Embed Size (px)
Citation preview

Electromyographic Analysis ofTraditional and NontraditionalAbdominal Exercises: Implicationsfor Rehabilitation and Training
Background and Purpose. Performing nontraditional abdominal exercises withdevices such as abdominal straps, the Power Wheel, and the Ab Revolutionizerhas been suggested as a way to activate abdominal and extraneous (non-abdominal) musculature as effectively as more traditional abdominal exer-cises, such as the crunch and bent-knee sit-up. The purpose of this study wasto test the effectiveness of traditional and nontraditional abdominal exercisesin activating abdominal and extraneous musculature. Subjects. Twenty-onemen and women who were healthy and between 23 and 43 years of age wererecruited for this study. Methods. Surface electromyography (EMG) was usedto assess muscle activity from the upper and lower rectus abdominis, externaland internal oblique, rectus femoris, latissimus dorsi, and lumbar paraspinalmuscles while each exercise was performed. The EMG data were normalizedto maximum voluntary muscle contractions. Differences in muscle activitywere assessed by a 1-way, repeated-measures analysis of variance. Results.Upper and lower rectus abdominis, internal oblique, and latissimus dorsimuscle EMG activity were highest for the Power Wheel (pike, knee-up, androll-out), hanging knee-up with straps, and reverse crunch inclined 30degrees. External oblique muscle EMG activity was highest for the PowerWheel (pike, knee-up, and roll-out) and hanging knee-up with straps. Rectusfemoris muscle EMG activity was highest for the Power Wheel (pike andknee-up), reverse crunch inclined 30 degrees, and bent-knee sit-up. Lumbarparaspinal muscle EMG activity was low and similar among exercises. Discus-sion and Conclusion. The Power Wheel (pike, knee-up, and roll-out), hangingknee-up with straps, and reverse crunch inclined 30 degrees not only were themost effective exercises in activating abdominal musculature but also were themost effective in activating extraneous musculature. The relatively high rectusfemoris muscle activity obtained with the Power Wheel (pike and knee-up),reverse crunch inclined 30 degrees, and bent-knee sit-up may be problematicfor some people with low back problems. [Escamilla RF, Babb E, DeWitt R,et al. Electromyographic analysis of traditional and nontraditional abdominalexercises: implications for rehabilitation and training. Phys Ther. 2006;86:656–671.]
Key Words: Back pain, Crunch, Electromyography, Lumbar spine, Normalization, Oblique musculature,
Rectus muscle, Sit-up.
Rafael F Escamilla, Eric Babb, Ryan DeWitt, Patrick Jew, Peter Kelleher, Toni Burnham, Juliann Busch,Kristen D’Anna, Ryan Mowbray, Rodney T Imamura
656 Physical Therapy . Volume 86 . Number 5 . May 2006
Rese
arch
Repo
rt �
���������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������
�����

Understanding how different abdominal exer-cises elicit muscle activity is useful to thera-pists and other health care or fitness special-ists who develop specific abdominal exercises
for their patients or clients to facilitate their rehabilita-tion or training needs and objectives. For example,abdominal exercises that actively flex the trunk may beproblematic for some people with lumbar disk patholo-gies because of increased intradiskal pressure1 and lum-bar spine compression2 as well as people with osteo-porosis because of the risk of vertebral compressionfractures.3 However, some of these same individuals maybe asymptomatic during abdominal exercises that resisttrunk extension and maintain a relatively neutral spineand pelvis. In contrast, some people with facet jointsyndrome, spondylolisthesis, and vertebral or interverte-bral foramen stenosis may not tolerate exercises thatextend the trunk.
Strong abdominal muscles help stabilize the trunk andunload lumbar spine stress.2,4 Abdominal muscles com-monly are activated by active flexion of the trunkthrough a concentric muscle contraction. Trunk flexionoccurs during traditional abdominal exercises, such asabdominal curl-up (crunch) or sit-up exercises, as aperson raises the head and shoulders off the floor froma supine position toward a sitting position. During thecrunch exercise, the hips remain at a constant angle andthe pelvis does not rotate. In contrast, during thebent-knee or extended-knee sit-up exercise, the hips flexand the pelvis rotates.5 Bent-knee and extended-kneesit-up exercises have been shown to be effective inactivating the rectus abdominis and internal and exter-nal oblique musculature.6–8 The crunch exercise hasbeen recommended in place of sit-up exercises becausethe crunch has been shown to activate abdominal mus-
culature as effectively as the sit-up but without therelatively high hip flexor activity that occurs during thesit-up.2,8–10
Nontraditional abdominal exercises activate abdominalmusculature in a manner different from that of tradi-tional crunch and sit-up exercises. An example of anontraditional exercise is performing the traditionalcrunch in reverse (reverse crunch), which involves flex-ing the trunk by posteriorly rotating the pelvis andflexing the hips. Nontraditional abdominal exercisesalso may involve resisting trunk extension (through anexternal force, such as gravity) through isometric oreccentric muscle contractions, such as maintaining apush-up position by keeping a neutral spine and pelvis.
Many nontraditional exercises also may be performedwith abdominal devices. Manufacturers of these abdom-inal devices often claim that their devices are moreeffective in activating abdominal musculature than aretraditional abdominal exercises. However, there are lim-ited electromyographic (EMG) data in the scientificliterature for nontraditional abdominal exercises, per-formed with or without devices. A limited number ofstudies compared selected abdominal muscle activitiesduring nontraditional abdominal exercises performedwith various commercially available abdominal strength-ening devices9,11–14; however, to our knowledge, nostudies have quantified abdominal muscle activities dur-ing exercises performed with the Power Wheel,* Ab
* Jon H Hinds, inventor of the Power Wheel and owner of Monkey BarGymnasium, 600 Williamson St, Suite K-2, Madison, WI 53703 (www.monkeybargym.com).
RF Escamilla, PT, PhD, CSCS, is Associate Professor, Department of Physical Therapy, California State University, Sacramento, 6000 J St,Sacramento, CA 95819-6020 (USA) ([email protected]). Address all correspondence to Dr Escamilla.
E Babb, PT, MPT, R DeWitt, PT, MPT, P Jew, PT, MPT, P Kelleher, PT, MPT, T Burnham, PT, MPT, J Busch, PT, MPT, K D’Anna, PT, MPT, andR Mowbray, PT, MPT, were students at California State University, Sacramento, at the time of the study.
RT Imamura, PhD, is Assistant Professor of Kinesiology and Health Science, California State University, Sacramento.
All authors provided concept/idea/research design, data collection and analysis, and consultation (including review of manuscript beforesubmission). Dr Escamilla, Mr Babb, Mr Jew, Mr Kelleher, Ms Burnham, Ms Busch, Ms D’Anna, Mr Mowbray, and Dr Imamura provided projectmanagement and subjects. Dr Escamilla provided facilities/equipment. The authors acknowledge Bobby and Jon Hinds of Lifeline International,Inc, and Ralf Leszinski of Buckhead Marketing and Distribution, LLC, for their support throughout this project. The authors affirm that they haveno financial affiliation (including research funding) or involvement with any commercial organization that has a direct financial interest in anymatter included in the article.
This research was presented as a poster presentation at the 2004 California Physical Therapy Association Annual Conference; October 2004;Anaheim, Calif.
The protocol used in this study was approved by the Institutional Review Board of California State University, Sacramento.
This article was received March 22, 2005, and was accepted December 7, 2005.
Physical Therapy . Volume 86 . Number 5 . May 2006 Escamilla et al . 657

