Embed Size (px)
Citation preview

C211 COG Track ‐ AALL1331: Blinatumomab in First Relaspe of B‐Lineage ALL 1
1
Debra Schissel RN, CPON, CCRP Sue Zupanec MN, NPCOG Track at APHON 2016
AALL1331: Blinatumomab in First Relapse of Childhood
B-Lineage Lymphoblastic Leukemia
2
COG Disclosure
The information in this presentation is intended for educational purposes only and is solely for the use of the individual nurse learner. This information is not intended as the sole source of guidance in providing Children’s Oncology Group (COG) protocol-directed nursing care, and current COG protocols should always be consulted prior to making patient care decisions for any patient enrolled on a COG protocol. Learners should also be aware that COG protocols are research plans designed to investigate particular study questions, that recommendations for treatment and dosing are made within the context of specific research aims, and that these recommendations are intended only for use within a structured research setting. Although every attempt has been made to assure that the informational content contained herein is as accurate and complete as possible as of the date of presentation, no warranty or representation, express or implied, is made as to the accuracy, reliability, completeness, relevance, or timeliness of this content. This information may not be copied or redistributed in any form, or used for any purpose other than nursing education.
3
Disclosure
Debra Schissel and Sue Zupanec have no industry relationships to disclose
Off label use of blinatumomab will be discussed

C211 COG Track ‐ AALL1331: Blinatumomab in First Relaspe of B‐Lineage ALL 2
4
Definitions
Event Free Survival Survival free from unfavorable events (including induction failure, relapse, death from any cause, or SMN)
Overall Survival Survival regardless of disease status (includes all patients that are alive, even those who are relapsed)
Disease Free Survival Survival free from the disease under study (alive patients in remission)
Progression Free Survival Length of time during and after treatment that patient lives with the disease, but it does not get worse
5
Objectives
Review background for Relapsed B-ALL♦ Currently reported EFS♦ Best published therapy: UKALLR3 (backbone)
Discuss blinatumomab – BiTE♦ Mechanism of action♦ Toxicity profile ♦ Unique delivery and practical considerations♦ Outcomes/lessons learned from early phase trials
Review current COG phase III trial AALL1331
6
Relapsed ALL Risk Stratification
Time of Relapse
Early < 18 mos since initial diagnosis
Intermediate > 18 mos but < 36 mos since initial diagnosis
Late >36 mos since initial diagnosis
Site of Relapse
Isolated bone marrow
Isolated extramedullary
Combined bone marrow and extramedullary

C211 COG Track ‐ AALL1331: Blinatumomab in First Relaspe of B‐Lineage ALL 3
7
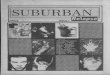
Survival in Relapsed ALL: Timing and Site
Data from Nguyen et al. (2008)
• COG patients with B- or T-ALL from 1988-2002• 1961/9585 (20.5%) experienced a relapse
12%
18%
44%
24%
12%
40%
60%
39%44%
68%
78%
59%
0%
20%
40%
60%
80%
Early Intermediate Late Overall
Isolated Marrow Combined Isolated CNS
8
Survival Rates: Relapsed ALLEarly Isolated Bone Marrow: 12%
Intermediate Combined BM and CNS: 40%
Late Isolated CNS: 78%
Wide Range of EFS for Relapsed ALL
Complex Risk Stratification
9
Survival Rates: Risk Factors
Evidence of refractory or resistant disease: Intervention!
At time of relapse •Site •Location
Disease response to re-induction
•Post re-induction response (BLK/Cycle1)•Measured by MRD
Disease persistence •MRD Pre-SCT
Post-SCT factors •Positive MRD•Lack of clinical aGVHD

