Embed Size (px)
Citation preview
1
A . W . F O T H E R G I L L , M A , M B AU N I V E R S I T Y O F T E X A S H E A L T H S C I E N C E C E N T E R
S A N A N T O N I O , T E X A SA S S O C I A T E P R O F E S S O R , D E P A R T M E N T O F P A T H O L O G Y
T E C H N I C A L D I R E C T O R , F U N G U S T E S T I N G L A B O R A T O R Y
1
Interpreting Antifungal Susceptibility Testing:Science or Smoke and Mirrors
Antifungal Pharmacotherapy2
Current options for the treatment of systemic fungal infections are limited
Amphotericin B Nystatin
Fluconazole Itraconazole
Voriconazole Posaconazole
Caspofungin Micafungin
Anidulafungin
Combinations?
Considerable confusion/disagreement regarding appropriate use of these agents
Antifungal Agents3
Amphotericin B
“Standard Therapy” for invasive, life-threatening fungal infections.
Works by attaching to sterols in cell wall
Toxic
Infusion related: chills, fever, headache
Dose-limiting nephrotoxicity
Clinical efficacy poor in some settings
Invasive aspergillosis in immunocompromised
2
Amphotericin B Lipid Formulations4
Chemical Differences from AMB Deoxycholate NONE
Advantages Increased daily dose of parent drug
High tissue concentration
Fewer infusion related side effects
Decreased nephrotoxicity
Disadvantages Superior clinical efficacy not proven
Extremely expensive
Amphotericin B Lipid Formulation Use5
Systemic mycoses, intolerant of or refractory to conventional AMB
Renal dysfunction during treatment (Cr>2.5)
Severe/persistent infusion-related side effects
Disease progression after 500 mg total dose
Typically invasive aspergillosis in patients that are severely immunocompromised
Azoles6
Favorable side effect profile
Act by inhibition of ergosterol synthesis
Ease of administration
Limitations:
Drug interactions
Static rather than cidal activity
Emergence of resistance, even during therapy, especially Candida spp. to FLU
3
Echinocandins7
Favorable side effect profile
Inhibit fungal cell wall synthesis Glucan synthase inhibitors
Broadly active in vitro
Generally well tolerated Warning for co-administration with cyclosporine
