Embed Size (px)
Citation preview

EXPERIMENTAL AND MOLECULAR PATHOLOGY 43, 13-21 (1985)
Abnormal Cilia in the Small Airways of Mice Induced by Bleomycin
TOSHIO SATO,KIMIHIKOTAKUSAGAWA, NOBORU Asoo, AND KIYOSHI KONNO
Depurtment of Internal Medicine, the Research Institute for Tuberculosis und Cancer. Tohoku University, Sendai, Japun
Received May 23, 1984, and in relised form January 2. 1985
The frequency and types of abnormal cilia in the small airways before and after parenteral administration of bleomycin were examined by transmission electron microscopy. Bleo- mycin was injected subcutaneously at a dose of 40 mgikg twice weekly for 6 weeks. Bron- chioles less than 0.1 mm in diameter from animals sacrificed I day after a single dose, I day after three doses, 3 days after 8 doses, and 13 days after 12 doses were selected for evaluation. Although ciliated cells proper did not show pronounced alterations, abnormal cilia such as swollen cilia, compound cilia, and cilia with abnormal axonemes frequently occurred. Repeated injections did not necessarily induce much more abnormal cilia than one dose. The results suggested that ciliated cells remain undamaged and that normal cilia can be restored. The specific type of abnormal cilia induced by bleomycin was not identi- fied. 0 1985 Academic Press. Inc.
INTRODUCTION
Bleomycin is an excellent anticancer drug and does not have hemopoietic tox- icity or immunosuppressive activity (Blum et al., 1973). However, it produces interstitial pneumonitis and subsequent pulmonary fibrosis as a potentially fatal side effect (Luna et al., 1972), a phenomenon which has been extensively de- scribed in animals as well as in humans (Luna et al., 1972; Bedrossian et al., 1977; Jones and Reeve, 1978). Although many authors have described the changes of blood vessels and alveolar epithelial cells in alveolar areas, little attention has been paid to changes of the epithelial cells in the respiratory tracts (Collins et al., 1982), despite the fact that abnormal cilia have been observed in a variety of animal species and in humans under various conditions (Harris et al., 1974; Lun- garella et al., 1980; Afzelius, 1979) and despite the interest of many investigators in pathological changes of the cilia.
Abnormalities of cilia in small airways were first noted in the course of an ultrastructural observation of bleomycin-induced fibrosis in mice, and thus we examined the frequency and types of abnormal cilia in relation to doses of bleo- mycin by transmission electron microscopy in this study.
MATERIALS AND METHODS
Twenty-week-old male ddY mice weighing 35-45 g were used. Bleomycin (Nippon Kayaku, Co. Ltd., Tokyo) was dissolved in sterile saline and injected subcutaneously into the dorsum of mice at a dose of 40 mg/kg twice weekly for 6 weeks. Control animals (n = 7) received saline subcutaneously. These mice were sacrificed 1 day after a single dose (Bl group, n = 5), 1 day after three doses (B3 group, n = 3), 3 days after 8 doses (B8 group, II = 3), and 13 days after 12 doses (B12 group, n = 3). Small pieces of lung randomly selected were fixed in 2.5% Millonig-buffered glutaraldehyde (pH 7.4) for 2 hr, postfixed in 1% Millonig-buffered 0~0, (pH 7.4) for 2 hr and then dehydrated in an ethanol series,
13
0014-4800185 $3.00 Copyright 0 1985 by Academic Press. Inc. All rights of reproduction in any form reserved.

14 SAT0 ET AL.
FIG. 1. Cross section of two cilia from bronchiole. Left cilium shows the normal configuration of nine peripheral microtubular doublets and two central microtubules. Nexin links, radial spokes, and a central sheath are recognized. Dynein arms are attached to each outer doublet. Right cilium lacks one outer doublet. x 143,500.
and finally embedded in Epon 812. Semithin sections of the pieces were stained with toluidine blue, and bronchioles less than 0.1 mm in diameter from more than four blocks per animal were selected for ultrathin sectioning. The ultrathin sec- tions were stained with uranyl acetate and lead citrate and examined with a Hitachi H-600 electron microscope operated at 75 kV.
TABLE I Abnormal Cilia in Bronchiolar Epithelium
Treatment
Control
Bleomycin 1 treatment
3 treatments
8 treatments
12 treatments
Number of animals
7
5
3
3
3
Abnormal Swollen Compound axonemes cilia cilia
411721” 4513398 013398 (5.5) (1.3) (0)
85/468* 224/3672* 1713672* (18.1) (6.1) (0.46) 901489* 151/4077* 1714077* (18.4) (3.7) (0.41)
144/490** 182/3074* 16/3074* (29.4) (5.9) (0.52)
120/457*** 139/3681* 6613681t (26.2) (3.7) (1.79)
’ Number of abnormal cilia/total number of cilia counted. Number in parentheses represents per- centage.
