Embed Size (px)
Citation preview
Journal of Diabetes and Its Complications 28 (2014) 762–766
Contents lists available at ScienceDirect
Journal of Diabetes and Its Complications
j ourna l homepage: WWW.JDCJOURNAL.COM
ABC goal achievement predicts microvascular but not macrovascular
complications over 6-years in adults with type 1 diabetes:The Coronary Artery Calcification in Type 1 Diabetes StudyPetter Bjornstad a,⁎, David M. Maahs a,b,c, Marian Rewers a,b, Richard J. Johnson c, Janet K. Snell-Bergeon a,b
a Department of Pediatrics, University of Colorado School of Medicine, Aurora, COb Barbara Davis Center for Diabetes, University of Colorado Denver, Aurora, COc Department of Nephrology, University of Colorado Denver, Aurora, CO
Duality of interest: Drs. Bjornstad, Snell-Bergeon, Johno conflict of interest to disclose.⁎ Corresponding author at: Barbara Davis Center for Ch
Colorado, Denver, 1775 Aurora Court, Aurora, CO 8004+1 303 724 6779.
E-mail address: Petter.Bjornstad@childrenscolorado.
http://dx.doi.org/10.1016/j.jdiacomp.2014.06.0171056-8727/© 2014 Elsevier Inc. All rights reserved.
a b s t r a c t
a r t i c l e i n f oArticle history:
Received 5 June 2014Received in revised form 27 June 2014Accepted 30 June 2014Available online 4 July 2014Keywords:Type 1 diabetesMicrovascular complicationsMacrovascular complicationsHbA1cBlood pressureLDL-cholesterol
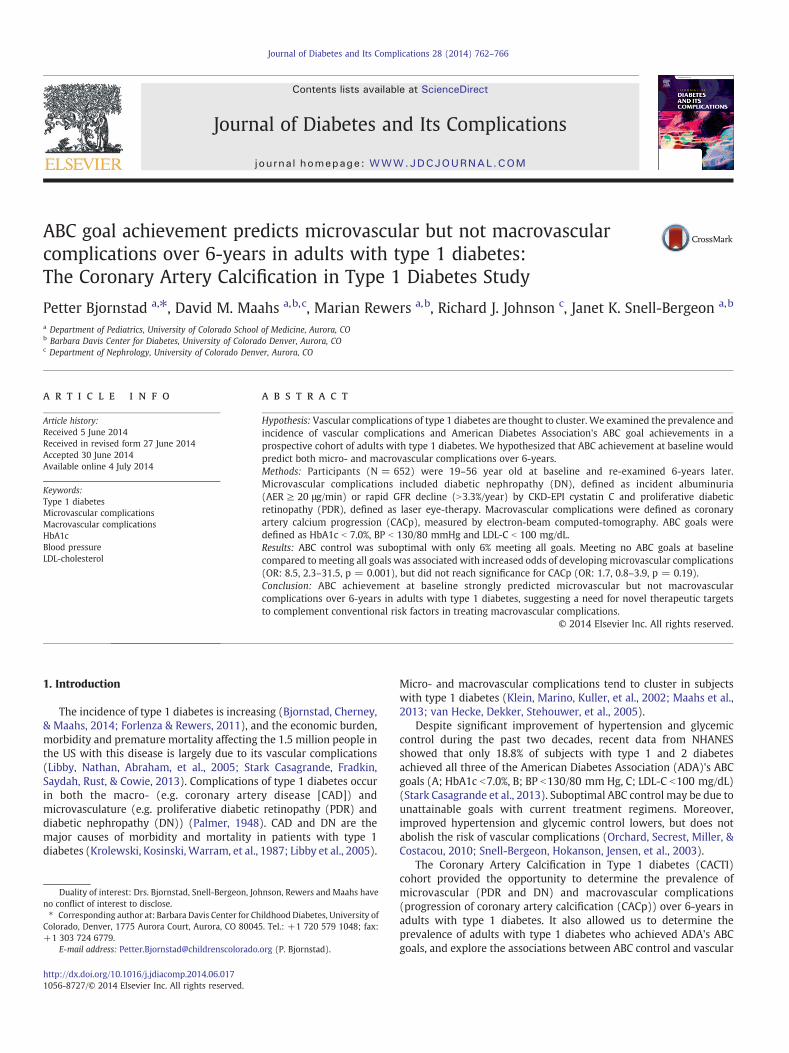
Hypothesis: Vascular complications of type 1 diabetes are thought to cluster. We examined the prevalence andincidence of vascular complications and American Diabetes Association's ABC goal achievements in aprospective cohort of adults with type 1 diabetes. We hypothesized that ABC achievement at baseline wouldpredict both micro- and macrovascular complications over 6-years.Methods: Participants (N = 652) were 19–56 year old at baseline and re-examined 6-years later.Microvascular complications included diabetic nephropathy (DN), defined as incident albuminuria(AER ≥ 20 μg/min) or rapid GFR decline (N3.3%/year) by CKD-EPI cystatin C and proliferative diabeticretinopathy (PDR), defined as laser eye-therapy. Macrovascular complications were defined as coronaryartery calcium progression (CACp), measured by electron-beam computed-tomography. ABC goals weredefined as HbA1c b 7.0%, BP b 130/80 mmHg and LDL-C b 100 mg/dL.Results: ABC control was suboptimal with only 6% meeting all goals. Meeting no ABC goals at baselinecompared to meeting all goals was associated with increased odds of developing microvascular complications
(OR: 8.5, 2.3–31.5, p = 0.001), but did not reach significance for CACp (OR: 1.7, 0.8–3.9, p = 0.19).Conclusion: ABC achievement at baseline strongly predicted microvascular but not macrovascularcomplications over 6-years in adults with type 1 diabetes, suggesting a need for novel therapeutic targetsto complement conventional risk factors in treating macrovascular complications.© 2014 Elsevier Inc. All rights reserved.
