Embed Size (px)
Citation preview

Dietary Fiber inManagement of Diabetes
Aaron I. Vinik, MDDavid J.A. Jenkins, MD
Current evidence suggests that high-fiber diets,especially of the soluble variety, and soluble fibersupplements may offer some improvement incarbohydrate metabolism, lower total cholesterol andlow-density lipoprotein (LDL) cholesterol, and haveother beneficial effects in patients with non-insulin-dependent diabetes mellitus (NIDDM). Diets enrichedwith wheat bran and guar gum induce 10-20%reductions in serum cholesterol and LDL in both normo-and hypercholesterolemic subjects and have the abilityto blunt the hypertriglyceridemic effects of diets high incarbohydrate and low in fiber. In insulin-dependentdiabetes mellitus (IDDM) the situation is less clear, buta decrement of the circadian glucose profile has beenshown. Americans, in general, consume too little fiber.With the need to restrict fat and reduce protein, anincrease in carbohydrates is mandatory. A practical goalwould be to establish the present level of fiber intake(15-30 g/day) and to gradually increase it. An intake ofup to 40 g of fiber per day or 25 g/1000 kcal of foodintake appears beneficial; in many individuals onweight-reducing diets higher levels may be unacceptablebecause of gastrointestinal side effects. The level ofmaximum benefit has not been determined. Fibersupplementation appears beneficial only if given witha diet comprising approximately half of the calories ascarbohydrate. Foods should be selected with moderateto high amounts of dietary fiber from a wide variety ofchoices to include both soluble and insoluble types offiber. Insufficient data are available on the long-termsafety of high-fiber supplements. People at risk fordeficiencies, such as postmenopausal women, the
From the Departments of Internal Medicine and Surgery, The University ofMichigan, Ann Arbor, Michigan, and the Departments of Medicine and Nutri-tional Sciences, St. Michael's Hospital, University of Toronto, Toronto, Canada.
Address correspondence and reprint requests to Aaron I. Vinik, MD, Univer-sity of Michigan Medical Center, 2922 B. Taubman Health Center, 1500 E.Medical Center Drive, Ann Arbor, Ml 48109.
elderly, or growing children, may require supplementsof calcium and trace minerals. People with uppergastrointestinal dysfunction are at risk of bezoarformation and cautioned against a diet high in fiber ofthe leafy vegetable type. Careful attention must be paidto insulin dose because hypoglycemia can result if thereis a radical change in fiber intake and insulin dose is notreduced appropriately. Care must be exercised in theuse of "novel" fibers, including the wood celluloses,because little is known of their safety and efficacy.Diabetes Care 11:160-73,1988
The diabetic diet has undergone considerable re-vision, often without scientific basis, yet a num-ber of highly controversial issues remain. Centralto these issues is the liberalization of carbo-
hydrate intake and the recommended increases inconsumption of fiber. In the 1971 guidelines of theAmerican Diabetes Association (ADA), a liberalizedcarbohydrate intake was recommended but no specificmention of the fiber content was made (1). In the 1979policy statement, the ADA recommended reducing theintake of fat and increasing that of complex carbohy-drates to -50% of the total calories with the ingestionof foods high in fiber as desirable (2). Dietary advice topatients with diabetes continues to emphasize the vir-tues of complex carbohydrates rich in fiber, but thedogma is coming under closer scrutiny and remains acontroversial issue (3-6). These diets are substantiallydifferent from the average American diet, and it has beensuggested that they may not be effective if the insulinsecretory capacity is compromised. These diets may proveunacceptable in certain people and may have untowardeffects in patients with autonomic neuropathy (7,8). In
160 DIABETES CARE, VOL. 11, NO. 2, FEBRUARY 1988

A.I. VINIK AND D.J.A. JENKINS
addition, they have not been tested adequately in spe-cial subsets of patients whose vitamin and mineral statusmay in the long term be at risk.
We briefly review the history of dietary vicissitudes indiabetes, including what the term fiber means and itspossible mode of action. More recent studies will bereviewed that have shed light on the value of fiber man-agement of diabetes, obesity, hyperlipidemia, and thespecial needs of subsets of patients with diabetes. Rec-ommendations will be made that are based on the evi-dence adduced.
HISTORICAL NOTE
High-carbohydrate diets are not new to diabetes. Morethan 2000 years ago, physicians in India were treatingtype II (non-insulin-dependent) obese diabetic patientswith high-carbohydrate diets containing cereal grainsand legumes. Some 1900 years ago, Aretaeus of Cap-padocia (9) advised people with the symptoms of dia-betes to eat a diet consisting of milk, cereals, and starch.Other famous protagonists of high-carbohydrate dietswere von Duering (10), who in 1868 introduced the ricediet, Mosse (11), who developed the potato diet in 1903,and van Noorden (12), who in 1912 recommended oat-meal as a cure. It took almost a quarter of a century forthese suggestions to be examined seriously, and Hims-worth in 1935 (13) showed that in normal healthy sub-jects the ingestion of a diet high in carbohydrate im-proved glucose tolerance. This he attributed to increasedinsulin sensitivity.
The first suggestion that dietary fiber may be involvedwith diabetes was made by Trowell (14). Diabetes wasrare in the ancient empires of Rome and Greece. It wasalso rare in primitive people living in rural East Africawho had high-fiber intakes but became prevalent withthe processing of food. Trowell also noted that the di-abetes mortality during World War II closely followedthe use of low-extraction, low-fiber white flour in placeof the high-extraction, high-fiber natural flour (15). In1976, Trowell hypothesized that fiber-depleted diets areconducive to diabetes in susceptible human genotypes.This hypothesis is supported by the relative rarity of di-abetes in adult African men (1%), who consume 10-25g of crude fiber per day, and the frequency of diabetesin American and British men (>3%), who eat 3.5-11 gof crude fiber per day (16-18).
In the mid to late 1970s, Anderson and colleagues(19-22) showed that diabetic subjects fed a diet high incarbohydrate and fiber had reduced blood glucose lev-els and diminished insulin requirements. At the sametime, Jenkins and colleagues (23,24) demonstrated thatpurified viscous fiber without alteration in the carbo-hydrate intake reduced postprandial glucose and insulinresponses to test meals in both diabetic and nondiabeticvolunteers. Addition of purified viscous fiber to meta-bolic diets resulted in reduced urinary losses of glucoseand ketone bodies (25). The results of these studies havebeen confirmed by others (26-31).
These epidemiological leads and the evidence thathas accumulated on use of fiber in treatment of diabeteshave led to recommendations by the American (2), Ca-nadian (32), and British (33) Diabetes Associations toincrease fiber as a means of reducing the postprandialblood glucose rise. In fact, the American College ofCardiology has now adopted these recommendations.However, diabetes is a complex disease in which theexact relevance of postprandial hyperglycemia is notalways clear, and the issue of reducing the fasting orbasal blood glucose appears more important. Also obes-ity and hyperlipidemia may be of greater consequencein the long term than postprandial hyperglycemia. Be-fore embarking on an examination of the different stud-ies and their implications, the definition of the term fiberand its proposed mechanism of action must be dis-cussed.
DEFINITION OF DIETARY FIBER
Many terms have been used interchangeably to refer tofiber. It has most recently been defined as "endogenouscomponents of plant material in the diet which are re-sistant to digestive enzymes produced by man. They arepredominantly nonstarch polysaccharides and lignin andmay include, in addition, associated substances" (34,35).Dietary fiber should not be confused with crude fiber,which is a term referring to the residue of plant foodremaining after the sequential extraction with a solvent,dilute acid, and alkali (36) and eliminates hemicel-lulose and soluble fiber fractions, giving a value thatmay be one-fifth that of the true dietary-fiber value (37).
Several other terms are loosely used interchangeablyas "fiber" but do not necessarily mean the same. Resi-due or bulk refers to the indigestible content of foodsuch as is found in plant fiber but is also used to referto increases in fecal output regardless of whether anyportion of the food being referred to remains in the colonafter digestion. Roughage describes certain types of foodsin the diet and includes high-fiber foods. Bulk simplyrefers to that component of foods that has the capacityto retain water and thereby to increase the weight of thestool, such as wheat bran, which is a by-product of themilling process and comprises the outer layers of thewheat grain including the aleurone layer.
The quantitation of total dietary fiber has proved dif-ficult until recently because of the lack of appropriatemethodology. The Association of Official AnalyticalChemists (AOAC), after conducting an extensive study(36), agreed to accept a standard method (37,38) formeasuring total dietary fiber in food based on the en-zymatic degradation and gravimetric determination ofthe residue. The needs of physiologists, however, differfrom those of the analytical chemists. A standardizedmethod is needed to quantify the content of the water-soluble and -insoluble components and identify theindividual sugar polymers, polygalacturonic acids, ga-lactomannans, (3-glucans, rhamnogalacturans, arabi-nogalactans, and others that may contribute to the ef-
DIABETES CARE, VOL. 11 , NO. 2, FEBRUARY 1988 161

DIETARY FIBER
fects observed. Among the methods currently availableto measure these various subfractions, the Southgatechemical fractionation procedure (37) coupled with gas-liquid chromatography (38) appears to be the best avail-able standard; it has been used by Anderson (39) toderive an extensive list of the fiber content of variousfoodstuffs in common usage.
