-
BASIC ARTERIAL BLOOD GAS (ABG) INTERPRETATION
By: Jesus Mario A Lopez Jr., R.T.,R.N.
-
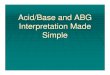
Common Arterial Blood Gas Puncture Sites
4.bin
-
Obtaining ABG Puncture Sites
AdultChild (> 24 months)Neonate(< 12 months)1* - Radial A.2*
- Brachial A.3* - Femoral A. 4* -Dorsalis Pedis A.5* - Posterior
Tibial A. 1* - Radial A.2* - Brachial A.1* Brachial A. 2* Umbilical
V.3* Capilliary and Heel Stick samples (opitional)
- 50.bin
-
30-40
45-60
90
Radial
Brachial
Femoral
10-20
Dorsalis P. & Posterior T.
-
Modified Allens Test
-
Sampling Hazards
Disruption of blood flow (e.g. Hematoma)
Clotting
Bleeding
Vessel spasm
Fistulas
Tissue trauma
Under Anticoagulant Therapy
Poor skin healing (underlying dse.)
-
Sampling Problems
Air Bubbles
* PaCo2
* Pa02 or
* pH
Improper cooling (> 1 hr.)
* PaCo2
* Pa02
* pH
Too much heparin
*pH
-
Factors may alter ABG results
Post suctioning
Nebulization (after?)
Movement (Turning)
Medications (I.V.)
Activity/Procedures
Handling of sample
-
Normal Values:
ParametersRangeAbsoluteMixed
VenouspH7.35-7.457.407.31-7.41PaCO235-45 mmHg40 mmHg41-51
mmHgPaO280-100 mmHg95 mmHg37-43 mmHgHCO322-26 mmHg24 mEq/L22-26
mEq/LBE/BD-2 to +2 mEq/L 0 mEq/L-2 to +2 mEq/LO2 Sat %>
95%98%68-75 %
-
pH - 7.45=Alkalotic
HCO3 - 26mEq/L=Alkalotic
BE/BD - +2 Alkalotic
PaCO2 - > 45mmHg=Acidotic
< 35mmHg=Alkatotic
-
Organs involved in ABG
Respiratory Component = Lungs PaCo2
- minutes to compensate
Metabolic Component = Kidneys HCO3
- days/weeks to compensate
-
Primary and Compensatory response for acid-base disorders:
Primary Event Compensatory Response PaCO2 HCO3 PaCO2 HCO3
-
Arterial Oxygenation Status (PaO2)
* Note for individuals over age of 60 y/o, 1mmHg should be
subtracted from the lower limits of mild and moderate hypoxemia for
each year over 60 y/o. At any age a PaO2 < 40mmHg indicates
severe hypoxemia, and a PaO2 of 100mmHgCorrected oxygenation=
80-100mmHgUncorrected/inadequate oxygenation=
-
Monitoring of O2 & CO2 status
ABG analysis (Confirmatory!!!)Pulse oximetry (least)EtCO2
monitoring (spot check/transport vent )Capillary gas
determination(infants only)Transcutaneous monitoringOxygenation
indices
-
Steps in ABG Interpretation:
Determine the pH
Determine whether respiratory or metabolic in origin
Determine the compensation
Determine the Oxygenation Status
________ _______ _______ ________
4
3
2
1
- 7.bin
-
pH= 6.90
PaCO2=70mmHg
PaO2=39mmHg
HCO3= 23mEq/L
BE/BD= -4mEq/L
O2 Sat= 90%
Age: 20 y/o
Fi02: R.A.
