Embed Size (px)
Citation preview

ORIGINAL ARTICLE
ABCB1 G2677 Allele Is Associated with High Dose Requirement ofCyclosporin A to Prevent Renal Allograft Rejection in North India
Ranjana Singh, Pravin Kesarwani, Aneesh Srivastava, and Rama Devi Mittal
Department of Urology and Renal Transplantation, Sanjay Gandhi Post Graduate Institute of Medical Sciences,
Raebareli Road, Lucknow, Uttar Pradesh, India
Received for publication April 21, 2008; accepted June 19, 2008 (ARCMED-D-08-00176).
Background. Interindividual heterogeneity in expression of ABCB1 gene has been sus-pected to be one of the factors resulting in cyclosporin (CsA) pharmacokinetic variation.The present study explored the association of ABCB1 SNPs on CsA dose requirementsand dose-adjusted C2 levels (CsA level/daily dose requirement) in renal allograft recipients.
Methods. Daily doses (mg/kg/day) and dose-adjusted C2 levels (mg/mL per mg/kg/day)at 1 and 3 months for 155 recipients on CsA therapy were compared according to allelicstatus of ABCB1 c.1236COT, c. 2064-76TOA, c.2677GOT and c.3435COT.
Results. Dose-adjusted C2 levels were lower in ABCB1 c.2677GOT GG genotype ascompared to GT/TT genotypes at 1 and 3 months, suggesting that for a given dose theirCsA blood concentration is lower ( p 5 0.009 and p 5 0.043). GG genotype was furtherassociated with lower allograft survival as revealed by Kaplan-Meier analysis ( p 5 0.021).
Conclusions. Identification of ABCB12677GG patients may have a clinically significantimpact on allograft outcome and may be helpful in providing pre-transplant pharmacoge-netic information to individualize CsA dosing. � 2008 IMSS. Published by ElsevierInc.
Key Words: ABCB1 gene, P-glycoprotein (P-gp), Cyclosporin A, Renal transplantation.
Archives of Medical Research 39 (2008) 695e701
Introduction
Cyclosporin A (CsA) is a drug with a narrow therapeuticindex and poor oral bioavailability. It is widely used as animmunosuppressant in patients undergoing renal transplan-tation in India. As the pharmacokinetic characteristics ofCsA vary greatly among individuals, daily dose must be ad-justed to whole blood CsA concentrations to accomplishoptimal immunosuppressive effect as well as to limit toxic-ity. CsA is dosed according to blood concentrations, i.e., C2levels by therapeutic drug monitoring (1).
To achieve therapeutic CsA blood concentrations, wideinterindividual variability in dose requirement is observed.A study showing a relationship between rejection episodesand individual CsA pharmacokinetic profiles during the
Address reprint requests to: Dr. Rama Devi Mittal, Additional Profes-
sor (Biochemistry), Department of Urology, SGPGIMS, Raebareli Road,
Lucknow-226014, India; E-mail: [email protected] or rmittal@
sgpgi.ac.in
0188-4409/08 $esee front matter. Copyright � 2008 IMSS. Published by Eldoi: 10.1016/j.arcmed.2008.06.008
first 3 months post-transplant suggested that 27% of thetotal risk of rejection was attributable to O20% variationin dose-corrected CsA concentration (2). Among differentphysiological factors contributing to CsA pharmacokinet-ics, interindividual variation in genetic composition seemsto play a pivotal role.
CsA is a substrate of P-glycoprotein (P-gp), an ATP-dependent transmembrane transporter of xenobiotics ex-pressed at the surface of epithelial and lymphoid cells ofmany organs and tissues including proximal renal tubules(3). P-gp is encoded by ATP binding cassette subfamily Bmember 1 (ABCB1), also known as multidrug resistancegene MDR1, and was first described in cancer cells whereit extrudes chemotherapeutic agents out of the cell, therebyconferring multidrug resistance. The gatekeeper function ofP-gp in gut influences drug pharmacokinetics by extrudingCsA out of the gut wall into the intestinal lumen, limitingCsA bioavailability (4). Individual differences in activityand/or expression of the protein were shown to lead tochanges in drug bioavailability.
sevier Inc.

696 Singh et al. / Archives of Medical Research 39 (2008) 695e701
ABCB1 is a highly polymorphic gene with various singlenucleotide polymorphisms (SNPs) and some of these SNPsare known to be functionally relevant and can alter thepharmacokinetics of substrate drugs. They include ABCB1c.1236COT in exon 12, c.2064-76 TOA in intron 16,c.2677GOT in exon 21, and c.3435COT in exon 26.Among these ABCB1 c.3435COT (non-amino acidsubstituting) and ABCB1 c.2677GOT (ala893ser) havebeen associated with P-gp expression and function (5,6).