For convenience, fibers may be divided into two broadclasses: the so-called soluble and the insoluble. The sol-uble consist of the gums, gels, mucillages, pectic sub-stances, and a portion of what used to be called thehemicelluloses. The insoluble consist of the noncarbo-hydrate fiber component, lignin, cellulose, and some ofthe hemicelluloses, especially those combined with lig-nin. In general, it is the soluble fibers that have beendemonstrated to have effects on carbohydrate and lipidmetabolism. They are fermented to gas and short-chainfatty acids in the colon and contribute little to fecal bulkbecause the acids are rapidly cleared. The insoluble fi-bers, on the other hand, are largely responsible for in-creasing the bulk of the feces but have little metaboliceffect. The effects of the soluble fibers may relate to theirability to reduce the rate of absorption of nutrients fromthe bulk phase in the lumen of the small intestine (40).In addition, soluble fibers appear to prolong the rate ofgastric emptying and intestinal transit time (41). The in-soluble fibers have the opposite effects, reducing gastricemptying and intestinal and colonic transit times (42).
There have been several attempts to determine whetherthe effects of fiber can be predicted on the basis of itsphysiochemical properties. The specific polysaccharidecomposition of each plant food may contribute to itsbiologic effects. The more pentoses in a plant food, thegreater its ability to increase fecal bulk. There is alsoevidence that particle size may be critical and the mill-ing process may yield particles that are coarse, whichhave been shown to normalize intestinal transit time(43), whereas fine bran may have much less effect onfecal bulk and may even induce constipation (44).Cooking and drying, boiling, or pureeing of cereals, len-tils, or fruit may disrupt the fiber structure or other as-pects of the food and result in the loss of capacity tonormalize metabolism with lower postprandial levels ofglucose and insulin (45). Nevertheless, an exact quan-titation of the effects of fiber on homeostasis based onthe physiochemical properties is difficult.
The claim of "high-fiber food" by various manufac-turers needs to be viewed with caution if the nature ofthe fiber and its effect on the food have not been dem-onstrated. There are a number of "novel" fibers that donot occur naturally. In addition, nonabsorbable carbo-hydrates are generated in the food preparation process,and even the physiochemical properties of the endog-enous fiber are altered. Purified cellulose preparationsare being used as a means of fortifying foods commer-cially (46) and wood cellulose has been used on theassumption that it represents natural fiber. Evidence islacking that these fibers will produce the effects asso-ciated with the ingestion of fiber-containing foods. In
addition, the safety and efficacy of these fibers have notbeen evaluated; the mechanism of action of these fiberswill be reviewed in more detail.
PHYSIOLOGIC EFFECTS OF FIBER
The suggested benefits of increased intake of fiber in-clude not only the reduction in postprandial rise in bloodglucose concentration but also lower basal glucose con-centration, enhanced sensitivity to insulin, and lowercholesterol level. Any theories of the mechanism of ac-tion of fiber should therefore address all these obser-vations.Altered transit time. Early studies indicated that fiberof the gelling variety was capable of reducing the rateof bulk-phase diffusion in a model for small intestineabsorption (40). However, subsequent studies focusedon the effect of viscous fiber to delay gastric emptyingtime (41). It was thought that the slowing of gastric emp-tying was the most important mechanism for the ob-served effects of fiber coupled with the information that,when added to meals, postprandial hyperglycemia wasreduced. However, the results of gastric emptying stud-ies depend on the conditions at the time of testing. Muchof the work relating to the slowing of gastric emptyingby guar gum and pectin used hypertonic liquid test meals(41,47,48) and the results may not be relevant to theemptying of solid meals of dry matter (49,50). Harju etal. (51,52) have used pectin and guar gum to relievesymptoms of patients with dumping syndrome. In thelatter study, prolongation of the gastric emptying timefor solids was noted with guar (52). Blackburn et al. (53)have shown that in diabetic subjects, although there isa delay in gastric emptying and glucose levels are re-duced, there is no correlation between the two, sug-gesting that this mechanism might contribute but cannotbe the sole mechanism contributing to the reduced post-prandial responses.Effects within small intestine. The soluble fibers, e.g.,guar and pectin, increase intestinal transit time (41),whereas the insoluble fibers such as wheat bran andwhole grain decrease the intestinal transit time and in-crease intestinal bulk. Studies with D-xylose have shownthat the glucose-lowering effects may be a consequenceof decreased rate of carbohydrate absorption rather thanincreased total glucose utilization or suppression of he-patic glucose production (40). The possible effects offiber within the small intestine include changes in mix-ing, motility, and convection; intraluminal digestionrates; thickness of the unstirred layer; inhibition of max-imum transport capacity; altered pH profile; and, withlong-term treatment, altered intestinal morphology.Blackburn et al. (53), on the basis of small intestineperfusion studies in normal individuals, suggested thatfiber inhibited intestinal motility and thus decreasedconvection. There is also some evidence from in vitrostudies that the thickness of the unstirred layer may beincreased by the tendency of the soluble fibers to form
162 DIABETES CARE, VOL. 11, NO. 2, FEBRUARY 1988

A.I. VINIK AND D.J.A. JENKINS
gels and thus to effectively create a gel-filtration systemwith the gut (42). However, studies in humans showedthat only with pectin was there evidence of an increasein the thickness of the unstirred water layer. With guarthis was not found and here the weight of evidencepoints to a reduced rate of bulk diffusion (53). There isalso speculation that fiber may package carbohydratemolecules and insulate them from the digestive enzymesin the intestine and decrease access to the intestinal wall(50). Certain high fibers may have antienzyme activity(50). Fiber has been shown to reduce pancreatic en-zyme activity and decrease pancreatic enzyme secretion(54,55).Gut hormone effects. As might be expected from itsability to alter the rate and site of nutrient absorption inthe gut, dietary fiber has been shown to influence therelease of gut hormones. The response of gastric inhib-itory polypeptide (GIP), a stimulus for insulin secretion,was more attenuated in healthy diabetic subjects and inpatients with postgastrectomy dumping syndrome afteringesting fiber-supplemented meals than after controlmeals (56,57). With smaller amounts of fiber, Levitt etal. (7) found no reduction in GIP response to a mixedmeal but did record distinctly lower plasma glucagonresponses, an observation confirmed by others (58). Al-though this may have contributed to the lesser hyper-glycemia, it may be due to reduction in amino acidabsorption with the fiber-supplemented meal. An inter-esting observation has been the demonstration of an en-hanced release of plasma somatostatin with fiber (59).Somatostatin delays the absorption of carbohydrate andglucose from the small intestine and could be partlymediating the effects of fiber. Further studies are clearlyneeded.Peripheral metabolic effects. Numerous studies havedemonstrated that the lowered blood glucose levels seenafter fiber consumption are associated with either un-changed or lowered insulin levels (49,56). These acuteeffects cannot be ascribed to increased insulin sensitivitybut may be due to the slowed rate of intestinal transitand an attenuated stimulus; however, the observationin some studies that chronic ingestion of fiber is asso-ciated with lower basal glucose levels and decreasedurinary excretion of C-peptide (60,61) suggest an in-crease in insulin sensitivity or a decreased demand forinsulin. Indeed, in the studies where this has been ex-amined (62-64), an increase in insulin binding to mon-ocyte receptors for insulin has been found. This effectmay clearly have some importance in the obese patient.The changes in binding, however, must be separatedfrom those of weight reduction and improvement in di-abetes control.
Using an artifical pancreas (Biostator), Christiansen etal. (65a) endeavored to measure the effect of guar oninsulin requirements in seven patients with insulin-de-pendent diabetes mellitus (IDDM). They found that themean 24-h requirements were reduced by 12.4%.Absorption of organic substances. The cation-ex-change capacity of fibers relates to their content of ion-
izable groups such as the uronic acid residues of thepectins and hemicelluloses. This property enables somefibers to bind minerals (64) such as calcium, iron, andzinc and to bind organic substances as well (65,66).Insoluble fibers such as cellulose have been shown tobind Ca2+, and the presence of phytin foods, rich ininsoluble fiber, have been associated with minimal de-ficiency. It has been suggested from in vitro studies thatfiber in the diet may bind cholesterol and bile salts inthe gut, thus interfering in the enterohepatic circulationof cholesterol (67,68). Changes in lipid metabolism sug-gest that fiber may exert actions in the intestine thatfacilitate the lipid- and cholesterol-lowering effects offiber (69,70). These include effects on low-density chy-lomicra synthesis and the site of absorption of lipids(69-79). Alternative mechanisms embrace the alteredvery-low-density lipoprotein (VLDL) turnover discussedelsewhere in this issue.Effects in large bowel. Bacterial fermentation of fiberin the colon generates short-chain fatty acids that mayinhibit fatty acid mobilization and intestinal synthesisand decrease gluconeogenesis (45,53). Indeed, this hasbeen the basis of the development of a number of pu-tative oral hypoglycemic agents. The role of the short-chain fatty acids in enhanced glucose utilization, insulinsecretion, and hepatic glucose utilization needs furtherelaboration.
EFFECTS OF HIGH-FIBER DIETS ON PATIENTSWITH DIABETES
Two major approaches have been used to study the ef-fects of fiber on carbohydrate metabolism in diabetes:the first uses purified fiber such as guar and pectin, andthe second increases the fiber content of the diet withnormally available fibers. There are many papers in theliterature dealing with the role of dietary fiber in man-agement of diabetes. All have made important contri-butions to understanding the possible role of fiber; how-ever, it has been difficult to arrive at a consensus opinionbecause of the widely different strategies used to studythe problem. Studies have used different types of fiberthat may have very different effects, and the dose of fiberused has varied among studies. Soluble and insolublefibers whose effects may counteract each other havebeen used in combination. Studies that examined acuteeffects or studies carried out for only short periods in ametabolic ward may not necessarily apply in the homeor natural environment. Altering fiber and macronutrientcontent of the diet has led to difficulty in ascribing theeffects to fiber alone. Separation of the effects of fiberfrom those of weight reduction, calorie restriction, car-bohydrate restriction, and the initial level of diabetescontrol have all made interpretation difficult. Testing theeffects of fiber on plasma lipids and lipoproteins hasbeen inconsistent. The evaluation of responses based onthe different reports with fasting blood glucose, post-
DIABETES CARE, VOL. 11 , NO. 2, FEBRUARY 1988 163

DIETARY FIBER
prandial glucose, urinary glucose, and HbA, has beenhighly varied.
