Embed Size (px)
Citation preview

6/16/2016
1
1
Heart Failure Review Course
Part 4
Connie M. LewisMSN, ACNP-C, NP-C, CCRN, CHFN, FHFSA
Vanderbilt University Medical Center
June 2016
Objectives
♥ Discuss heart failure disease management.
♥ Describe transition of care
♥ Review professionalism
Case Study 1 Myocarditis, Spironolactone,
Research Study-consent, Obesity
36 year old Caucasian firefighter from 220 miles, 2 states
away from main campus referred for transplant evaluation
Myocarditis, diagnosed with nonischemic
cardiomyopathy
PMH: hyperlipidemia, hypertension, obesity (BMI 38)
ECHO: LVEF: 20-25%. LVEDD: 6.3 cm. Mild MR and TR
Cardiopulmonary exercise test: SVO2: 24.3 ml/kg/min.
RQ: 1.02 ml/kg/min
Medications
VanderbiltHeart.com
Carvedilol 6.25 mg bid
Furosemide 40 mg bid
6/16/2016
2
Obesity
Prevalence of overweight (BMI 25-29.9 kg/m2) and
obesity (BMI >30 kg/m2) is increasing
Elevated BMI alone is an independent risk factor for
development of HF
Obesity paradox - Higher BMI associated with better
outcomes in HF
Lavie CJ. JACC. 2013;1(2):93-102
Case Study 1
Myocarditis, Spironolactone, Research Study-consent, Obesity
Review of Symptoms
Fatigue
Short of breath with walking < one block on level ground
Cough
No chest pain, palpitations, syncope, near syncope,
PND, or orthopnea
Physical Exam
104/70, HR 56, BMI 38
JVD 10 cm, + HJR, 2+ LE edema
VanderbiltHeart.com
Case Study 1
Myocarditis, Spironolactone, Research Study-consent, Obesity
• ACCF/AHA stage C, NYHA class III
Hemodynamic Profile Assessment?
VanderbiltHeart.com
ACCF/AHA stage?
NYHA class?

6/16/2016
3
Case Study 1
Plan
Enroll in HF Disease Management Program
VanderbiltHeart.com
HF Disease Management Programs
(HFDMP) HFDMP provide specialty and individualized care (eg, extensive education,
symptom management, financial and social assistance, dietary referrals and consultation, laboratory and other diagnostic testing, pharmacology management)
Recommended components of a HFDMP:– Comprehensive education and counseling individualized to patient
needs– Promotion of self-care and engagement, including self-adjustment of
diuretic therapy in appropriate patients (or with family member/caregiver assistance)
– Emphasis on behavioral strategies to increase adherence– Vigilant follow-up after hospital discharge or prolonged periods of
instability – Coordination of care between the primary care physician and HF care
specialists and other agencies (eg, home health, cardiac rehabilitation) Patients recently hospitalized for HF and those at high risk for HF
decompensation should be considered for a referral to a HFDMP.
HF Nursing Certification: Core Curriculum Review 2nd Edition
Heart Failure Disease Management
Effective collaboration that prevents lapses in care and services for patients when transitioning from hospital to home include:
– Familiarity with one another’s practice and backgrounds
– Clear delineation of roles, responsibilities, and expectations related to individual cases
– Forums for ongoing communication and follow-up
– Recognizing that responsibility for certain aspects of the discharge planning process may
be shared but that one individual is in charge

6/16/2016
4
Patients May Be Discharged From the HFDMP
Program If: Patient or their family/caregiver demonstrate independence in
following prescribed treatment plan
Adequate or improved adherence to treatment guidelines
Improved functional capacity or cardiac function
Symptom stability
*Patients experiencing increased episodes of exacerbation or
demonstrate instability after discharge should be referred again to
the service
Pharmacologic Treatment for Stage C HFrEFHFrEF Stage C
NYHA Class I – IV
Treatment:
For NYHA class II-IV patients.
Provided estimated creatinine
>30 mL/min and K+ <5.0 mEq/dL
For persistently symptomatic
African Americans,
NYHA class III-IV
Class I, LOE A
ACEI or ARB AND
Beta Blocker
Class I, LOE C
Loop Diuretics
Class I, LOE A
Hydral-Nitrates
Class I, LOE A
Aldosterone
Antagonist
AddAdd Add
For all volume overload,
NYHA class II-IV patients
ACCF/AHA Guidelines for the Management of Heart Failure.
Circulation.2013
Case Study 1
VanderbiltHeart.com
Creatinine should be 2.5 mg/dL or less in men or 2.0 mg/dL orless in women (or estimated glomerular filtration rate >30 mL/min/1.73 m2), and potassium should be less than 5.0 mEq/L. Careful monitoring of potassium, renal
function, and diuretic dosing should be performed at initiation and closely followed thereafter to minimize risk of hyperkalemia and renal insufficiency
ACCF/AHA Guidelines for the Management of Heart Failure.
Circulation.2013

