Embed Size (px)
Citation preview
9/13/15
1
Feeding and swallowing in cerebral palsy:
Evidence-‐based prac6ce and beyond
Georgia A. Malandraki, PhD, CCC-SLP, BCS-S1 Jaime L. Bauer Malandraki, MS, CCC-SLP1
Justine Joan Sheppard, Ph.D., CCC-SLP, BCS-S2
1Dept. of Speech, Language and Hearing Sciences, Purdue University 2Dept. of Biobehavioral Sciences, Teachers College, Columbia University
AACPDM, October 2015
Disclosure Information AACPDM 69th Annual Meeting | October 21-24, 2015
Speaker Name: Georgia A. Malandraki Disclosure of Relevant Financial Relationships I have the following financial relationships to disclose: - Grant/Research support from: Purdue University - Employee of: Purdue University
Disclosure of Off-Label and/or investigative uses: I will not discuss off label use and/or investigational use in my presentation
Speaker Name: Jaime Bauer Malandraki
Disclosure of Relevant Financial Relationships I have the following financial relationships to disclose: - Employee of: Purdue University
Disclosure of Off-Label and/or investigative uses: I will not discuss off label use and/or investigational use in my presentation
Disclosure Information AACPDM 69th Annual Meeting | October 21-24, 2015
Speaker Name: Justine Joan Sheppard Disclosure of Relevant Financial Relationships I have the following financial relationships to disclose: - Member, Nutritional Management Associates, LLC - Honorary Associate Professor, Teachers College, Columbia University
Disclosure of Off-Label and/or investigative uses: I will discuss the following investigational use in my presentation: - The Dysphagia Disorder Survey (results of research)
Purdue I-‐EaT Research Lab and Clinic
(Imaging, Evalua/on and Treatment of Swallowing Laboratory)
Lab email: [email protected]
Course Outline
1. Brief Introduc/on -‐ Feeding and swallowing in CP 2. Review of current literature on evalua/on tools 3. Review of current literature on treatment and
research evidence 4. What to do when research evidence is limited?
1. Other types of evidence 2. Overview of principles of neuroplas/city and motor
learning for swallowing rehabilita/on 5. Case studies / Discussion
5
Learning Objec6ves
Learning Objec6ve 1: – To be able to define specific swallowing evalua/on and treatment techniques and iden/fy those that are evidence-‐based.
Learning Objec6ve 2: – To understand the extent and limita/ons of current swallowing evalua/on and treatment techniques.
Learning Objec6ve 3: – To develop skills in how to incorporate principles of motor learning and neuroplas/city into clinical prac/ce.
6
9/13/15
2
INTRODUCTION
FEEDING AND SWALLOWING IN CP
7
Feeding and swallowing in CP • Physiology and Func6on
8
PHYSIOLOGY Stages
FUNCTION Behavior
Pre-‐oral
Posi6oning An6cipa6on
(saliva)
Oral
Containment Chewing Transport
Pharyngeal
Timing Efficiency
Esophageal
Post swallow behaviors
Feeding and swallowing in CP (Cont.)
• Pre-‐oral Stage
9
PHYSIOLOGY FUNCTION
Poor posi6oning
Instability Poor orien6ng Poor recep6on
Inability to self-‐feed
Poor head control /
hyperextension
Poor orien6ng Poor recep6on
Inability to self-‐feed
Cogni6ve challenges
Poor orien6ng Inability to self-‐feed
Autonomic system challenges
Excess saliva Poor containment
Feeding and swallowing in CP (Cont.)
• Oral Stage
10
PHYSIOLOGY FUNCTION
Tongue thrust
Difficulty with tongue propulsion
Poor containment Poor oral transport
Poor labial seal Difficulty with tongue propulsion
Poor containment Poor oral transport
Oral hypersensi6vity /
reflexes
Poor recep6on Poor containment
Poor lingual coordina6on/
strength
Poor oral transport Poor oral control Inefficient chewing
Feeding and swallowing in CP (Cont.)
• Pharyngeal Stage
11
PHYSIOLOGY FUNCTION
Delayed pharyngeal response
Risk for aspira6on (coughing) Residue (mul6ple swallows)
Pharyngeal dysmo6lity
Risk for aspira6on (coughing) Residue (mul6ple swallows)
Reduced hyolaryngeal excursion
Risk for aspira6on (coughing) Residue (mul6ple swallows)
Reduced UES opening
Risk for aspira6on (coughing) Residue (mul6ple swallows)
Regurgita6on/reflux
Feeding and swallowing in CP (Cont.)