As the majority of allograft rejections occur during theinitial few months (1e3 months) after renal transplanteither due to under-immunosuppression or overdose of im-munosuppressant leading to toxicity, we attempted to eluci-date the influence of ABCB1 c.1236COT, c.2064e76TOA,c.2677GOT, and c.3435COT polymorphisms and theirhaplotypes on CsA daily dose requirement and dose-adjusted CsA levels (C2/dose ratio) at 1 and 3 month inrenal transplant recipients from North India.
Materials and Methods
Study Population
One hundred and fifty five renal allograft recipients whounderwent transplantation from live related kidney donorsat Sanjay Gandhi Post Graduate Institute (Lucknow, India)between 2004 and 2007 participated in the present study.Selection for transplantation was based on ABO bloodgroup compatibility, a negative complement-dependent cy-totoxicity cross-match using all historic positive and currentsera. Patients were molecular typed for human leukocyteantigen (HLA) class IA and B and class II DR and DQ an-tigens. All subjects received oral CsA (Neoral; NovartisPharmaceuticals Corp., Bern, Switzerland) formulation aspart of their immunosuppressive treatment consisting ofa combination of CsA as a calcineurin inhibitor with myco-phenolate mofetil/azathioprine as a purine inhibitor andprednisolone as a steroid. Initial dose of CsA was 8 mg/kg/day given in two equal doses. Daily dose was then adap-ted to blood CsA concentrations to achieve target C2 levelof 1.8 mg/mL at 1 week, which was subsequently reduced to1.6, 1.2, 1.0, and 0.8 after 1, 3, 6, 12 months, respectively.Steroid was given at a standard dosage regimen of 500 mgIV methylprednisolone at the time of surgery, 125 mg IVthe following day, and then 20 mg of prednislolone daily.Any other medication interfering with CsA drug metabo-lism was not prescribed to these subjects during the studyperiod. Demographic and clinical characteristics of patientsare presented in Table 1.
Allograft outcome based on rejection episode and stablegraft function of all the recipients was studied. Maximumfollow-up period was 36 months. Thirty one patients expe-rienced biopsy-proven acute (n 5 25)/chronic rejection(n 5 6) during the post-transplant period. All biopsies werereviewed by a renal pathologist, and Banff 97 working
classification criteria were used in the histological classifi-cation of biopsies (7). Three patients experienced CsAtoxicity at 3 months post-transplantation; however, biopsyin these recipients did not reveal allograft rejection.Informed and written consent was obtained from all pa-tients, and ethical clearance for this study was obtainedfrom the Ethical Committee of the Institute.
Data Collection
Therapeutic drug monitoring by determining C2 level (CsAlevels after 2 h of drug administration) in transplant recip-ients is a routine clinical practice at our center. C2 levelwas assayed by CsA-specific assay using EMIT (EnzymeMultiplied Immunologic Technique kit; Dade BehringInc., Cupertino, CA). For C2 level assay, 1 mL of bloodwas extracted in EDTA vials from transplant patients at2-h post-morning dose of CsA. Patient weight (kg), dailydose of CsA (mg/day) and C2 levels (mg/mL) were re-corded at 1 and 3 month post-transplantation. Dose-ad-justed CsA concentrations (C2/dose ratio) were therebycalculated by dividing C2 level with the corresponding24-h dose on an mg/kg basis. The information thus obtainedwas the CsA dose needed to achieve therapeutic C2 level.
Identification of Genotypes
Peripheral blood (3 mL) was collected in EDTA vials fromall renal transplant patients, and genomic DNA was ex-tracted using the salting out method (8). The regions of
Table 1. Demographic and clinical data of 155 renal allograft
recipients
Age (years) 35.28 � 10.4, 34 (17e59)
Male/Female 131/24
Body weight (kg) 52.95 � 8.8, 52 (30e80)
Serum creatinine (mg/dL) 1.17 � 0.26, 1.15 (0.7e2.4)
Transplant number (1/2) 152/3
Cause of end-stage
renal disease, n (%)
Glomerulonephritis 64 (41.3)
Diabetic nephropathy 20 (13.1)
Hypertension 17 (11.2)
Chronic interstitial nephropathy 28 (18.2)
Other 25 (16.2)
Rejection episodes n (%) 31 (20.0)
C2 levels (mg/mL)
1 month 1.62 � 0.13, 1.62 (0.99e1.92)
3 months 1.32 � 0.24, 1.32 (0.69e1.80)
Daily dose of CsA (mg/kg/day)
1 month 7.09 � 1.23, 6.94 (4.09e11.11)
3 months 4.24 � 0.85, 4.17 (2.23e8.15)
Dose-adjusted C2 levels
(mg/mL/mg/kg/day)
1 month 0.24 � 0.05, 0.23 (0.12e0.39)
3 months 0.34 � 0.10, 0.34 (0.14e0.76)
Mean � SD, median (range).

