Embed Size (px)
Citation preview

at SciVerse ScienceDirect
Social Science & Medicine 75 (2012) 1836e1843
Contents lists available
Social Science & Medicine
journal homepage: www.elsevier .com/locate/socscimed
A universal preference for equality in health? Reasons to reconsider propertiesof applied social welfare functions
Ottar Mæstad a,*, Ole Frithjof Norheim b
aChr. Michelsen Institute, Bergen, NorwaybDepartment of Public Health and Primary Health Care, University of Bergen, Norway
a r t i c l e i n f o
Article history:Available online 20 July 2012
Keywords:Health equitySocial welfare functionEliciting preferences
* Corresponding author.E-mail address: [email protected] (O. Mæstad)
0277-9536/$ e see front matter � 2012 Elsevier Ltd.http://dx.doi.org/10.1016/j.socscimed.2012.07.001
a b s t r a c t
The literature on how to combine efficiency and equity considerations in the social valuation of healthallocations has borrowed extensively from applied welfare economics, including the literature oninequality measurement. By so doing, it has adopted normative assumptions that have been applied forevaluating the allocation of welfare (or income) rather than the allocation of health, including theassumption of a monotonically declining social marginal value of welfare/income/health. At the sametime, empirical studies that have elicited social preferences for allocation of health have reported resultsthat are seemingly incompatible with this assumption. There are two ways of addressing this incon-sistency; we may censor the stated preferences by arguing that they cannot be supported by normativearguments, or we may reject or modify the analytical framework in order to accommodate the statedpreferences. We argue that the stated preferences can be supported by normative reasoning andtherefore conclude that one should be cautious in applying the standard welfare economic framework tothe allocation of health.
� 2012 Elsevier Ltd. All rights reserved.
Introduction
An important question in the allocation of scarce resources forhealth is how to balance the goal of achieving a high aggregate levelof health against the aim to distribute health equitably. This classicdilemma is usually referred to as the efficiencyeequity trade-off.Several methods have been suggested for how to deal with thetrade-off in a consistent way in the evaluation of health policies.Common tomost of them are that they borrow heavily fromwelfareeconomics and the literature on measurement of incomeinequality. In this paper we ask whether they have borrowed toomuch. Are there any important differences between the allocationof health and the allocation of welfare or income, with implicationsfor the choice of analytical framework?
Wagstaff, Paci, and van Doorslaer (1991) proposed to representthe efficiencyeequity trade-off in health by an iso-elastic socialwelfare function. This approach dates back to Atkinson (1970), whoused an iso-elastic social welfare function as the theoretical foun-dation for his well-knownmeasure of income inequality. One of theneat properties of the iso-elastic welfare function is that socialpreferences for equality can be summarised in a single parameter,
.
All rights reserved.
the inequality aversion parameter. This property also characterizesthe social welfare functions proposed by Williams (1997), Dolan(1998) and Olsen (1994), as well as Wagstaff’s (2002) achieve-ment index.
A classical social welfare functions approach is currently beingused to represent the efficiencyeequity trade-off in health in theInequality-adjusted Human Development Index (IHDI), first pub-lished in 2010. In the IHDI, the social loss due to inequality in lifeexpectancy is captured by a social welfare function derived fromthe Atkinson measure of inequality, again with a single parameterrepresenting the preferences for equality.
Being able to capture the trade-off between efficiency andequity in a single parameter comes at the cost of reduced flexibility,in the sense that certain preference structures cannot be repre-sented by the proposed social welfare functions. As will bedemonstrated below, one of the implications is that onewill alwaysput a higher social value on health gains to people with a low levelof initial health relative to health gains for personwith higher levelsof health. A second implication is that a given health gain should bedispersed on many rather than concentrated on a few, provided allindividuals are starting from the same initial level of health.
These theoretical properties do not receive unanimous supportin empirical studies of the social preferences for allocation of healthbenefits. For instance, several studies have reported that people

O. Mæstad, O.F. Norheim / Social Science & Medicine 75 (2012) 1836e1843 1837
typically hold the view that society should allocate health gains (inthe form of a larger number of life-years) to patients with inter-mediary life-expectancies rather than to patients with lower life-expectancies (Busschbach, Hessing, & Decharro, 1993; Cropper,Aydede, & Portney, 1994; Mæstad & Norheim, 2009; Ottersen,Mbilinyi, Mæstad, & Norheim, 2007; Rodriguez-Míguez & Pinto,2000; Tsuchiya, 2001; 1 and Tsuchiyaa, Dolan, & Shaw, 2003).Others have suggested that people think social planners shouldconcentrate a given health gain on a few individuals rather than tospread the health gain on a larger number of persons (Olsen, 2000and Rodríguez-Míguez & Pinto-Prades, 2002). These preferencestructures are seemingly incompatible with the structure of thosesocial welfare functions that have been recommended foraddressing the efficiencyeequity trade-off in the evaluation ofhealth programmes.
There are in principle two ways of addressing this incompati-bility. One is to argue that the revealed preferences are not justi-fiable on normative grounds. In this case, one has to examine thereasons behind the stated preferences and assess their normativevalidity. The second alternative, as suggested by Rodríguez-Míguezand Pinto-Prades (2002), is to abandon the standard welfarefunctions and adopt more flexible functional forms which are ableto capture the revealed preference structures.