6/16/2016
5
Case Study 1
Already on carvedilol and furosemide
What would medication would you add next?
A. ACE-I/ARB (RAAS)
B. Aldosterone antagonist
C. Statin
D. Digoxin
Lisinopril 2.5 mg daily
Spironolactone 25 mg daily
VanderbiltHeart.com
A. ACE-I/ARB first
Medication Management
Strategies
Use once-daily dosing whenever possible
Tailor medications to patients’ daily schedules
Consider providing pre-prepared pill dispensers
Pill bottles should be labeled in large print with drug name and
dosing regimen
Provide updated medication list and written instructions for
medication changes at every visit
Ask about over-the-counter medications
Check with the patient about how they are tolerating their
medications; do not assume they are taking them as prescribed
Case Study 1
Medication were maximized
♥ Carvedilol 25 mg bid
♥ Lisinopril 20 mg daily
♥ Spironolactone 25 mg
♥ Repeat ECHO after 3 months of GDMT: LVEF 30%
♥ ACCF/AHA stage C, NYHA class II
♥ EKG: QRS 120 ms
VanderbiltHeart.com
Next Steps????

6/16/2016
6
Case Study 1
Plan
♥ Refer for ICD
♥ Enroll in research study
VanderbiltHeart.com
ICD Device Therapy for Stage C HFrEF
Recommendations COR LOE
ICD therapy is indicated in patients who are survivors of cardiac arrest due to VF or
hemodynamically unstable sustained VT after evaluation to define the cause of the
event and to exclude any completely reversible causes.
I A
ICD therapy is indicated in patients with structural heart disease and spontaneous
sustained VT, whether hemodynamically stable or unstable. (Level of Evidence: B) I B
ICD therapy is indicated in patients with syncope of undetermined origin with
clinically relevant, hemodynamically significant sustained VT or VF induced at
electrophysiological study.
I B
ICD therapy is indicated in patients with LVEF less than or equal to 35% due to prior
MI who are at least 40 days post-MI and are in NYHA functional Class II or III. I A
ICD therapy is indicated in patients with nonischemic DCM who have an LVEF less
than or equal to 35% and who are in NYHA functional Class II or III. I
B
ICD therapy is indicated in patients with LV dysfunction due to prior MI who are at
least 40 days post-MI, have an LVEF less than or equal to 30%, and are in NYHA
functional Class I. I A
ICD therapy is indicated in patients with nonsustained VT due to prior MI, LVEF less
than or equal to 40%, and inducible VF or sustained VT at electrophysiological
study. I B
ACCF/AHA Guidelines for the Management of Heart Failure.
Circulation.2013
CRT Device Therapy for Stage C HFrEF
Recommendations COR LOE
CRT is indicated for patients who have LVEF ≤35%, sinus rhythm, LBBB with a
QRS ≥150 msI
A (NYHA class
III/IV)
B (NYHA class
II)
CRT can be useful for patients who have LVEF ≤35%, sinus rhythm, a non-LBBB
pattern with a QRS ≥150 ms, and NYHA class III/ambulatory class IV symptoms on
GDMT.
IIa A
CRT can be useful for patients who have LVEF ≤35%, sinus rhythm, LBBB with a
QRS 120 to 149 ms, and NYHA class II, III or ambulatory IV symptoms on GDMT
IIaB
CRT can be useful in patients with AF and LVEF ≤35% on GDMT if a) the patient
requires ventricular pacing or otherwise meets CRT criteria and b) AV nodal ablation
or rate control allows near 100% ventricular pacing with CRT
IIa B
ACCF/AHA Guidelines for the Management of Heart Failure.
Circulation.2013

6/16/2016
7
Legal Principles
Health Insurance Portability and Accountability Act (HIPPA)
– Provides federal protection for privacy of personal health information (PHI).
– Allows PHI to be shared for patient care and claims submissions
– Reasonable and appropriate safeguards must be in place for written communication to maintain privacy. Email should be encrypted or have a mechanism in place to
send securely Fax transmission should be sent to a secure location with a
privacy notice on the cover sheet
HF Nursing Certification: Core Curriculum Review 2nd Edition
Legal Principles
Consent Informed:
– An individual understands the risks and benefitsassociated with the course of treatment.
Implied: – Inferred from inaction or circumstances of the situation – Unconscious patient– Language barrier– Cognitive impairment
Expressed: – Written or verbal agreement from an individual to proceed with treatment
HF Nursing Certification: Core Curriculum Review 2nd Edition
Case Study 1
The rest of the story: now 38
ECHO 6/2015: LVEF 40-45%. LVIDd 4.66 cm. Mild-moderate concentric LVH. LA 3.74 cm.
Trace MR and TR
Cardiopulmonary Test 10/2015: VO2 24.2 mL/kg/min. RQ 1.11. VE/VCO2 slope is 20.3
Continues to call and/or send message with changes
Emails symptoms, weights and blood pressures every other month, seen in clinic every three
months
VanderbiltHeart.com

