Embed Size (px)
Citation preview

J. Behov. Ther. & Exp. P.~.vchiar. Vol 25, No. 4. pp. 283-291. 1994. 0 1994 Elsevier Science Ltd
Printed in Great Britain. All rights reserved OCO-7916/94 $7.00 + O.lXl
00057916(94)00051-4
A TRIAL OF EYE MOVEMENT DESENSITIZATION COMPARED TO IMAGE HABITUATION TRAINING AND APPLIED MUSCLE RELAXATION IN POST-
TRAUMATIC STRESS DISORDER
KEVIN VAUGHAN
University of Sydney
MICHAEL S. ARMSTRONG
School of Psychiatry, University of New South Wales
RUTH GOLD, NICHOLAS O’CONNOR and WILLIAM JENNEKE
Homsby and Ku-Ring-Gai Hospital
NICHOLAS TARRIER
Department of Psychiatry, University of Manchester
Summary - Thirty-six patients with PTSD were randomly allocated to individual treatment with imaginal exposure (image habituation training - IHT), or applied muscle relaxation (AMR) or eye movement desensitization (EMD). Assessment by a blind independent rater and self-report instruments applied pre and posttreatment and at 3-month follow-up indicated that all groups improved significantly compared with a waiting list and that treatment benefits were maintained at follow-up. Despite a failure to demonstrate differences among groups, there was some suggestion that immediately after treatment EMD was superior for intrusive memories.
Various cognitive-behavioral treatments (CBT) of In eye movement desensitization (Shapiro, post-traumatic stress disorder (PTSD) have been 1989a, b) the patient is asked to perform eye described since this disorder was included in movements by tracking the therapist’s hand as it DSM-III (American Psychiatric Association, moves rapidly from side to side across his visual 1980). These treatments include exposure, anxiety field, while attending to one or more of the management techniques, and a new and elements of the traumatic memory - its image, controversial method, eye movement negative thoughts, affects and associated desensitization. Exposure techniques require the kinesthetic sensations. In a later phase a negative individual to confront the feared memory until it interpretation of the image such as “I am helpless” loses its arousal-provoking properties, through a is reprocessed using further eye movements to a process of habituation (Foa & Rothbaum, 1989). more positive, realistic cognition such as “Now I Anxiety management techniques teach methods of have control”. These procedures are repeatedly regulating arousal provoked by memories of the applied to the memory, until ideally it can no trauma, and may include progressive muscle longer evoke any bodily arousal. Related traumatic relaxation, and anger control training (Keane, memories or issues of self-esteem may emerge Zimering & Caddell, 1985). during treatment and these are also treated using
Requests for reprints should be addressed to Dr Kevin Vaughan, Palmerston Centre, Palmerston Road, Hornsby and Ku-Ring-Gai Hospital, Homsby NSW, Australia 2077.
283

284 K. VAUGHAN el al
the eye movement procedure. Shapiro (1991) renamed her method eye movement desensitiza- tion and reprocessing (EMDR) “. . in order to reflect its wide range of application and the information processing evident in the overall effect .”
The suggestion that EMD enhances desensitization and accelerates information processing opens EMD to controversy, as the method lacks both a theoretical foundation (Wolpe & Abrams, 1991) and empirical support. While various case reports and multiple case studies have reported EMD strikingly effective in trauma victims (Shapiro, 1989a, b; Wolpe & Abrams, 1991; Puk, 1991; Marquis, 1991; Kleinknecht & Morgan, 1992; McCann, 1992; Page & Crino, 1993; Spector & Huthwaite, 1993; Vaughan, Wiese, Gold & Tarrier, 1994), not all of the outcomes achieve in one session the magnitude of effects reported by Shapiro (1989b) in her controlled trial. Two studies (Lipke & Botkin, 1992; Oswalt, Anderson, Hagstrom & Berkowitz, 1993). which included inpatients with PTSD, reported results notably inferior to Shapiro’s. A number of authors (Lohr et al., 1992; Herbert & Mueser, 1992; Page & Crino, 1993) have called attention to methodological shortcomings in published work. Some of the major concerns voiced were: ( 1) lack of objective assessment of symptoms, (2) successful reports may reflect author selection and publishing bias and, in the only controlled trial (Shapiro, 1989b), (3) a possibly less plausible placebo condition. and the presence of therapist demand characteristics in the EMD condition, since treatments were continued until significant therapeutic changes were achieved.