1. Introduction
The incidence of type 1 diabetes is increasing (Bjornstad, Cherney,& Maahs, 2014; Forlenza & Rewers, 2011), and the economic burden,morbidity and premature mortality affecting the 1.5 million people inthe US with this disease is largely due to its vascular complications(Libby, Nathan, Abraham, et al., 2005; Stark Casagrande, Fradkin,Saydah, Rust, & Cowie, 2013). Complications of type 1 diabetes occurin both the macro- (e.g. coronary artery disease [CAD]) andmicrovasculature (e.g. proliferative diabetic retinopathy (PDR) anddiabetic nephropathy (DN)) (Palmer, 1948). CAD and DN are themajor causes of morbidity and mortality in patients with type 1diabetes (Krolewski, Kosinski, Warram, et al., 1987; Libby et al., 2005).
nson, Rewers and Maahs have
ildhood Diabetes, University of5. Tel.: +1 720 579 1048; fax:
org (P. Bjornstad).
Micro- and macrovascular complications tend to cluster in subjectswith type 1 diabetes (Klein, Marino, Kuller, et al., 2002; Maahs et al.,2013; van Hecke, Dekker, Stehouwer, et al., 2005).
Despite significant improvement of hypertension and glycemiccontrol during the past two decades, recent data from NHANESshowed that only 18.8% of subjects with type 1 and 2 diabetesachieved all three of the American Diabetes Association (ADA)'s ABCgoals (A; HbA1c b7.0%, B; BP b130/80 mm Hg, C; LDL-C b100 mg/dL)(Stark Casagrande et al., 2013). Suboptimal ABC control may be due tounattainable goals with current treatment regimens. Moreover,improved hypertension and glycemic control lowers, but does notabolish the risk of vascular complications (Orchard, Secrest, Miller, &Costacou, 2010; Snell-Bergeon, Hokanson, Jensen, et al., 2003).
The Coronary Artery Calcification in Type 1 diabetes (CACTI)cohort provided the opportunity to determine the prevalence ofmicrovascular (PDR and DN) and macrovascular complications(progression of coronary artery calcification (CACp)) over 6-years inadults with type 1 diabetes. It also allowed us to determine theprevalence of adults with type 1 diabetes who achieved ADA's ABCgoals, and explore the associations between ABC control and vascular

763P. Bjornstad et al. / Journal of Diabetes and Its Complications 28 (2014) 762–766
complications. We hypothesized that ABC goal achievement atbaseline would predict the development of micro- and macrovascularcomplications over 6-years.
2. Materials and methods
The CACTI Study enrolled 1416 subjects 19–56 years old, 652 withtype 1 diabetes and 764 without diabetes, who were asymptomaticfor cardiovascular disease (CVD) at the baseline visit in 2000-02 andthen were re-examined 3 and 6 years later, as previously described(Maahs, Kinney, Wadwa, et al., 2005). Only the 652 participants withtype 1 diabetes were included in this analysis. The study wasapproved by the Colorado Multiple Institutional Review Board, andall participants provided informed consent.
We measured height and weight, and calculated BMI in kg/m2.Resting systolic (SBP) and fifth-phase diastolic blood pressure (DBP)(i.e. the silence as the cuff pressure drops below the DBP) weremeasured three times while the patient was seated, and the secondand thirdmeasurements were averaged. After an overnight fast, bloodwas collected, centrifuged, and separated. Plasma was stored at 4 °Cuntil assayed. The results were reported in milligrams per deciliter.Total plasma cholesterol and triglyceride levels were measured usingstandard enzymatic methods; HDL cholesterol (HDL-C)was separatedusing dextran sulfate and LDL cholesterol (LDL-C) was calculatedusing the Friedewald formula. High performance liquid chromatog-raphy was used to measure HbA1c (HPLC, BioRad variant).
2.1. Diabetic nephropathy
We defined DN as incident albuminuria or rapid GFR decline.Albuminuria was defined as microalbuminuria or greater; albuminexcretion rate (AER) ≥20 μg/min if timed urine samples wereobtained or albumin/creatinine ratio (ACR) ≥30 mg/g for spotsamples (if timed urine samples were not available). Two timedovernight urine samples were collected, and urine creatinine andalbumin were measured (RIA, Diagnostic Products) and averaged. Atboth visits, urinary albumin excretion rate (AER) and albumin/creatinine ratio (ACR) were calculated. Incident albuminuria wasdefined as the development of albuminuria at the 6-year follow-up inthose without albuminuria at baseline. Of the 27 subjects whodeveloped incident albuminuria all had AER calculated, and all buttwo (n = 326/328) of those who did not develop incident albumin-uria had AER calculated. Estimated GFR (mL/min/1.73 m2) wasdetermined using the CKD-EPI cystatin C equation (Inker, Schmid,Tighiouart, et al., 2012). There is no standard cutoff for rapid GFRdecline, but we employed annual GFR loss N 3.3% to define rapid GFRdecline which has been used by the Joslin Kidney Study, a studypopulation similar to CACTI (Krolewski, Niewczas, Skupien, et al.,2014). Cystatin C wasmeasured in the University of Colorado Hospitalclinical lab using the commercially available Dade-Behring assayfollowing package insert instructions on a BNII or Prospec instrumentas previously described in detail (Maahs, Jalal, McFann, Rewers, &Snell-Bergeon, 2011).