6/16/2016
8
Definitions of HFrEF and HFpEF
Classification EF (%) Description
I. Heart failure withreduced ejection fraction(HFrEF)
≤40 Also referred to as systolic HF. Randomized clinical trials have mainlyenrolled patients with HFrEF, and it is only in these patients thatefficacious therapies have been demonstrated to date.
II. Heart failure withpreserved ejection fraction(HFpEF)
≥50 Also referred to as diastolic HF. Several different criteria have beenused to further define HFpEF. The diagnosis of HFpEF is challengingbecause it is largely one of excluding other potential noncardiac causesof symptoms suggestive of HF. To date, efficacious therapies have notbeen identified.
a. HFpEF, borderline 41 to 49 These patients fall into a borderline or intermediate group. Theircharacteristics, treatment patterns, and outcomes appear similar tothose of patients with HFpEF.
b. HFpEF, improved >40 It has been recognized that a subset of patients with HFpEF previouslyhad HFrEF. These patients with improvement or recovery in EF maybe clinically distinct from those with persistently preserved or reducedEF. Further research is needed to better characterize these patients.
ACCF/AHA Guidelines for the Management of Heart Failure.
Circulation.2013
Cardiorenal Syndrone
Case Study 2
65 year old male ischemic cardiomyopathy, HFrEF, and chronic
kidney disease. Two HF admissions in past 6 months
HF symptoms: Cough, fatigue, shortness of breath walking 50 feet,
LE edema, early satiety, weight gain
Medications: Lisinopril 5 mg daily, carvedilol 12.5 mg bid, torsemide
50 mg bid, Kcl 20 meq bid, spironolactone 25 mg
Vital signs: BP 94/50, HR 90, weight 160
PE: S3, JVD 12 cm, + HJR, 2+ LE edema, bibasilar crackles
Labs: Na 135, K 4.3, BUN 47, creatinine 3.08 BNP 2985
Cardiorenal Syndrone
Case Study 2
10 pound weight gain above dry weight
Unresponsive to usual daily diuretic doses
Metolazone 5 mg, 30 minutes prior to PM torsemide 100 mg with
additional Kcl 20 meq

6/16/2016
9
Case Study 2
Cardiorenal Syndrone, diuretic resistance
9 lb weight loss
Cardiorenal Syndrome of
Heart Failure
VanderbiltHeart.com
Decreased cardiac output
Neurohormonal activation
Diminished blood flow
Decreased renal perfusion
Decreased cardiacPerformance: right and left
Increased sodium and water retention
Decreased renalfunction
Renal congestion:Increased renal venous pressure
Chronic kidney disease
UpToDate 2016
Cardiorenal Syndrome
Cardio renal syndrome occurs when reduction in cardiac output results in disproportionate reduction in renal perfusion
Leads to diminished glomerular filtration rate (GFR) and increased serum creatinine levels
Worsening renal function:
– Change in serum creatinine >0.3 mg/dL or >25% over baseline (normal range: adult male: 0.8 to 1.4 mg/dL; adult female: 0.6 –1.4 mg/dL)
– >70% of patients will experience increase in creatinine during hospitalization
– 20% to 30% of patients experience increase of >0.3 mg/dL
– Any increase of >0.3 mg/dL is associated with longer LOS and increased mortality
Ronco C. JACC 2008;52(19):1527-1539

6/16/2016
10
Diuretic Resistance
Diuretic Resistance is the persistence of congestion despite diuretic
therapy
– May result from renal under-perfusion
– Distal tubules develop hypertrophy
– There is enhanced sodium reuptake downstream from loop
diuretic site of action
– Oral absorption of loop diuretics is impaired in the setting of gut
hypoperfusion and edema
Treatments
– Restricting NA intake
– Change timing of dose
– Use of combination diuretic therapies
– Ultrafiltration and hemodialysis
Case Study 3
Depression, Fatigue, Family Care-Giver Awareness
42 year old gentleman with ischemic cardiomyopathy, chronic heart failure,
diabetes, HTN, hyperlipidemia, obesity, and depression
He looks sad and doesn't smile. His wife also has health issues also. She is
working 3 jobs to help support the family and they have 2 teenage daughters
that are a challenge at times. He has a poor appetite and has lost >30
pounds since last fall
Complains of fatigue, positional dizziness, and a poor appetite.
Depression in HF Patients
Depression prevalence- 3 times more likely after myocardial infarction
More common in women
More common in HF patients
– 11-48% of outpatients
– 35-70% of inpatients
Severity of depression is linearly related to short and long-term mortality
rates
Heart failure patients with severe depression are four times more likely to die
within 2 years than those non-depressed.
HF Nursing Certification: Core Curriculum Review 2nd Edition