697Effect of ABCB1 SNPs on Cyclosporin Dose Requirement
interest in c.1236 C OT (exon 12), c.2064�76 T OA (intron16), c.2677 G OT (exon 21), and c.3435 C OT (exon 26)SNPs of ABCB1 gene were amplified using primer sequencesas described previously (6,9,5,10) using polymerase chainreaction restriction fragment length polymorphism(PCReRFLP). Restriction enzymes used for genotypingc.1236COT, c.2064�76TOA, c.2677GOT, and c.3435COTwere HaeIII (Fermentas, Inc., Glen Burnie, MD), ApoI (NewEngland Biolabs, Stamford Hill, UK), XbaI (Fermentas) andDpnII (New England Biolabs) respectively. Digestion wascarried out at 37�C for 6e8 h and was analyzed by electro-phoretic separation on a 12% polyacrylamide gel stainedwith ethidium bromide followed by visualization under ul-traviolet light.
Haplotype Determination
Arlequin version 2.0 (http://anthro.unige.ch/software/arlequin/) was used to infer the linkage disequilibrium(LD) between the four SNPs. Haplotype genotype analysisincluded SNPs ABCB1 c.1236COT, c.2064e76TOA,c.2677GOT, and c.3435COT based on strong LD betweenthese loci. Haplotype analysis was restricted to only homo-zygotes for the four polymorphic sites, as only these couldbe unambiguously assigned haplotypes. Furthermore, forcomparison between haplogenotypes and their possible rolein CsA pharmacokinetics we compared these haplogeno-type groups with CsA daily dose requirement and dose-ad-justed C2 levels.
Statistical Analysis
Statistical analysis was performed using SPSS 11.5 softwarefor Windows (Chicago, IL). Data were expressed as mean�SD. Genotype frequencies for ABCB1 SNPs were tested fordeviation from the Hardy-Weinberg equilibrium using c2
test. For analysis of continuous pharmacological variables,patient genotypes/haplotypes were used as categorical inde-pendent variables. Genotype/haplotype groups were furthercompared for differences in mean daily dose requirementand dose-adjusted C2 levels using non-parametric tests suchas Mann-Whitney U test for pairwise comparison betweengroups and Kruskal-Wallis test for multiple group compari-sons. Allograft outcome in terms of rejection episodes was
analyzed with Kaplan-Meier estimates considering rejectionepisode as an event. Groups were compared with log ranktest. Cox regression analysis was performed to calculate haz-ards ratio (HR). p values were adjusted for multiple testingaccording to the Bonferroni method; p values #0.05 wereconsidered statistically significant.
Results
Interindividual Variation in CsADaily Dose and Dose-adjusted C2 Levels
Daily dose requirement ranged from 4.09 to 11.11 and2.23 to 8.15 mg/kg/day for 1 and 3 months, respectively.Dose-adjusted C2 levels of 0.12 to 0.39 and 0.14 to 0.76mg/mL/mg/kg/day were observed at 1 and 3 months, re-spectively (Table 1). The wide ranges of daily dose require-ment and dose-adjusted C2 levels confirmed the extensiveinterindividual variations in CsA metabolism.
Frequency of ABCB1 Variants in Renal TransplantPatients
Genotype and allelic frequencies of ABCB1 variants for 155recipients are listed in Table 2. The frequency expectedfor each genotype was evaluated on the basis of Hardy-Weinberg equilibrium proportions. None of the observedfrequencies was significantly different from the expectedfrequencies. In our population, allele frequency for T at po-sition 1236 was 67.1%. A-76 allele at c.2064�76TOA wasfound to be 21.9%. The variant T2677 and T3435 allele fre-quency at ABCB1 c.2677GOT and ABCB1 c.3435COTwas 59.4% and 60.3%, respectively.
Effect of ABCB1 SNPs on CsA Daily Doseand Dose-adjusted C2 Levels
Distribution of mean CsA dose and dose-adjusted C2 levelsfor all subjects in different genotype groups of ABCB1SNPs is illustrated in Table 3. Stratified for c.2064e76TOAgenotype, mean daily dose requirement at 1 month ex-hibited a decreasing trend with the number of A-alleles atposition -76 in intron 16 (TT 7.27 � 1.05, TA 6.91 �1.27 and AA 6.15 � 1.05 mg/kg/day; p 5 0.027).
