-
8/19/2019 Abdominal Aortic Aneurysm_ an Illustrated Narrative
Review
1/31
12/1/2016 Abdominal aortic aneurysm: an illustrated narrative
review
http://www.sciencedirect.com/science/article/pii/S0161475402541117
Article outline Show full outline
Abstract
Keywords
Introduction
Discussion
Conclusion Acknowledgements
References
Figures and tables
doi:10.1016/S0161-4754(02)54111-7
Journal of Manipulative and Physiological
Therapeutics
Volume 26, Issue 3, March 2003, Pages 184–195
Review of the literature
Abdominal aortic aneurysm: an illustrated narrative review
☆
Colin M Crawford, BAppSc (Chiro)a, , , Kristin Hurtgen-Grace,
DCb, Ernest Talarico, BAppSc (Chiro)c,
John Marley, MD, MBChB, FRACGPd
Show more
Abstract
Objective
To present a descriptive review of abdominal aortic
aneurysm (AAA), including a review
of risk factors for and case finding in AAA for chiropractors as
primary contact health care
practitioners.
Data sources
Clinical and scientific literature identified through various
sources including MEDLINE
and citation tracking.
Data synthesis
Selective narrative review of relevant literature.
Results
AAA may be asymptomatic; however, back pain is a common
presenting feature. Risk
factors include male gender, increasing age, cigarette smoking,
hypertension, chronic
obstructive airway disease, claudication, and AAA in a
first-degree relative. AAA should
be considered in the differential diagnosis of older white
patients, especially males, with
low back pain. Estimated prevalence for AAAs in older males is
in the order of 3% to 5%;
rupture accounts for 1.7% of deaths in men aged 65 to 75 years.
Elective surgical
resection of AAAs (prior to rupture) offers a low operative
mortality and good prognosis.
Conclusion
AAA should be considered in the differential diagnosis of
older patients presenting withlow back pain and those with risk
factors for AAA. Chiropractors, as primary contact
health care practitioners, have a responsibility to refer
patients suspected of having AAA
for appropriate imaging and, where indicated, vascular surgical
opinion.
Keywords
Abdominal Aneurysm; Chiropractic; Diagnosis; Low Back
Pain
Introduction
Low back pain is the most common disabling musculoskeletal
symptom.1 It is the second
most common reason prompting patients to seek care from
physicians 2 and the
Get rights and content
Search ScienceDirect Advanced s earch
Download PD F Export
Journals Books Remote access HelpSign in
http://dx.doi.org/10.1016/S0161-4754(02)54111-7https://s100.copyright.com/AppDispatchServlet?publisherName=ELS&contentID=S0161475402541117&orderBeanReset=truehttp://www.sciencedirect.com/science/journal/01614754http://-/?-http://-/?-http://-/?-http://-/?-http://-/?-http://-/?-http://-/?-http://-/?-http://-/?-http://-/?-http://-/?-http://-/?-http://-/?-http://-/?-http://-/?-http://-/?-http://-/?-http://-/?-http://-/?-http://-/?-http://-/?-http://-/?-http://-/?-http://www.sciencedirect.com/science?_ob=HelpURL&_file=browse_open_doc.htm&_btn=Y&_zone=TopNavBar&_origin=articlehttp://www.sciencedirect.com/science/activateaccesshttps://www.clinicalkey.com/#!/http://www.sciencedirect.com/science/bookbshsrwhttp://www.sciencedirect.com/science/journalshttp://www.sciencedirect.com/http://www.sciencedirect.com/science/article/pii/S0161475402541117/pdfft?md5=d2903bbba2ffb539a686517b54e446a8&pid=1-s2.0-S0161475402541117-main.pdfhttp://www.sciencedirect.com/science/searchhttps://s100.copyright.com/AppDispatchServlet?publisherName=ELS&contentID=S0161475402541117&orderBeanReset=truemailto:[email protected]://www.sciencedirect.com/science/journal/01614754/26/3http://www.sciencedirect.com/science/journal/01614754/26/3http://www.sciencedirect.com/science/journal/01614754http://dx.doi.org/10.1016/S0161-4754(02)54111-7
-
8/19/2019 Abdominal Aortic Aneurysm_ an Illustrated Narrative
Review
2/31
12/1/2016 Abdominal aortic aneurysm: an illustrated narrative
review
http://www.sciencedirect.com/science/article/pii/S0161475402541117
2
predominant presenting complaint to
chiropractors.3 and4 While most back pain may be
of “mechanical” origin,5 careful consideration must be
given to other causes, especially in
an aging population. Abdominal aortic aneurysm (AAA) is a
significant cause of low back
pain and an important cause of preventable death in the older
person. 6 Unlike coronary
artery disease and cerebrovascular disease, the incidence of AAA
dramatically
increased over the 3 decades to 19897 and may be rising.
AAA should therefore be
considered in the differential diagnosis of an older patient
with low back pain, particularly
in those patients with known risk factors for AAA.
“A significant number of lives might be saved…if clinicians
(especially rheumatologists
and orthopedic surgeons) were made more aware of this
possibility.” 8 The quote by
Duthie8 applies equally to chiropractors purporting primary
contact status as it does to
general and specialist medical practitioners. This article
reviews pathology and
pathogenesis, epidemiology and screening, clinical presentation
and assessment,
imaging, case finding,9, 10 and11 natural history, and
management of AAA.
Discussion
Pathology and pathogenesis
An aneurysm is a pathologic,
irreversible12 dilatation of a segment of a blood
vessel,13
caused by a congenital or acquired weakness.14 Aneurysms
are classified according to
their site, configuration, and etiology.14 Seventy-five
percent of abdominal aortic
aneurysms are located below the renal arteries in the distal
abdominal aorta. 13 AAAs are
usually ovoid swellings affecting the entire circumference of a
segment of the distal aorta
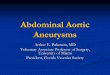
and are described as fusiform. 14 A saccular aneurysm is an
eccentric, localized
distended sac affecting only part of the circumference of the
arterial wall ( Fig 1). 15
Fig 1.
Cadaveric specimen of lower abdominal aorta and iliac
bifurcation demonstrating saccular aneurysms, the
lower of which extends, as a fusiform aneurysm, into right
proximal iliac artery. Horizontal metal marker
approximately 2.5 c m below intercristal (iliac crest)
line. A, Pin in lumbosacral disk; B, pin in L4-5 disk;
C ,
pin in L3-4 disk; D, pin (head) at origin of inferior mesenteric
artery; E , pin in L2-3 disk. Right renal artery
(small arrow ). Unmarked pin in L1-2 disk. Left psoas
muscle (arrow ). Incidentally, this cadaver has an
anomalous inferior vena cava (not shown here). (Man, white, aged
68 years; cause of death: congestive
http://-/?-http://-/?-http://-/?-http://-/?-http://-/?-http://-/?-http://-/?-http://-/?-http://-/?-http://-/?-http://-/?-http://-/?-http://-/?-http://-/?-http://-/?-http://-/?-http://-/?-http://-/?-
-
8/19/2019 Abdominal Aortic Aneurysm_ an Illustrated Narrative
Review
3/31
12/1/2016 Abdominal aortic aneurysm: an illustrated narrative
review
http://www.sciencedirect.com/science/article/pii/S0161475402541117
3
heart f ailure, also chronic obstructive airway disease.)
A true aneurysm involves all 3 layers of the vessel wall.
Pseudoaneurysms involve
disruption of the intimal and medial layers, with the dilatation
lined by adventitia and
sometimes by a perivascular clot.13 A dissecting aneurysm
is, in fact, a dissecting
hematoma in which hemorrhage into the media separates the layers
of the vessel. 14
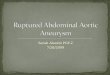
In studies of anatomical specimens, the diameter of the inferior
aspect of the normal
abdominal aorta was less than 15 mm (Fig 2). Radiological
studies have found the
diameter of the normal abdominal aorta to measure, on average,
19 mm.16 Despite these
established standards, a consensus definition of AAA does not
exist.17 An increase in
diameter of 50% is one accepted criterion for defining an
abdominal aortic aneurysm. 12
Other definitions include an infrarenal aorta measurement of 30
mm or more17, 18 and19 or
a ratio of infrarenal to suprarenal diameters greater than
1.5:1.17
Fig 2.
