Embed Size (px)
Citation preview

ABRAMSON ET Ai 1163POST -TRANSFUSION PURPURAVol. 291 No. 22
sensitivity to antibiotics: studies on the accuracy of the technique.Scand J Clin Lab Invest 12:408-413.1960
5. Stamey TA: Urinary Infections. Baltimore. Williams and WilkinsCompany, 1972, pp 31-53
6. Ericsson H: Assay of antibiotics in small amounts of fluid. Scand JClin Lab Invest 12:423-432,1960
7. Regna PP, Solomons IA: The chemical and physical properties of ter-ramycin. Ann NY Acad Sci 53:229-237, 1950
8. Welch H: Absorption, excretion. and distribution of terramycin. AnnNY Acad Sci 53:253-265, 1950
9. Fairley KF, Bond AG, Adey FD: The site of infection in pregnancybacteriuria. Lancet 1:939-941,1966
10. Reeves DS, Brumfitt W: Localization of urinary tract infection: acomparative study of methods, Urinary Tract Infection. Edited by FO'Grady, W Brumfitt. London, Oxford University Press, 1968, pp53-67
II. Ronald AR, Cutler RE, Turck M: Effect of bacteriuria on renal con-centrating mechanisms. Ann Intern Med 70:723-733,1969
12. Eykyn S, Lloyd-Davies RW, Shuttleworth KED, et al: The localiza-tion of urinary tract infection by ureteric catheterization. Invest Urol9:271-275,1972
13. Nemoy NJ, Stamey TA: Surgical, bacteriological, and biochemicalmanagement of "infection stones." JAMA 215: 1470-1476, 1971
14. Meares EM, Stamey TA: Bacteriologic localization patterns in bac-terial prostatitis and urethritis. Invest UroI5:492-518, 1968
15. Lincoln K, Lidin-Janson G, Winberg J: Faecal and periurethral floraafter oral administration of sulphonamide, nitrofurantoin and nalidixicacid. Acta Paediatr Scand 61 :643-647, 1972
16. Daikos GK, Kontomichalou P, Bilalis D, et al: Intestinal flora ecologyafter oral use of antibiotics. Chemotherapy 13:146-160, 1968
17. Hinton NA: The effect of oral tetracycline HCI and doxycycline onthe intestinal flora. Curr Ther Res 12:341-352, 1970
18. Datta N, Faiers MC, Reeves DS, et al: R factors in Escherichia coli infaeces after oral chemotherapy in general practice. Lancet 1:312-315,1971
19. Winberg J, Bergstrom T, Lincoln K, et al: Treatment trials in urinarytract infection (UTI) with special reference to the effect of an-timicrobials on the fecal and periurethral flora. Clin Nephrol I:142-148,1973
resistance (R factors) to ampicillin, sulfonamides, strep-tomycin, and chloramphenicol,Is reinfection will often re-
quire multisensitivity testing to find an antimicrobial
agent that will cure the infection. The advantage of select-
ing drugs that do not change the fecal reservoir, as e)ll-phasized by Winberg, 19 is obvious.
In conclusion, the usefulness of oxytetracycline in uri-
nary-tract infections is directly related to whether or not
the infecting strain can be killed by the concentrations ob-
tained in the urine. Although this phenomenon is widely
appreciated for antimicrobial agents like the nitrofuran-
toins, whose serum levels during therapy are recognized
as being a fraction of what is required for antimicrobial ac-
tivity, it has not been appreciated that the same principle is
true of the so-called "broad-spectrum" antibiotics used at
the recommended oral dosage. We hope these data will
serve as additional impetus for the development and ap-
proval of sensitivity disks where the antimicrobiafcontent
of the disk reflects the urinary concentrations.:;
REFERENCES
I. Stamey TA, Govan DE, Palmer JM: The localization and treatment ofurinary tract infections: the role of bactericidal urine levels as op-posed to serum levels. Medicine (Baltimore) 44:1-36. 1%5
2. McCabe WR, Jackson GG: Treatment of pyelonephritis: bacterial,drug and host factors in success or failure among 252 patients. N EnglJ Med 272:1037-1044,1%5
3. Stamey TA, Timothy M, Millar M, et al: Recurrent urinary infectionsin adult women: the role of introital enterobacteria. Calif Med 115:1-19,1971
4. Ericsson H: The paper disk method for determination of bacterial
POST-TRANSFUSION PURPURA: IMMUNOLOGIC ASPECTS AND THERAPY
NEIL ABRAMSON, M.D., PETER D. EISENBERG, M.D., AND RICHARD H. ASTER, M.D.