Revolutionizer,† and hanging-strap devices, which alsoare marketed for abdominal muscle strengthening.
Many traditional or nontraditional abdominal exercisesalso may activate extraneous (nonabdominal) muscles,such as the hip flexor and lumbar paraspinal muscula-ture, a result that may or may not be beneficial. Forexample, high activation levels from the hip flexor andlumbar paraspinal muscles tend to generate a forcecouple that attempts to anteriorly rotate the pelvis andincrease lumbar lordosis as well as to increase L4–L5compression; when these conditions are coupled withweak abdominal musculature, the risk of low backpathologies increases.3 The efficacy of recruiting extra-neous musculature, such as lumbar paraspinal muscula-ture or upper- and lower-extremity musculature, cur-rently is unknown, because, to our knowledge, no studieshave reported extraneous muscle activity during non-traditional abdominal exercises.
The purpose of this study was to compare the effective-ness of traditional and nontraditional abdominal exer-cises in activating abdominal and extraneous muscula-ture. Traditional exercises included the crunch andbent-knee sit-up; nontraditional exercises included 2variations of the reverse crunch, 4 variations of exercisesperformed with the Ab Revolutionizer device, 3 varia-tions of exercises performed with the Power Wheeldevice, and 1 hanging knee-up exercise performed withan abdominal strap device. It was hypothesized thatsignificant differences would be found in both abdomi-nal and extraneous muscle activity with traditional andnontraditional abdominal exercises.
Method
SubjectsTo achieve the best EMG signal possible and to minimizethe attenuating effects of excess body fat on the EMGsignal, this study was limited to a convenience sample of21 healthy young subjects (10 men and 11 women) whohad age-related average or below-average body composi-tion, as reported in ACSM’s Guidelines for Exercise Testingand Prescription.15 Baseline skin-fold calipers (model68900‡) and appropriate regression equations were usedto assess body composition. Mean age, mass, height, andbody fat measurements are shown in Table 1. All subjectsprovided written informed consent in accordance withthe guidelines of the Institutional Review Board atCalifornia State University, Sacramento. Subjects wereexcluded from the study if they had a history of abdom-inal or back pain or were unable to perform all exercises
pain free and with proper form and technique for 12consecutive repetitions.
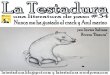
Exercise DescriptionsThe 10 nontraditional abdominal exercises were the AbRevolutionizer double crunch (Fig. 1A), Ab Revolution-izer oblique crunch (Fig. 1B), Ab Revolutionizer reversecrunch (Fig. 1C), Ab Revolutionizer reverse crunch withweights (Fig. 1D), hanging knee-up with straps (Fig. 2),Power Wheel pike (Fig. 3A), Power Wheel knee-up(Fig. 3B), Power Wheel roll-out (Fig. 3C), reverse crunchflat (Fig. 4A), and reverse crunch inclined 30 degrees(Fig. 4B). The 2 traditional abdominal exercises werethe bent-knee sit-up (Fig. 5) and the crunch (Fig. 6).Each subject had no prior experience in performing thenontraditional abdominal exercises and moderate experi-ence in performing the traditional abdominal exercises.
The Ab Revolutionizer exercises started and ended inthe supine position with the thumbs in the ears, thehands relaxed against the head, the trunk and headresting on the floor, the hips and knees flexed approx-imately 90 degrees, and the body positioned within theAb Revolutionizer device as shown in Figure 1. From thisstarting position, all 4 exercise variations of the AbRevolutionizer involved posterior pelvic tilt and flatten-ing of the lumbar spine attained through hips beingflexed 125 to 135 degrees. In addition to the posteriorpelvic tilt and hip flexion motions, a curl-up motion(attained by lifting the head and both scapulae off thefloor) was performed simultaneously during the AbRevolutionizer double crunch (Fig. 1A), and a left trunkrotation motion (attained by lifting the right scapula offthe floor and moving the right elbow toward the leftknee) was performed simultaneously during the AbRevolutionizer oblique crunch (Fig. 1B). Posterior pelvictilt and hip flexion were the primary motions thatoccurred during the Ab Revolutionizer reverse crunch(Fig. 1C) and the Ab Revolutionizer reverse crunch withweights (Fig. 1D), with the only difference between these2 variations being a higher intensity and difficulty levelwhen weights were used. The amount of weight used forthe Ab Revolutionizer reverse crunch with weights wasnormalized for all subjects by determining each subject’s20-repetition maximum weight for this exercise, whichwas based on recommendations from the manufacturerof the Ab Revolutionizer.
† Ralf Leszinski, Buckhead Marketing and Distribution, LLC ([email protected]).‡ Country Technology Inc, PO Box 87, Gays Mill, WI 54631-0087.
Table 1.Subject Anthropometric and Body Composition Dataa
SexAge(y)
Mass(kg)
Height(cm)
Body Fat(%)
Male 29.6�5.9 82.5�11.5 178.0�6.8 12.5�2.8Female 26.0�3.3 58.6�4.9 164.8�4.1 17.7�1.7
a Data are reported as mean � standard deviation.
658 . Escamilla et al Physical Therapy . Volume 86 . Number 5 . May 2006
������
������
������
�����

The hanging knee-up with straps exercise started andended with the arms supported within the straps, theshoulders and elbows flexed approximately 90 degrees,and the body hanging in a vertical position with thetrunk, hips, and knees in full extension. From thisposition, the subject maximally flexed the hips, resultingin 125 to 135 degrees of hip and knee flexion and aposteriorly tilted pelvis (Fig. 2). A tester maintained 1hand on the lumbar spine throughout the movement toprevent the body from swaying back and forth.
The Power Wheel pike and power wheel knee-up exer-cises started and ended with the subject in the push-upposition (trunk, hips, knees, and elbows in full exten-sion, shoulders flexed 90°, and hands on the floorapproximately a shoulder width apart), the feet abovethe floor and attached to Power Wheel straps, and thewheel in a vertical position on the floor (Figs. 3A and3B). For the Power Wheel pike, from the starting posi-tion the wheel was rolled toward the hands as the subjectperformed a “body pike” by maximally flexing the hips
Figure 1.Abdominal exercises. (A) Ab Revolutionizer double crunch, (B) Ab Revolutionizer oblique crunch, (C) Ab Revolutionizer reverse crunch, (D) AbRevolutionizer reverse crunch with weights.
Physical Therapy . Volume 86 . Number 5 . May 2006 Escamilla et al . 659