2.2. Coronary artery calcification
CAC measurements were obtained in duplicate using an ultrafastImatron C-150XLP electron beam computed tomography scanner(Imatron, San Francisco, CA). The average of the two scores was usedas the CAC score for that visit. Scans were repeated on follow-up, anaverage of 6.1 years after the baseline exam. Progression of CAC wasdefined as an increase in volume of CAC of ≥2.5 square roottransformed units. Both subjects with CAC 0 (incident CAC) andpositive score (CAC+) at baseline were included in the analyses. Thisdefinition of progression has previously been shown to represent
significant progression of atherosclerosis (Hokanson, MacKenzie,Kinney, et al., 2004; Snell-Bergeon et al., 2003).
2.3. Proliferative diabetic retinopathy
Diagnosis of PDR was based on self-reported history of prolifer-ative retinopathy with laser eye treatment. Self-reported prior lasertreatment has been validated as both a sensitive and specific tool fordetermining PDR (Grassi, Mazzulla, Knudtson, et al., 2009; Grassi, Sun,Gangaputra, et al., 2013).
2.4. ABC control
ADA's ABC goals are defined as (A; HbA1c b7.0%, B; BP b130/80 mm Hg, C; LDL-C b 100 mg/dL) (Stark Casagrande et al., 2013).Anti-hypertension medication use was determined by a medicationinventory as previously described (Maahs et al., 2005), and all anti-hypertension medications (including beta-blockers, calcium channelblockers, diuretics, ACE inhibitor (ACEi) and/or angiotensin receptorblockers (ARB) were combined for these analyses.
3. Statistical analysis
Analyses were performed in SAS (version 9.3 for Windows; SASInstitute, Cary, NC). Differences between ABC goal achievements wereassessed using ANOVA for continuous variables and chi-squared forcategorical variables. Differences between CAC progressors and non-progressors were assessed using chi-square for categorical variables,t-test for continuous parametric variables and Wilcoxon signed rank-test for continuous non-parametric variables. Incident albuminuria(n = 27), incident PDR (n = 35) and rapid GFR decline (n = 52)were examined separately and together as microvascular complica-tions (n = 99, as 15 subjects experienced more than one microvas-cular complication).
Logistic regression models were employed to determine if CAC atbaseline was associated with development of incident albuminuria,incident PDR and rapid GFR decline and CACp. For that reason, weexcluded subjects with albuminuria and PDR at baseline in therespective analyses with incident albuminuria and PDR as theoutcomes. For rapid GFR decline and CACp, however, we examinedprogression and therefore did not exclude baseline disease. Thefollowing variables were considered for inclusion in these models:age, sex, diabetes duration, BMI, HDL-C, LDL-C, HbA1c, SBP, DBP,antihypertensive medications, statins and smoking status. Logisticregressionmodels were also used to examine the association betweenABC goal achievement at baseline with the development of micro-vascular complications and CACp. The following variables wereconsidered for inclusion in these models: age, sex, diabetes duration,BMI, antihypertensive medications, statins, smoking status andbaseline CAC. Significance was based on an α-level of 0.05.
4. Results
At baseline, 49% of men and 28% of women had detectable CAC(p b 0.0001), 27% of men and 17% of women had evidence ofalbuminuria (p = 0.005), and 27% of men and 19% of womenreported PDR (p = 0.02). Baseline subject characteristics stratifiedby ABC goal achievements are shown in Table 1. More women met allgoals and some goals, and those that met all goals had significantlylower BMI and waist circumference (Table 1).
Over 6-years 9.6% of men and 6.1% of women developed incidentalbuminuria (p = 0.22), 11% of men and 10% of women developedrapid GFR decline (p = 0.92), 11.3% of men and 6.0% of womendeveloped PDR (p = 0.05) and 52.5% of men and 34.0% of womenexperienced CACp (p b 0.0001). Incidence of vascular complicationsstratified by ABC goal achievement at baseline is shown in Fig. 1.