Table 2. Genotype and allele frequencies of ABCB1 SNPs in renal allograft recipients
Polymorphism Genotype frequencies n (%) Allele frequencies n (%)
c.1236COT (rs1128503) CC CT TT C T
17 (11.0) 68 (43.9) 70 (45.1) 102 (32.9) 208 (67.1)
c.2064e76TOA (rs1922242) TT TA AA T A
94 (60.6) 54 (34.8) 7 (4.6) 242 (78.1) 68 (21.9)
c.2677GOT (rs2032582) GG GT TT G T
34 (22.0) 58 (37.4) 63 (40.6) 126 (40.6) 184 (59.4)
c.3435COT (rs1045642) CC CT TT C T
29 (18.7) 65 (41.9) 61 (39.4) 123 (39.7) 187 (60.3)
rs: reference sequence number according to NCBI database.

698 Singh et al. / Archives of Medical Research 39 (2008) 695e701
Table 3. Influence of ABCB1 SNPs on CsA daily dose (mg/kg/day) and dose-adjusted C2 levels (mg/mL/mg/kg/day) in all patients at 1 and 3 months after
transplantation
No. of months post-transplantation
1 3
Polymorphism Genotypes (n) p value* Genotypes (n) p value*
c.1236COT CC (17) CT (68) TT (70) CC (17) CT (68) TT (70)
Daily dose 7.44 � 1.08 7.00 � 1.19 7.10 � 1.43 0.387 4.45 � 0.98 4.35 � 0.91 4.06 � 0.72 0.068
Dose-adjusted C2 levels 0.22 � 0.03 0.24 � 0.05 0.24 � 0.05 0.406 0.34 � 0.06 0.32 � 0.09 0.36 � 0.12 0.051
c.2064e76TOA TT (94) TA (54) AA (7) TT (94) TA (54) AA (7)
Daily dose 7.27 � 1.05 6.91 � 1.27 6.15 � 1.05 0.027 4.25 �1.26 4.09 � 1.39 4.40 � 0.71 0.587
Dose-adjusted C2 levels 0.22 � 0.04 0.25 � 0.05 0.27 � 0.03 0.004 0.34 � 0.09 0.35 � 0.12 0.34 � 0.08 0.846
c.2677GOT GG (34) GT (58) TT (63) GG (34) GT (58) TT (63)
Daily dose 7.65 � 1.05 6.97 � 1.28 6.91 � 1.35 0.004 4.40 � 0.93 4.28 � 0.87 4.12 � 0.77 0.102
Dose-adjusted C2 levels 0.22 � 0.03 0.24 � 0.05 0.24 � 0.05 0.036 0.32 � 0.07 0.35 � 0.09 0.35 � 0.12 0.069
c.3435COT CC (29) CT (65) TT (61) CC (29) CT (65) TT (61)
Daily dose 7.39 � 1.25 6.95 � 1.16 7.11 � 1.42 0.365 4.22 � 0.81 4.27 � 0.86 4.22 � 0.873
Dose-adjusted C2 levels 0.23 � 0.05 0.24 � 0.05 0.24 � 0.05 0.568 0.36 � 0.06 0.35 � 0.10 0.32 � 0.12 0.334
All values are expressed as mean � SD.
*Kruskal-Wallis U test.
Consequently, the mean dose-adjusted C2 levels showed anincreasing trend with the number of variant allele (TT 0.22� 0.04, TA 0.25 � 0.05 and AA 0.27 � 0.03 mg/mL/mg/kg/day; p 5 0.004). However, a similar trend was not followedat 3 months post-transplantation. A comparable decreasingtrend in daily dose requirement at 1 month was observedwith ABCB1 c.2677GOT in exon 21 with GG 7.65 �1.05, GT 6.97 � 1.28 and TT 6.91 � 1.35 mg/kg/day; p5 0.004). Dose-adjusted C2 levels exhibited an increasingtrend between GG and T allele carriers with 0.22 � 0.03,0.24 � 0.05 and 0.24 � 0.05 mg/mL/mg/kg/day ( p 5
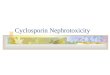
0.036). Further, our analysis found that (GG)2677 patientshad a significantly greater daily dose requirement of CsAthan a paired group of (GT)2677 and (TT)2677 individualsat 1 month and 3 months ( p 5 0.001 and 0.041; Figure 1).Dose-adjusted C2 levels were also significantly lower in(GG)2677 in comparison to a paired group of (GT)2677and (TT)2677 individuals at 1 and 3 months posttransplan-tation ( p 5 0.009 and 0.043; Figure 2). No statistically sig-nificant association was observed between daily doserequirement and dose-adjusted C2 levels for ABCB1c.1236COT and ABCB1 c.3435COT polymorphisms.