6/16/2016
11
Family/Caregiver Awareness & Involvement
in Care Planning and Delivery
Advocacy is a process in which a healthcare professional provides a
patient with the information needed to make decisions about some
aspect of his/her health care
Respect cultural and spiritual beliefs
Include family and support systems in care planning
and delivery
Identify a proxy if patient is unable to advocate for him/herself.
Caregiver awareness Be aware of signs and symptoms of worsening HF HF follows a chronic illness trajectory with a poor prognosis Understand the physical, mental and emotional aspects of HF care
Caregiver health Should not neglect their own physical, mental and emotional needs Research indicates all caregivers report mild to significant decline in their
own health including: sleep deprivation, weight loss/gain, depression and anxiety.
Seek opportunities for respite care
Case Study 4
Readmissions, Hospital Discharge,Transitions of Care,
62 year old gentleman with ischemic cardiomyopathy,
chronic systolic and diastolic dysfunction, HTN, CKD,
and nonalcoholic fatty liver disease
Admitted with acute on chronic heart failure, altered
mental status, and hepatic encephalopathy
Discharged to Skilled Nursing Facility (SNF)
Readmitted 5 days later with dehydration, weight loss
was attributed to lactulose and excessive bowel
movements, >10/day.
Hospital Readmissions
Represent a significant clinical and economic burden
Healthcare costs for HF in 2009 were > $37 billion with over one million hospital discharges; most costly expense for Medicare (> $4.5 billion annually)
Nearly 1/3 of ALL patients with diagnosis of HF are admitted within 30 days following discharge
Nearly 30% of Medicare HF patients readmitted within 30 days following discharge
HF readmissions could be prevented in at least 40% of cases

6/16/2016
12
Heart Failure Readmissions
Retrospective analyses have shown a markedly increased risk of death in the
first month following discharge; the absolute increase in risk was clearly
related to the number of previous admissions:
Failure to identify precipitant for HF decompensation
Under-treatment of excess volume prior to discharge
Underutilization of evidence-based guidelines for drug and device
therapies
Lack of cardiac specialist consultations
Therapies in the Hospitalized HF Patient
Recommendation COR LOE
HF patients hospitalized with fluid overload should be treated with
intravenous diureticsI B
HF patients receiving loop diuretic therapy, should receive an initial
parenteral dose greater than or equal to their chronic oral daily
dose, then should be serially adjusted
I B
HFrEF patients requiring HF hospitalization on GDMT should
continue GDMT unless hemodynamic instability or contraindicationsI B
Initiation of beta-blocker therapy at a low dose is recommended
after optimization of volume status and discontinuation of
intravenous agents
I B
Thrombosis/thromboembolism prophylaxis is recommended for
patients hospitalized with HFI B
Serum electrolytes, urea nitrogen, and creatinine should be
measured during the titration of HF medications, including diureticsI C
ACCF/AHA 2013 HF Guideline
Address Conditions That May
Cause Increased Heart Failure Symptoms
♥ Ischemia
♥ Anemia
♥ Irregular heart rhythms (Afib,
increased PVC burden)
♥ Electrolyte imbalances
♥ Sleep disordered breathing
♥ COPD
♥ Uncontrolled high blood pressure
♥ Too low or too high thyroid levels
♥ Depression and anxiety
6/16/2016
13
Oral medication regimen stable for 24 hours
No intravenous vasodilator or inotropic agent needed
during previous 24 hours
Ambulation before discharge to assess functional
capacity
Plans for post-discharge management
are initiated (eg, scales to weigh in next care site, visiting
nurse or phone call follow-up within 3 days of discharge)
Heart failure education complete
Criteria that Should be Considered for
Patients with Advanced HF and
Recurrent Readmissions
Hospital DischargeRecommendation or Indication COR LOE
Performance improvement systems in the hospital and early post discharge
outpatient setting to identify HF for GDMTI B
Before hospital discharge, at the first post discharge visit, and in subsequent follow-
up visits, the following should be addressed:
initiation of GDMT if not done or contraindicated
causes of HF, barriers to care, and limitations in support
assessment of volume status and blood pressure with adjustment of HF
therapy
optimization of chronic oral HF therapy
renal function and electrolytes
management of comorbid conditions
HF education, self-care, emergency plans, and adherence; and
palliative or hospice care.
I B
Multidisciplinary HF disease-management programs for patients at high risk for
hospital readmission are recommended I B
A follow-up visit within 7 to 14 days and/or a telephone follow-up within 3 days of
hospital discharge is reasonableIIa B
Use of clinical risk-prediction tools and/or biomarkers to identify higher-risk patients
is reasonableIIa B
ACCF/AHA 2013 HF Guideline
Quality Metrics/Performance
Measures
Guideline for HF