(resulting in 110°–120° of hip flexion and a posteriorlytilted pelvis) while maintaining an extended-knee posi-tion (Fig. 3A). For the Power Wheel knee-up, from thestarting position the wheel was rolled toward the handsas the subject maximally flexed the hips and knees(resulting in 125°–135° of hip and knee flexion and aposteriorly tilted pelvis) (Fig. 3B).
The Power Wheel roll-out exercise started and ended inthe quadruped position (on hands and knees with hipsand shoulders flexed approximately 90°) with a neutralspine and pelvis. From this position, the subject straight-ened out the body by rolling forward in a straight linewhile maintaining a neutral spine and pelvis (Fig. 3C).
The reverse crunch flat and reverse crunch inclined 30degrees started and ended in the supine position on aflat surface (reverse crunch flat) or on a surface inclined30 degrees from horizontal (reverse crunch inclined30°), with hips and knees flexed approximately 90degrees and the arms positioned as shown in Figure 4.From this starting position, the subject maximally flexedthe hips (resulting in 125°–135° of hip and knee flexionand a posteriorly tilted pelvis) (Fig. 4).
The crunch and bent-knee sit-up exercises started andended in a supine position with the thumbs positionedin the ears, the hands relaxed against the head, the
knees flexed approximately 90 degrees, and the hipsflexed approximately 45 degrees. During the crunch, thesubject flexed the trunk by performing a curling-upmotion until both scapulae were off the floor (Fig. 5).During the bent-knee sit-up, the feet were supported,and the subject simultaneously flexed the trunk and hipsuntil the elbows were even with the knees (Fig. 6).
ProcedureAll subjects became familiar with and practiced allabdominal exercises during a pretesting session thattook place approximately 1 week before the testingsession. During this time, each subject received instruc-tional sessions explaining how to perform each of theabdominal exercises correctly (each abdominal devicecame with written or video instructions for its use). Allexercises were performed with a 3-second cadence(1 second from start of exercise to end range, 1-secondisometric hold at end range, 1 second to return tostarting position) and a 1-second rest between repeti-tions. The subjects practiced multiple repetitions foreach exercise under the supervision of trained researchpersonnel. A metronome (set at 1 beat per second) wasused to help ensure proper cadence during both thepretesting and the testing sessions. Once a subject wasable to perform each exercise correctly with the propercadence, a testing session was scheduled.
Blue Sensor disposable surface electrodes (type M-00-S§)were used to collect EMG data. These oval electrodes(22 mm wide and 30 mm long) were placed in a bipolarelectrode configuration along the longitudinal axis of amuscle, with a center-to-center distance of approxi-mately 3 cm between electrodes. Before the electrodeswere positioned over each muscle, the skin was preparedby shaving, abrading, and cleaning with isopropyl alco-hol wipes to reduce skin impedance values, which typi-cally were �10 k�. Electrode pairs then were placed onthe subject’s right side (except for the internal obliquemuscle electrode pair, which was positioned on thesubject’s left side because the rotational function of theinternal oblique muscle is opposite that of the externaloblique muscle) for the following muscles in accordancewith procedures previously described16–19:
(1) upper rectus abdominis—positioned vertically andcentered on the muscle belly (not on the tendinousintersection) near the midpoint between the umbi-licus and the xiphoid process and 3 cm lateral fromthe midline;
(2) lower rectus abdominis—positioned 8 degrees fromvertical in the inferomedial direction and centeredon the muscle belly near the midpoint between the
§ Ambu Inc, 611 N Hammonds Ferry Rd, Linthicum, MD 21090-1356.
Figure 2.Abdominal exercise. Hanging knee-up with straps.
660 . Escamilla et al Physical Therapy . Volume 86 . Number 5 . May 2006
������
������
������
�����

umbilicus and the pubic symphysis and 3 cm lateralfrom the midline;
(3) external oblique—positioned obliquely approxi-mately 45 degrees (parallel to a line connecting themost inferior point of the costal margin of the ribsand the contralateral pubic tubercle) above theanterior superior iliac spine (ASIS) at the level ofthe umbilicus;
(4) internal oblique—positioned horizontally 2 cminferomedial to the ASIS within a triangle outlinedby the inguinal ligament, the lateral border of therectus sheath, and a line connecting the ASISs;
(5) latissimus dorsi—positioned obliquely (approxi-mately 25° from horizontal in the inferomedialdirection) 4 cm below the inferior angle of thescapula;
(6) rectus femoris—positioned vertically near the mid-line of the thigh, approximately halfway between theASIS and the proximal patella; and
(7) lumbar paraspinal—positioned vertically 3 cm lat-eral to the spine and near the level of the iliac crestbetween the L3 and L4 vertebrae. A ground (refer-ence) electrode was positioned over the skin of theright acromion. Electrode cables were connected tothe electrodes and taped to skin appropriately tominimize pull on the electrodes and movement ofthe cables.
Once the electrodes were positioned, the subjectwarmed up and practiced the exercises as needed, andthen data collection commenced. The EMG data werecollected by use of a Myosystem EMG unit.� The ampli-fier bandwidth frequency was 10 to 500 Hz, with an input
� Noraxon USA Inc, 13430 N Scottsdale Rd, Suite 104, Scottsdale, AZ 85254.
Figure 3.Abdominal exercises. (A) Power Wheel pike, (B) Power Wheel knee-up, (C) Power Wheel roll-out.
Physical Therapy . Volume 86 . Number 5 . May 2006 Escamilla et al . 661

voltage of 12 V (direct current) at 1.5 A.The input impedance of the amplifierwas 20,000 k�, and the common-moderejection ratio was 130 dB. The EMGdata were sampled at 1,000 Hz, and therecorded signals were processedthrough an analog-to-digital converterby use of a 16-bit analog-to-digitalboard.
The EMG data were collected during 5repetitions of each exercise, with allexercises being performed in a ran-domized order. Each repetition wasperformed in a slow and controlledmanner with the 3-second cadence pre-viously described and a 1-second restbetween repetitions. With the relativelysmall number of repetitions per-formed, all subjects acknowledged thatfatigue was minimal. A testing sessiontook 30 to 45 minutes to complete.
Randomly interspersed within the exer-cise testing session, EMG data fromeach muscle tested were collected dur-ing two 5-second maximum voluntary
Figure 4.Abdominal exercises. (A) Reverse crunch flat, (B) Reverse crunch inclined 30 degrees.
Figure 5.Abdominal exercise. Bent-knee sit-up.
662 . Escamilla et al Physical Therapy . Volume 86 . Number 5 . May 2006
������
������
������
�����

isometric contractions (MVICs). After conducting pilotwork, we adopted for MVIC testing the following proto-cols, which were based on the positions that elicited thehighest MVIC for each respective muscle (all MVICswere collected on a plinth with the subject in a prone,supine, or short sitting position):
(1) upper and lower rectus abdominis—body supinewith hips and knees flexed 90 degrees, feet sup-ported, and trunk maximally flexed (ie, curl-upposition), with resistance at the shoulders in thetrunk extension direction;
(2) external and internal oblique—body supine withhips and knees flexed 90 degrees, feet supported,and trunk maximally flexed and rotated to the left,with resistance at the shoulders in the trunk exten-sion and right rotation directions;
(3) latissimus dorsi—body prone with right shoulderabducted 0 degrees and extended maximally, withresistance at the right distal arm in the direction ofshoulder flexion;
(4) lumbar paraspinal—body prone with trunk fullyextended and hands clasped behind head, withresistance at the shoulders in the direction of trunkflexion; and
(5) rectus femoris—body in short sitting position withhips and knees flexed 90 degrees, with resistance atthe distal leg in the knee flexion direction.
The MVICs were collected to normalize the EMG datafrom the abdominal exercises in order for the activity ofa muscle during exercise to be compared with theactivity of that same muscle during MVIC. Subjects weregiven similar verbal encouragements for each of theMVICs to help ensure a maximum effort throughout the5-second duration, and the subjects was asked after each
MVIC if they thought it required max-imum effort. If not, the MVIC wasrepeated. Approximately 1 minute ofrest was given between the MVICs,and approximately 2 minutes of restwere given between the exercise trials.
Data ProcessingRaw EMG signals were full-wave recti-fied, smoothed with a 10-millisecondmoving average window, and thenaveraged over the entire duration ofeach exercise repetition or MVIC per-formed. For each repetition, the EMGdata were normalized for each muscleand expressed as a percentage of the
EMG data for a subject’s highest corresponding MVICtrial, determined by calculating throughout the 5-secondMVIC the highest average EMG signal over a 1-secondinterval. Normalized EMG data then were averaged overthe 5 repetition trials performed for each exercise andused in statistical analyses.
Data AnalysisA 1-factor, repeated-measures analysis of variance wasused to assess differences in normalized EMG muscleactivity among the different exercise variations, and posthoc analyses were performed with the Bonferroni test toevaluate the significance of between-exercise pair-wisecomparisons. The significance level was set at P�.01.
ResultsNormalized EMG data for each muscle and exercise areshown in Table 2. Among all exercises tested, upperrectus abdominis muscle EMG activity was highest forthe Power Wheel roll-out, hanging knee-up with straps,and reverse crunch inclined 30 degrees and lowest forthe Ab Revolutionizer reverse crunch. Lower rectusabdominis muscle EMG activity was highest for thePower Wheel roll-out and hanging knee-up with strapsand lowest for the Ab Revolutionizer reverse crunch.Graphical representations of upper and lower rectusabdominis muscle activity ranked from highest to lowestamong all exercises are shown in Figures 7 and 8.
External oblique muscle EMG activity was highest for thePower Wheel pike, Power Wheel knee-up, and hangingknee-up with straps and lowest for the crunch. Internaloblique EMG activity was highest for the Power Wheelroll-out, Power Wheel pike, Power Wheel knee-up, hang-ing knee-up with straps, and reverse crunch inclined 30degrees and lowest for the 7 remaining exercises. Graph-ical representations of external and internal obliquemuscle activity ranked from highest to lowest among allexercises are shown in Figures 9 and 10.
Figure 6.Abdominal exercise. Crunch.
Physical Therapy . Volume 86 . Number 5 . May 2006 Escamilla et al . 663

Table
2.
Elec
trom
yogr
aphi
c(E
MG
)Act
ivity
for
Each
Mus
cle
and
Exer
cise
Expr
esse
das
aPe
rcen
tage
ofth
eM
axim
umIso
met
ricVo
lunt
ary
Con
tract
ion
Exer
cise
Musc
le
Upper
Rec
tus
Abdom
inis
*Lo
wer
Rec
tus
Abdom
inis
*Ex
tern
al
Obliq
ues
*In
tern
al
Obliq
ues
*La
tiss
imus
Dors
i*Lu
mbar
Para
spin
als
*Rec
tus
Fem
ori
s*
Pow
erW
heel
roll-
out
76�
2681
�29
64�
27b
66�
2515
�7b
,c,f
5�2b
,c,d
,e6�
4b,c
,d,e
,h,i
Pow
erW
heel
pike
41�
11a,d
,e,g
53�
16a,d
96�
3283
�31
27�
168�
326
�11
c
Pow
erW
heel
knee
-up
41�
18a,d
,e,g
45�
12a,d
80�
3072
�32
25�
128�
443
�18
Han
ging
knee
-up
with
strap
s69
�21
75�
1679
�25
85�
4021
�12
7�3
15�
8b,c
Reve
rse
crun
chin
clin
ed30
°77
�27
53�
13a,d
50�
19b,c
,d86
�37
14�
8b,c
,f8�
422
�12
c
Reve
rse
crun
chfla
t41
�20
a,d
,e,g
30�
13a,b
,c,d
,e,g
39�
16a,b
,c,d
52�
24b,c
,d,e
23�
146�
3b,c
,e11
�5b
,c,e
,h
Cru
nch
56�
17a,e
48�
13a,d
27�
16a,b
,c,d
,e,h
,i,k
42�
10b,c
,d,e
5�3a
,b,c
,d,e
,f3�
1b,c
,d,e
,f,h
,i3�
3b,c
,d,e
,h,i
Bent
-kne
esi
t-up
39�
9a,d
,e,g
38�
11a,b
,d,e
50�
16b,c
,d49
�22
b,c
,d,e
6�3a
,b,c
,d,f
6�3b
,c,e
22�
12c
Ab
Revo
lutio
nize
rre
vers
ecr
unch
with
wei
ghts
44�
18a,d
,e40
�17
a,b
,d,e
55�
24b,c
,d51
�22
b,c
,d,e
4�2a
,b,c
,d,e
,f6�
3b,c
,e16
�13
b,c
Ab
Revo
lutio
nize
rdo
uble
crun
ch53
�17
a,e
40�
16a,b
,d,e
34�
18a,b
,c,d
,i51
�25
b,c
,d,e
4�2a
,b,c
,d,e
,f4�
2b,c
,d,e
,f,h
,i7�
6b,c
,d,e
,h,i
Ab
Revo
lutio
nize
rob
lique
crun
ch49
�14
a,d
,e39
�12
a,b
,d,e
49�
20b,c
,d48
�25
b,c
,d,e
7�3a
,b,c
,d,f
4�2b
,c,d
,e,f,h
,i5�
5b,c
,d,e
,h,i
Ab
Revo
lutio
nize
rre
vers
ecr
unch
30�
13a,d
,e,g
,i,j,k
24�
10a,b
,c,d
,e,g
,h,i,j,k
38�
16a,b
,c,d
33�
19b,c
,d,e
3�2a
,b,c
,d,e
,f4�
2b,c
,d,e
,f,h
,i6�
5b,c
,d,e
,h,i
*T
her
ew
asa
sign
ific
ant
diff
eren
ce(P
�.0
01)
inE
MG
acti
vity
amon
gth
eab
dom
inal
exer
cise
s.
Pair
-wis
eco
mpa
riso
ns
(P�
.01)
:a
Sign
ific
antl
yle
ssE
MG
acti
vity
than
obta
ined
wit
hth
ePo
wer
Wh
eel
roll-
out.
bSi
gnif
ican
tly
less
EM
Gac
tivi
tyth
anob
tain
edw
ith
the
Pow
erW
hee
lpi
ke.
cSi
gnif
ican
tly
less
EM
Gac
tivi
tyth
anob
tain
edw
ith
the
Pow
erW
hee
lkn
ee-u
p.d
Sign
ific
antl
yle
ssE
MG
acti
vity
than
obta
ined
wit
hth
eh
angi
ng
knee
-up
wit
hst
raps
.e
Sign
ific
antl
yle
ssE
MG
acti
vity
than
obta
ined
wit
hth
ere
vers
ecr
unch
incl
ined
30de
gree
s.fSi
gnif
ican
tly
less
EM
Gac
tivi
tyth
anob
tain
edw
ith
the
reve
rse
crun
chfl
at.
gSi
gnif
ican
tly
less
EM
Gac
tivi
tyth
anob
tain
edw
ith
the
crun
ch.
hSi
gnif
ican
tly
less
EM
Gac
tivi
tyth
anob
tain
edw
ith
the
ben
t-kn
eesi
t-up.
iSi
gnif
ican
tly
less
EM
Gac
tivi
tyth
anob
tain
edw
ith
the
Ab
Rev
olut
ion
izer
reve
rse
crun
chw
ith
wei
ghts
.jSi
gnif
ican
tly
less
EM
Gac
tivi
tyth
anob
tain
edw
ith
the
Ab
Rev
olut
ion
izer
doub
lecr
unch
.k
Sign
ific
antl
yle
ssE
MG
acti
vity
than
obta
ined
wit
hth
eA
bR
evol
utio
niz
erob
lique
crun
ch.
lSi
gnif
ican
tly
less
EM
Gac
tivi
tyth
anob
tain
edw
ith
the
Ab
Rev
olut
ion
izer
reve
rse
crun
ch.
664 . Escamilla et al Physical Therapy . Volume 86 . Number 5 . May 2006
������
������
������
�����

Latissimus dorsi muscle EMG activity was highest for thePower Wheel pike, Power Wheel knee-up, hangingknee-up with straps, and reverse crunch flat and lowestfor the crunch, Ab Revolutionizer double crunch, AbRevolutionizer reverse crunch, and Ab Revolutionizerreverse crunch with weights. Lumbar paraspinal muscleEMG activity was highest for the Power Wheel pike,Power Wheel knee-up, hanging knee-up with straps, andreverse crunch inclined 30 degrees and lowest for thecrunch, Ab Revolutionizer double crunch, Ab Revolu-tionizer reverse crunch, and Ab Revolutionizer obliquecrunch. Rectus femoris muscle EMG activity was highestfor the Power Wheel knee-up and lowest for the PowerWheel roll-out, crunch, Ab Revolutionizer doublecrunch, Ab Revolutionizer reverse crunch, and Ab Rev-olutionizer oblique crunch.
Discussion
Biomechanical Differences Between Trunk Flexion andExtension ExercisesUnderstanding biomechanical differences between exer-cises is important because trunk flexion, like that used intraditional exercises, such as the crunch or bent-kneesit-up, may be a contraindication or precaution in cer-tain populations (eg, those with lumbar disk pathologiesor osteoporosis). In such individuals, it may be morebeneficial to maintain a neutral pelvis and spine, like
that used in the Power Wheel roll-out, than to useforceful flexion of the lumbar spine, like that used in thebent-knee sit-up. In contrast, some people with facetjoint pain, spondylolisthesis, and vertebral or interverte-bral foramen stenosis may not benefit from exercisesthat maintain the spine and pelvis in a neutral orextended position, because these exercises may contrib-ute to spinal cord or nerve root compression. However,trunk flexion exercises, such as the crunch or reversecrunch, may decrease facet joint pain and increasevertebral or intervertebral foraminal openings, decreas-ing the risk of spinal cord or nerve root impingement.
Although the Power Wheel roll-out and hangingknee-up with straps were both effective in activatingabdominal musculature, these 2 exercises were per-formed in different manners. During the roll-out por-tion of the Power Wheel roll-out exercise, the abdominalmusculature contracts eccentrically or isometrically toresist the attempt of gravity to extend the trunk androtate the pelvis. During the return motion, the abdom-inal musculature contracts concentrically or isometri-cally. If the pelvis and spine are stabilized and main-tained in a neutral position throughout the roll-out andreturn movements, then the abdominal musculaturecontracts primarily isometrically. While subjects wereperforming the roll-out exercise, a relatively neutralpelvis and spine were maintained throughout the move-
Figure 7.Upper rectus abdominis muscle normalized electromyographic (EMG) activity (mean � SD) among exercises. MVIC�maximum voluntary isometriccontraction, deg�degrees, Ab Rev�Ab Revolutionizer, Wts�weights.
Physical Therapy . Volume 86 . Number 5 . May 2006 Escamilla et al . 665

ments. In contrast, during the hanging knee-up exercisewith straps, the abdominal musculature contracts con-centrically initially as the hips flex, the pelvis rotatesposteriorly, and the lumbar spine is flattened and movestoward lumbar flexion. As the knees are lowered and thehips are extended, the reverse movements occur, andthe abdominal musculature contracts eccentrically tocontrol the rate of return to the starting position.
The hanging knee-up with straps exercise and the PowerWheel pike and Power Wheel knee-up exercises all wereperformed similarly by flexing the hips, posteriorly ro-tating the pelvis, and flattening the lumbar spine—basically the reverse of what occurs during the crunchand bent-knee sit-up exercises, which involve trunkflexion followed by hip flexion (bent-knee sit-up only).One limitation to the hanging knee-up with strapsexercise is the occurrence of relatively high L4–L5 diskcompression.2 However, L4–L5 disk compression hasbeen shown to be slightly higher in the bent-knee sit-upexercise than in the hanging knee-up with straps exer-cise.2 Furthermore, in the present study, EMG valuesfrom the upper and lower rectus abdominis and internal
and external oblique muscles all were significantlyhigher in the hanging knee-up with straps exercise thanin the bent-knee sit-up exercise. Therefore, the hangingknee-up with straps exercise may be preferred over thebent-knee sit-up exercise for more fit individuals whowant to elicit a high-level challenge to the abdominalmusculature. Neither exercise, however, may be appro-priate for some people with low back pathologiesbecause of the relatively high L4–L5 compression.
In general, all exercise variations of the Ab Revolution-izer device produced abdominal muscle activity similarto that produced by the crunch, bent-knee sit-up, andreverse crunch flat exercises. Therefore, purchasing thisabdominal device does not appear to offer any advan-tage in recruiting abdominal musculature over perform-ing traditional exercises that require no additionalequipment, such as the crunch, bent-knee sit-up, andreverse crunch flat exercises. However, one advantage ofthe Ab Revolutionizer device is that external weight canbe added, thereby allowing exercise intensity to bevaried. The reverse crunch flat and Ab Revolutionizerreverse crunch exercises were performed nearly identi-
Figure 8.Lower rectus abdominis muscle normalized electromyographic (EMG) activity (mean � SD) among exercises. MVIC�maximum voluntary isometriccontraction, deg�degrees, Ab Rev�Ab Revolutionizer, Wts�weights.
666 . Escamilla et al Physical Therapy . Volume 86 . Number 5 . May 2006
������
������
������
�����

cally, with the only difference being that the reversecrunch flat exercise was performed without the use of anabdominal device.
Biomechanical Differences Between Crunch andBent-Knee Sit-up ExercisesNot all abdominal exercises involve the same degree offlexion of the lumbar spine. Halpern and Bleck7 dem-onstrated that lumbar spinal flexion was only 3 degreesduring the crunch exercise but was approximately 30degrees during the bent-knee sit-up exercise. In addi-tion, the bent-knee sit-up exercise has been shown togenerate greater lumbar intradiskal pressure1,20 andcompression2 than have exercises similar to the crunchexercise, largely because of increased lumbar flexionand muscle activity from the rectus femoris and psoasmuscles.8,10 These findings suggest that the crunch exer-cise may be a safer exercise to perform than the bent-knee sit-up exercise for some people who need tominimize lumbar spinal flexion or compressive forcesbecause of lumbar pathologies.2
Although both the crunch and the bent-knee sit-upexercises were effective in recruiting abdominal muscu-lature, there were some differences. Several studies,including the present study, have shown that externaloblique muscle activity and, to a lesser extent, internaloblique muscle activity are significantly greater in thebent-knee sit-up exercise than in the crunch exer-cise.2,8,21,22 However, upper and lower rectus abdominismuscle activity have been shown to be greater in thecrunch exercise than in the bent-knee sit-up exercise.7,9
In addition, rectus femoris and psoas muscle activityhave been shown to be greater in the bent-knee sit-upexercise than in the crunch exercise,8,10 findings that areconsistent with the rectus femoris muscle EMG datafrom the present study. Increased muscle activity fromthe rectus femoris and psoas muscles may exacerbate lowback pain in some people with low back pathologies.
Abdominal and Oblique Muscle Recruitment in Crunchand Reverse Crunch ExercisesThere are beliefs that performing reverse crunch exer-cises activates the lower abdominal muscles to a greater
Figure 9.External oblique muscle normalized electromyographic (EMG) activity (mean � SD) among exercises. MVIC�maximum voluntary isometriccontraction, deg�degrees, Ab Rev�Ab Revolutionizer, Wts�weights.
Physical Therapy . Volume 86 . Number 5 . May 2006 Escamilla et al . 667

extent than does performing crunch exercises and thatperforming crunch exercises activates the upper abdom-inal muscles to a greater extent than does performingreverse crunch exercises, but the results from thepresent study do not substantiate these beliefs. In acomparison of the crunch and reverse crunch flat exer-cises, both upper and lower rectus abdominis muscleEMG activity were significantly greater during thecrunch, whereas the external and internal oblique mus-cle EMG activity were not significantly different betweenthe 2 exercises. Our data are similar to the findingsreported by Clark et al11 but different from the abdom-inal muscle EMG data reported by Willett et al,23 whofound greater lower rectus abdominis and externaloblique muscle activity with the reverse crunch exercisethan with the crunch exercise. These discrepancies mayhave been attributable to methodological differencesamong the studies. For example, in the study of Willettet al,23 the reverse crunch exercise was performed byhaving subjects raise the lower half of the body off thetable as far as possible, whereas in the present study,subjects were instructed to maximally posteriorly tilt thepelvis and flex the hips. However, significantly greaterupper rectus abdominis, internal oblique, and external
oblique muscle activity was seen when the reverse crunchinclined 30 degrees was performed rather than thecrunch exercise, but the lower rectus abdominis muscleactivity was not significantly different between the 2exercises.
Role of Abdominal Muscles in Trunk StabilityThe role of the abdominal muscles, especially the trans-verse abdominal and internal oblique muscles, inenhancing spinal and pelvic stabilization and increasingintra-abdominal pressure is well known.24–28 Intra-abdominal pressure unloads the spine by generating atrunk extensor moment and tensile loading to the spineand reduces spinal axial compression and shear loads.29
The attachments of the transverse abdominal and inter-nal oblique muscles to the thoracolumbar fascia furtherenhance spinal and pelvic stabilization, because whenthese muscles contract, they tense the thoracolumbarfascia. The transverse abdominal muscle, which is thedeepest of the abdominal muscles, exhibits a muscleactivation pattern and an amplitude similar (within15%) to those of the internal oblique muscle duringmany of the same trunk flexion movements as those usedin the present study.8,18 The highest EMG activity from
Figure 10.Internal oblique muscle normalized electromyographic (EMG) activity (mean � SD) among exercises. MVIC�maximum voluntary isometriccontraction, deg�degrees, Ab Rev�Ab Revolutionizer, Wts�weights.
668 . Escamilla et al Physical Therapy . Volume 86 . Number 5 . May 2006
������
������
������
�����

the internal oblique muscle was obtained with the fol-lowing exercises: the Power Wheel roll-out, Power Wheelpike, Power Wheel knee-up, hanging knee-up withstraps, and reverse crunch inclined 30 degrees; thesedata suggest that these exercises also may offer moreeffective stabilization to the spine and pelvis than mayother exercises used in the present study, assuming thattransverse abdominal muscle activity is similar to internaloblique muscle activity during these exercises.
Exercise IntensityThe exercises used in the present study provide acontinuum of lower- to higher-intensity exercisesthrough which patients or clients can progress within atraining or rehabilitation program. Exercises involvingthe Ab Revolutionizer and abdominal crunch typicallywere easier for the subjects to perform than were exer-cises involving the hanging knee-ups with straps, PowerWheel pike and knee-up, and reverse crunch inclined 30degrees. However, because external weights could beadded to the Ab Revolutionizer, this exercise could beused to allow a person to progress from lower- tohigher-intensity exercises. The subjects participating inthe present study were all relatively young, active peoplewho were all able to perform both easier and moredifficult abdominal exercises. However, older, less active,or weaker people or people with trunk pathologies maynot be able to perform the more difficult exercises usedin the present study correctly. These higher-intensityexercises may be reserved for more fit patients andclients, such as athletes who are involved in rehabilita-tion and whose desire is to return to playing sports.
Extraneous (Nonabdominal) Muscle ActivityTo our knowledge, no studies have reported extraneousmuscle activity for any of the exercises used in thepresent study, except for the traditional crunch andbent-knee sit-up exercises, for which rectus femoris andpsoas muscle activity have been reported.8,10,18 To ourknowledge, no studies have reported latissimus dorsi orlumbar paraspinal muscle activity for any of the exercisesused in the present study. Interestingly, the Power Wheelroll-out, Power Wheel pike, Power Wheel knee-up, hang-ing knee-up with straps, and reverse crunch inclined 30degrees exercises not only were the most effective exer-cises in activating abdominal musculature but also werethe most effective exercises in activating the latissimusdorsi muscle. However, all of these exercises, except forthe Power Wheel roll-out, also exhibited relatively highrectus femoris and lumbar paraspinal muscle activitycompared with the other exercises, a finding that may beproblematic for some people with low back pathologies.Therefore, the Power Wheel roll-out may be the mosteffective exercise in recruiting abdominal and latissimusdorsi musculature while minimizing rectus femoris andlumbar paraspinal muscle activity.
During the Power Wheel roll-out exercise, the latissimusdorsi muscle contracts eccentrically during the initialroll-out phase to control the rate of shoulder flexionattributable to gravity and concentrically in the returnphase as the shoulder extends. Although the rectusfemoris muscle appears to contract eccentrically duringthe initial roll-out phase (to control the rate of hipextension) and concentrically during the return phaseto aid in hip flexion, we did not expect to find very lowrectus femoris muscle activity during the Power Wheelroll-out exercise. Although the psoas muscle EMG mag-nitudes were not measured in the present study becauseit is a deep muscle, it has been demonstrated that duringexercises performed in a position and manner similar tothose of the Power Wheel roll-out exercise, psoas muscleEMG magnitudes are low and typically are withinapproximately 10% of rectus femoris muscle EMG mag-nitudes.8,18 From these data, it can be hypothesized thatboth psoas and rectus femoris muscle activity is relativelylow during the Power Wheel roll-out exercise and thatthe latissimus dorsi muscle may have a greater role thanthe rectus femoris and psoas muscles in controlling andcausing exercise movements during the Power Wheelroll-out exercise.
Because of the effectiveness of the Power Wheel roll-out,Power Wheel pike, Power Wheel knee-up, hangingknee-up with straps, and reverse crunch inclined 30degrees exercises in recruiting abdominal and extrane-ous musculature, these exercises may be beneficial forsome people who have limited workout time and whosegoal is to perform exercises that provide not only anabdominal workout but also more of a total-body work-out. The greater relative intensity and number of mus-cles used during these exercises suggest that theseexercises also may achieve a greater energy expenditurethan may other exercises used in the present study.Moreover, tension in the latissimus dorsi muscle inaddition to the internal oblique muscle (and presumablythe transverse abdominal muscle), each of which tensesthe thoracolumbar fascia, may enhance trunk stabiliza-tion during these exercises.
Performing exercises that recruit the rectus femoris andlumbar paraspinal muscles may not be advantageous forthose with weak abdominal muscles or lumbar instability,because the forces generated when these muscles con-tract act to anteriorly rotate the pelvis and increase thelordotic curve of the lumbar spine. Some people withweak abdominal muscles or lumbar instability may wantto avoid the bent-knee sit-up, Power Wheel pike, PowerWheel knee-up, and reverse crunch inclined 30 degreesexercises because of the relatively high rectus femorisand lumbar paraspinal muscle activity obtained withthese exercises compared with other exercises. In addi-tion, exercises performed in a manner similar to that of
Physical Therapy . Volume 86 . Number 5 . May 2006 Escamilla et al . 669

the aforementioned exercises exhibited psoas and ilia-cus muscle EMG magnitudes and recruitment patternssimilar to the EMG magnitudes and recruitment pat-terns of the rectus femoris muscle.18,21,22
These data suggest that the 3 primary hip flexors—thepsoas, iliacus, and rectus femoris muscles—may exhibitsimilar EMG recruitment patterns and magnitudes whenthe exercises used in the present study are performed.The psoas muscle, through its attachments to the lumbarspine, attempts to hyperextend the spine as it helps flexthe hip, and this action may be detrimental to somepeople with lumbar instability. In addition, it has beendemonstrated that the psoas muscle can generate lum-bar compression and anterior shear force at L5–S18,30;these effects may be problematic for some people withlumbar disk pathologies. Although muscle force fromthe lumbar paraspinal muscle also can increase thecompression of the lumbar spine, it should be noted thatall exercises used in the present study generated rela-tively low muscle activity (�10% of an MVIC) from thelumbar paraspinal muscle.
Effects of Electrode Placement on EMG Cross TalkThe electrode positions used in the present study havebeen shown to minimize EMG cross talk from othermuscles.15,17,19 This is especially true for the internaloblique muscle, the only muscle tested that was not asuperficial muscle. The internal oblique muscle nor-mally lies deep in relation to the external oblique muscleand therefore is susceptible to considerable EMG crosstalk from this muscle. However, it has been shown thatthe internal oblique muscle is covered only by theaponeurosis of the external oblique muscle and not theexternal oblique muscle, within the triangle outlined bythe inguinal ligament, the lateral border of the rectussheath, and a line connecting the ASISs.19 Therefore,surface electrodes appear to be appropriate for use withthe internal oblique muscle when electrode placement iswithin this area, especially when clinical questions arebeing considered and when a small percentage of EMGcross talk is acceptable. It was shown that for trunkflexion exercises similar to the exercises performed inthe present study, mean internal and external obliquemuscle EMG data obtained from surface electrodes wereonly approximately 10% different from mean internaland external oblique EMG data obtained from intramus-cular electrodes.18 These authors demonstrated thatappropriately placed surface electrodes accuratelyreflect (within 10%) the muscle activity within theinternal or external oblique muscle.
Correlation Between EMG Amplitude and Muscle ForceLinear, quasi-linear (nearly linear), and nonlinear cor-relations have been reported for EMG amplitude andmuscle force (strength) in the literature.31,32 In general,
the relationship between EMG amplitude and muscleforce is most linear during isometric contractions orduring activities in which muscle length is not changingrapidly, which is what occurred with the exercises used inthe present study. In contrast, the relationship betweenEMG amplitude and muscle force is most nonlinearduring activities in which muscles change length rapidlyor during muscle fatigue. Therefore, the clinicianshould be cautious when relating EMG amplitude tomuscle force and strength during dynamic exercises.
ConclusionThe exercises used in the present study activated abdom-inal muscles by flexing the trunk (crunch and bent-kneesit-up), by flexing the hips with posterior pelvis rotation(Power Wheel pike, Power Wheel knee-up, hangingknee-up with straps, reverse crunch inclined 30 degrees,reverse crunch flat, Ab Revolutionizer reverse crunchwith weights, and Ab Revolutionizer reverse crunch), bya combination of flexing the trunk and flexing the hipswith posterior pelvis rotation (Ab Revolutionizer doublecrunch and Ab Revolutionizer oblique crunch), and byresisting trunk extension (Power Wheel roll-out). ThePower Wheel roll-out exercise was the most effectiveexercise in activating abdominal and latissimus dorsimuscles while minimizing lumbar paraspinal and rectusfemoris muscle activity. The Power Wheel roll-out, PowerWheel pike, Power Wheel knee-up, hanging knee-upwith straps, and reverse crunch inclined 30 degreesexercises were the most effective exercises in recruitingboth abdominal musculature and extraneous muscula-ture. Although both the bent-knee sit-up and the crunchinvolved similar amounts of abdominal muscle activity,the crunch may be a safer exercise for people with lowback pathologies because of the relatively high rectusfemoris muscle activity. Moreover, the bent-knee sit-up,Power Wheel pike, Power Wheel knee-up, and reversecrunch inclined 30 degrees exercises may be problem-atic exercises for people with low back pathologiesbecause of the relatively high rectus femoris and lumbarparaspinal muscle activity.
References1 Nachemson A. Lumbar intradiscal pressure. In: Jayson MIV, ed. TheLumbar Spine and Back Pain. Edinburgh, Scotland: Churchill Living-stone; 1987:191–203.
2 Axler CT, McGill SM. Low back loads over a variety of abdominalexercises: searching for the safest abdominal challenge. Med Sci SportsExerc. 1997;29:804–811.
3 Ralston SH, Urquhart GD, Brzeski M, Sturrock RD. Prevalence ofvertebral compression fractures due to osteoporosis in ankylosingspondylitis. BMJ. 1990;300:563–565.
4 Gardner-Morse MG, Stokes IA. The effects of abdominal musclecoactivation on lumbar spine stability. Spine. 1998;23:86–91.
5 Ricci B, Marchetti M, Figura F. Biomechanics of sit-up exercises. MedSci Sports Exerc. 1981;13:54–59.
670 . Escamilla et al Physical Therapy . Volume 86 . Number 5 . May 2006
������
������
������
�����

6 Godfrey KE, Kindig LE, Windell EJ. Electromyographic study ofduration of muscle activity in sit-up variations. Arch Phys Med Rehabil.1977;58:132–135.
7 Halpern AA, Bleck EE. Sit-up exercises: an electromyographic study.Clin Orthop. 1979;145:172–178.
8 Juker D, McGill S, Kropf P, Steffen T. Quantitative intramuscularmyoelectric activity of lumbar portions of psoas and the abdominal wallduring a wide variety of tasks. Med Sci Sports Exerc. 1998;30:301–310.
9 Beim GM, Giraldo JL, Pincivero DM, et al. Abdominal strengtheningexercises: a comparative EMG study. Journal of Sport Rehabilitation.1997;6:11–20.
10 Guimaraes AC, Vaz MA, De Campos MI, Marantes R. The contri-bution of the rectus abdominis and rectus femoris in twelve selectedabdominal exercises: an electromyographic study. J Sports Med PhysFitness. 1991;31:222–230.
11 Clark KM, Holt LE, Sinyard J. Electromyographic comparison of theupper and lower rectus abdominis during abdominal exercises.J Strength Cond Res. 2003;17:475–483.
12 Demont RG, Lephart SM, Giraldo JL, et al. Comparison of twoabdominal training devices with an abdominal crunch using strengthand EMG measurements. J Sports Med Phys Fitness. 1999;39:253–258.
13 Sternlicht E, Rugg S. Electromyographic analysis of abdominalmuscle activity using portable abdominal exercise devices and atraditional crunch. J Strength Cond Res. 2003;17:463–468.
14 Warden SJ, Wajswelner H, Bennell KL. Comparison of Abshaperand conventionally performed abdominal exercises using surfaceelectromyography. Med Sci Sports Exerc. 1999;31:1656–1664.
15 Balady GJ, Berra KA, Golding LA, et al. ACSM’s Guidelines for ExerciseTesting and Prescription. Baltimore, Md: Lippincott Williams & Wilkins;2000:35–312.
16 Basmajian J, Blumenstein R. Electrode Placement in EMG Biofeedback.Baltimore, Md: Williams & Wilkins; 1980:79–86.
17 Cram J, Kasman G. Introduction to Surface Electromyography. Gaithers-burg, Md: Aspen Publishers Inc; 1998:273–374.
18 McGill S, Juker D, Kropf P. Appropriately placed surface EMGelectrodes reflect deep muscle activity (psoas, quadratus lumborum,abdominal wall) in the lumbar spine. J Biomech. 1996;29:1503–1507.
19 Ng JK, Kippers V, Richardson CA. Muscle fibre orientation ofabdominal muscles and suggested surface EMG electrode positions.Electromyogr Clin Neurophysiol. 1998;38:51–58.
20 Nachemson AL. The lumbar spine: an orthopaedic challenge. Spine.1976;1:59–71.
21 Andersson EA, Ma Z, Thorstensson A. Relative EMG levels intraining exercises for abdominal and hip flexor muscles. Scand J RehabilMed. 1998;30:175–183.
22 Andersson EA, Nilsson J, Ma Z, Thorstensson A. Abdominal and hipflexor muscle activation during various training exercises. Eur J ApplPhysiol Occup Physiol. 1997;75:115–123.
23 Willett GM, Hyde JE, Uhrlaub MB, et al. Relative activity of abdom-inal muscles during commonly prescribed strengthening exercises.J Strength Cond Res. 2001;15:480–485.
24 Thomson KD. Estimation of loads and stresses in abdominalmuscles during slow lifts. Proc Inst Mech Eng. 1997;211:271–274.
25 Richardson CA, Snijders CJ, Hides JA, et al. The relation betweenthe transversus abdominis muscles, sacroiliac joint mechanics, and lowback pain. Spine. 2002;27:399–405.
26 Hodges PW, Richardson CA. Contraction of the abdominal musclesassociated with movement of the lower limb. Phys Ther. 1997;77:132–142.
27 Cresswell AG, Blake PL, Thorstensson A. The effect of an abdomi-nal muscle training program on intra-abdominal pressure. Scand JRehabil Med. 1994;26:79–86.
28 Cresswell AG, Grundstrom H, Thorstensson A. Observations onintra-abdominal pressure and patterns of abdominal intra-muscularactivity in man. Acta Physiol Scand. 1992;144:409–418.
29 Daggfeldt K, Thorstensson A. The role of intra-abdominal pressurein spinal unloading. J Biomech. 1997;30:1149–1155.
30 Santaguida PL, McGill SM. The psoas major muscle: a threedimensional geometric study. J Biomech. 1995;28:339–345.
31 Lippold OC. The relation between integrated action potentials in ahuman muscle and its isometric tension. J Physiol. 1952;117:492–499.
32 Lawrence JH, DeLuca CJ. Myoelectric signal versus force relation-ship in different human muscles. J Appl Physiol. 1983;54:1653–1659.
Physical Therapy . Volume 86 . Number 5 . May 2006 Escamilla et al . 671














![Patologias Hepáticas Exclusivas da Gravidez · abdominais geralmente são vagas[4]. Patologias endócrinas como a cetoacidose diabética e o hipertiroidismo não transitório devem](https://img.pdfslide.us/doc/110x75/5c101a1609d3f2801b8c1b76/patologias-hepaticas-exclusivas-da-gravidez-abdominais-geralmente-sao-vagas4.jpg)