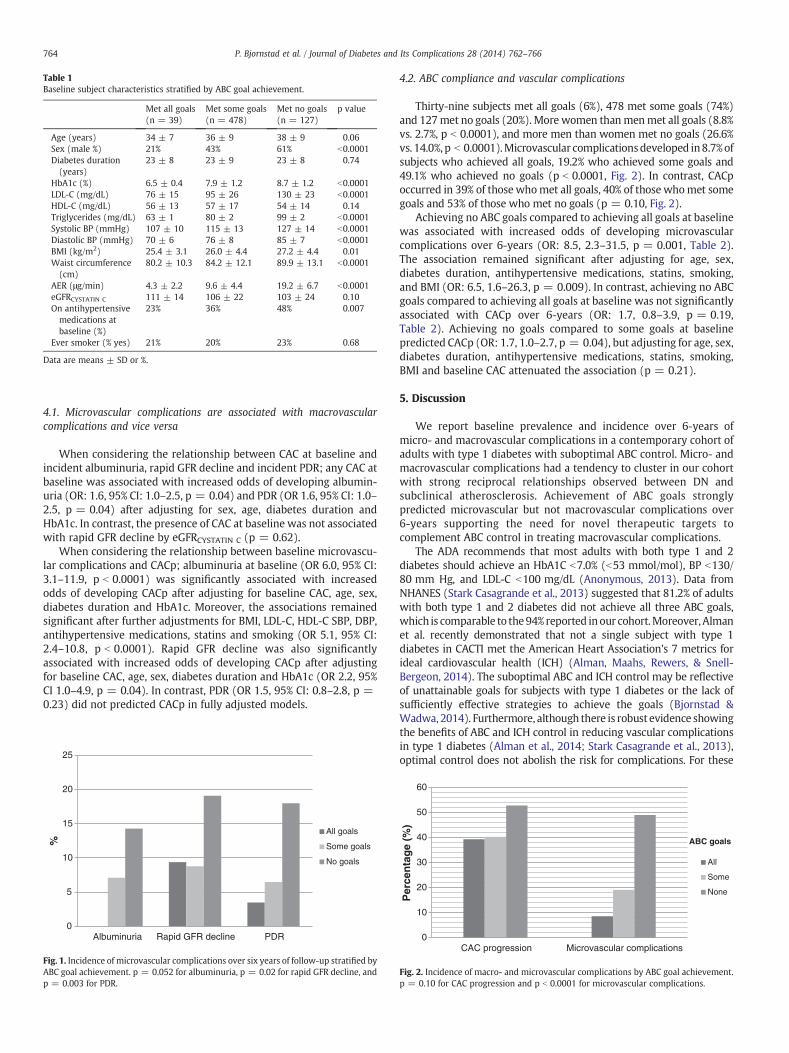
Table 1Baseline subject characteristics stratified by ABC goal achievement.
Met all goals(n = 39)
Met some goals(n = 478)
Met no goals(n = 127)
p value
Age (years) 34 ± 7 36 ± 9 38 ± 9 0.06Sex (male %) 21% 43% 61% b0.0001Diabetes duration(years)
23 ± 8 23 ± 9 23 ± 8 0.74
HbA1c (%) 6.5 ± 0.4 7.9 ± 1.2 8.7 ± 1.2 b0.0001LDL-C (mg/dL) 76 ± 15 95 ± 26 130 ± 23 b0.0001HDL-C (mg/dL) 56 ± 13 57 ± 17 54 ± 14 0.14Triglycerides (mg/dL) 63 ± 1 80 ± 2 99 ± 2 b0.0001Systolic BP (mmHg) 107 ± 10 115 ± 13 127 ± 14 b0.0001Diastolic BP (mmHg) 70 ± 6 76 ± 8 85 ± 7 b0.0001BMI (kg/m2) 25.4 ± 3.1 26.0 ± 4.4 27.2 ± 4.4 0.01Waist circumference(cm)
80.2 ± 10.3 84.2 ± 12.1 89.9 ± 13.1 b0.0001
AER (μg/min) 4.3 ± 2.2 9.6 ± 4.4 19.2 ± 6.7 b0.0001eGFRCYSTATIN C 111 ± 14 106 ± 22 103 ± 24 0.10On antihypertensivemedications atbaseline (%)
23% 36% 48% 0.007
Ever smoker (% yes) 21% 20% 23% 0.68
Data are means ± SD or %.
764 P. Bjornstad et al. / Journal of Diabetes and Its Complications 28 (2014) 762–766
4.1. Microvascular complications are associated with macrovascularcomplications and vice versa
When considering the relationship between CAC at baseline andincident albuminuria, rapid GFR decline and incident PDR; any CAC atbaseline was associated with increased odds of developing albumin-uria (OR: 1.6, 95% CI: 1.0–2.5, p = 0.04) and PDR (OR 1.6, 95% CI: 1.0–2.5, p = 0.04) after adjusting for sex, age, diabetes duration andHbA1c. In contrast, the presence of CAC at baseline was not associatedwith rapid GFR decline by eGFRCYSTATIN C (p = 0.62).
When considering the relationship between baseline microvascu-lar complications and CACp; albuminuria at baseline (OR 6.0, 95% CI:3.1–11.9, p b 0.0001) was significantly associated with increasedodds of developing CACp after adjusting for baseline CAC, age, sex,diabetes duration and HbA1c. Moreover, the associations remainedsignificant after further adjustments for BMI, LDL-C, HDL-C SBP, DBP,antihypertensive medications, statins and smoking (OR 5.1, 95% CI:2.4–10.8, p b 0.0001). Rapid GFR decline was also significantlyassociated with increased odds of developing CACp after adjustingfor baseline CAC, age, sex, diabetes duration and HbA1c (OR 2.2, 95%CI 1.0–4.9, p = 0.04). In contrast, PDR (OR 1.5, 95% CI: 0.8–2.8, p =0.23) did not predicted CACp in fully adjusted models.
0
5
10
15
20
25
Albuminuria Rapid GFR decline PDR
%
All goals
Some goals
No goals
Fig. 1. Incidence of microvascular complications over six years of follow-up stratified byABC goal achievement. p = 0.052 for albuminuria, p = 0.02 for rapid GFR decline, andp = 0.003 for PDR.