This paper discusses four reasons why people’s social prefer-ences for the allocation of health do not follow standard welfareeconomic assumptions: 1) non-diminishing marginal utility ofhealth, 2) effects of people’s health on own consumption of non-health goods, 3) effects of people’s health on other’s consumptionof non-health goods, and 3) systematic statistical correlationsbetween the level of health and the level of non-health goods. Weargue that (1), (2), and (3) provide normatively justifiable reasonsfor not necessarily applying the standard welfare economicassumptions to the allocation of health.
Section 2 presents some of the core properties of the socialwelfare functions commonly applied in quantitative analyses of theequityeefficiency trade-off in health. In Section 3, these propertiesare contrasted with empirical results on social preferences forallocation of health. Section 4 presents a set of hypotheses andnormative arguments which may serve to explain and justify theobserved distributional preferences. Conclusions are drawn inSection 5.
Properties of social welfare functions applied to the allocationof health
The social welfare function
A social welfare function characterises the social desirability ofalternative allocations of health. Define a health profile as a partic-ular allocation of health among the members of society. (If hi is thehealth of individual i, the vector (h1,.,hn) is a health profile ina society with a population of n individuals.) A social welfarefunction ranks alternative health profiles in terms of their socialdesirability.
The classical formulation of the social welfare function,following the tradition of Bergson (1938) and Samuelson (1947), isa welfare function with individual welfare (or utility) as its argu-ments. In applied work, however, the sources of individual welfare
1 Cited in Dolan, Shaw, Tsuchiya, and Williams (2005).2 The health related social welfare function has been discussed and/or applied by
for instance Wagstaff et al. (1991), Olsen (1994), Williams (1997), Dolan andRobinson (2001), Abasolo and Tsuchiya (2004), Osterdal (2005), Dolan et al.(2008), Dolan and Tsuchiya (2009, 2011), among others.
(e.g., income and health) have commonly been used as argumentsof the social welfare function. A social welfare function that useshealth as its arguments is known as a health related social welfarefunction (Dolan, 1998).2
An analytical framework that captures both the classical and theapplied approaches can be formulated by letting the social welfarefunction take the following form:
W ¼ Wðuðx1Þ;.;uðxnÞÞ; (1)
where ui ¼ uðxiÞ represents thewelfare of individual i as a functionof (a vector of) valued goods xi (e.g., income, health). In a healthrelatedwelfare function, health is the direct source of social welfare(technically, hi replaces u(xi) as arguments in the social welfarefunction).
In this paper, we will presume that the social welfare function isapplied to a lifetime measure of health.3 Examples of lifetimemeasures of health include the number of life years and the numberof quality adjusted life years (QALYs).
The PigoueDalton transfer principle
A standard assumption in welfare economics is that the socialwelfare function displays a (weak) preference for equality of indi-vidual utilities.4 Economists have usually taken the PigoueDaltontransfer principle as a necessary defining characteristic of anysocial welfare function with preference for equality (Tungodden,2003). The PigoueDalton principle states that a pure transfer ofwelfare from someone with less welfare to someone with morewelfare, without affecting the welfare of anyone else, always mustbe seen as a worsening (Adler, 2012; Foster & Sen, 1997).
When standard welfare functions have been applied to incomeor health, all the properties of the standard welfare functions havebeen retained, except that income or health have replaced indi-vidual utilities as arguments of the welfare functions. This is alsothe case in Wagstaff et al. (1991) iso-elastic welfare function,Williams’ (1997) constant elasticity of substitution (CES) welfarefunction, Dolan’s (1998) CobbeDouglas welfare function, Olsen’s(1994) constant absolute inequality aversion welfare function,and Wagstaff’s (2002) achievement index. By implication, all thesesocial welfare functions satisfy the PigoueDalton principle, appliedto transfers of health among individuals.
Social health weights
One way of expressing the PigoueDalton principle applied tohealth is to say that the social value of health improvements issmaller the higher is the initial level of health, or equivalently, thatthe social weight attached to health improvements decreases withhigher initial levels of health. The following example illustrates thepoint: Consider two health profiles H1 ¼ (31, 59) and H2 ¼ (30, 60).In moving fromH1 toH2, we have effectively transferred one unit ofhealth from the worst off to the better off. According to thePigoueDalton principle, as well as all the welfare functions dis-cussed above, H1 is therefore preferable to H2. This is equivalent tosaying that the one unit of health that was transferred between thetwo has a higher social value when in the hands of the worst offthan when in the hands of the better off. Indeed, any differentiable
3 A social welfare function can also be applied to the sub-lifetime measures ofhealth, i.e., to a vector of health levels representing health in particular period of life(e.g., a year). Such an approach is required in order to put a particular weight on theseverity of disease.
4 The utilitarian welfare function, for instance, exhibits only a weak preferencefor equality of welfare since it is just the sum of individual utilities.

Health
Rank dependent social welfare function (e.g., the achievement index)
Standard social welfare function
Fig. 1. Marginal health weights.