C211 COG Track ‐ AALL1331: Blinatumomab in First Relaspe of B‐Lineage ALL 4
Risk Assessment: Relapsed B-ALL
Site Isolated bone marrow Unfavorable
Isolated extramedullary Favorable
Combined bone marrow & extramedullary
Unfavorable (maybe slightly more favorable compared to isolated bone marrow)
Timing of Relapse Early Unfavorable
Intermediate Unfavorable
Late Favorable
Post Re-InductionResponse
MRD negative Favorable
M2/M3 or MRD positive Unfavorable
Pre-SCT MRD MRD negative Favorable
MRD positive Unfavorable
Post-SCT MRD detectable Unfavorable
No aGVHD Unfavorable
11
MRD Predicts Survival in Relapsed ALL Disease response post initial Re-induction BLK♦ N = 60 BFM HR relapsed patients
MRD response remains a strong predictor of outcome!♦ 73% if MRD-♦ 19% if MRD+
Paganin, M. et al. (2008)
© 2
008
12
MRD Prior to SCT SCT remains standard of care for subsets of patients with
relapsed ALL♦ HR/IR patients♦ MRD positive post re-induction
Relapse post SCT is a significant cause of treatment failure BFM Relapsed Patients with SCT indication♦ MRD level prior to SCT predicts EFS
• MRD < 0.001 EFS 61%• MRD > 0.001 EFS 27%
Bader et al. 2009
Resistant Disease!

C211 COG Track ‐ AALL1331: Blinatumomab in First Relaspe of B‐Lineage ALL 5
13
MRD pre SCT and Predicted Survival
Bader et al. 2009
© 2
009
14
More Predictors of Survival: Post SCT
ASCT0431: Predictors of Poor EFS post-SCT ♦ Detection of MRD+ disease♦ No aGVHD
Pulsipher, Blood (ASH Abstract), 2012
GVHD Status EFS PredictionNone •19%
Grade II-IV •35%
MRD+ post-SCT •14-fold increased relapse risk
Need for new/novel interventions post-SCT

C211 COG Track ‐ AALL1331: Blinatumomab in First Relaspe of B‐Lineage ALL 6
16
Treatment Options for Relapsed B-ALL
17
Case Examples
Presentation: WBC 4 x 109/L/CNS negative Neutral cytogenetics /EOI M1 and MRD-Prior treatment: AALL0932 AR Arm CRelapse timing: 37 mos post diagnosis (late)Site: Isolated bone marrow diseaseRisk Classification at Relapse: LR
Jacob 7-yrs-old
Presentation: WBC 115 x 109/L CNS negative t(1:19)/EOI M1 and MRD-
Prior treatment: AALL1131 HR Arm BRelapse timing: 28 mos post diagnosis (early)Site: Isolated bone marrow diseaseRisk Classification at Relapse: HR
Georgie11-yrs-old
18
UKALLR3: Backbone for AALL1331 Randomization occurs during induction♦ Idarubicin vs. mitoxantrone♦ 216 participants randomized
Primary outcome goal♦ PFS
Parker, C. et al. (2010)
Randomization stopped early due to significant differences in PFS and OS between groups

C211 COG Track ‐ AALL1331: Blinatumomab in First Relaspe of B‐Lineage ALL 7
19Parker, C. et al. (2010)
UKALLR3: Results
© 2
010
Survival Mitox Arm IDA Arm3-yr PFS •64.6% •35.9%
3-yr OS •69% •45.2%
20
Challenges in Relapsed ALLOutcomes for patients remain unsatisfactory♦ Suboptimal remission rates (MRD response)♦ Poor OS rates
Treatment for relapsed ALL♦ Involves traditional cytotoxic chemotherapy ♦ SCT
• Unclear benefit of intensive chemotherapy versus SCT• Both strategies result in poor outcomes and undesired long term sequelae
Nguyen et al. 2008
New Agents Needed!!
https://visualsonline.cancer.gov/details.cfm?imageid=2191
21
Targeted TherapiesAALL1331
https://en.wikipedia.org/wiki/Blinatumomab#/media/File:BiTE_antibody_en.svg

C211 COG Track ‐ AALL1331: Blinatumomab in First Relaspe of B‐Lineage ALL 8
22
New Targeted Agents for Relapsed ALL
Potential Benefits of a Targeted New Agent♦ Improve EFS and OS without further intensification of
standard chemotherapy♦ Reduce detectable MRD prior to SCT to improve outcomes
Picking a promising agent♦ A targeted approach!!!♦ CD19
https://visualsonline.cancer.gov/details.cfm?imageid=2192
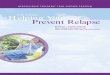
CD3
CD19
TCR
BlinatumomabMechanism of Action(BiTE = Bi-specific T-Cell Engager)
Does not require MHC Class I and/or peptide antigen
Acts independently of specificity of TCR
Allows T cells recognition of TAA
Blina-tumomab
Tumor Cell
Any T Cell
Slide courtesy of Dr. Lia Gore
24
Blinatumomab: BiTE
CD19 is an excellent target!!!♦ CD19 not expressed on pluripotent stem cells
Expressed on B Lymphocytes, from early precursor cells through mature B cells♦ Expressed on the majority of B precursor ALL cells
Aimee Ermel, 2012