* Significantly different from control group, P < 0.001. ** Significantly different from Bl and B3 groups, P < 0.0001.
*** Significantly different from Bl and B3 groups, P < 0.0005. t Significantly different from Bl, B3, and B8 groups, P < 0.0001.

BLEOMYCIN-INDUCED ABNORMAL CILIA I5
Quantitative morphologic studies on the cilia present in bronchiolar epithelial cells were performed. Cilia sectioned transversely were photographed at random at an original magnification of 20,000, and the electron micrographs were enlarged in prints to a final magnification of 50,000. Cilia in which a microtubular pattern was clearly recognized were counted for abnormal number and disarrangement of an axial filament complex in the middle portion of the cilium. Oblique and longitudinal sections of cilia as well as cross sections were also counted for swollen cilia and compound cilia.
To assess the orientation of cilia, many lines were drawn, each of which passed through the two central microtubules of a cilium on the photograph. Then an arbitrary line was drawn with an orientation similar to that of the majority of the lines on the same photograph. The angle that each line made with this arbitrary line was estimated. Angles greater than 90” were subtracted from 180”.
RESULTS
Normal cilia in cross sections were observed to have an arrangement of 9 + 2 axoneme with dynein arms, radial spokes, nexin links, and a central sheath (Fig. 1). Although bleomycin caused frequent and various changes in the cilia, loss of cilia and destruction of ciliated cells were rarely observed in any of the treatment groups. The results are summarized in Table I. Swollen cilia with an excess of cytoplasmic matrix occurred in 1.3% of total cilia counted in the control
FIG. 2. Some cilia lack a few outer doublets, or show complete disarrangement of microtubules. Swollen cilia with much excess matrix have only a few microtubules. x 43,300.
16 SAT0 ET AL.
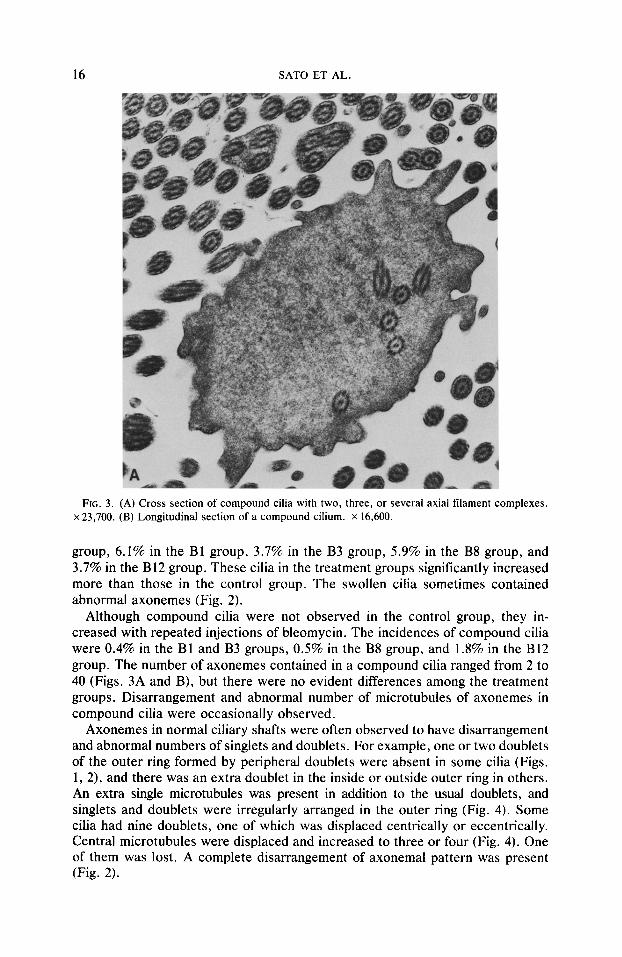
FIG. 3. (A) Cross section of compound cilia with two, three, or several axial filament complexes. x 23,700. (B) Longitudinal section of a compound cilium. X 16,600.
group, 6.1% in the Bl group, 3.7% in the B3 group, 5.9% in the B8 group, and 3.7% in the B12 group. These cilia in the treatment groups significantly increased more than those in the control group. The swollen cilia sometimes contained abnormal axonemes (Fig. 2).