Interpretation: Uncompensated Respiratory Acidosis w/ Severe
Hypoxemia
-
ABG: RESPIRATORY ACIDOSIS
Causes (mainly airway obstruction & resp. depression)COPD:
Asthma, Bronchiectasis, Bronchitis, EmphysemaAtelectasisBrain
traumaHypoventilation Sedatives, narcotics, anesthetics Pulmonary
edema
-
ABG: RESPIRATORY ACIDOSIS
S/Sx RR & depthHA, visual disturbance, restlessness,
drowsiness, confusionDiaphoresisCyanosisHyper Kdysrhythmias
(VF)
-
ABG: RESPIRATORY ACIDOSIS
TxSemi-Fowlers, O2, coughingHydration Suction secretionsWOF RR
distress, hyper KAntibiotics & other meds as ordered
-
pH= 7.60
PaCO2=52mmHg
PaO2=77mmHg
HCO3= 28mEq/L
BE/BD= +3mEq/L
O2 Sat= 94%
Age: 35 y/o
Fi02: 50% Simple Face Mask
Interpretation: Partially compensated Respiratory Alkalosis w/
uncorrected oxygenation
-
ABG: RESPIRATORY ALKALOSIS
Causes (mainly overstimulation of the respiratory
system)HyperventilationFeverHypoxiaHysteriaOverventilation by mech
vent.Pain Salicylates
-
ABG: RESPIRATORY ALKALOSIS
S/Sx RR & depth then RRHA, light-headedness, vertigoHypo Ca:
paresthesia, tetany, convulsionHypo K
-
pH= 7.00
PaCO2=40mmHg
PaO2=88mmHg
HCO3= 29mEq/L
BE/BD= -8mEq/L
O2 Sat= 90%
Age: 54y/o
Fi02: 2LPM Via nasal cannula
Interpretation: Uncompensated metabolic acidosis w/ corrected
oxygenation
-
ABG: METABOLIC ACIDOSIS
CausesDM & DKAASA toxicityHigh fat dietInsufficient CHO
metabolismMalnutritionRFSevere diarrhea
-
ABG: METABOLIC ACIDOSIS
S/Sx RR, Kussmauls respirationHA, N/V/diarrheaFruity-smelling
breathCNS depressionTwitching, convulsionHyper K
-
ABG: METABOLIC ACIDOSIS
TxNaHCO3 IVSz precautionFor DKA: NS & Regular Insulin IVFor RF:
CHON, calorie diet; dialysis
-
pH= 7.48
PaCO2= 42mmHg
PaO2= 73mmHg
HCO3= 30mEq/L
BE/BD= +8.8mEq/L
O2 Sat= 96.21%
Age: 10 y/o
Fi02: R.A.
Interpretation: Uncompensated Metabolic Alkalosis w/ mild
hypoxemia
-
ABG: METABOLIC ALKALOSIS
CausesDiureticsExcessive vomiting or GI
suctioningHyperaldosteronismExcessive NaHCO3 intakeMassive BT
(citrate converted to HCO3)
-
ABG: METABOLIC ALKALOSIS
S/Sx RR & depthN/V/diarrheaRestlessnessParesthesia,
twitchingHypoK, HypoCa HR, dysrhythmias
-
Case Studies:
1. A 20 y/o female with known DM II entered the ER with
Kussmauls breathing and irregular pulse. 02 @ 4Lpm via nasal prong,
V/S and ABG were taken.
V/S = RR-25 bpmABG = pH 7.12
CR-108 bpm PaCO2 35mmHg
BP- 100/50 mmHg PaO2- 101mmHg
HCO3- 13 mEq/L
O2 Sat%- 99.0%
Interpretation: Uncompensated metabolic acidosis w/ over
corrected oxygenation.
-
Case Studies:
2., A client recovering from surgery in the post-anesthesia care
unit (PACU) is difficult to arouse two hours following surgery. The
nurse in the PACU has been administering Morphine Sulfate
intravenously to the client for complaints of post-surgical pain.
The clients respiratory rate is 7 per minute and demonstrates
shallow breathing. The patient does not respond to any stimuli
.
V/S = RR- 8 bpmABG = pH 7.10
CR- 40bpmPaCO2 60mmHg
BP- 50 palpPaO2- 41mmHg
O2 3lpm n.c.HCO3- 29mEq/L
O2 Sat%- 85%
Interpretation: Partially compensated respiratory acidosis w/
moderate hypoxemia.
-
Case Studies:
3. A two-year-old is admitted to the hospital with a diagnosis
of asthma and respiratory distress syndrome. The father of the
infant reports to the nurse that he has observed slight tremors and
behavioral changes in his child over the past three days. The
attending physician orders routine ABGs following an assessment of
the ABCs. The ABG results are:
V/S = RR-25 bpmABG = pH 7.40
CR-135 bpmPaCO2 47mmHg
BP- 175/110 mmHgPaO2- 115mmHg
O2 7lpm tusk mask HCO3- 39mEq/L
O2 Sat%- 100.0%
Interpretation: Compensated metabolic alkalosis w/ over
corrected oxygenation.