Embed Size (px)
Citation preview

Abdominal PainAbdominal PainAssessment and Diagnosis
Lawrence R. Kosinski,MD,MBA,AGAF
Principles of Gastroenterology for the Nurse Practitioner and Physician AssistantAugust 10-12, 2012g ,
What is Abdominal Pain?An unpleasant experience commonly associated with tissue injury or tissue distressassociated with tissue injury or tissue distress
R t i t l fRepresents an interplay of: pathophysiologic and psychosocial factors
Physiologic Determinantsy gThe nature of the stimuliThe type of receptor involvedModifying influences – psychosocial?

Today’s Algorhithmy g

Anatomic Basis of Abd PainLocation of Sensory Neuroreceptors
Muscularis of hollow visceraOn Serosal StructuresIn the Mesentery
Types of Sensory NeuroreceptorsMyelinated A Delta Fibers: somatoparietal painUnmyelinated C Fibers: visceral pain

Abdominal Pain‐Stimuli
St t hStretchInflammation
Ischemia
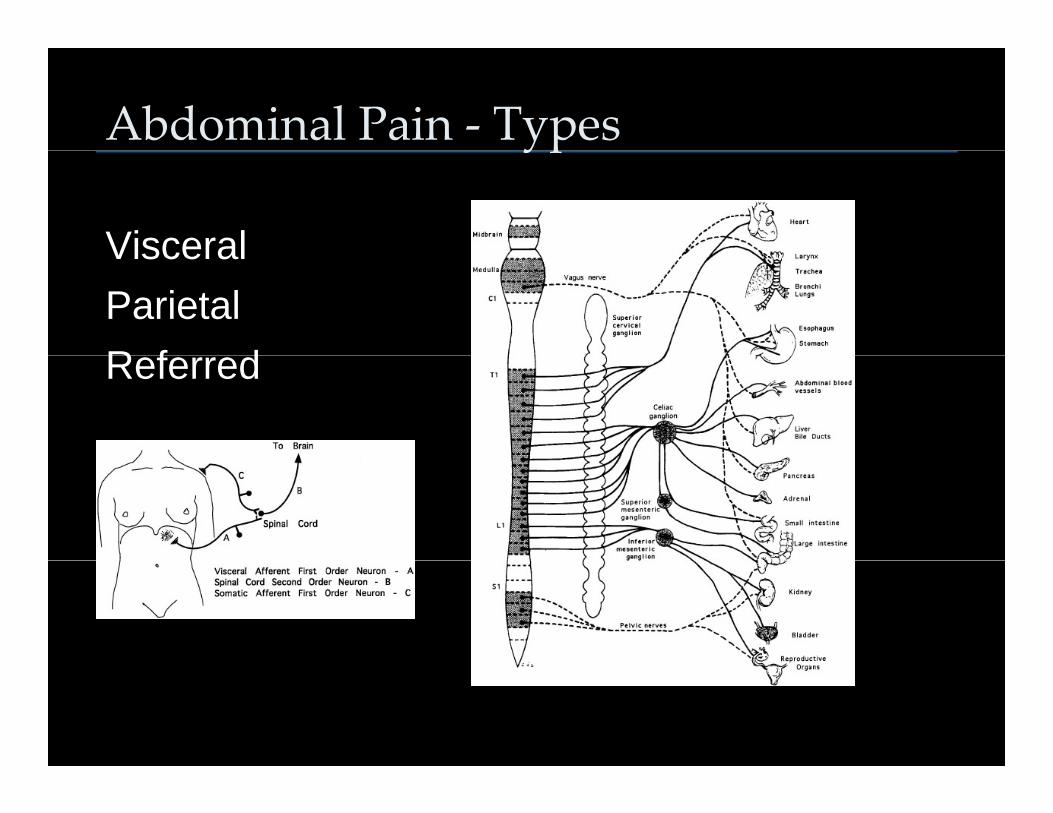
Abdominal Pain ‐ Typesyp
VisceralVisceralParietalR f dReferred

Abdominal Pain ‐ Historyy
LocationQualityChronologyChronologyAggravating FactorsA i t d S tAssociated Symptoms

LocationEpigastrium
EsophagusEsophagusStomachDuodenumG llbl ddGallbladderPancreas
PeriumbilicalPeriumbilicalSmall IntestineAscending Colon
Lower AbdomenEntire ColonGyne SourcesGyne Sources

Location
QualityyVisceral Pain
Dull, Cramping, Burning, Gnawingu , C a p g, u g, G a g
Parietal PainSharp and intenseSharp and intense
ExamplesAppendicitisAppendicitisUlcers GnawAneurysms tearAneurysms tear

Pearl #1
The patient with Visceral Pain won’t stop moving
The patient with Parietal Pain doesn’t want to move at all.move at all.