FDA approved for aspergillosis and candidiasis, refractory or AMB/ITRA intolerant
Antifungal Susceptibility Testing Methods8
Macrobroth dilution
Microbroth dilution
Disk diffusion
Agar diffusion
Solid agar with wells
CLSI (NCCLS) Publications9
2008 – M27-A3Third edition
2008 – M38-A2Second edition
2004 – M44-AApproved Standard
4
Previous Susceptibility Cutoffs for Candida spp. (µg/ml)
10
S SDD I R NS
5FC <4 -- 8-16 >32 --
FLU <8 16-32 -- >64 --
ITRA <0.125 0.25-0.5 -- >1 --
VORI <1 2 -- >4 --
ANID <2 -- -- -- >2
CAS <2 -- -- -- >2
MICA <2 -- -- -- >2
M27-A3 Approved BreakpointsCandida albicans, C. tropicalis, C. krusei
Time S SDD I R
AMB 24 H -- -- -- --
ANID 24 H <0.25 -- 0.5 >1
CAS 24 H <0.25 -- 0.5 >1
MICA 24 H <0.25 -- 0.5 >1
FLU 24 H <2* 4* -- >8*
POS 24 H -- -- -- --
VORI 24/48 H <0.125 0.25-0.5 -- >1
ITRA 24/48 H -- -- -- --
5FC 24/48 H -- -- -- --
*None for C. krusei
M27-A3 Approved BreakpointsCandida glabrata
Time S SDD I R
AMB 24 H -- -- -- --
ANID 24 H <0.125 -- 0.25 >0.5
CAS 24 H <0.125 -- 0.25 >0.5
MICA 24 H <0.06 -- 0.125 >0.25
FLU 24 H -- <32 -- >64
POS 24 H -- -- -- --
VORI 24/48 H -- -- -- --
ITRA 24/48 H -- -- -- --
5FC 24/48 H -- -- -- --
5
M27-A3 Approved BreakpointsCandida parapsilosis, C. guilliermondii
Time S SDD I R
AMB 24 H -- -- -- --
ANID 24 H <2 -- 4 >8
CAS 24 H <2 -- 4 >8
MICA 24 H <2 -- 4 >8
FLU 24 H <2* 4* -- >8*
POS 24 H -- -- -- --
VORI 24/48 H <0.125* 0.25-0.5* -- >1*
ITRA 24/48 H -- -- -- --
5FC 24/48 H -- -- -- --
*None for C. guilliermondii
Reading MICs14
AMB
No visible growth
Azoles/5FC
80% reduction in turbidity (macro)
50% reduction in turbidity (micro)
100% reduction in turbidity (moulds – ITRA, POSA, VORI)
Echinocandins
50% reduction in turbidity (yeast)
Minimum Effective Concentration (mould)
Macrobroth Procedure15
6
Microtiter Method16
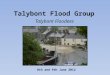
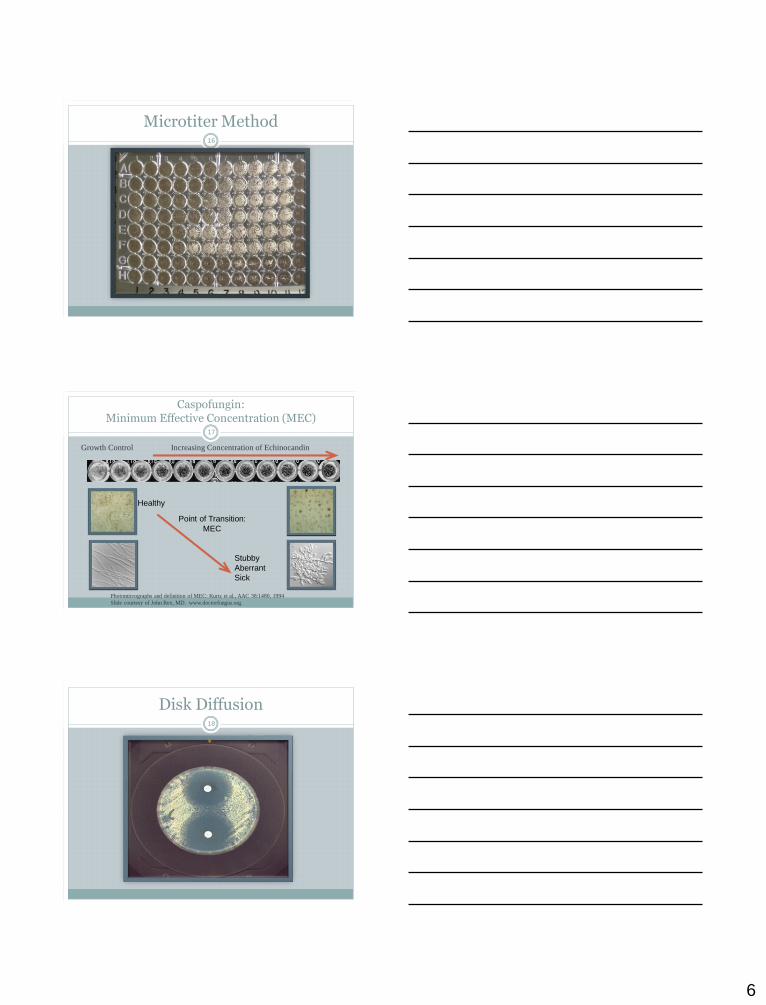
Caspofungin: Minimum Effective Concentration (MEC)
17
Growth Control Increasing Concentration of Echinocandin
Healthy
Stubby
Aberrant
Sick
Point of Transition:
MEC