O. Mæstad, O.F. Norheim / Social Science & Medicine 75 (2012) 1836e18431838
social welfare function that satisfies the PigoueDalton principlewill attach a higher weight to health improvements for individualswith low health than to those with higher levels of health.5
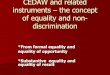
Wagstaff’s achievement index differs from the other socialwelfare functions above in that the weight attached to a person’shealth improvements does not depend directly on that person’slevel of health, but on his/her rank in the health distribution. Thehigher the rank, the lower is the weight attached to healthimprovements. A small health improvement that does not changethe person’s rank in the health distributionwill therefore not causeany change in the weight attached to further health improvements,while a larger health improvement which moves the person toa higher rank will imply a decline in the weight on further healthimprovements. As a consequence, the weights on health improve-ments will decline in a stepwise fashion as the initial level of healthincreases (see Fig. 1 for an illustration).
In the following, we will use the concept marginal health weightto refer to the social value of a small (or marginal) healthimprovement. In general, the marginal health weight on healthimprovements for individual i, wi, will vary with the level of healthhi in accordance with the function
wi ¼ wðhiÞ ¼ vWvui
vuðhiÞvhi
(2)
We call this the marginal weighting function. The equation saysthat the marginal weighting function at any level of hi is equal tothe change in social welfare from a marginal increase in hi. Thissection has demonstrated that the standard social welfare func-tions applied to health imply that the marginal weighting functionis monotonically declining in health (see Fig. 1).6 This property ishowever challenged by the empirical literature on health weights.
The challenge from empirical studies
A few empirical studies have utilised the social welfare func-tions discussed above as a basis for empirical estimation of socialpreferences for allocation of health (examples include Dolan, Edlin,and Tsuchiya (2008), Dolan and Robinson (2001), Dolan andTsuchiya (2011), Johannesson and Gerdtham (1996), and Olsen(1994)). However, most empirical studies have used a non-parametric approach, i.e., preferences structures have been eli-cited without any attempt to make them fit a particular normativetheoretical framework.
The objective of the empirical studies has been to investigate therelationship between the marginal social value of health gains andinitial health levels.7 In practice, the approach has been to measurethe marginal social value of health gains at arbitrary health levels hrelative to the marginal social value of health at a reference level ofhealth hr. What is usually denoted the “health weight” in thisliterature is the relative social marginal value of health gainswðhÞ=wðhrÞ. But since the reference level of health hr is kept
5 Assume that two individuals have health levels h1 < h2 and that a small amountof health Dh is transferred from individual 1 to individual 2. The PigoueDaltonprinciple implies that the initial situation is preferable, i.e.,Wðh1; h2Þ > Wðh1 � Dh; h2 þ DhÞ. Since this relationship also holds for infinites-imal transfers of health, we can differentiate and derive the following condition byimplication; Wðh1; h2Þ > Wðh1; h2Þ þ ð�vW=vh1 þ vW=vh2ÞDh, which furtherimplies that �vW=vh1 þ vW=vh2 < 0. vW/vhi is the marginal social value ofa marginal increase in hi. Hence, the marginal social value of improved health isalways higher for people with low levels of initial health.
6 Formal proofs can be obtained from the authors upon request.7 The distinction between marginal and infra-marginal health gains is however
somewhat blurred in this literature (see Mæstad and Norheim (2009) fora discussion).
constant in the analysis,w(hr) will be a constant, and the propertiesof these “health weights” will be identical to the marginalweighting function w(h) defined above.
Several of the empirical studies cast doubt on the validity ofthe monotonically declining marginal weighting function.Although there is a clear tendency that health gains to individualswith high initial levels of health are valued less than health gainsto individuals with intermediary health levels, the evidence is lessconclusive regarding the marginal weights on health gains toindividuals with intermediary levels of health compared to thosewith low levels of health. Some people appear to hold the viewthat health gains to individuals with low initial levels of healthshould be valued less than health gains to individuals withintermediary levels of health. In particular, this preference patternseems to emerge when the level of health is expressed as the(expected) number of life years (see Busschbach et al., 1993;Cropper et al., 1994; Rodriguez-Míguez & Pinto, 2000; Tsuchiya,2001; Tsuchiyaa et al., 2003 and Ottersen et al., 2007). This pref-erence structure implies that the marginal weighting function ishump-shaped, i.e., the marginal health weights are increasing inthe level of health at low levels of health and decreasing in thelevel of health at higher health levels e which is in conflict witha direct application of the PigoueDalton principle in the healthspace.8
A hump-shaped marginal weighting function of this kind isincorporated into the DALY measure of health through the use ofage weights. The DALY age weighting function takes the formaxe�bx, where x denotes age and a and b are constants (Murray &Acharya, 1997). Fig. 2 provides a graphical illustration for the casea ¼ .1 and b ¼ .033. One interpretation of the DALY age weights isthat the value of a marginal increase in the number of life years ishigher at intermediary ages.9
Another strand of the empirical literature has arrived at similarconclusions by investigating people’s preferences for dispersionversus concentration of health gains. Rodríguez-Míguez andPinto-Prades (2002) estimated the social value of giving extralife years to people of age 20 and then fitted their data to a non-
8 See Amiel and Cowell (1999) for a discussion of whether individuals satisfy thePigoueDalton principle in their ranking of income distributions. See Kaplow (2010)for a discussion of the hazards of using a social welfare function applied directly toan attribute such as income (or health) rather than to utility as a function ofattributes.