an aggregometer, and by 51Cr release. Antibody activ-ity, as measured with the aggregometer, seemed re-stricted to the IgG3 class of immunoglobulin. Plasma-pheresis resulted in clinical improvement associatedwith disappearance of antibody activity. Thus, thispatient with post-transfusion purpura demon-strated anti-PIA1, and anti-HLA (lgG3) anti-platelet an-tibodies. Plasmapheresis with removal of the antibodyproved effective therapy. (N Engl J Med 291 :1163-1166,1974)
Abstract To determine the mechanisms of post-transfusion thrombocytopenia, platelet antibodieswere studied in a 45-year-old woman in whom severethrombocytopenia with lingual and buccal hemorrhag-ic bullae and purpura developed seven days after thetransfusion of whole blood. Her platelets were latertyped as PIA1 negative, and her plasma and serumcontained anti-PIA1 and anti-HLA antibodies. Anti-body activity was demonstrated by microscopicalagglutination and lysis, by aggregation with use of
own platelets were negative for the PIA 1 antigen, suggest-ing that the disorder results from an isoimmunization toincompatible transfused platelet antigen. Treatment forthis severe thrombocytopenic state has included exchangetransfusion, which, although seemingly successful, hasbeen associated with hazardous, antigen-antibody reac-tions in vivo.1.3 In the case of post-transfusion purpurapresented below, at least two antibodies reactive withplatelets were present, and antibody could be detectedwith the platelet aggregometer. Finally, plasmapheresisproved to be a safe and effective method of therapy.
P OST -TRANSFUSION purpura is an acute, severe,thrombocytopenic state that has been described in 15
patients. Thrombocytopenia occurs approximately oneweek after the administration of blood, 1.2 and, in each casestudied, the antibody present in the recipient plasma re-acted with the platelet antigen designated PIA 1. With theexception of a patient recently described,2 the recipients'
From the Division of Hematology and Medical Oncology Universtiy ofFlorida - Jacksonville Hospitals Educational Program. Jacksonville. FL.
and the Milwaukee Blood Center. Milwaukee. WI (address reprint requeststo Dr. Abramson at the Division of Hematology and Medical Oncology.University of Florida-Jacksonville Hospitals Educational Programs. 800Prudential Dr.. Jacksonville. FL 32207).
Supported by a Florida Heart Grant (73-AG-10) and by a grant from theNational Heart and Lung Institute HL-13629.
Presented at the annual meeting of the American Society of Hematology,necemner I 97J IRlood42: 1024. 1973).
CASE REPORT
A 45-year-old married woman was admitted to the hospitalwith a two-month history of heavy vaginal bleeding. The pastmedical historv included two uneventful childbirths in 1950 and

THE NEW ENGLAND JOURNAL OF MEDICINE Nov. 28. 19741164
1954, a dilatation and curettage in August, 1959, and a chole-cystectomy in May, 1970. A reactive Venereal Disease ResearchLaboratory test discovered previously had been appropriatelytreated. There was no history of transfusion, blood donation,bleeding problems or drug allergies. The family history revealedno blood dyscras!as. Physical examination showed an obesewoman in no distress, with a right-up per-quadrant subcostal scar,large uterus, rectocele and cystocele.
The admission laboratory data included a hemoglobin of 9.8 gper 100 mi.; hematocrit of 30 per cent, and hypochromic mi-crocytic red cells. The white-cell count was 10,700, with 74 percent neutrophils, 25 per cent lymphocytes and 1 per centeosinophils. Platelets were adequate on initial smears.
