Embed Size (px)
Citation preview

Received: 27 February 2004Revised: 3 August 2004Accepted: 23 August 2004Published online: 16 October 2004© Springer-Verlag 2004
Abstract The study describes theapplication of a web-based soft-ware in the planning of the endovas-cular treatment of abdominal aorticaneurysms (AAA). The software has been developed in the frame-work of a 2-year research projectcalled Aneurysm QUAntificationThrough an Internet CollaborativeSystem (AQUATICS); it allows tomanage remotely Virtual RealityModeling Language (VRML) modelsof the abdominal aorta, derived frommultirow computed tomography angiography (CTA) data sets, and toobtain measurements of diameters,angles and centerline lengths. To test the reliability of measurements,two radiologists performed a detailedanalysis of multiple 3D models generated from a synthetic phantom,mimicking an AAA. The system was tested on 30 patients with AAA;
CTA data sets were mailed and thetime required for segmentation andmeasurement were collected for each case. The Bland-Altman plotanalysis showed that the mean intra-and inter-observer differences inmeasures on phantoms were clini-cally acceptable. The mean time required for segmentation was 1 h(range 45–120 min). The mean timerequired for measurements on theweb was 7 min (range 4–11 min).The AQUATICS web server mayprovide a rapid, standardized and accurate tool for the evaluation ofAAA prior to the endovascular treat-ment.
Keywords Abdominal aortic aneurysm · Computed tomographyangiography post-processing · Endoluminal aneurysm repair · Internet
Eur Radiol (2005) 15:348–352DOI 10.1007/s00330-004-2500-4 VA S C U L A R - I N T E RV E N T I O N A L
Emanuele NeriIrene BargelliniMichael RiegerAndrea GiachettiClaudio VignaliMassimiliano TuveriWerner JaschkeCarlo Bartolozzi
Abdominal aortic aneurysms: virtual imagingand analysis through a remote web server
Introduction
The current standard treatment for abdominal aortic aneurysm (AAA) in patients without substantial comor-bidities is elective open surgical repair. Since the originalclinical report by Parodi et al. [1] in 1991, endovascularrepair of AAA has gained popularity worldwide as a lessinvasive alternative to conventional surgery [2, 3].
To be considered candidates for endovascular repair,patients must meet certain anatomic criteria, regarding,for example, proximal and distal necks lengths, diame-ters and angulations. Preprocedural measurements aretherefore required for the selection of the appropriatestent-graft to minimize the most common complications
of endovascular repair of AAA, such as endoleak andkinking resulting in graft thrombosis [4–7].
The most accurate imaging technique used to evalu-ated AAA is computed tomography angiography (CTA)[8–12]. Raw data can be effectively post-processed onindependent workstations, obtaining 2D and 3D recon-structions, such as multiplanar reformations (MPRs),maximum intensity projections (MIPs), volume render-ings (VRs) and curved planar reformations (CPRs),which allow accurate length measurements of curvedstructures [9].
Nevertheless, image post-processing is time consum-ing, requires experienced operators and may imply con-siderable intra- and inter-observer errors. Therefore, a
E. Neri (✉) · I. Bargellini · C. VignaliC. BartolozziDiagnostic and Interventional Radiology,Department of Oncology, Transplants, and Advanced Technologies in Medicine,University of Pisa,Via Roma 67, 56100 Pisa, Italye-mail: [email protected].: +39-50-993560Fax: +39-50-993560
M. Rieger · W. JaschkeDiagnostic and Interventional Radiology,University of Innsbruck,Innsbruck, Austria
A. Giachetti · M. TuveriCenter for Research and Study,Sardinia, Italy
349
more rapid and reproducible system is desirable, with theuse of a standard approach, reducing operator variability.
In the framework of a project funded by the EuropeanUnion called Aneurysm QUAntification Through an Internet Collaborative System (AQUATICS; Project ISTIST-1999-20226 EUTIST-M), we developed a web-basedapplication for the planning of endovascular treatment ofAAA. The study describes the system and its application.
Materials and methods
AQUATICS system configuration
The web-based application was based on a client-server architec-ture, where the central node is a Web server, a Database server, aDICOM image server and a DICOM structured report server.