C211 COG Track ‐ AALL1331: Blinatumomab in First Relaspe of B‐Lineage ALL 9
25Over 16 years to get to current Phase III study!
History of BiTE
• Three phase I trials (NHL, CLL)• Phase II MRD+ ALL trial (First pivotal study in EU – 2010)• Compassionate use in Pediatric ALL• Phase III trial as COG AALL1331
Clinical Studies
• Started as short-term IV infusion• Changed to continuous IV infusionAdministration
• 1990’s preclinical development• 2001 clinical development• 2003 switched to continuous IV infusion• 2008 clinical concept published • 2010 start of 1st pivotal study
Key Milestones
26
Relapsed/Refractory B-ALL: Adult Trials
Author Adult Patients Phase Outcomes
Topp(2014)
• n = 36•Ages 18-77 yrs •Refractory or relapsed B-ALL
• II • CR/CRh♦25/36 (69%)
•Responders♦22/25 (88%) ♦MRD negative
Topp(2015)
• n = 189•Refractory or relapsed B All
•II •Evaluated post 2nd cycle•CR/CRh♦81/189 (43%) ♦MRD evaluable responders 73/81♦60/73 (82%) MRD negative
Topp et al. (2014), Topp et al. (2015)
27
Early Peds Experience with BiTE
Author Number of Patients
Phase Reported Outcomes
Handgretinger (2011)
• 3 All post HSCT • 3 patient cohort• Compassionate
• All 3 achieved MRD CR at day 28
Shlegel(2014)
• 9 - All patientsprior HSCT
• Cohort study• Compassionate
• 5/9 achieved MRD CR at day 28
VonStackelberg(2016)
• N=49 at phase I
• n=44 treated at phase II dose
• Phase I/II• Primary
endpoint CR within 2 cycles
• 70 evaluable – (27/70) achieved CR
• Those in CR (14/27) 53% MRD negative
Ability to achieve MRD negative Remission

C211 COG Track ‐ AALL1331: Blinatumomab in First Relaspe of B‐Lineage ALL 10
28
FDA Approval
Sept. 1, 2016
FDA approval of Blinatumomab for use in Pediatric Patients with Philadelphia Chromosome-Negative Relapsed or Refractory B-cell Precursor Acute Lymphoblastic Leukemia♦ Accelerated approval
29
Lessons Learned From Early BiTE Trials
Evidence of clinical activity
Very short half-life: 2 hours♦ Required continuous exposure
for clinical benefit
Results in T-cell Activation:♦ T-cell proliferation♦ Lysis of tumor cells♦ Cytokine release
Development of AALL1331 ♦ Blinatumomab with UKALLR3 backbone
Aimee Ermel, 2012
Pluripotent Stem Cell
Lymphoid Progenitor
Myeloid Progenitor
B-lymphocyte
T-lymphocyte
30
COG AALL1331Protocol Details

C211 COG Track ‐ AALL1331: Blinatumomab in First Relaspe of B‐Lineage ALL 11
31
AALL1331: Primary Aim
Will addition of blinatumomab to UKALLR3 backbone improve DFS for pediatric patients in first relapse of B-ALL?
32
AALL1331 Schema
Induction – same for all patients♦ Risk classification occurs at end of BLK 1
• LR, IR/HR or treatment failure♦ Treatment failure at end of BLK 1 or 2
• Off protocol• May have BLINA salvage therapy x 2 cycle• Relapse at end of BLK 2 or pre SCT → OFF THERAPY
Therapy arms – IR/HR
ARM A No BLINA SCT
ARM B BLINA X 2 cycles SCT
33
AALL1331 Schema
Induction – same for all patients♦ Risk classification occurs at end of BLK 1
• LR, IR/HR or treatment failure♦ Treatment failure at end of BLK 1 or 2
• Off protocol• May have BLINA salvage therapy x 2 cycles• Relapse at end of BLK 2 or pre SCT → OFF THERAPY
Therapy arms - LR
ARM C No BLINA, BLK 2 & 3, Continuation 1 &2 Maintenance
ARM D BLINA, Continuation1, BLINA, Continuation 2 Maintenance

