Embed Size (px)
Citation preview

www.elsevier.com/locate/ygyno
Gynecologic Oncology
Abdominal carcinomatosis in women with a history of breast cancer
Ruchi Garga, Mariana L. Zahurakb, Edward L. Trimblea,
Deborah K. Armstrongc, Robert E. Bristowa,c,*
aDepartment of Gynecology and Obstetrics, The Sidney Kimmel Comprehensive Cancer Center,
The Johns Hopkins Medical Institutions, Baltimore, MD 21287-1281, USAbDepartment of Biostatistics, The Sidney Kimmel Comprehensive Cancer Center, The Johns Hopkins Medical Institutions, Baltimore, MD 21287-1281, USAcDepartment of Oncology, The Sidney Kimmel Comprehensive Cancer Center, The Johns Hopkins Medical Institutions, Baltimore, MD 21287-1281, USA
Received 23 December 2004
Available online 23 June 2005
Abstract
Objectives. The goals of this study were to: (1) characterize the etiology of abdominal carcinomatosis, (2) identify clinical features
predictive of primary ovarian/peritoneal cancer, and (3) evaluate the survival impact of cytoreductive surgery among patients with advanced
ovarian/peritoneal cancer and a history of breast cancer.
Methods. Patients with a history of prior breast cancer undergoing surgical exploration for abdominal carcinomatosis between 1/1/88 and
12/31/02 were retrospectively identified from tumor registry databases. Logistic regression analysis was used to explore clinical
characteristics predictive of primary ovarian/peritoneal cancer versus recurrent breast cancer. Survival analyses and comparisons were
performed using the Kaplan–Meier and Cox proportional hazard models.
Results. Seventy-nine patients underwent surgery for abdominal carcinomatosis a median of 5.39 years after initial breast cancer
diagnosis. Abdominal carcinomatosis was due to primary ovarian/primary peritoneal cancer in 74.7% of cases. A history of Stage I breast
cancer [OR = 10.73, 95%CI = 2.6–43.7, P < 0.001] and the lack of a prior breast cancer recurrence [OR = 10.60, 95%CI = 2.5–45.2, P <
0.001] were independently predictive of primary ovarian/peritoneal cancer. Among patients with primary ovarian/peritoneal cancer, optimal
(�1 cm) cytoreductive surgery was associated with a median survival of 44.0 months compared to 18.0 months for patients with suboptimal
residual disease [HR = 6.81, 95%CI = 3.37–13.77, P < 0.0001]. Recurrent breast cancer was associated with a median survival time of 6.4
months.
Conclusions. Among patients with prior breast cancer presenting with abdominal carcinomatosis, early-stage disease and the absence of a
prior recurrence were predictive of primary ovarian/peritoneal cancer. Optimal cytoreductive surgery was associated with a significant
survival advantage for patients with primary ovarian/peritoneal cancer.
D 2005 Elsevier Inc. All rights reserved.
Keywords: Abdominal carcinomatosis; Ascites; Breast cancer; Ovarian cancer; Peritoneal cancer
Introduction
Breast cancer is the most common malignancy among
women in the United States. The current 5-year relative
survival rates of 97% and 78% for localized and regional
0090-8258/$ - see front matter D 2005 Elsevier Inc. All rights reserved.
doi:10.1016/j.ygyno.2005.05.013
* Corresponding author. The Kelly Gynecologic Oncology Service,
Department of Gynecology and Obstetrics, The Sidney Kimmel Compre-
hensive Cancer Center, The Johns Hopkins Medical Institutions, 600 N.
Wolfe Street, Phipps #281, Baltimore, MD 21287-1281, USA. Fax: +1 410
614 8718.
E-mail address: [email protected] (R.E. Bristow).
disease, respectively, indicate that a significant proportion of
breast cancer patients will experience prolonged survival
[1]. Although the risk of breast cancer recurrence diminishes
over time, late recurrences well into the second decade of
surveillance can occur. Among patients with metastatic
breast cancer, extra-hepatic and extra-skeletal abdominal
locales account for 10% of cases. Ascites and carcinoma-
tosis may be present in as many as 5.4% and 2.6% of cases,
respectively [2].