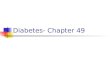
Several early investigators, including Jenkins et al. inOxford (79,80), Levitt et al. in South Africa (7), andGoulder and colleagues in Britain (57,81), have dem-onstrated that the addition of the unabsorbable polysac-charides guar and pectin reduced postprandial glycemiain both normal and diabetic subjects, often with a re-duced need for insulin secretion. The fibers that weremost effective were those with the highest viscosity (40),which may be related to an effect on the slowing ofgastric emptying (40,41), or limited diffusion of diges-tive products (40,42). To be effective, the fiber had tobe incorporated into the food (82), because fiber thatwas given in capsule (83), sprinkled on food (84), ortaken before a meal (85) was found to be ineffective.The ingestion of fiber with one meal was found to retardthe hyperglycemia with a second meal (60). Nonviscousfibers such as those found in wheat bran had less markedeffects than the viscous fibers that were reported to besuccessful (27,69,86,87). The acute effects of fiber maybe dose dependent. Both glucose and insulin responseswere lowered in diabetic subjects given test meals sup-plemented with a total of 26 g guar and pectin. Glucoseresponse fell 30% in IDDM and from 30 to 60% in non-insulin-dependent diabetes mellitus (NIDDM) with a 42to 60% decrease in the insulin response (56,79). In thestudies carried out by others, the reduction in the insulinresponse was not found with 9-18 g but did occur with26 g, suggesting a dose-dependent effect (Fig. 1).
Test-meal studies were followed up with short-termmetabolic studies in which 14-26 g guar given daily,mixed with the food, reduced the urinary glucose and3-hydroxybutyrate losses by 40% compared with thecontrol period. In further studies with guar crispbread,relative reductions in fasting blood glucose were seen.Such findings were confirmed in longer-term studies witha guar granulate that demonstrated, in addition, im-proved postprandial blood glucose levels and lower in-sulin responses. Reduced urinary glucose levels and in-
EFFECTS OF FIBERS ON CHOLESTEROL AND GLUCOSE
oQHIoc
0 10 20 30% REDUCTION OF FASTING BLOOD GLUCOSE
FIG. 1. Compilation of data in literature showing bene-ficial effects of soluble fibers on cholesterol and glucoseand relatively weak or negative effects of insoluble andfruit fibers.
sulin requirements were sustained for studies lasting upto 1 yr.
Until recently, however, no acceptable purified fiberpreparation was commercially available for clinical use.Currently, several preparations are available, and thesehave been employed in studies in Europe and more re-cently in the United States and elsewhere.
Several new studies from England, Ireland, and Fin-land were described at a Guar Symposium held in Lon-don in December 1985. Most studies showed beneficialeffects of adding varying amounts of guar to the regularmeal plan but were short term and not well controlled(88).
INCREASING FIBER IN ORDINARY FOODS
Rather than supplementing diets with purified fibers,many investigators have studied the relationship of dietto diabetes control by modifying the traditional diabeticdiet by use of ordinary foods high in fiber content. Thesediets generally contain substantial amounts of foods inwhich the carbohydrate is slowly digested and absorbedand could also be described as lente carbohydrate (89).Legumes such as peas and beans produce the least risein blood glucose (90). Anderson et al. (20-22,77,91)devised high-fiber diets that have been very successfulin improving diabetic control. These diets contain 70%carbohydrate and 35 g dietary fiber/1000 kcal. BothIDDM and NIDDM patients on this regimen for 16-18days showed significant decreases in both fasting andpostprandial glucose concentrations. A majority of pa-tients had decreased or discontinued insulin or sulfo-nylurea therapy (77,91). Those patients who followedhigh-fiber maintenance diets with 60% carbohydrate forup to 15-21 mo have shown additional reduction infasting blood glucose levels that enabled further de-crease or discontinuation of the hyperglycemic medi-cation. Many obese subjects were able to decrease theirinsulin dose or discontinue sulfonylurea on the high-carbohydrate high-fiber diet. The greatest reduction inglucose levels and insulin doses, however, occurred inthose who had the greatest degree of weight reduction(92). In a 6-wk study, Simpson et al. (26) reported amodest reduction in fasting and postprandial glucoseconcentrations but a significant reduction in 24-h urineglucose on a diet containing large amounts of legumes.In this study and others, however, it was difficult todetermine whether the improved glucose control wasdue to the high-carbohydrate content of the diet or therate of digestion of the legume starch or the fiber (93).
LONG-TERM EFFECTS
Contrasting with these observations are those of an 8-wk metabolic study in which the amount and source ofthe carbohydrate were kept constant and the fiber waseither low (11 g/1000 kcal) or high (27 g/1000 kcal)
164 DIABETES CARE, VOL. 11, NO. 2, FEBRUARY 1988

A.I. VINIK AND D.).A. JENKINS
(94,95). No significant effects were found in glucosecontrol, postprandial glucoses, or HbA, or in the insulinrequirements in adult patients with NIDDM.
The problems in interpreting findings is further illus-trated by the impact of the associated carbohydrate con-tent of the diet on the effects of fiber. Studies with guarhad only demonstrated consistent effects in reducingurinary glucose levels where patients were on highercarbohydrate intakes. Riccardi et al. (74) studied theeffects of three outpatient diets (low CHO, 42%, lowfiber, 20 g; high CHO, 53%, low fiber, 16 g; and highCHO, 53%, high fiber, 54 g) over a 10-day period andfound that improved glucose tolerance was observedonly with the high-carbohydrate high-fiber diet.
Mann (61) examined 18 patients with NIDDM on alow-carbohydrate diet in a crossover design with a high-carbohydrate diet rich in cereal, vegetable, and fruitfiber. Each diet was carried out for a period of 6 wkand, after a metabolic profile, the diets were reversedfor a further 6 wk, after which the volunteers were ad-mitted for a final 24-h profile. Carbohydrate comprised59% of the total energy, with 44 g total dietary fiber. Inpatients with IDDM as well as those with NIDDM asignificant improvement was seen in fasting and pre-prandial blood glucose levels as well as in the HbA!.No significant change was found, however, in post-prandial glucose levels. In a further series of experi-ments, the incorporation of substantial quantities ofcooked dried beans into ordinary meals (e.g., haricot,red kidney beans, and lentils) as a source of soluble fiberwas examined in both IDDM and NIDDM patients (93).Significant reduction was found in the basal, prepran-dial, 2-h postprandial, daily mean, and 24-h urine glu-cose excretion on this high-carbohydrate diet. In addi-tion, total and low-density lipoprotein (LDL) cholesterollevels fell without any associated increase in triglyceridelevels. High-density lipoprotein (HDL) cholesterol andHDL/LDL ratio tended to increase (28).
These findings have been confirmed and appear toapply equally well to diabetic children (24). These stud-ies, however, were done in both NIDDM and IDDMpatients who were relatively well controlled. Patientswho had NIDDM were more prone to significant de-grees of hypoglycemia; 6 wk of this high-carbohydratediet caused a significant reduction in HbA, (from 10.6to 8.5%), fasting glucose dropped from 9.6 to 6.8 mM,preprandial glucose from 9.9 to 7.5 mM, and the 2-hpostprandial glucose from 12.1 to 10.8 mM. Mean24-h blood glucose profile was also markedly improved,with a reduction from 11.6 to 9.3 mM (21).
In the 1970s, Brunzell et al. (95) showed that in non-diabetic subjects, patients with mild diabetes, and dia-betic patients established on treatment, a high-carbo-hydrate formula feed containing principally dextrose wasassociated with lower blood glucose levels and insulinrequirements than a low-carbohydrate high-fat formula.Simpson et al. (27) found that, on a diet of this nature,the postprandial glucose levels were significantly higher,and overall there appeared to be no difference in gly-
cemic control between the two diets. Almost identicalfindings have been reported by Riccardi et al. (74). Thus,whereas digestible carbohydrate may have a small effecton fasting blood glucose levels or basal blood glucoselevels, the predominant effect of high-carbohydrate high-fiber diets results from the increase in dietary fiber. Fur-thermore, increasing carbohydrate but not dietary fiberresults in a significant decrease in HDL cholesterol. Forfiber to exert its optimum effect, it may have to be givenas a part of a high-carbohydrate diet. Viscous fiber addedto a low-carbohydrate diet of diabetic patients appearsto have little effect (50) in contrast to the same fiberadded to high-carbohydrate diets, where consistent im-provements were seen.
FIBER ENRICHMENT OFHIGH-CARBOHYDRATE FOODS
Perhaps an ideal way to achieve the maximum fibereffect is to incorporate the most effective soluble fiberforms into starchy foods. The mixing that seems impor-tant to ensure maximum effectiveness of fiber is therebyachieved, and the higher carbohydrate content of thediet is also ensured. This was achieved early with guar-enriched crispbread, and long-term studies became pos-sible that had not been possible previously due to poorpalatability of purified guar and pectin.
Gatti et al. (96) in Italy produced guar-enriched pastathat was fed in chronic studies to normal, diabetic, andhypercholesterolemic patients. A significant improve-ment in plasma glucose, daily glucose profile, and gly-cosuria was observed. In hyperlipidemic subjects areduction of triglycerides and a significant hypocho-lesterolemic effect were demonstrated.