The usual work-flow starts by sending DICOM CTA data to aDICOM image server located in a specialized remote reconstruc-tion center. These data are processed by a team composed by a radiologist and two engineers, working on a PC with a segmenta-tion/conversion module. The reconstruction ends with the genera-tion of a Virtual Reality Modeling Language (VRML) model in-cluding the abdominal aorta surface geometry, the centerline, ahidden eXtended Mark-up Language (XML) file containing all thepatient and acquisition data and a Javascript code to support usermeasurements.
The heart of the measurement and model distribution system isthe Database/Web server. It is based on the following open sourcepackages: database MySql 3.23 (MySQL AB, Sweden), Apacheweb server (Apache Digital Corporation, Durango, Colorado) withPHP programming language for data processing and web pages dis-tribution and Mallinckrodt Central Test Node 3.04 (Mallinckrodt Institute of Radiology, Washington University, St Louis, Mo.) asDICOM server for images.
Web pages are realized in PHP, allowing the search of imagesand VRML models from patient’s names and ID’s. The databasecan be accessed remotely by the radiologists who sent the raw CTAdata to the reconstruction center. For security issues, patient data areanonymous, and the access is regulated by codes and passwords.
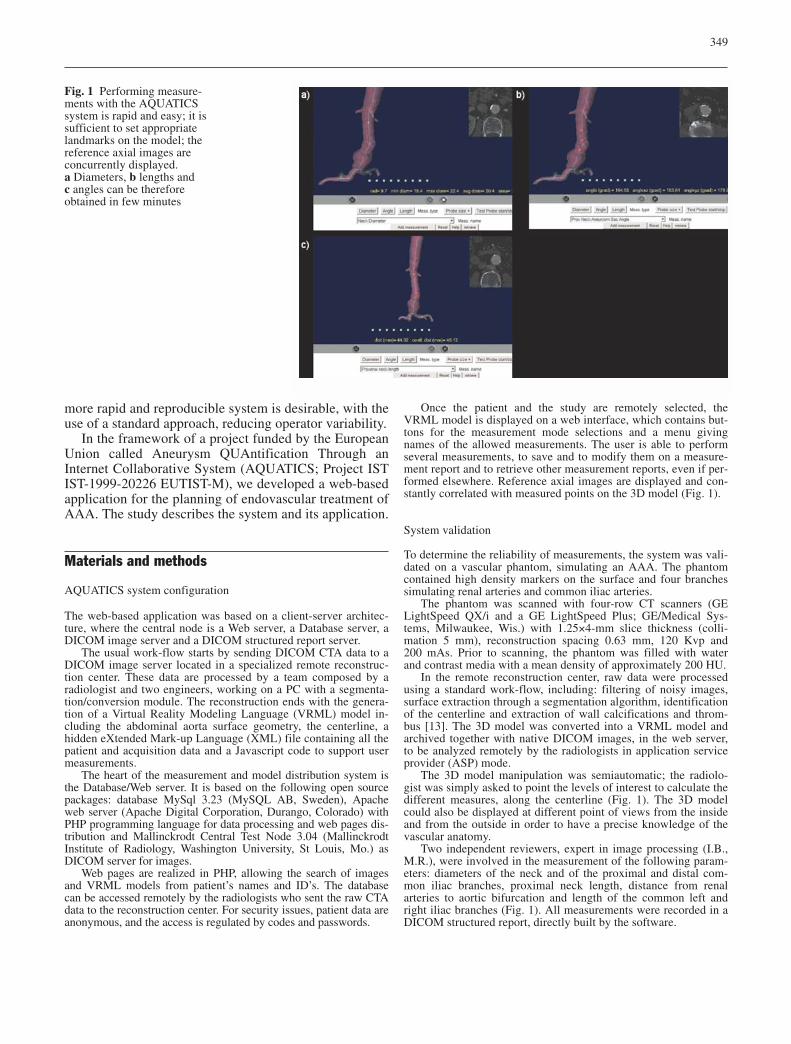
Once the patient and the study are remotely selected, theVRML model is displayed on a web interface, which contains but-tons for the measurement mode selections and a menu givingnames of the allowed measurements. The user is able to performseveral measurements, to save and to modify them on a measure-ment report and to retrieve other measurement reports, even if per-formed elsewhere. Reference axial images are displayed and con-stantly correlated with measured points on the 3D model (Fig. 1).