C211 COG Track ‐ AALL1331: Blinatumomab in First Relaspe of B‐Lineage ALL 12
34
AALL1331 Schema – Blinatumomab-S
Salvage Arm♦ For patients who
• Are classified as treatment failure after BLK 1 or 2 treatment• Have NOT previously received BLINA on study• Do not have CNS disease
♦ Non-randomly assigned♦ Remain on study if CR obtained♦ Different dosing than BLK cycles (dose escalation)
BLINA-S BLINA 1, +/- BLINA 2 SCT
35
Risk Classification AALL1331
Low Risk •Late -(> 36 mos) marrow, end-BLK 1, MRD <0.1%-(> 18 mos) IEM, end-BLK 1, MRD <0.1%
Intermediate Risk •Late -(> 36 mos) marrow, end-BLK 1, MRD >0.1%-(> 18 mos) IEM, end-BLK 1, MRD >0.1%
High Risk •Early -(< 36 mos) marrow-(< 18 mos) IEM
Treatment Failure(at end of BLK 1)
•Failure to achieve-M2 or better marrow-CNS1
36
Hematopoietic Stem Cell Transplant
Decisions around transplant at discretion of transplant center♦ Donor selection♦ Transplant conditioning
Rapid taper of immunosuppression for patients with HR predictors of relapse post SCT♦ Early MRD detection post SCT♦ No aGVHD

C211 COG Track ‐ AALL1331: Blinatumomab in First Relaspe of B‐Lineage ALL 13
37
AALL1331: Exploratory Aims
To estimate for TF for patients not previously receiving blinatumomab, the CR and rate of MRD <0.01% prior to SCT, and the proportion able to proceed to SCT in CR after treatment with blinatumomab
To assess the feasibility and safety of rapid taper of immune suppression for the subset of SCT patients with MRD ≥0.01% pre-and/or post-SCT with no aGVHD
38
AALL1331: Eligibility
Inclusion •>1 and < 31 yrs at time of relapse•First relapse of B-ALL +/- extramedullary disease
Exclusion •Ph+ ALL, T-ALL or TLL•Mature B-ALL or B-LL•Preexisting CNS pathology •Uncontrolled seizure disorder•Known concomitant genetic syndrome (e.g. DS)
See protocol for more specific inclusion and exclusion criteria
39
Block 1 Timing
Complete BLK 1
Post-BLK 1 Evaluation♦ Risk assignment based on end-BLK 1 criteria
• End-BLK 1 cannot be done prior to Day 29 (+/- 1 day)
♦ Post-BLK1 treatment begins after end-BLK 1 • Patients should have full or partial recovery• Requires callback and receipt of treatment assignment• Must begin treatment according to time frames listed in the protocol

C211 COG Track ‐ AALL1331: Blinatumomab in First Relaspe of B‐Lineage ALL 14
40
Case Study - Georgie
Due for day 29 end-Induction evaluation♦ ANC 150/μL and platelets 31,000/μL
Can this evaluation be delayed?
The evaluation may be delayed no later than Day 36 (+/- 1 day) •If ANC < 500/μL and platelets < 50,000/μL on Day 29
41
Case Studies: Risk Allocation
Jacob Georgie
Relapse Late Isolated BM Early Isolated BM
Post BLK 1 Response
M1 (<5% blasts)MRD 0.02% (<0.1%) = MRD negative
M2 (17% blasts)MRD positive
Eligible Arm LR randomization HR/IR randomization
SCT No Yes
Randomized ARM D ARM B
Blinatumomab
42
When must the second block start?
HR/IR must begin within 14 days after risk assignment for patient to continue on protocol
Jacob Georgie
Protocol Arm LR Arm D HR/IR Arm B
2nd Course •LR pts- proceed to BLK 2• Chemo must start within 5
days of callback
•Blinatumomab
Count RecoveryRequired?
•No•LR arm proceeds to BLK 2 for Day 1 VCR and DEX
•Recommend await count recovery for Day 8 IV MTX
•Recommended but NOT required to have
- ANC ≥ 500/μL- Platelets ≥ 50,000/μL

