Embed Size (px)
Citation preview
Journal of Surgical Research 163, 214–220 (2010)doi:10.1016/j.jss.2010.03.021
ASSOCIATION FOR ACADEMIC SURGERY
A Third-Generation Herpesvirus Is Effective Against Gastroesophageal
Cancer
Joyce Wong, M.D.,* Kaitlyn Kelly, M.D.,* Arjun Mittra, M.D.,* Segundo Jaime Gonzalez, M.D.,*Kyo Young Song, M.D.,* Guy Simpson, M.D.,† Robert Coffin, M.D.,† and Yuman Fong, M.D.*,1
*Department of Surgery, Memorial Sloan-Kettering Cancer Center, New York, New York; and †BioVex, Inc., Woburn, Massachusetts
Submitted for publication January 8, 2010
Background. Gastroesophageal cancer remains aleading cause of cancer deaths and is uniformly fatalin patients presenting with metastases and recur-rence. This study sets out to determine the effect ofa third-generation, replication-competent, oncolyticherpes simplex type 1 virus containing transgenesencoding for a fusogenic membrane glycoprotein andFcy::Fur, against gastroesophageal cancer.
Methods. The cytotoxic effect of the virus was testedon human gastroesophageal cancer cell lines OCUM-2MD3, MKN-45, AGS, MKN-1, MKN-74, and BE-3 at se-quential multiplicities of infection (MOI). Cytotoxicitywas measured using a lactate dehydrogenase assay. Vi-ral replication was tested by serially diluting superna-tants from viral infections and titering on VERO cellsvia standard plaque assay. Correlations of cytotoxicityand viral replication were also investigated.
Results. All cell lines were susceptible to viral infec-tion and demonstrated a dose-dependent effect, withgreater and faster cytotoxicity at higher MOIs. Viralreplication was supported in the cell lines tested, withpeak titers by d 5, some supporting as high as>40,0003 amplification. Cell lines with longer dou-bling times (>30 h) also achieved higher viral titers ata MOI of 0.1. Cell lines with shorter doubling timesachieved 50% cell kill in fewer days, with an averageof 2.3 d for cell lines with doubling times under 30 hcompared with 4.4 d for cell lines with doubling timesover 30 h.
Conclusion. These results suggest that this third-generation oncolytic herpesvirus can effectivelyinfect and lyse gastroesophageal cancer cells andmay provide a novel therapy against gastroesophagealcancer. � 2010 Elsevier Inc. All rights reserved.
1 To whom correspondence and reprint requests should be ad-dressed at Memorial Sloan-Kettering Cancer Center, 1275 York Ave-nue, New York, NY 10065. E-mail: [email protected]
0022-4804/$36.00� 2010 Elsevier Inc. All rights reserved.
214
Key Words: gastroesophageal cancer; herpesvirus;oncolytic.
INTRODUCTION
Gastroesophageal cancer remains one of the mostcommon malignancies worldwide and is the secondleading cause of cancer-related death. A significant pro-portion of patients will also either present with metas-tasis or develop recurrent disease despite treatment.Five-year survival rates for surgically resectable dis-ease are 45%–47% [1]. However, for patients who pres-ent with unresectable disease or who recur afterresection, the disease is nearly uniformly fatal. It is ev-ident that novel therapies are needed.
Oncolytic herpesviruses have been proven effectiveagainst a wide variety of malignancies, both in vitroand in vivo. Several viruses have been brought to clini-cal trials for patients with metastatic colorectal, headand neck, breast, and prostate cancer, melanoma, andglioma [2]. These modified viruses have been engi-neered to be tumor-specific with less systemic toxicity.The third-generation virus vector studied here (Onco-vexGALV/CD; Biovex Inc., Woburn, MA) was designedto more specifically target cancer cells via double dele-tions of g134.5, a neurovirulence gene, as well as a singledeletion of the US12 gene, which codes for the ICP 47protein. Also added is gibbon ape leukemia virus(GALV) fusogenic membrane glycoprotein and theFcy::Fur gene. The resulting virus is more lytic to tumorcells with a lessened toxic effect on normal cells, andpresents almost no chance for reversion to wild type.
In this study, we report preclinical data supportingthis third-generation, attenuated oncolytic herpesvirus
WONG ET AL.: HERPES VIRUS IS EFFECTIVE AGAINST GASTROESOPHAGEAL CANCER 215
as an effective therapeutic agent against gastroesopha-geal cancer.