Photomicrographs and definition of MEC: Kurtz et al., AAC 38:1480, 1994
Slide courtesy of John Rex, MD. www.doctorfungus.org.
Disk Diffusion18
7
NCCLS M44-A19
Provides
Zone interpretive criteria for FLU & VORI
QC ranges for FLU & VORI
R SDD S
FLU 25µg <14mm 15-18mm >19mm
VORI1µg <13mm 14-16mm >17mm
Sensititre Yeast One Panel20
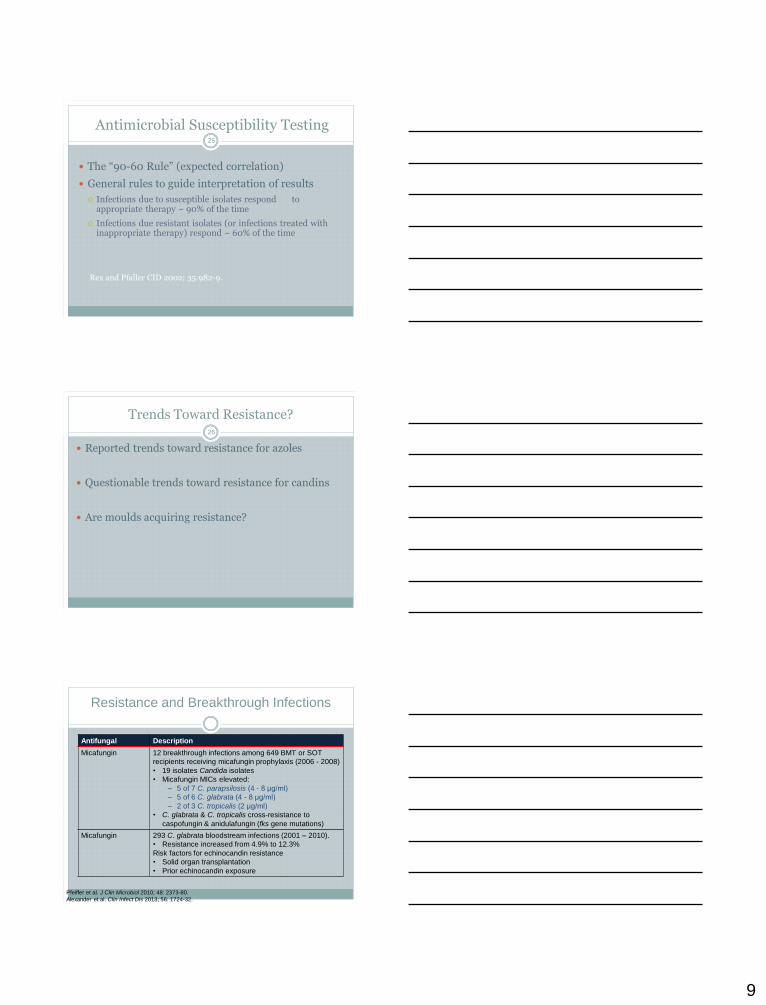
Etest – Technical Manual21
8
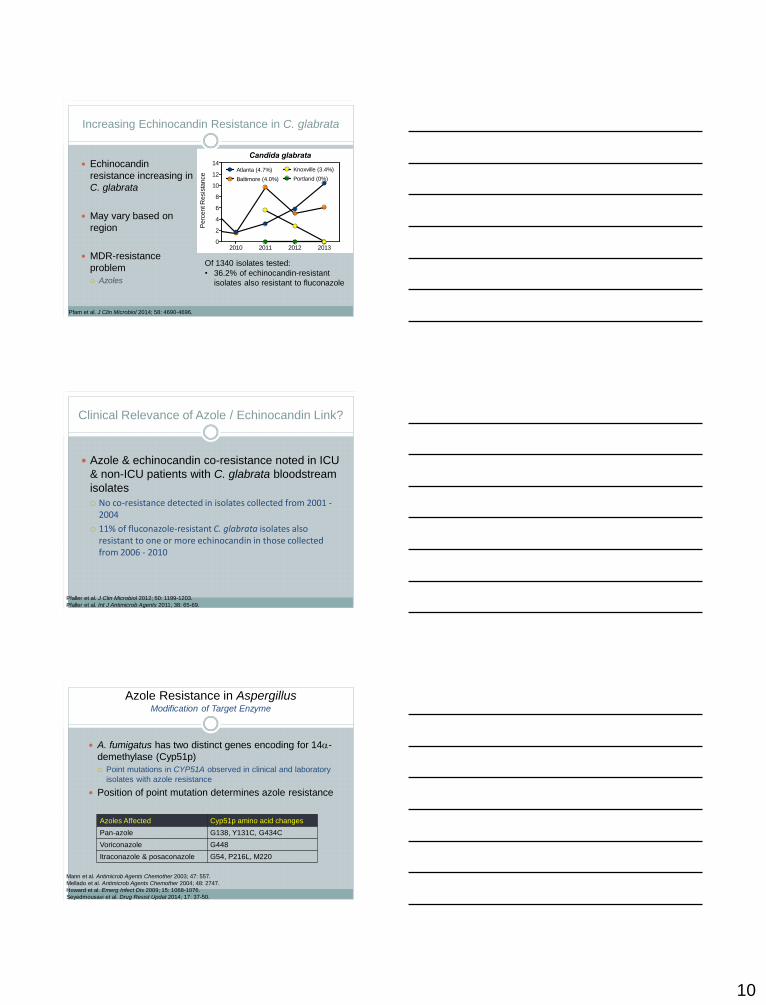
Etest – Technical Manual22
Is Susceptibility Testing a Predictor of Clinical Response?
23
MIC is not a physical or chemical measurement
Dependant upon testing variables
Host factors are more predictive:
Immune response, underlying disease
Drainage/removal of infected foci
Drug level to site of infection
Susceptibility Testing Clinical Utility24
Low MIC does not predict success
High MIC does not predict failure
In vitro resistance may select a population less likely to respond to a particular agent
Other factors (host, drug) are more important as predictors of outcome
Both antibacterial AND antifungal susceptibility
testing share these limitations.
9
Antimicrobial Susceptibility Testing25
The “90-60 Rule” (expected correlation)
General rules to guide interpretation of results
Infections due to susceptible isolates respond to appropriate therapy ~ 90% of the time
Infections due resistant isolates (or infections treated with inappropriate therapy) respond ~ 60% of the time
Rex and Pfaller CID 2002; 35:982-9.
Trends Toward Resistance?26
Reported trends toward resistance for azoles
Questionable trends toward resistance for candins
Are moulds acquiring resistance?
Resistance and Breakthrough Infections
Antifungal Description
Micafungin 12 breakthrough infections among 649 BMT or SOT
recipients receiving micafungin prophylaxis (2006 - 2008)
• 19 isolates Candida isolates
• Micafungin MICs elevated:
‒ 5 of 7 C. parapsilosis (4 - 8 μg/ml)
‒ 5 of 6 C. glabrata (4 - 8 μg/ml)
‒ 2 of 3 C. tropicalis (2 μg/ml)
• C. glabrata & C. tropicalis cross-resistance to
caspofungin & anidulafungin (fks gene mutations)
Micafungin 293 C. glabrata bloodstream infections (2001 – 2010).