The female genital system is a common site of second
primary non-mammary malignancies. Specifically, a per-
99 (2005) 65 – 70

R. Garg et al. / Gynecologic Oncology 99 (2005) 65–7066
sonal history of breast cancer is associated with a two to four-
fold increase in the risk of ovarian cancer [3]. In breast
cancer patients, the clinical distinction between recurrent
metastatic breast cancer and a new, second primary ma-
lignancy of the ovary or peritoneum can be difficult. The
clinical relevance of this distinction is predicated on the
disparate management strategies for ovarian/peritoneal
cancer (cytoreductive surgery followed by platinum-based
combination chemotherapy) compared to metastatic breast
cancer (hormonal therapy versus chemotherapy). Conse-
quently, the goals of this study were to: (1) characterize the
etiology of abdominal carcinomatosis in women with a
history of breast cancer, (2) identify clinical features
predictive of primary ovarian/peritoneal cancer, and (3)
evaluate the survival impact of cytoreductive surgery among
patients with advanced ovarian/peritoneal cancer subsequent
to a diagnosis of breast cancer.
Table 1
Demographic characteristics of breast cancer diagnosis
Age at diagnosis
Median 49 years
Mean 49.9 years
Range 25 to 82 years
Postmenopausal 46.8% (37 patients)
AJCC staging
Stage I 62.0%
Stage II 21.5%
Stage III 13.9%
Stage IV 2.5%
Methods
Approval to conduct this study was obtained from the
Johns Hopkins Medical Institutions (JHMI) Clinical
Research Committee and Joint Committee on Clinical
Investigation. All patients with a personal history of primary
breast cancer who subsequently underwent clinical manage-
ment for a diagnosis of abdominal carcinomatosis at the
JHMI between 1/1/88 and 12/31/02 were identified through
the JHMI Tumor Registry, the Kelly Gynecologic Oncology
Service clinical database, and the Department of Pathology
database by a computerized query for diagnoses of recurrent
breast cancer and breast cancer with dual primary sites (i.e. a
second primary malignancy). Of those with dual primary
sites, only patients with a second primary malignancy
diagnosed subsequent to primary breast cancer were selected
for further study. Selection criteria for initial data review also
required adequate clinical documentation of the initial breast
cancer stage of disease and histologic findings; however,
institutional pathologic review of breast cancer specimens
was not required. Finally, an exploratory laparotomy or
diagnostic laparoscopy with definitive pathologic documen-
tation of abdominal carcinomatosis was also required for
study inclusion.
Individual subject data were collected retrospectively
from in-patient and ambulatory medical records. Demo-
graphic data included the date of breast cancer diagnosis,
patient age and menopausal status at breast cancer diag-
nosis, tumor histology, and a family history of breast cancer
in a first-degree relative. American Joint Committee on
Cancer (AJCC) breast cancer stage of disease was assigned
retrospectively using the 2002 modified staging system [4].
With regard to abdominal carcinomatosis, abstracted vari-
ables included the date of diagnosis, patient age and
menopausal status, the interval between breast cancer
diagnosis and abdominal carcinomatosis, clinical presenta-
tion (ascites and carcinomatosis only; ascites and carcino-
matosis plus a pelvic mass; or ascites and carcinomatosis
plus liver metastases, with or without a pelvic mass), and
serum CA125 level when available. Following surgical
exploration and cytoreduction, the amount of residual
disease was considered optimal when the maximal diameter
of the largest residual tumor mass was �1 cm. Patients with
residual disease >1 cm were classified as having undergone
a suboptimal cytoreductive effort. All cases had been
previously reviewed in the multidisciplinary gynecologic
oncology tumor conference, and the specific post-operative
therapy program for each patient was prescribed by the
treating gynecologic oncologist. Surveillance data included
the date of last follow-up and disease status or the date and
cause of death.