MATERIALS AND METHODS
Cell Lines
Human gastric cancer OCUM-2MD3 cells were a gift fromDr. Masakazu Yashiro (Osaka City University Medical School,Japan) and were grown in Dulbecco’s modified Eagle’s medium(DMEM) supplemented with high glucose, 2 mmol/L L-glutamine,0.5 mmol/L sodium pyruvate, 100 U/mL penicillin, 100 mg/mL strep-tomycin, and 10% fetal calf serum (FCS). The human gastric cancercell line MKN-45, a poorly differentiated adenocarcinoma, was ob-tained as a gift from Dr. Yutaka Yoneumura (Kanazawa University,Japan) and was maintained in Roswell Park Memorial Institute(RPMI) medium supplemented with 10% FCS, 1% penicillin, and1% streptomycin. Human AGS cells (a gastric adenocarcinoma epi-thelial cell line) were obtained from American Type Culture Collec-tion (ATCC; Manassas, VA) and were routinely cultured in Ham’sF-12K medium with 10% fetal bovine serum (FBS). MKN-1, anadenosquamous cell carcinoma, and MKN-74, a well-differentiatedadenocarcinoma cell line, were kindly provided by Dr. T. Suzuki(Fukushima Medical College, Japan) and were cultured in RPMIsupplemented with 10% FBS, 1% penicillin, and 1% streptomycin.BE-3 is a human esophageal adenocarcinoma cell line and was pro-vided by Dr. Nasser Altorki (New York Presbyterian Hospital, NY).BE-3 was cultured in RPMI supplemented with 10% FBS, 1% peni-cillin, and 1% streptomycin.
Virus
This third-generation herpesvirus is an attenuated, replication-competent, oncolytic herpes simplex type 1 virus, derived from theJS-1 strain. It contains double deletions of the g134.5 gene and dele-tion of the US12 gene. The GALV env gene, which codes for the mem-brane glycoprotein of the gibbon ape leukemia virus, was cloned intothe ICP34.5 locus with truncation of 16 amino acids in the transmem-brane R peptide, thereby rendering the GALV glycoprotein constitu-tively active. The Fcy::Fur gene was also cloned into an ICP34.5locus. The GALV env R- gene and Fcy::Fur gene are under CMVand RSV promoters, respectively.
Cytotoxicity Assay
All gastroesophageal cell lines were plated at a density of 2 3104
cells per well in 12-well plates in 1 mL of medium. The plates wereincubated for 4 h, after which the medium was carefully suctionedoff. Virus was diluted in 100 mL of cold medium and then added inthree sequential multiplicities of infection (MOI, number of viralparticles per cancer cell), ranging from 0.001 to 1.0. Medium wasadded back to each well to a total volume of 1 mL after 20 min.An additional 1 mL of medium was added to all wells on d 4. At dailyintervals, the supernatants were collected from each well and fro-zen. The cells were then washed with phosphate-buffered saline(PBS) and lysed with 1.35% Triton-X solution to release intracellularlactate dehydrogenase (LDH). The amount of LDH present directlycorrelated to the number of lysed cells. This was quantified usinga Cytotox 96 colorimetric assay (Promega, Madison, WI), which mea-sured the conversion of a tetrazolium salt into a red formazan prod-uct in the presence of LDH, using a microplate spectrophotometer at490 nm. Results are demonstrated as percentages of survivingtreated cells to control, untreated cells. All conditions were testedin triplicate.
Viral Replication
Five gastroesophageal cell lines, AGS, BE3, MKN-1, MKN-45, andMKN-74, were plated at a density of 2 3 104 cells per well in 12-wellplates in 1 mL of medium. After incubation for 4 h, the medium wassuctioned off, and virus was added to each well in 100 mL of mediumat a MOI of 0.1. After 20 min, medium was added back to each wellto a total volume of 1 mL. On d 1, 3, 5, and 7, the supernatant was col-lected and frozen at –80�C. Serial dilutions of supernatant were addedto confluent VERO cells and incubated for 4 h. The wells were thenwashed with medium and 1% agarose with medium was added. After48 h of incubation, 2 mL of 2% neutral red was added to each well.Viral plaques were counted at 24 h. Supernatants from each cellline were counted in triplicate.
RESULTS
Viral Cytotoxicity
All six human gastroesophageal cancer cell lines weresusceptible to oncolysis by this third-generation onco-lytic herpesvirus. The OCUM-2MD3, MKN-45, andAGS cell lines overall were more sensitive to viral lysiscompared with MKN-74, MKN-1 and BE-3. All cell linesdemonstrated a dose-dependent effect, with greater andfaster cytotoxicity at higher MOI concentrations. InOCUM-2MD3, MKN-45, and AGS cell lines, virus killedall cells within 24 h at a MOI of 1.0 (data not shown).Comparing cytotoxicity with a MOI of 0.1 across thesix cell lines, the least sensitive cell line was MKN-1,followed by BE-3, MKN-74, AGS, MKN-45, andOCUM-2MD3. Cytotoxicity ranged from 56.1% to98.1%, respectively (Fig. 1).