Chronologygy
SuddenSuddenRapidG d lGradual

Case #1Hx: 86 y/o female A/W the acute onset of severe diffuse abdominal pain. No bowel activity. She is lying motionless in the bed and is somewhat lethargic/confused.
Px: T 101, P100, R 20, 180/90Px: T 101, P100, R 20, 180/90Abd: Mildly distended, relatively soft, No BS
Labs: WBC 22K, Hb. 10, PC 110K

Differential Diagnosis of Abd Pain ofSudden Onset (<1 hour)( )
Perforated UlcerRuptured AbcessRuptured HematomaRuptured HematomaEsophageal RuptureDi ti A
Mechanical Process
Dissecting AneurysmEctopic PregnancyMesenteric Infarction

CT Findingg
Diagnosis: SMA Thrombosis with Ischemic Infarction of the Small Bowel

Pearl #2
When you are presented with sudden severe abdominal pain
THINK MECHANICAL PROCESSES: RUPTURERUPTURE
OR INFARCTION
Pearl #3
When pain is out of proportion to physical findings, think:
ISCHEMIA

Case #2Hx: 42 y/o obese female admitted with the several hours of epigastric and RUQ p g Qabdominal pain associated with nausea and vomitingPx: T 100, P 90, R 18, BP: 150/89Abd: Obese soft BS absent Tender to lightAbd: Obese, soft, BS absent. Tender to light palpation in the RUQ
Labs: WBC 13K, Hb 12, AST 180, ALT 160, AP 131
Abdominal Pain ‐ ChronologyRapid Onset (>1 hour)p ( )
All causes of Sudden Pain +Intestinal ObstructionAcute CholecystitisAcute CholecystitisAcute PancreatitisA t Di ti liti
InflammationAcute DiverticulitisUreteral Colic

Ultrasound
Diagnosis: Acute Cholecystitis

Pearl #4Pain of Rapid onset (>1 hour)
THINK OBSTRUCTION OR INFLAMMATIONOBSTRUCTION OR INFLAMMATION

Case #361yo w/m presented two days of LLQ abdominal pain, described as sharp, constant with no radiation. He has had no bowel movement during that time. PMH: Totally negative No medsNo medsPx: T101, VSSAbd: Mildly distended no BS tender in LLQAbd: Mildly distended, no BS, tender in LLQ with guarding

Abdominal Pain – ChronologyGradual Onset
All causes of Sudden and RapidAppendicitisMeckel’s DiverticulitisMeckel s DiverticulitisAbdominal Abcess

Imagingg g
Diagnosis: Diverticulitis with Abcess
Pearl #5
Pain nearly always precedes vomiting with surgical problems whereas with most nonsurgical causes, it follows and vomiting comes first.
Nonsurgical Problem: Vomiting before PainSurgical Problem: Pain before VomitingSurgical Problem: Pain before Vomiting

Abdominal PainAggravating and Alleviating Factorsgg g g
Postural EffectsRemember the Mesentery
Meal Related EffectsRemember the Gastro-colic Reflex
Bowel Related EffectsBowel Related EffectsThey will tell you if the colon is involved
MedicationsMedicationsEspecially those taken at night

Abdominal Examination
InspectionAuscultationPalpationPalpationPercussion

Physical Exam ‐ Inspectiony p
DistentionDistentionScarsE h iEcchymosisVenous PatternStriaJaundice

Abdominal DistentionThink of the 6Fs
FatFluid - AscitesFlatus - GasFlatus GasFetus - PregnancyF Ob ti tiFeces - ObstipationFatal Growths - Tumors