• Resistance increased from 4.9% to 12.3%
Risk factors for echinocandin resistance
• Solid organ transplantation
• Prior echinocandin exposure
Pfeiffer et al. J Clin Microbiol 2010; 48: 2373-80.
Alexander et al. Clin Infect Dis 2013; 56: 1724-32.
10
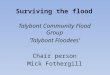
Increasing Echinocandin Resistance in C. glabrata
Echinocandin
resistance increasing in
C. glabrata
May vary based on
region
MDR-resistance
problem
Azoles
Candida glabrata
2010 2011 2012 20130
2
4
6
8
10
12
14
Perc
ent R
esis
tance
Atlanta (4.7%)
Baltimore (4.0%)
Knoxville (3.4%)
Portland (0%)
Of 1340 isolates tested:
• 36.2% of echinocandin-resistant
isolates also resistant to fluconazole
Pfam et al. J Clin Microbiol 2014; 58: 4690-4696.
Clinical Relevance of Azole / Echinocandin Link?
Azole & echinocandin co-resistance noted in ICU
& non-ICU patients with C. glabrata bloodstream
isolates
No co-resistance detected in isolates collected from 2001 -2004
11% of fluconazole-resistant C. glabrata isolates also resistant to one or more echinocandin in those collected from 2006 - 2010
Pfaller et al. J Clin Microbiol 2012; 50: 1199-1203.
Pfaller et al. Int J Antimicrob Agents 2011; 38: 65-69.
Azole Resistance in AspergillusModification of Target Enzyme
A. fumigatus has two distinct genes encoding for 14-
demethylase (Cyp51p)
Point mutations in CYP51A observed in clinical and laboratory
isolates with azole resistance
Position of point mutation determines azole resistance
Mann et al. Antimicrob Agents Chemother 2003; 47: 557.
Mellado et al. Antimicrob Agents Chemother 2004; 48: 2747.
Howard et al. Emerg Infect Dis 2009; 15: 1068-1076.
Seyedmousavi et al. Drug Resist Updat 2014; 17: 37-50.
Azoles Affected Cyp51p amino acid changes
Pan-azole G138, Y131C, G434C
Voriconazole G448
Itraconazole & posaconazole G54, P216L, M220
11
Environmental Exposure to Azoles
Azole-resistant IA identified in patients without prior
azole exposure in parts of Europe
Indoor environment in hospitals & direct proximity to medical centers
Fields where azole fungicides used
Tandem repeat in CYP51A promoter + point
mutation in gene
TR34/L98H
TR46/Y121F/T289A
Snelders et al. Appl Environ Microbiol 2009; 75: 4053-3057. Chowdhary et al. PLoS One 2012; 7: e52871.
van der Linder et al. Clin Infect Dis 2013; 57: 513-520. Chowdhary et al. J Antimicrob Chemother 2014; 69: 555-557.
Chowdhary et al. J Antimicrob Chemother 2014; 69: 69: 2979-2983.
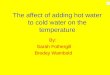
Global Azole ResistanceTR32/L98H & TR46/Y121F/T289A
Belgium, Denmark,
France, Germany,
the Netherlands,
Norway, UK, Spain
Tanzania India
Iran China
Australia
Becoming a global issue
Kuwait
Antifungal Resistance
33
Yeasts Candida krusei fluconazole intrinsic
Candida albicans fluconazole acquired
Candida glabrata fluconazole acquired
Candida albicans caspofungin acquired?
Candida glabrata caspofungin acquired?