The OCUM-2MD3 cell line proved to be particularlysusceptible to viral oncolysis, with near 100% cell killby d 5, at a MOI of 0.001. With a MOI of 0.1, >90% cellkill was achieved by d 3. The AGS cell line also provedquite susceptible with a MOI of 0.1, with 95% cell killby d 6. At a MOI of 0.01, 90% cytotoxicity was seen byd 7. The MKN-74 cell line demonstrated 80% cytotoxic-ity by d 5 at a MOI of 1.0 and 80% cytotoxicity by d 7 ata MOI of 0.1 (Fig. 1).
The MKN-1, BE-3, and MKN-45 cell lines requiredhigher viral doses to achieve cytotoxicity. Fifty percentcell kill was achieved in both BE-3 and MKN-1 by d 2at a MOI of 1.0 and by d 5 at a MOI of 0.1. The MKN-45 cell line achieved 50% cell kill by d 3 and 100% byd 5 at a MOI of 0.1. MKN-1 showed 95% cytotoxicityby d 5 at a MOI of 1.0 and 78% cell kill by d 7 at a MOIof 0.1. BE-3 similarly showed 95% cytotoxicity by d 5and 74% cytotoxicity by d 7 with a MOI of 0.1.
Viral Replication
Viral replication was supported in the five cell linestested, and all demonstrated peak viral titers on d 5(Fig. 2). BE-3 demonstrated the greatest viral titer,with a peak of 8.125 3 107 plaque-forming units (pfu)
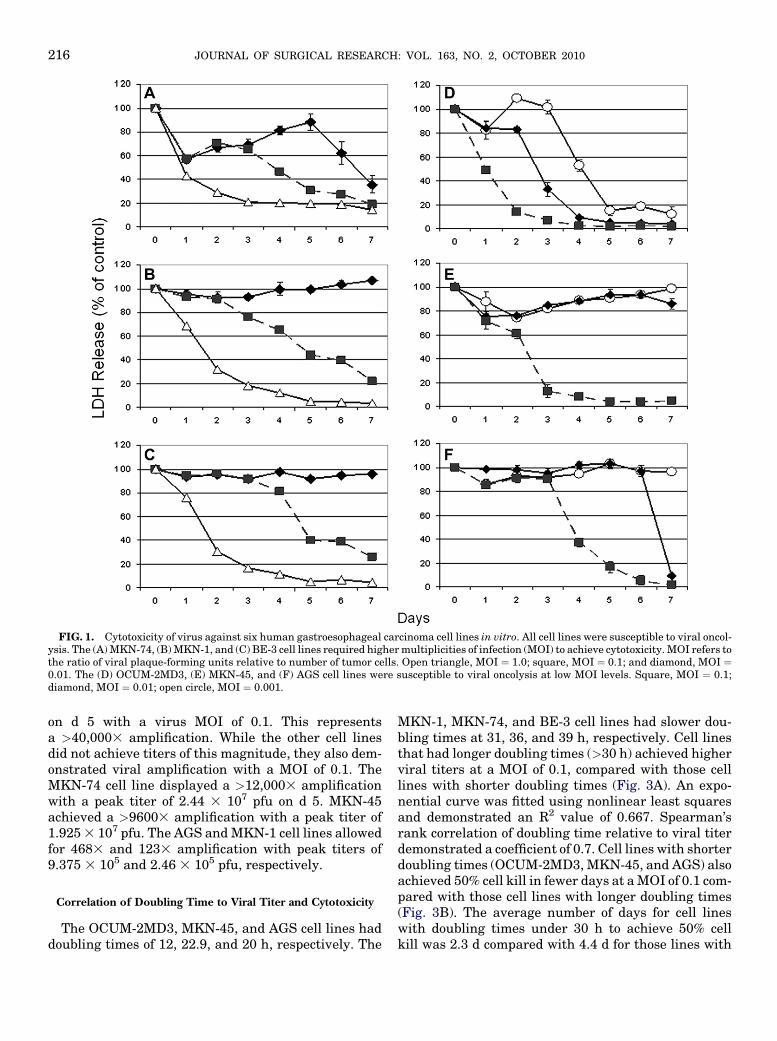
FIG. 1. Cytotoxicity of virus against six human gastroesophageal carcinoma cell lines in vitro. All cell lines were susceptible to viral oncol-ysis. The (A) MKN-74, (B) MKN-1, and (C) BE-3 cell lines required higher multiplicities of infection (MOI) to achieve cytotoxicity. MOI refers tothe ratio of viral plaque-forming units relative to number of tumor cells. Open triangle, MOI ¼ 1.0; square, MOI ¼ 0.1; and diamond, MOI ¼0.01. The (D) OCUM-2MD3, (E) MKN-45, and (F) AGS cell lines were susceptible to viral oncolysis at low MOI levels. Square, MOI ¼ 0.1;diamond, MOI ¼ 0.01; open circle, MOI ¼ 0.001.