Thompson and colleagues (97) compared the acuteresponse in 19 IDDM and NIDDM diabetic subjects tothree test meals (white bread, control pasta, and guar-enriched pasta), each containing 50 g available carbo-hydrate. They found the least postprandial rise in thegroup receiving guar pasta (4.4 ± 0.5 vs. 5.4 ± 0.4 mMin control pasta). Furthermore, guar significantly re-duced the incremental glucose area under the 3-h glu-cose-response curve. Urinary C-peptide and urinary glu-cose were also significantly reduced by guar. Nodifference was seen between IDDM and NIDDM pa-tients. The authors concluded that enriching commonlyeaten foods with guar appears an effective method ofreducing blood glucose levels and urinary glucose levelsin diabetic patients.
FIBER AND HYPERLIPIDEMIA
Of major concern in NIDDM and more recently IDDMis the increased risk of atherosclerotic heart disease, amajor cause of death (98). The possible effects of fiber
DIABETES CARE, VOL. 11, NO. 2, FEBRUARY 1988 165

DIETARY FIBER
on bile acid metabolism have been alluded to above(99,100). Of the supplemental fibers, only the solublefibers such as pectin, oat bran, and guar appear to havea cholesterol-lowering effect; 12-40 g of guar or pectin(19,72) or 50-100 g of oat bran (75) have been foundto consistently lower cholesterol in patients with hyper-cholesterolemia by —6—15%. These fibers have also beenshown to lower LDL cholesterol without a rise in tri-glycerides (19,69,70,72). In studies with natural foodsrather than supplements, a lipid-lowering effect can alsobe demonstrated if the diet is high in legumes (101,102).The rise in fasting triglyceride levels that accompany anearly increase in carbohydrate intake can often be pre-vented by a simultaneous increase in fiber intake (103).In one study in IDDM patients, addition of fiber signif-icantly reduced serum cholesterol levels from 206 to147 mg/dl without a change in triglyceride level (16).In obese diabetic outpatients after high-carbohydrate high-fiber diets, serum cholesterol and triglycerides werelowered, which may have been due partly to weightloss (92).
Where diets high in legumes (76) or where increasedproportions of soluble fiber in a variety of food sources(e.g., oats and barley) have been incorporated into thediet, levels of both serum cholesterol and triglycerideshave fallen (79). Decreases in serum triglycerides in di-abetic patients on increased-carbohydrate high-fiber dietswere also reported by Anderson and Ward {77), whomeasured the lipid responses in diabetic patients after adiet containing 60% carbohydrate and high fiber for 15mo. When fiber intakes were increased, serum triglyc-eride levels also fell from —250 to 126 mg/dl, and totalLDL cholesterol and VLDL triglycerides decreased sig-nificantly in another group of patients on a high-fiberdiet with 42% carbohydrate (78).
Long-term studies by Anderson and Ward {77) showedthat home maintenance diets containing 55-60% car-bohydrate, 20-25% fat, and 50 g plant fiber signifi-cantly reduced triglyceride concentrations while de-creasing insulin requirements in insulin-requiring NIDDMpatients. These diets were maintained for up to 4 yr(104). The exact contribution to the lipid changes of thedecrease in insulin requirement, the weight loss, or thedecrease in caloric intake is unknown.
fIBER SUPPLEMENTS
The international medical literature from 1975 to 1985contains over 100 clinical studies on the therapeutic useof guar gum, primarily in the treatment of diabetes andhypercholesterolemia, and the vast majority confirm thepromise shown in the earlier studies of Jenkins and col-leagues. The only findings to contrast with these obser-vations are those in which the fiber derived from naturalfoods or where a significant portion of the fiber wasinsoluble. In these cases, studies have been unable toshow a reduction in serum lipids (4,5,74,94,105-114).
Fiber and obesity. The suggestion that the replacementof fiber-rich foods by those depleted in fiber was a factorin the obesity of Western countries stimulated interestin the use of fiber for treatment of obesity (14). How-ever, the potential role of fiber in preventing or treatingobesity has remained an open question (115-126). Ata recent symposium on fiber and obesity, investigatorsreported on the effects of fiber on weight reduction,satiety, and compliance with complex dietary restric-tions (127). These studies were in general carried out inlarge numbers of patients attending weight-loss clinicsor in people on diets for various reasons. Although theresults appear to be conflicting, they may be related tothe dose of guar used.
In addition, where dietary advice is already being fol-lowed and in well-controlled studies, the effect of fibersupplementation may have been masked by adher-ence to a hypocaloric diet with weight loss in both testand control situations. Most agreed that fiber-treated pa-tients were more compliant and experienced less hungerand greater satiety with their meals. Forster (128) sug-gested that fiber should be used in conjunction with dietand should not be relied on as the sole means of at-tempting weight reduction.
There are therefore some encouraging data to supportthe continued need to carry out long-term studies in acontrolled manner to determine the safety and efficacyof fiber supplementation as a form of treatment of theobese diabetic patient.Fiber and pregnancy. There are few data available onthe use of fiber in pregnancy. This is mainly due to theprevailing attitude in the United States that it is inap-propriate to starve women during pregnancy. In the fewstudies that have been reported, fiber seems to be rel-atively safe. Paired oral glucose tolerance tests were per-formed during the third trimester of pregnancy in fourgestational diabetic patients. Guar produced a signifi-cant reduction in mean serum glucose at 1, 2, and 3 h,and each of the four patients showed a normal glucosetolerance curve. The authors concluded "the improve-ment is sufficient to suggest a potential clinical value inthe treatment of gestational diabetes" (129).Fiber and the elderly. Age ranges of NIDDM patientsin many of the studies described above frequently in-cluded patients ^65 yr of age. Kyllastinen and Lahikai-nen (130) supplemented the diet of 14 elderly (67- to75-yr-old) diabetic patients on oral hypoglycemics with16 g guar daily. They found a reduction (12.7%) in serumcholesterol, whereas serum calcium, magnesium, iron,and zinc were unchanged. The authors concluded that"in some elderly diabetics guar supplementation im-proved glycemic control" (130). Patient-to-patient re-sponse was variable. Uusitupa et al. (108) similarly con-cluded a study in seven elderly patients (aged 65-81yr), one on diet therapy, the others on oral hypoglycem-ics. The results showed that adding guar to the diet (5g/meal) significantly reduced postprandial blood glu-cose levels in fairly well controlled subjects. Studies car-ried out in Toronto by Kay (131) also concluded that
166 DIABETES CARE, VOL. 11, NO. 2, FEBRUARY 1988

A.I. VINIK AND D.J.A. JENKINS
increasing the fiber intake from some foods was bene-ficial if well tolerated by elderly diabetic patients.
FACTORS TO CONSIDER IN ADDITION TO FIBER
High-fiber diets that contain substantial amounts of fi-ber-rich starchy foods have been successfully used byseveral investigators (19-30). Whereas the effects wereattributed to fiber, other studies indicated that the actionmay be complex and related to the physical form of thefood, the ingestion of the previous meal, the type of foodeaten, and the rate of release of carbohydrate from thefood (40,45,50,90,115).
The fact that not all carbohydrate foods produce thesame glycemic response has long been recognized, es-pecially in the German literature. Recently, attentionhas been drawn to this by several studies (132-135)noting the very different glycemic responses generatedby the starchy foods, potato, bread, rice, and corn. Mostinteresting was the fact that potatoes elicit a glycemicresponse similar to that of an equivalent amount of glu-cose, whereas parboiled rice elicits a much flatter re-sponse (132). Further studies emphasized that the formof the food is important; i.e., parboiled rice produces amuch flatter response than regular rice, and ground ricea much greater elevation of glucose and insulin levelsthan whole rice (135). Presumably, grinding the rice hasthe effect of making the starch more available to amyl-olytic digestion. This effect is also seen with other ce-reals such as oats, wheat, and rye. Pureed apples alsoinduce a much greater rise than whole apple (136). Asdiscussed elsewhere in this issue, studies on a variety offoods of equivalent carbohydrate content showed theglycemic response varied from 15 to 98%. Of specialinterest was the finding that, as a class, the legumesproduce the lowest glycemic response (76), which maybe due to the slow release of carbohydrate during diges-tion rather than to carbohydrate malabsorption (50,103).
Jenkins and colleagues (45,90) have demonstrated invitro, with human digestive juices, that some starchyfoods release their products of carbohydrate digestionmore slowly than others. There appears to be a goodrelationship between the rate of digestion of foods invitro and the glycemic response elicited by the foods inboth nondiabetic and diabetic people (137,138). Thedifferences in responses to different foods may be relatedto many other components in foods that alter their di-gestibility, such as fiber, enzyme inhibitors, lectins, tan-nins, phytates, sugars, fats, proteins, and starches (89).Interactions between different macronutrients (81) andthe structure of food may alter the digestibility and pro-duce very different glycemic responses. The effects offat, especially in large amounts, on the rate of gastricemptying may certainly alter the glycemic response. Thus,analysis of the dietary fiber intake and even fiber typemay not be sufficient to determine the response in anygiven situation (139).
SIDE EFFECTS OF HIGH FIBER DIETS
Concerns have been raised about the vitamin and min-eral status of people who change from a habitually lowfiber diet to one rich in fiber. Studies of vitamin andmineral status in adults on high-fiber diets have not foundevidence of deficiency (72,140).