System validation
To determine the reliability of measurements, the system was vali-dated on a vascular phantom, simulating an AAA. The phantomcontained high density markers on the surface and four branchessimulating renal arteries and common iliac arteries.
The phantom was scanned with four-row CT scanners (GELightSpeed QX/i and a GE LightSpeed Plus; GE/Medical Sys-tems, Milwaukee, Wis.) with 1.25×4-mm slice thickness (colli-mation 5 mm), reconstruction spacing 0.63 mm, 120 Kvp and200 mAs. Prior to scanning, the phantom was filled with waterand contrast media with a mean density of approximately 200 HU.
In the remote reconstruction center, raw data were processedusing a standard work-flow, including: filtering of noisy images,surface extraction through a segmentation algorithm, identificationof the centerline and extraction of wall calcifications and throm-bus [13]. The 3D model was converted into a VRML model andarchived together with native DICOM images, in the web server,to be analyzed remotely by the radiologists in application serviceprovider (ASP) mode.
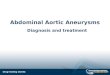
The 3D model manipulation was semiautomatic; the radiolo-gist was simply asked to point the levels of interest to calculate thedifferent measures, along the centerline (Fig. 1). The 3D modelcould also be displayed at different point of views from the insideand from the outside in order to have a precise knowledge of thevascular anatomy.
Two independent reviewers, expert in image processing (I.B.,M.R.), were involved in the measurement of the following param-eters: diameters of the neck and of the proximal and distal com-mon iliac branches, proximal neck length, distance from renal arteries to aortic bifurcation and length of the common left andright iliac branches (Fig. 1). All measurements were recorded in aDICOM structured report, directly built by the software.
Fig. 1 Performing measure-ments with the AQUATICSsystem is rapid and easy; it issufficient to set appropriatelandmarks on the model; thereference axial images are concurrently displayed. a Diameters, b lengths and c angles can be therefore obtained in few minutes
350
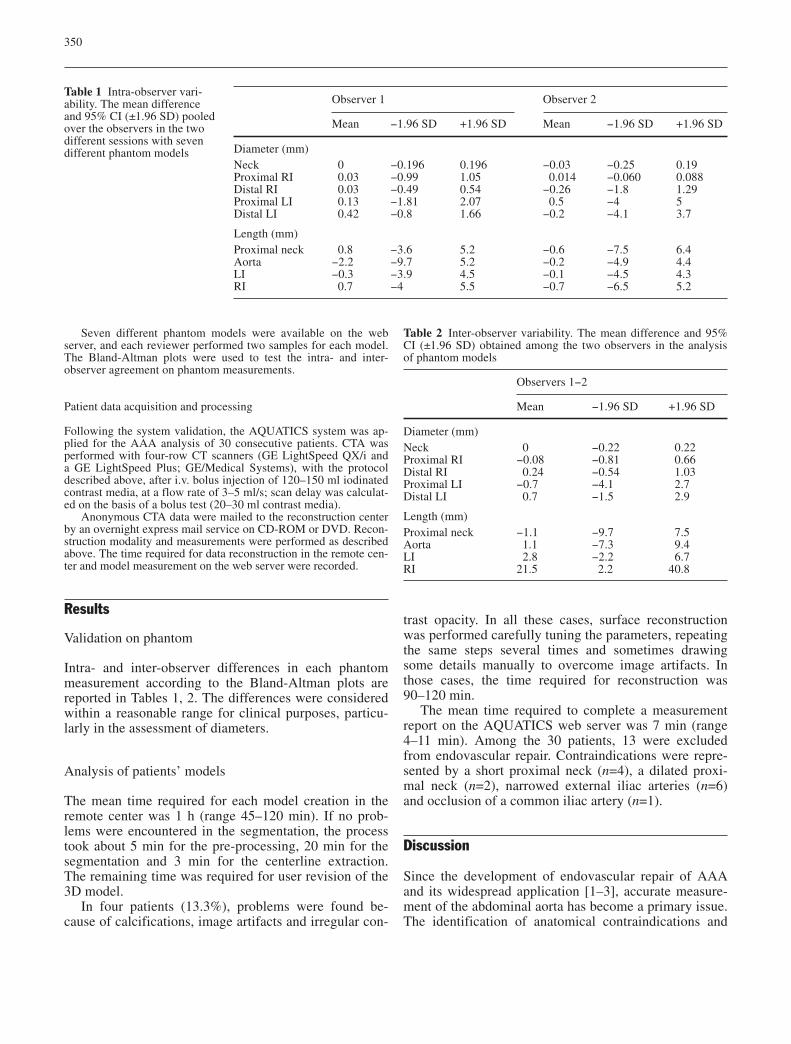
Seven different phantom models were available on the webserver, and each reviewer performed two samples for each model.The Bland-Altman plots were used to test the intra- and inter-observer agreement on phantom measurements.