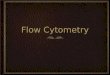
On the second hospital day, after receiving a unit of wholeblood, the patient underwent a cold-knife conization and diag-nostic dilatation and curettage. In preparation for an anteriorcolporrhaphy and vaginal hysterectomy on the fourth hospitalday, she received another 2 units of whole blood. The operationwas completed without complications, and the postoperativeperiod was uneventful until the ninth hospital day, when a fe\\."blood blisters" on the tongue and buccal mucosa were noted.Within 24 hours, bloody urine was observed flowing from theFoley catheter, and multiple petechiae and purpura appeared onall extremities, chest and abdomen. There was no lymphadenop-athy or hepatosplenomegaly. At that time the hemoglobin was10.9 g per 100 ml, the hematocrit 32 per cent, and, as shown inFigure I, the platelet count 12,000.3 Prothrombin time, thrombin
A diagnosis of post-transfusion purpura was made, and on the14th hospital day (13 days after the first unit of transfused bloodand five days after the onset of purpura), plasmapheresis wasbegun. Blood was removed one unit at a time into a standard acidcitrate dextrose plastic collection bag,* and centrifuged at 2100rpm at 4°C for 20 minutes. The plasma was expressed, and re-maining red cells were resuspended in saline a!:td retransfused.Intravascular volume was maintained by infusion of 5 per centdextrose in 0.5N saline. Twenty-five grams of albumin was trans-fused for every 2 units of plasma removed.
At the end of the first day of plasmapheresis, during which 7units (approximately 1550 ml) were removed, the platelet countwas 7000, and an occasional platelet was noted on the bloodsmear. The next morning the platelet count was 2000, and plas-mapheresis was reinstituted. Over the next two hospital days, 9and 6 units of plasma (approximately 2000 and 1350 ml) were re-moved respectively. The entire procedure was without com plica-tion except for transient hypotension during the removal of thelast unit of blood on the first day. As shown in Figure I, over thenext several days the platelet level rose to 17,000, 27,000, and156,000. The patient became asymptomatic, and the platelet levelhas remained normal during the ensuing 12 months.
METHODS
Platelet counts were done by phase microscopy. Platelet an-tibody was assessed in several ways. Agglutination and lysis werefirst observed after the addition of one part of normal platelet-rich plasma to four parts of test plasma (citrate or acid citrate dex-trose). This mixture was observed by light microscopy imme-diately and after a 30-minute incubation at 37°C. Agglutinationwas judged by clumping of platelets, and lysis by the appearanceof platelet stromal clumps. Also, aggregation was studied with aplatelet aggregometer (Chrono-Log) with use of modifiedtechnics previously reported.4 To one part of platelet-ri.ch plasmafrom a normal person one part of test plasma was added, and ob-servations were made for spontaneous aggregation. After at leastthree minutes of observation, ADP was added. When aggrega-tion took place during the primary incubation, ADP induced nofurther aggregation (ADP unresponsiveness). Serial dilutions ofthe test plasma were made; the antibody titers recorded are thehighest dilutions at which aggregation in the primary mixtureand ADP unresponsiveness were noted. The IgG subclass of theanti-platelet antibody was evaluated by the addition to the pa-tient's plasma of purified anti-IgG subclass antiserum (prepared,purified, absorbed, and judged for specificity as previously not-edS). To five parts of the patient's plasma or normal plasma, onepart of the purified anti-IgG subclass antiserum was added. Aftera two-hour incubation at 3rC the mixture was spun to removeany precipitate and supernatant added to an equal quantity ofplatelet-rich plasma from a normal person. Aggregation and,subsequently, ADP responsiveness were again judged with use ofthe aggregometer. Finally, s'Chromium release, using PIAI-positive and PIAl-negative platelets, was used for identificationand measurement of platelet antibody as previously described.6.7
Figure 1. Hospital Course of Patient.Ordinate to right refers to antibody levels expressed as apercentage of initial "A-HLA" and "A-PIA1" activity asmeasured by 51Cr release. "Ab (Aggr.)" refers to antibody ac-tivity measured by aggregometer. Each arrow under blooddenotes a transfusion, and the numbers under plas-
mapheresis indicate the units of plasma removed.