• Esophageal and lower GI concerns (briefly): – GERD – Esophageal Dysmo/lity – Delayed gastric emptying – Cons/pa/on – And more …
12
Sullivan, 2009
9/13/15
3
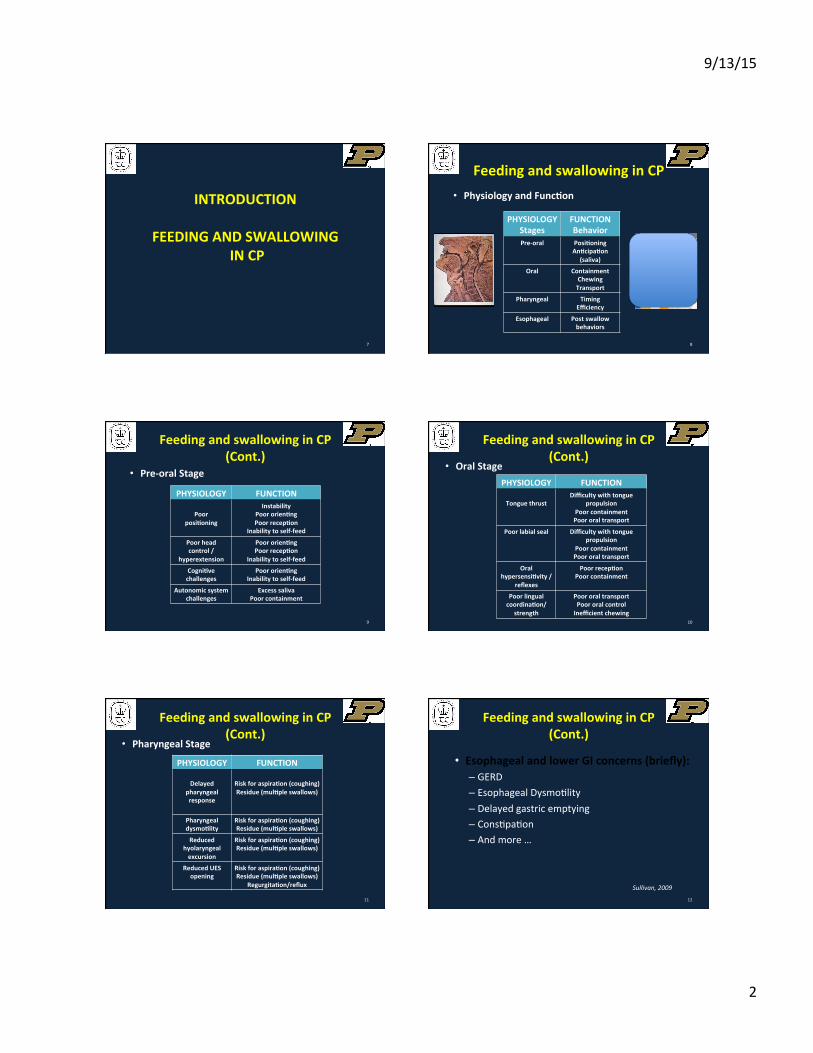
Esophageal Mo6lity Problems in Cerebral Palsy
Normal Hypotensive LES Hypomo/lity
13 Staiano & Mar2nelli, 2013
ASSESSMENT OF FEEDING AND SWALLOWING
IN CP
14
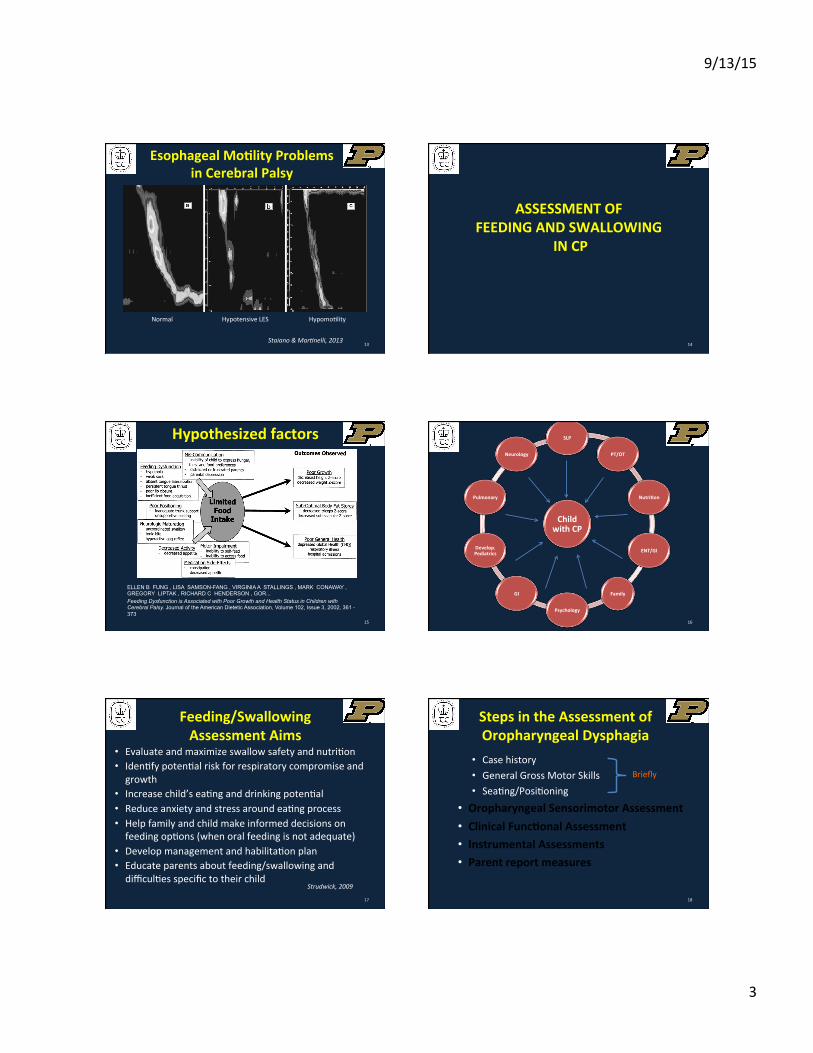
ELLEN B FUNG , LISA SAMSON-FANG , VIRGINIA A STALLINGS , MARK CONAWAY , GREGORY LIPTAK , RICHARD C HENDERSON , GOR... Feeding Dysfunction is Associated with Poor Growth and Health Status in Children with Cerebral Palsy. Journal of the American Dietetic Association, Volume 102, Issue 3, 2002, 361 - 373
Hypothesized factors
15 16
Child with CP
SLP
PT/OT
Nutri6on
ENT/GI
Family
Psychology
GI
Develop. Pediatrics
Pulmonary
Neurology
Feeding/Swallowing Assessment Aims
• Evaluate and maximize swallow safety and nutri/on • Iden/fy poten/al risk for respiratory compromise and growth
• Increase child’s ea/ng and drinking poten/al • Reduce anxiety and stress around ea/ng process • Help family and child make informed decisions on feeding op/ons (when oral feeding is not adequate)