9 If health were measured as the number of life years, the DALY age weightswould be equivalent to our concept of a marginal weighting function of health. Butsince the DALY concept of health adjusts the value of life years with disabilityweights, the correspondence is somewhat less clear-cut. Nevertheless, the impliedproblems for the use of standard social welfare functions in makingequityeefficiency trade-offs remain the same.

0
0.2
0.4
0.6
0.8
1
1.2
1.4
0 5 10 15 20 25 30 35 40 45 50
Life years beyond 20 years
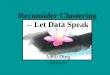
Fig. 3. Marginal weights for additional life years beyond 20 years, calculated fromRodríguez-Míguez and Pinto-Prades (2002).
0.0
0.2
0.4
0.6
0.8
1.0
1.2
0 10 20 30 40 50 60 70 80Age
Fig. 2. DALY age weights.
11 This idea is related to the concept of ALP (Acquisition of Life Potential), whichhas been used in the discussion of the moral status of embryos and fetuses (e.g.,Steinbock, 1992). Dworkin (1993), following a similar line of reasoning, argues thata premature death for an adolescent is a greater tragedy than the death of an infant.This view seems to imply, at least within our analytical framework, that the socialvalue of the first years of life is negative, which is a far more extreme position than
O. Mæstad, O.F. Norheim / Social Science & Medicine 75 (2012) 1836e1843 1839
standard social welfare function. Their estimated marginalweighting function for additional life years beyond 20 years isdisplayed in Fig. 3.10
The pattern reported in Fig. 3 is consistent with age weightswitha peak around age 30. But it is also possible, as claimed byRodriguez-Miguez and Pinto-Prades, that their results reveala more general preference for concentration rather than dispersionof small health gains. In that case, the same pattern should beobserved irrespective of the initial level of health. Olsen (2000), ina study where initial health levels were not conveyed, found that21% of his sample preferred a programme that increased life-expectancy by 20 years in five people over a programme thatincrease life-expectancy by one year in 100 people. Similarly toRodriguez-Miguez and Pinto-Prades, he suggested that there maybe a threshold level of health gains, below which people prefer toconcentrate health gains. However, it is also possible to interpretthese findings as age weights with a peak at intermediary ages,noting that “intermediary” here should be understood in relation tothe respondents’ implicit assumptions about initial life-expectancies.
In light of these empirical findings, there seems to be a need toreconsider the normative justification of the standard socialwelfare functions for addressing the efficiencyeequity trade-off inthe allocation of health. We now turn to a discussion of the possiblenormative reasons behind the elicited social preferences and askwhether these reasons are strong enough to abandon or modify thestandard welfare economic approach.
Can empirical results be justified by valid normativearguments?
Social preferences over the allocation of health should bejustified by acceptable normative arguments. In Sections 4.1 and4.2 we present two normative arguments why a social welfarefunction over the allocation of health should not necessarily beexpected to conform to the PigoueDalton principle. Both reasonsrelate to particular aspects of the transformation of health intoindividual utility. We will not question the appropriateness of thePigoueDalton principle in the welfare space, i.e., concerning theallocation of utilities among individuals. It is only theapplication of this principle in the health space that is up fordiscussion. In Section 4.3, we discuss the possibility that thefindings in the empirical literature could be the result of somekind of omitted variable bias, but we argue that this is not a likelyexplanation.
Before turning to the normative discussion, note that there aredifferent interpretations of what it means to apply the social
10 Their welfare function takes the following form: DW ¼ P
ie�0:026DhiDh1:435i
welfare function directly to individual health utilities, i.e., to workdirectly in the health space. One interpretation is that all non-health factors that generate well-being (e.g., income) are heldfixed. A different interpretation is that non-health factors, albeit notexplicitly described, are understood to vary along with health, inaccordance with standard, empirical correlations. The latter inter-pretation is the basis for the discussion in Sections 4.2 and 4.3,while the argument in Section 4.1 is relevant to either to the twointerpretations.
Since most of the empirical studies referred to above measurehealth in terms of number of life years, this definition of health willbe the basis for our discussions below, although the normativearguments are also valid for other lifetime measures of health.Some of the arguments may however be less plausible if health isdefined more broadly (see Sections 4.1 and 4.2).
Better life years
It is not uncommon to hear people talk about persons who are“in their best years of life”. Reference is then usually made toadulthood, not childhood. Such statements seem to presume thatthere is a period somewhere around the middle of life where eachlife year produces higher well-being than life years at earlier andlater stages of life. We call this the better life years argument.
“Old age will not come alone”, says a Welsh proverb whichseems to capture, at least partly, the idea behind the better life yearsargument. Extra life years usually come together with some kind ofpersonal development e some physical and mental changes. At oldage, the changes often reduce our ability to enjoy life and thedifferent non-health sources of well-being. The opposite is the caseat young age; the increase in awareness and other mental andphysical capabilities will then enable gradually greater enjoymentof life and the goods that follow with it.11
One implication of the better life years argument is thata person’s well-being gain (or utility gain) from one extra life year
we put forth here (see also Persad et al., 2009). There is however no consensusabout this view in the normative literature (e.g., Kerstein & Bognar, 2010). See alsoJamison, Shahid-Salles, Jamison, Lawn, and Zupan (2006).