6/16/2016
14
ACCF/AHA/AMA-PCPI 2011 HF
Performance Measurement Set
Measure Description* Care
Setting
Level of
Measurement
1. LVEF
assessment
Percentage of patients aged ≥18 y with a diagnosis of HF for whom the
quantitative or qualitative results of a recent or prior (any time in the
past) LVEF assessment is documented within a 12 mo period
Outpatient Individual
practitioner
2. LVEF
assessment
Percentage of patients aged ≥18 y with a principal discharge diagnosis
of HF with documentation in the hospital record of the results of an
LVEF assessment that was performed either before arrival or during
hospitalization, OR documentation in the hospital record that LVEF
assessment is planned for after discharge
Inpatient Individual
practitioner
Facility
3. Symptom
and activity
assessment
Percentage of patient visits for those patients aged ≥18 y with a
diagnosis of HF with quantitative results of an evaluation of both
current level of activity and clinical symptoms documented
Outpatien
t
Individual
practitioner
*Please refer to the complete measures for comprehensive information, including measure exception.
Adapted from Bonow et al. J Am Coll Cardiol. 2012;59:1812-32.
ACCF/AHA/AMA-PCPI 2011 HF Performance
Measurement Set (cont.)Measure Description* Care
Setting
Level of
Measuremen
t
4. Symptom
management†
Percentage of patient visits for those patients aged ≥18 y with a
diagnosis of HF and with quantitative results of an evaluation of both
level of activity AND clinical symptoms documented in which patient
symptoms have improved or remained consistent with treatment goals
since last assessment OR patient symptoms have demonstrated
clinically important deterioration since last assessment with a
documented plan of care
Outpatient Individual
practitioner
5. Patient self-
care education†‡
Percentage of patients aged ≥18 y with a diagnosis of HF who were
provided with self-care education on ≥3 elements of education during ≥1
visits within a 12 mo period
Outpatient Individual
practitioner
6. Beta-blocker
therapy for LVSD
(outpatient and
inpatient setting)
Percentage of patients aged ≥18 y with a diagnosis of HF with a current
or prior LVEF <40% who were prescribed beta-blocker therapy with
bisoprolol, carvedilol, or sustained release metoprolol succinate either
within a 12 mo period when seen in the outpatient setting or at hospital
discharge
Inpatient
and
Outpatient
Individual
practitioner
Facility
*Please refer to the complete measures for comprehensive information, including measure exception.
†Test measure designated for use in internal quality improvement programs only. These measures are not appropriate for any
other purpose, e.g., pay for performance, physician ranking or public reporting programs.
‡New measure.
Adapted from Bonow et al. J Am Coll Cardiol. 2012;59:1812-32.
ACCF/AHA/AMA-PCPI 2011 HF Performance Measurement
Set (cont.)
Measure Description* Care Setting Level of
Measurement
7. ACE Inhibitor or
ARB Therapy for
LVSD (outpatient and
inpatient setting)
Percentage of patients aged ≥18 y with a diagnosis of HF with a
current or prior LVEF <40% who were prescribed ACE inhibitor or
ARB therapy either within a 12 mo period when seen in the outpatient
setting or at hospital discharge
Inpatient
and
Outpatient
Individual
practitioner
Facility
8. Counseling
regarding ICD
implantation for
patients with LVSD
on combination
medical therapy†‡
Percentage of patients aged ≥18 y with a diagnosis of HF with current
LVEF ≤35% despite ACE inhibitor/ARB and beta-blocker therapy for at
least 3 mo who were counseled regarding ICD implantation as a
treatment option for the prophylaxis of sudden death
Outpatient Individual
practitioner
9. Post-discharge
appointment for heart
failure patients
Percentage of patients, regardless of age, discharged from an
inpatient facility to ambulatory care or home health care with a
principal discharge diagnosis of HF for whom a follow-up appointment
was scheduled and documented including location, date and time for
a follow-up office visit, or home health visit (as specified)
Inpatient Facility
*Please refer to the complete measures for comprehensive information, including measure exception.
†Test measure designated for use in internal quality improvement programs only. These measures are not appropriate for any o ther
purpose, e.g., pay for performance, physician ranking or public reporting programs.
‡New measure.
Adapted from Bonow et al. J Am Coll Cardiol. 2012;59:1812-32.

6/16/2016
15
Transitional CareBreaking the Cycle of Readmission
Transitional Care
Transitional Care: set of actions designed to ensure coordination and continuity of
health care as patients transfer between different
locations or different levels of care
Hospital Discharge Discharge
Planning
Follow upHospitalization
andTreatment
Admission
Transition of Care Recommendations for Clinical Practice
Recommendations Considerations for Implementation of Recommendation
Systematically implement principles of transition of care programs in high-risk patients with chronic HF.
Include*Medication reconciliation*Very early postdischarge contact and communication with patient and/or care provider*Early office follow-up within first week of discharge*Patient education on chronic HF self-care, including skills for recognizing early warning signs of worsening *HF and independently completing HF self-carebehaviors *Communication of patient health record with patient and postdischarge healthcare providers*Integrated, interdisciplinary collaboration and coordination*A framework that ensures that education is initiated in the hospital before the day of discharge and continues during initial community-based care
Albert et al Transitions of Care in Heart Failure. Circulation Heart
Failure. 2015
Transition of Care Recommendations for Clinical Practice
Recommendations Considerations for Implementation of Recommendation
Routinely assess patients for high-risk characteristics that may be associatedwith poor post-discharge clinical outcomes.
Exemplars include cognitive difficulties, impaired learning capabilities, non–Englishspeaking, and long travel time to healthcare providers
Ensure that qualified and trained HF nurse or other healthcare providers of clinical HF provide care services.
Assess healthcare provider knowledge and comfort in delivering patient education and interdisciplinary care coordination services
Allot adequate time in the hospital and postacutesetting to deliver complex chronic HF interventions and to assess patient and caregiver responsiveness
Incorporate time to complete high-level interventions into care plans, including patients’ ability to understand HF self-management interventions and to complete skills and expectations independently
Albert et al Transitions of Care in Heart Failure. Circulation Heart
Failure. 2015