RESULTS
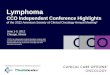
platelet aggregation and ADP responsiveness of normal(ABO-compatible) platelets incubated in the patient's orin normal plasma. The patient's plasma caused sponta-neous aggregation whereas, as expected, no aggregationoccurred with normal plasma and normal platelets untilADP was added. However, when ADP was added to thepatient's plasma and normal platelets after spontaneous
time. partial thromboplastin time. and whole-blood coagulationtime were all normal. A peripheral blood smear revealed an in-creased number of polychromatophilic cells (reticulocytes). nored-cell fragmentation and normal white cells. A sternal bone-marrow aspirate was cellular, with an increased number ofmegakar,ocytes and diminished iron stores.
On the II th hospital day a single-unit transfusion of freshwhole blood was begun. but shaking chills and fever (temperatureof 39°C) occurred promptly. The platelet count fell to 5000 on thenext hospital day. Another unit of whole blood was administeredwith similar results. and prednisone. by mouth 20 mg four times aday. was administered. By the 13th hospital day the platelet countwas 1200. .Cutter Laboratories, Berkeley, CA.

POST -TRANSFUSION PURPURA - ABRAMSON ET AL. 1165Vol. 291 No. 22
-TIME (minutes)
Figure 2. Diagram of Aggregation, as Measured in the Ag-gregometer, of Normal Platelets in Normal Plasma andNormal Platelets in Patient's Plasma (ADP [10-SM] Was
Added at the Points Noted).
aggregation, no further aggregation could be induced.The aggregating factor in the patient's plasma persistedafter heating at 56°C for 30 minutes.
Figure I shows the clinical course and the effect ofplasmapheresis on antibody levels. Antibody activity is ex-pressed as a percentage of initial activity with use of the ag-gregometer and 51Cr-release measurement methods. An-tiplatelet antibody activity decreased notably after the firstday's plasmapheresis, during which the platelet countrose; by the next morning the antibody activity rose againand the platelet count returned to approximately 1000.Anti-platelet antibody, as measured by the aggregometermethod, paralleled that of anti-PIA I measured by 51Cr re-lease with use of HLA-compatible PIA I-positive platelets.When antibody was evaluated by the 51Cr release technicwith use of PIAl-positive and PIAl-negative platelets, twoantibodies were noted to be present. The major one react-ed in high dilution wtih PIAl-positive but not with PIAI-negative platelets and therefore appeared to be a typicalanti-PIAl antibody. The second antibody reacted undilut-ed with platelets from PIAl-negative donors and with thelymphocytes of 22 of 25 donors in conventional Iym-phocytotoxicity assay, suggesting that a mixture of anti-HLA isoantibodies was present. Three weeks after thethrombocytopenia occurred, the patient's platelets weretyped as PIAl negative, and the pre-plasmapheresis plas-ma was found to have no antibody activity against her
platelets.Absorption experiments were performed with use of
purified anti-IgG subclass antiserums as shown in Table I.Anti-IgG1, IgG2, and IgG.. did not affect platelet antibodyactivity, \\'t!ereas anti-IgG3 removed it completely. At aI: 10 dilution of anti-IgG subclass antiserum, no effect wasobserved.
Soluble PIAl antigen was sought in the serum andplasma by inhibition of platelet lysis with use of an an-tibody of known anti-PIA 1 specificity. No evidence of solu-ble PIAl antigen was found in the serum of any of thedonors whose blood was transfused to this patient.6.7
DISCUSSION
The thrombocytopenia that occurred in this patientprovides et another exam Ie of" ost-transfusion ur-
ra." The patient's serum contained an anti-PIAl anti-body 1 Y2 weeks after initial transfusions, and the plateletswere later found to be PIAl negative. Like all but one ofthe previous patients,2 she was a woman who had previ-ously been pregnant. Upon transfusion after the onset ofsymptoms, the characteristic chill and fever of a platelet-antibody reaction developed. The antibody was a heat-stable IgG Klobulin with s . .cit directed a ainst PIAl.