O. Mæstad, O.F. Norheim / Social Science & Medicine 75 (2012) 1836e18431840
increases with the initial number of life years when the initialnumber of life years is low. In other words, a person’s marginalutility of health is increasing at low levels of health.
The fact that health in the form of extra life years inevitablycomes together with some kind of personal development, makeshealth different from other goods, such as income. This may explainwhy increasing marginal utility of health in some instances may bea reasonable idea despite the widely held assumption ofa decreasing marginal utility of income.
If the marginal utility of health is first increasing and thendecreasing, the result may be a hump-shaped marginal weightingfunction. Fig. 4a and b illustrate. Fig. 4a displays a utility functionwith increasing marginal utility of health at low levels of health anddecreasing marginal utility of health at higher health levels(graphically, the marginal utility of health equals the slope of theutility function.) The shape of the marginal utility of health curve isshown as the solid line in Fig. 4b. Hence, the better life yearsargument implies a hump-shaped individual marginal utility curve.
A hump-shaped individual marginal utility curve does notnecessarily imply a hump-shaped marginal weighting function,though. Moving from the individual utility function to the socialwelfare function involves an additional level of transformation. Wehave argued that the transformation of individual utilities to socialwelfare should satisfy the PigoueDalton principle, which impliesthat utility gains at low levels of utility (which here correspond tolow levels of health) should receive higher weight than utility gainsat higher levels of utility. Such a transformation is illustrated inFig. 4b by the social marginal value of health curve, which is tiltedclockwise compared to the individual marginal utility curve,reflecting that a relatively high social value is placed on healthimprovements at low initial levels of health.
In the figure, the social marginal value of health, which isequivalent to the marginal weighting function, is hump-shaped.This illustrates that the better life years argument indeed isa possible explanation for the hump-shaped marginal weightingfunction. But it is also possible, if social preferences for equality ofwelfare are strong enough, that the social marginal value of healthcurve may be tilted so much that is becomes monotonicallydownward sloping, even though the individual marginal utility isincreasing in health. The better life years argument is thus nota sufficient condition for a hump-shaped marginal weightingfunction; at the same time the social preference for equality ofwelfare must not be too strong.
Hence, if we accept the better life years argument, there is noreason to object to the hump-shaped marginal weighting functionsin the health space. As long as we are working in the health space,
AHealth ( ih )
Utility, )( ihu
a
Fig. 4. a. The individual utility of health. b. The individual m
therefore, we ought to work with analytical frameworks that areable to accommodate the hump-shaped weighting structure (seeAppendix A.1 for a formal exposition).
Note that, in principle, the aspects related to the better lifeyears argument, such as personal development and capacity toenjoy life, can be incorporated into the very measure of health,thus obviating the need to take this aspect into account in thefunctional form of the social welfare function. However, as long aswe are working with life years and other health measures that donot (fully) take these considerations into account, there is a needto critically reflect on the functional form of the social welfarefunction.
Welfare interdependence and welfare intradependence
Another possible reason underlying the findings in the empiricalliterature is that health improvements for some individuals mayhave positive impacts on the utility of others (welfare interdepen-dence) and that respondents think that extra life years for peoplewith an intermediary number of initial life years systematicallygenerate larger positive externalities than similar health improve-ments for other groups. For example, some have argued that peoplein their middle ages play a particularly important role in society,e.g., as caretakers for children and elderly parents, and that healthimprovements for this segment of the population therefore shouldbe assigned a relatively high social value. High economic produc-tivity e which also may raise the utility of others through the taxsystem or other transfer mechanisms e is another argument thatmay lead to the same conclusion (Murray, 1996; Murray & Acharya,1997). Judgements of this kind may explain a hump-shapedmarginal weighting function in the health space, especially whenhealth is measured as the number of life years.
The underlying premise of the welfare interdependence argu-ment is that better health for somewill make them produce certainnon-health goods that are valued by others. It is possible to makea parallel argument based on the obvious fact that these goods alsomay be valuable to themselves; better health for me makes me ableto generate more income and other non-health goods that benefitme. This may be called welfare intradependence; a person’sconsumption of non-health goods depends on his level of health.(Note the difference compared to the better life years argumentwhich is applicable also when the amount of non-health goodsremain constant.) Technically speaking, there is no fundamentaldifference between welfare inter- and intradependence. Both mayresult in a hump-shaped marginal weighting function (SeeAppendix A.2 for a formal exposition).
Socialmarginalvalue
A
Individual marginal utility
Health ( ih )
b
arginal utility and the social marginal value of health.

O. Mæstad, O.F. Norheim / Social Science & Medicine 75 (2012) 1836e1843 1841
An important counterargument that has been raised against thewelfare interdependence argument e and is relevant also to thewelfare intradependence argument e is that it may lead todiscrimination based on morally irrelevant factors. For instance, itmay be argued that economic productivity depends to a large degreeon talent and other factors beyond individual control, and for whichindividuals should not be held morally responsible. Similarly,whether or not a particular individual becomes a parent alsodepends on genes and other factors beyond individual control.12
These are all arguments against applying the welfare interde-pendence argument (and intradependence argument) directly to theallocation of health across particular individuals. Even if we acceptthese objections, we may still accept a non-discriminatory welfareinterdependence argument; that the social value of health gainsshould be identical for all individuals with the same initial healthlevel, at the same time as the social value of health gains may varysystematically across health levels due to the associationbetween thelevel of health and the impact of improved health on the amount ofnon-health goods. This is all that is needed to justify the hump-shaped marginal weighting function in the health space. If health ismeasured as the number of life years, the non-discriminatorywelfareinterdependence argument implies that the weight attached to anadditional life year should be identical for all individuals with thesame number of life years, whereas the weights may differ acrosspeoplewith different number of life years due to systematic variationin the impact of health on the generation of non-health goods. Thesame reasoning applies to the welfare intradependence argument.