In terms of soluble fiber supplements, Mclvor and col-leagues (141) gave at least 30 g of guar daily for 16 wkto 8 NIDDM patients, resulting in no significant changesin hematologic or hepatorenal function. Serologicscreening did not reveal a change in protein or mineralmetabolism or in electrolyte balance. Jenkins et al. (25)administered 14-26 g of guar daily for 6 mo to 8 dia-betic patients. Biochemical tests of blood showed thatguar produced no evidence of serum zinc, copper, orcalcium changes. Tuomilehto et al. (67) gave 15 g ofguar daily for 3 mo to 12 obese hypercholesterolemicpatients and at the end of this time, noted no significantchanges in 24-h urinary sodium, potassium, calcium,or magnesium. Aro et al. (142) and James et al. (65)have found no effects on serum calcium, magnesium,phosphate, iron, or urinary calcium excretion. Har-muth-Hoene (66) added 22.5 g of guar daily to a mixeddiet for 12 days and found that this did not significantlyinfluence nitrogen balance, mineral absorption, or di-gestible energy. These findings support similar obser-vations in normal volunteers on metabolic diets.
A number of studies have been carried out to examinethe absorption of important drugs such as digoxin, par-acetamol, glipizide, and penicillin. Huupponen et al.(143,144) have shown a reduction in peak levels of di-goxin and penicillin but glipizide absorption was un-changed.
Nevertheless, it is possible, especially with diets richin phytate and insoluble fiber, that absorption of cal-cium, iron, and zinc could be impaired and result indeficiencies if used for a long time in susceptible indi-viduals (114), although these deficiencies may have lit-tle significance in terms of energy balance. High-fiberdiets have also been reported to cause small increasesin fecal loss oi food energy in the form of nitrogen andfat (114). Theoretically, vitamin B12 and iron deficiencycould result if the high-fiber diets are low in ani-mal protein, but the abundance of epidemiologicaldata points against this in traditional normal fiber di-ets.
Although there is no incontrovertible evidence thatsoluble fiber supplements or moderate increases in fiberintake from mixed sources causes malabsorption ofmacro- or micronutrients, it is prudent to caution againstthe unmonitored long-term use of fiber in individuals atrisk, such as the elderly. Deleterious effects of recom-mended levels of fiber in pregnant or growing childrenare not known. No data are available on the effects ontrace minerals such as cobalt, manganese, and chro-mium, which may have further ramifications for insulinsensitivity in NIDDM.
DIABETES CARE, VOL. 11, NO. 2, FEBRUARY 1988 167

DIETARY FIBER
ADHERENCE TO MEAL-PLANNING REGIMENS
McCulloch and colleagues (145) studied 178 IDDM pa-tients focusing on their understanding of, and compli-ance with, a controlled carbohydrate diet. They foundthat 40% could not remember their dietary prescriptionand 35% did not estimate carbohydrate and scored badlyon a quiz on carbohydrate content of common foods.Quiz scores were significantly associated with HbA, lev-els. The authors concluded that "adequate dietary com-pliance is rare." To assess patients' perception of ad-vice, Cantrill and Wright (146) interviewed 56 diabeticpatients managed at diabetic clinics and a matched groupof 58 diabetic patients managed in general practice.Thirty-one percent of the general practice group and 7%of the hospital group claimed to have received no die-tary advice from any source since diagnosis. Of the 18patients who monitored their blood glucose, all wereinsulin dependent. Fifteen of the general practice groupand 16 of the hospital group did not monitor blood orurinary glucose. Of those who monitored urinary glu-cose, only 44% recorded the results, hospital patientsrecording most frequently. Of 11 patients for whom ahigh-carbohydrate high-fiber diet was prescribed, ad-herence was evaluated over a 4-yr period. Nine patientshad good to excellent adherence, one had fair adher-ence, and one had poor adherence. In the studies re-ported on fiber in the management of obesity, 67% ofpatients on fiber adhered to the weight-reduction pro-gram and could satisfy their hunger and satiety needs,whereas only 27% on the weight-reduction programwithout fiber adhered to the program and lost weight. Itdoes seem that availability of a low-calorie, guar-en-riched supplement may help individuals adhere to a se-verely calorie-restricted meal plan.
RECOMMENDATIONS FOR THE USE OF FIBER
With the recommendation of restricting fat intake to<30% and a protein intake of 0.8 g/kg (12-20% oftotal kcal) there is a need to increase carbohydrate to50-60% of the caloric intake. This amount of refinedcarbohydrate can have deleterious effects on glucoseand lipoproteins. Evidence suggests that fiber may offersome improvement in carbohydrate metabolism andlower total cholesterol, LDL cholesterol, and triglycer-ides. Fiber may also contribute to lower blood pressureand enhance weight loss in obese subjects on hypoca-loric diets. Estimates of the current dietary fiber intakeof adults in the United States range from 13 to 30g/day, with men averaging 19.1 g/day and women 13.4g/day. A practical goal would be to establish the currentintake and gradually increase it toward a goal of dou-bling the intake. Fiber should be taken in a range offoods to include both soluble and insoluble forms. Fibersupplementation appears to provide benefit only if givenwith a diet comprising at least 50% of calories as car-
bohydrate. Foods should be selected with moderate tohigh amounts of dietary fiber. The 1986/1987 exchangelists compiled by the American Diabetes Association inconjunction with the American Dietetic Association usea symbol to indicate foods with a fiber content of atleast 3 g per serving. These foods include legumes, roots,tubers, green leafy vegetables, all types of whole-graincereals (including wheat, barley, oats, corn, and rye),and fruits. Fruits and vegetables should be eaten rawand not pureed, which causes loss or reduction of thefiber effect. Abdominal cramping, discomfort, and fla-tulence can be minimized by starting with small servingsand increasing gradually. Insufficient data are availableon the long-term safety of very high fiber diets or fibersupplements, although, to date, there are no deleteriousreports. People at risk of deficiencies, e.g., postmeno-pausal women, the elderly, and growing children, mayrequire supplements of calcium and trace minerals. Sub-jects with upper gastrointestinal dysfunction are at riskof bezoar formation and should be cautioned against adiet high in leafy vegetables such as cabbage. Carefulattention must be paid to insulin dose, because hypo-glycemia can result if the dose is not reduced appropri-ately. Children may also benefit from an increase in thefiber content of their diets but may not tolerate largeamounts. Pregnant diabetic women appear to toleratefiber well, but there are too few studies to advise for oragainst its use in pregnancy. Care must be exercised inthe use of novel fibers, because little is known of theirsafety or efficacy.
SUMMARY
Whereas there is still considerable controversy over useof the high-fiber diet in treatment of diabetes and somefeel that it is premature to impose these diets on thediabetic population, others have strong convictions aboutthe benefits to be obtained. These diets appear to havebeen most effective in patients taking fewer than 30 Uof insulin daily or in NIDDM patients who are beingtreated with a diet or a sulfonylurea agent. Hyperlipid-emia has clearly shown benefit in some patients takinglarge quantities of fiber. In obese subjects, dietary fibermay aid in weight control by slowing the rate of foodingestion, inducing satiety, and decreasing the caloricdensity of the diet. However, these options should bemade available to patients with diabetes only after de-tailed discussion with the health-care providers, includ-ing the physician and the nutritionist, to determinewhether individuals can comply with the diet day today. A thorough discussion of the data, the possiblebenefits, and untoward effects of the diet is essential.In-depth counseling and individualizing meal plans foreach patient's need, with the provision of extensive rec-ipes and information on the dietary content of foods aswell as what is known of their physiologic effects, areessential for successful use of this dietary approach totreatment.
168 DIABETES CARE, VOL. 11, NO. 2, FEBRUARY 1988

A.I. VINIK AND D.J.A. JENKINS
Although much has been learned in the last few yearsabout the role of fiber in the management of the patientwith diabetes, much has yet to be learned. Central tothe whole issue is the long-term safety of high-fiber diets.The impact on calcium, trace mineral metabolism, andvitamins needs to be defined. Because patients with di-abetes may be at risk for osteopenia, it seems prudentto avoid an additional risk of negative calcium balance.
Information on the interactions of different fibers witheach other and the macronutrients of the diet is sorelyneeded. Comparisons are needed of the effects of die-tary supplements of fiber and natural selection of high-fiber foods with measurement of standardized variables,e.g., HbA,, glucose profiles, C-peptide, cholesterol (LDLand HDL), and triglycerides.
New insights into the physiologic effects of fiber inthe small intestine and the colon and the role of theshort-chain fatty acids that are generated will help in theunderstanding of their mechanism of action.
For the guidance of the individual and the generalpublic, honest labeling of food products should be en-couraged. Guidelines should be established for thestandardization of the techniques for measurements andfor validation of physiologic effects claimed for high-fiber products. The novel fibers that are appearing needto undergo as close and circumspect a scrutiny as wasdirected at the naturally occurring fibers.