In a ltlon, a second antibody was present in this case,which reacted with platelets and lymphocytes from anumber of donors, suggesting that it had HLA activity; itis likely that this antibody (or antibodies) was unrelated tothe thrombocytopenia, since it persisted after clinical re-
mission.Antibody activity was demonstrated by aggregation of
platelets. The aggregometer provided a convenient andrapid means of determining antibody activity. Our datasuggest that the technic can also be used to identify theIgG subclass of the antibody causing platelet aggregation.It is of interest that other workers have suggested thatplatelet autoantibodies of idiopathic thrombocytopenicpur ura are also of the I G3 subclass.8
In al the previous cases 0 post-trans USlon purpu-ra, with one exception, the patients' platelets have beennegative for the PIAl antigen. PIAl antigen is absent inonly 2 per cent of the general population. Since antibody'is formed in PIAl-negative persons when PIAl-positive I
platelets are infused, one would expect this disease to oc-cur more frequently than reports indicate. A unique fea-ture of this disorder is the destruction of recipient plate-lets, which are PIA 1 negative and pr abl do n t reactdirectl with anti-PIAl isoantibod It has been hypoth-esized that destruction of autologous platelets is related toquantity of PIA 1 antigen eluting from donor platelets or toantigen-antibody complexes absorbing to recipientplatelets. Serum of donors whose blood was transfused toour patient was tested for soluble PIAl antigen, but nonewas detected by the method used.
In previous reports of post-transfusion purpura, se-vere, life-threatening thrombocytopenia has lasted for aslong as five weeks and has not been affected by treatmentwith corticosteroids. Remission has been induced in atleast two cases by exchange transfusion with wholebloodl.3; however, these were attended by severe chill-fever reactions and, in one case, severe hypotension. Withplasmapheresis, of course, in vivo antigen-antibody reac-tions are avoided. As shown in Figure 1, after the firstday's plasmapheresis, antibody activity was definitely de-creased; however, by the next morning, levels increased.In this connection, it is of interest that platelets werevisible on the peripheral smear after the first day's
Table 1. Antibody Activity after Addition of Anti-lgG Sub-classes or Sal ine.*

1166 THE NEW ENGLAND JOURNAL OF MEDICINE Nov. 28, 1974
plasmapheresis, but disappeared by the next morning.Since the anti-platelet antibody was of the IgG class, pre-sumably only 50 per cent was present in the intravascularcompartment. It is likely, therefore, that the increase inplasma antibody that appeared overnight was related to acompartmental shift. Also, synthesis may have occurred.It can be noted that the antibody activity decreased to aneven greater degree over the next several days and, at thesame time, the platelets rose to normal levels. Althoughclinical improvement might have occurred after only twodays of plasmapheresis, a third day of this therapy was un-dertaken as a precaution, in view of the safety of the pro-cedure. This method of therapy appears to be effectiveand safe and circumvents the potential hazards of ex-change transfusion.