Scars
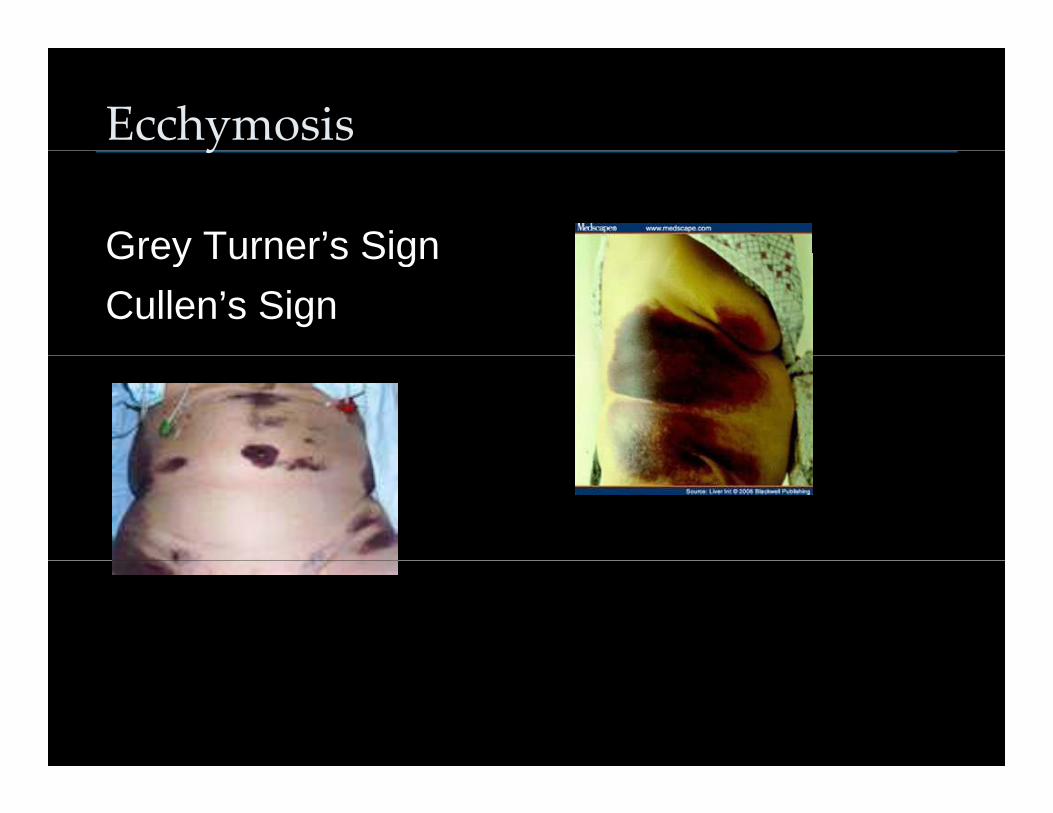
Ecchymosisy
Grey Turner’s SignGrey Turner s SignCullen’s Sign

Venous Pattern
Caput Medusa
Caput Medusae - flow is towards the legsCaput Medusae flow is towards the legsInferior vena cava obstruction - flow is towards the head

Stria

Physical Exam ‐ Auscultationy
Bowel SoundsNormalHyperactive: Obstruction or ColitisHypoactive: IleusAbsent: Acute Abdomen
Bruits

Physical Exam ‐ Palpationy p
Light PalpationLight PalpationBuild ConfidenceStart away from the painStart away from the painTenderness
Direct TendernessRebound Tenderness
Deep PalpationOrgan Size Masses

Physical Exam ‐ Percussiony
Organ size and DensityOrgan size and DensityTypes of Sounds
Tympani to DullnessTympani to Dullness
AscitesB f l i h i i hBe careful in the patient with abdominal pain

Rectal Examination
Don’t forget a rectalDon t forget a rectal examPelvic AbscessPelvic AbscessMassesV i i iVaricosities

Laboratory Evaluationy
CBC: Anemia, leukocytosis, thrombocytopenia, MCV
CMPRenal Function, Acid Base, LFTs
Amylase/LipaseAmylase/LipasePT/INR: liver disease, WarfarinUrinalysisUrinalysisPregnancy Test

Imagingg g
Obstructive Series: DistentionFree Air
US: CholecystitisPelvic Processes
CT:

Plain X‐raysyUtility
Gas PatternsCalcifications
BenefitsInexpensiveEasy to doN i iNoninvasive
LimitationsLimited Detail of hollow organsLimited Detail of hollow organs

Example 1

Example 2

Example 3

UltrasoundIndications
Evaluation of the Biliary Tree, Liver, Pancreasy , ,Pelvic Organs
BenefitsNoninvasiveNo Radiation doseP ti t T lPatient Tolerance
LimitationsPoor visualization of hollow GI organsPoor visualization of hollow GI organsLimited visualization in obese or distended patients

Nuclear Medicine Studies
IndicationsLiver and Biliary ScanningLiver and Biliary ScanningGI BleedingGastric Emptying
BenefitsNoninvasiveGood Patient Compliance
LimitationsP I i d t ilPoor Imaging detailInconclusive results

