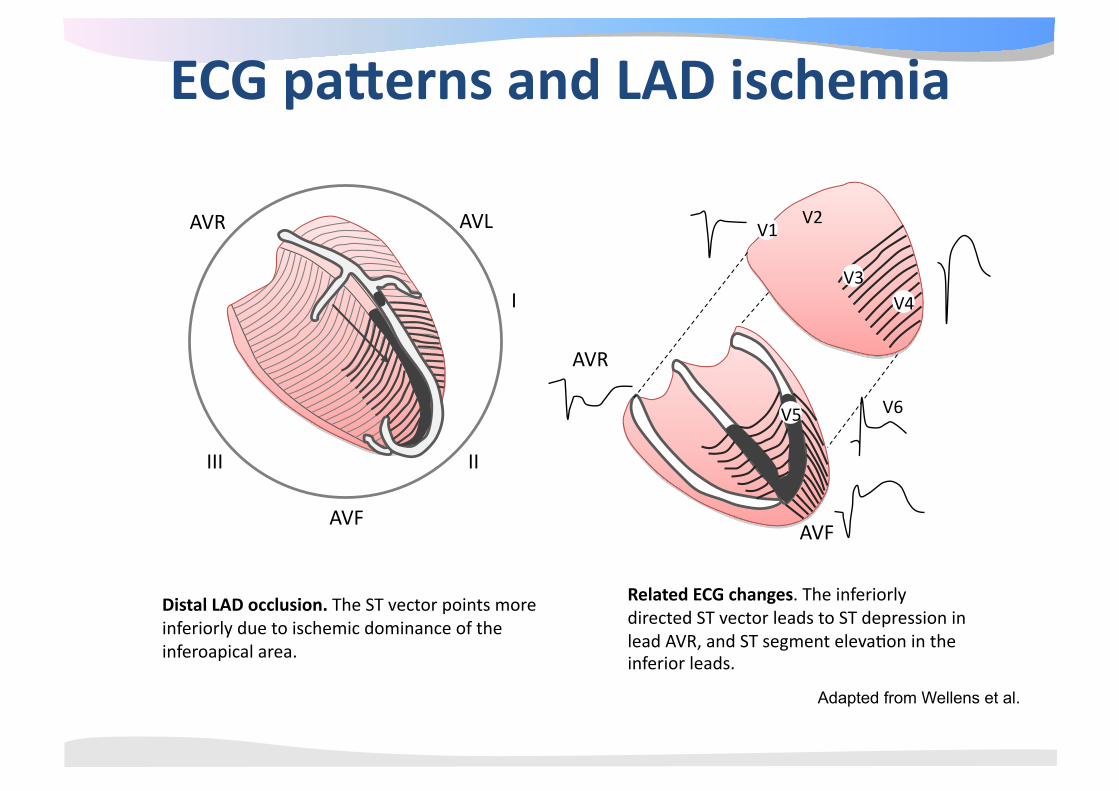
Related ECG changes. The inferiorly directed ST vector leads to ST depression in lead AVR, and ST segment eleva@on in the inferior leads.
AVR AVL
I
II
AVF
III
V1
V3 V4
V2
V5
AVF
AVR
V6
ECG panerns and LAD ischemia
Distal LAD occlusion. The ST vector points more inferiorly due to ischemic dominance of the inferoapical area.
Adapted from Wellens et al.