• Develop management and habilita/on plan • Educate parents about feeding/swallowing and difficul/es specific to their child
Strudwick, 2009
17
Steps in the Assessment of Oropharyngeal Dysphagia
• Case history • General Gross Motor Skills • Sea/ng/Posi/oning
• Oropharyngeal Sensorimotor Assessment • Clinical Func6onal Assessment • Instrumental Assessments • Parent report measures
18
Briefly
9/13/15
4
Oropharyngeal Sensorimotor Evalua6on
• Evalua6ng CN func6ons – Examina6on of structures at rest and during
directed tasks – Can the child perform these func6ons?
• Spontaneously • With Imita/on • With Verbal Instruc/on
19
Oropharyngeal Sensorimotor Evalua6on (Cont.)
• Face – Motor – CN VII • Jaw/Face – Motor and sensory – CN V • Tongue – Motor – CN XII • Velum – Motor – CNs V and X • Oral sensa6on and taste – CNs V, VII and IX • Examina6on of primi6ve reflexes
20
Clinical Func6onal Assessments
• Trial Swallows – Assess aspects of CN func/on but during ea/ng and drinking
– “Clinical Dysphagia Evalua/on” or “Clinical Bedside Swallow Evalua/on”
– No standardiza/on between clinicians
21
Clinical Func6onal Assessments (Cont.)