Example 1Normal Biliary Imagingy g g
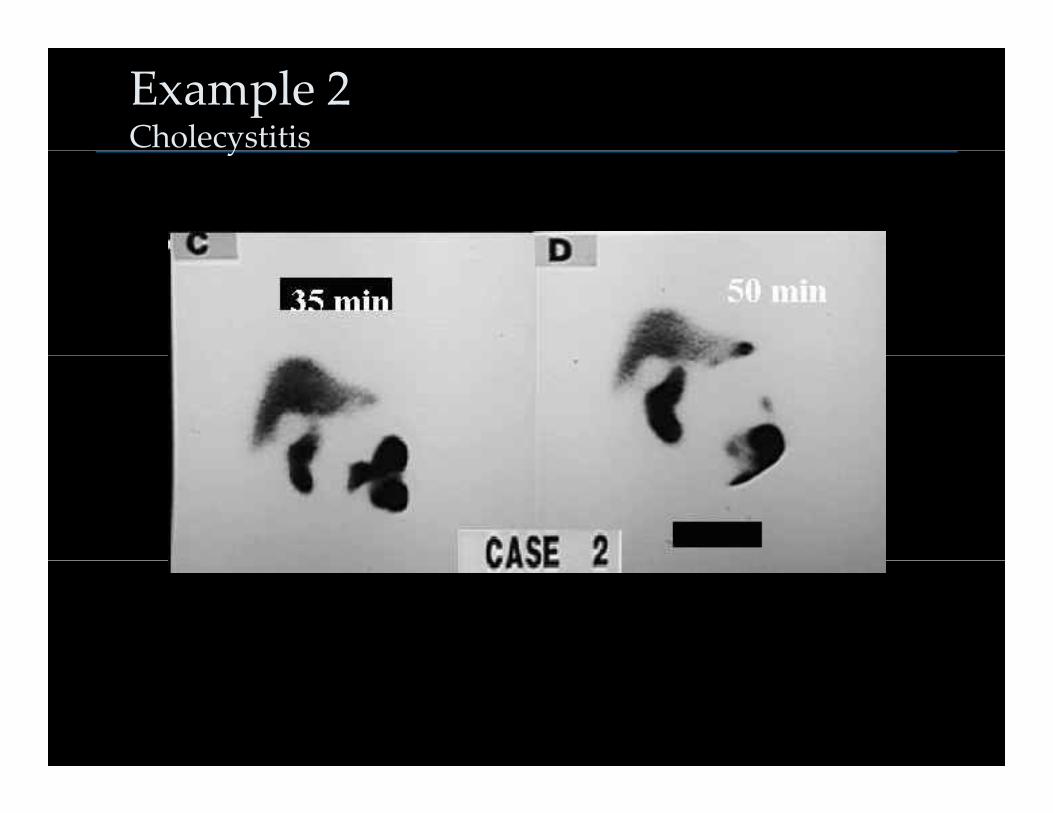
Example 2 Cholecystitisy

CT ScanningIndications
Evaluation of Solid organs, ie: Liver, Pancreas, S lSpleen
Requires IV ContrastBowel Wall Evaluation
Requires Oral Contrast
BenefitsEasily DoneEasily DoneGood Patient Compliance
LimitationsHollow organs not visualized in detailImmobile (Cannot be done at bedside)

CT Overview

Slices

Example 1Cirrhosis with Ascites

Example 2Bowel Wall Infarct

Example 3Retroperitoneal Abcessp

Example 4Crohn’s Disease
Differential Diagnosisg
Epigastric PainGERDPeptic Ulcer DiseaseGastritisPancreatitisIschemia/Infarction
Pearl #8
Bleeders don’t hurt and hurters don’t bleedWhen you see a bleeder that hurts, think ischemia

Differential Diagnosis – RUQ Paing Q
Acute CholecystitisPeptic Ulcer DiseaseHepatic DisordersHepatic DisordersColon Disorders

Differential Diagnosis – LUQ Paing Q
Splenic DisordersColon DisordersIBSIBSPancreatitis

Differential Diagnosis – Periumbilicalg
Intestinal DisordersObstructionIBD
V l Di dVascular DisordersAAAI f tiInfarction

Differential Diagnosis – RLQ Paing Q
Acute AppendicitisMeckel’s DiverticulitisCrohn’s DiseaseCrohn s DiseaseValentino AppendicitisO i C tOvarian CystIBS

Differential Diagnosis – LLQ Paing Q
Colonic DisordersDiverticulitisIBDIBS
Ovarian Disorders

Differential Diagnosis – Suprapubic g p p
Bladder DisordersOvarian CystOvarian CystRuptured Endometrioma

Patience and Wisdom

DISCUSSION
Lawrence R. Kosinski, MD, MBA, AGAFManaging PartnerIllinois Gastroenterology Group745 Fletcher Drive745 Fletcher DriveElgin, Illinois 60123