Normal lower abdominal aorta, iliac bifurcation (arrow )
and right (R ) and left (L) iliac arteries in a cadaveric
specimen (Man, white, aged 68 years).
Traditionally, AAAs have been associated with atherosclerotic
disease and frequently
referred to as atherosclerotic aneurysms. However, it appears
that atheroscleroticchanges may be secondary to abdominal aortic
aneurysms rather than being primary. 7
Epidemiological characteristics and genetic risk factors are
different in patients with AAA
compared to those with stenosing arterial disease.20 The
lower abdominal aorta depends
on diffusion of nutrients from the aortic lumen, because vasa
vasorum are deficient in this
part of the aorta.12 Impaired diffusion through damaged
intima, atherosclerotic plaques
and overlying thrombi, and vessel wall vibration may further
weaken the aortic media and
facilitate the development of infrarenal abdominal aortic
aneurysm. 12 and20
Histologically, the aneurysmal aortic wall contains inflammatory
infiltrate and
inflammatory mediators, which may contribute to the destruction
and weakening of the
aortic media. In patients undergoing surgery for AAA, the
aneurysm is considered to be
inflammatory in about 3% to 10% of cases.
20 and21 Traditionally, inflammatory
Figure options
Figure options
http://-/?-http://-/?-http://-/?-http://-/?-http://-/?-http://-/?-http://-/?-http://-/?-http://-/?-http://-/?-http://-/?-http://-/?-http://-/?-http://-/?-http://-/?-http://-/?-http://-/?-
-
8/19/2019 Abdominal Aortic Aneurysm_ an Illustrated Narrative
Review
4/31
12/1/2016 Abdominal aortic aneurysm: an illustrated narrative
review
http://www.sciencedirect.com/science/article/pii/S0161475402541117
4
aneurysms have been viewed as a distinct clinical and
pathological entity caused by an
autoimmune response to components of the aortic wall.
20 Inflammatory AAAs are
characterized by a triad of thickened aneurysm wall, extensive
perianeurysmal and
retroperitoneal fibrosis, and dense adhesions of adjacent
abdominal organs.21 Intense
inflammatory cell infiltrate often extends beyond the aortic
wall into surrounding
tissues.20 Recent evidence suggests that although
inflammatory AAAs arise from the
same stimuli responsible for noninflammatory AAAs, they
represent one extreme of an
inflammatory spectrum.21
Many factors, acting over time, contribute to the pathogenesis
of abdominal aortic
aneurysm. Elastin and collagen are important structural
components of the aortic wall.
Elastin is easily stretched and provides the elastic recoil of
large arteries, while aortic
collagen is coiled such that the initial load in the aorta is
borne by elastin. As the vessel
continues to stretch, collagen fibers become load bearing.
Aortic collagen has a tensile
strength more than 20 times greater than that of elastin but
cannot extend beyond a small
proportion of its original length before structural damage
occurs. Initially, destruction of
elastin shifts the load of pulsatile blood flow in the lower
aorta from elastin to collagen.
Part of the marked stiffness or inelasticity of dilated or
aneurysmal vessels is attributable
to the loss of elastin. Years of pulsatile blood flow through
the degenerated vessel wall
exacerbate the process, and the collagen is continuously exposed
to the expansile force
of intraluminal blood pressure. The extent of dilatation and
subsequent rupture depends
on the properties of the collagen and the net effect of collagen
degradation, turnover, and
remodeling.20
Familial clustering of AAA suggests a genetic basis to this
disease. Inherited defects in
elastin and collagen might weaken the aortic wall, or genetic
variables may increase
enzymatic destruction of vessel wall constituents.20 Both
X-linked and autosomal
dominant modes of inheritance have been
suggested.22 and23
Certain heritable diseases of connective tissue have an
association with AAA, including
Marfan syndrome and Ehlers-Danlos syndromes (EDS). Marfan
syndrome results from a
mutation in the gene that codes for fibrillin, a family of
connective tissue proteins that
serve as scaffolding for the deposition of elastin during
embryonic development. This
genetic mutation weakens the aortic media and dilatation occurs,
resulting in a high
incidence of dissecting aneurysms, especially in the ascending
aorta. The EDS are a
rare group of disorders characterized by hyperelasticity and
fragility of the skin, jointhypermobility, and a bleeding
diathesis. EDS IV is associated with a tendency to
spontaneous rupture of large arteries.24
Cigarette smoking has been strongly associated with the presence
of AAA, death from
rupture, and aneurysm expansion rates. The mechanism is thought
to be enhancement
of proteolytic enzyme degradation of the aortic wall by gaseous
and blood-borne
products of tobacco combustion.20 and25 The only
prophylactic advice that appears
useful is cessation of smoking.26
Hypertension is associated with increased prevalence and
increased risk of rupture.
Hypertension may be related directly to pathogenesis or may
merely exacerbate the
effect of blood flow forces on an already weakened aortic wall.
20 A recent study found a
low incidence of AAAs in elderly patients with treated,
uncomplicated hypertension and
concluded that uncomplicated hypertension by itself was not an
indication for
screening.27
AAA is uncommon before 50 years of age. Normal aging is
associated with alterations in
the structure and, consequently, the mechanical properties of
the aortic wall. Thus, the
aging aorta may be less able to withstand the force of pulsatile
blood flow, resulting in
aneurysmal dilatation.20
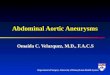
The different processes involved in the pathogenesis of AAA are
integrated
diagrammatically in Figure 3. Their relative importance may vary
from one patient to
another.20
http://-/?-http://-/?-http://-/?-http://-/?-http://-/?-http://-/?-http://-/?-http://-/?-http://-/?-http://-/?-http://-/?-http://-/?-http://-/?-http://-/?-http://-/?-http://-/?-http://-/?-
-
8/19/2019 Abdominal Aortic Aneurysm_ an Illustrated Narrative
Review
5/31
12/1/2016 Abdominal aortic aneurysm: an illustrated narrative
review
http://www.sciencedirect.com/science/article/pii/S0161475402541117
5
Fig 3.
Pathogenesis of abdominal aortic aneurysm. Reproduced with
permission of the Editors of the British
Journal of Surgery.20
Epidemiology and risk factors
AAA is 10 times more common in 65- to 75-year-old men
compared to women of the
same age. This is in contrast to the male-to-female ratio for
atherosclerotic disease,
which is closer to 2:1. The gender-related difference in AAA
diminishes to about 3:1 in the
85- to 89-year-old age group.25 The prevalence of aneurysms
greater than 4.0 cm in
diameter in men aged between 65 and 75 years is approximately
3%. Other studies have
estimated the prevalence of unsuspected aortic aneurysm to be
5.4%. 28 Studies have
reported prevalence rates of 12% to 33% in first-degree
relatives.12 and17
Abdominal aortic aneurysm (with elective repair or
rupture) is the 10th to 13th leading
cause of death in the United States.7 The death rate for
AAA (rupture) in the United
Kingdom peaks at 65 to 75 years of age; rupture accounts for
1.7% of all deaths in men in
this age group in the United Kingdom. Death from AAA in England
and Wales showed a
progressive and continuing increase over a 30-year period to
1988. 25 and29 The
increased prevalence of aneurysm has paralleled the pattern of
tobacco addiction, which
rose during the period 1916 to 1948; a cohort effect with a
40-year time lag has been
suggested to explain this observation.25 Increased
awareness of abdominal aortic
aneurysms, screening programs, and the aging population are also
thought to have
contributed to an increase in the incidence of asymptomatic
AAAs. In a study in the
United States, white men had higher age-adjusted death rates for
aortic aneurysm than
black men. The age-specific rates were similar or higher in
black men under age 65
years. Black women had higher rates than white women under age
65 years, similar
rates at ages 65 to 84 years, and lower rates above 85
years.30
Correlation between hypertension and cigarette smoking and the
development of AAA
was found in studies reviewed by Reilly and
Tilson.7 However, a substantial number of
patients without hypertension or a history of smoking develop
abdominal aortic
aneurysms.7 The presence of chronic obstructive pulmonary
(airway) disease,
independent of smoking, was found to be predictive of rupture of
aortic aneurysm. 31
Reilly and Tilson7 concluded that further research is
needed to look at the clinical
expression of the disease and the interplay of environmental
factors, such as smoking,
against a background of defined genetic risk. Claudication was
the only cardiovascular
complication independently associated with the presence of AAA
in a study of
predominantly white men presenting to a hypertension
clinic.27
The mean body mass index (weight in kg/height in m 2)10 in
men and women with
aneurysms was not significantly greater than that of normal
subjects in an Italian study. 32
However, a North American study found height to be related to
the presence of aortic
Figure options
http://-/?-http://-/?-http://-/?-http://-/?-http://-/?-http://-/?-http://-/?-http://-/?-http://-/?-http://-/?-http://-/?-http://-/?-http://-/?-http://-/?-http://-/?-http://-/?-http://-/?-
-
8/19/2019 Abdominal Aortic Aneurysm_ an Illustrated Narrative
Review
6/31
12/1/2016 Abdominal aortic aneurysm: an illustrated narrative
review
http://www.sciencedirect.com/science/article/pii/S0161475402541117
6
aneurysms and a positive association between body weight and
aneurysms.33 This
study documented the strong association of cardiovascular risk
factors and measures of
clinical and subclinical atherosclerosis, cardiovascular
disease, and prevalence of
aneurysms.