Few adequate controlled studies of traditional CBT approaches to PTSD exist. Major findings from studies which examined exposure and anxiety management techniques (Keane, Fairbank. Caddell & Zimering, 1989; Foa, Rothbaum, Riggs & Murdock, 199 I ; Resick, Jordan, Girelli, Hutter & Marhoefer-Dvorak, 1988; Resick & Schnicke. 1992) are: (1) active treatments are superior to wait list. (2) treatments are more effective if they deal with symptoms directly associated with
traumatic memories, and (3) treatment gains consolidate during follow-up, especially with exposure, (4) gains with anxiety management techniques may be transitory (Foa & Rothbaum, 1989).
The present research compares the efficacy of EMD, IHT, AMR and wait list control in treating PTSD.
Subjects
Thirty-six outpatients referred to the PTSD Clinic for treatment served as subjects. There were 23 females and 13 males, aged 20-78 years (mean 32, SD 14.7). Experiences of traumatic events included: victim of violent crime (I 5), rape (5), child abuse (5), motor accident (6); the events had occurred on average 6.6 years earlier (SD 8.9). Eleven subjects had received previous psychiatric treatment.
All potential subjects seeking treatment at the PTSD Clinic were briefly interviewed by telephone. Those who reported a traumatic experience and one or more Re-
experiencing/intrusive symptoms of at least moderate severity (PTSD Category B, DSM-III- R), were sent an information package about the study, a consent form for participation in the study. and demographic and symptom questionnaires. Over 60 packages were sent out and 39 individuals whose questionnaires indicated probable PTSD participated in the trial. At assessment, three people were eliminated from the study, two because of severe personality disorder and one because of schizophrenia.
Assessment
Structured interview. This was conducted by a blind rater (RG) on four occasions during the study - initial entry, wait list reassessment (17 individuals), posttreatment and follow-up.
PTSD diagnosis and symptom severity: The PTSD Structured Interview (SI-PTSD; Davidson, Smith & Kudler. 1989), which scores each of 17 DSM-III-R criteria for severity on a scale of O-4, was administered.
A Trial of Eye Movement Desensitization 285
Comorbidity: The Anxiety Disorders Interview Schedule Revised (ADIS-R; Di Nardo & Barlow, 1988) was utilized to obtain measures of Generalized Anxiety Disorder (GAD) and Panic Disorder (PD). The 17-item Hamilton Rating Scale for Depression (HRSD; Hamilton, 1960) was used as a measure of depression.
Self-report symptom measures. Subjects completed the State form of the State-Trait Anxiety Inventory (STAI; Spielberger, 1983), the Beck Depression Inventory (BDI; Beck, 1978) and the Impact of Events Scale (IES; Horowitz, Wilner & Alverez, 1979).
Patient report of therapist characteristics. A questionnaire which indexed therapist empathy, warmth and genuiness was developed. For example, subjects could rate the statement “the therapist showed warmth towards me during the session” on a scale from “not at all” to “very much so” (04).
Procedure
After assessment each subject was randomly assigned to a treatment group and also to a wait list or nonwait list group. The procedure resulted in unequal numbers of subjects in the treatment groups - 12 in EMD, 13 in IHT and 11 in AMR. Seventeen of the 36 were initially assigned to the wait list and were reassessed after 2-3 weeks (mean 18.2 days, SD 0.8) before undergoing their active treatment. All subjects were reassessed posttreatment and at the approximately 3-month follow-up (mean 75.7 days, SD 27.8).
Treatment
Therapists were asked to treat patients for four sessions. Treatment was administered in 3-5 (mean 4.3, SD 0.7) individual sessions (mean 50 mins, SD 8.6) over a 2-3 week period. The three treatment conditions were as follows:
EMD: Treatment is described in more detail by Vaughan et al. (1994). It should be noted that
EMD includes techniques regarded as part and parcel of many psychotherapy packages: Emotional reframing and distancing techniques, exposure, and identification and rehearsal of coping self-statements. All therapists were trained by Dr Shapiro, and the protocol described by Shapiro (1989a, b) was followed as closely as possible.
IHT: This method is described by Vaughan & Tarrier (1992) who reported a case series which found it effective in PTSD. Subjects are required to listen to continuous loop audiotaped descriptions of their trauma and to record cognitions and anxiety levels on a homework sheet for 60 minutes per day.