For statistical outcomes, logistic regression analysis was
used to identify clinical characteristics predictive of primary
ovarian/peritoneal cancer as the etiology of abdominal
carcinomatosis. For survival analysis, event time distribu-
tions were estimated using the method of Kaplan–Meier,
and survival rates were compared using the Cox propor-
tional hazards model or the log rank test. All computations
were performed using the Statistical Analysis System or
EGRET. A P value of <0.05 was considered statistically
significant, and all P values reported are two-sided [5–10].
Results
Patient characteristics
A total of 1501 patients with a history of recurrent breast
cancer (n = 1274) or breast cancer with another primary site
of malignancy (n = 227) were identified through the JHMI
databases during the study interval. Of these, 79 patients
were documented as presenting with abdominal carcinoma-
tosis �30 days subsequent to the diagnosis of primary breast
cancer. The demographic characteristics of patients with
breast cancer diagnosis are shown in Table 1.
The median patient age at breast cancer diagnosis was
49 years (mean 49.9 years, range 25 to 82 years), with
37 patients (46.8%) being post-menopausal. According to
AJCC criteria, the stage distribution of breast cancer was
as follows: Stage I—62.0%, Stage II—21.5%, Stage

Table 2
Clinical characteristics associated with abdominal carcinomatosis due to
primary ovarian/peritoneal cancer versus recurrent breast cancer
Variable Odds
ratio
95%CIa Significance
( P)
Univariate logistic regression
Age at breast cancer 0.99 0.94–1.03 0.480
Family history breast cancerb 1.09 0.37–3.21 0.880
AJCC Stage I breast cancer 7.70 2.39–24.81 0.001
Postmenopausal breast cancer 0.74 0.26–2.07 0.560
Postmenopausal carcinomatosis 1.79 0.52–6.09 0.350
No prior breast cancer recurrence 7.22 2.25–23.23 0.001
Breast cancer pathologyc 1.19 0.33–4.28 0.790
Age at abdominal carcinomatosis 1.01 0.97–1.05 0.690
Breast cancer/carcinomatosis
interval
1.00 1.00–1.00 0.150
Abdominal presentationd 0.69 0.23–2.07 0.510
CA125e 1.37 0.89–2.08 0.150
Multivariate logistic regression
AJCC Stage I breast cancer 10.73 2.60–43.70 0.001
No prior breast cancer recurrence 10.60 2.50–45.20 0.001
a CI: Confidence Interval.b In a first-degree relative.c Infiltrating ductal carcinoma versus all others.d Isolated carcinomatosis and ascites versus pelvic mass or liver
metastases.e Log CA125.
R. Garg et al. / Gynecologic Oncology 99 (2005) 65–70 67
III—13.9%, and Stage IV—2.5%. Breast cancer pathology
was: infiltrating ductal carcinoma in 64 patients (81.0%),
lobular carcinoma in 12 patients (15.2%), serous adenocar-
cinoma in 1 patient (1.3%), medullary carcinoma in 1 patient
(1.3%), and papillary adenocarcinoma in 1 patient (1.3%).
Eighteen patients (22.8%) had experienced a non-abdominal
recurrence of breast cancer prior to diagnosis of abdominal
carcinomatosis.
The median age at diagnosis of abdominal carcinoma-
tosis was 58 years (mean 58.3 years, range 33 to 82 years),
with a median interval of 5.39 years (mean 8.47 years, range
0.10 to 33.55 years) between breast cancer diagnosis and
presentation with abdominal carcinomatosis. All patients
presented with ascites and abdominal carcinomatosis that
was confirmed radiographically (computed tomography,
magnetic resonance imaging, or positron emission tomo-
graphy). Thirty patients (37.9%) presented with abdominal
carcinomatosis and ascites as isolated findings. Forty-five
patients (57.0%) had concomitant pelvic mass in addition to
ascites and carcinomatosis, while 4 patients (5.1%) also had
liver metastases with or without a pelvic mass. The majority
of patients (81.0%) were post-menopausal at the time of
abdominal carcinomatosis presentation. Serum CA125
levels were available in 53 of 79 cases and yielded a
median value of 572 U/ml (mean 1445 U/ml, range 20 to
14,000 U/ml).