4.2. ABC compliance and vascular complications
Thirty-nine subjects met all goals (6%), 478 met some goals (74%)and 127met no goals (20%). More women thanmenmet all goals (8.8%vs. 2.7%, p b 0.0001), and more men than women met no goals (26.6%vs. 14.0%, p b 0.0001).Microvascular complicationsdeveloped in8.7%ofsubjects who achieved all goals, 19.2% who achieved some goals and49.1% who achieved no goals (p b 0.0001, Fig. 2). In contrast, CACpoccurred in 39% of those whomet all goals, 40% of those whomet somegoals and 53% of those who met no goals (p = 0.10, Fig. 2).
Achieving no ABC goals compared to achieving all goals at baselinewas associated with increased odds of developing microvascularcomplications over 6-years (OR: 8.5, 2.3–31.5, p = 0.001, Table 2).The association remained significant after adjusting for age, sex,diabetes duration, antihypertensive medications, statins, smoking,and BMI (OR: 6.5, 1.6–26.3, p = 0.009). In contrast, achieving no ABCgoals compared to achieving all goals at baseline was not significantlyassociated with CACp over 6-years (OR: 1.7, 0.8–3.9, p = 0.19,Table 2). Achieving no goals compared to some goals at baselinepredicted CACp (OR: 1.7, 1.0–2.7, p = 0.04), but adjusting for age, sex,diabetes duration, antihypertensive medications, statins, smoking,BMI and baseline CAC attenuated the association (p = 0.21).
5. Discussion
We report baseline prevalence and incidence over 6-years ofmicro- and macrovascular complications in a contemporary cohort ofadults with type 1 diabetes with suboptimal ABC control. Micro- andmacrovascular complications had a tendency to cluster in our cohortwith strong reciprocal relationships observed between DN andsubclinical atherosclerosis. Achievement of ABC goals stronglypredicted microvascular but not macrovascular complications over6-years supporting the need for novel therapeutic targets tocomplement ABC control in treating macrovascular complications.
The ADA recommends that most adults with both type 1 and 2diabetes should achieve an HbA1C b7.0% (b53 mmol/mol), BP b130/80 mm Hg, and LDL-C b100 mg/dL (Anonymous, 2013). Data fromNHANES (Stark Casagrande et al., 2013) suggested that 81.2% of adultswith both type 1 and 2 diabetes did not achieve all three ABC goals,which is comparable to the94% reported inour cohort.Moreover,Almanet al. recently demonstrated that not a single subject with type 1diabetes in CACTI met the American Heart Association's 7 metrics forideal cardiovascular health (ICH) (Alman, Maahs, Rewers, & Snell-Bergeon, 2014). The suboptimal ABC and ICH control may be reflectiveof unattainable goals for subjects with type 1 diabetes or the lack ofsufficiently effective strategies to achieve the goals (Bjornstad &Wadwa, 2014). Furthermore, although there is robust evidence showingthe benefits of ABC and ICH control in reducing vascular complicationsin type 1 diabetes (Alman et al., 2014; Stark Casagrande et al., 2013),optimal control does not abolish the risk for complications. For these
0
10
20
30
40
50
60
CAC progression Microvascular complications
Per
cen
tag
e (%
)
ABC goals
All
Some
None
Fig. 2. Incidence of macro- and microvascular complications by ABC goal achievement.p = 0.10 for CAC progression and p b 0.0001 for microvascular complications.

Table 2Goal achievement and micro- and macrovascular complications over 6-years.
Microvascular complicationsover 6-years (n = 99)
CACp over 6-years(n = 199)
UnadjustedOR (95% CI)
AdjustedOR (95% CI)⁎
UnadjustedOR (95% CI)
AdjustedOR (95% CI)⁎⁎
No goals vs.some goals
3.6 (2.0–6.5)p b 0.0001
3.5 (1.8–6.7)p = 0.0002
1.7 (1.0–2.7)p = 0.04
1.0 (0.5–1.8)p = 0.21
No goals vs.all goals
8.5 (2.3–31.5)p = 0.001
6.5 (1.6–26.3)p = 0.009
1.7 (0.8–3.9)p = 0.19
1.8 (0.6–5.0)p = 0.29
⁎ Adjusted for age, sex, duration, BP meds, statins, smoking and BMI.⁎⁎ Adjusted for age, sex, duration, BP meds, statins, smoking, BMI and baseline CAC.
765P. Bjornstad et al. / Journal of Diabetes and Its Complications 28 (2014) 762–766
reasons there is a call for novel therapeutic targets to supplementconventional therapies.
Incidence and prevalence of vascular complications in the presentcohort are comparable towhat has been reported in other studies whentaking into account the studies' time to follow-up (Ficociello, Perkins,Roshan, et al., 2009; Gunnlaugsdottir, Halldorsdottir, Klein, et al., 2012).An important finding in our study is the strong association between DNand macrovascular complications. Emerging data suggest that micro-vascular disease can lead to dysfunction and ischemia of the macro-vasculature (Hallen, Jensen, Buser, Jaffe, & Atar, 2011). Several studieshave demonstrated relationships between cardiac biomarkers andmicrovascular complications in type 2 diabetes (Boertien, Riphagen,Drion, et al., 2013; Chalmers & Arima, 2010; Fenske, Wanner, Allolio,et al., 2011). Similarly, prospective studies have demonstrated thatmarkers of microvascular disease, such asmicroalbuminuria, decreasedeGFR or retinal vascular abnormalities, are associated with an increasedrisk of macrovascular events (Akasaka, Yoshida, Hozumi, et al., 1997;Gerstein, 2002; Gerstein, Mann, Yi, et al., 2001; Maahs et al., 2013; vanHecke et al., 2005). In CACTI, PDR did not independently predict CACpover 6-years. This stands in contrast to what has been reported by theCardiovascular Health Study (Klein et al., 2002), but is consistent withthe findings of EURODIAB (van Hecke et al., 2005), where PDR failed toindependently predict fatal and nonfatal CVD in fully adjustedmodels insubjects with type 1 diabetes.