Clinical presentation and examination
Abdominal aortic aneurysm is usually asymptomatic until
rupture or size draws the
attention of the patient or physician to it.25 A feeling of
fullness or pulsations in the
abdomen may be early symptoms.34 In one review of 528
patients with aneurysms, 91%
had symptoms at their first presentation; the most common
symptoms at firstpresentation were abdominal pain and backache.
Only 48 of the 528 patients in this study
were completely asymptomatic, with an aneurysm found at
examination for another
complaint.35 The clinician should consider the possibility
of rupture of an AAA in a male
patient over the age of 60 years who presents with sudden onset
back and/or loin pain 8
with shock and/or syncope.12 In addition, patient
characteristics which may raise clinical
suspicion of AAA include being a current smoker or with a
significant smoking history,
increased weight, a history of myocardial infarction,6 and
claudication.27 As discussed
above, a strong familial occurrence of AAA should also raise
diagnostic suspicion, as
should the presence of hypertension.7
Clinically, the abdominal aorta may be located anteriorly in the
midline between a point
2.5 cm above the transpyloric plane and a point slightly
inferior and a little to the left of the
umbilicus. The transpyloric plane is an imaginary horizontal
plane located midway
between the xiphisternal joint and the umbilicus. The aortic
bifurcation into the common
iliac arteries occurs just to the left of the midpoint of the
line joining the highest points of
the iliac crests (intercristal line) (Fig 1, Fig 2 and Fig
6).36 Appleberg12 highlights the need
to palpate specifically for abdominal aneurysm. The examination
should be conducted
with the supine patient’s knees raised and the abdomen relaxed.
37 The technique
involves deep and careful palpation with the palms down, to the
left of the midline,
keeping the hands steady in one position until the aortic pulse
is felt, and then carefully
evaluating the transverse extent of the expansile pulse with the
pads of the index
fingers.12 and37 Physical findings may include a
tender,38 palpable, pulsatile abdominal
mass35 with abdominal bruit.34
It is important to recognize that abdominal palpation for the
detection of abdominal aortic
aneurysms has low overall sensitivity (ie, high
false-negatives).6 One study, the purpose
of which was inter alia “to determine the accuracy of physical
examination in AAA
detection,”6(p1753) found that abdominal palpation detected
only half of 18 previously
unsuspected aneurysms in 201 patients. This study found that
abdominal girth was an
important factor in detecting AAA by physical examination. No
AAA was missed on
palpation by the study team, comprising staff internists, when
the girth was less than 100
cm. In 109 subjects with a girth of 100 cm or greater, only 3 of
12 AAAs were palpable. 6
Five patients in this study with AAAs who had a definite
pulsatile mass detected by
palpation had, on chart review, abdominal examinations recorded
as negative by their
primary care physicians. The authors of this study did not
comment specifically on
interexaminer or intraexaminer reliability of abdominal
examination findings. A later study
found fair to good interobserver mean pair agreement and kappa
scores for the presence
or not of AAA. It found high sensitivity for diagnosis of
abdominal aortic aneurysms large
enough to warrant elective intervention in patients who did not
have a large abdominal
girth and good sensitivity in patients with a large girth if the
aorta was palpable. 37
Unusual clinical presentations
Unusual clinical presentations of AAA may result from chronic
contained rupture,
inflammatory aneurysm, aortovenous fistula, and atheroembolism.
These manifestations
may complicate surgery and raise operative morbidity and
mortality.38 A chronic
contained rupture may, in addition to abdominal or low back
pain, cause pressure effects
resulting in jaundice from common bile duct compression or in
ureteral obstruction,
femoral neuropathy, or extension of the hematoma into the
femoral sheath, simulating a
http://-/?-http://-/?-http://-/?-http://-/?-http://-/?-http://-/?-http://-/?-http://-/?-http://-/?-http://-/?-http://-/?-http://-/?-http://-/?-http://-/?-http://-/?-http://-/?-http://-/?-http://-/?-http://-/?-http://-/?-http://-/?-http://-/?-http://-/?-http://-/?-http://-/?-
-
8/19/2019 Abdominal Aortic Aneurysm_ an Illustrated Narrative
Review
7/31
12/1/2016 Abdominal aortic aneurysm: an illustrated narrative
review
http://www.sciencedirect.com/science/article/pii/S0161475402541117
7
groin hernia.38
So-called inflammatory aneurysms (see comments above) may result
in adhesions
involving structures such as the duodenum, inferior vena cava,
and left renal vein. Two
thirds or more of patients with inflammatory aneurysms are
symptomatic at the time of
presentation; common symptoms include abdominal, flank, and/or
back pain; anorexia;
weight loss; and elevated erythrocyte sedimentation
rate.21 and38
Aortocaval and aortorenal vein fistulas result from
rupture of an AAA into the inferior vena
cava or the left renal vein. Clinical presentation includes
high-output heart failure,
cardiomegaly, a palpable abdominal mass, audible continuous
bruit, hypotension,
oliguria, and abdominal and back pain.38
Infected aneurysms are rare and may result from superimposed
infection or arise
secondarily from an infection. Clinically, infected aneurysms
may present with the
sudden appearance of a pulsatile mass or recent enlargement of a
known AAA in
combination with fever or recent febrile illness.38
Atheroembolism from an abdominal aortic aneurysm to 1 or
both of the lower extremities
is a well-documented occurrence.38 Thrombus within the
lumen of the aneurysm or
cholesterol debris from within the intima of the wall can be the
source of macroemboli or
microemboli, respectively. Macroembolism presents with symptoms
and signs of large-
vessel occlusion and sudden ischemia of the lower limbs.
Small-vessel occlusion
resulting from microemboli presents as slowly evolving livedo
reticularis, painful cyanotic
toes, and palpable pedal pulses. Microembolism has been termed
blue toe syndrome
because of the characteristic cyanosis of the toes; if both
lower extremities are involved,
an AAA or other aortic source should be considered. 38
Other unusual complications of AAAs include recurrent ischemic
myelopathy and/or
paraparesis. Ischemic spinal cord lesions may present with
bladder incontinence, a
mixture of upper and lower motor neuron lower limbs signs, and
patchy sensory loss. 39
Paraparesis may result from anterior spinal artery syndrome,
which presents as a
varying degree of muscle weakness and dissociated sensory loss
of pain with sparing of
proprioception.40
Imaging
There are numerous modalities available for imaging the aorta;
each has strengths andweaknesses. Variations in individual cases,
equipment availability, technical expertise,
and surgeon preference all influence imaging modality
selection.41
Abdominal aortic aneurysms are frequently noted on frontal
(anterior-posterior [AP]) (Fig
4), lateral (Fig 5), and oblique low back plain film
radiographs. Most AAAs occur between
the renal arteries and the iliac bifurcation; that is, between
the L2 and L4 vertebral levels,
respectively. In the frontal (AP) projection, an AAA is usually
seen on the left side of the
spine and appears as a soft tissue density demarcated by a thin,
curvilinear rim of
continuous or discontinuous calcification. On the lateral view,
collimation may prevent
the anterior margin from being visualized. At times on the
lateral view, the only indication
of AAA may be a horizontally oriented calcified
plaque.19 Calcification is noted in 55% to
85% of AAAs41 and42; in the remainder, a soft tissue
density may be identifiable. Erosion
of the anterior margins of the vertebral bodies (Oppenheimer
erosions) may be noted
with inflammatory and saccular (Fig 1 and Fig 6) aneurysms
and those involving
contained rupture.19 and43
http://-/?-http://-/?-http://-/?-http://-/?-http://-/?-http://-/?-http://-/?-http://-/?-http://-/?-http://-/?-http://-/?-http://-/?-http://-/?-http://-/?-http://-/?-http://-/?-http://-/?-http://-/?-http://-/?-
-
8/19/2019 Abdominal Aortic Aneurysm_ an Illustrated Narrative
Review
8/31
12/1/2016 Abdominal aortic aneurysm: an illustrated narrative
review
http://www.sciencedirect.com/science/article/pii/S0161475402541117
8
Fig 4.