The objections against the welfare inter- and intradependencearguments may be stronger if health is not measured as life years.Letting marginal health weights depend on life years can be said tobe non-discriminatory because everyone who is alive will follow thesame path of life years. With other measures of health, it may be lessclear that this kind of differentiation of marginal health weights iscompletely non-discriminatory, even though the weights are thesame for all individuals with the same level of health.
One principal difference between welfare interdependence andwelfare intradependence is that the latter concerns the instru-mental effect of health in people’s own lives, whereas the formerconcerns the instrumental effect of health on other people’s lives. Itis uncontroversial to acknowledge the instrumental effect of healthin people’s own lives. Health in the form of extra life years is valued,at least partly, because of the added opportunities for enjoyingother goods. Health in the form of ability to hear, see or walk makesother goods more valuable and enhances welfare. We will arguethat if one acknowledges the instrumental value of health inpeople’s own life, it would be inconsistent not to acknowledge theinstrumental value of health in other people’s lives. Hence, thereappears to be a firm normative basis for applying the non-discriminatory welfare interdependence arguments e along witha non-discriminatory welfare intradependence argument e indiscussions about the social valuation of health, especially whenhealth is measured as life years.
We conclude that the welfare inter- and intradependencearguments are supported by sufficiently strong normative argu-ments to make them acceptable reasons for a hump-shapedmarginal health weighting function.
A more difficult question is whether there are morally relevantdifferences between different types of non-health impacts. Forexample, is there a difference between the fact that people in theirmiddle ages play an important role as caretakers for children andthe fact that they on average are economically more productive
12 See Fleurbaey (2008) for a comprehensive discussion of the importance ofresponsibility in relation to distributive justice.
than others? And how should any such difference be taken intoaccount in the social welfare function? The answers to thesequestions are not essential to our argument here, and we thereforeleave these issues for future work.
Healthy, but worse off?
The discussion above presumed that health is instrumental ingenerating non-health goods, implying a positive correlationbetween the level of health and the amount of non-health goods. Itis also possible, at least in theory, that health is systematicallynegatively correlated with the amount of (some) non-health goods.This could lead to a hump-shapedmarginal weighting function (seeAppendix A.3). If it were a statistical fact that more healthy peoplealso are worse off, all factors considered, then the respondents inempirical studies would have a reason to put lower weight onhealth improvements for people with poor health than for peoplewith better health.
Bleichrodt and van Doorslaer (2006) argue that the possibility ofsuch statistical correlations is a reason to question the applicationof the standard measures of inequality for the measurement ofhealth inequalities. We strongly doubt, however, that these asso-ciations explain the hump-shaped weighting functions. As arguedby Asada (2006), poor health likely goes together with low levels ofother valued variables. This may have an impact on the healthweights but will most likely not produce a hump-shaped weightingfunction (see Appendix A.3 for a formal exposition).
Conclusions
We have pointed out that the social welfare functions thatcommonly have been applied to represent the efficiencyeequitytrade-off in the allocation of health imply that the social value ofhealth improvements is declining in the initial level of health. Thisis a direct implication of applying the PigoueDalton principledirectly to the allocation of health.
A number of empirical studies have elicited social preferences forthe allocationof health that violate this property. Inparticular, studiesthat have measured health as number of life years (or similar) havefound that the social value of marginal health improvements may beincreasing in health at low levels of initial health.
We have discussed four possible reasons for the observedempirical results. Three normative arguments, the better life yearsargument, the welfare interdependence argument, and the welfareintradependence argument suggest that the empirical findings canbe supported by valid normative reasons.
We conclude that care should be taken in applying standardwelfare functions to the health space, in particular when workingwith lifetime measures of health such as the number of (expected)life years. In this case, more flexible functional forms that are betterable to capture the elicited social preferences might be appropriate.
Acknowledgements
We are grateful to Ivar Kolstad, Bertil Tungodden, two anony-mous referees, and to participants at the international workshop onPriority Setting in Health, Arusha, Tanzania, June 2009, for usefulcomments and suggestions. Financial support from the ResearchCouncil of Norway and from the Human Rights Programme at Chr.Michelsen Institute is gratefully acknowledged.
Appendix A.1
The better years argument can be formulated formally asfollows: From Eq. (2) we have that the marginal weighting function

O. Mæstad, O.F. Norheim / Social Science & Medicine 75 (2012) 1836e18431842
is upward sloping (i.e., vw/vhi > 0) if and only ifðu0ðhiÞÞ2v2W=vu2i þ u00ðhiÞvW=vui > 0. With a social preference forequality of welfare ðv2W=vu2i < 0Þ and a positive marginal utility ofhealth ðu0ðhiÞ > 0Þ, a necessary condition for an upward slopingmarginal weighting function is that u00ðhiÞ > 0. When health ismeasure as life years u00ðhiÞ > 0 is equivalent to subsequent lifeyears becoming “better and better”. Hence, if the better years arenot the first years of life and the social preference for equality ofwelfare is not too strong, the marginal weighting function will beupward sloping at low levels of health.