Overall, 54 patients (68.4%) were diagnosed with
primary ovarian cancer and 5 patients (6.3%) were
diagnosed with primary peritoneal cancer. In total, therefore,
primary ovarian/peritoneal cancer accounted for 74.7% of
all cases of abdominal carcinomatosis in women with a prior
history of breast cancer. Of these 59 patients, 7 (11.9%) had
FIGO Stage IIIB disease, 41 (69.5%) had FIGO Stage IIIC
disease, and 11 (18.6%) had FIGO Stage IV disease.
Histopathologically, 98.3% of these cases were epithelial
tumors (serous carcinoma, n = 47; mixed serous and
endometrioid carcinoma, n = 4; micropapillary serous
carcinoma with invasive implants, n = 3; clear cell
carcinoma, n = 3; endometrioid carcinoma, n = 1; serous
borderline tumor with non-invasive implants, n = 1), and
there was 1 case of a granulosa cell tumor. Eight out of 59
patients (13.6%) had a family history of ovarian cancer
whereas 29 patients (49%) had a family history of breast
cancer.
Recurrent breast cancer accounted for 19 cases (24.0%)
of abdominal carcinomatosis. Majority (10 patients i.e.
52.6%) had a family history of breast cancer with none
who reported a known family history of ovarian cancer
among this group of patients. Of the 18 patients with a
prior breast cancer recurrence, abdominal carcinomatosis
was due to a second recurrence of breast cancer in 9
patients (50%). Conversely, of the 19 patients with
recurrent breast cancer as the cause of abdominal
carcinomatosis, 9 patients (47.4%) had experienced a prior
recurrence of breast cancer (in other words, abdominal
carcinomatosis was their second breast cancer recurrence).
One patient (1.3%) had primary FIGO Stage IVB uterine
papillary serous carcinoma.
Predictors of primary ovarian/peritoneal cancer
Multivariate logistic regression analysis of demographic
and clinical variables revealed that only AJCC Stage I breast
cancer (odds ratio [OR] = 10.73, 95% confidence interval
[95%CI] = 2.6–43.7, P = 0.001) and the absence of a prior
breast cancer recurrence (OR=10.60, 95%CI = 2.5–45.2,P =
0.001) were independently and statistically significantly
associated with a diagnosis of primary ovarian/peritoneal
cancer versus recurrent breast cancer (Table 2).
Although not statistically significant, the interval
between breast cancer diagnosis and abdominal carcinoma-
tosis for patients with primary ovarian/peritoneal cancer
was notably longer (median 7.06 years, mean 9.37 years,
range 0.10 to 33.55 years) compared to patients with
recurrent breast cancer (median 3.00 years, mean 6.02
years, range 0.27 to 28.68 years). Serum CA125 levels
were available for 36/59 patients with primary ovarian/
peritoneal cancer and 16/19 patients with recurrent breast
cancer. There was a trend, although again not statistically
significant, toward higher serum CA125 levels in patients
with primary ovarian/peritoneal cancer (median 683 U/ml,
mean 1809.6 U/ml, range 20 to 14000 U/ml) compared to
patients with recurrent breast cancer (median 350 U/ml,
mean 709.2 U/ml, range 24 to 2617 U/ml).

R. Garg et al. / Gynecologic Oncology 99 (2005) 65–7068
Surgical outcome and survival analysis
All patients underwent a minimum of exploratory
laparotomy or diagnostic laparoscopy with tissue biopsy,
which was the only procedure performed in 9 cases.