Antero-posterior lumbo-pelvic (AP LP) plain film
radiograph: Curvilinear rim of discontinuous calcif ication
of
the wall of AAA (large arrows); maximum transverse diameter 8.5
cm. Bilateral iliac artery calcification
(seen clearly on right side only–small arrow ).
Fig 5.
Lateral lumbosacral (LAT LS) plain film radiograph: Horizontally
oriented calcified plaque on the superior
margin of AAA (arrows) just anterior to the L3 vertebral
body.
Figure options
Figure options
-
8/19/2019 Abdominal Aortic Aneurysm_ an Illustrated Narrative
Review
9/31
12/1/2016 Abdominal aortic aneurysm: an illustrated narrative
review
http://www.sciencedirect.com/science/article/pii/S0161475402541117
9
Fig 6.
Anterior-posterior (AP) radiograph of cadaveric specimen
in Figure 1. A, Pin in lumbosacral disk; B, pin in
L4-5 disk; C , pin in L3-4 disk; D, pin (head) in origin of
inferior mesenteric artery; E , pin in L2-3 disk; F ,
pin
in L1-2 disk. Right proximal iliac artery aneurysm (small
arrows). Larger arrow at level of aortic
bifurcation.
Ultrasound scanning is currently the most practical and accurate
way of detecting
abdominal aortic aneurysms in large numbers of people
17 and44 and has become the
most commonly used method of screening.41, 44,
45 and46 Ultrasound enables diagnostic
confirmation, evaluation of size, and monitoring of
progression.44 Measurements of
AAAs from ultrasound correlate within 3 mm of surgical
specimens.41 Diagnostic
ultrasound may show thrombus (Fig 7), periaortic abnormalities,
dissections, and the
cephalic and caudal extent of the lesion.41 Diagnostic
limitations of ultrasound include
difficulties imaging obese patients and those with abundant
overlying bowel gas.41 The
renal arteries can only rarely be visualized directly and
inferences regarding suprarenal
extension of an AAA can only be made from the relationship of
the aneurysm to the
superior mesenteric artery.41 Graham and
Chan44 studied ultrasound screening for
clinically occult AAA and concluded that the false-negative
results for the ultrasound
detection of AAAs was probably low, suggesting that ultrasound
scanning was a
sensitive procedure for the diagnosis of AAA. The specificity
and positive predictive value
of ultrasound have been shown to be 100%,6 and thus, this
modality is optimal for
screening and follow-up in noncomplicated cases.41 Clinical
suspicion of AAA should
lead to confirmation with ultrasound.19
Figure options
http://-/?-http://-/?-http://-/?-http://-/?-http://-/?-http://-/?-http://-/?-http://-/?-http://-/?-http://-/?-http://-/?-http://-/?-http://-/?-http://-/?-http://-/?-http://-/?-http://-/?-
-
8/19/2019 Abdominal Aortic Aneurysm_ an Illustrated Narrative
Review
10/31
12/1/2016 Abdominal aortic aneurysm: an illustrated narrative
review
http://www.sciencedirect.com/science/article/pii/S0161475402541117
10
Fig 7.
Ultrasound of a l arge AAA. The t ransverse diameter of this AAA
measures 7.91 cm ; intraluminal diameter
is 4.73 cm. Intraluminal clot is clearly visible. (Courtesy of
Sulzer Vascutek, Australia.)
Computed tomography (CT) accurately demonstrates the size and
craniocaudal extent
of an abdominal aortic aneurysm and is usually able to detect
intraluminal thrombus. CT
also enables visualization of the retroperitoneum, allowing
detection of aneurysmal leak,
ureteral obstruction, perianeurysmal fibrosis, and other unusual
causes of abdominal or
back pain.41 Postinfusion CT scans facilitate
differentiation of the patent lumen of the
aneurysm from surrounding intraluminal thrombus (Fig 8). CT
scanning is the modality of
choice for postsurgical repair evaluation of
AAAs.41 However, CT scanning of AAAs
requires exposing the patient to ionizing radiation and the
administration of contrast
material.47
Fig 8.
CT scan with contrast in the patent lumen (small arrow ) of
a typical AAA; thrombus (large arrow ).
The multiplanar display capability of magnetic resonance imaging
(MRI) can
demonstrate the features discussed above without the need for
contrast; it allowsaccurate measurement, isolates flow
abnormalities, identifies clot, and allows
assessment of visceral involvement.19 MRI is noninvasive
and reduces the need for
angiography (Fig 9). MRI may be contraindicated in patients
requiring respirators or
monitoring equipment. Gadolinium-enhanced magnetic resonance
angiography (MRA)
is a variation of standard magnetic resonance imaging, utilizing
a paramagnetic contrast
agent. This modality provides anatomic information for aortic
reconstructive surgery
without the contrast-related renal toxicity or
catheterization-related complications
attending conventional arteriography.48 Further, the
advantages of MR angiography
include the lack of ionizing radiation and need for iodinated
contrast material and its
ability to image the entire abdomen and pelvis, as well as the
thorax and lower
extremities if necessary.49
Figure options
Figure options
http://-/?-http://-/?-http://-/?-http://-/?-http://-/?-http://-/?-http://-/?-http://-/?-
-
8/19/2019 Abdominal Aortic Aneurysm_ an Illustrated Narrative
Review
11/31
12/1/2016 Abdominal aortic aneurysm: an illustrated narrative
review
http://www.sciencedirect.com/science/article/pii/S0161475402541117
1
Fig 9.
MRI scans and aortograms of large infrarenal AAA in a
67-year-old man. A, Oblique coronal 2-dimensional
(time-of-flight) magnetic resonance (MR) angiogram demonstrates
the widest dimension of the AAA. B,
Three-dimensional (maximum intensity projection) MR angiogram
reconstructed from multiple 2-
dimensional sect ions shows the AA A s tarting below the renal
arteries (white arrows) and extending into
both iliac arteries (black arrows). C, Conventional aortogram
helps confirm the iliac artery extension of the
AAA. D, Targeted (maximum intensity projection) image
helps confirm normal proximal renal arteries
(arrows) reconstructed from 2-dimensional MR angiograms. E,
Conventional aortogram helps confirm
patent renal arteries. Reproduced with permission of the Editors
of Radiology and the authors. 67
Angiography is used to evaluate the state of the renal
arteries and other vessels in the
iliac artery system in patients with AAA12 (Fig 9,
C and E ). It is the gold standard for
demonstrating visceral-branch involvement and vascular anatomy.