Although compound cilia were not observed in the control group, they in- creased with repeated injections of bleomycin. The incidences of compound cilia were 0.4% in the Bl and B3 groups, 0.5% in the B8 group, and 1.8% in the B12 group. The number of axonemes contained in a compound cilia ranged from 2 to 40 (Figs. 3A and B), but there were no evident differences among the treatment groups. Disarrangement and abnormal number of microtubules of axonemes in compound cilia were occasionally observed.
Axonemes in normal ciliary shafts were often observed to have disarrangement and abnormal numbers of singlets and doublets. For example, one or two doublets of the outer ring formed by peripheral doublets were absent in some cilia (Figs. 1, 2), and there was an extra doublet in the inside or outside outer ring in others. An extra single microtubules was present in addition to the usual doublets, and singlets and doublets were irregularly arranged in the outer ring (Fig. 4). Some cilia had nine doublets, one of which was displaced centrically or eccentrically. Central microtubules were displaced and increased to three or four (Fig. 4). One of them was lost. A complete disarrangement of axonemal pattern was present (Fig. 2).

BLEOMYCIN-INDUCED ABNORMAL CILIA 17
FIG. 3-Continued.
The occurrence of abnormal axonemes was 5.5% in the control group and 18- 26% in the treatment groups. Abnormal axonemes in the B8 and B12 groups increased significantly more than those in the B 1 and B3 groups. Disarrangement of ciliary axonemes was most frequently observed in all groups classified as to abnormal axonemes as shown in Table II. The incidence of cilia with abnormal numbers of doublets was second to the former. However, the percentages of various types of abnormal axonemes were not different between the control group and the treatment groups, and specific changes of cilia induced by bleomycin were not observed.
The orientation of cilia varied from 0” to 90”, and no difference in the distri- bution of orientation was recognized among all groups (Fig. 5).
DISCUSSION
Bleomycin caused an increase in the occurrence of abnormal cilia, such as swollen cilia, compound cilia, and cilia with abnormal numbers and disarrange- ment of axonemes. In spite of many reports of abnormal cilia, quantitative data on the incidence of such cilia before and after treatment of injurious agents in experimental animals have been very few (Ranga and Kleinerman, 1981). Afzelius (1981) regarded compound cilia, disorganized axonemes, internalized or shed cilia, and flaccid cilia as nonspecific lesions.
Abnormal cilia that were observed after exposure to tobacco smoke, some other irritants, and ionizing radiation mostly consisted of cilia with swollen shafts

18 SAT0 ET AL.
FIG. 4. Cross-sectioned cilia with three or four central microtubules are seen (right). Singlets and doublets are irregularly seen in the outer ring and are dislocated (left). x 93.800.
or compound cilia (Ranga and Kleinerman, 1981; Kennedy and Allen, 1976; Bal- detrop et al., 1977; Wakefield and Wate, 1980). Swollen cilia and compound cilia clearly increased in the treatment groups in our study. The results could be re- garded as indicating a pathological change caused by bleomycin. Although com- pound cilia resulted from local damage of cilia as frequently seen in chronic infection (Stake et al., 1981; Konradova et al., 1974; Cornille et al., 1980) and bronchial carcinoma (Harris et al., 1974; Ailsby and Ghadially, 1973; McDowell et al., 1976), the mechanism of formation of compound cilia is not evident. Ta- kasaka et al. (1980) classified compound cilia into two groups, namely, the adhesive type produced by fusion of ciliary membranes and the bulging type resulting from cytoplasmic protrusions.