AMR: Subjects were taught to recognize early signals of anxiety so that they could then apply the relaxation technique of Ost (1987). They were expected to practice the relaxation technique for two 20-minute periods per day. Thus although subjects in the three treatment groups were to receive the same number of treatment sessions, homework was also expected in the IHT and AMR groups, but not in the EMD group.
Results
At entry to the study all patients satisfied DSM- III-R Category B (Re-experiencing/intrusive) and Category D (Hyperarousal) criteria for PTSD: However 22% failed to qualify for a diagnosis of PTSD because they had less than the three required Category C (Avoidance/numbing) symptoms. This is a symptom pattern common in community samples (Creamer, 1989; Solomon & Canino, 1990) and has promoted moves to reduce the number of Category criteria from three to two in DSM-IV (Davidson & Foa, 1993). Comorbid diagnoses of PD were made in 11 patients (31%), GAD in 20 (55%) and Major Depression in six (17%). Treatment groups did not differ on number of treatment sessions, demographic, trauma- related or symptom variables except that GAD was over-represented in IHT (77%) compared to AMR (27%) (x2, p = .035).
Paired sample t-tests on SI-PTSD total scores

286 K. VAUGHAN et al.
Table 1
SI-PTSD Symptom categor) and Hamilton Rating Scale for Depre.ssion (HRSD) Mean Scores: Post-wit List Compared to Posttreatment
Wait list Symptom Mean (SD)
SI-Total Pre 30.4 (7.7 Post 28.5 (8.9)
St-Category B (Re-exphntrusive) Pre 7.7 (3.3) Post 6.6 (3.2)
Sl-Category C (Avoidance) Pre 9.5 (2.8) Post 9.5 (4.2)
Sl-Category D (Hyperarousal) Pre 13.2 (3.2) Post 12.4 (3.0)
HRSD (Depression) Pre 14.2 (4.2) Post 13.8 (4.7)
Treatment Mean (SD)
28.5 (8.9) 20.5 (I 1.3)
6.6 (3.2) 4.5 (4.3)
9.5 (4.2) 6.7 (3.8)
12.4 (3.0) 9.3 (4. I)
13.8 (4.7) 9.6 (6.7)
t (significance)
1.1 (ns) 3.7 (.002)*
I .4 (ns) 2.1 (.057)
-0.1 (ns) 4.1 (.ool)*
I .5 (ns) 2.9 (.Ol)*
0.6 (ns) 3.1 (.008)*
*Significant following Bonferroni correction.
in wait list subjects (post-wait list vs posttreatment) revealed a significant effect of treatment @ < .0.5). Examination of scores on SI- PTSD Categories and HRSD revealed that after Bonferroni adjustment (p = .Ol), treatment was significantly superior to no treatment for Category C and D (Avoidance and Hyperarousal symptoms) and HRSD, and failed to reach significance for Category B (re-experiencing) symptoms (see Table I).
The improvement in all treatment groups is further illustrated by the fall in number of patients diagnosed with PTSD, from 78% of patient at entry to the study to 47% after treatment and 30% at follow-up.
The effects of individual treatment on measures of symptomatology were examined by 2 x 3 MANOVAs, Occasion (pretreatment, posttreatment) x Treatment (EMD, IHT, AMR) with Occasion as a within-subject factor.
PTSD and depressive symptomatology as measured by SI-PTSD Category and HRSD are shown in Table 2. MANOVA yielded significant Occasion effects (all p < .OOl) but no Treatment interactions were significant.
Total PTSD symptoms: All three groups improved significantly after treatment (EMD, t = 3.58, p = ,004; IHT, t = 2.15, p = .05; AMR, t = 3.24, p = .009) and at follow-up (EMD, t = 6.88, p < ,001; IHT, t = 2.19, p = .05; AMR, t = 5.26, p =
.OOl). The groups did not differ posttreatment or at follow-up in number of subjects qualifying for a diagnosis of PTSD.
Category B: Re-experiencing/intrusive symptoms improved in all three groups with treatment, and improvement was sustained at follow-up. Only EMD produced significant improvement in Flashbacks and Nightmares posttreatment (t = 2.77, p = .O 1; t = 3.19, p = .009) and at follow-up (t = 4.69, p c ,001; t = 3.22, p =
.OOS) - indeed only one patient continued to report mild nightmares (see Table 3).