Additional procedures were performed with the following
frequencies: unilateral or bilateral salpingo-oophorectomy
(n = 68), omentectomy or omental biopsy (n = 59), total or
supracervical hysterectomy (n = 54), tumor cytoreduction
(n = 43), retroperitoneal lymph node sampling (n = 39),
small bowel resection (n = 11), large bowl resection (n = 5).
For the 59 patients with primary ovarian/peritoneal
cancer, optimal cytoreduction was achieved in 33 cases
(55.9%), while suboptimal residual disease was left in 26
cases (44.1%). Fifty-five patients (93.2%) received plati-
num-based chemotherapy post-operatively, either alone or
in combination with a variety of other agents (cyclo-
phosphamide, adriamycin, paclitaxel, topotecan). The
median follow-up for patients with primary ovarian/
peritoneal cancer was 51.6 months and the median survival
time was 30.0 months. At last follow-up, 49 of 59 patients
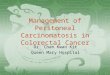
(83.1%) were dead of disease. The median survival time for
patients undergoing optimal cytoreduction was 44.0 months,
compared to 18.0 months for patients left with suboptimal
residual disease (hazard ratio [HR] = 6.81, 95%CI = 3.37–
13.77, P < 0.001) (Fig. 1). Among patients with primary
ovarian/peritoneal cancer, 19 (32.2%) had no gross residual
disease, 14 (23.7%) had visible disease �1 cm, and 26
(44.1%) had suboptimal residual disease. The median
survival times according to residual disease were: micro-
scopic (no gross) residual 82.0 months, optimal (0.1 to 1.0
cm) but visible 33.0 months (HR 10.07, 95%CI 3.24–31.26,
P = 0.0001), and for suboptimal (>1.0 cm) residual disease
Fig. 1. Primary ovarian/peritoneal cancer survival outcome by post-
operative residual disease for 59 patients.
18.0 months (HR 26.37, 95%CI 8.30–83.74, P < 0.0001).
All 10 long-term (�5 years) surviving patients had no
visible residual disease.
Of the 19 patients with recurrent breast cancer, 5
underwent optimal cytoreductive surgery and experienced
a median survival time of 34.4 months compared to 3.9
months for the 14 patients left with suboptimal residual
disease (P = 0.001, log rank test). The median follow-up
time for these patients was 16.0 months.
Discussion
Breast cancer and ovarian cancer rank as the second and
fifth leading causes of cancer-related death, respectively,
among United States women [1]. One in eight women will
have breast cancer during their lifetimes and one in 70 will be
diagnosed with ovarian cancer [3]. Currently, about half of
all patients with a diagnosis of breast cancer will experience
a recurrence and one third will die of their disease [11].
Several factors may predispose a patient to develop both
breast cancer and ovarian cancer: (1) breast–ovarian cancers
(BOC) family syndrome and/or BRCA mutations, (2)
relatively high incidence of both breast cancer and ovarian
cancer, (3) similar risk factors for both cancers including age,
family history, reproductive and menstrual history along
with estrogen exposure [1,3]. We attempted to determine the
clinical, demographic, and etiologic features of women who
present with abdominal carcinomatosis with a history of
breast cancer. The clinical relevance being that the treatments
of these two entities are dramatically different. Curtin et al.
[12] reported on 121 women with a history of breast cancer
who underwent surgery for an adnexal or pelvic mass. A
benign process was discovered in 50% of cases. The
remaining patients were found to have a malignant process
as the etiology of the adnexal mass, with new ovarian or
fallopian tube primary malignancies accounting for 73%
cases; metastatic breast cancer was the cause of the adnexal
mass in 27% of patients. In other words, a new gynecologic
primary malignancy predominated over metastatic breast
cancer in a ratio of 3:1 in the setting of a pelvic mass
following a diagnosis of primary breast cancer. This
distinction is clinically important because the likelihood of
a non-ovarian metastatic tumor being the source of a
malignant ovarian neoplasm ranges between 3 and 37%.