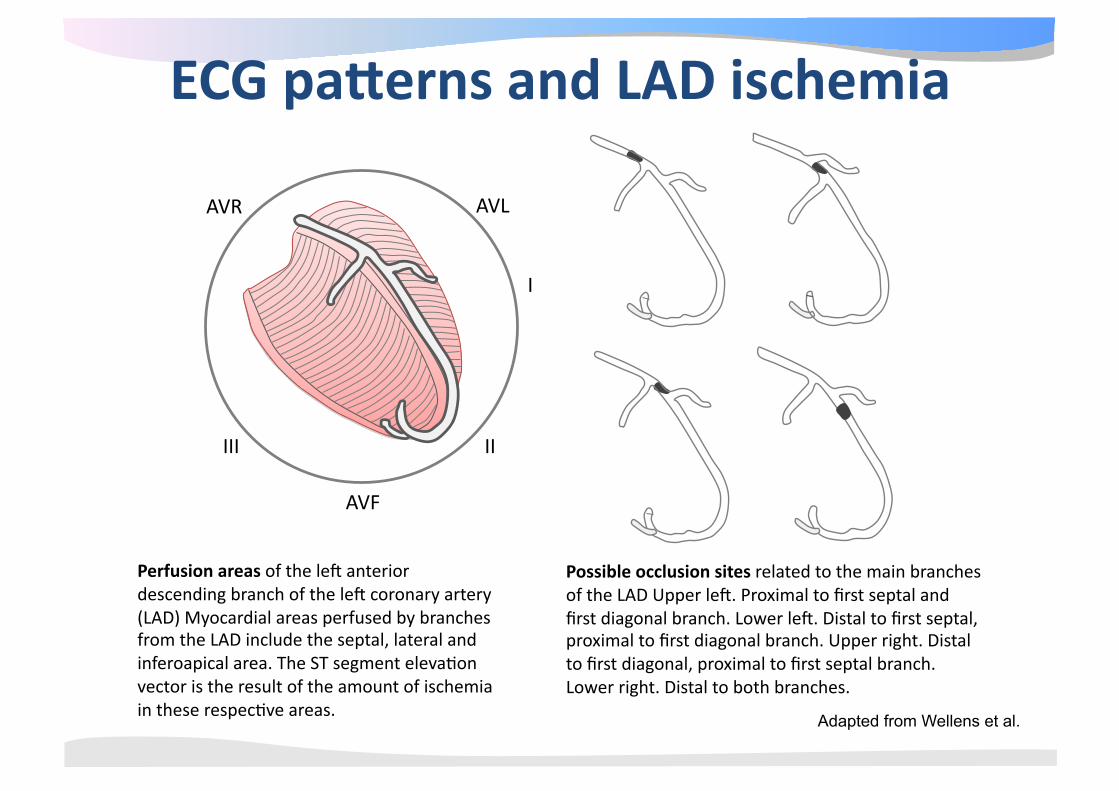
Possible occlusion sites related to the main branches of the LAD Upper lek. Proximal to first septal and first diagonal branch. Lower lek. Distal to first septal, proximal to first diagonal branch. Upper right. Distal to first diagonal, proximal to first septal branch. Lower right. Distal to both branches.
AVR AVL
I
II
AVF
III
ECG panerns and LAD ischemia