Effectiveness of EMD with intrusive symptoms was reinforced by results on the self-report measure IES-Intrusion: For posttreatment, only EMD showed significant improvement (t = 6.28, p
< ,001). MANOVA demonstrated a significant Occasion x Treatment interaction for IES- Intrusion (one-way ANOVA F[2, 311 = 3.77, p =
.034), with EMD superior to AMR (t = 2.57, p =

Table 2
A Trial of Eye Movement Desensitization 287
SI-PTSD Symptom Category and Hamilton Rating Scale for Depression (HRSD) Scores Across Groups at Pre, Post and Follow- Up, and MANOVA Significance Values (N = 36)
Symptom EMD(N= 12)
Mean (SD) IHT (N= 13)
Mean (SD) AMR(N= 11)
Mean (SD) Significance
Occas. Occas. x Treat.
SI-Total Pre 27.9 (9.5) Post 16.8 (6.2) FU 15.6 (7.4)
SI-Category B (Re-exp./intrusive) Pre 7.2 (3.8) Post 3.1 (2.6) FIJ 2.6 (2.7)
%-Category C (Avoidance) Pre 9.1 (3.7) Post 5.8 (1.9) FU 5.6 (3.5)
SI Category D (Hyperarousal) Pre 11.7 (3.6) Post 7.8 (3.1) FU 7.4 (3.5)
HRSD (Depression) Pre 13.0 (5.30) Post 6.3 (3.8) FU 6.9 (4.9)
27.8 (4.7) 29.9 (9.7) 23.0 (10.2) 23.1 (12.5) .0OOt ns 20.6 (14.1) 19.6 (10.9) .0OOt ns
6.3 (2.4) 7.4 (2.9) 5.4 (3.6) 5.1 (4.2) .001* ns 3.9 (4.4) 4.4 (3.2) .ooot “E
9.7 (2.9) 10.0 (5.3) 7.9 (3.8) 8.0 (5.2) .0OOt ns 7.9 (6.0) 6.7 (4.4) .ooot ns
11.8 (1.9) 12.6 (3.9) 9.8 (4.0) 10.0 (4.7) .ooot ns 8.9 (5.3) 8.6 (4.7) .ooot ns
13.1 (3.6) 14.2 (5.2) 11.2 (5.8) 10.6 (6.3) .ooot ns 11.5 (6.9) 8.2 (5.2) .ooot ns
*p I .05; tp 5 .Ol.
Table 3
St-PTSD Flashback and Nightmare Mean Scores, Pre, Post and Follow-Up for Treatment Groups (N = 36)
Symptom EMD
Mean (SD) IHT AMR
Mean (SD) Mean (SD)
SI-Flashbacks Pre Post FU
2.1 (1.2) 1.9 (1.2) 1.5 (1.5) 0.8 (1.1) 1.2 (1.5) l.O(l.5) 0.4 (1.0) 1.0 (1.5) 0.6(1.2)
SI-Nightmares Pre Post FU
1.9 (1.9) 1.6(1.7) 1.7 (1.6) 0.1 (0.2) 1.1 (1.5) 1.6 (1.5) 0.6 (0.9) 0.8 (1.5) 1.5 (1.7)
.023). At follow-up EMD improved further (t = 6.9, p < .OOl) but significant superiority was lost due to the improvement in IHT (t = 2.39, p < .05) and AMR groups (t = 3.6 1, p < .006).
Category C symptoms: On SI-PTSD significant improvement in Avoidance occurred only in the EMD group (t = 3.22, p = .008), a trend
maintained at follow-up (t = 3.27, p = .007). Immediately posttreatment IHT was superior to the other two groups on IES-Avoidance (t = 2.31, p < .0.5) however this advantage was lost at follow-up.