Breast cancer is one of the common non-genital tumors to
metastasize to the ovary. Women with metastatic breast
cancer to the ovary have been reported to have a poor
prognosis, with a 5-year survival rate of 0–10% [13–16].
The reported survival time subsequent to the manifestation
of metastatic disease is approximately 3 years [11].
In 1997, Abu-Rustum et al. reported on 40 patients with
breast cancer and metachronous abdominal and/or pelvic
metastases. The median interval between breast cancer
diagnosis and surgical exploration was 80 months. The
median survival for all patients was 24.1 months. Patients

R. Garg et al. / Gynecologic Oncology 99 (2005) 65–70 69
left with no gross residual disease survived longer than
those with gross residual disease, although the difference
was not statistically significant. Eighty-five percent of
patients had infiltrating ductal carcinoma, 15% had invasive
lobular carcinoma. In addition, 45% of patients had
previously documented metastatic breast cancer to other
sites, a finding confirmed by the 47.4% rate observed in the
current study [17].
Eitan et al., in 2003, reported on 59 women with
metastatic breast cancer to the abdomen and pelvis, re-
examining the role of surgical resection as an update to the
report of Abu-Rustum et al. Exploratory surgery was
performed a median of 5 years after initial diagnosis of
breast cancer, with median survival time of 23 months from
the diagnosis of abdominal disease. Suboptimal residual
disease was significantly associated with an increased risk
of death due to disease [18]. Primary surgery with optimal
cytoreduction for advanced-stage ovarian cancer has con-
sistently been associated with a clinically and statistically
significant survival advantage compared to patients left with
large-volume residual disease [19]. Our data confirm the
positive impact on survival of optimal cytroreductive
surgery for patients with primary ovarian/peritoneal cancer
and further suggest that survival time is inversely propor-
tional to the volume of residual tumor.
Among patients with prior breast cancer presenting with
abdominal carcinomatosis, early-stage disease and the
absence of a prior recurrence were the only clinico-
pathological factors significantly associated with a diagnosis
of primary ovarian/peritoneal cancer, which accounted for
the majority of cases. Although not statistically significant,
there was a trend noted for a shorter interval until the
diagnosis of abdominal disease to be more likely recurrent
breast cancer, and higher CA125 levels to be more
predictive of primary ovarian/peritoneal disease. Interest-
ingly, optimal cytoreduction was associated with a signifi-
cant extension in median survival time (34.4 months)
compared to patients left with bulky residual disease (3.9
months, P = 0.001); however, the number of patients is too
small to reach definitive conclusions about the role of
cytoreductive surgery in this setting.
There are several limitations of the current study that must
be considered in interpreting the results. As with all
retrospective studies, the potential for selection bias must
be acknowledged. In an attempt to minimize such bias, study
selection criteria were strictly maintained. Furthermore, the
lack of all potentially clinically relevant factors in each
patient medical record is another limitation of a retrospective
study. Specifically, the inadequate data with regard to the
genetic history/family history of individual patients, BRCA
mutation data, tumor markers and specific laboratory values
if normal or elevated, ER/PR data. Secondly, the relatively
long time interval necessary to accrue a satisfactory number
of subjects may have introduced a component of potential
treatment bias. In other words, observed survival differences
may have been effected by the evolution of treatment
regimens over time. A third potentially confounding factor
may be the subjective nature of the designation of optimal
residual disease and the completeness of surgical resection,
as defined in medical records by individual surgeons.
Finally, given the nature of our practice as a tertiary referral
center, it was impossible to evaluate the true incidence of
abdominal carcinomatosis arising after a diagnosis of breast
cancer.
In conclusion, our data indicate that the majority of
women presenting with abdominal carcinomatosis after a
diagnosis of breast cancer will have a new primary ovarian
cancer or primary peritoneal cancer. We were unable to
identify reliable predictors of recurrent breast cancer as the
etiology of abdominal carcinomatosis that would preclude
exploratory surgery for diagnostic and therapeutic purposes.