C211 COG Track ‐ AALL1331: Blinatumomab in First Relaspe of B‐Lineage ALL 15
43
Blinatumomab: ♦ Continuous IV infusion over 28 days (Days 1-28)
♦ IV bag changes every 96 hours
Premedication: DEX♦ Day 1: 6-12 hours prior to initiation of infusion♦ Day 1: 30 minutes prior to infusion
Intrathecal therapyDay 8: IT MTX CNS1 and 2*, ITT CNS3Day 15: IT MTX CNS2*, ITT CNS3Day 22: IT MTX CNS2*, ITT CNS3, *CNS2 weekly ITs until 2 clear CSF samples
Blinatumomab Course
Blinatumomab infusion should not be interrupted for LPs!
44
Case Study: Georgie – Adverse Event
20 hours into infusion Georgie spikes a fever (39.7⁰C )♦ She feels achy, has chills and is fatigued♦ O2 sats < 90 while she is sleeping- requires O2 support ♦ SOB with ambulation ♦ Crackles in right lower lobe with auscultation
What are concerns in caring for Georgie?♦ Hypoxia♦ Fever/Sepsis♦ Pulmonary edema♦ Capillary leak syndrome♦ Cytokine release syndrome
Aimee Ermel, 2012
45
Cytokine Release Syndrome
Most common toxicity associated with BiTE
Constellation of inflammatory symptoms♦ Results from cytokine elevations
♦ Associated with T-cell proliferation
CRS ranges from mild to severe to life threatening♦ Mild: flu-like symptoms, fever, myalgia
♦ Severe: vascular leak, hypotension, pulmonary edema, coagulopathy
♦ Life threatening: can lead to multi-system organ failure
Cytokine elevations can be measured ♦ Degree of elevation does not always correlate with clinical severity
Barrett, D. et al. (2014)
Image from Blausen.com staff. "Blausen gallery 2014". Wikiversity Journal of Medicine. DOI:10.15347/wjm/2014.010. ISSN 20018762. -

C211 COG Track ‐ AALL1331: Blinatumomab in First Relaspe of B‐Lineage ALL 16
46
CRS: How Common?
Pediatric reported CRS based on high tumor burden♦ Blintatumomab as single agent at time of relapse
Gore et al. (2014, ASH)♦ n = 39 pediatric patients♦ CRS 8% (3/39) of patients
• Two with Grade 3 events
Topp et al. (2015, Lancet Oncology)♦ n =189 adult patients with relapsed or refractory B-ALL♦ Received Dex in prephase to reduce tumor burden♦ 2% of patients had Grade 3 CRS
47
Klinger et al. (2012)© 2012
Cytokine Concentrations
48
Management of CRS
Reported with first cycle of BiTE♦ Typically within first 12-72 hours
Most Significantly elevated cytokines:♦ IL10, IL6, IFNy
Is it possible to target the cytokines themselves?
Anti IL6 (tocilizumab) – resolution of CRS ♦ Reversal and clinical improvement seen within 24 hours♦ FDA approved for JIA in children as young as 2 years
Maude, 2014; Barrett, 2014
https://upload.wikimedia.org/wikipedia/commons/3/38/IL10_Crystal_Structure.rsh.png

C211 COG Track ‐ AALL1331: Blinatumomab in First Relaspe of B‐Lineage ALL 17
49
New CRS Toxicity Grading System
Porter, D. ASH, December 14, 2014 © 2014
Grade Clinical Picture Management
1 Mild: Flu-like symptoms, fever, myalgia •Antipyretics•Supportive care
2 Moderate: beginning S/S of organ dysfunction (e.g. grade 2 creatinine, grade 3 LFTs)
•Hospitalization•IV therapies
3 Severe: ↑ing S/S of organ dysfunction (e.g. grade 3 creatinine, grade 4 LFTs),hypotension, coagulopathy, hypoxia
•O2/IVFs/pressors•FFP/Cryo•Anti IL-6-Tocilizumab
4 Life threatening: Significant hypotension/ Hypoxia
•Multiple pressors•Ventilator support •Anti IL-6-Tocilizumab
50
Tocilizumab: When and How?
Grade 1 and 2♦ Supportive interventions
Grade 3 and 4♦ Patient likely in PICU♦ Consideration for administration of Tocilizumab
• Dosing per institutional guidelines
https://visualsonline.cancer.gov/details.cfm?imageid=2502
51
Case Study: Georgie
To PICU for grade 3 CRS♦ Receives Tocilizumab
What happened?♦ By hour 72, CRS has resolved to grade 1
What to do about blinatumomab?♦ Can resume at a lower dose for the remainder of this cycle
♦ Follow protocol dose modifications for next cycle
• Georgie should be in hospital for dose escalation