Haplotype Analysis
The in vivo effects of individual mutations are difficult toevaluate because of the close linkage disequilibrium de-tected among the four ABCB1 SNPs. This prompted us toperform haplotype analysis of ABCB1 SNPs to identifythe association between carriers and non-carriers of wildand variant alleles represented by each haplotype andCsA dose requirements. Of the 12 possible ABCB1 haplo-type combinations derived from the homozygous genotypesof ABCB1 c.1236COT-2064e76TOAe2677GOTe3435-
COT, only six appeared in our patient population. Haplo-types could be ascribed with certainty in only 33 patients(21.3%) who were homozygous at all loci. The mostfrequent homozygous genotype derived haplotype was T-T-T-T (1236Te76Te2677Te3435T): in 19 patients. Thiswas followed by T-A-T-T: 5; T-T-T-C: 4; C-T-G-C: 2;T-A-G-T: 2 and C-T-G-T in one patient. Haplogenotypesand mean CsA daily dose and dose-adjusted C2 levels at1 month and 3 months are represented in Table 4. However,
Figure 1. The association of ABCB1 c.2677GOT with CsA daily dose re-
quirement (mg/kg/day) at 1 and 3 months post-transplantation. The box
plots show the mean daily dose requirement, clustered according to
2677GOT SNPs. Error bars represent 25th and 75th percentiles. Carriers
and homozygotes for the T allele were pooled and compared with homozy-
gous wild type patients (GG). Outliers are plotted separately. *p 5 0.001
(1 month) and 0.041 (3 months) for (GG)2677 vs. (GT)2677e(TT)2677.

699Effect of ABCB1 SNPs on Cyclosporin Dose Requirement
no significant influence of these haplogenotypes with CsAdaily dose and dose-adjusted C2 levels at 1 or 3 monthscould be observed in our patient group.
Influence of ABCB1 c.2677GOT on Allograft Outcome
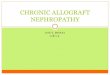
The above results suggested that patients with GG genotypeat locus 2677 in exon 21 were likely to receive suboptimaldoses of CsA; therefore, we performed Kaplan-Meier allo-graft survival analysis to analyze whether this suboptimaldose of CsA due to high expression of P-gp in these patientsinfluenced allograft survival. Allograft survival plot withrespect to genotypes of ABCB1 c.2677GOT is shown inFigure 3. The GG genotype resulted in significant reductionin mean graft survival (log rank p 5 0.0216) as comparedwith the heterozygous (GT) or variant genotype (TT).Cox proportional hazard was further performed to inferHR (hazard ratio) associated with genotypes keeping GGas reference. GT and TT genotypes were associated with
Figure 2. Association of ABCB1 c.2677GOT with dose-adjusted C2 levels
(mg/mL/mg/kg/day) at 1 and 3 months post-transplantation. Box plots show
the mean dose-adjusted C2 levels clustered according to 2677GOT SNPs.
Error bars represent 25th and 75th percentiles. Carriers and homozygotes
for the T allele were pooled and compared with homozygous wild-type pa-
tients (GG). Outliers are plotted separately. *p 5 0.009 (1 month) and
0.043 (3 months) for (GG)2677 vs. (GT)2677e(TT)2677.
reduced HR (GT-HR 5 0.33, p 5 0.016 and TT-HR 5
0.43, p 5 0.045) (Table 5).
Discussion
Genetic polymorphism studies in genes encoding drugtransporters (ABCB1) have contributed significantly inunderstanding the interindividual variability in doseeconcentration relationships and drug response of immuno-suppressants in different ethnic populations of transplantrecipients (11,12). Failure to achieve adequate CsA levelsin the immediate posttransplant period has been suggestedto be one of the major risk factors associated with develop-ment of acute rejection episodes. In a study on the impactof variability of CsA levels on long-term chronic allograftdysfunction, Citterio et al. suggested that patients withmean C2 levels O900 ng/mL are associated with reducedrisk of rejection (13). In addition, CsA levels of 175 mg/Lor more in the early post-transplant period were found toreduce chronic rejection in liver transplant patients (14).These results suggested that early detection of patients withlow mean CsA levels is important in minimizing allograftrejection.
Frequency of variant allele in ABCB1 c.1236COT(67.1%), c.2677GOT (59.4%) and c.3435COT (60.3%)was in concordance with the study of Chowbay et al. report-ing 67.2%, 59.8% and 63.2%, respectively, in Indian popu-lation (15). In our population, we observed a lowerincidence of variant A allele at c.2064-76TOA (21.9%),which was in contradiction to other reports in the Caucasianpopulation (10).