Appendix A.2
To show that welfare interdependence and welfare intra-dependence can result in an upward sloping marginal weightingfunction, assume there are two individuals i and j, and that i’s utilityfunctions takes the form ui ¼ uðhi; xiðhi;hjÞÞ, where xi is a non-health good which becomes available in higher quantities if thehealth of individual j (hj) improves (welfare interdependence) and/or if own health (hi) improves (welfare intradependence). Similarly,the utility function of individual j is uj ¼ uðhj; xjðhj;hiÞÞ.
Consider first the situation with only welfare interdependenceand no welfare intradependence (i.e., vxi=vhi ¼ vxj=vhj ¼ 0). Themarginal weighting function (evaluated at hi) is then wðhiÞ ¼ððvW=vuiÞðvui=vhiÞÞ þ ððvW=vujÞðvuj=vxjÞðvxj=vhiÞÞ. Assuming thatthere are no better (nor worse) life years arguments e becauseindividual welfare is linear in its arguments e the slope of themarginal weighting function is w0ðhiÞ ¼ ððv2W=vu2i Þðvui=vhiÞÞþððv2W=vu2j Þðvuj=vxjÞðvxj=vhiÞÞ þ ðvW=vujÞðvuj=vxjÞ ðv2xj=vh2i Þ. Thewelfare interdependence argument is captured by the last term,which is positive if v2xj=vh2i > 0, i.e., when the impact of i’s health onj’s consumption of non-health goods increases with the level of j’shealth. Note that the first two terms are negative due to the socialpreference for equality ofwelfare. Hence, a hump-shapedweightingfunction requires both that the welfare interdependence effectincreaseswith the level ofhealth at certainhealth levels and that thiseffect more than outweighs the effect on the marginal weightingfunction of the social preference for equality of welfare.
Consider next the case of welfare intradependence (whileassuming vxi=vhj ¼ vxj=vhi ¼ 0). The marginal weighting function(evaluated at hi) is then given by wðhiÞ ¼ vW=vuiððvui=vhiÞþððvui=vxiÞðvxi=vhiÞÞÞ. Assuming again that individual welfare islinear in its arguments, the slope of themarginalweighting functionis w0ðhiÞ ¼ v2W=vuiððvui=vhiÞ þððvui=vxiÞðvxi=vhiÞÞÞþ ððvW=vuiÞðvui=vxiÞðv2xi=vhiÞÞ. The welfare intradependence argument iscaptured by the last term, similarly to above. Again, a hump-shapedweighting function requires both that the welfare intradependenceeffect increases with the level of health at certain health levels andthat this effect more than outweighs the effect on the marginalweighting function of the social preference for equality of welfare.
Appendix A.3
Let individual utility be u(hi, xi), where xi is a non-health good.Assume that there is an empirical relationship between the level ofxi and the level of hi, given by xi ¼ bhi þ εi, where b is a constantand εi is random noise. If respondents take the correlation betweenxi and hi into account when they calculate the marginal utility ofhealth, the marginal weighting function will be wðhiÞ ¼ vW=vuiððvui=vhiÞ þ ððvui=vxiÞbÞÞ. The slope of the marginal weightingfunction, assuming again that individual welfare is linear in itsarguments, is wðhiÞ ¼ v2W=vuiððvui=vhiÞ þ ððvui=vxiÞbÞÞ. The termin brackets will be negative if there is a strong negative relationshipbetween xi and hi, i.e., if b < �ððvui=vhiÞ=ðvui=vxiÞÞ. In this case,
higher levels of health are associated with lower individual welfaredue to the negative statistical correlation between health and non-health goods. The marginal weighting functionwill then be upwardsloping in health.
References
Abasolo, I., & Tsuchiya, A. (2004). Exploring social welfare functions and violation ofmonotonicity: an example from inequalities in health. Journal of HealthEconomics, 23, 313e329.
Adler, M. D. (2012). Well-being and fair distribution: Beyond cost-benefit analysis.Oxford University Press.
Amiel, Y., & Cowell, F. A. (1999). Thinking about inequality: Personal judgment andincome distributions. Cambridge University Press.
Asada, Y. (2006). Is health inequality across individuals of moral concern? HealthCare Analysis, 14, 25e36.
Atkinson, A. (1970). On the measurement of inequality. Journal of Economic Theory,2, 244e263.
Bergson, A. (1938). A reformulation of certain aspects of welfare economics.Quarterly Journal of Economics, 52, 310e334.
Bleichrodt, H., & van Doorslaer, E. (2006). A welfare economics foundation forhealth inequality measurement. Journal of Health Economics, 25, 945e957.
Busschbach, J. J. V., Hessing, D. J., & Decharro, F. T. (1993). The utility of health atdifferent stages in life e a quantitative approach. Social Science & Medicine, 37,153e158.