• Standardized assessments (many) (Benfer et al. 2012)
• 3 with highest clinical u6lity – Dysphagia Disorder Survey [DDS] (Sheppard et al. 2014)
– Schedule for Oral Motor Assessment [SOMA] (Skuse et al. 1995)
– Pre-‐Speech Assessment Scale [PSAS] (Morris, 1982)
22
Important terms • Reliability = overall consistency of a measure
– Intra-‐ and inter-‐rater
• Specificity = the propor/on of nega/ves that are correctly iden/fied as nega/ve
• Sensi6vity = propor/on of posi/ves that are correctly iden/fied as such (true posi/ves)
• Validity = the extent to which a test measures what it is supposed to measure – Content validity (is it measuring OPD) – Construct validity (convergent and discrimina/ve)
23
Clinical Func6onal Assessments (Cont.)
• Dysphagia Disorder Survey (Sheppard et al. 2014) • During a func/onal ea/ng task: natural environment • Includes: five bites/sips of each texture of food and liquid that are typical in the child’s diet
• Binary scoring of different items – Training and cer/fica/on required – Reliability: κw =0.4; 0.7 (97.5% and 92.5%) (intra and inter) – High sensi/vity; low or moderate specificity (especially in younger children)
– Validity: content; convergent and discrimina/ve
Benfer et al. 2012; Benfer et al. 2014; Sheppard et al. 2014
24
9/13/15
5
Clinical Func6onal Assessments (Cont.)
• Schedule for Oral Motor Assessment (SOMA) (Skuse et al. 1995)
• Also, during ea/ng tasks • Binary scoring of different items (80 items) • OMC scored for every food item
– Training and cer/fica/on required – Reliability: κw = 0.9; 0.7 (92.5%; 85%) (intra; inter) – High specificity (especially for oral phase impairments); low sensi/vity
– Validity: content (strong); limited convergent and discrimina/ve
Benfer et al. 2012; Benfer et al. 2014; Ju Ko et al. 2011
25
Clinical Func6onal Assessments (Cont.)
• Pre-‐Speech Assessment Scale (PSAS) – Examines 27 pre-‐speech feeding behaviors up to 24+ months – Performance areas: sucking, swallowing, bi/ng, chewing, respira/on-‐phona/on, sound play
– Reliability: κw = 0.5; 0.5 (92.5%; 95%) (intra; inter) – High sensi/vity; low specificity – Validity: moderate content; no other types
Benfer et al. 2012; Benfer et al. 2014
26
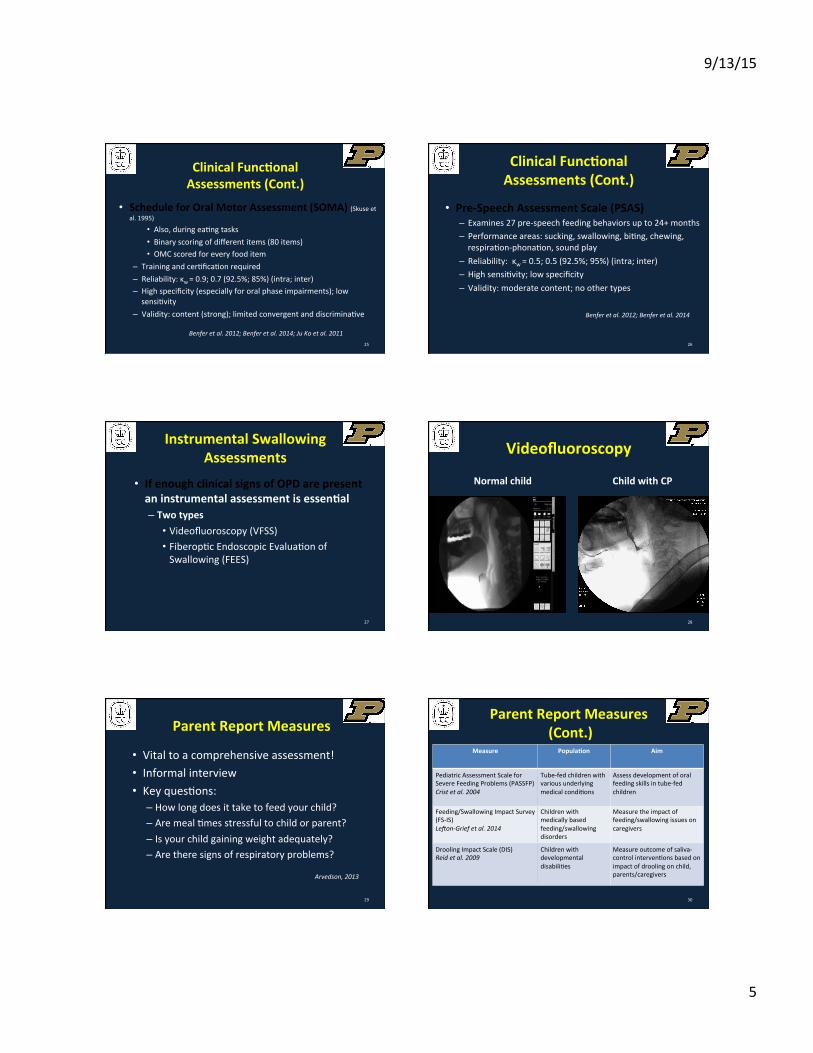
Instrumental Swallowing Assessments
• If enough clinical signs of OPD are present an instrumental assessment is essen6al – Two types
• Videofluoroscopy (VFSS) • Fiberop/c Endoscopic Evalua/on of Swallowing (FEES)
27
Videofluoroscopy
28
Normal child Child with CP
Parent Report Measures
• Vital to a comprehensive assessment! • Informal interview • Key ques/ons:
– How long does it take to feed your child? – Are meal /mes stressful to child or parent? – Is your child gaining weight adequately? – Are there signs of respiratory problems?
Arvedson, 2013
29
Measure Popula6on Aim
Pediatric Assessment Scale for Severe Feeding Problems (PASSFP) Crist et al. 2004
Tube-‐fed children with various underlying medical condi/ons
Assess development of oral feeding skills in tube-‐fed children
Feeding/Swallowing Impact Survey (FS-‐IS) LeGon-‐Grief et al. 2014
Children with medically based feeding/swallowing disorders
Measure the impact of feeding/swallowing issues on caregivers
Drooling Impact Scale (DIS) Reid et al. 2009
Children with developmental disabili/es
Measure outcome of saliva-‐control interven/ons based on impact of drooling on child, parents/caregivers
30
Parent Report Measures (Cont.)
9/13/15
6
EDACS
31
• Ea6ng and Drinking Ability Classifica6on System for individuals with CP (EDACS) (Sellers et al. 2014) Swallowing and Feeding
Management in CP
32
Management of feeding and swallowing
• Aim – Op6mum quality of life for child and family – Health and safety
• Minimizing aspira/on, choking and respiratory infec/ons
• Op/mizing nutri/on and hydra/on – Advancing ea6ng and drinking skills and behaviors
• Improve swallowing and oropharyngeal skills to support oral feeding and saliva control
• Take advantage of developmental neuroplas/city for motor learning!
Sheppard & Malandraki, 2015
33
Management of feeding and swallowing (Cont.)
• Exact management plan will depend on evalua6on outcomes for feeding and swallowing
– Medical – Developmental – Neuro-‐motor – Family issues
Sheppard & Malandraki, 2015
34
Outcomes of Treatment (WHO 2001)
Body structures and func/on
Ac/vi/es Par/cipa/on
35 Bilbao et al. 2002
Compensatory Strategies (Environmental Manipula6ons)
• Interven6ons that support improved swallowing performance but results do not con6nue once the strategy is withdrawn
• In children, compensatory strategies may be used to support prac6ce in less demanding ea6ng tasks to improve skill
Arvedson, 2013; Sheppard & Malandraki, 2005
36
9/13/15
7
Compensatory Strategies
• Sea6ng posture • Diet consistencies • Environmental changes • Adap6ve oral feeding techniques and equipment
• Gastrostomy feeding
Sheppard & Malandraki, 2015
37
Sea6ng Posi6on for Feeding and Swallowing
• Sea6ng (by team, PT, OT and SLP) – The child’s postural aims
• Lower body (hips and lower extremi/es) stable on suppor/ng surfaces
• Balance of stability and mobility in upper body; balance of flexion and extension overall
• Head-‐neck upright with chin downward (capitol ventro-‐flexion)
• Forearms supported on anterior surface
Myhr & von Wendt, 1991; Snider et al. 2011 38
Sea6ng Posi6on for Feeding and Swallowing (Cont.)