It is known that 9 + 2 pattern of the axoneme is observed in various species and is genetically stable (Fawcett, 1961). Atypical cilia with abnormal axonemes were less than 0.1% in tracheal epithelia of normal guinea pigs (Dalen, 1981), 2% in tracheal epithelia of normal dogs (Wilsman, Farnum and Reed, 1982), and 2- 5% in nasal or bronchial and bronchiolar epithelia of normal humans (Fox and Bull, 1981; Wisseman et al., 1981). In the control group examined here, cilia with abnormal axonemes were 5.5%. Such a difference in incidence might be due to species and sampling differences. The pattern of abnormal axonemes found in this experiment was very similar to the ciliary abnormalities described in many other reports (Afzelius, 1979; Katz and Holsclaw, 1980; Wakefield and Wate,

BLEOMYCIN-INDUCED ABNORMAL CILIA 19
TABLE 11 Classification of Abnormal Axonemes
Treatment
Abnormal Abnormal Abnormal Abnormal arrange- axonemes in number of number of ment of swollen doublets” singlets doublets cilia Miscellaneous
Control
Bleomycin 1 treatment
3 treatments
8 treatments
12 treatments
1 ll4lb (26.8)
15185 (17.6) 14190 (15.5) 441144 (30.5) 341120 (28.3)
514 1 (12.2)
13185 27185 (15.3) (31.7)
8190 40190 (8.8) (44.4)
101144 551144 (6.9) (38.2) 41120 541120 (3.3) (45 .O)
17141 (41.4)
214 1 (4.9)
11185 (12.9)
9190 (10.0)
51144 (3.4)
151120 (12.5)
614 1 (14.8)
19185 (22.4) 19190 (21.1) 30044 (20.8) 13/120 (10.8)
a The number of doublets are 7. 8. 10. b Number of cilia with abnormal axonemes/total number of cilia with abnormal axonemes. Number
in parentheses represents percentage.
1980; Starke et al., 1981; McDowell et al., 1976; Takasaka et al., 1980; Fawcett, 1961; Konradova, 1973). The mechanism of occurrence of abnormal axonemes is not known.
Since the animals were not injected with bleomycin consecutively and were sacrificed at irregular intervals in the B8 and B12 groups, the extent of revers- ibility could not be precisely evaluated. However, there was no great increase in abnormal cilia in proportion to repeated doses of bleomycin. Moreover, bleo- mycin caused injury to cilia without destruction of the ciliated cell. This suggests that cilia regenerate continuously but that normal cilia are replaced with abnormal cilia. Ranga and Kleinerman (1981) also considered the regeneration of normal cilia from the surviving cell rather than the necessity of cell regeneration. Cilia might be the part of the cell structure most susceptible to injury.
The orientation of cilia was irregular and was not different between the control group and the treatment groups. This disorientation might be due to an artifact
- Control
ANGLES
FIG. 5. Angles of approximately 170 cilia in each group were measured. An angle greater than 90” was subtracted from 180”. Each point represents incidence of orientation of cilia in every range of 10” in each group.

20 SAT0 ET AL.
produced by differences in the rapidity of fixation of cells and cilia (Fox et al., 1980) or by postmortem changes due to anoxia and autolysis (Kollberg et al., 1978).
Although there is no report concerning the effect of anticancer drugs on cilia, bleomycin produces many abnormal cilia in small airways of mice. Other anti- cancer drugs may also induce abnormal cilia. It is possible that these changes impede mucociliary clearance and contribute to progressive pulmonary degen- eration (Cuts et al., 1978; Katz and Holsclaw, 1980).
REFERENCES AFZELIUS, B. A. (1979). The immotile-cilia syndrome and other ciliary diseases. Int. Ret?. Exp. P&o/.
19, l-43. AFZELIUS, B. A. (1981). “Immotile-cilia” syndrome and ciliary abnormalities induced by infection
and injury. Amer. Rev. Resp. Dis. 124, 107-109. AILSBY, R. L., and GHADIALLY, F. N. (1973). Atypical cilia in human bronchial mucosa. J. Puthol.
109, 7.5-78. BALDETROP, P. L., VAN MECKLENBERG, C., and HAKKANSON, C. H. (1977). Ultrastructural alterations
in ciliary cells exposed to ionizing radiation. A scanning and transmission electron microscopic study. Cell Tissue Res. 180, 421-431.
BEDROSSIAN, C. W. M., GREENBERG, S. D., YAWN, D. H., and O’NEAL. R. M. (1977). Experimentally induced bleomycin sulfate pulmonary toxicity. Arch. Pathol. Lab. Med. 101, 248-254.
BLUM, R. H., CARTER, S. K., and ACRE, K. (1973). A clinical review of bleomycin-A new antineo- plastic agent. Cancer 31, 903-914.
COLLINS, J. F., OROZCO, C. R., MCCULLOUGH, B., COALSON, J. J., and JOHANSON, W. G., JR. (1982). Pulmonary fibrosis with small-airway disease: A model in nonhuman primates. Exp. Lung Res. 3, 91-108.
CORNILLE, F., LAUWERIJINS, J., CORBEEL. L., BOEL. M., EECKELS, R., and VAN DE WALLE, J. (1980). Acquired ultrastructural abnormalities of bronchial cilia in recurrent airway infections and bron- chiectasis as compared with the findings in Kartagener’s syndrome. Pediatr. Res. 14, 168-169.