Moulds Pseudallescheria boydii amphotericin B intrinsic
Fusarium spp. ALL intrinsic
Paecilomyces lilacinus amphotericin B intrinsic
Aspergillus terreus amphotericin B intrinsic
12
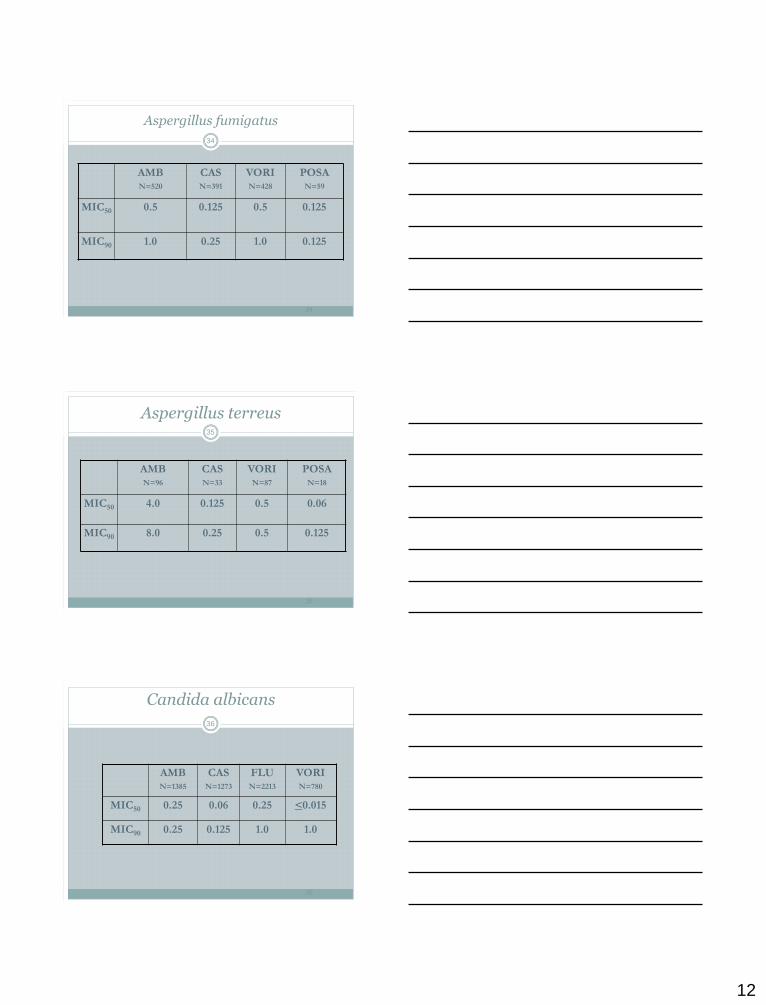
Aspergillus fumigatus
AMBN=520
CASN=391
VORIN=428
POSAN=59
MIC50 0.5 0.125 0.5 0.125
MIC90 1.0 0.25 1.0 0.125
34
34
Aspergillus terreus
AMBN=96
CASN=33
VORIN=87
POSAN=18
MIC50 4.0 0.125 0.5 0.06
MIC90 8.0 0.25 0.5 0.125
35
35
Candida albicans
AMBN=1385
CASN=1273
FLUN=2213
VORIN=780
MIC50 0.25 0.06 0.25 <0.015
MIC90 0.25 0.125 1.0 1.0
36
36
13
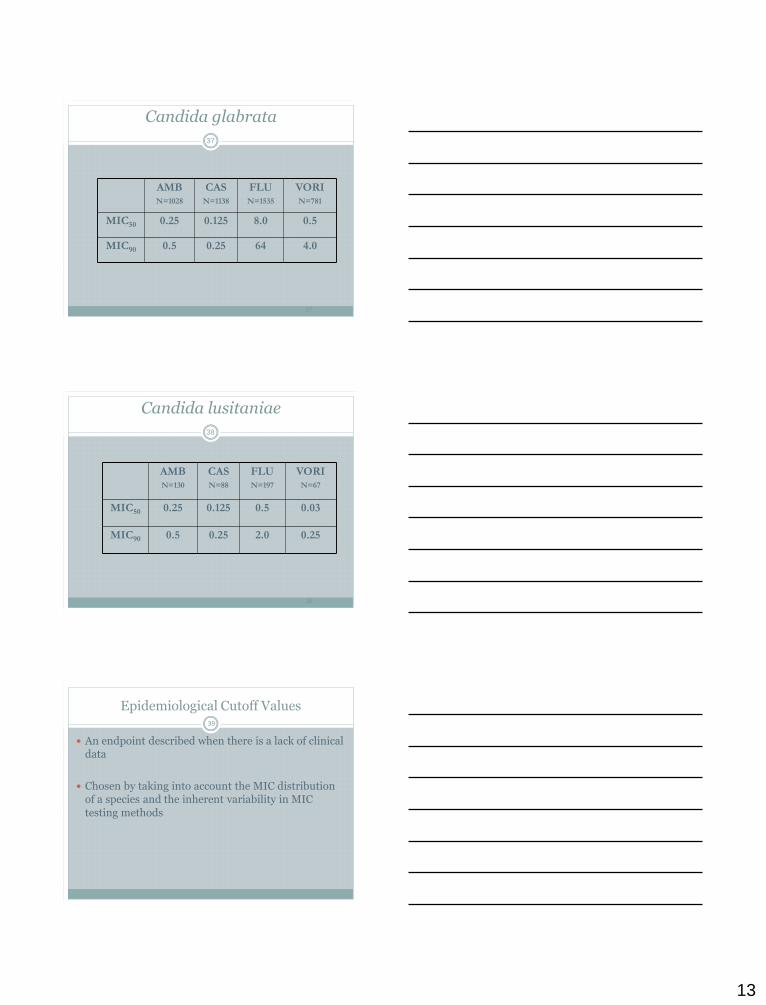
Candida glabrata
AMBN=1028
CASN=1138
FLUN=1535
VORIN=781
MIC50 0.25 0.125 8.0 0.5
MIC90 0.5 0.25 64 4.0
37
37
Candida lusitaniae
AMBN=130
CASN=88
FLUN=197
VORIN=67
MIC50 0.25 0.125 0.5 0.03
MIC90 0.5 0.25 2.0 0.25
38
38
Epidemiological Cutoff Values39
An endpoint described when there is a lack of clinical data
Chosen by taking into account the MIC distribution of a species and the inherent variability in MIC
testing methods
14
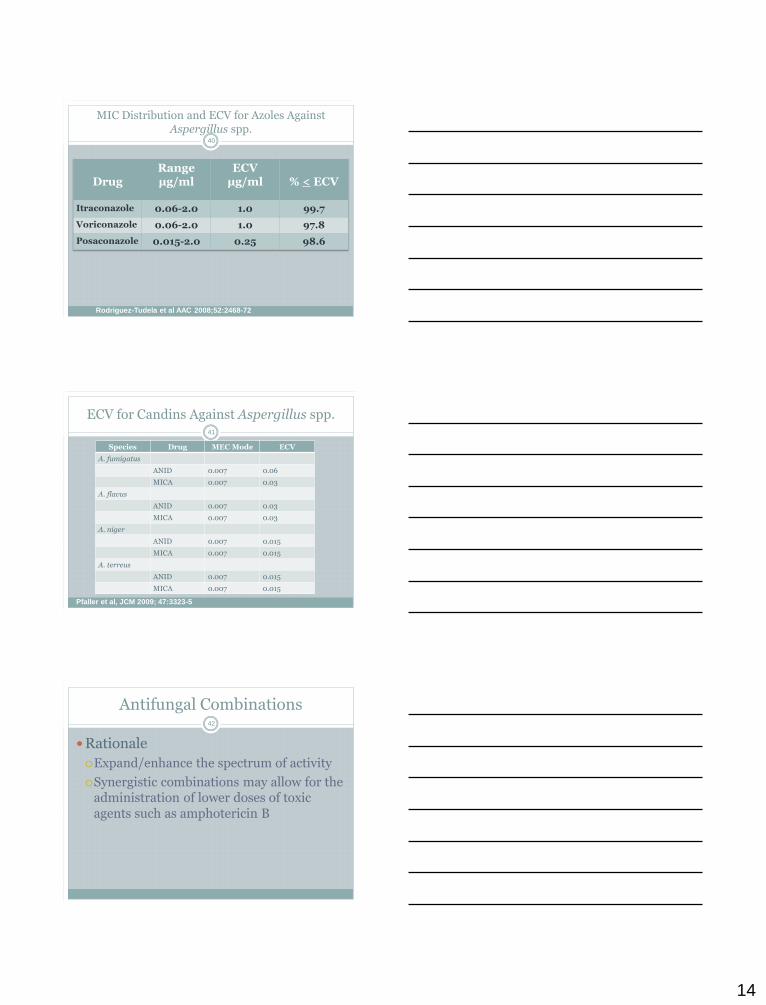
MIC Distribution and ECV for Azoles Against Aspergillus spp.
40
DrugRange µg/ml
ECVµg/ml % < ECV
Itraconazole 0.06-2.0 1.0 99.7