• The Chair op6ons for achieving aims • Lower and mid-‐body stabiliza6on
• Foot rest • Seat • Arm rest • Tray • Bel/ng
• Upper body balance – stability and tone • Tray height • Seat back/seat angle • Seat back height • Head rest Myhr & von Wendt, 1991; Snider et al. 2011
39
SiOng in original posi2on, in own adapted 'Relax' chair. Line of gravity (arrow) is posterior to fulcrum at ischial tuberosi2es (circle). Postural control and arm and hand func2on were worst on this posi2on and pathological movements (asymmetric
tonic neck reflex) were most frequent.
Same girl in func2onal siOng posi2on in 'Real' chair, with line of gravity (arrow) anterior to ischial tuberosi2es (circle). Asymmetric tonic neck reflex is inhibited and postural control enhanced, so she is able to use arms and hands to learn
computer programme.
Illustra6on of “func6onal sea6ng”
40 Myhr & von Wendt, 1991
Illustra6on of Suppor6ve Sea6ng
41
Tradi6onal Diet Modifica6ons – The Interna6onal Dysphagia Diet Standardisa6on Ini6a6ve
42
9/13/15
8
Criteria for Selec6ng Diet Modifica6ons
• Pre-‐oral and Oral prepara6on tolerances, skills and competencies
• Oral-‐pharyngeal competencies • Esophageal mo6lity • Demands for
§ Nutri/on § Hydra/on § Airway protec/on
43
Environmental Considera6ons
• Monitoring and assis/ng • Encouraging/allowing independence • Modera/ng acous/c and visual complexity • Maintaining familiarity • Establishing op/mum ea/ng-‐/me • Modera/ng stressful environments
44
Adap6ve oral feeding techniques and equipment
45
§ Adapta6ons in Technique § Size of bite -‐ Smaller bites / sips § Rate of bite presenta/on § Alternate solids with liquids § Control of texture and viscosity § More frequent, smaller meals § Reflux precau/ons following ea/ng
Sheppard, 1995
Assis6ve feeding devices
§ Special feeding spoons and forks
§ Sculptured / nosey cups § One-‐way valve straws § Wide straws § Mechanized self-‐feeders
46
47
Gastrostomy Feeding
• Benefits – Nutri/onal status – Number of hospital admissions for chest infec/on – Quality of life for child and family
• Special considera6ons for dysphagia treatment – Medical management for transi/on – Day/me, meal/me hunger-‐sa/a/on GT feeding schedule
– Bolus GT feedings – Exposure to family/classroom ea/ng environments – Therapeu/c tastes and pleasure feedings
48 McKirdy et al. 2008; Mehta & Acerni, 2015; Rempel, 2015
9/13/15
9
Habilita6ve Management for Dysphagia
• Medical treatments – Aim: Op/mize esophageal and GI func/on
• Behavior modifica6on strategies – Aim: improve ea/ng mo/va/on and coopera/ve pragma/cs for ea/ng/meal/me
• Motor learning strategies for func6onal skills – Aim: op/mize prac/ce of goal oriented tasks for skill acquisi/on and improvements in performance quality for oral-‐pharyngeal swallow
Sheppard & Malandraki, 2015; Novak et al. 2013
49
Research Evidence for Habilita6ve Swallowing Treatments in CP
Snider, L., Majnemer, A., & Darsaklis, V. (2011). Feeding Interven6ons for Children with Cerebral Palsy: A review of the evidence. Physical & Occupa;onal Therapy in Pediatrics, 31(1)58-‐77 Interpreta/on: Feeding interven/ons demonstrate poten/al benefits for children with cerebral palsy. However the current level of evidence is poor, and empirical data are lacking. Methodologically, rigorous studies are required par/cularly inves/ga/ng mul/modal approaches.