REFERENCES
1. American Diabetes Association: Special report: princi-ples of nutrition and dietary recommendations for pa-tients with diabetes mellitus: 1971. Diabetes 20:633-34, 1971
2. American Diabetes Association: Special report: princi-ples of nutrition and dietary recommendations for indi-viduals with diabetes mellitus: 1979. Diabetes Care2:520-23, 1979
3. Reaven GM: How high the carbohydrate? Diabetologia19:409-13, 1980
4. Coulston A, Greenfield M, Kraemer F, Tobery T, ReavenG: Effect of source of dietary carbohydrate on plasmaglucose and insulin responses to test meals in normalsubjects. Am ) Clin Nutr 33:1279-82, 1980
5. Coulston A, Greenfield MS, Kraemer FB, Tobery TA,Reaven GM: Effect of differences in source of dietarycarbohydrate on plasma glucose and insulin responsesto meals in patients with impaired carbohydrate toler-ance. Am } Clin Nutr 34:2716-20, 1981
6. Jarrett RJ: More about carbohydrates. Diabetologia 21:427-28, 1981
7. Levitt NS, Vinik Al, Sive AA, Child PT, Jackson WPU:The effect of dietary fiber on glucose and hormone re-sponses to a mixed meal in normal subjects and in di-abetic subjects with and without autonomic neuropathy.Diabetes Care 4:515-19, 1980
8. Vinik Al, Glowniak J: Hormonal secretion in diabeticautonomic neuropathy. NY State} Med 82:871-86, 1982
9. Aretaeus: On the Causes, Symptoms and Cure of Acuteand Chronic Diseases. Moffat J, Trans. London, Rich-ardson, 1785
10. Von Duering AN: Ursache und Heilung des DiabetesMellitus. Hanover, Schmorlund Seefeld, 1868
11. Mosse A: Le diabete et I'alimentation aux pommes deterre. Paris, Alcan, 1903
12. Von Noorden C: New Aspects of Diabetes. Pathologyand Treatment. Bristol, UK, Wright, 1912, p. 100-10
13. Himsworth HP: Dietetic factor determining glucose tol-erance and sensitivity to insulin of healthy men. Clin Sci2:67-94, 1935
14. Trowell HC: Dietary-fiber hypothesis of the etiology ofdiabetes mellitus. Diabetes 24:762-65, 1975
15. Trowell HC: Definition of dietary fiber and hypothesisthat it is a protective factor in certain diseases. Am} ClinNutr 29:417-27, 1976
16. Trowell HC: Diabetes mellitus and dietary fiber of starchyfoods. Am I Clin Nutr 31 :S53-57, 1978
17. Ahrens EH Jr, Boucher CA: The composition of a sim-ulated American diet. J Am Diet Assoc 73:613-20, 1978
18. MarlettJA, Bokram RL: Relationship between calculateddietary and crude fiber intakes of 200 college students.Am 1 Clin Nutr 34:335-42, 1981
19. Kiehm TG, Anderson JW, Ward K: Beneficial effects ofa high carbohydrate, high fiber diet on hyperglycemicdiabetic men. Am ) Clin Nutr 29:895-99, 1976
20. Anderson JW, Midgley WR, Wedman B: Fiber and dia-betes. Diabetes Care 2:369-79, 1979
21. Anderson JW, Chen WL: Plant fiber: carbohydrate andlipid metabolism. Am J Clin Nutr 32:346-63, 1979
22. Anderson JW: The role of dietary carbohydrate and fiberin the control of diabetes. Adv Intern Med 26:67-96,1980
23. Jenkins DJA, Wolever TMS, Haworth R, Leeds AR,Hockaday TDR: Guar gum in diabetes. Lancet 2:1086-87, 1976
24. Kinmouth AL, Angus RM, Jenkins PA, Smith MA, BaumJD: Whole foods and increased dietary fibre improveblood glucose control in diabetic children. Arch Dis Child57:187-94, 1982
25. Jenkins DJA, Wolever TMS, Bacon S, Nineham R, LeesR, Rowden R, Lover M, Hockaday TD: Diabetic diets:high carbohydrate combined with high fiber. Am J ClinNutr 33:1729-33, 1980
26. Simpson HCR, Simpson RW, Lousley S, Carter RD, GeekieM, Hockaday TD, Mann Jl: A high carbohydrate le-guminous fibre diet improves all aspects of diabetic con-trol. Lancet 1:1-5, 1981
27. Simpson RW, Mann Jl, Eaton J, Moore RA, Carter R,Hockaday TDR: Improved glucose control in maturity-onset diabetes treated with high-carbohydrate modifiedfat diet. Br Med ] 1:1753-56, 1979
28. Simpson RW, Mann Jl, Eaton J, Carter RD, HockadayTDR: High-carbohydrate diets and insulin-dependent di-abetics. Br Med J 2:523-25, 1979
29. Simpson HCR, Carter RD, Lousley S, Mann Jl: Digestiblecarbohydrate—an independent effect on diabetic con-trol in type 2 (non-insulin dependent) diabetic patients?Diabetologia 23:235-39, 1982
30. Rivellese A, Riccardi G, Giacco A, Pacioni D, GenoveseS, Mattioli PL, Mancini M: Effect of dietary fibre on glu-cose control and serum lipoproteins in diabetic patients.Lancet 2:447-50, 1980
31. Munoz JM, Sandstead HH, Jacob RA, Logan GM Jr, ReckSJ, Klevay LM, Dintzis FR, Inglett GE, Shuey WC: Effectsof some cereal brans and textured vegetable protein onplasma lipids. Am I Clin Nutr 32:580-92, 1979
DIABETES CARE, VOL. 11 , NO. 2, FEBRUARY 1988 169

DIETARY FIBER
32. Special Report Committee of the Canadian Diabetes As-sociation: 1980 guidelines for the nutritional manage-ment of diabetes mellitus. J Can Diabetes Assoc 42:110-18, 1981
33. Nutrition Sub-Committee of the British Diabetic Asso-ciation Medical Advisory Committee: Dietary recom-mendations for the 1980s—a policy statement by theBritish Diabetic Association. Hum Nutr Appl Nutr 36:378-86, 1982
34. Report of the Expert Advisory Committee on Dietary Fiberto the Health Protection Branch. Ontario, Canada, Natl.Health and Welfare, 1985
35. Prosky L: Analysis of total dietary fiber: the collaborativestudy. In Dietary Fiber. Vahouny GV, Kritchevsky D,Eds. New York, Plenum, 1985, p. 1-16
36. Deutsch MJ: Vitamins and other nutrients. General Ref-eree Reports, Committee on Foods II. / Assoc Off AnalChem 69:259, 1986
37. Southgate DAT: Determination of carbohydrates in foods.II. Unavailable carbohydrates, j Sci Food Agric 20:331-35, 1969
38. Southgate DAT: The measurement and characterisationof cereal dietary fiber. In Proc Brood and Gezondheid,Brussels, September 10, 1985, p. 17-27
39. Anderson JW: Plant Fiber in Foods. Lexington, KY, HCFDiabetes Res. Found., 1986
40. Jenkins DJA, Wolever TMS, Leeds AR, Gassull MA,Haisman P, Dilawarie JB, Goff DV, Metz GL, AlbertiKGMM: Dietary fibres, fibre analogues and glucose tol-erance: importance of viscosity. Br Med J 1:1392-94,1978
41. Holt S, Heading RC, Carter DC, Prescott LF, Tothill P:Effect of gel fibre on gastric emptying and absorption ofglucose and paracetamol. Lancet 1:636-39, 1979
42. Eisenhans B, Sufke U, Blume R, Caspary WF: The influ-ence of carbohydrate gelling agents on rat intestinaltransport of monosaccharides and neutral amino acidsin vitro. Clin Sci 59:373-80, 1980
43. Payler DK, Pomare EW, Heaton KW, Harvery RF: Theeffect of wheat bran on intestinal transit. Gut 16:209-13, 1975
44. Wrick KL: The influence of dietary fiber source on hu-man intestinal transit and stool output, j Nutr 29:1474-79, 1976
45. Jenkins DJA, Thorne MJ, Camelon K, Jenkins A, Rao AV,Taylor RH, Thompson LU, Kalmusky J, Reichert R, Fran-cis T: Effect of processing on digestibility and the bloodglucose response: a study of lentils. Am ) Clin Nutr36:1093-101, 1982
46. Wrick KL, Robertson JB, Van Soest PJ, Lewis BA, RiversJM, Roe DA, Hackler LR: The influence of dietary fibersource on human intestinal transit and stool output. JNutr 113:1464-79, 1983
47. Wilmshurst P, Crawley JCW: The measurement of gastrictransit time in obese subjects using 24Na and the effectsof energy content and guar gum on gastric emptying andsatiety. Br j Nutr 44:1-6, 1980
48. Leeds AR, Ralphs DNL, Ebied F, Metz G, Dilawari JB:Pectin in the dumping syndrome: reduction of symptomsand plasma volume changes. Lancet 1:1075-78, 1981
49. Jenkins DJA, Leeds AR, Gassull MA, Cochet B, AlbertiKGMM: Decrease in postprandial insulin and glucoseconcentrations by guar and pectin. Ann Intern Med 86:20-23, 1977
50. Jenkins DJA, Wolever TMS, Taylor RH, Ghafari H, Jen-
kins AL, Barker H, Jenkins MJ: Rate of digestion of foodsand postprandial glycaemia in normal and diabetic sub-jects, fir Med jf 281:14-17, 1980
51. Harju E, Larmi TK: Efficacy of guar gum in preventingthe dumping syndrome. ) Parenter Enterol Nutr 7:470-72, 1983
52. Harju E, Heikkila J, Larmi TK: Effect of guar gum ongastric emptying after gastric resection.) Parenter EnterolNutr 8:18-20, 1984