Perfusion areas of the lek anterior descending branch of the lek coronary artery (LAD) Myocardial areas perfused by branches from the LAD include the septal, lateral and inferoapical area. The ST segment eleva@on vector is the result of the amount of ischemia in these respec@ve areas. Adapted from Wellens et al.
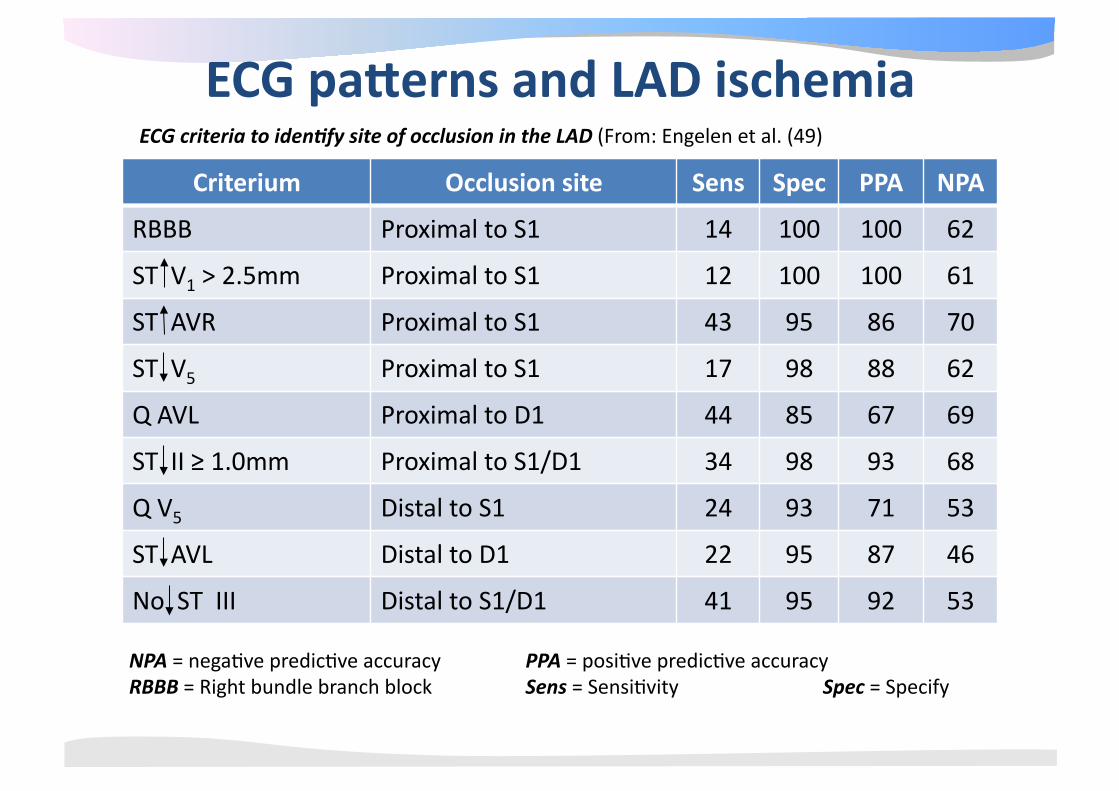
Criterium Occlusion site Sens Spec PPA NPA
RBBB Proximal to S1 14 100 100 62
ST V1 > 2.5mm Proximal to S1 12 100 100 61