C211 COG Track ‐ AALL1331: Blinatumomab in First Relaspe of B‐Lineage ALL 18
52
Jacob’s nursing assessment at hour 24♦ Easily wakes, seems confused ♦ Struggles to perform finger-to-nose assessment ♦ He experiences a brief generalized seizure
(Grade 2 toxicity ) What to do?♦ Stop infusion♦ Administer DEX per protocol/Seizure medications♦ Investigate other causes
Can blinatumomab resume?♦ Refer to dose modification table (may
restart of resolves with 14 days)
Can dose be escalated?♦ Not allowed following neurotoxic event
Case Study: Jacob
53
Unique Neurotoxicity with BiTE
All CNS reported toxicities with BiTE have been reversible!
Temporary CNS dysfunction may include♦ Encephalopathy♦ Trembling/Apraxia♦ Reversible seizures♦ Somnolence/Agitation♦ Dizziness/Confusion/Disorientation ♦ Speech/Coordination disorders/Loss of movement
54
Daily Neurotoxicity Assessments
Adults♦ Daily handwriting sample predicts future nervous system toxicity
before clinical toxicity develops♦ Earlier introduction of DEX
Children♦ Daily finger-nose-finger or writing sample test is recommended
as age-appropriate for patient
If change noted in finger-nose-finger or handwriting test, it is recommended to start DEX

C211 COG Track ‐ AALL1331: Blinatumomab in First Relaspe of B‐Lineage ALL 19
55
Adverse Events: Criteria to Resume
If eligible to resume♦ The 28-days of infusion must be completed
♦ Subsequent cycles• After 7days of dose reduction – if no further AE may dose escalate
♦ No dose escalations following > Grade 2 neurotoxicity
Permanent discontinuation/Off protocol♦ AEs requiring interruption of infusion that do not resolve to
< Grade 1 toxicity within 14 days
♦ Second AE requiring interruption of infusion
56
Practical Considerations
Double lumen central venous access♦ Dedicated line for blinatumomab
Hospitalization: close observation♦ Limited nursing assignment for first 72 hours
• Highest risk period for CRS
♦ Vital signs q 4hours♦ Daily Neuro checks: Finger-nose-finger, writing sample, sticker charts
Hospitalization is STRONGLY recommended for:- First 3 days of blinatumomab cycle AND- First 2 days s of subsequent blinatumomab cycles
57
Blinatumomab/Equipment for Administration Infusion♦ Requires 0.2 micometer filter, and DEHP-free tubing♦ Rate of infusion: 5 mL/hr♦ BiTE stable 96 hours at room temperature
• IV bag change q 96 hours• IV bags can be made up to 8 days in advance
Infusion pumps must meet study requirements♦ CADD VIP and VIP Solis, Prizm or Legacy ♦ Must have visual/auditory alarms and be lockable♦ No cassettes (they have DEHP)♦ Spare pumps available (2 per patient) and 9-volt batteries as back-up
Home care pumps have lower infusion rate calibrations. Consider using it while patient in hospital to provide hands-on training.

C211 COG Track ‐ AALL1331: Blinatumomab in First Relaspe of B‐Lineage ALL 20
59
Other Tips!
Bags •Have child in clinic at least 1-hr prior to needed bag change
•Expect overfill•Have prepared back-ups
Pumps/Battery •Store where readily available if needed after-hours
Tubing/Caps •Do changes with 2 nurses to ↓ interruption time
CVL Flushing •Avoid flushing dedicated BiTEline to ↓ chance of bolus dose (less concerning on AALL1331 compared to early trials)
•Unavoidable in clearing occlusions/ or at end of 28-day infusion
Interruptions •Interruption > 1 hr must be recorded•Interruption > 4 hours requires readmission to hospital and use of new bag to resume infusion
60
Jacob Case Study: Infusion Issues
Day 21 of blinatumomab♦ Jacob has a episode of bacteremia which requires antibiotic therapy
IV over an hour 4 times a day
How do you work this therapy around the continuous blinatumomab infusion?
Record all infusion interruptions Must be as minimal as possible
Re-start infusion as soon as possible