6/16/2016
16
Transition of Care Recommendations for Clinical Practice
Recommendations Considerations for Implementation of Recommendation
Implement handoff procedures at hospital or post–acute care discharge
*Provide patient health records with key details of the hospital/postacute experience (medications used, discharge medications, procedures, treatments, postdischarge care expectations, planned rehospitalization and/or follow-up services, knownpsychosocial issues, and medication reconciliation)*Ensure that handoff documents are transmitted to postdischarge care providers ina timely manner
Albert et al Transitions of Care in Heart Failure. Circulation Heart
Failure. 2015
Transition of Care Recommendations for Clinical Practice
Recommendations Considerations for Implementation of Recommendation
Develop, monitor, and ensure transparency of results of quality measures using a structure, process, and outcome framework.
*Promote fidelity of the program and consistent application by healthcare providers*Ensure leadership and administrative support, including clinical leaders (navigators, advocates, etc)
Consider patients’ perceptions of QOL as a surrogate for physical, psychological, and social concerns that require support during the transition of care process.
Provide bridging for specific patient support needs
Albert et al Transitions of Care in Heart Failure. Circulation Heart
Failure. 2015
Transition of Care Recommendations for Clinical Practice
Recommendations Considerations for Implementation of Recommendation
Ensure availability of transition of care component details in writing (eg, a training manual)
Promote fidelity of the program and consistent application by healthcare providersEnsure leadership and administrative support, including clinical leaders (navigators, advocates, etc)
Use health informatics technology to assist with program sustainability. Informatics should be patient and healthcare provider centric.
Evaluate data for applicability and completeness in facilitating patient communication and care coordination, quality metrics, research, and financialAnalyses
Albert et al Transitions of Care in Heart Failure. Circulation Heart Failure. 2015

6/16/2016
17
Improving Transition
Nurses play a key role in inpatient and outpatient management and improving patient outcomes using a comprehensive, integrated system to manage patients
Nurse-coordinated outpatient care has been shown to reduce HF hospitalizations by more than 60%
Studies have found that specifically trained HF nurses are one crucial element found in HF multidisciplinary management models (eg, clinic visits, pt education, medication titration, device management, research, support groups)
Case Study 5 Professionalism
40 year old with nonischemic cardiomyopathy, chronic heart failure, morbid obesity,
hypertension, with a recent admission for atrial fibrillation with rapid ventricular response. He
has been a “no-show” or canceled multiple visits. He has not refilled any of his medications,
he is only taking a baby aspirin a day
He comes to the clinic with an offensive odor and dirty clothing
BP 170/110, heart rate 100
Professionalism
Reflects the values and behaviors of the nurse caring for patients demonstrated by:
Following ethical principles
Advocating for the patient and his/her family
Keeping abreast of research
Using evidence to guide clinical practice

6/16/2016
18
Ethical/Legal Principles
Preventing Health Care Disparities Disparities are the differences in health outcomes which occur even when
patient preferences, access and clinical factors are controlled
The United States demographics continue to change with increasing numbers of Hispanics, Asians and African Americans
Including under-represented individuals in quality improvement activities and clinical research will promote understanding of differences and potentially reduce disparities
Scope of practice Determines who can legally perform specific duties in the care of a patient Nurses are responsible for the delivery of nursing care and are accountable
for activities delegated to others including but not limited to licensed practical nurses, certified nursing assistants and certified medical technologists
Nurses act as a liaison with other medical professionals
Advance practice nurses scope of practice is determined by the state in which they are licensed
Ethical Principles
• Respect for Persons – Respect is both a behavior and an act
– Demonstrates honor to another individual
– Address patient with proper surname and
avoid terms of endearment
• Autonomy refers to the ability to make decisions– May be compromised due to illness or cognitive disorder
– May need to appoint someone else as proxy
• Individual rights – Right to privacy
– Right treatment
– Right to be informed
• Justice refers to being fair, not necessarily equitable – Seeks to focus on the common good
– May be in conflict with respect for persons
HF Nursing Certification: Core Curriculum Review 2nd Edition
Ethical/Legal Principles
Beneficence The state or quality of being kind, charitable, or beneficial in action that is done for the
benefit of others. Doing good.
Resuscitating a drowning victim, providing vaccinations for the general population,
encouraging a patient to quit smoking and start an exercise program, talking to the
community about STD prevention.
Non-Maleficence “Do no harm.” we must refrain from providing ineffective treatments or acting with malice
toward patients. Maximize benefits and minimize harm
– Stopping a medication that is shown to be harmful, refusing to provide a treatment that has not been shown to be effective.
HF Nursing Certification: Core Curriculum Review 2nd Edition