Our data support the need for novel therapeutic targets tocomplement ABC control in treating macrovascular complications inadults with type 1 diabetes.We have previously shown that both serumuric acid (Bjornstad, Maahs, Rivard, et al., 2014) and insulin sensitivity(Bjornstad, Maahs, Johnson, Rewers, & Snell-Bergeon, in press;Bjornstad, Snell-Bergeon, Rewers, et al., 2013; Schauer, Snell-Bergeon,Bergman, et al., 2011; Bjornstad, Maahs, Cherney, et al., 2014) areimportant and potentially modifiable risk factors for macrovascularcomplications in type 1 diabetes. Moreover, we have published datademonstrating very weak associations between serum uric acid andinsulin sensitivity in type 1 diabetes, supporting their independence asrisk factors and possibly therapeutic targets (Bjornstad, Snell-Bergeon,McFann, et al., 2014). Another important finding of this paper is thestrong association between DN and subclinical atherosclerosis whichmay refine risk stratification for CACp, and enable development of newtherapeutic strategies. There is growing evidence that fibroblast growthfactor 23 (FGF23) and Klotho factor are mediators of coronary arterycalcification in the setting of nephropathy (Hu, Shi, Zhang, et al., 2011;Lim, Lu, Molostvov, et al., 2012), but it remains uncertain whetherregulation of these factors will prevent or delay development ofmacrovascular disease.
There are limitations of this study worth mentioning. First, PDRwas self-reported and could have been affected by poor recall, butself-reporting of PDR has recently been validated for subjects withtype 1 diabetes with sensitivity and specificity greater than 90%(Grassi et al., 2009; Grassi et al., 2013). Moreover, we did not havedata on diabetic neuropathy, another important microvascularcomplication in type 1 diabetes. The use of CAC as a marker of CAD
rather than traditional end points such as coronary artery stenosis,myocardial infarction, or death is another important limitation of thisstudy. However, CAC is accepted as a quantifiable, reliable, noninva-sive marker of the extent of coronary atherosclerosis, and CACpprogression predicts both fatal and nonfatal coronary events (Shaw,Raggi, Schisterman, Berman, & Callister, 2003). Although we adjustedfor a variety of important confounding variables, we cannot rule outthe presence of unknown risk factors that may have biased orconfounded the present analyses. Results from this study may not begeneralizable to significantly younger or older subjects with type 1diabetes or to cohorts with optimal ABC control, however our data onABC control is comparable to what was recently published by NHANES(Stark Casagrande et al., 2013). We also acknowledge that micro-albuminuria as a proxy for DN is not without controversy (Perkinset al., 2003), and for that reason added rapid GFR decline by cystatin Cas a renal outcome, which is a strength of our study.
In summary, micro- and macrovascular complications clustered inour cohort of adults with type 1 diabetes. Especially the presence ofDN was strongly associated with increased odds of progression ofsubclinical atherosclerosis, independent of glycemic control, dyslip-idemia and hypertension. ABC goal achievement at baseline stronglypredicted microvascular complications, but not progression ofsubclinical atherosclerosis. We must create better strategies toovercome current barriers to optimal ABC control and also identifynovel therapeutic targets to supplement conventional risk factors soindividuals with diabetes can live longer and healthier lives withoutdebilitating vascular complications.
Author contributions
PB researched, wrote, contributed to discussion, and reviewed/edited the manuscript; DMM researched, contributed to discussion,and reviewed/edited the manuscript; MR designed the CACTI Study,researched, contributed to the discussion and reviewed/edited themanuscript; RJJ contributed to the discussion and reviewed/edited themanuscript; JKSB researched, contributed to the discussion, andreviewed/edited the manuscript.
Acknowledgments
Support for this study was provided by NHLBI grant R01 HL61753,HL79611, and HL113029, JDRF grant 17-2013-313, and DERC ClinicalInvestigation Core P30 DK57516. The study was performed at theAdult CTRC at UCD support by NIH-M01-RR00051, at the BarbaraDavis Center for Childhood Diabetes and at Colorado Heart ImagingCenter in Denver, CO. Dr. Maahswas supported by a grant fromNIDDK(DK075360), Dr. Snell-Bergeon by an American Diabetes AssociationJunior Faculty Award (1-10-JF-50) and Career Development Award(7-13-CD-10). Drs. Petter Bjornstad and Janet K. Snell-Bergeon areguarantors of this work and, as such, had full access to all the data inthe study and take responsibility for the integrity of the data and theaccuracy of the data analysis.
References
Akasaka, T., Yoshida, K., Hozumi, T., et al. (1997). Retinopathy identifies markedrestriction of coronary flow reserve in patients with diabetes mellitus. Journal of theAmerican College of Cardiology, 30, 935–941.