41 However,
angiography may underdemonstrate the size and extent of the
thrombus-filled
aneurysm, as only the lumen is demonstrated.41 The use of
angiography may alter the
surgical approach utilized in up to 25% of cases. 19
Natural history
Most AAAs continue to enlarge progressively.12 Small
aneurysms increase in transverse
diameter by up to 5 mm per year 31 and50; the
anteroposterior diameter increases by an
average of 2.2 mm per year.31 Large aneurysms expand more
rapidly than smaller
ones.12 and50 The risk of rupture increases
significantly as the size of the aneurysm
increases, with a 43% risk of rupture within 12 months of
aneurysms greater than 6 cm. 51
Patients with aneurysms less than 5 cm also run the risk of
rupture in 2% to 32.9% of
cases.12
The nonoperative mortality of ruptured abdominal aortic aneurysm
is 100%. The
operative mortality of ruptured aneurysm is around 50%; survival
prospects are
enhanced by admittance to a specialist surgical unit (ie, by
surgical skill) and relate
inversely to increasing severity and duration of preoperative
hypotension.25 In a
retrospective review of 528 cases, the mortality rate for acute
presentations, as opposed
Figure options
http://-/?-http://-/?-http://-/?-http://-/?-http://-/?-http://-/?-http://-/?-http://-/?-http://-/?-http://-/?-http://-/?-http://-/?-http://-/?-http://-/?-http://-/?-
-
8/19/2019 Abdominal Aortic Aneurysm_ an Illustrated Narrative
Review
12/31
12/1/2016 Abdominal aortic aneurysm: an illustrated narrative
review
http://www.sciencedirect.com/science/article/pii/S0161475402541117
12
to rupture, was 19%.35 Over the 3 decades to 1988, the
mortality for elective AAA
surgery progressively fell to less than 3%.25 Some centers
claim an elective mortality as
low as 1.4%.25 Age is not an indication to forego surgery;
safe aneurysm repair is
possible for many patients over 80 years of age. 52
Role of screening
Screening is the presumptive identification of unrecognized
disease or defect by the
application of tests, examinations, or other procedures which
can be applied rapidly.53
To qualify as a target for a screening program, a disorder needs
to be fairly prevalent and
detectable by tests that are inexpensive, accurate, acceptable
to patients, and treatablewith low risk.54 Screening
procedures also need to be both sensitive and
specific.44Sensitivity refers to “positivity in
disease,” 55(p81) or the proportion of patients
with the target disorder who have a positive test.
Specificity refers to the ability of a test to
correctly identify those patients without the target disorder
(ie, “negativity in health”).55(p82)
In one study of patients with girth measurement of less than 100
cm, no AAA was missed
on abdominal palpation,6 suggesting high sensitivity of
abdominal palpation in this group.
This degree of sensitivity was not obtained with “routine”
examinations, and the study
concluded that the examination needed to be directed
specifically toward AAA detection.
The caution given by Appleberg12 is worthy of reiteration,
namely, the need for deep and
careful palpation specifically for AAA (see above). In the
Oxford Screening Programme
for AAA in men aged 65 to 74 years, the sensitivity and positive
predictive value of
abdominal palpation for epigastric and/or infraumbilical midline
pulsations were poor,
while specificity was over 90%.28 Overall, abdominal
palpation has been reported to
have low sensitivity in detecting AAA.6 and56 Except
in a small number of patients,
therefore, abdominal palpation fails to meet the requirements
for a screening tool.
On the other hand, ultrasound screening meets the criteria to be
considered an
acceptable screening test for the detection of AAA, including
acceptable sensitivity and
specificity.6 and44 A recent prospective study
supported annual screening using serial
ultrasound for small aneurysms (2.5 to 3.9 cm) and 6-month
screening for those
measuring 4.0 cm or greater.50 Arguably, with high
mortality rates associated with
surgical repair of ruptured AAAs and the low mortality rate
associated with elective repair
of aneurysms, obese males over the age of 55 years with
hypertension, coronary artery
disease, cerebrovascular disease, or peripheral artery
disease56 should be routinely
screened with ultrasound.44 Patients, especially men with
chronic obstructive airway
disease, or those who are first-degree relatives of a known
aneurysm patient, should also
undergo screening.26 and54 As smoking is a significant
risk factor, the screening of
smokers in the 65- to 80-year-old age group may also constitute
a cost-effective
strategy.26 and54 Recently, a study concluded that
uncomplicated hypertension by itself
was not an indication for screening but recommended screening
for AAA in elderly white
patients with claudication.27
The introduction of the Oxford Screening Programme nationally
(in the United Kingdom)
a decade ago was estimated to prevent potentially some 6000
unnecessary deaths. 28 A
study in Gloucestershire (United Kingdom) demonstrated a
significant reduction in
number of deaths from all aortic aneurysm-related causes in the
screened portion of themale population.57 In one study, 45
male patients aged 55 years or older, with a waist
measurement greater than 101 cm and no abdominal aortic aneurysm
detected on
clinical examination, were referred to a tertiary referral
center. In addition, these patients
had at least one of the following conditions: hypertension,
coronary artery disease,
cerebrovascular disease, and peripheral vascular disease.
Subsequent ultrasonography
(ultrasound) revealed 6 aneurysms, giving a detection rate of
13%. 44 Existing evidence
seems to favor screening at least for men aged 65 to
7554 or 60 to 80,58 but the costs and
benefits of more general screening have not been calculated.
54
The findings of a recent study indicate that a second screening,
approximately 4 years
after the initial examination, is of little practical value,
mainly because the AAAs detected
are small. Screening after 8 years may provide total yields
similar to those seen in initial
http://-/?-http://-/?-http://-/?-http://-/?-http://-/?-http://-/?-http://-/?-http://-/?-http://-/?-http://-/?-http://-/?-http://-/?-http://-/?-http://-/?-http://-/?-http://-/?-http://-/?-http://-/?-http://-/?-http://-/?-http://-/?-http://-/?-http://-/?-http://-/?-http://-/?-http://-/?-http://-/?-http://-/?-http://-/?-http://-/?-
-
8/19/2019 Abdominal Aortic Aneurysm_ an Illustrated Narrative
Review
13/31
12/1/2016 Abdominal aortic aneurysm: an illustrated narrative
review
http://www.sciencedirect.com/science/article/pii/S0161475402541117
13
screening. Further, this study found that rescreening only those
subjects with an
infrarenal aortic diameter of 2.5 cm or greater on initial
examination would have missed
more than two thirds of new AAAs.59
Management
Surgical resection of abdominal aortic aneurysm was first
described in 1952. Discussion
of the various repair options is outside the scope of this
report; interested readers are
referred to other sources, including the editorial by Ernst.
60 Appropriate management of
patients with clinically suspected or diagnosed AAA by primary
contact health
practitioners is referral for imaging studies and/or surgical
opinion. Surgery is indicated incases of both small and large AAAs
25, 31 and52 (Fig 10 and Fig 11). As discussed
above,
patients with small aneurysms run a risk of rupture, which may
be as high as 9.5%. With
large AAAs, the risk of rupture is between 60% and
80%.44 The operative mortality from
elective surgery has progressively fallen to less than 3%. Thus,
the risk of death without
surgery, even with small aneurysms, is significant. Naturally,
other significant medical
problems need to be considered in making the decision to
operate. 44 The authors of a
retrospective study of 1000 consecutive elective AAA repairs
concluded that pulmonary
and renal disease did not, and should not, pose a significant
risk for elective infrarenal
AAA replacement, although cardiac dysfunction and coronary
artery disease increased
morbidity and mortality.61 The long-term survival of a
patient undergoing surgical
resection and repair of an AAA with an artificial graft who
survives the immediate
postoperative period is comparable to that in persons who never
had an AAA.58
Collinemphatically states that “any doctor who .. does
not refer the problem to a vascular
surgeon should be aware that he may willfully be condemning his
(sic) patient to a totally
preventable premature death.”25 and67
Fig 10.
Operative v iew of AA A and bifurcation into the iliac arteries
(bottom of f igure) seen through a long midline
incision. (Courtesy of Sulzer Vascutek, Australia.)
Figure options
http://-/?-http://-/?-http://-/?-http://-/?-http://-/?-http://-/?-http://-/?-http://-/?-http://-/?-http://-/?-http://-/?-http://-/?-http://-/?-
-
8/19/2019 Abdominal Aortic Aneurysm_ an Illustrated Narrative
Review
14/31
12/1/2016 Abdominal aortic aneurysm: an illustrated narrative
review
http://www.sciencedirect.com/science/article/pii/S0161475402541117
14
Fig 11.
Operative v iew of AA A graft replacement. AAA graft replacement
secured in place; the original aneurysm
sac is now sutured over the front of the graft in order to
prevent aortoenteric fistula. (Courtesy of Sulzer
Vascutek, Australia.)
Chiropractors are, by training and legislation, primary contact
health care practitioners.
Inherent in such status is the responsibility to consider
conditions other than mechanical
back pain in patients presenting with spinal pain and putative
spinal dysfunction in
patients presenting for so-called chiropractic maintenance
care62 or wellness care.