C211 COG Track ‐ AALL1331: Blinatumomab in First Relaspe of B‐Lineage ALL 21
61
Georgie Case Study: Pump/Infusion Issues
What to do????
Must follow institutional guidelines for unblocking CVL♦ Blinatumomab will likely be interrupted for >4 hours to unblock CVL♦ Patient to be admitted to hospital to resume infusion
• New bag of blinatumomab should be hung when infusion resumes
Georgie is at home and the mother calls to report the pump has malfunctioned and is no longer infusing the blinatumomab. They live 60 minutes from the hospital. When they arrive, the nurse is unable to flush or obtain blood return from the blinatumomab lumen.
62
Research Studies
Immunogenicity/PK peripheral samples are required:♦ Pre Cycle 1: Immuno Hour 0 prior to start of blinatumomab♦ Day 2 Cycle 1: PK ♦ Day 14 Cycle 1: PK♦ Post Cycle 2: Immuno♦ Pre-maintenance: Immuno prior to start of Cycle 1 maintenance
In cases where blinatumomab treatment will not continue to Cycle 2, collect sample at the end of Cycle 1 • See section 13.0 for optional research studies
63
Honoring our Patients
“Far and away the best prize that life offers is the chance to work hard at work worth doing”
- Theodore Roosevelt

C211 COG Track ‐ AALL1331: Blinatumomab in First Relaspe of B‐Lineage ALL 22
64
AALL1331: Discussion
We want to hear from you!
65
Abbreviations
TERM ABBREVIATIONDi(2-ethylhexyl) phthalate DEHP
Absolute neutrophil count ANCAcute graft versus host disease aGVHDAcute lymphoblastic leukemia ALLAdverse events AEAmerican Society of Hematology ASHAverage risk ARBerlin Frankfurt Munster BFMBi-specific T-cell Engager BITE®Blinatumomab BLINABlock BLKBone marrow BM
66
AbbreviationsTERM ABBREVIATION
Centigrade CCentral nervous system CNSCentral venous line CVLCerebrospinal fluid CSFChemotherapy ChemoChildren's Oncology Group COGChronic lymphocytic leukemia CLLClinical Remission WITHOUT Complete Hematologic Recovery CRhCryoprecipitate CryoCytokine Release Syndrome CRSDexamethasone DEX

C211 COG Track ‐ AALL1331: Blinatumomab in First Relaspe of B‐Lineage ALL 23
67
AbbreviationsTERM ABBREVIATION
Di(2-ethylhexyl) phthalate DEHPDisease free survival DFSDown syndrome DSEvent free survival EFSEvery qExample e.g.Fresh frozen plasma FFPGraft versus host disease GVHDHigh risk HRInterleukin ILIntermediate risk IRIntrathecal Triple ITT
68
Abbreviations
TERM ABBREVIATIONIntravenous IVIsolated extramedullary disease IEMLiver function tests LFTEvent free survival EFSEvery qExample e.g.Fresh frozen plasma FFPGraft versus host disease GVHDHigh risk HRInterleukin ILIntermediate risk IRIntrathecal Triple ITT
69
Abbreviations
TERM ABBREVIATIONIntravenous IVIsolated extramedullary disease IEMLiver function tests LFTLow risk LRLumbar puncture LPMajor Histocompatability Complex MHcMatched related donor MRDMethotrexate MTXMilliliter(s) mL(s) or ml(s)Mitoxantrone MITOXMonths mosNon-Hodgkin lymphoma NHL

