Embed Size (px)
Citation preview

Abstract
Preemptive Liver Transplant To Prevent Cardiovascular Complications Of Homozygous
Familial HypercholesterolemiaArpan R. Doshi, M.D., PGY5, Duraisamy Balaguru, M.D.
Division of Pediatric Cardiology, University of Texas Medical School at Houston
IntroductionHomozygous familial hypercholesterolemia is a rare disorder of LDL receptor deficiency. It is strongly associated with premature atherosclerosis and premature death due to cardiovascular complications. Multiple therapies including lipid lowering medications, lipid apheresis and liver transplant have been used for management1. Frequently, liver transplantation is reserved for individuals who have developed advanced cardiovascular complications2. At that stage, these individuals need additional cardiac surgery or cardiac transplantation along with the liver transplantation2. Therefore, it is argued that liver transplantation should be performed before cardiovascular complications develop into significant disease3. We report 2 siblings with Homozygous FH Type 2a. Patients had severe extracardiac complications of FH and started to have subclinical cardiac complications. They received orthotropic liver transplant with normalization of lipid profile.
Figure 1: Multiple cutaneous xanthomas prior to liver transplant in case 1.
Case Report
ConclusionsWe report two cases of young siblings with familial hypercholesterolemia. They received preemptive orthotropic liver transplant prior to development of advanced coronary artery changes with normalization of the cholesterol level and gradual resolution of other manifestations of familial hypercholesterolemia.
References
2013 Texas Pediatric Society Electronic Poster Contest
Case 1: A 6-year-old girl from Saudi Arabia with diagnosis of homozygous FH type 2a presented for outpatient cardiac evaluation. She developed cutaneous xanthomas (Figure 1) during infancy. She was diagnosed with FH type 2a during further evaluation. Laboratory findings revealed total cholesterol level as high as 2316 mg/dl and LDL level of 733 mg/dl over past 6 years. She was treated with multiple lipid lowering agents (including statins and Ezetemibe) with no success. In addition to cutaneous xanthomas she also developed bilateral knee arthritis. Family history was significant for both parents with consanguinity and diagnosis of FH. She weighed 27 kg (92nd percentile) with BMI of 22.3 kg/m2 (>97th percentile) during her visit. Exam was significant for multiple cutaneous xanthomas over the body, 3/6 medium-frequency systolic ejection murmur at left upper and right upper sternal border radiating to both carotids and minimal hepatomegaly. The echocardiogram revealed mild flow acceleration at aortic valve with normal thickness and milt aortic regurgitation. Carotid artery duplex imaging did reveal early plaque formation with CIMT exceeding upper limit of normal for a 14 yrs old. Cardiac catheterization revealed normal coronary arteries. She underwent orthotropic liver transplant at 7 years of age with no complications. Follow up cholesterol level 1 week after the transplant was down to 222 mg/dl. Case 2: A 4-year-old girl from Saudi Arabia with diagnosis of homozygous FH type 2a presented for outpatient cardiac evaluation. She also developed cutaneous xanthomas during infancy like her sister described in case 1. She was also diagnosed with FH type 2a during further evaluation. Laboratory findings revealed total cholesterol as high as 887 mg/dl and LDL level of 772 mg/dl over past 6 years. She was treated with multiple lipid lowering agents with no success. She weighed 14.7 kg (10th percentile) with BMI of 15.1 kg/m2 (50th percentile). Exam was significant for multiple cutaneous xanthomas, normal cardiac exam and no hepatomegaly. The echocardiogram revealed mildly thickened aortic cusps with mild aortic regurgitation. Carotid artery duplex showed bilaterally increased common carotid intimal-medial thickness (Figure 2). Cardiac catheterization revealed mild irregularity of left main coronary artery (Figure 3). She underwent orthotropic liver transplant at 5 years of age with no complications. Follow up carotid artery duplex ultrasound 1 month after transplant was normal. Her total serum cholesterol level 2 months after the orthotropic liver transplant was down to 157 mg/dl.
We report two young siblings from Saudi Arabia with homozygous familial hypercholesterolemia (FH) type 2a. They developed extracardiac manifestations of FH including cutaneous xanthoma, arthralgia, joint swelling and significantly elevated cholesterol level (highest total cholesterol of 2316 and 882 mg/dl and highest LDL level of 733 and 772 mg/dl for both patients, respectively). Cardiovascular manifestations included thickened aortic valve leaflets, mild aortic regurgitation and increased carotid artery intimal thickness. One of the patient had mild left main coronary artery irregularity. Both patients received orthotropic liver transplant with normalization of cholesterol levels and normalization of carotid artery intimal thickness on duplex ultrasound imaging.
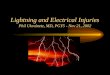
Figure 2: Carotid duplex imaging of patient 2 showing early plaque (arrow) in the right common carotid artery.
Figure 3: Coronary artery angiogram of patient 2 showing irregularity (arrow) of left main coronary artery without stenosis.
1. Maiorana A et.al. Preemptive liver transplantation in a child with familial hypercholesterolemia. Pediatr Transplant. 2011 Mar;15(2):E25-9.2. Offstad J et.al. Plasma exchange and heart-liver transplantation in a patient with homozygous familial hypercholesterolemia. Clin Transplant. 2001 Dec;15(6):432-6.3. Sokal EM et. al. Liver transplantation for familial hypercholesterolemia before the onset of cardiovascular complications. Transplantation. 1993 Feb;55(2):432-3.4. Naoumova RP et. al. Current management of severe homozygous hypercholesterolaemias. Curr Opin Lipidol. 2004 Aug;15(4):413-22.
Early Plaque inCommon Carotid Artery
DiscussionFamilial hypercholesterolemia is a disorder of cholesterol metabolism characterized by deficiency of LDL receptors4. Homozygous form of FH is very rare with incidence of 1 in a million. Patients with homozygous form of the disease have aggressive disease presentation with cardiac and extracardiac manifestations like cutaneous xanthoma, arcus cornealis, arthralgia, cardiac valve thickening with development of aortic stenosis and progressive atherosclerosis1. Medical therapy with lipid lowering agents is minimally effective with no significant effects on systemic manifestations of the disease. Lipid apheresis helps with short term lowering of cholesterol levels but does not prevent long-term complications. Liver transplant is a proven therapy for homozygous FH2. Patients who have developed advanced coronary artery disease require coronary bypass surgery with liver transplant, or combined heart and liver transplant. Hence preemptive liver transplant before the development of advanced atherosclerotic changes provide definitive therapy and the best opportunity to prevent significant coronary disease.