Alman, A. C., Maahs, D. M., Rewers, M. J., & Snell-Bergeon, J. K. (2014). Idealcardiovascular health and the prevalence and progression of coronary arterycalcification in adults with and without type 1 diabetes. Diabetes Care, 37, 521–528.
(2013) Standards of medical care in diabetes. Diabetes Care, 36(Suppl 1), S11–S66.Bjornstad, P., Cherney, D., & Maahs, D. M. (2014). Early diabetic nephropathy in type 1
diabetes – new insights. Current opinion in endocrinology, diabetes, and obesity, 21,279–286.
Bjornstad, P., Maahs, D. M., Cherney, D. Z., Cree-Green, M., West, A., Pyle, L., & Nadeau, K.J. (2014). Insulin Sensitivity Is an Important Determinant of Renal Health inAdolescents With Type 2 Diabetes. Diabetes Care. pii: DC_141331. [Epub ahead ofprint] PMID: 25071077.

766 P. Bjornstad et al. / Journal of Diabetes and Its Complications 28 (2014) 762–766
Bjornstad, P., Maahs, D., Johnson, R., Rewers, M., & Snell-Bergeon, J. (2014). Estimatedinsulin sensitivity predicts regression of albuminuria in type 1 diabetes. Diabeticmedicine: a journal of the British Diabetic Association (In Press).
Bjornstad, P., Maahs, D. M., Rivard, C. J., Pyle., L., Rewers, M., Johnson, R. J., et al. (2014).Serum uric acid predicts vascular complications in adults with type 1 diabetes: Thecoronary artery calcification in type 1 diabetes study. Acta Diabetologica [Epubahead of print].
Bjornstad, P., Snell-Bergeon, J. K., McFann, K., et al. (2014). Serum uric acid and insulinsensitivity in adolescents and adults with and without type 1 diabetes. Journal ofDiabetes and its Complications, 28, 298–304.
Bjornstad, P., Snell-Bergeon, J. K., Rewers, M., Jalal, D., Chonchol, M. B., Johnson, R. J.,et al. (2013). Early diabetic nephropathy: A complication of reduced insulinsensitivity in type 1 diabetes. Diabetes Care, 36, 3678–3683.
Bjornstad, P., & Wadwa, R. P. (2014). Risks and benefits of statin use in young peoplewith type 1 diabetes. Current Diabetes Reports, 14, 499.
Boertien, W. E., Riphagen, I. J., Drion, I., et al. (2013). Copeptin, a surrogate marker forarginine vasopressin, is associated with declining glomerular filtration in patientswith diabetes mellitus (ZODIAC-33). Diabetologia, 56, 1680–1688.
Chalmers, J., & Arima, H. (2010). Importance of blood pressure lowering in type 2diabetes: Focus on ADVANCE. Journal of Cardiovascular Pharmacology, 55, 340–347.
Fenske, W., Wanner, C., Allolio, B., Drechsler, C., Blouin, K., Lilienthal, J., et al. (2011).Copeptin levels associate with cardiovascular events in patients with ESRD andtype 2 diabetes mellitus. Journal of the American Society of Nephrology: JASN, 22,782–790.
Ficociello, L. H., Perkins, B. A., Roshan, B., Weinberg, J. M., Aschengrau, A., Warram, J. H.,et al. (2009). Renal hyperfiltration and the development of microalbuminuria intype 1 diabetes. Diabetes Care, 32, 889–893.
Forlenza, G. P., & Rewers, M. (2011). The epidemic of type 1 diabetes: What is it tellingus? Current Opinion in Endocrinology, Diabetes, and Obesity, 18, 248–251.
Gerstein, H. C. (2002). Epidemiologic analyses of risk factors, risk indicators, riskmarkers, and causal factors. The example of albuminuria and the risk ofcardiovascular disease in diabetes. Endocrinology and Metabolism Clinics of NorthAmerica, 31, 537–551.
Gerstein, H. C., Mann, J. F., Yi, Q., Zinman, B., Dinneen, S. F., Hoogwerf, B., et al. (2001).Albuminuria and risk of cardiovascular events, death, and heart failure in diabeticand nondiabetic individuals. JAMA: The Journal of the American Medical Association,286, 421–426.
Grassi, M. A., Mazzulla, D. A., Knudtson, M. D., Huang, W. W., Lee, K. E., Klein, B. E., et al.(2009). Patient self-report of prior laser treatment reliably indicates presence ofsevere diabetic retinopathy. American Journal of Ophthalmology, 147, 501–504.
Grassi, M. A., Sun, W., Gangaputra, S., Cleary, P. A., Hubbard, L., Lachin, J. M., et al. (2013).Validity of self-report in type 1 diabetic subjects for laser treatment of retinopathy.Ophthalmology, 120, 2580–2586.
Gunnlaugsdottir, E., Halldorsdottir, S., Klein, R., et al. (2012). Retinopathy in old personswith and without diabetes mellitus: The Age, Gene/Environment Susceptibility–Reykjavik Study (AGES-R). Diabetologia, 55, 671–680.
Hallen, J., Jensen, J. K., Buser, P., Jaffe, A. S., & Atar, D. (2011). Relation of cardiac troponinI andmicrovascular obstruction following ST-elevationmyocardial infarction. AcuteCardiac Care, 13, 48–51.