CUTS, E., LEVISON, H., and COOPER, D. M. (1978). Ultrastructure of airways in children with asthma. Histopathology 2, 407-421.
DALEN, H. (1981). An ultrastructural study of primary cilia, abnormal cilia, and ciliary knobs from the ciliated cells of the guinea pig trachea. Cell Tissue Res. 220, 685-697.
FAWCETT, D. (1961). Cilia and flagella. In “The Cell” (J. Brachet and A. E. Mirsky, eds.), Vol. 2, pp. 217-297. Academic Press, New York/London.
FOX, B., BULL, T. B., and ARDEN, G. B. (1980). Variations in the ultrastructure of human nasal cilia including abnormalities found in retinitis pigmentosa. J. C/in. Puthol. 33, 327-335.
FOX, B., and BULL. T. B. (1981). Abnormal cilia in Polynesians with bronchiectasis. Amer. Rev. Respir. Dis. 123, 142-143.
HARRIS, C. C.. KAUFMAN, D. G., JACKSON, F., SMITH, J. M., DEDICK, P., and SAFFIOTTI, U. (1974). Atypical cilia in the tracheobronchial epithelium of the hamster during respiratory carcinogenesis. J. Putho/. 114, 17-19.
JONES, A. W., and REEVE, N. L. (1978). Ultrastructural study of bleomycin-induced pulmonary changes in mice. 3. Puthol. 124, 227-233.
KATZ, S. M.. and HOLSCLAW. D. S.. JR. (1980). Ultrastructural features of respiratory cilia in cystic fibrosis. Amer. J. Clin. Pathol. 73, 682-685.
KENNEDY, J. R.. and ALLEN. P. L. (1976). Cigarette smoke induced cytopathology in tracheal epithe- lium. J. Cell Rio/. 70, 80a.
KOLLBERG, H., MOSSBERG, B., AFZELIUS, B. A., PHILIPSON, K., and CAMNER, P. (1978). Cystic fi- brosis compared with the immotile-cilia syndrome-A study of mucociliary clearance, ciliary ul- trastructure, clinical picture and ventilatory function. Stand. .I. Resp. Dis. 59, 297-306.
KONRADOVA V. (1973). Atypical kinocilia in the tracheal epithelium. Folk Morphol. 21, 71-78. KONRADOVP~ V., HLOUSKOVA, Z., and TOMANEK, A. (1975). Atypical cilia in human epithelium from
large bronchus. Folia Morphol. 23, 293-295. LUNA, M. A., BEDROSSIAN, C. W. M.. LICHTIGER B., and SALEN, P. A. (1972). Interstitial pneumonitis
associated with bleomycin therapy. Amer. J. Clin. Pathol. 58, 501-510.

BLEOMYCIN-INDUCED ABNORMAL CILIA 21
LUNGARELLA, G., FONZ~, L., and PACINI, E. (1980) A typical cilia in rabbit bronchial epithelial cells induced by elastase: An ultrastructural study. J. Puthol. 131, 379-383.
MCDOWELL, E. M., BARRETT, L. A., HARRIS, C. C., and TRUMP, B. E (1976). Abnormal cilia in human bronchial epithelium. Arch. Purhol. Lab. Med. 100, 429-436.
RANGA, V.. and KLEINERMAN, J. (1981). A quantitative study of ciliary injury in the small airways of mice: The effects of nitrogen dioxide. Exp. Lung Res. 2, 49-55.
STARKE. I. D., CORRIN, B., SELBY, P. J.. WEBSTER, A. D. B., and TURNER-WARWICK, M. (1981). Recurrent chest infections, ciliary abnormalities and partial complement deficiency in a Jordanian family. Thorar 36, 502-507.
TAKASAKA, T., SATO. M., and ONODERA, A. (1980). Atypical cilia of the human nasal mucosa. Ann. Oral. 89, 37-45.
WAKEFIELD, J. ST. J.. and WATE. D. (1980). Abnormal cilia in polynesians with bronchiectasis. Amer. Rev. Resp. Dis. 121, 1003-1010.
WILSMAN, N. L.. FARNUM. C. E.. and REED, D. K. (1982). Variability of ciliary ultrastructure in normal dogs. Amer. J. Anal. 164, 343-352.
WISSEMAN, C. L.. SIMEL. D. L., SPOCK, A., and SHELLBLJRNE, J. D. (1981). The prevalence of ab- normal cilia in normal pediatric lungs. Arch. Parho/. 105, 552-555.





























