Embed Size (px)
Citation preview

Ablation for Paroxysmal Atrial Fibrillation (APAF) Ablation for Paroxysmal Atrial Fibrillation (APAF) TrialTrial
Ablation for Paroxysmal Atrial Fibrillation (APAF) Ablation for Paroxysmal Atrial Fibrillation (APAF) TrialTrial
Presented atPresented atThe American College of CardiologyThe American College of Cardiology
Scientific Session 2006Scientific Session 2006
Presented by Dr. Carlo PapponePresented by Dr. Carlo Pappone
APAF TrialAPAF TrialAPAF TrialAPAF Trial

www. Clinical trial results.org
APAF Trial: BackgroundAPAF Trial: BackgroundAPAF Trial: BackgroundAPAF Trial: Background
• AF affects between 2 and 3 million people in the United StatesAF affects between 2 and 3 million people in the United States
• Antiarrhythmic drugs have limited use in treating AF due to side Antiarrhythmic drugs have limited use in treating AF due to side effects and increased mortalityeffects and increased mortality
• The present trial sought to investigate the treatment of paroxysmal The present trial sought to investigate the treatment of paroxysmal atrial fibrillation using an alternative to pharmacologic treatmentatrial fibrillation using an alternative to pharmacologic treatment
• AF affects between 2 and 3 million people in the United StatesAF affects between 2 and 3 million people in the United States
• Antiarrhythmic drugs have limited use in treating AF due to side Antiarrhythmic drugs have limited use in treating AF due to side effects and increased mortalityeffects and increased mortality
• The present trial sought to investigate the treatment of paroxysmal The present trial sought to investigate the treatment of paroxysmal atrial fibrillation using an alternative to pharmacologic treatmentatrial fibrillation using an alternative to pharmacologic treatment
Presented at ACC 2006Presented at ACC 2006

www. Clinical trial results.org
APAF Trial: Study DesignAPAF Trial: Study DesignAPAF Trial: Study DesignAPAF Trial: Study Design
Primary Endpoint: Freedom from recurrent atrial arrhythmiasPrimary Endpoint: Freedom from recurrent atrial arrhythmias Secondary Endpoint: Monthly rhythm analysis; adverse events, left atrium remodelingSecondary Endpoint: Monthly rhythm analysis; adverse events, left atrium remodeling
Primary Endpoint: Freedom from recurrent atrial arrhythmiasPrimary Endpoint: Freedom from recurrent atrial arrhythmias Secondary Endpoint: Monthly rhythm analysis; adverse events, left atrium remodelingSecondary Endpoint: Monthly rhythm analysis; adverse events, left atrium remodeling
Circumferential pulmonary vein ablation (CPVA)
n=99
Circumferential pulmonary vein ablation (CPVA)
n=99
Antiarrhythmic medical therapyn=99
with flecainide (n=33)with sotalol (n=33)
with amiodarone (n=33)
Antiarrhythmic medical therapyn=99
with flecainide (n=33)with sotalol (n=33)
with amiodarone (n=33)
198 patients age 18-70 presenting with paroxysmal atrial fibrillation >6 months and qualifying atrial fibrillation burden >2 episodes per month/
Randomized.33% female, mean age 56 years, mean follow-up 12 months
198 patients age 18-70 presenting with paroxysmal atrial fibrillation >6 months and qualifying atrial fibrillation burden >2 episodes per month/
Randomized.33% female, mean age 56 years, mean follow-up 12 months
Presented at ACC 2006Presented at ACC 2006
Following a 1-month run-in phase to uptitrate antiarrhythmic medical therapy in both arms, ablation was performed Following a 1-month run-in phase to uptitrate antiarrhythmic medical therapy in both arms, ablation was performed in patients randomized to CPVA to encircle all 4 PVs with 3 additional lines to prevent atrial tachycardias (ATs) using in patients randomized to CPVA to encircle all 4 PVs with 3 additional lines to prevent atrial tachycardias (ATs) using either a 8mm or a 3.5mm irrigated tip catheter and with the guide of CARTO or NavX system. Medical therapy was either a 8mm or a 3.5mm irrigated tip catheter and with the guide of CARTO or NavX system. Medical therapy was discontinued in the CPVA group. Crossovers were allowed after 3 months.discontinued in the CPVA group. Crossovers were allowed after 3 months.
Following a 1-month run-in phase to uptitrate antiarrhythmic medical therapy in both arms, ablation was performed Following a 1-month run-in phase to uptitrate antiarrhythmic medical therapy in both arms, ablation was performed in patients randomized to CPVA to encircle all 4 PVs with 3 additional lines to prevent atrial tachycardias (ATs) using in patients randomized to CPVA to encircle all 4 PVs with 3 additional lines to prevent atrial tachycardias (ATs) using either a 8mm or a 3.5mm irrigated tip catheter and with the guide of CARTO or NavX system. Medical therapy was either a 8mm or a 3.5mm irrigated tip catheter and with the guide of CARTO or NavX system. Medical therapy was discontinued in the CPVA group. Crossovers were allowed after 3 months.discontinued in the CPVA group. Crossovers were allowed after 3 months.