Category D symptoms: Hyperarousal improved significantly with EMD and IHT (t = 2.7, p = .025; t = 2.55, p = .025), AMR just failing to reach significance (t = 2.07, p = .06). At follow-up all groups showed improvement (EMD, I = 3.23, p =
.008; IHT, I = 2.34, p = .04; AMR, r = 3.71, p =
.004) (see Table 2). Comorbidity: Pretreatment diagnoses of PD did
not differ significantly between EMD, IHT and AMR (N = 5, 4 and 2). With treatment, PD was eliminated in EMD (EMD > AMR, x2, p = .035) however one patient relapsed at follow-up (N = 1, 4 and 1). GAD was over-represented in IHT pretreatment and although reductions in diagnoses occurred for EMD and IHT posttreatment (N = 1, 5 and 3 for EMD, IHT and AMR) and at follow- up (Iv’ = 2, 5 and 4), the groups did not differ
288
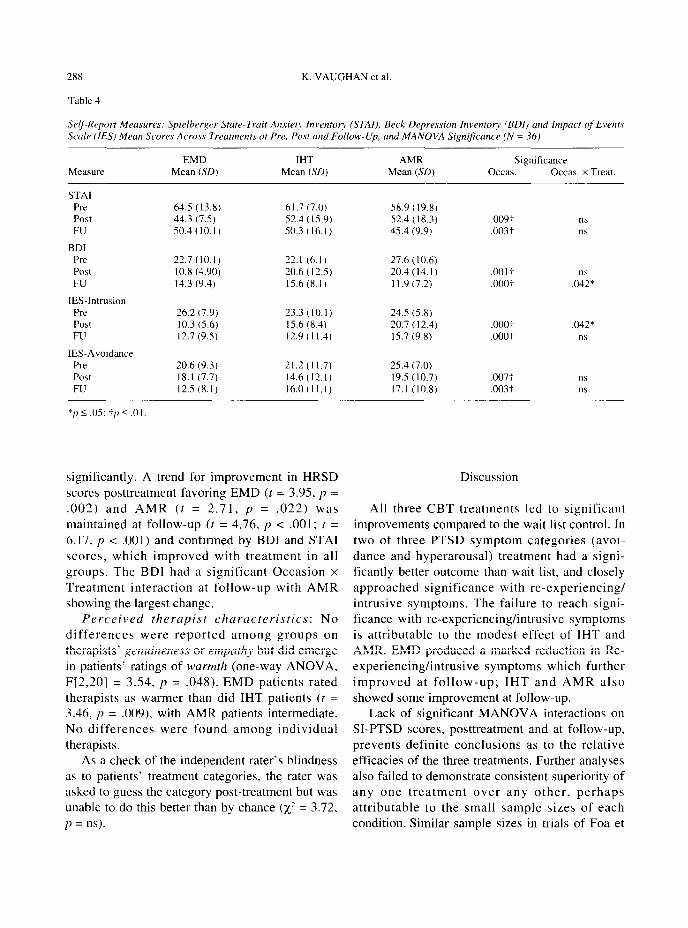
Table 4
K. VAUGHAN et al.
Selj-Report Measures: Spielbrrger StowTrait Anxiety Inventog~ (STAI), Beck Depression Inventory (BDI) and Impcrct of Evmt.s Scale (1E.S) Mean Scores Across Treatments at Pre, Post und Follow-Up, and MANOVA Significance (N = 36)
Measure
STAI Pre Post FU
BDI Pre Post FU
IES-Intrusion Pre Post FU
IES-Avoidance Pre Post FU
*p 5 .05: -t/1 5 .Ol,
EMD IHT Mean (SD) Mean (SD)
64.5 (13.8) 61.7 (7.0) 44.3 (7.5) 52.4 (15.9) 50.4(lO.l) 50.3 (16. I)
22.7(lO.l) 22.1 (6.1) 10.8 (4.90) 20.6 (12.5) 14.3 (9.4) 15.6 (8.1)
26.2 (7.9) 23.3 (10.1) 10.3 (5.6) 15.6 (8.4) 12.7 (9.5) 12.9 (I 1.4)
20.6 (9.3) 21.2(11.7) 18.1 (7.7) 14.6 (12.1) 12.5 (8.1) 16.0 (I 1.1)
AMR Mean (SD)
58.9 (19.8) 52.4 (I 8.3) 45.4 (9.9)
27.6 (10.6) 20.4 (14.1) 1 I .9 (7.2)
24.5 (5.8) 20.7 (12.4) 15.7 (9.8)
25.4 (7.0) 19.5 (10.7) 17.1 (10.8)
Significance Occas. Occas. x Treat.
.009t ns
.003+ ns
.OOlf ns ,000: .042*
.ooo:- .042*
.ooot ns
.007; “S
.003-i ns
significantly. A trend for improvement in HRSD scores posttreatment favoring EMD (t = 3.95, p = .002) and AMR (t = 2.71, p = .022) was maintained at follow-up (t = 4.76, p < ,001; t = 6.17, p < .OOl) and confirmed by BDI and STAI scores, which improved with treatment in all groups. The BDI had a significant Occasion x Treatment interaction at follow-up with AMR showing the largest change.