Voriconazole 0.06-2.0 1.0 97.8
Posaconazole 0.015-2.0 0.25 98.6
Rodriguez-Tudela et al AAC 2008;52:2468-72
ECV for Candins Against Aspergillus spp.41
Species Drug MEC Mode ECV
A. fumigatus
ANID 0.007 0.06
MICA 0.007 0.03
A. flavus
ANID 0.007 0.03
MICA 0.007 0.03
A. niger
ANID 0.007 0.015
MICA 0.007 0.015
A. terreus
ANID 0.007 0.015
MICA 0.007 0.015
Pfaller et al, JCM 2009; 47:3323-5
Antifungal Combinations
Rationale
Expand/enhance the spectrum of activity
Synergistic combinations may allow for the administration of lower doses of toxic agents such as amphotericin B
42
15
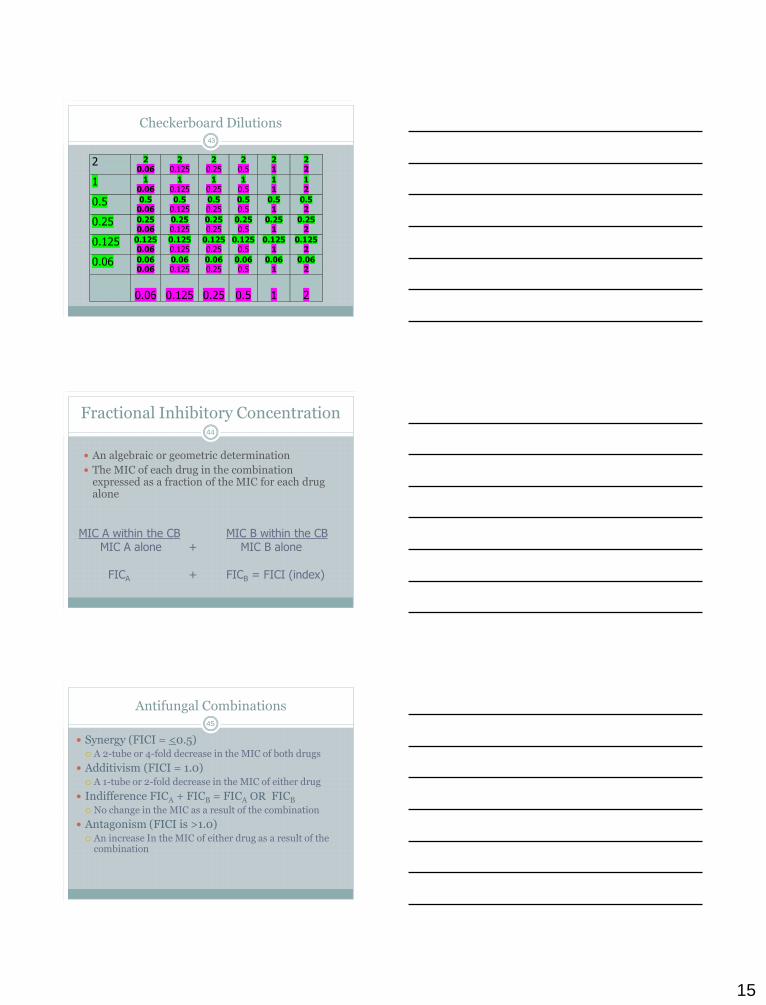
Checkerboard Dilutions
2 2 0.06
2 0.125
2 0.25
2 0.5
2 1
2 2
1 1 0.06
1 0.125
1 0.25
1 0.5
1 1
1 2
0.5 0.5 0.06
0.5 0.125
0.5 0.25
0.5 0.5
0.5 1
0.5 2
0.25 0.25 0.06
0.25 0.125
0.25 0.25
0.25 0.5
0.25 1
0.25 2
0.125 0.125 0.06
0.125 0.125
0.125 0.25
0.125 0.5
0.125 1
0.125 2
0.06 0.06 0.06
0.06 0.125
0.06 0.25
0.06 0.5
0.06 1
0.06 2
0.06
0.125
0.25
0.5
1
2
43
Fractional Inhibitory Concentration
An algebraic or geometric determination
The MIC of each drug in the combination expressed as a fraction of the MIC for each drug alone
MIC A within the CB MIC B within the CBMIC A alone + MIC B alone