www. Clinical trial results.org
APAF Trial: Baseline APAF Trial: Baseline data from 150 patientsdata from 150 patients
APAF Trial: Baseline APAF Trial: Baseline data from 150 patientsdata from 150 patients
Presented at ACC 2006Presented at ACC 2006
num
ber
of A
F e
piso
des
per
year
num
ber
of A
F e
piso
des
per
year
52
30
0
15
30
45
60
CPVA group Control group
52
30
0
15
30
45
60
CPVA group Control group
Atrial Fibrillation Episodes per Year at Time of EnrollmentAtrial Fibrillation Episodes per Year at Time of Enrollmentp=0.05p=0.05
• Paroxysmal atrial fibrillation Paroxysmal atrial fibrillation duration averaged 6 years at duration averaged 6 years at the time of enrollmentthe time of enrollment
• AF episodes per year were AF episodes per year were more common in the CPVA more common in the CPVA group at baseline (52 vs 30; group at baseline (52 vs 30; p=0.05)p=0.05)
• Baseline ejection fraction Baseline ejection fraction was 60%was 60%
• History of hypertension was History of hypertension was found in 56% of patientsfound in 56% of patients

www. Clinical trial results.org
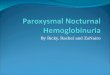
APAF Trial: Primary Endpoint at 9 monthsAPAF Trial: Primary Endpoint at 9 monthsAPAF Trial: Primary Endpoint at 9 monthsAPAF Trial: Primary Endpoint at 9 months
Presented at ACC 2006Presented at ACC 2006
Freedom from recurrent AF and AT at 9 months (%)Freedom from recurrent AF and AT at 9 months (%)p<0.001p<0.001
87%
29%
0%
25%
50%
75%
100%
CPVA group Control group
87%
29%
0%
25%
50%
75%
100%
CPVA group Control group
• At 9 months, a greater At 9 months, a greater number of patients in the number of patients in the CPVA group were free CPVA group were free from recurrent AF and from recurrent AF and AT (all CPVA patients in AT (all CPVA patients in the absence of the absence of antiarrhythmic drug antiarrhythmic drug therapy) (87% vs 29%; therapy) (87% vs 29%; p<0.001)p<0.001)

www. Clinical trial results.org
APAF Trial: Recurrent AFAPAF Trial: Recurrent AFAPAF Trial: Recurrent AFAPAF Trial: Recurrent AF
Presented at ACC 2006Presented at ACC 2006
• Of the 8 patients who had recurrent AF in the CPVA Of the 8 patients who had recurrent AF in the CPVA group, repeat ablation procedure was performed in 3 group, repeat ablation procedure was performed in 3 patients, one of whom still had additional recurrent AF.patients, one of whom still had additional recurrent AF.
• Of the 52 patients who had recurrent AF in the control Of the 52 patients who had recurrent AF in the control group, 38 had CPVA performed, 4 of whom still had group, 38 had CPVA performed, 4 of whom still had additional recurrent atrial fibrillationadditional recurrent atrial fibrillation

www. Clinical trial results.org
APAF Trial: Secondary EndpointsAPAF Trial: Secondary EndpointsAPAF Trial: Secondary EndpointsAPAF Trial: Secondary Endpoints
Presented at ACC 2006Presented at ACC 2006
• At 12 months, there was a significant decrease in left At 12 months, there was a significant decrease in left atrium diameter in patients randomized to CPVA atrium diameter in patients randomized to CPVA (p<0.05), but no difference in patients randomized to (p<0.05), but no difference in patients randomized to the control groupthe control group
• Adverse events in the CPVA group included 1 TIA and Adverse events in the CPVA group included 1 TIA and 1 pericardial effusion1 pericardial effusion