Cropper, M. L., Aydede, S. K., & Portney, P. R. (1994). Preferences for life savingprograms e how the public discounts time and age. Journal of Risk and Uncer-tainty, 8, 243e265.
Dolan, P. (1998). The measurement of individual utility and social welfare. Journal ofHealth Economics, 17, 39e52.
Dolan, P., Edlin, R., & Tsuchiya, A. (2008). The relative societal value of health gains todifferent beneficiaries. Health Economics and Decision Science Discussion PaperSeries no 08/12. University of Sheffield.
Dolan, P., & Robinson, A. (2001). The measurement of preferences over the distri-bution of benefits: the importance of the reference point. European EconomicReview, 45, 1687e1709.
Dolan, P., Shaw, R., Tsuchiya, A., & Williams, A. (2005). QALY maximisation andpeople’s preferences: a methodological review of the literature. HealthEconomics, 14, 197e208.
Dolan, P., & Tsuchiya, A. (2009). The social welfare function and individualresponsibility: some theoretical issues and empirical evidence. Journal of HealthEconomics, 28, 210e220.
Dolan, P., & Tsuchiya, A. (2011). Determining the parameters in a social welfarefunction using stated preference data: an application to health. AppliedEconomics, 43, 2241e2250.
Dworkin, R. (1993). Life’s dominion. An argument about abortion, euthanasia, andindividual freedom. New York: Knopf.
Fleurbaey, M. (2008). Fairness, responsibility, and welfare. Oxford: Oxford UniversityPress.
Foster, J., & Sen, A. (1997). On economic inequality. Oxford: Clarendon Press.Jamison, D., Shahid-Salles, S. A., Jamison, J., Lawn, J. E., & Zupan, J. (2006). Incorpo-
rating deaths near the time of birth into estimates of the global burden of disease.In A. D. Lopez, C. Mathers, M. Ezzati, D. T. Jamison, & C. J. L. Murray (Eds.), Globalburden of disease and the risk factors. New York: Oxford University Press.
Johannesson, M., & Gerdtham, U.-G. (1996). A note on the estimation of the equity-efficiency trade-off for QALYs. Journal of Health Economics, 15, 359e368.
Kaplow, L. (2010). Concavity of utility, concavity of welfare, and redistribution ofincome. International Tax and Public Finance, 17, 25e42.
Kerstein, S. J., & Bognar, G. (2010). Complete lives in the balance. The AmericanJournal of Bioethics, 10(4), 37e45.
Mæstad, O., & Norheim, O. F. (2009). Eliciting people’s preferences for the distri-bution of health. A procedure for a more precise estimation of distributionalweights. Journal of Health Economics, 28, 570e577.
Murray, C. J. L. (1996). Rethinking DALYs. In C. J. L. Murray, & A. D. Lopez (Eds.), Theglobal burden of disease. Cambridge, MA: Harvard University Press.
Murray, C. J. L., & Acharya, A. K. (1997). Understanding DALYs. Journal of HealthEconomics, 16, 703e730.
Olsen, J. A. (1994). Persons vs years: two ways of eliciting implicit weights. HealthEconomics, 3, 39e46.
Olsen, J. A. (2000). A note on eliciting distributive preferences for health. Journal ofHealth Economics, 19, 541e550.
Osterdal, L. P. (2005). Axioms for health care resource allocation. Journal of HealthEconomics, 24, 679e702.
Ottersen,T.,Mbilinyi,D.,Mæstad,O.,&Norheim,O.F. (2007).Distributionmatters:equityconsiderations among health planners in Tanzania. Health Policy, 85, 218e227.
Persad, G., Wertheimer, A., et al. (2009). Principles for allocation of scarce medicalinterventions. The Lancet, 373(9661), 423e431.
Rodriguez-Míguez, E., & Pinto, J. L. (2000). The social value of health programmes: isage a relevant factor? Health Economics, 9, 611e621.
Rodríguez-Míguez, E., & Pinto-Prades, J. L. (2002). Measuring the social importance ofconcentrationordispersionof individualhealthbenefits.HealthEconomics,11, 43e53.
Samuelson, P. A. (1947). Foundations of economic analysis (1983 edition).. Cam-bridge, Mass: Harvard University Press.

O. Mæstad, O.F. Norheim / Social Science & Medicine 75 (2012) 1836e1843 1843
Steinbock, B. (1992). Life before birth, the moral and legal status of embryos andfetuses. New York: Oxford University Press.
Tsuchiya, A. (2001). The value of health at different ages. Discussion Paper 184. York:Centre for Health Economics, University of York.
Tsuchiyaa, A., Dolan, P., & Shaw, R. (2003). Measuring people’s preferencesregarding ageism in health: some methodological issues and some freshevidence. Social Science & Medicine, 57, 687e696.
Tungodden, B. (2003). The value of equality. Economics and Philosophy, 19, 1e44.Wagstaff, A. (2002). Inequality aversion, health inequalities and health achieve-
ment. Journal of Health Economics, 21, 627e641.Wagstaff, A., Paci, P., & van Doorslaer, E. (1991). On the measurement of inequalities
in health. Social Science & Medicine, 33, 545e577.Williams, A. (1997). Intergenerational equity: an exploration of the “fair innings”
argument. Health Economics, 6, 117e132.