Embed Size (px)
Citation preview

CLOSED
trauma of
abdomen
Abdominal trauma is a
violation of the
anatomical integrity or
functional state of the
abdominal cavity organs,
retroperitoneal space and
pelvis caused by external
influence.

Prevalence Abdominal trauma in
peacetime is 0.5-1% of all
injuries. In wartime 4-5%.
In peacetime, closed injuries
prevail, ranging from 54.2% to
62%.
The lethality with closed
injuries of the peacetime
reaches 10-15%.
Causes of closed abdominal injuries:
1. Household injuries: falling from a height or falling on an obtuse hard object.
2. Injuries in the workplace.
3. Car accidents.

Clinical classification of Closed injury
І. By the prevalence (scale) of the injury:a) isolated trauma;b)combined trauma: in combination with
trauma of the head, spine, spinal cord, neck, chest, musculoskeletal system.
ІІ. By the nature of injury:a) the abdominal wall;b) the organs of the abdominal cavity;c) retroperitoneal space.
The symptoms of closed
trauma of abdomen
1. Contusion of abdominal
wall.
2. Intra-abdominal bleeding
3. Peritonitis.

ComplaintsAbdominal pain of different localization, intensity and irradiation.Vomiting is characteristic in the development of peritonitis. With blood if the esophagus and stomach are damaged.Gas retention and bowel movements develop with peritonitis, retroperitoneal hematoma.
Blood excretion from the rectum when it is damaged.Complaints related to intra-abdominal bleeding: weakness, dizziness, cold sweat.
Objective examination (Inspection)
With intra-abdominal hemorrhage: Skin and mucous are pale, cold sweat, cold sticky sweat.
Pulse is weak and rapid.
Arterial pressure decreased.
Frequent shallow breathing.
Patient's position is forced - semi-sitting (Fowler's), because the congestion of blood under the diaphragm causes the pain, besides that the patient can’t find a final position, he wants to move all the time (symptom of "tilting doll").
With peritonitis: Mucous membranes dry.
The anterior abdominal wall does not participate in the act of breathing.
The stomach is swollen (abdominal distension).

Objective examination (Palpation)Abdominal bleeding is characterized by pain, muscle tension in the anterior abdominal wall (sometimes weak, not pronounced).
Peritonitis is characterized by:Pain and tension of the muscles of the anterior abdominal wallShchetkin-Blumberg symptom - increased pain when pressing on the front abdominal wall followed by rapid finger-taking.Razdolsky symptom - soreness with percussion of the anterior abdominal wall.Kulenkampf symptom - soreness of Douglas space in digital rectal examination.
Objective examinationPercussion:
if the hollow organ damages, hepatic dullness will disappear (Spijanij′s symptom).
in the presence of fluid - dullness in the sloping places of the abdomen.Auscultation: with peritonitis may be no intestinal noises (Shlange symptom).Finger rectal examination (per rectum):
sharp tenderness of pelvic peritoneum.
rectal wall defects.
the presence of bone fragments with a fracture. of the pelvic bones.
the presence of blood.

Laboratory diagnostics
Clinical blood test:
Decrease in the level of erythrocytes,
hemoglobin with bleeding.
Leukocytosis with peritonitis.
Clinical analysis of urine: with a
trauma of the kidney - hematuria.
Additional diagnostic methods Ultrasonography abdominal cavity: the presence of free fluid in the abdominal cavity (blood) with the rupture of the parenchymalorgans.FGDS: to specify of damage to the stomach and duodenum.X-ray: free gas under the dome of the diaphragm, the presence of gas in the retroperitoneal cellulose. To clarify the damage, contrast examination methods are performed.Cystography: the flow of contrast into the abdominal cavity or into the peri-urinary bladder tissue when there is a rupture of the bladder and urethra.

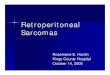
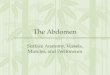
Computed tomography
The subcapsular rupture of
the spleen
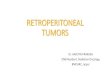
Survey radiography of the
ACO: free gas under the dome
of the diaphragm
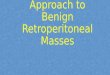
Additional diagnostic methods Laparocentesis is performed when it is impossible to exclude damage to the internal organs due to an unclear clinical picture, especially when combined craniocerebraltrauma and pronounced alcohol intoxication.
Laparoscopy. Study with a laparoscope.

Laparocentesis
Laparoscopy
First aid To drink is forbidden.
With closed damage, the administration of analgesics is contraindicated.
Emergency hospitalization is necessary.
If the condition is severe, venous access should be provided at the site of the incident and antishock therapy initiated.

Stages of surgical intervention Access. Laparotomy.
Stop bleeding. Bleeding is first stopped by pressing with your finger or clam ping the vascular pedicle, then clam ps are placed on the vessels and ligated.
Revision of the abdominal cavity. Revision begins with the stom ach. Further, the intestine and bladder are exam ined. Then they exam ine the parenchym al organs, retroperitoneal space.
Intervention on damaged organs. Sewing dam age, resection or removal of the organ.
Sanitation of the abdominal cavity. Rinse with warm isotonic sodium chloride solution.
Drainage of the abdominal cavity. All drains are removed through separate punctures in the abdom inal wall.
Laparotomic wound suturing. Produced in layers.