Novak, I., McIntyre, S., Morgan, C., et al. (2013). A systema6c review of interven6ons for children with cerebral palsy: State of the evidence. Developmental Medicine Child Neurology, 55: 885-‐910. Interpreta/on: Evidence for supports across treatments. Green Light interven/ons – ‘use it’. Yellow Light interven/ons should be accompanied by a sensi/ve outcome measure to monitor progress – ‘probably use it’. Red Light interven/ons should be discon/nued.
*******
50
Evidence for Habilita6ve Interven6ons
• Top-‐down approach – Use neuroplas/city to change func/on through treatments aimed at ac/vity and par/cipa/on!
• Green Light (general) – Context focused – Goal-‐based using motor learning approach – Home-‐based, goal-‐based tasks by parent supported by clinician
Novak et al. 2013; Snider et al. 2011; Sheppard & Malandraki, 2015
51
Evidence for Habilita6ve Interven6ons (Cont.)
• Yellow Light (Meal/me specific) – Dysphagia Management – safe swallowing and skills
– Gastrostomy – Fundoplica/on
• Yellow Light (General) – Parent educa/on for behavior management – Sea/ng and posi/oning
52
Novak et al. 2013
Evidence for Habilita6ve Interven6ons (Cont.)
• Meal6me specific insufficient evidence (weak evidence*) – Sensory processing – Oral motor treatments
*probably do not do it. Stronger evidence for task specific strategies.
Novak et al. 2013
53
Special Notes on Interven6ons for Drooling
• Problem: 40% of 7-‐14 yo children with CP • Treatments that have been studied
– Sensorimotor therapy and swallow improvement – Oral appliance – Systemic an/cholinergic medica/ons – Botulinum toxin therapy to the submandibular and/or paro/d glands
– Surgery Johnson et al. 2004; Reid et al. 2012; Snider et al. 2011; Walshe et al. 2012
54
9/13/15
10
Habilita6on What do we do when research
evidence is so poor??
In absence of well-‐documented clinical efficacy, clinicians have to base their treatment decisions on the underlying theore2cal or physiological basis of a treatment or disorder respec2vely
Arvedson et al. 2010; Clark, 2003
55
Case Study 1
56
Case Study 2
57
Case Studies
• What dysphagia treatment(s) would you recommend? – Design and write the outline of a treatment plan for these pa6ents • Compensatory strategies • Habilita/ve strategies (amount, repe//ons, days etc.)
• Dura/on • Follow-‐up
We will discuss this at the end of the session
58
Habilita6on What do we do when research
evidence is so poor??
59 Puddy, R. W. & Wilkins, N. (2011)
Levels of Evidence
60
9/13/15
11
61
By enhancing our ...
• Experien6al Evidence
• Contextual Evidence
62
Experiential Evidence Enhancement
• “Evidence-‐based rehabilita6on programs need to be developed upon the knowledge of nervous system func6on and control over the sensorimotor task being rehabilitated”
• “AND follow principles of experience-‐dependent plas6city and motor learning” Charles & Gordon, 2006; Kleim & Jones, 2008
63
Swallowing Neurophysiology Highly Complex
Malandraki et al. 2009; 2011; Mar2n & Sessle, 1993; Miller, 1986; Miller, 1993
PNS
NOT A MERE REFLEX ANYMORE, BUT A RESPONSE!
Principles of experience-‐dependent plas6city and motor learning approaches
1. Use it or lose it 2. Use it and improve it 3. Plas/city is experience-‐specific (specificity of learning) 4. Repe//on mayers (maximizing opportuni/es for prac/ce) 5. Intensity mayers
6. Time mayers
7. Salience mayers (ayen/on and mo/va/on)
8. Age mayers
9. Transference
10. Interference
Kleim & Jones, 2008; Sheppard, 2008 64
More motor learning approaches • Implicit learning • Rehearsal strategies
– Through different steps in the learning process
• Blocked and random prac6ce • Distributed vs. massed prac6ce • Feedback • Transfer of learning
Sheppard, 2008
65
What could that look like??