Our analysis showed significant association of ABCB1c.2677GOT SNP with CsA dose requirements and dose-adjusted C2 levels at 1 and 3 months post-transplantation,whereas c.3435COT and c.1236COT demonstrated no as-sociation. The c.2064e76TOA SNP was also significantlyassociated with CsA dose requirement and dose-adjustedC2 levels at 1 month; however, a similar trend was not seenat 3 months suggesting marginal influence of this polymor-phism on CsA metabolism.
The significant association of ABCB1 c.2677GOT poly-morphism with CsA pharmacokinetics in the present studysuggested that dose requirement was 10.7% and 5.01%
Table 4. Influence of ABCB1 haplo genotypes on CsA daily dose and dose-adjusted C2 levels in patients at 1 and 3 months post-transplantation
1 month 3 months
Haplogenotypes n Daily dose* Dose-adjusted C2 levels* Daily dose* Dose-adjusted C2 levels*
1/1 19 7.28 � 1.99 0.25 � 0.07 4.21 � 0.73 0.37 � 0.11
2/2 4 7.97 � 0.88 0.18 � 0.05 4.41 � 1.39 0.24 � 0.16
3/3 5 6.91 � 0.66 0.22 � 0.03 4.19 � 1.06 0.40 � 0.07
Haplotypes 1, 2, and 3 are derived from homozygous genotypes of ABCB1 c.1236COT, c.2064e76TOA, c.2677GOT, and c.3435COT SNPs. Haplotype
1- T-T-T-T; haplotype 2eT-T-T-C, haplotype 3eT-A-T-T. The three haplo-genotype groups were compared using Kruskal-Wallis test. *p O0.05

700 Singh et al. / Archives of Medical Research 39 (2008) 695e701
higher in patients with wild type genotype (GG) at 1 month(Mann-Whitney p 5 0.001) and 3 months (Mann-Whitneyp 5 0.041), respectively, in comparison to patients carryingTT genotype. This can be supported by the fact that patientswith no mutation in ABCB1 gene are more likely to extrudeimmunosuppressant drug from intestinal cells and therebyrequire higher daily dose to achieve therapeutic bloodlevels. Significant association of similar (c.2677GOT )polymorphism has been demonstrated in another study byAnglicheau et al.; however, patients in their study receivedtacrolimus (a substrate of ABCB1) as an immunosuppres-sant in contrast to CsA used in our study. Our findingscorroborated their study reporting higher dose-adjustedtacrolimus concentrations in wild-type patients (16).
The implication of ABCB1 gene polymorphisms in CsAdose requirements prompted us to perform haplotyping be-cause it can serve as better biomarkers over the single locusanalysis. Because all four polymorphic sites were in linkagedisequilibrium, haplotype analysis was done using the ho-mozygous genotypes of ABCB1 SNPs. However, haploge-notype groups could be established in only 33 patients,limiting the haplotype analysis in the present study. No sig-nificant association was observed when we compared themost prevalent haplogenotype with CsA pharmacokinetics,which is consistent with the recent results of Fredericks
Figure 3. Kaplan-Meier estimate of graft survival in recipients of renal
transplant and number of rejections with respect to ABCB1 c.2677GOT.
Cross bars represent the censored patients who have experienced rejection
episode. Homozygosity for the wild 2677G allele is associated with signif-
icantly higher rates of graft failure (log rank p 5 0.024).
et al. who concluded that ABCB1 haplotypes have only a mi-nor influence on CsA pharmacokinetics (12).
As analyzed from the above results, transplant recipientswith GG genotype of ABCB1 c.2677GOT were associatedwith higher dose requirement of CsA and, therefore, athigher risk of rejection due to constant under-immunosup-pression. Therefore, we performed allograft survival analy-sis to analyze the influence of ABCB1 c.2677GOTgenotypes on allograft outcome. Kaplan-Meier allograftsurvival analysis revealed significantly low graft survivalin homozygous G carriers as compared to T allele carriers( p 5 0.021). Further, Cox regression analysis revealed re-duced risk of rejection episodes in variant T allele carriers[HR 5 0.33 (GT), 0.43 (TT)]. Consequently, these findingssupport our earlier observation, which suggested that recip-ients with GG genotype required higher CsA dose to attainthe target C2 level so as to avoid rejection. Due to the lowfrequency of rejection episodes (20%) at our center, a largemulticentric study is warranted to confirm the above find-ings. Results obtained from this study constituted a prelim-inary step in initial understanding of the influence ofABCB1 gene on CsA dose requirements in our population,although similar studies have been conducted in differentethnic groups.