Patient data acquisition and processing
Following the system validation, the AQUATICS system was ap-plied for the AAA analysis of 30 consecutive patients. CTA wasperformed with four-row CT scanners (GE LightSpeed QX/i and a GE LightSpeed Plus; GE/Medical Systems), with the protocoldescribed above, after i.v. bolus injection of 120–150 ml iodinatedcontrast media, at a flow rate of 3–5 ml/s; scan delay was calculat-ed on the basis of a bolus test (20–30 ml contrast media).
Anonymous CTA data were mailed to the reconstruction centerby an overnight express mail service on CD-ROM or DVD. Recon-struction modality and measurements were performed as describedabove. The time required for data reconstruction in the remote cen-ter and model measurement on the web server were recorded.
Results
Validation on phantom
Intra- and inter-observer differences in each phantommeasurement according to the Bland-Altman plots arereported in Tables 1, 2. The differences were consideredwithin a reasonable range for clinical purposes, particu-larly in the assessment of diameters.
Analysis of patients’ models
The mean time required for each model creation in theremote center was 1 h (range 45–120 min). If no prob-lems were encountered in the segmentation, the processtook about 5 min for the pre-processing, 20 min for thesegmentation and 3 min for the centerline extraction.The remaining time was required for user revision of the3D model.
In four patients (13.3%), problems were found be-cause of calcifications, image artifacts and irregular con-
trast opacity. In all these cases, surface reconstructionwas performed carefully tuning the parameters, repeatingthe same steps several times and sometimes drawingsome details manually to overcome image artifacts. Inthose cases, the time required for reconstruction was90–120 min.
The mean time required to complete a measurementreport on the AQUATICS web server was 7 min (range4–11 min). Among the 30 patients, 13 were excludedfrom endovascular repair. Contraindications were repre-sented by a short proximal neck (n=4), a dilated proxi-mal neck (n=2), narrowed external iliac arteries (n=6)and occlusion of a common iliac artery (n=1).
Discussion
Since the development of endovascular repair of AAAand its widespread application [1–3], accurate measure-ment of the abdominal aorta has become a primary issue.The identification of anatomical contraindications and
Table 1 Intra-observer vari-ability. The mean differenceand 95% CI (±1.96 SD) pooledover the observers in the twodifferent sessions with sevendifferent phantom models
Observer 1 Observer 2
Mean −1.96 SD +1.96 SD Mean −1.96 SD +1.96 SD
Diameter (mm)Neck 0 −0.196 0.196 −0.03 −0.25 0.19Proximal RI 0.03 −0.99 1.05 0.014 −0.060 0.088Distal RI 0.03 −0.49 0.54 −0.26 −1.8 1.29Proximal LI 0.13 −1.81 2.07 0.5 −4 5Distal LI 0.42 −0.8 1.66 −0.2 −4.1 3.7
Length (mm)Proximal neck 0.8 −3.6 5.2 −0.6 −7.5 6.4Aorta −2.2 −9.7 5.2 −0.2 −4.9 4.4LI −0.3 −3.9 4.5 −0.1 −4.5 4.3RI 0.7 −4 5.5 −0.7 −6.5 5.2
Table 2 Inter-observer variability. The mean difference and 95%CI (±1.96 SD) obtained among the two observers in the analysisof phantom models
Observers 1−2
Mean −1.96 SD +1.96 SD
Diameter (mm)Neck 0 −0.22 0.22Proximal RI −0.08 −0.81 0.66Distal RI 0.24 −0.54 1.03Proximal LI −0.7 −4.1 2.7Distal LI 0.7 −1.5 2.9
Length (mm)Proximal neck −1.1 −9.7 7.5Aorta 1.1 −7.3 9.4LI 2.8 −2.2 6.7RI 21.5 2.2 40.8

351
the selection of the proper stent-graft are of outmost importance to determine early and mid-term outcomes[6–9]. Vessel diameters can be accurately calculated bymagnified digital images perpendicular to the lumen centerline [14–17], whereas lengths should be calculatedeither along the centerline of the aortic lumen usingCPRs [9, 18] or, as proposed by Tillich et al. [19], alongthe shortest aorto-iliac path, to better predict stent-graftlength. Finally, angles should be obtained by using 3Dreconstructions of the aorta.