FICA + FICB = FICI (index)
44
Antifungal Combinations
Synergy (FICI = <0.5) A 2-tube or 4-fold decrease in the MIC of both drugs
Additivism (FICI = 1.0) A 1-tube or 2-fold decrease in the MIC of either drug
Indifference FICA + FICB = FICA OR FICB
No change in the MIC as a result of the combination
Antagonism (FICI is >1.0) An increase In the MIC of either drug as a result of the
combination
45
16
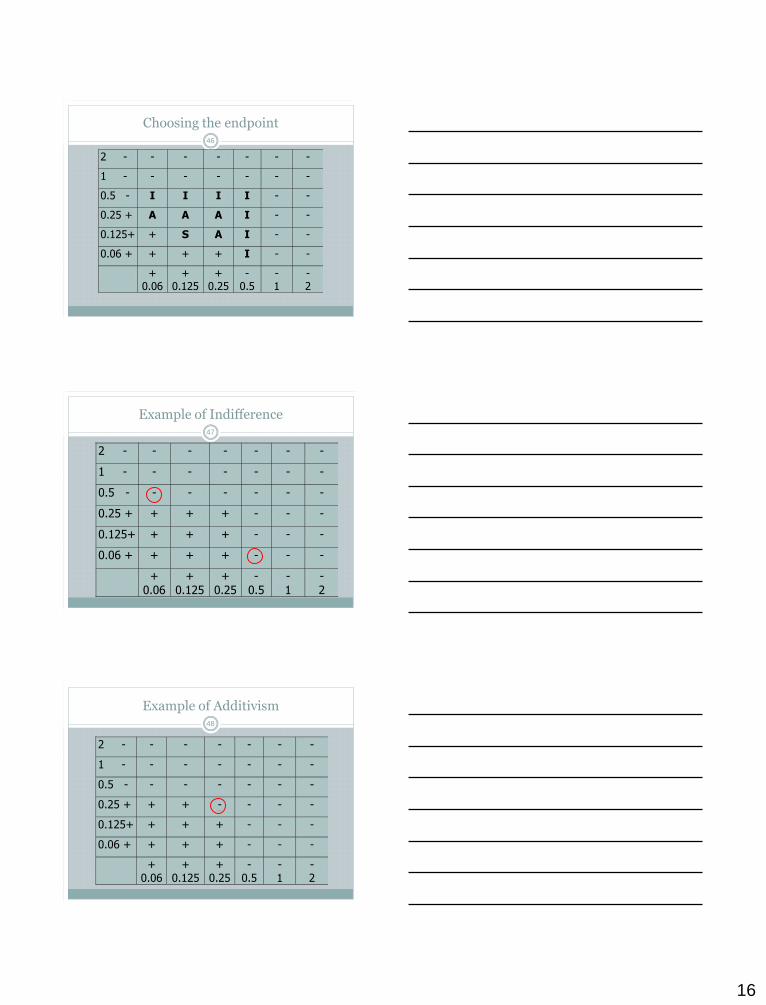
Choosing the endpoint
2 - - - - - - -
1 - - - - - - -
0.5 - I I I I - -
0.25 + A A A I - -
0.125+ + S A I - -
0.06 + + + + I - -
+ 0.06
+ 0.125
+ 0.25
- 0.5
- 1
- 2
46
Example of Indifference
2 - - - - - - -
1 - - - - - - -
0.5 - - - - - - -
0.25 + + + + - - -
0.125+ + + + - - -
0.06 + + + + - - -
+ 0.06
+ 0.125
+ 0.25
- 0.5
- 1
- 2
47
Example of Additivism48
2 - - - - - - -
1 - - - - - - -
0.5 - - - - - - -
0.25 + + + - - - -
0.125+ + + + - - -
0.06 + + + + - - -
+ 0.06
+ 0.125
+ 0.25
- 0.5
- 1
- 2
17
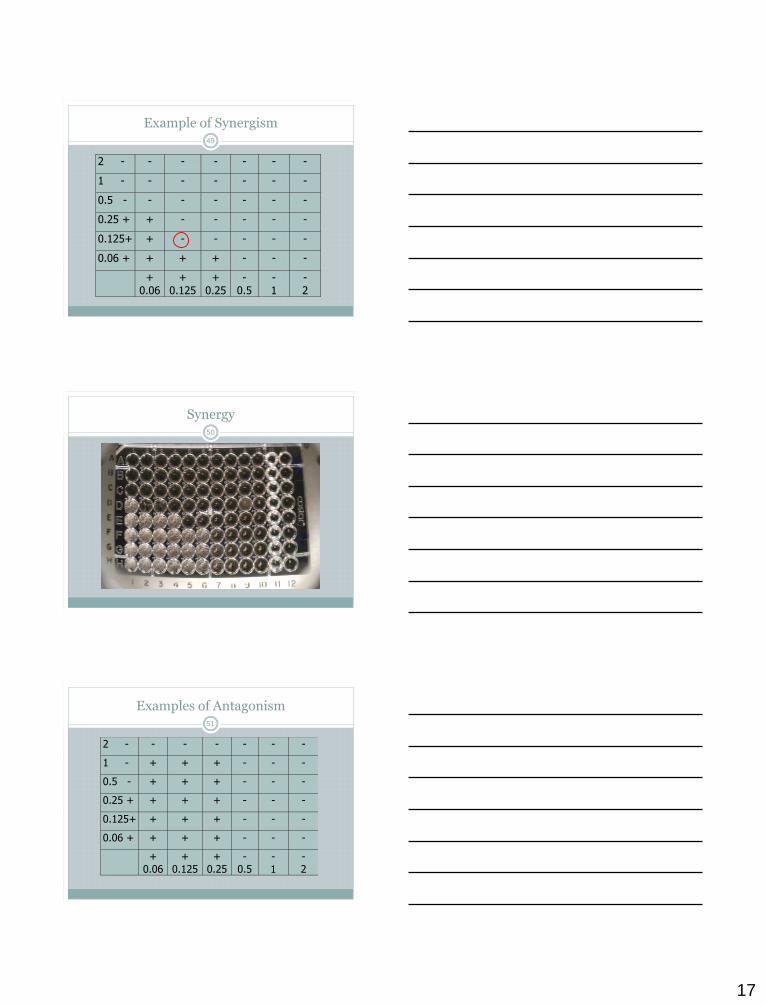
Example of Synergism49
2 - - - - - - -
1 - - - - - - -
0.5 - - - - - - -
0.25 + + - - - - -
0.125+ + - - - - -
0.06 + + + + - - -
+ 0.06
+ 0.125
+ 0.25
- 0.5
- 1
- 2
Synergy50
Examples of Antagonism51