Given the significant survival advantage associated with
optimal residual disease for patients with a primary ovarian/
peritoneal cancer, an attempt at maximal cytoreductive
surgery is warranted for most patients with this clinical
presentation.
References
[1] American Cancer Society. Cancer facts and figures: American Cancer
Society, IncR; 2003 [Available at http://www.cancer.org/downloads/
stt/caff2003pwsecured.pdf ].
[2] Caskey CI, Scatarige JC, Fishman EK. Distribution of metastases in
breast carcinoma: CT evaluation of abdomen. Clin Imaging 1991;
15(3):166–71.
[3] National Cancer Institute, National Institutes of Health. Genetics of
breast and ovarian cancer; 2004 [Available at http://www.cancer.gov/
cancerinfo/pdq/genetics/breast-and-ovarian].
[4] AJCC (American Joint Committee on Cancer). In: Greene FL, Page
DL, Fleming ID, et al, editors. Cancer staging manual. 6th ed. New
York’ Springer-Verlag; 2002. p. 223–40.[5] Melfi C, Holleman E, Arthur D, Katz B. Selecting a patient
characteristics index for prediction of medical outcomes using
administrative claims data. J Clin Epidemiol 1995;48:917–26.
[6] Kaplan EL, Meier P. Nonparametric estimation from incomplete
observations. J Am Stat Assoc 1958;53:457–80.
[7] Mantel N, Haenszel W. Statistical aspects of the analysis of data from
retrospective studies of disease. J Natl Cancer Inst 1959;22:719–748.
[8] Cox DR. The analysis of binary data. London’ Methuen; 1970.
[9] SAS Institute Inc. SAS user’s guide: statistics. Version 5 Edition. Cary,
NC: SAS Institute Inc; 1985.
[10] Statistics and Epidemiology Research Corporation. EGRET user’s
manual. Seattle, WA: Statistics and Epidemiology Research Corpo-
ration; 1988.
[11] Winer EP, Morrow M, Osbome CK, Harris JR. Malignant tumors of
the breast. In: DeVita VT, Hellman S, Rosenberg SA, editors. Cancer:
principles and practice of oncology. 6th ed. Baltimore’ Lippincott
Williams and Wilkins; 2001. p. 1651–706.
[12] Curtin JP, Barakat RR, Hoskins WJ. Ovarian disease in women with
breast cancer. Obstet Gynecol 1994;84:449–52.
[13] Ayhan A, Tuncer S, Bukulmez O. Malignant tumors metastatic to the
ovaries. J Surg Oncol 1995;60:268–76.
[14] Ulbright TM, Roth LM, Stehman FB. Secondary ovarian neoplasia.
Cancer 1984;53:1164–74.
[15] Webb MJ, Decker DG, Mussey E. Cancer metastatic to the ovary-
factors influencing survival. Obstet Gynecol 1975;45:391–6.
[16] Petru E, Pickel H, Heydarfadai M, Lahousen M, Hass J, Schaider H,

R. Garg et al. / Gynecologic Oncology 99 (2005) 65–7070
et al. Nongenital cancers metastatic to the ovary. Gynecol Oncol
1992;44:83–6.
[17] Abu-Rustum NR, Aghajanian CA, Venkatraman ES, Feroz F, Barakat
RR. Metastatic breast carcinoma to the abdomen and pelvis. Gynecol
Oncol 1997;66:41–4.
[18] Eitan R, Gemignani ML, Venkatraman ES, Barakat RR, Abu-Rustum
NR. Breast cancer metastatic to abdomen and pelvis: role of surgical
resection. Gynecol Oncol 2003;90:397–401.
[19] Munstedt K, Franke FE. Role of primary surgery in advanced ovarian
cancer. World J Surg Oncol 2004;2:32–40.