Several semiautomatic software tools have been re-cently developed, which enable rapid, consistent and repeatable quantitative analysis of 3D CTA/MRA data[20–23]. The software automatically detects the vesselcenterline and computes the cross section area and themean and minimum diameters at each point, perpendicu-lar to the lumen centerline. To produce a report, the usermarks characteristic landmarks on the 3D model, such as start and end of an aneurysm, position of supplied/supplying vessels, bifurcations, etc. Nevertheless, thesesoftwares are not widely available and require powerfulhardware local resources.
Differently to the actual approaches to aneurysm anal-ysis, the aim of the AQUATICS service is to provide apowerful system available for multiple users who exploitthe potential of the Internet by accessing to a centralserver through a simple PC. Thus, there is no need forspecific and costly equipment.
Moreover, the system provides a standardized methodto obtain all the required measurements and to identifycontraindications to endovascular treatment. Physicianscan access the system and obtain all the required datawith no need for advanced training in 3D vascular post-processing specifically for endovascular repair. Since
image post-processing is performed remotely by selectedand dedicated operators, the web-based system mini-mizes the time of interaction for the radiologist or physi-cian [13], obtaining measurements in less than 10 min.
The use of a DICOM structured measurement reportallows the export of the collected data in the DICOM environment (i.e., to remote clinicians). The system validation demonstrated the high accuracy of measure-ments, with an acceptable mean intra- and inter-observerdifference. Accuracy could be improved by using more powerful multirow CT scanners, increasing contrastopacity and reducing image artifacts, which would alsoreduce the time required for segmentation.
However, this could result in an increased time fordata transmission. Data transmission represents an is-sue. The system is configured so as to obtain data se-curely over a telephone line; by now, this process re-quires time and a high-flow web connection. The alter-native is represented by data transportation through CD-ROM or DVD using an efficient overnight express mailservice.
The AQUATICS system represents a step forward inthe management of CTA post-processing for endovascu-lar treatment planning of AAA. It is a user-friendly sys-tem, is efficient and secure, and is based on standard pro-tocols and open software. Each component can be inde-pendently updated or replaced, maintaining the workingof the system. This allows the modification of the work-flow according to the physician’s needs and also the re-use of most of the system components for other applica-tions.
Being web-based, it will be widely available, and itwould allow a specialized AAA analysis, even in thosefacilities where such resources are not available.