66
R A
Child 11 yoa with spas6c hemiplegia A) Not affected B) Mildly C) Moderately D) Severely
9/13/15
12
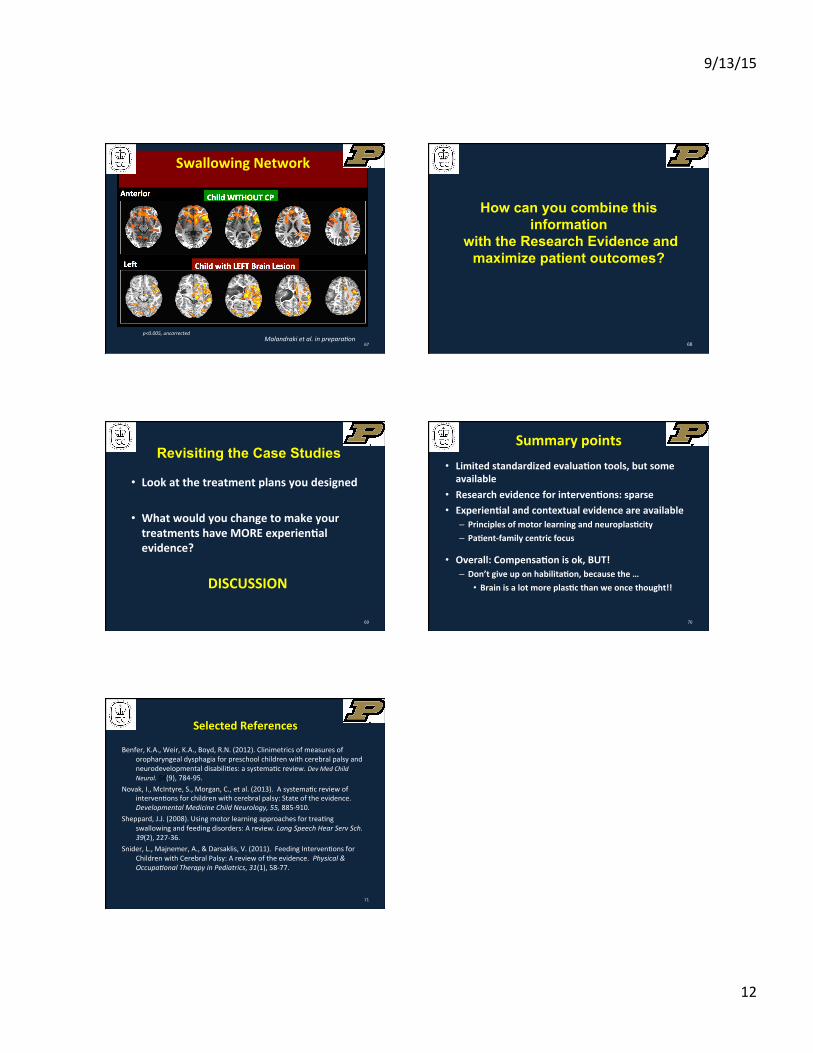
67 Malandraki et al. in prepara2on
Central Plas6city
p<0.005, uncorrected
Swallowing Network
68
How can you combine this information
with the Research Evidence and maximize patient outcomes?
Revisiting the Case Studies
• Look at the treatment plans you designed
• What would you change to make your treatments have MORE experien6al evidence?
DISCUSSION
69
Summary points • Limited standardized evalua6on tools, but some available
• Research evidence for interven6ons: sparse • Experien6al and contextual evidence are available
– Principles of motor learning and neuroplas6city – Pa6ent-‐family centric focus
• Overall: Compensa6on is ok, BUT! – Don’t give up on habilita6on, because the …
• Brain is a lot more plas6c than we once thought!!
70
Selected References
Benfer, K.A., Weir, K.A., Boyd, R.N. (2012). Clinimetrics of measures of oropharyngeal dysphagia for preschool children with cerebral palsy and neurodevelopmental disabili/es: a systema/c review. Dev Med Child Neurol. 54(9), 784-‐95.
Novak, I., McIntyre, S., Morgan, C., et al. (2013). A systema/c review of interven/ons for children with cerebral palsy: State of the evidence. Developmental Medicine Child Neurology, 55, 885-‐910.
Sheppard, J.J. (2008). Using motor learning approaches for trea/ng swallowing and feeding disorders: A review. Lang Speech Hear Serv Sch. 39(2), 227-‐36.
Snider, L., Majnemer, A., & Darsaklis, V. (2011). Feeding Interven/ons for Children with Cerebral Palsy: A review of the evidence. Physical & Occupa2onal Therapy in Pediatrics, 31(1), 58-‐77.
71