C211 COG Track ‐ AALL1331: Blinatumomab in First Relaspe of B‐Lineage ALL 24
70
Abbreviations
TERM ABBREVIATIONOverall survival OSOxygen O2Pediatric intensive care unit PICUPharmacokinetics PKProgression free survival PFSSaturation satsSecond malignant neoplasm SMNShortness of breath SOBSigns and symptoms S/SStem cell transplant SCTT-cell receptor TCR
71
Abbreviations
TERM ABBREVIATIONTranslocation tTreatment failure TFTumor-associated surface antigen TAAVersus vs.Vincristine VCRWhite blood count WBC
72
References
Bader, P. Kreyenberg, H., Henze, GH, et al. Prognostic value of minimal residual disease quantification before allogeneic stem-cell transplantation in relapsed childhood acute lymphoblastic leukemia: the ALL-REZ BFM Study Group, Journal of Clinical Oncology, (2009), 27:377-384.
Gore, L., Locatelli, F., Zugmaier, G. Initial results from a phase 2 study of blinatumomab in pediatric patients with relapsed/refractory B-cell precursor acute lymphoblastic leukemia, Blood, (2014), 124, 3703.
Handgretinger, R., Zugmaier, G., Henze, G., et al. Complete remission after blinatumomab-induced donor T-cell activation in three pediatric patients with post=transplant relapsed acute lymphoblastic leukemia, Leukemia (2011), 25, 181-184.

C211 COG Track ‐ AALL1331: Blinatumomab in First Relaspe of B‐Lineage ALL 25
73
References
Klinger, M., Brandl, C., Zugmaier, G. et al. Immunopharmacologic response of patients with B-lineage acute lymphoblastic leukemia to continuous infusion of T-cell engaging CD19/CD3 specific BiTE antibody blinatumomab, Blood (2012), 119, 6226-6233.
Nagorsen, D., Kufer, P., Baeurle, PA, Bargou, R., Blinatumomab: a historical perspective, Pharmacology Therapeutics, (2012), 136(3), 334-342.
Nguyen, K., Devidas, M., Cheng, SC et al. Factors influencing survival after relapse from acute lymphoblastic leukemia: a Children’s Oncology Group study, Leukemia (2008), 22, 2142-2150.
74
References
Paganin, M., Zecca, M., Fabbri, G. et al. Minimal residual disease is an important predictive factor of outcome in children with relapsed high risk acute lymphoblastic leukemia, Leukemia (2008), 22, 193-200.
Parker, C., Waters, R., Leighton, C. et al. Effect of Mitoxantrone on outcome of children with first relapse of acute lymphoblastic leukemia (ALLR3): an open-label randomized trial, Lancet (2009), 376, 2009-2017.
Pulishpher, MA, Langholz, B, Wall, DA, et al. The relationship of acute GVHD and pre-and post transplant flow-MRD to the incidence and timing of relapse in children undergoing allogeneic transplantation for high risk ALL: defining a target population and window for immunologic intervention to prevent relapse (2012) ASH annual meeting abstracts, 120, 470.
75
References
Schegel, P., Lang, P., Zugmaier, G., et al. Pediatric post transplant relapsed/refractory B-precursor acute lymphoblastic leukemia shows durable response by therapy with T-cell engaging bispecific antibody blinatumomab, Haematologica (2014), 99(7), 1212-1219.
Teachy, DT, Rheingold, SR, Maude, SL, et al. Cytokine release syndrome after blinatumomab treatment related to abnormal macrophage activation and ameliorated with cytokine-directed therapy, Blood (2013), 121: 5154-5157.

C211 COG Track ‐ AALL1331: Blinatumomab in First Relaspe of B‐Lineage ALL 26
76
References
Topp, MS, Gokbuget, ., Zugmaier, G., et al. Phase II trial of the anit-CD19 bispecific T cell-engager blinatumomab shows hematologic and molecular remission in patients with relapsed or refractory B-precursor acute lymphoblastic leukemia, Journal of Clinical Oncology, (2014), 32, 4134-4140.
Topp, MS, Gokbuget, N., Stein, AS, et al. Safety and activity of blinatumomab for adult patients with relapsed or refractory B-precursor acute lymphoblastic leukemia: a multi-center, single arm, phase 2 study, Lancet (2015), April 16 (4).










![Relapse of drug addictors; A review€¦ · 2.Relapse rate: Relapse is very common after treatment for drug addiction [3], it was stated that 25-50% of substance abusers will relapse](https://img.pdfslide.us/doc/110x75/5f2c786cf88b454211793241/relapse-of-drug-addictors-a-review-2relapse-rate-relapse-is-very-common-after.jpg)