Perceived therapist characteristics: No
differences were reported among groups on therapists’ genuineness or empathy but did emerge in patients’ ratings of warmth (one-way ANOVA, F[2,20] = 3.54, p = ,048). EMD patients rated therapists as warmer than did IHT patients (t = 3.46, p = .009), with AMR patients intermediate. No differences were found among individual therapists.
As a check of the independent rater’s blindness as to patients’ treatment categories, the rater was asked to guess the category post-treatment but was unable to do this better than by chance (x2 = 3.72, p = ns).
Discussion
All three CBT treatments led to significant improvements compared to the wait list control. In two of three PTSD symptom categories (avoi- dance and hyperarousal) treatment had a signi- ficantly better outcome than wait list, and closely approached significance with re-experiencing/ intrusive symptoms. The failure to reach signi- ficance with re-experiencing/intrusive symptoms is attributable to the modest effect of IHT and AMR. EMD produced a marked reduction in Re- experiencing/intrusive symptoms which further improved at follow-up; IHT and AMR also showed some improvement at follow-up.
Lack of significant MANOVA interactions on SI-PTSD scores, posttreatment and at follow-up. prevents definite conclusions as to the relative efficacies of the three treatments. Further analyses also failed to demonstrate consistent superiority of any one treatment over any other, perhaps attributable to the small sample sizes of each condition. Similar sample sizes in trials of Foa et

A Trial of Eye Movement Desensitization 289
al. (1991) and Resick et al. (1988) may also have prevented them from demonstrating clear differences between active treatment. It may be that the relative strengths of CBT treatments for PTSD are such that larger numbers of subjects are required to minimize Type II errors.
There was no evidence for superiority of the more established treatments over EMD. If anything the trend was in the opposite direction. Total PTSD symptoms were reduced by 45% in the EMD group as compared to IHT (25%) and AMR (34%). Immediately after treatment, EMD had a striking impact on re-experiencing/intrusive symptoms on SI-PTSD and on IES-Intrusion. The marked clinical improvement on flashbacks and nightmares is consistent with a previous report (Vaughan et al., 1994) and may distinguish EMD from other treatments.
It could be argued that greater therapist warmth in the EMD group might account for any particular benefits of EMD. However findings such as those of Sloane, Staples, Cristol, Yorkston and Whipple (1975) offer little support to the notion of perceived warmth as a predictor of outcome. A possible explanation of greater rated warmth in EMD is that the procedure fostered a more spontaneous, nondirective relationship, unlike IHT, with its use of audiotaped recordings and homework.
The findings that EMD is comparable in effectiveness to two other CBT treatments must be interpreted with knowledge of the limitations of the study. As well as the standard problems inherent in finding no differences, the study’s limitations include: the limited time devoted to treatment; lack of specification of criteria for terminating treatment other than at the end of the fourth session (although in practice the groups did not differ in number of sessions); and different amounts of treatment received by the groups (IHT and AMR groups carried out 60 and 40 minutes, respectively, of additional daily homework sessions in between treatment sessions).
Although the major finding of superiority of active treatments over wait list is encouraging for therapists who treat PTSD, this finding cannot be used to support the validity of theoretical
rationales of the individual treatments. A wait list is not a placebo psychological treatment, and because meta-analytic studies consistently demonstrate superiority of placebo treatments over wait lists (McConaghy, 1990), it is possible that improved outcome in active treatments could have stemmed from nonspecific effects of therapy.
Reasons for the apparent effectiveness of EMD remain to be elucidated, although various authors, including Shapiro (1991) have speculated on mechanisms. Whether the eye movements themselves are necessary is unknown, but concentration on traumatic imagery may reflect focused imaginal exposure and working through of the preferred positive belief various cognitive strategies. The hypnosis-like altered state of consciousness reported by many subjects could aid self-induced suggestions. Demands for attention to the novel stimulus offered by the therapist’s hand movements in the presence of a cortical set directed towards the traumatic memory could elicit intense and persistent orienting responses (Pavlov, 1927; Sokolov, 1963) which would facilitate learning. Recently Dyck (1993) has proposed a cognitive conditioning model based on the principles of respondent and operant conditioning and emotional interference with learning.