ST AVR Proximal to S1 43 95 86 70
ST V5 Proximal to S1 17 98 88 62
Q AVL Proximal to D1 44 85 67 69
ST II ≥ 1.0mm Proximal to S1/D1 34 98 93 68
Q V5 Distal to S1 24 93 71 53
ST AVL Distal to D1 22 95 87 46
No ST III Distal to S1/D1 41 95 92 53
NPA = nega@ve predic@ve accuracy PPA = posi@ve predic@ve accuracy RBBB = Right bundle branch block Sens = Sensi@vity Spec = Specify
ECG criteria to iden,fy site of occlusion in the LAD (From: Engelen et al. (49)
ECG panerns and LAD ischemia
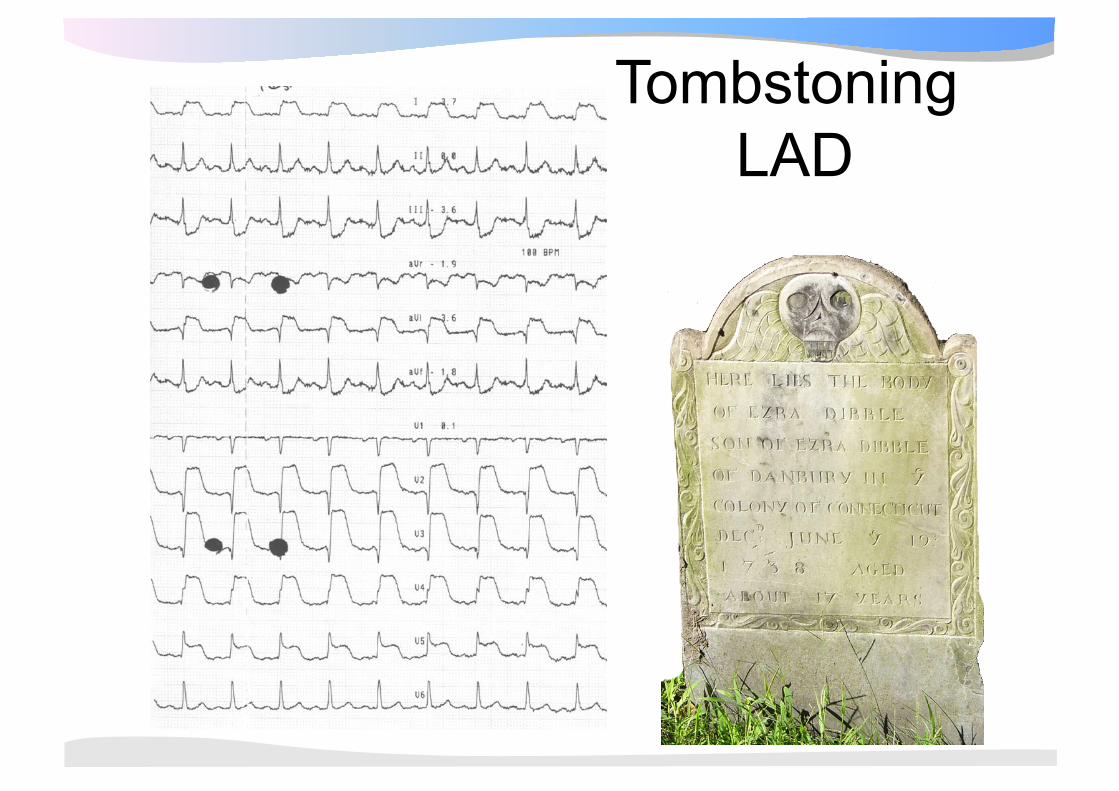
Tombstoning LAD
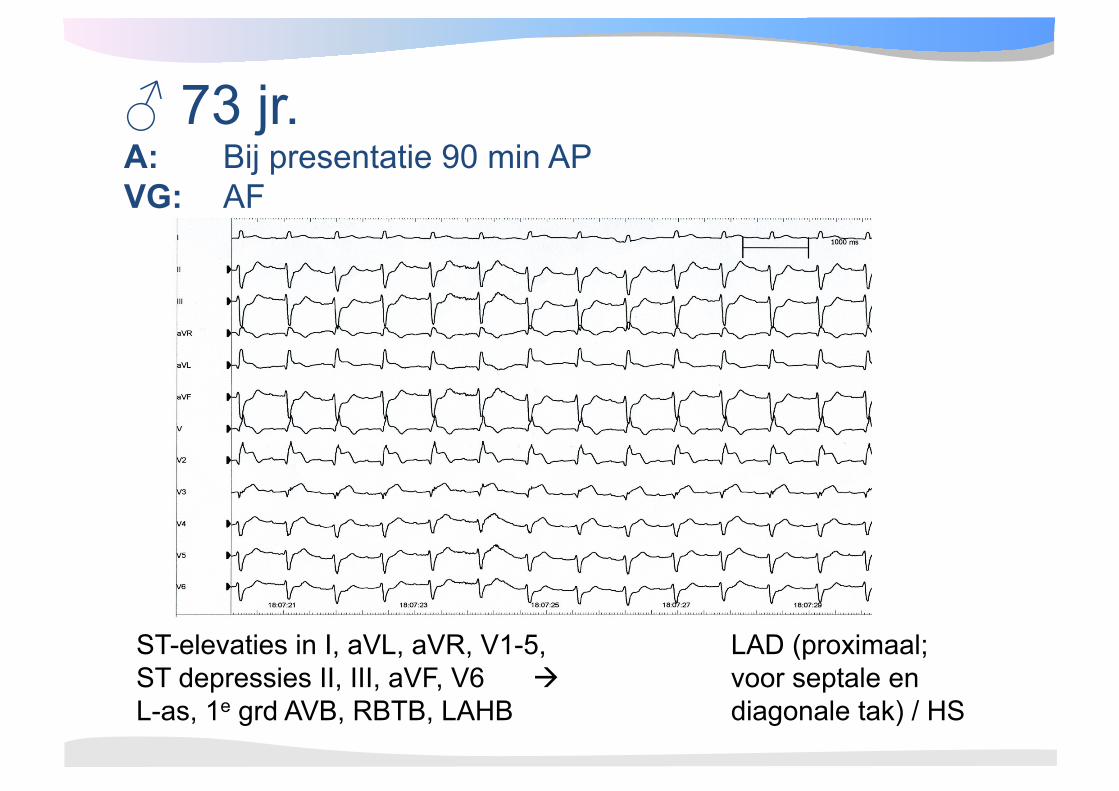
♂ 73 jr. A: Bij presentatie 90 min AP VG: AF
ST-elevaties in I, aVL, aVR, V1-5, LAD (proximaal; ST depressies II, III, aVF, V6 voor septale en L-as, 1e grd AVB, RBTB, LAHB diagonale tak) / HS

Bloedvoorziening geleidingssysteem
• SA knoop: RCA in 55% • AV knoop: RCA in 90% (RCX) • Bundel van His: RCA / LAD • Rechter bundeltak: LAD (S1) • Linkerbundeltak:
• An@cus: LAD • Pos@cus: LAD/ RCA
LAD
CX
RBB His
AF
PF
AV node
RCA
Geleidingsproblemen bij AMI • Sinus bradycardie/ ‐arrest ‐/ totaal AV Blok(RCA):
– Vagaal/ ischemisch/ neurolgisch (Bezold‐ Jarisch reflex), humoraal (pH, adenosine) atropine/ aminophylline
– 10‐20%, (meestal) smalcomplex escape ritmeHR: 40‐60/ min, voorbijgaand, wel mortaliteit↑ (2‐3x)
• Totaal AV blok (LCA): – Ischemisch (septale necrose) – 5%, breedcomplex escape ritmeHR: <40/ min, voorbijgaand, wel mortaliteit↑ (4x), pacemakerindica@e (primaire PCI)
– Bij proximale LAD: RBTB, LAHB, 1e grds AVB
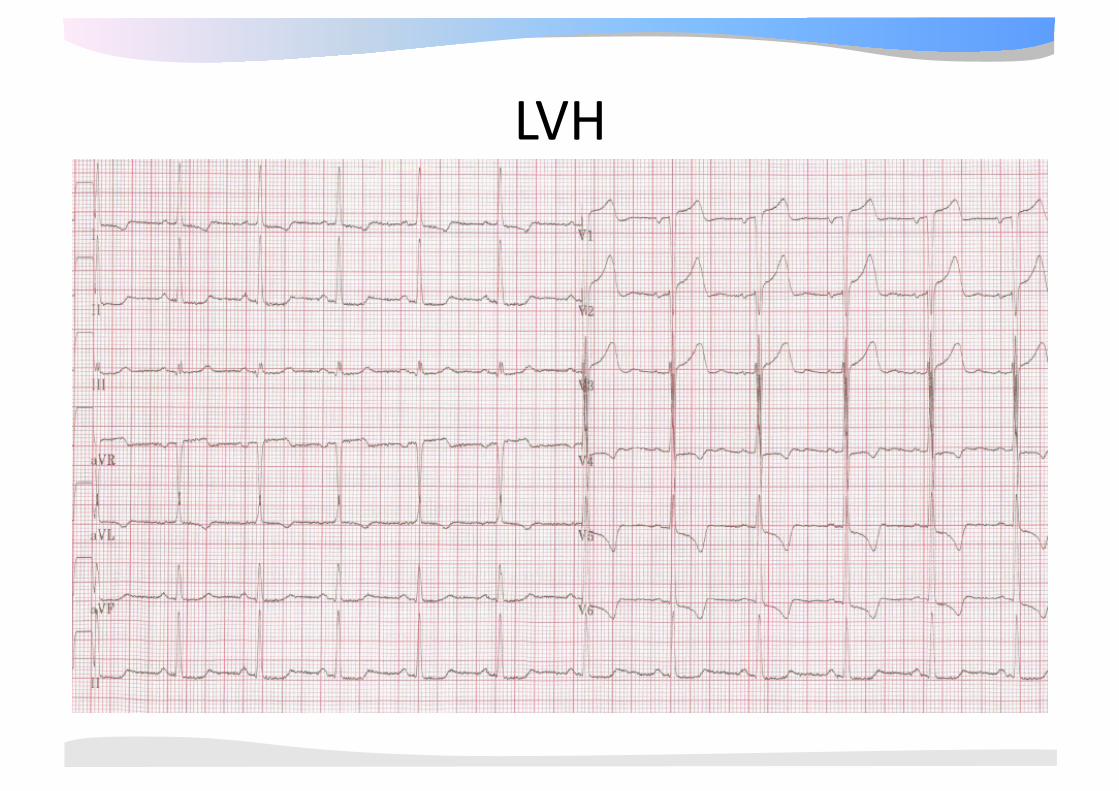
LVH
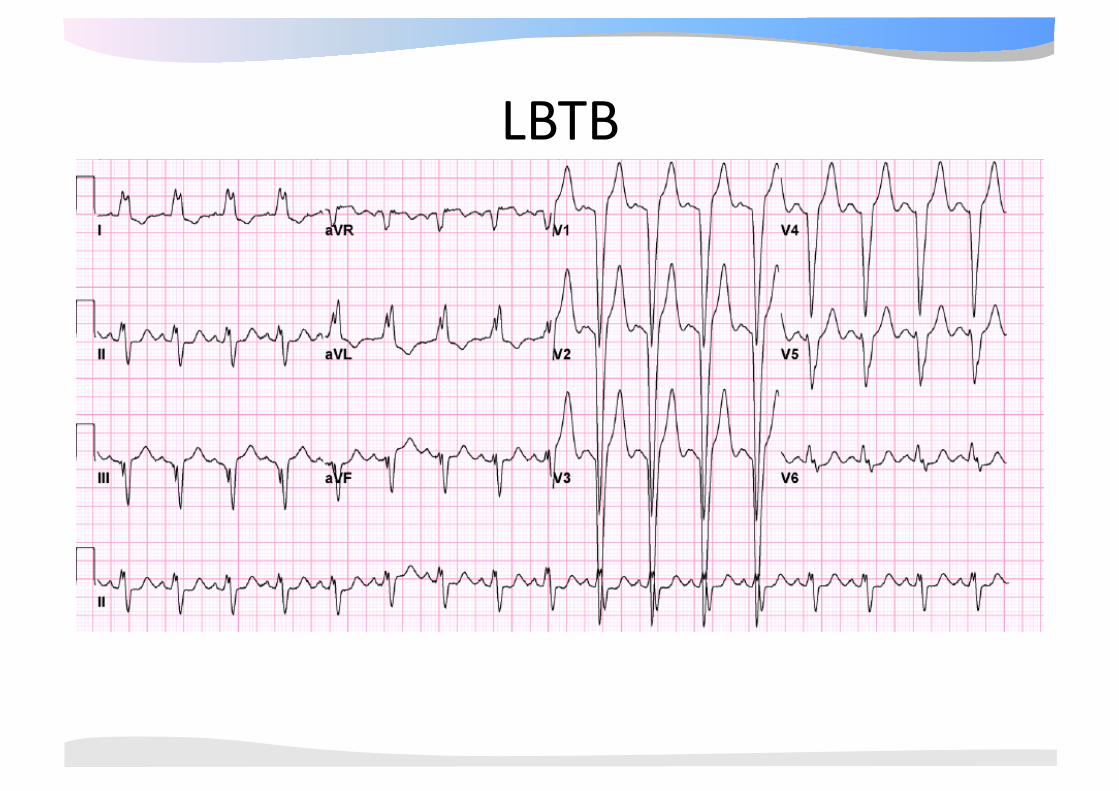
LBTB
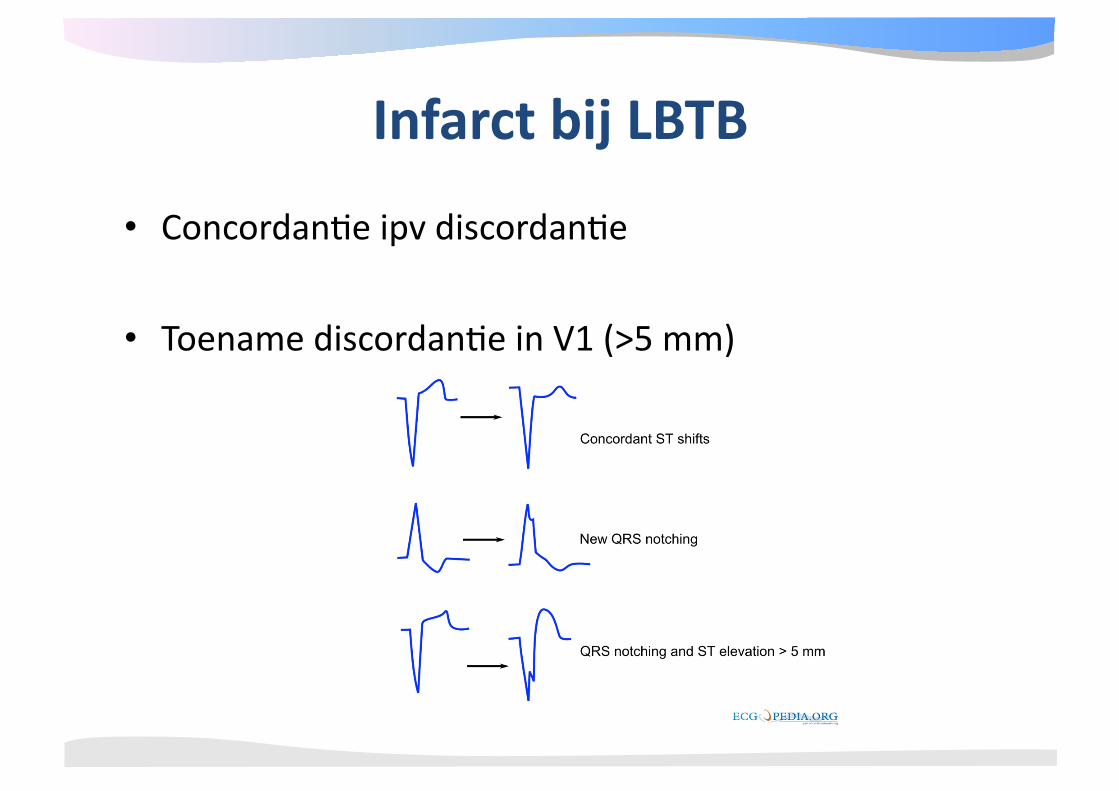
• Concordan@e ipv discordan@e
• Toename discordan@e in V1 (>5 mm)
Infarct bij LBTB
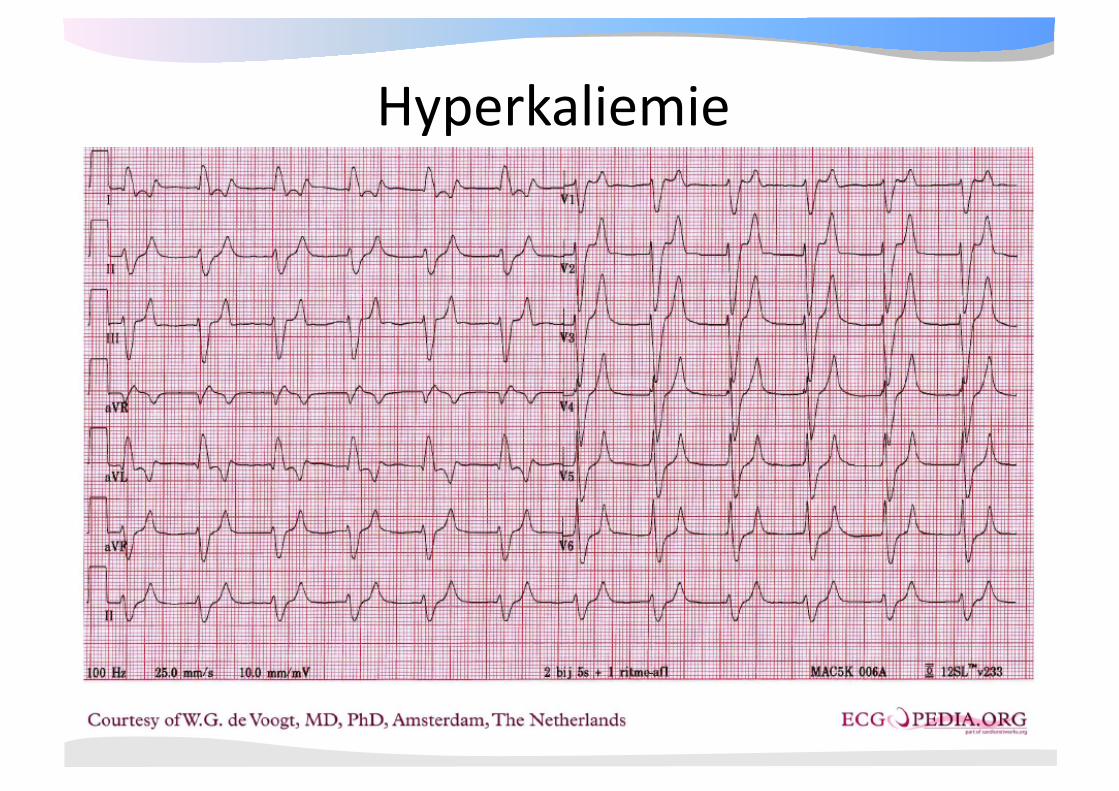