53. Blackburn NA, Redfern JS, Jarjis H, Holgate AM, Han-ning I, ScarpelloJHB, Johnson IT, Read NW: The mech-anism of action of guar gum in improving glucose tol-erance in man. Clin Sci 66:329-36, 1984
54. Sommer H, Kasper H: The effect of dietary fiber on thepancreatic excretory function. Hepato-Gastroenterology27:477-83, 1980
55. Dunaif G, Schneeman BO: The effect of dietary fiber onhuman pancreatic enzyme activity in vitro. Am ) ClinNutr 34:1034-35, 1981
56. Kay RM, Grobin W, Track NS: Diets rich in natural fiberimprove carbohydrate tolerance in maturity-onset, non-insulin dependent diabetics. Diabetologia 20:18-21,1981
57. Morgan LM, Goulder TJ, Tsiolakis D, Marks V, AlbertiKGMM: The effect of unabsorbable carbohydrate on guthormones: modification of post-prandial GIP secretionby guar. Diabetologia 17:85-89, 1979
58. Jenkins DJA, Wolever TMS, Nineham R, Bacon S, SmithR, Hockaday TD: Dietary fiber and diabetic therapy: aprogressive effect with time. Adv Exp Med Biol 119:275-79, 1979
59. Shimoyama R, Uehara S, Itagaki Y, Izumiyama S, Hir-ayama A: Effects of guar intake on plasma somatostatin-like immunoreactivity in diabetic patients. HokkaidoIgaku Zasshi 57:727-32, 1982
60. Jenkins DJA, Wolever TMS, Nineham R, Sarson DL, BloomSR, Ahern J, Albert KGMM, Hockaday TDR: Improvedglucose tolerance four hours after taking guar with glu-cose. Diabetologia 19:21-24, 1980
61. Mann Jl: Lines to legumes: changing concepts of dia-betic diets. Diabetic Med 1:191-98, 1984
62. Pederson O, Hjollund E, Lindskov HO, Helms P, Soren-sen NS, Ditzel J: Increased insulin receptor binding tomonocytes from insulin-dependent diabetic patients aftera low-fat, high-starch, high-fiber diet. Diabetes Care5:284-91, 1982
63. Hjollund E, Pedersen O, Richelsen B, Beck-Nielsen H,Sorensen NS: Increased insulin binding to adipocytesand monocytes and increased insulin sensitivity of glu-cose transport and metabolism in adipocytes from non-insulin-dependent diabetics after a low-fat/high-starch/high-fiber diet. Metabolism 32:1067-75, 1983
64. Ward GM, Simpson RW, Simpson HCR, Naylor BA, MannJl, Turner RC: Insulin receptor binding increased by highcarbohydrate low fat diet in non-insulin-dependent di-abetics. Eur) Clin Invest 12:93-96, 1982
65. James WPT, Branch WJ, Southgate DA: Calcium bindingby dietary fibre. Lancet 1:638-39, 1978
65a.Christiansen JS, Bonnevie-Neilsen V, Svendsen PA, RubinP, R0nn B, NerupJ: Effect of guar gum on 24-hour insulinrequirements of insulin-dependent diabetic subjects asassessed by an artificial pancreas. Diabetes Care 3:659-62, 1980
66. Harmuth-Hoene AE: Der Einfluss von Guar auf die Stick-stoffbilanz, die Resorption von Mineralstoffen und Spu-
170 DIABETES CARE, VOL. 11, NO. 2, FEBRUARY 1988

A.I. VINIK AND D.J.A. JENKINS
renelementen und die verdauliche Energie bei 6 wei-blichen Versuchspersonen. Beitr Infusionther Klin ErnaehrForsch Prax 12:68-80, 1983
67. Tuomilehto J, Karttunen P, Vinni S, Kostiainen E, Uusi-tupa M: A double-blind evaluation of guar gum in pa-tients with dyslipidaemia. Hum Nutr Appl Nutr 37:109-16, 1983
68. Simpson HCR, Simpson RW, Lousley S, Carter RD, GeekieM, Hockaday TDR, Mann Jl: A high carbohydrate le-guminous fibre diet improves all aspects of diabetic con-trol. Lancet 1:1-5, 1981
69. Bosello O, Ostuzzi R, Armellini F, Micciolo R, ScuroLA: Glucose tolerance and blood lipids in bran-fed pa-tients with impaired glucose tolerance. Diabetes Care3:46-49, 1980
70. Gatti E, Catenazzo G, Camisasca E, Torri A, Denegri E,Sirtori CR: Effects of guar-enriched pasta in the treatmentof diabetes and hyperlipidemia. Ann Nutr Metab 28:1 —10, 1984
71. Munoz JM, Sandstead HH, Jacob RA, Logan GM Jr,Reck SJ, Klevay LM, Dintzis FR, Inglett GE, Shuey WC:Effects of some cereal brans and textured vegetableprotein on plasma lipids. Am j Clin Nutr 32:580-92,1979
72. Jenkins DJA, Wolever TM, Taylor RH, Reynolds LK,Nineham R, Hockaday TD: Diabetic glucose control,lipids and trace elements on long term guar. Br Med J280:1353-54, 1980
73. MahalkoJR, Sandstead HH, Johnson LK, Inman LF, MilneDB, Warner RC, Haung EA: Effect of consuming fiberfrom corn bran, soy hulls, or apple powder on glucosetolerance and plasma lipids in type II diabetes. Am I ClinNutr 39:25-34, 1984
74. Riccardi G, Rivellese A, Pacioni D, Genovese D, Mas-tranzo P, Mancini M: Separate influence of dietary car-bohydrate and fibre on the metabolic control in diabe-tes. Diabetologia 26:116-21, 1984
75. Anderson JW: Hypocholesterolemic effects of oat-branor bean intake for hypercholesterolemic men. Am \ ClinNutr 40:1146-55, 1984
76. Jenkins DJA: Leguminous seeds in the dietary manage-ment of hyperlipidemia. Am ) Clin Nutr 38:567-73,1983
77. Anderson JW, Ward K: Long-term effects of high-car-bohydrate, high-fiber diets on glucose and lipid metab-olism: a preliminary report on patients with diabetes.Diabetes Care 1:77-82, 1978
78. Rivellese A, Riccardi G, Giacco A, Postiglione A, Mas-tranzo P, Mattioli PL: Reduction of risk factors for ath-erosclerosis in diabetic patients treated with high fiberdiets. Prev Med 12:128-32, 1983
79. Jenkins DJA, Leeds AR, Gassull MA, Cochet B, AlbertiKGMM: Decrease in postprandial insulin and glucoseconcentrations for guar and pectin. Ann Intern Med86:20-23, 1977
80. Jenkins DJA, Goff DV, Leeds AR, Alberti KGMM, Wol-ever TMS, Gassull MA, Hockaday TDR: Unabsorbablecarbohydrates and diabetes: decreased post-prandial hy-perglycemia. Lancet 2:172-74, 1976
81. Goulder TJ, Alberti KGMM, Jenkins DA: Effect of addedfiber on the glucose and metabolic response to a mixedmeal in normal and diabetic subjects. Diabetes Care1:351-55, 1978
82. Hall SEH, Bolton TM, Hetenyi G Jr: The effect of branon glucose kinetics and plasma insulin in non-insulin-
dependent diabetes mellitus. Diabetes Care 3:520-25,1980
83. Cohen M, Leong VW, Salmon E, Martin FIR: The roleof guar and dietary fibre in the management of diabetesmellitus. Med J Aust 1:59-61, 1980
84. Williams DRR, James WPT, Evans IE: Dietary fibre sup-plementation of a "normal" breakfast administered todiabetics. Diabetologia 18:379-83, 1980
85. Jenkins DJA, Nineham R, Craddock C, Craig-McFeely P,Donaldson K, Leigh T, Snook J: Fibre and diabetes. Lan-cet 1:434-35, 1979
86. Miranda PM, Horwitz DL: High-fiber diets in the treat-ment of diabetes mellitus. Ann Intern Med 88:482-86,1978
87. Monnier LH, Blotman MJ, Colette C, Monnier MP, Mir-ouse J: Effects of dietary fibre supplementation in stableand labile insulin-independent diabetics. Diabetologia20:12-17, 1981
88. Fuessl H, Adrian TE, Bacarese-Hamilton AJ, Bloom SR:Effects of guar on plasma glucose and gut hormone re-sponse in type II diabetics. Br Diabetes Assoc SpringMeeting, Oxford, UK, 1985, p. 59
89. Jenkins DJA: Lente carbohydrate: a newer approach tothe dietary management of diabetes. Diabetes Care 5:634-41, 1982
90. Jenkins DJA, Wolever TMS, Taylor RH, Barker H, Fiel-den H, Baldwin JM, Bowling AC, Newman HC, JenkinsAL, Goff DV: Glycemic index of foods: a physiologicalbasis for carbohydrate exchange. Am) Clin Nutr 34:362-66, 1981
91. Anderson JW, Sieling B: High fiber diets for obesediabetic patients. Obesity Bariatric Med 9:109-17,1980
92. Nuttall FQ: Diet and the diabetic patient. Diabetes Care6:197-207, 1983
93. Hollenbeck CB, Coulston AM, Donner CC, WilliamsRA, Reaven GM: The effects of variations in percent ofnaturally occurring complex and simple carbohydrateson plasma glucose and insulin response in individualswith non-insulin-dependent diabetes mellitus. Diabetes34:151-55, 1985
94. Hollenbeck CB, Coulston AM, Reaven GM: To whatextent does increased dietary fiber improve glucose andlipid metabolism in patients with noninsulin-dependentdiabetes mellitus (NIDDM)? Am ) Clin Nutr 43:16-24,1986
95. Brunzell JD, Lerner RL, Hazzard WR, Porte D, BiermanEL: Improved glucose tolerance with high carbohydratefeeding in mild diabetes. N Engl I Med 284:521-24,1974
96. Gatti E, Catenazzo G, Camisasca E, Torri A, Denegri E,Sirtori CR: Effects of guar-enriched pasta in the treatmentof diabetes and hyperlipidemia. Ann Nutr Metab 28:1-10, 1984