No significant association observed between ABCB1c.3435COT polymorphism and dose-adjusted C2 levelwas confirmed by two previous studies in Caucasians(16,17). A recent study by Kotrych et al. also suggested nosignificant influence of this polymorphism on risk of allo-graft rejection in a group of 116 Polish transplant recipientson CsA therapy (18). In contrast, Azarpira et al. observeda significant correlation between the dose-adjusted C0values and 3435COT during the initial days after transplan-tation (19). ABCB1 c.3435COT is a synonymous SNP inexon 26 of ABCB1 and is often associated with alteredP-gp activity. Previously, this altered activity was associateddue to linkage disequilibrium with other common functionalnon- synonymous SNPs such as ABCB1 c.2677GOT. How-ever, a recent study by Kimchi-Sarfaty et al. reported that thesilent polymorphism in exon 26 results in P-gp with altereddrug and inhibitor interactions (20).
In a similar study showing the association of ABCB1polymorphisms on CsA exposure, Foote et al. demonstratedsignificantly higher CsA dose requirement in (CC)3435 pa-tients as compared to (CT) and (TT)3435 patients, whereasABCB1 c.2677GOT polymorphism was not significantly
Table 5. Survival time of renal allograft according to ABCB1 c.2677GOT genotypes
Genotypes Number of rejection episodes (%) Graft survival time in months (mean � SEM) 95% CI HR (95% CI) p value
GG (34) 12 (35.3) 25.12 � 2.62 19.98e30.26 Ref e
GT (58) 8 (13.8) 32.01 � 1.36 29.34e34.68 0.33 (0.14e0.81) 0.016
TT (63) 11(17.5) 30.09 � 1.62 26.91e33.27 0.43 (0.19e0.98) 0.045
HR, hazard ratios.

701Effect of ABCB1 SNPs on Cyclosporin Dose Requirement
correlated with CsA pharmacokinetics (21). To the best ofour knowledge these findings constituted the first attemptto explore the association of ABCB1 polymorphisms withCsA pharmacokinetics in a cohort of renal transplant pa-tients from North India receiving CsA as a part of a mainte-nance immunosuppressive regimen.
In conclusion, patients with GG genotype of ABCB1c.2677GOT polymorphism in exon 21 of ABCB1 are likelyto receive suboptimal doses of CsA during the initial period(1e3 months) after renal transplantation and are thereby ata higher risk of rejection, which may adversely affect long-term graft survival. Occasionally, clinical observation ofrecipients with less body weight requiring higher CsA doseand with more body weight requiring low dose can now becorrelated to individual variability in drug metabolizing anddrug transport genes, although the influence of diet, age, en-vironmental exposure on drug metabolism cannot be ig-nored.
Thus, additional pretransplant genotyping of ABCB1may have an important clinical role in individualizing andoptimizing CsA dose requirement in transplant patients inthe initial period when the chances of immunosuppressionor toxicity are greatest. Because the gene variants are dueto intraethnicity, multicentric trials from different ethnicgroups are suggested.
AcknowledgmentsThis study was funded by a grant from the Department of Biotech-nology, New Delhi (to RDM). We acknowledge the assistance ofthe Department of Nephrology and Hospital Transplant Unit inblood collection of the patients and the relevant clinical informa-tion. The authors are grateful to Drs. Parmeet and Anupama forcritical suggestions in drafting the manuscript. R.S. thanks theCouncil of Scientific and Industrial Research, New Delhi, for pro-viding a senior research fellowship.
References1. Knight SR, Morris PJ. The clinical benefits of cyclosporine C2 level
monitoring: a systematic review. Transplantation 2007;83:1525e1535.
2. Kahan BD, Welsh M, Schoenberg L, Rutzky LP, Katz SM,
Urbauer DL, et al. Variable oral absorption of cyclosporine. A bio-
pharmaceutical risk factor for chronic renal allograft rejection. Trans-
plantation 1996;62:599e606.
3. Fojo AT, Ueda K, Slamon DJ, Poplack DG, Gottesman MM, Pastan I,
et al. Expression of a multidrug-resistance gene in human tumors and
tissues. Proc Natl Acad Sci 1987;84:265e269.
4. Fromm MF. The influence of MDR1 polymorphisms on P-glycopro-
tein expression and function in humans. Adv Drug Deliv Rev 2002;
54:1295e1310.
5. Tanabe M, Ieiri I, Nagata N, Inoue K, Ito S, Kanamori Y, et al. Expres-
sion of P-glycoprotein in human placenta: relation to genetic polymor-
phism of the multidrug resistance (MDR)-1 gene. J Pharmacol Exp
Ther 2001;297:1137e1143.