Approximately 80% of patients presenting for chiropractic
care do so for
neuromusculoskeletal pain, with low back pain being the
predominant presenting
complaint.3 and4 With the aging
population44 noted in western countries and with certain
groups of older patients, who until recently may have been
denied access to chiropractic
care, now gaining access (for example, Australian armed
services’ veterans through
recognition of chiropractic services by the Department of
Veterans’ Affairs), chiropractors
need to be cognizant of AAA and vigilant in assessing their
older patients for the
possibility inter alia of AAA. This involves not only
circumstances where an abdominal
aortic aneurysm is the cause of the presenting back pain
63 but also case finding involving
the consideration of unrelated, intercurrent illnesses (eg, AAA)
in presenting patients9
due to the presence of known risk factors.
Should a patient with risk factors associated with AAA present
to a chiropractor, referral
for imaging (usually ultrasound) with subsequent vascular
surgical opinion, where
appropriate, is required.64 and65 In Australia,
referral is usually via the patient’s general
medical practitioner. Should an aneurysm present fortuitously on
radiographic
examination, such referral is also mandatory. Patients known to
have an abdominal
aortic aneurysm should be warned of the importance of
characteristic symptoms of
rupture and the necessity for immediate attention should they
arise. 12
It is not known whether an AAA is a definite contraindication to
chiropractic manipulation
per se, although large AAAs are considered so.66 Further,
it is not known if the forces
utilized in spinal manipulation are of sufficient magnitude to
cause rupture of an AAA or if
patient positioning required for low back spinal
manipulation/adjustment66 is such that
the risk of rupture of an AAA is increased by such positioning.
Referral should be made
Figure options
http://-/?-http://-/?-http://-/?-http://-/?-http://-/?-http://-/?-http://-/?-http://-/?-http://-/?-http://-/?-http://-/?-
-
8/19/2019 Abdominal Aortic Aneurysm_ an Illustrated Narrative
Review
15/31
12/1/2016 Abdominal aortic aneurysm: an illustrated narrative
review
http://www.sciencedirect.com/science/article/pii/S0161475402541117
15
1
2
3
4
5
6
for further assessment because of the risk of spontaneous
rupture and the high mortality
associated with rupture. Consideration should also be given to
the relatively low surgical
mortality rate should surgery be indicated and the possibility
that the AAA is the cause of
low back pain when this is the presenting complaint. Delay in
referring an at-risk patient in
order to offer a trial of therapy may be indefensible morally,
clinically, and in a
medicolegal context.
Conclusion
AAA should be considered in the differential diagnosis of
older patients presenting with
low back pain. The possibility of abdominal aortic aneurysm
should also be considered inasymptomatic, at-risk patients.
Patients at risk for AAA include male patients over the
age of 65 years, with a history of smoking, hypertension,
chronic obstructive airway
disease, claudication, and a first-degree relative with an AAA.
Elective surgery offers a
cure with low operative mortality. Chiropractors, as primary
contact practitioners, have a
responsibility to refer patients suspected of having AAA for
appropriate imaging and,
where indicated, for a vascular surgical opinion.
Acknowledgements
The authors would like to thank and acknowledge the assistance
of the following: Dr
Dennis Middendorp, DC (RMIT, Melbourne, Australia) for
assistance with clinical details;
Dr Antony M. Hatton, BAppSc-Chiropractic, MSc, kindly reviewed
the section on
pathology and pathogenesis; Roy Webb, MSc, Alex Zabobonin, MD,
and Peter
Cauwenbergs, DC, PhD (CMCC, Toronto, Canada) for preparation and
anatomic
orientation of the cadaveric specimen (Fig 1 and Fig 2);
and Renata Lumsden, BSc,
MRT(R) and Lynda Tanner, MRT(R) (CMCC Radiology Department,
Toronto, Canada)
who radiographed the specimen (Fig 6). Thanks also to Liz
Holden, RN, of Sulzer
Vascutek (Australia) who kindly provided and granted permission
to reproduce the
original slides of Fig 7, Fig 10 and Fig 11. The permission
of the Editors of the British
Journal of Surgery to reproduce the diagram in Figure 3 and
the permission of the Editors
of Radiology and the Authors to reproduce the diagnostic imaging
in Figure 9 are
appreciated. Bryan Groulx and Michael Craven (Media Services,
CMCC, Toronto,
Canada) provided assistance with reproduction of the figures for
publication. The
Division of Graduate Studies & Research at CMCC provided
financial assistance.
References
J.W. Frymoyer, M.H. Pope, J.H. Clements, D.G. Wilder, B.
MacPherson, T. Ashikaga
Risk factors in low-back pain: an epidemiological survey
J Bone Joint Surg Am, 65 (1983), pp. 213–218
B.K. Cypress
Characteristics of physician visits for back symptoms: a
national perspective
Am J Public Health, 73 (1983), pp. 389–395
D. Chapman-Smith
The chiropractic profession
Chiropr Rep, 7 (1993), pp. 1–8
D.A. Chapman-Smith
The chiropractic profession: its education, practice, research,
and future directions, NCMIC Group,
West Des Moines (IA) (2000), pp. 65–98
N. Bogduk, L.T. Twomey
Clinical anatomy of the lumbar spine (2nd ed), Churchill
Livingstone, Melbourne (1991), pp. 161–173
F.A. Lederle, J.M. Walker, D.B. Reinke
Selective screening for abdominal aortic aneurysms with physical
examination and ultrasound
http://-/?-http://-/?-http://-/?-http://-/?-http://-/?-http://-/?-http://-/?-http://-/?-http://-/?-http://-/?-http://-/?-http://-/?-http://-/?-http://-/?-
-
8/19/2019 Abdominal Aortic Aneurysm_ an Illustrated Narrative
Review
16/31
12/1/2016 Abdominal aortic aneurysm: an illustrated narrative
review
http://www.sciencedirect.com/science/article/pii/S0161475402541117
16
7
8
9
10
11
12
13
14
15
16
17
18
19
20
Arch Intern Med, 148 (1988), pp. 1753–1756
J.M. Reilly, M.D. Tilson
Incidence and etiology of abdominal aortic aneurysms
Surg Clin North Am, 69 (1989), pp. 705–711
J.J. Duthie
Screening for abdominal aortic aneurysm
Lancet, 2 (1988), p. 1319
D.L. Sackett, R.B. Haynes, G.H. Guyatt, P. Tugwell
Clinical epidemiology: a basic science for clinical medicine
(2nd ed), Little, Brown and Company,
Boston (1991), pp. 153–170
J.R. Jamison
Maintaining health in primary care, Churchill Livingstone,
Edinburgh (2001), pp. 47–76
J.R. Jamison
Maintaining health in primary care, Churchill Livingstone,
Edinburgh (2001), pp. 37–46
M. Appleberg
Abdominal aortic aneurysms: pathogenesis, diagnosis and
management
Mod Med Aust, 37 (1994), pp. 54–63
V.J. Dzau, M.A. Creager
Diseases of the aorta
R.K. Root (Ed.), Harrison’s principles of internal medicine
(12th ed), McGraw-Hill, New York (1991), pp.
1015–1018
E.P. Benditt, S.M. Schwartz
Blood vessels
J.L. Farber (Ed.), Essential pathology (2nd ed), JB Lippincott,
Philadelphia (1995), pp. 245–275
Dorland’s illustrated medical dictionary (27th ed), W. B.
Saunders, Philadelphia (1988)
P.L. Williams, R. Warwick, M. Dyson, L.H. Bannister
Angiology
L.H. Bannister (Ed.), Gray’s anatomy (37th ed), Churchill
Livingstone, Edinburgh (1989), pp. 662–858
A. Verloes, N. Sakalihasan, L. Koulischer, R. Limet
Aneurysms of the abdominal aorta: familial and genetic aspects
in three hundred thirteen
pedigrees
J Vasc Surg, 21 (1995), pp. 646–655
J. Holdsworth
Screening for abdominal aortic aneurysm in Northumberland
Br J Surg, 81 (1994), pp. 710–712
L.J. Rowe, T.R. Yochum
Hematologic and vascular disorders
L.J. Rowe (Ed.), E ssentials of skeletal radiology (2nd ed),
Williams & Wilkins, B altimore (1996), pp.