6/16/2016
19
Case Study 5 Professionalism
Provide quality care for the patient !
EKG shows sinus rhythm, medications resumed
Individual follow up plan was agreed upon: text and 8:30 AM clinic visits
Beneficence: providing health benefits to the patient, active promotion of good.
Legal Principles
Negligence
A lack of care and vigilance demanded by the situation
Results in harm to an individual
Malpractice
An omission or negligence by act as a result of deviating from the standard of practice which results in harm to an individual
HF Nursing Certification:
Core Curriculum Review 2nd
Edition
Case Study 6
Ethical Principles
56 year old female with metastatic cancer and heart failure
She has now been treated for 1.5 years with chemotherapy. Worsening LVEF, 20%. After
extensive discussions with cardiologist and oncologist, she decides that she no longer
desires curative cancer treatment. She would rather live remaining days with Hospice Care.
This is an example of impeding which ethical principle?
A. Justice
B. Respect for Persons
C. Beneficence
D. Maleficence
B. Respect for persons
*She has the right to make an informed
decision*Further chemotherapy may not prolong life.
*She prefers quality of life over quantity.

6/16/2016
20
Test Taking Strategies
Test Taking Strategies
• Write down information you’re worried about remembering (ICD
criteria, wedge pressure)
• Read each question all the way through before looking at the
answer choices.
• Try to solve each problem before looking at the answer alternatives
to avoid being thrown off by the choices given.
• Make educated guesses; eliminate the obvious incorrect answer
choices right away and use reasoning to find the best possible
answer choice through the process of elimination.
• Pick answers that honor the patient first

6/16/2016
21
Test Taking Strategies
• Determine precisely what the question is asking; one solution will plainly be the best choice, so read through all answer choices since the best answer could be the last choice in the list.
• Do not spend too much time on any one question; skip more difficult questions and go back to those once all other questions have been answered.
• Do not change an answer-unless the question was misread; the first answer selected is usually the correct choice.
• Do not stay up all night studying; get a good night’s sleep.
Test Taking Strategies
• When it seems like more than one answer is correct there are some strategies for narrowing
down the choices in order to find the right choice.
• Examine the answer being considered and determine whether it is only partly true when
addressing the question, or if it would only be true under certain circumstances. If this is the
case, it is probably not the correct answer.
• Take each question at face value; do not assume the instructor has created any “trick”
questions. Avoid reading too much into a question.
CHFN or CHFN-K: Is in YOUR Future

6/16/2016
22
For Your InformationNot on 2016 CHFN/CHFN-K Test
Guideline-Directed Evaluation and Management
(GDEM)
• Refers to ACC/AHA Class I recommendations
Yancy CW, et al Heart Failure Focused Update
on Pharmacological Therapy 2016