The particular focus on eye movements in Sanderson & Carpenter (1992) points to a possible problem in assessing reports of the effectiveness of EMD. The strikingly successful single-session case reports, and perhaps also the analogy with imaginal desensitisation, appear to have given many the idea that EMD is a quick and easy therapy, with eye movements its most important and characteristic feature. In the present study improvements in the EMD group required four sessions of therapy and many of the patients could have benefited from more. It is the authors’ experience, in treating patients referred to a general hospital PTSD clinic with EMD, that while excellent therapeutic outcomes can be achieved, EMD needs to be carried out in a therapeutic context, requires highly developed clinical skills, including a solid grounding in

290 K. VAUGHAN et al.
cognitive therapy, and calls for persistence and resourcefulness.
A~~knohledgements - We are indebted to the NSW Department of Health and to the generosity of Mr Don Heggie. Dr Michael Jones, School of Behavioral Sciences, Macquarie University provided statistical advice.
References
American Psychiatric Association (1980). Diagnostic and Srutisticul Manucrl of Mental Disorders (3rd edition). Washington. D.C.
Beck. A. T. (I 97X). Depression invento?. Philadelphia: Center for Cognitive Therapy.
Creamer, M. ( 1989). Post-traumatic stress disorder: some diagnostic and clinical issues. Australian and New Zealand Journal of Psychiat~, 23. 5 17-522.
Davidson. J., & Foa, E. B. (1993). Epilogue. In: Post-traumatic Stress Di.sordrr: DSM-IV and Beyond. Washington: American Psychiatric Press Inc.
Davidson. J.. Smith, R.. & Kudler, H. (1989). Validity and reliability of the DSM-III criteria for post-traumatic stress disorder: experience with a structured interview. Journal of Nervous and Mental Disease, 177, 336-341.
Di Nardo, P. A., & Barlow, D. H. (1988). AnxieQ Disorders Interviebv Schedule Revised (ADIS-R). Albany, N.Y.: Centre for Stress and Anxiety Disorders.
Dyck, M. J. (1993). A proposal for a conditioning model of eye movement desensitization treatment for posttraumatic stress disorder. Journal of Behavior Therapy and Experimental l+hiatry, 24. 201-210.
Foa. E.. & Rothbaum, B. 0. (1989). Behavioural psychotherapy for post-traumatic stress disorder. International Revie\t, qf Psychiatry, I, 219-226.
Foa, E., Rothbaum, B. O., Riggs, D. S., & Murdock, T. B. (1991). Treatment of post-traumatic stress disorder in rape victims: a comparison between cognitive-behavioral procedure< and counseling. Journal of Consulting and Clinical Psychology, 5. 7 15-723.
Hamilton. M. (1960). A rating scale for depression. Journal of
Nerrrolog~, Nerrrorurge~ and Psychiatry. 23, 56-62. Herbert, J. D.. & Mueser, K. T. (1992). Eye movement
desensitization: a critique of the evidence. Journal of
Rrhtr\~ior- Therapy and Experimental Ps.vchiatry, 23, 169- 174.
Horowitz, Wilner. N., & Alverez, W. (1979). Impact of Event Scale: a measure of subjective stress. Psychosomatic Medicine. 41, 209-2 18.
Keane, T. M., Zimering. R. T., & Caddell, J. M. (1985). A behavioral formulation of PTSD in Vietnam veterans. B~/w~~ior Thrrapi.st, h’. 9- 12.
Keane, T. M.. Fairbunk, J. A., Caddell. J. M., & Zimering, R. T. ( 1989). Implosive (flooding) therapy reduces symptoms of PTSD in Vietnam combat veterans. Behavior Therapy, 20. 245-260.
Kleinknecht. R. A.. & Morgan, M. P. (1992). Treatment of
post-traumatic stress disorder with EMD. Journal of
Behavior Therapy and Experimental Psychiatry, 23.4349. Lipke, H. J., & Botkin, A. L. (1992). Case studies of eye
movement desensitization and reprocessing (EMD/R) with chronic post-traumatic stress disorder. Psychotherapy, 29, 591-595.
Lohr, J. M., Kleinknecht, R. A., Conley, A. T., da1 Cerro, S., Schmidt, J., & Sonntag, M. E. (1992). A methodological critique of the current status of eye movement desensitization (EMD). Journal of Behavior Therapy and Experimental Psychiatry,23, 159-167.