97. Thompson LU, Ferrari F, Bosello O, Rao AV, Wong G:Effect of guar-enriched pasta on blood glucose controlin diabetics (Abstract). Diabetes 34:205A, 1985
98. Lipid Research Clinics Program: Lipid research clinicscoronary primary prevention trial results. I. Reductionin incidence of coronary heart disease. II. The relation-ship of reduction in incidence coronary heart disease tocholesterol lowering. JAMA 3:351-74, 1984
99. Kritchevsky D, Story J: Binding of bile salts in vitro bynonnutritive fiber. I Nutr 104:458-62, 1974
100. Story J, Kritchevsky D: Comparison of the binding of
DIABETES CARE, VOL. 11 , NO. 2, FEBRUARY 1988 171

DIETARY FIBER
various bile acids and salts in vitro by several types offiber. J Nutr 106:1292-94, 1976
101. Anderson JW: Hypocholesterolemic effects of oat-branor bean intake for hypercholesterolemic men. Am ) ClinNutr 40:1146-55, 1984
102. Jenkins DJA, Wolever TMS, Taylor RH, Barker H, Fiel-den H: Exceptionally low blood glucose response to driedbeans: comparison with other carbohydrate foods. BrMedy 281:578-80, 1980
103. Anderson JW: High-fibre diets for diabetic and hyper-triglyceridemic patients. Can Med Assoc j 123:975-79,1980
104. Story L, Anderson JW, Chen WJ, Karounos D, JeffersonB: Adherence to high carbohydrate, high fiber diets: long-term studies of non-obese diabetic men. / Am Diet Assoc85:1105-10, 1985
105. Wirth A, Middelhoff G, Braeuning C, Schlierf G: Treat-ment of familial hypercholesterolemia with a combina-tion of bezafibrate and guar. Atherosclerosis 45:291-97,1982
106. Najemnik C, Kritz H, Irsliger K, Laube H, Knick B, KlimmHD, Wahl P, Vollmar J, Brauning C: Guar and its met-abolic effects in type II diabetic subjects. Diabetes Care7:215-20, 1984
108. Uusitupa M, Tuomilehto J, Karttunen P, Wolf E: Long-term effects of guar gum on metabolic control, serumcholesterol and blood pressure levels in type 2 (non-insulin-dependent) diabetic patients with high bloodpressure. Ann Clin Res Suppl 43:126-31, 1984
109. Virtanen V, Maenpaa J, Pitkanen L: Problem cases inscreening for congenital hypothyroidism. Pediatr Res18:119, 1984
110. Farrell R, Owens D, Tyrrell D, Thompkins GH: Is guaruseful in type II diabetics? Br Diabetes Assoc SpringMeeting, Oxford, UK, 1985, p. 60
111. Bosello O, Cominacini L, Zocca I, Garbin U, Ferrari F,Davoli A: Effects of guar gum on plasma lipoproteinsand apolipoproteins C-ll and C-lll in patients affected byfamilial combined hyperlipoproteinemia. Am) Clin Nutr40:1165-74, 1984
112. Dalzell GW, MacNeil AJ, Hadden DR, Atkinson AB,Weaver JA, Kennedy AL, Holmes J: Effects of guar onpoorly controlled non-insulin dependent diabetes mel-litus. Br Diabetes Assoc Meeting, Belfast, UK, 1985, p.34
113. Jenkins DJA: Dietary fiber, diabetes and hyperlipidemia:progress and prospects. Lancet 2:1287-90, 1979
114. Jenkins DJA, Wolever TMS, Jenkins AL, Lee R, WongGS, Josse R: Glycemic response to wheat products: re-duced response to pasta but no effect of fiber. DiabetesCare 6:155-59, 1983
115. Heaton KW: Food intake regulation and fibre. In Med-ical Aspects of Dietary Fiber. Spiller GA, Kays RM, Eds.New York, Plenum, 1980, p. 223-38
116. Van Itallie TB: Dietary fiber and obesity. Am J Clin Nutr31:S43-52, 1978
117. AM R, Staub H, Leveille GA, Boyle PC: Dietary fiber andobesity: a review. In Dietary Fibre in Health and Disease.Vahouny GV, Kritchevsky D, Eds. New York, Plenum,1982, p. 139-49
118. Heaton KW: Food fibre as an obstacle to energy intake.Lancet 2:1418-21, 1973
119. Heaton KW: Fibre, satiety and insulin—a new approachto overnutrition and obesity. In Dietary Fibre: Current
Developments of Importance to Health. Heaton KW, Ed.London, Newman, 1978, p. 141-49
120. Haber GB, Heaton KW, Murphy D, Burroughs LF: De-pletion and disruption of dietary fibre: effects on satiety,plasma-glucose, and serum-insulin. Lancet 2:679-82,1977
121. Grimes DS, Gordon C: Satiety value of wholemeal andwhite bread. Lancet 2:106, 1978
122. Duncan KH, Bacon JA, Weinsier RL: The effects of highand low energy density diets on satiety, energy intakeand eating time of obese and nonobese subjects. Am /Clin Nutr 37:763-67, 1983
123. Krotkiewski M: Effect of guar gum on body weight, hun-ger ratings and metabolism in obese subjects. Br j Nutr52:97-105, 1984
124. Arsenio L, Cavalli Sforza LT, Magnati G, Strata A: Ri-cerca clinica sull' impiego di una farina deproteinizzatadi guar nel trattamento dell' obesita. Ada Bio-Med Ate-neo Parmense 52:149-57, 1981
125. Evans E, Miller DS: Bulking agents in the treatment ofobesity. Nutr Metab 18:199-203, 1975
126. Leeds AR, Judd PA: Dietary fiber and weight manage-ment. In Dietary Fiber. Basic and Clinical Aspects. Va-houny GV, Kritchevsky D, Eds. New York, Plenum, 1986,p. 335-42.
127. Bjorntorp P, Vahouny GV, Kritchevsky D (Eds.): Dietaryfiber and obesity. In Proc Satellite Symp to the SecondWashington Symposium on Dietary Fiber, Washington,DC, April 28, 1984. New York, Liss, 1985
128. Forster H: Treatment of obesity with low energy diet andfiber. In Dietary Fiber in Health and Disease. VahounyGV, Kirtchevsky, Eds. New York, Plenum, 1985
129. Gabbe SG, Cohen AW, Herman GO, Schwartz S: Effectof dietary fiber on the oral glucose tolerance test in preg-nancy. Am j Obstet Cynecol 143:514-17, 1982
130. Kyllastinen M, Lahikainen T: Long-term dietary supple-mentation with a fiber product (guar gum) in elderlydiabetics. Curr Ther Res Clin Exp 30:872-79, 1981
131. Kay RM: Dietary fiber. / Lipid Res 23:221-42, 1982132. Crapo PA, Reaven G, Olefsky J: Postprandial plasma
glucose and insulin responses to different complex car-bohydrates. Diabetes 26:1178-83, 1977
133. Crapo PA, Kolterman OG, Waldeck N, Reaven GM,Olefsky JM: Postprandial hormone responses to differenttypes of complex carbohydrates in individuals with im-paired glucose tolerance. Am ) Clin Nutr 33:1723-28,1980
134. Schauberger G, Brinck UC, GuldnerG, Spaethe R, Nik-las L, Otto H: Exchange of carbohydrates according totheir effect on blood glucose (Abstract). Diabetes 26(Suppl. 1):415, 1977
135. O'Dea K, Nestel PJ, Antonoff L: Physical factors influ-encing postprandial glucose and insulin responses tostarch. Am I Clin Nutr 33:760-65, 1980
136. Haber GB, Heaton KW, Murphy D, Burroughs LF: De-pletion and disruption of dietary fibre: effects on satiety,plasma-glucose, and serum-insulin. Lancet 2:679-82,1977
137. Jenkins DJA, Ghafari H, Wolever TMS, Taylor RH, Bar-ker HM, Fielden H, Jenkins AL, Bowling AC: Relation-ship between the rate of digestion of foods and post-prandial glycaemia. Diabetologia 22:450-55, 1982
138. Eno J: A new approach to diet for diabetes. / Can DietAssoc 40:118-22, 1979
172 DIABETES CARE, VOL. 11, NO. 2, FEBRUARY 1988

A.I. VINIK AND D.J.A. JENKINS
139. Collings P, Williams C, MacDonald I: Effect of cooking 143.on serum glucose and insulin responses to starch. BrMedy 282:1032, 1981
140. Anderson JW, Ferguson SK, Karounos D, O'Malley L, 144.Sieling B, Chen W-JL: Mineral and vitamin status onhigh-fiber diets: long-term studies of diabetic patients.Diabetes Care 3:38-40, 1980 145.
141. Mclvor ME, Cummings CC, Leo TA, Mendeloff Al: Flat-tening postprandial blood glucose responses with guargum: acute effects. Diabetes Care 8:274-78, 1985
142. Aro A, Uusitupa M, Voutilainen E, Korhonen T: Effects 146.of guar gum in male subjects with hypercholesterolemia.Am J Clin Nutr 39:911-16, 1984
Huupponen R, Seppala P, lisalo E: Effect of guar gum,a fibre preparation, on digoxin and penicillin absorptionin man. Eur) Pharm 26:279-81, 1984Huupponen R, Karhuvaara S, Seppala P: Effect of guargum on glipizide absorption in man. Eur J Clin Phar-macol 28:717-19, 1985McCulloch DK, Young RJ, Steel JM, Wilson EM, PrescottRJ, Duncan LJ: Effectof dietary compliance on metaboliccontrol in insulin-dependent diabetics. Hum Nutr ApplNutr 37A:287-92, 1983Cantrill JA, Wright C: Community pharmacists and thehealth education of diabetic patients. Pharm I 235:449,1985
DIABETES CARE, VOL. 1 1 , NO. 2, FEBRUARY 1988 173