6/16/2016
23
ACC/AHA Recommended System 2015 update
ACE-I/ARB
ARNI
Drugs Commonly Used for HFrEF
(Stage C HF)Drug Initial Daily Dose(s) Maximum Doses(s)
Mean Doses Achieved in
Clinical Trials
ACE Inhibitors
Captopril 6.25 mg 3 times 50 mg 3 times 122.7 mg/d (421)
Enalapril 2.5 mg twice 10 to 20 mg twice 16.6 mg/d (412)
Fosinopril 5 to 10 mg once 40 mg once ---------
Lisinopril 2.5 to 5 mg once 20 to 40 mg once 32.5 to 35.0 mg/d (444)
Perindopril 2 mg once 8 to 16 mg once ---------
Quinapril 5 mg twice 20 mg twice ---------
Ramipril 1.25 to 2.5 mg once 10 mg once ---------
Trandolapril 1 mg once 4 mg once ---------
ARNI
Sacubitril/valsartan 24 mg/26 mg bid 49 mg/51 mg bid 97 mg/103 mg bid
ARBs
Candesartan 4 to 8 mg once 32 mg once 24 mg/d (419)
Losartan 25 to 50 mg once 50 to 150 mg once 129 mg/d (420)
Valsartan 20 to 40 mg twice 160 mg twice 254 mg/d (109)
Aldosterone Antagonists
Spironolactone 12.5 to 25 mg once 25 mg once or twice 26 mg/d (424)
Eplerenone 25 mg once 50 mg once 42.6 mg/d (445)
Yancy C et al. Circulation 2013;128:e240-e327
Yancy C.et al. JACC 2016; 05.011
ARNIWhen compared to enalapril:
Reduced cardiovascular death by 20%
Reduced HF hospitalizations by 20%
May lead to angioedema
Caution with low BP and renal insufficiency
Although the use of an ARNI in lieu of an ACE inhibitor
for HFrEF has been found to be superior, for those
patients for whom ARNI is not appropriate, continued
use of an ACE inhibitor for all classes of HFrEF remains
strongly advisedYancy CW, et al Heart Failure Focused Update on
Pharmacological Therapy 2016
6/16/2016
24
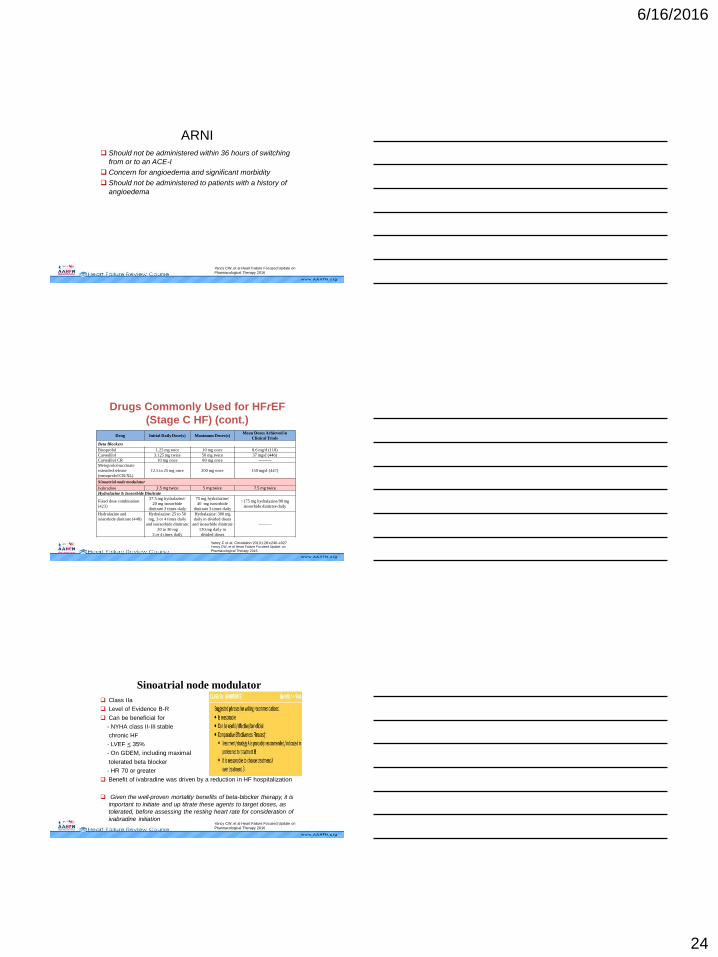
ARNI Should not be administered within 36 hours of switching
from or to an ACE-I
Concern for angioedema and significant morbidity
Should not be administered to patients with a history of
angioedema
Yancy CW, et al Heart Failure Focused Update on
Pharmacological Therapy 2016
Drugs Commonly Used for HFrEF
(Stage C HF) (cont.)
Drug Initial Daily Dose(s) Maximum Doses(s)Mean Doses Achieved in
Clinical Trials
Beta Blockers
Bisoprolol 1.25 mg once 10 mg once 8.6 mg/d (118)
Carvedilol 3.125 mg twice 50 mg twice 37 mg/d (446)
Carvedilol CR 10 mg once 80 mg once ---------
Metoprolol succinate
extended release
(metoprolol CR/XL)
12.5 to 25 mg once 200 mg once 159 mg/d (447)
Sinoatrial node modulator
Ivabradine 2.5 mg twice 5 mg twice 7.5 mg twiceHydralazine & Isosorbide Dinitrate
Fixed dose combination
(423)
37.5 mg hydralazine/
20 mg isosorbide
dinitrate 3 times daily
75 mg hydralazine/
40 mg isosorbide
dinitrate 3 times daily
~175 mg hydralazine/90 mg
isosorbide dinitrate daily
Hydralazine and
isosorbide dinitrate (448)
Hydralazine: 25 to 50
mg, 3 or 4 times daily
and isorsorbide dinitrate:
20 to 30 mg
3 or 4 times daily
Hydralazine: 300 mg
daily in divided doses
and isosorbide dinitrate
120 mg daily in
divided doses
---------
Yancy C et al. Circulation 2013;128:e240-e327 Yancy CW, et al Heart Failure Focused Update on
Pharmacological Therapy 2016
Sinoatrial node modulator
Class IIa
Level of Evidence B-R
Can be beneficial for
- NYHA class II-III stable
chronic HF
- LVEF < 35%
- On GDEM, including maximal
tolerated beta blocker
- HR 70 or greater
Benefit of ivabradine was driven by a reduction in HF hospitalization
Given the well-proven mortality benefits of beta-blocker therapy, it is
important to initiate and up titrate these agents to target doses, as
tolerated, before assessing the resting heart rate for consideration of
ivabradine initiation Yancy CW, et al Heart Failure Focused Update on
Pharmacological Therapy 2016