1243–1326
S. MacSweeney, J. Powell, R. Greenhalgh
http://-/?-http://-/?-http://-/?-http://-/?-http://-/?-http://-/?-http://-/?-http://-/?-http://-/?-http://-/?-http://-/?-http://-/?-http://-/?-http://-/?-
-
8/19/2019 Abdominal Aortic Aneurysm_ an Illustrated Narrative
Review
17/31
12/1/2016 Abdominal aortic aneurysm: an illustrated narrative
review
http://www.sciencedirect.com/science/article/pii/S0161475402541117
17
21
22
23
24
25
26
27
28
29
30
31
32
33
Pathogenesis of abdominal aortic aneurysm
Br J Surg, 81 (1994), pp. 935–941
T.E. Rasmussen, J.W. Hallett
Inflammatory aortic aneurysms: a clinical review with new
perpectives in pathogenesis
Ann Surg, 225 (1997), pp. 155–164
M. Tilson, M. Seashore
Human genetics of the abdominal aortic aneurysm
Surg Gynecol Obstet, 158 (1984), pp. 129–132
M.D. Tilson, M.R. Seashore
Fifty families with abdominal aortic aneurysms in two or more
first-order relatives
Am J Surg, 147 (1984), pp. 551–553
E. Rubin, J.L. Farber
Development and genetic diseases
J.L. Farber (Ed.), Essential pathology (2nd ed), JB Lippincott,
Philadelphia (1995), pp. 125–160
J. Collin
The epidemiology of abdominal aortic aneurysm
Br J Hosp Med, 39 (1988), pp. 64–67
T.R. Cheatle, J.H. Scurr
Abdominal aortic aneurysms: a review of current problems
Br J Surg, 76 (1989), pp. 826–829
G. Simon, D. Nordgren, S. Connelly, P.J. Shultz
Screening for abdominal aortic aneurysms in a hypertensive
patient population
Arch Intern Med, 156 (1996), pp. 2081–2084
J. Collin, L. Araujo, J. Walton, D. Lindsell
Oxford screening programme for abdominal aortic aneurysm in men
aged 65 to 74 years
Lancet, 2 (1988), pp. 613–615
F. Fowkes, C. Macintyre, C. Ruckley
Increasing incidence of aortic aneurysms in England and
Wales
Br Med J, 298 (1989), pp. 33–35
R.F. Gillum
Epidemiology of aortic aneurysm in the United States
J Clin Epidemiol, 48 (1995), pp. 1289–1298
J.L. Cronenwett, T.F. Murphy, G.B. Zelenock, W.M. Whitehouse,
M.S. Lindenauer, L.M. Graham, et al.
Actuarial analysis of variables associated with rupture of small
abdominal aortic aneurysms
Surgery, 98 (1985), pp. 472–483
G. Simoni, A. Gianotti, A. Ardia, A. Baiardi, R. Galleano, D.
Civalleri
Screening study of abdominal aortic aneurysm in a general
population: lipid parameters
Cardiovasc Surg, 4 (1996), pp. 445–448
H.G. Alcorn, S.K. Wolfson Jr, K. Sutton-Tyrrell, L.H. Kuller, D.
O’Leary
Risk factors for abdominal aortic aneurysms in older adults
enrolled in The Cardiovascular
Health Study
http://-/?-http://-/?-http://-/?-http://-/?-http://-/?-http://-/?-http://-/?-http://-/?-http://-/?-http://-/?-http://-/?-http://-/?-http://-/?-
-
8/19/2019 Abdominal Aortic Aneurysm_ an Illustrated Narrative
Review
18/31
12/1/2016 Abdominal aortic aneurysm: an illustrated narrative
review
http://www.sciencedirect.com/science/article/pii/S0161475402541117
18
34
35
36
37
38
39
40
41
42
43
44
45
46
Arterioscler Thromb Vasc B iol, 16 (1996), pp. 963–970
W.M. Miles, D.P. Zipes
Aortic and peripheral vascular disease
L.H. Smit h (Ed.), Cecil ess entials of medicine (2nd ed), W. B.
Saunders, Philadelphia (1990), pp. 114–
119
J.W.L. Fielding, J. Black, F. Ashton, G. Slaney, D.J.
Campbell
Diagnosis and management of 528 abdominal aortic aneurysms:
occasional review
Br Med J, 283 (1981), pp. 355–359
K.L. Moore
Clinically oriented anatomy (2nd ed), Williams & Wilkins,
Baltimore (1985), pp. 149–297
H.A. Fink, F.A. Lederle, C.S. Roth, C.A. Bowles, D.B. Nelson,
M.A. Haas
The accuracy of physical examination to detect abdominal aortic
aneurysm
Arch Intern Med, 160 (2000), pp. 833–836
T.C. Bower, K.J. Cherry, P.C. Pairolero
Unusual manifestations of abdominal aortic aneurysms
Surg Clin North Am, 69 (1989), pp. 745–754
H.B. Desai, A.H. Rajput, R.J. Uitti
Recurrent spinal cord ischemia due to abdominal aortic
aneurysm—a case report
Angiology, 40 (1989), pp. 682–687
M.G. Joseph, M.A. Langsfeld, R.J. Lusby
Infrarenal aortic aneurysm: unusual cause of paraparesis: case
reports
Aust N Z J Surg, 59 (1989), pp. 743–744
L.L. LaRoy, P.J. Cormier, T.A. Matalon, S.K. Patel, D.A. Turner,
B. Silver
Imaging of abdominal aortic aneurysms
Am J Roentgenol, 152 (1989), pp. 785–792
D.C. Brewster, R.C. Darling, J. Raines, R. Sarno, T. O’Donnell,
M. Ezpeleta, et al.
Assessment of abdominal aortic aneurysm size
Cardiovasc Surg, 56 (1976), pp. 164–169
Y. Nonami, S. Ogoshi
Chronic contained rupture of abdominal aortic aneurysms
J Cardiovasc Surg (Torino), 37 (1996), pp. 252–258
M. Graham, A. Chan
Ultrasound screening for clinically occult abdominal aortic
aneurysmCan Med Assoc J, 138 (1988), pp. 627–629
M.E. Gorton
Current trends in peripheral vascular surgery. When is surgical
intervention the best option?
Postgrad Med, 106 (1999), pp. 87–94
J.G. Wong
Appropriate abdominal aortic aneurysm screening
Postgrad Med, 107 (2000), pp. 21–22
http://-/?-http://-/?-http://-/?-http://-/?-http://-/?-http://-/?-http://-/?-http://-/?-http://-/?-http://-/?-http://-/?-http://-/?-http://-/?-
-
8/19/2019 Abdominal Aortic Aneurysm_ an Illustrated Narrative
Review
19/31
12/1/2016 Abdominal aortic aneurysm: an illustrated narrative
review
http://www.sciencedirect.com/science/article/pii/S0161475402541117
19
47
48
49
50
51
52
53
54
55
56
57
58
59
E.G. Amparo, W.K. Hoddick, H. Hricak, R. Sollitto, E. Justich,
R.A. Filly, et al.
Comparison of magnetic resonance imaging and ultrasonography in
the evaluation of
abdominal aortic aneurysms
Radiology, 154 (1985), pp. 451–456
M.R. Prince, D.L. Narasimham, J.C. Stanley, T.W. Wakefield, L.M.
Messina, G.B. Zelenock, et al.
Gadolinium-enhanced magnetic resonance angiography of abdominal
aortic aneurysms
J Vasc Surg, 21 (1995), pp. 656–669
E.K. YucelMR angiography for evaluation of abdominal aortic
aneurysm: has the time come?
Radiology, 192 (1994), pp. 321–323
T.A. Cook, R.B. Galland
A prospective study to define the optimum rescreening interval
for small abdominal aortic
aneurysm: vascular papers
Cardiovasc Surg, 4 (1996), pp. 441–444
D.E. Szilagyi, R.F. Smith, F.J. DeRusso, J.P. Elliott, F.W.
Sherrin
Contribution of abdominal aortic aneurysmectomy to prolongation
of life
Ann Surg, 164 (1966), pp. 678–679
K.A. Harris, F. Ameli, M. Lally, J.L. Provan, K.W. Johnston,
M.R. Goldberg, et al.