REFERENCES
I. Shulman NR, Aster RH, Leitner A, et al: Immunoreactions involvingplatelets. V. Post-transfusion purpura due to a complement-fixing an-tibody against a genetically controlled platelet antigen: a proposedmechanism for thrombocytopenia and its relevance in "autoimmuni-ty."]ClinInvest40:1597-1620, 1961
2. Zeigler ZR, Murphy S, Gardner FH: Post-transfusion purpura: reportof three cases emphasizing the heterogeneity of the syndrome and thesuperiority of 5'Cr release for detecting isoantibody. Blood 42:1023.1973
3. Cimo PL, Aster RH: Post-transfusion purpura: successful treatment byexchange transfusion, N Engl] Med 287:290-292, 1972
4, Deykin D, Hellerstein U: The assessment of drug-dependent andisoimmune antiplatelet antibodies by the use of platelet aggregometry. ]ClinInvest51:3142-3153,1972
5. Abramson N, Schur PH: The IgG subclasses of red cell antibodies andrelationship to monocyte binding. Blood 40:500-508, 1972
6, Aster RH, Enright SE: A platelet and granulocyte membrane defect inparoxysmal nocturnal hemoglobinuria: usefulness for the detection ofplatelet antibodies.] Clin Invest 48: 1199-1210, 1969
7. Aster RH, Miskovich BH, Rodey GE: Histocompatibility antigens ofhuman plasma: localization to the HLD-3 lipoprotein fraction.Transplantation 16:205-210, 1973
8. Karpatkin S, Schur PH, Strick N, et al: Heavy chain subclass of humananti-platelet antibodies. Clin Immunol ImmunopathoI2:1-8, 1973
We are indebted to Drs.J. Allgood and C. Guy for permissionto study the patient, to Dr. Scott Swisher for editorial comments,and to Mrs. J. DeLuca for technical assistance.
SPECIAL ARTICLE
ADVOCACY AND COMPLIANCE IN
Behavior of Physicians and Clients in a "
Tay-Sachs
ELLEN BECK, B.Sc., SHIRLEY BLAICHMAN, B.~AND CAROL
---,.:: SCREENING
Program of Testing for the
R. SCRIVER, M.D., F.R.S.C,CLaW
Abstract The relation between advocacy and com- pliant subjects.The physician is the most powerful potential ad-
vocate of testing, for the Tay-Sachs gene, but heperforms poorly in this role. Compliance rates can beimproved in the program when its advocates are wellinformed and motivated. Our findings indicate a needfor improved perception of the personal relevanceof heredity, not only among clients of genetic screen-ing programs but also among the personnel who func-tion as advocates. (N Engl J Med 291 :1166-1170,1974)
, ... - '--. '--""-,- -~ --!identify carriers of the Tay-Sachs gene among
~ o,o eligible subjects- The overall compliance rate was .8
per cent, and among subgroups of clients it was 7.6
per cent in final-year high-school students, 20 p cent
- . .--per cent in "random" eligible adults.knowledge and lack of motivation, ,exposure to the screening option, "the nonparticipant group by , with com-
persons withpracticed as a
- ---' of genetic~: :, so that
avert harm. Alter-
V OLUNTARY mass screening tospecific mutant genes is now "
technic of disease prevention.'.-screening is to find subjects withprompt medical interventionnatively, 0
offspring
Biochemical Genetics, McGillFrom the deBelle LaboratoryUniversity - --- --- - ' -.. , . -,-per St., Montreal, PQ, Canada H IP3, where reprint requests should beaddressed to Dr. Scriver.
Presented in part at the ann I meeting of the Ambulatory Pediatric As-sociation, Washington, DC, ay29,1974.
Supported by a private dation from Charles and Edward Bronfman, byresearch grants from the ebec Network of Genetic Medicine (Ministry ofSocial Affairs) and the edical Research Council of Canada, and by sum-mer-student bursaries from the Faculty of Medicine, McGill University, toMiss Beck and Miss Blaichman when they were second-year students inmedicine.
under certain conditions, and who could benefit fromgenetic counseling.
Rosenstock3 observes that people use health services ac-cording to their perception of health. In the absence ofsymptoms, a client's decision to comply with a screeningtest will be influenced by a number of factors including themotivation, his or her perception of the susceptibility to,and seriousness of, the inherited condition, of the possibleconsequence of noncompliance, and the potential bene-fits from participation. It is already known that geneticscreening of newborn populations for purposes ofmedical intervention, meets with high approval and com-pliance.4.s However, in this case the clients are a captivepopulation, and the advocate is often the state, on behalfof the parents; under these conditions, high compliancerates are not surprising.
In this paper we examine attitudes toward screenin~ for