www. Clinical trial results.org
TAXUS V ISR Trial: LimitationsTAXUS V ISR Trial: LimitationsTAXUS V ISR Trial: LimitationsTAXUS V ISR Trial: Limitations
• This trial excluded many AF patients on the basis of This trial excluded many AF patients on the basis of age and disease progression: patients older than 70 age and disease progression: patients older than 70 and those with an enlarged atrium or low ejection and those with an enlarged atrium or low ejection fraction (<35%) were excluded from the APAF Trial. fraction (<35%) were excluded from the APAF Trial. Future trials might look to include these patients who Future trials might look to include these patients who better represent the real-world AF population.better represent the real-world AF population.
• The current trial is too short to adequately assess and The current trial is too short to adequately assess and answer important safety concerns.answer important safety concerns.
• This trial excluded many AF patients on the basis of This trial excluded many AF patients on the basis of age and disease progression: patients older than 70 age and disease progression: patients older than 70 and those with an enlarged atrium or low ejection and those with an enlarged atrium or low ejection fraction (<35%) were excluded from the APAF Trial. fraction (<35%) were excluded from the APAF Trial. Future trials might look to include these patients who Future trials might look to include these patients who better represent the real-world AF population.better represent the real-world AF population.
• The current trial is too short to adequately assess and The current trial is too short to adequately assess and answer important safety concerns.answer important safety concerns.
Presented at ACC 2006Presented at ACC 2006

www. Clinical trial results.org
TAXUS V ISR Trial: SummaryTAXUS V ISR Trial: SummaryTAXUS V ISR Trial: SummaryTAXUS V ISR Trial: Summary
• Among patients with paroxysmal atrial fibrillation, treatment with Among patients with paroxysmal atrial fibrillation, treatment with circumferential pulmonary vein ablation was associated with a reduction in circumferential pulmonary vein ablation was associated with a reduction in recurrent AF and AT compared with conventional antiarrhythmic medical recurrent AF and AT compared with conventional antiarrhythmic medical therapy at 12 monthstherapy at 12 months
• Medical management of AF can be difficult as it requires frequent Medical management of AF can be difficult as it requires frequent monitoring. CPVA has been used as an alternative management strategy monitoring. CPVA has been used as an alternative management strategy for AF but randomized data comparing the two therapies are limited.for AF but randomized data comparing the two therapies are limited.
• The present trial is one of the first randomized trials of CPVA in the setting The present trial is one of the first randomized trials of CPVA in the setting of paroxysmal AF. CPVA was recently shown to be beneficial in of paroxysmal AF. CPVA was recently shown to be beneficial in maintaining sinus rhythm in the setting of chronic AF. maintaining sinus rhythm in the setting of chronic AF.
• Full one-year data for the entire cohort of this trial are not yet available, Full one-year data for the entire cohort of this trial are not yet available, although the 9-month data are very positive.although the 9-month data are very positive.
• Among patients with paroxysmal atrial fibrillation, treatment with Among patients with paroxysmal atrial fibrillation, treatment with circumferential pulmonary vein ablation was associated with a reduction in circumferential pulmonary vein ablation was associated with a reduction in recurrent AF and AT compared with conventional antiarrhythmic medical recurrent AF and AT compared with conventional antiarrhythmic medical therapy at 12 monthstherapy at 12 months
• Medical management of AF can be difficult as it requires frequent Medical management of AF can be difficult as it requires frequent monitoring. CPVA has been used as an alternative management strategy monitoring. CPVA has been used as an alternative management strategy for AF but randomized data comparing the two therapies are limited.for AF but randomized data comparing the two therapies are limited.
• The present trial is one of the first randomized trials of CPVA in the setting The present trial is one of the first randomized trials of CPVA in the setting of paroxysmal AF. CPVA was recently shown to be beneficial in of paroxysmal AF. CPVA was recently shown to be beneficial in maintaining sinus rhythm in the setting of chronic AF. maintaining sinus rhythm in the setting of chronic AF.
• Full one-year data for the entire cohort of this trial are not yet available, Full one-year data for the entire cohort of this trial are not yet available, although the 9-month data are very positive.although the 9-month data are very positive.
Presented at ACC 2006Presented at ACC 2006