Abdominal aortic aneurysm resection in patients more than 80
years old
Surg Gynecol Obstet, 162 (1986), pp. 536–538
J.M. Last
A dictionary of epidemiology (2nd ed.), Oxford University
Press, New York (1988)
C. Cole
Prospects for screening for abdominal aortic aneurysms
Lancet, 349 (1997), pp. 1490–1491
D.L. Sackett, R.B. Haynes, G.H. Guyatt, P. Tugwell
Clinical epidemiology: a basic science for clinical medicine
(2nd ed), Little, Brown and Company,
Boston (1991), pp. 69–152
H.A. Al Zahrani, M. Rawas, A. Maimani, M. Gasab, B. Aba Al
Khail
Screening for abdominal aortic aneurysm in the Jeddah area,
western Saudi Arabia
Cardiovasc Surg, 4 (1996), pp. 87–92
B.P. Heather, K.R. Poskitt, J.J. Earnshaw, M. Whyman, E.
Shaw
Population screening reduces mortality rate from aortic aneurysm
in men
Br J Surg, 87 (2000), pp. 750–753
P.S. Frame, D.G. Fryback, C. Patterson
Screening for abdominal aortic aneurysm in men ages 60 to 80
years. A cost-effectiveness
analysis
Ann Intern Med, 119 (1993), pp. 411–416
F.A. Lederle, G.R. Johnson, S.E. Wilson, F.N. Littooy, W.C.
Krupski, D. Bandyk, et al.
Yield of repeated screening for abdominal aortic aneurysm
after a 4-year interval. Aneurysm
Detection and Management Veterans Affairs Cooperative Study
Investigators
Arch Intern Med, 160 (2000), pp. 1117–1121
http://-/?-http://-/?-http://-/?-http://-/?-http://-/?-http://-/?-http://-/?-http://-/?-http://-/?-http://-/?-http://-/?-http://-/?-http://-/?-
-
8/19/2019 Abdominal Aortic Aneurysm_ an Illustrated Narrative
Review
20/31
12/1/2016 Abdominal aortic aneurysm: an illustrated narrative
review
http://www.sciencedirect.com/science/article/pii/S0161475402541117
20
60
61
62
63
64
65
66
67
☆
About ScienceDirect Contact and support
Term s and condit ions P rivacy pol icy
C.B. Ernst
Current therapy for infrarenal aortic aneurysms
N Engl J Med, 336 (1997), pp. 59–60
W.E. Lloyd, P.S.K. Paty, R.C. Darling III, B.B. Chang, K.M.
Fitzgerald, R.P. Leather, et al.
Results of 1000 consecutive elective abdominal aortic aneurysm
repairs
Cardiovasc Surg, 4 (1996), pp. 724–726
D. Henderson, D. Chapman-Smith, S. Mior, H. Vernon
Guidelines for chiropractic practice in CanadaJ Can Chiropr
Assoc (Suppl 1) (1994), p. 38
J.H. Wedge, S. Tchang
Differential diagnosis of low back pain
C.V. Burton (Ed.), Managing low back pain (3rd ed), Churchill
Livingstone, New York (1992), pp. 225–
241
J.P. Weston
Chiropractic management of abdominal aortic aneurysm: a case
report
J Can Chiropr Assoc, 39 (1995), pp. 75–79
G. van der Velde
Abdominal aortic aneurysm: two case reports and a brief review
of its clinical characteristics
and ramifications
J Neuromusculoskeletal Sys, 6 (1998), pp. 76–83
J.D. Cassidy, W.H. Kirkaldy-Willis, H.W. Thiel
Manipulation
C.V. Burton (Ed.), Managing low back pain (3rd ed), Churchill
Livingstone, New York (1992), pp. 283–
296
K. Ecklund, G.G. Hartnell, L.A. Hughes, K.R. Stokes, J.P.
Finn
MR angiography as the sole method in evaluating abdominal aortic
aneurysms: correlation with
conventional techniques and surgery
Radiology, 192 (1994), pp. 345–350
Financial assistance was provided by The Division of Graduate
Studies and Research
at Canadian Memorial Chiropractic College.
Submit requests for reprints to: Dr. Colin Crawford, Department
of Complementary Medicine, PO Box
71, Bundoora 3083, Victoria, Australia
Copyright © 2003 Elsevier Science Inc. All rights reserved.
Copyright © 2016 Elsevier B.V. or its licensors or contributors.
ScienceDirect® is a registered trademark of Elsevier B.V.
Cookies are used by this site. To decline or learn more, visit
our Cookies page.
Switch to Mobile Site
Recommended articles
Abdominal aortic aneurysm
Abdominal Aortic Aneurysm Presenting as …
Diagnosis and Monitoring of Abdominal Ao…
2005, The Lancet more
2006, Journal of Manipulative and Physiological T…
more
http://-/?-http://-/?-http://-/?-http://-/?-http://-/?-http://-/?-http://-/?-http://-/?-http://www.sciencedirect.com/science/article/pii/S014628061000085Xhttp://www.sciencedirect.com/science/article/pii/S0161475406000832http://www.sciencedirect.com/science/article/pii/S0140673605664598https://www.elsevier.com/solutions/sciencedirect/support/cookieshttp://www.elsevier.com/privacypolicy?utm_source=sciencedirect&utm_medium=link&utm_campaign=privacyhttp://www.elsevier.com/locate/termsandconditions?utm_source=sciencedirect&utm_medium=link&utm_campaign=termshttp://www.sciencedirect.com/science/contactushttp://www.elsevier.com/solutions/sciencedirecthttp://www.elsevier.com/
-
8/19/2019 Abdominal Aortic Aneurysm_ an Illustrated Narrative
Review
21/31
12/1/2016 Abdominal aortic aneurysm: an illustrated narrative
review
http://www.sciencedirect.com/science/article/pii/S0161475402541117
2
View more articles »
2010, Current Problems in Cardiology more
Citing articles (17)
Related book content
http://www.sciencedirect.com/science/recommended-articles/S0161475402541117
-
8/19/2019 Abdominal Aortic Aneurysm_ an Illustrated Narrative
Review
22/31
12/1/2016 Abdominal aortic aneurysm: an illustrated narrative
review
http://www.sciencedirect.com/science/article/pii/S0161475402541117
22
-
8/19/2019 Abdominal Aortic Aneurysm_ an Illustrated Narrative
Review
23/31
-
8/19/2019 Abdominal Aortic Aneurysm_ an Illustrated Narrative
Review
24/31
12/1/2016 Abdominal aortic aneurysm: an illustrated narrative
review
http://www.sciencedirect.com/science/article/pii/S0161475402541117
24
-
8/19/2019 Abdominal Aortic Aneurysm_ an Illustrated Narrative
Review
25/31
12/1/2016 Abdominal aortic aneurysm: an illustrated narrative
review
http://www.sciencedirect.com/science/article/pii/S0161475402541117
25
-
8/19/2019 Abdominal Aortic Aneurysm_ an Illustrated Narrative
Review
26/31
12/1/2016 Abdominal aortic aneurysm: an illustrated narrative
review
http://www.sciencedirect.com/science/article/pii/S0161475402541117
26
-
8/19/2019 Abdominal Aortic Aneurysm_ an Illustrated Narrative
Review
27/31
12/1/2016 Abdominal aortic aneurysm: an illustrated narrative
review
http://www.sciencedirect.com/science/article/pii/S0161475402541117
27
-
8/19/2019 Abdominal Aortic Aneurysm_ an Illustrated Narrative
Review
28/31
12/1/2016 Abdominal aortic aneurysm: an illustrated narrative
review
http://www.sciencedirect.com/science/article/pii/S0161475402541117
28
-
8/19/2019 Abdominal Aortic Aneurysm_ an Illustrated Narrative
Review
29/31
12/1/2016 Abdominal aortic aneurysm: an illustrated narrative
review
http://www.sciencedirect.com/science/article/pii/S0161475402541117
29
-
8/19/2019 Abdominal Aortic Aneurysm_ an Illustrated Narrative
Review
30/31
-
8/19/2019 Abdominal Aortic Aneurysm_ an Illustrated Narrative
Review
31/31
12/1/2016 Abdominal aortic aneurysm: an illustrated narrative
review