Marquis, J. N. (1991). A report on seventy-eight cases treated by eye movement desensitization. Journal of Behavior Therapy and Experimental Psychiatry, 22, 187-192.
McCann, D. L. (1992). Post-traumatic stress disorder due to devastating burns overcome by a single session of eye movement desensitization. Journal of Behavior Therapy and Experimental Psychiatry, 23,3 19-323.
McConaghy, N. (1990). Can reliance be placed on a single meta-analysis? Australian and New Zealand Journal of
Psychiatry, 24.405418. Ost, L. G. (1987). Applied relaxation: description of a coping
technique and review of controlled studies. Behavior Research and Therapy, 25, 397409.
Oswalt, R., Anderson, M., Hagstrom, K. & Berkowitz, B. (1993). Evaluation of the one-session eye-movement desensitization reprocessing procedure for eliminating traumatic memories. Psychological Reports, 73, 99.
Page, A. C., & Crino, R. (1993). Eye-movement desensitisa- tion: a simple treatment for post-traumatic stress disorder? Australian and New Zealand Journal of Psychiatry, 27, 288-293.
Parloff, M. B. (1986). Placebo controls in psychotherapy research: a sine qua non or a placebo of research problems? Journal of Consulting and Clinical Psychology, .54,79-87.
Pavlov, I. P. (1927). Conditioned rejlexes: an investigation of
the physiological activity of the cerebral cortex. New York: Dover Publications, Inc.
Puk, G. (1991). Treating traumatic memories: a case report on the eye movement desensitization procedure. Journal of
Behavior Therapy and Experimental Psychiatry, 22, 149-151.
Resick, P. A., & Schnicke, M. (1992). Cognitive processing therapy for sexual assault victims. Journal of Consulting and Clinical Psychology, 60, 748-756.
Resick, P. A., Jordan, C. G., Girelli, S. A., Hutter, C. K., & Marhoefer-Dvorak (1988). A comparative outcome study of behavioral group therapy for sexual assault victims. Behavior Therapy, 19.385-401.
Sanderson, A., & Carpenter, R. (1992). Eye movement desensitisation versus image confrontation: a single-session crossover study of 58 phobic subjects. Journal of Behavior Therapy and Experimental Psychiatry, 23, 269-275.
Shapiro, F. (1989a). Eye movement desensitization: a new treatment for Post-traumatic Stress Disorder. Journal of
Behavior Therapy and Experimental Psychiatry. 20, 21 l-217.
Shapiro, F. (1989b). Efficacy of the eye movement desensitization procedure in the treatment of traumatic memories. Journal of Traumatic Stress, 2, 1999223.
Shapiro, F. (1991). Eye movement desensitization and reprocessing procedure: from EMD to EMD/R - a new

A Trial of Eye Movement Desensitization 291
treatment model for anxiety and related traumata. Behavior Therapist, 12, 133-135.
Sloane, R. B., Staples, F. R., Cristol, A. H., Yorkston, N. H., & Whipple, K. (1975). Psychotherapy versus behavior therapy. Cambridge, MA: Harvard University Press.
Solomon, S. D., & Canino, G. J. (1990). Appropriateness of DSM-III-R criteria for post-traumatic stress disorder. Comprehensive Psychiatry, 31,227-237.
Sokolov, E. N. (1963). Perception and the conditioned reflex. Oxford: Pergamon Press.
Jacobs, G. A. (1983). Manual for the state-trait anxiet? inventory (STAI (FORM Y)). Palo Alto, CA: Consulting Psychologists Press, Inc.
Vaughan, K., & Tarrier, N. (1992). The use of image habituation training with post-traumatic stress disorder. British Journal of Psychiatq, 161, 658-664.
Vaughan, K., Wiese, M., Gold, R., & Tarrier, N. (I 994). Eye movement desensitisation: symptom change in post- traumatic stress disorder. British Journal of Psychintt~, 164, 533-541.
Spector, J., & Huthwaite, M. (1993). Eye-movement Wolpe, J., & Abrams, J. (1991). Post-traumatic stress disorder desensitisation to overcome post-traumatic stress disorder. overcome by eye movement desensitization: a case report. Brifish Journal ofPsychiatry, 163, 106-108. Journal of Behavior Therapy and Experimental Psychiatp.
Spielberger, C., Gorsuch, R. L., Lushene, R., Vagg, P. R., & 22. 3943.