2 - - - - - - -
1 - + + + - - -
0.5 - + + + - - -
0.25 + + + + - - -
0.125+ + + + - - -
0.06 + + + + - - -
+ 0.06
+ 0.125
+ 0.25
- 0.5
- 1
- 2
18
Antagonism52
Antifungal Combinations
Theoretical basis for antagonism:
Azole & polyene
No theoretical basis for antagonism:
Azole & 5FC
Azole & echinocandin
Polyene & 5FC
Polyene & echinocandin
Echinocandin & 5FC
53
Azole-Polyene Interaction
Several recently published studies have reported in vivo antagonism of the fungicidal activity of AMB
when administered concurrently with FLU or ITRA
Sugar et al., JID 1998;177:1660-3
AMB+ITRA against C. albicans
Louie et al., AAC 1999;43:2831-7
Louie et al., AAC 1999;43:2831-40
AMB+FLU against C. albicans
54
19
Azole-Polyene Interaction
Discourage concomitant use of AMB and azole antifungals.
A more rational approach may be to initiate therapy
with AMB and step down to an intravenous or oral azole when appropriate.
55
Summary56
Antifungal Susceptibility testing offers valuable information to assist with making treatment decisions
Trends in resistance remain stable over the last 20 years
New methods may make antifungal susceptibility testing routine in the microbiology laboratory
Questions?57