References
1. Parodi JC, Palmaz JC, Barone HD(1991) Transfemoral intraluminal graftimplantation for abdominal aorticaneurysms. Ann Vasc Surg 5:491–499
2. D’Ayala M, Hollier LH, Marin ML(1998) Endovascular grafting for abdominal aortic aneurysms. Surg Clin North Am 78:845–862
3. Moore WS, Rutherford RB (1996)Transfemoral endovascular repair ofabdominal aortic aneurysm: results ofthe North American EVT phase 1 trial.EVT Investigators. J Vasc Surg23:543–553
4. May J, White GH, Yu W, Waugh RC,Stephen MS, Harris JP (1996) Resultsof endoluminal grafting of abdominalaortic aneurysms are dependent on aneurysm morphology. Ann Vasc Surg10(3):254–261
5. Tillich M, Bell RE, Paik DS et al(2001) Iliac arterial injuries after endovascular repair of abdominal aortic aneurysms: correlation with iliaccurvature and diameter. Radiology219(1):129–136
6. Hovsepian DM, Hein AN, Pilgram TKet al (2001) Endovascular abdominalaortic aneurysm repair in 144 patients:correlation of aneurysm size, proximal aortic neck length, and procedure-related complications. J Vasc Interv Radiol 12(12):1373–1382
7. Wolf YG, Tillich M, Lee WA, RubinGD, Fogarty TJ, Zarins CK (2001) Impact of aortoiliac tortuosity on en-dovascular repair of abdominal aorticaneurysms: evaluation of 3D computer-based assessment. J Vasc Surg34(4):594–599
8. Gomes MN, Davros WJ, Zeman RK(1994) Preoperative assessment of abdominal aortic aneurysm: the valueof helical and three-dimensional com-puted tomography. J Vasc Surg20(3):367–375

352
9. Broeders IA, Blankensteijn JD, Olree M, Mali W, Eikelboom BC(1997) Preoperative sizing of grafts fortransfemoral endovascular aneurysmmanagement: a prospective compara-tive study of spiral CT angiography, arteriography, and conventional CT imaging. J Endovasc Surg 4(3):252–261
10. Broeders IA, Blankensteijn JD (1999)Preoperative imaging of the aortoiliacanatomy in endovascular aneurysmsurgery. Semin Vasc Surg 12(4):306–314
11. Armon MP, Whitaker SC, Gregson RH,Wenham PW, Hopkinson BR (1998)Spiral CT angiography versus aortography in the assessment of aortoiliac length in patients under-going endovascular abdominal aorticaneurysm repair. J Endovasc Surg5(3):222–227
12. Beebe HG, Kritpracha B, Serres S, Pigott JP, Price CI, Williams DM(2000) Endograft planning without preoperative arteriography: a clinicalfeasibility study. J Endovasc Ther7(1):8–15
13. Giachetti A, Tuveri M, Zanetti G(2003) Reconstruction and web distri-bution of measurable arterial models.Med Image Anal 7(1):79–93
14. Kritpracha B, Wolfe J, Beebe HG(2002) CT artifacts of the proximalaortic neck: an important problem inendograft planning. J Endovasc Ther9(1):103–110
15. Fillinger MF (1999) New imagingtechniques in endovascular surgery.Surg Clin North Am 79:451–475
16. Fillinger MF (2001) Computed tomographic scanning. In: Moore WS,Ahn SA (eds) Endovascular surgery,3rd edn. Saunders, Philadelphia, pp 114–124
17. Abada HT, Sapoval MR, Paul JF, de Maertelaer V, Mousseaux E, Gaux JC (2003) Aneurysmal sizing after endovascular repair in patientswith abdominal aortic aneurysm: interobserver variability of variousmeasurement protocols and its clinicalrelevance. Eur Radiol 13(12):2699–2704
18. Rubin GD, Paik DS, Johnston PC,Napel S (1998) Measurement of theaorta and its branches with helical CT.Radiology 206(3):823–829
19. Tillich M, Hill BB, Paik DS et al(2001) Prediction of aortoiliac stent-graft length: comparison of measure-ment methods. Radiology 220:475–483
20. Lutz AM, Willmann JK, Pfammatter Tet al (2003) Evaluation of aortoiliac aneurysm before endovascular repair:comparison of contrast-enhanced magnetic resonance angiography withmultidetector row computed tomo-graphic angiography with an automatedanalysis software tool. J Vasc Surg37(3):619–627
21. Aziz I, Lee J, Lee JT et al (2003) Accuracy of Three-dimensional imulation in the Sizing of Aortic Endoluminal Devices. Ann Vasc Surg17(2):129–136
22. Coenegrachts K, Rigauts H, De LetterJ (2003) Prediction of aortoiliac stentgraft length: comparison of a semi-automated computed tomography angiography method and calibratedaortography. J Comput Assist Tomogr27(2):284–288
23. Rott A, Boehm T, Soldner J et al(2002) Computerized modeling basedon spiral CT data for noninvasive determination of aortic stent-graftlength. J Endovasc Ther 9(4):520–528