6. Haufroid V, Mourad M, Van Kerckhove V, Wawrzyniak J, De
Meyer M, Eddour DC, et al. The effect of CYP3A5 and MDR1
(ABCB1) polymorphisms on cyclosporine and tacrolimus dose re-
quirements and through blood levels in stable renal transplant patients.
Pharmacogenetics 2004;14:147e154.
7. Racusen LC, Solez K, Colvin RB, Bonsib SM, Castro MC, Cavallo T,
et al. The Banff 97 working classification of renal allograft pathology.
Kidney Int 1999;55:713e723.
8. Miller SA, Dykes DD, Polesky HF. A simple salting out procedure for
extracting DNA from human nucleated cells. Nucleic Acids Res 1988;
16:1215.
9. Cascorbi I, Gerloff T, Johne A, Meisel C, Hoffmeyer S, Schwab M,
et al. Frequency of single nucleotide polymorphisms in the P-glyco-
protein drug transporter MDR1 gene in white subjects. Clin Pharmacol
Ther 2001;69:169e174.
10. Hamdy SI, Hiratsuka M, Narahara K, Endo N, El-Enany M, Moursi N,
et al. Genotype and allele frequencies of TPMT, NAT2, GST, SUL-
T1A1 and MDR-1 in the Egyptian population. Br J Clin Pharmacol
2003;55:560e569.
11. Sakaeda T. MDR1 genotype-related pharmacokinetics: fact or fiction?
Drug Metab Pharmacokinet 2005;20:391e414.
12. Fredericks S, Jorga A, MacPhee IA, Reboux S, Shiferaw E,
Moreton M, et al. A. Multi-drug resistance gene-1 (MDR-1) haplo-
types and the CYP3A5*1 genotype have no influence on ciclosporin
dose requirements as assessed by C0 or C2 measurements. Clin Trans-
plant 2007;21:252e257.
13. Citterio F, Scata MC, Pozzetto U, Nanni G, Castagneto M. Long-term
predictive value of cyclosporine microemulsion C2 level for chronic
renal allograft dysfunction. Transplant Proc 2003;35:2894e2898.
14. Domınguez J, Fuenzalida D, Norambuena R, Pais E, Cortes
Monroy G, et al. C2 monitoring of cyclosporine in stable renal trans-
plant patients results in lower costs and improved renal function.
Transplant Proc 2005;37:1583e1585.
15. Chowbay B, Cumaraswamy S, Cheung YB, Zhou Q, Lee EJ. Genetic
polymorphisms in MDR1 and CYP3A4 genes in Asians and the influ-
ence of MDR1 haplotypes on cyclosporin disposition in heart trans-
plant recipients. Pharmacogenetics 2003;13:89e95.
16. Anglicheau D, Verstuyft C, Laurent-Puig P, Becquemont L,
Schlageter MH, Cassinat B, et al. Association of the multidrug resis-
tance-1 gene single-nucleotide polymorphisms with the tacrolimus
dose requirements in renal transplant recipients. J Am Soc Nephrol
2003;14:1889e1896.
17. Hesselink DA, van Schaik RH, van der Heiden IP, van der Werf M,
Gregoor PJ, Lindemans J, et al. Genetic polymorphisms of the
CYP3A4, CYP3A5, and MDR-1 genes and pharmacokinetics of the
calcineurin inhibitors cyclosporine and tacrolimus. Clin Pharmacol
Ther 2003;74:245e254.
18. Kotrych K, Sulikowski T, Domanski L, Bia1ecka M, Drozdzik M.
Polymorphism in the P-glycoprotein drug transporter MDR1 gene in
renal transplant patients treated with cyclosporin A in a Polish popu-
lation. Pharmacol Rep 2007;59:199e205.
19. Azarpira N, Aghdaie MH, Behzad-Behbahanie A, Geramizadeh B,
Behzadi S, Malekhoseinie SA, et al. Association between cyclosporine
concentration and genetic polymorphisms of CYP3A5 and MDR1 dur-
ing the early stage after renal transplantation. Exp Clin Transplant
2006;4:416e419.
20. Kimchi-Sarfaty C, Oh JM, Kim IW, Sauna ZE, Calcagno AM,
Ambudkar SV, et al. A ‘‘silent’’ polymorphism in the MDR1 gene
changes substrate specificity. Science 2007;315:525e528.
21. Foote CJ, Greer W, Kiberd B, Fraser A, Lawen J, Nashan B,
Belitsky P. Polymorphisms of multidrug resistance gene (MDR1)
and cyclosporine absorption in de novo renal transplant patients.
Transplantation 2007;83:1380e1384.