Hokanson, J. E., MacKenzie, T., Kinney, G., et al. (2004). Evaluating changes in coronaryartery calcium: An analytic method that accounts for interscan variability. AJR.American Journal of Roentgenology, 182, 1327–1332.
Hu,M.C., Shi,M., Zhang, J., Quiñones,H., Griffith, C., Kuro-o,M., et al. (2011). Klothodeficiencycauses vascular calcification in chronic kidney disease. Journal of the American Society ofNephrology: JASN, 22, 124–136.
Inker, L. A., Schmid, C. H., Tighiouart, H., Eckfeldt, J. H., Feldman, H. I., Greene, T., et al.(2012). Estimating glomerularfiltration rate from serumcreatinine and cystatin C. TheNew England Journal of Medicine, 367, 20–29.
Klein, R., Marino, E. K., Kuller, L. H., et al. (2002). The relation of atheroscleroticcardiovascular disease to retinopathy in people with diabetes in the CardiovascularHealth Study. The British Journal of Ophthalmology, 86, 84–90.
Krolewski, A. S., Kosinski, E. J., Warram, J. H., Leland, O. S., Busick, E. J., Asmal, A. C., et al.(1987). Magnitude and determinants of coronary artery disease in juvenile-onset,insulin-dependent diabetes mellitus. The American Journal of Cardiology, 59, 750–755.
Krolewski, A. S., Niewczas, M. A., Skupien, J., Gohda, T., Smiles, A., Eckfeldt, J. H., et al.(2014). Early progressive renal decline precedes the onset of microalbuminuria andits progression to macroalbuminuria. Diabetes Care, 37, 226–234.
Libby, P., Nathan, D. M., Abraham, K., et al. (2005). Report of the National Heart, Lung,and Blood Institute-National Institute of Diabetes and Digestive and KidneyDiseases Working Group on Cardiovascular Complications of Type 1 DiabetesMellitus. Circulation, 111, 3489–3493.
Lim, K., Lu, T. S., Molostvov, G., Lee, C., Lam, F. T., Zehnder, D., et al. (2012). VascularKlotho deficiency potentiates the development of human artery calcification andmediates resistance to fibroblast growth factor 23. Circulation, 125, 2243–2255.
Maahs, D. M., Jalal, D., Chonchol, M., Johnson, R. J., Rewers, M., & Snell-Bergeon, J. K.(2013). Impaired renal function further increases odds of 6-year coronary arterycalcification progression in adults with type 1 diabetes: The CACTI study. DiabetesCare, 36, 2607–2614.
Maahs, D. M., Jalal, D., McFann, K., Rewers, M., & Snell-Bergeon, J. K. (2011). Systematicshifts in cystatin C between 2006 and 2010. Clinical journal of the American Societyof Nephrology: CJASN, 6, 1952–1955.
Maahs, D. M., Kinney, G. L., Wadwa, P., Snell-Bergeon, J. K., Dabelea, D., Hokanson, J., et al.(2005).Hypertensionprevalence, awareness, treatment, and control inanadult type1diabetes population and a comparable general population.Diabetes Care, 28, 301–306.
Orchard, T. J., Secrest, A. M., Miller, R. G., & Costacou, T. (2010). In the absence of renaldisease, 20 year mortality risk in type 1 diabetes is comparable to that of thegeneral population: A report from the Pittsburgh Epidemiology of DiabetesComplications Study. Diabetologia, 53, 2312–2319.
Palmer, L. J. (1948). Medical and surgical vascular complications of diabetes. Journal ofthe American Medical Association, 138, 351–353 (Disc, 355).
Perkins, B. A., Ficociello, L. H., Silva, K. H., Finkelstein, D. M., Warram, J. H., & Krolewski,A. S. (2003). Regression of microalbuminuria in type 1 diabetes. The New EnglandJournal of Medicine, 348, 2285–2293.
Schauer, I. E., Snell-Bergeon, J. K., Bergman, B. C., Maahs, D. M., Kretowski, A., Eckel, R. H.,et al. (2011). Insulin resistance, defective insulin-mediated fatty acid suppression,and coronary artery calcification in subjects with and without type 1 diabetes: TheCACTI study. Diabetes, 60, 306–314.
Shaw, L. J., Raggi, P., Schisterman, E., Berman, D. S., & Callister, T. Q. (2003). Prognosticvalue of cardiac risk factors and coronary artery calcium screening for all-causemortality. Radiology, 228, 826–833.
Snell-Bergeon, J. K., Hokanson, J. E., Jensen, L., MacKenzie, T., Kinney, G., Dabelea, D.,et al. (2003). Progression of coronary artery calcification in type 1 diabetes: Theimportance of glycemic control. Diabetes Care, 26, 2923–2928.
Stark Casagrande, S., Fradkin, J. E., Saydah, S. H., Rust, K. F., & Cowie, C. C. (2013). Theprevalence of meeting A1C, blood pressure, and LDL goals among people withdiabetes, 1988-2010. Diabetes Care, 36, 2271–2279.
van Hecke, M. V., Dekker, J. M., Stehouwer, C. D., Polak, B. C., Fuller, J. H., Sjolie, A. K., et al.(2005). Diabetic retinopathy is associated with mortality and cardiovasculardisease incidence: The EURODIAB prospective complications study. Diabetes Care,28, 1383–1389.