Hyperkaliemie
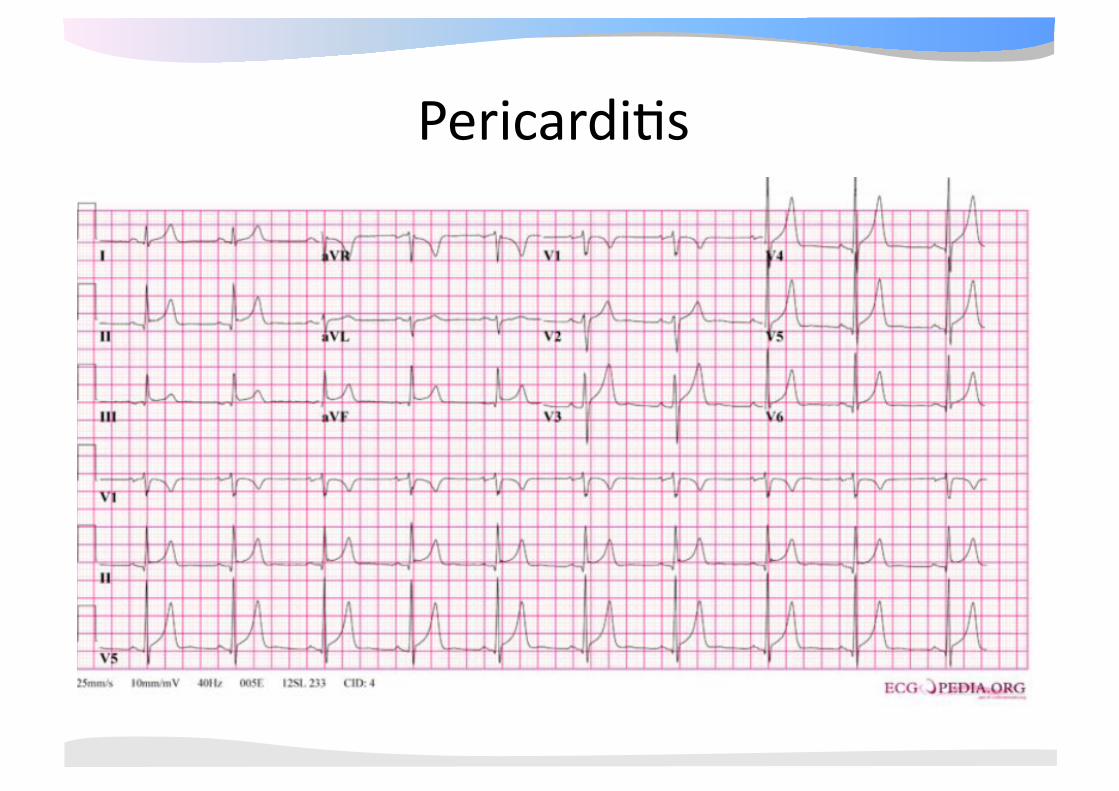
Pericardi@s





















![HD VIDEO CAMERA RECORDER GebruikershandleidingTijdzone/zomertijd instellen 1. Druk op de MENU-toets. 2. Draai het SELECT/SET-wiel naar [SYSTEM SETUP/ ] en druk op het wiel. 3. Selecteer](https://img.pdfslide.us/doc/110x75/6031454b3aefb73b224c6c3d/hd-video-camera-recorder-gebruikershandleiding-tijdzonezomertijd-instellen-1-druk.jpg)