JOURNAL OF SURGICAL RESEARCH: VOL. 163, NO. 2, OCTOBER 2010216
on d 5 with a virus MOI of 0.1. This representsa >40,0003 amplification. While the other cell linesdid not achieve titers of this magnitude, they also dem-onstrated viral amplification with a MOI of 0.1. TheMKN-74 cell line displayed a >12,0003 amplificationwith a peak titer of 2.44 3 107 pfu on d 5. MKN-45achieved a >96003 amplification with a peak titer of1.925 3 107 pfu. The AGS and MKN-1 cell lines allowedfor 4683 and 1233 amplification with peak titers of9.375 3 105 and 2.46 3 105 pfu, respectively.
Correlation of Doubling Time to Viral Titer and Cytotoxicity
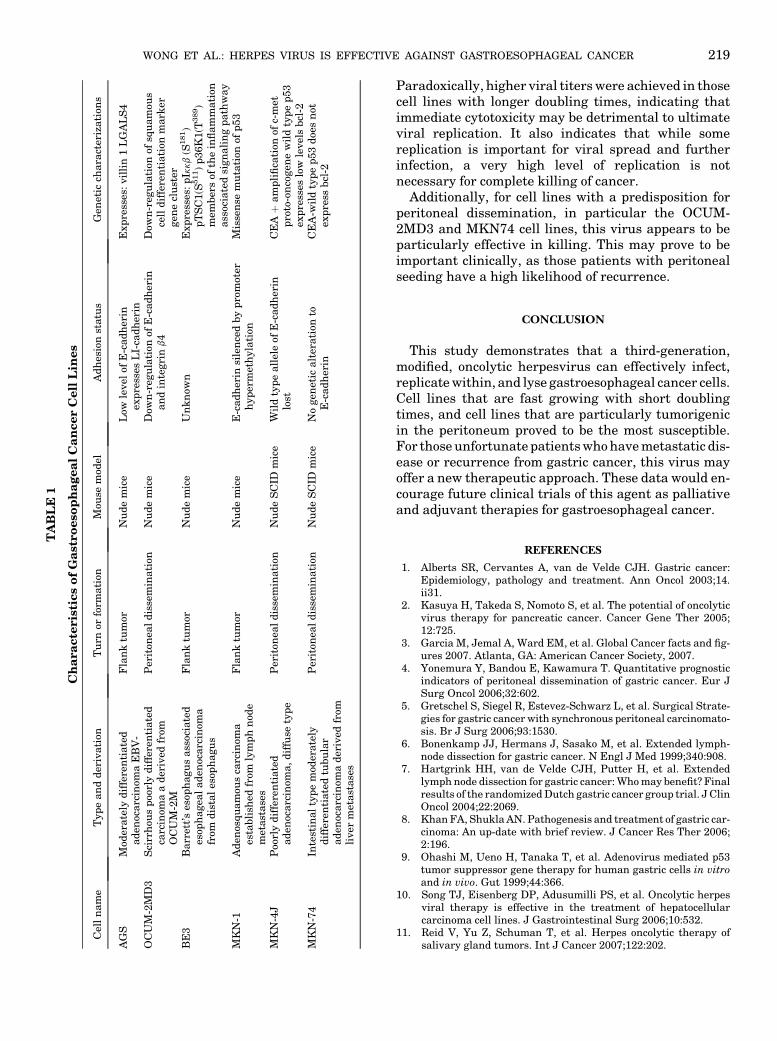
The OCUM-2MD3, MKN-45, and AGS cell lines haddoubling times of 12, 22.9, and 20 h, respectively. The
MKN-1, MKN-74, and BE-3 cell lines had slower dou-bling times at 31, 36, and 39 h, respectively. Cell linesthat had longer doubling times (>30 h) achieved higherviral titers at a MOI of 0.1, compared with those celllines with shorter doubling times (Fig. 3A). An expo-nential curve was fitted using nonlinear least squaresand demonstrated an R2 value of 0.667. Spearman’srank correlation of doubling time relative to viral titerdemonstrated a coefficient of 0.7. Cell lines with shorterdoubling times (OCUM-2MD3, MKN-45, and AGS) alsoachieved 50% cell kill in fewer days at a MOI of 0.1 com-pared with those cell lines with longer doubling times(Fig. 3B). The average number of days for cell lineswith doubling times under 30 h to achieve 50% cellkill was 2.3 d compared with 4.4 d for those lines with
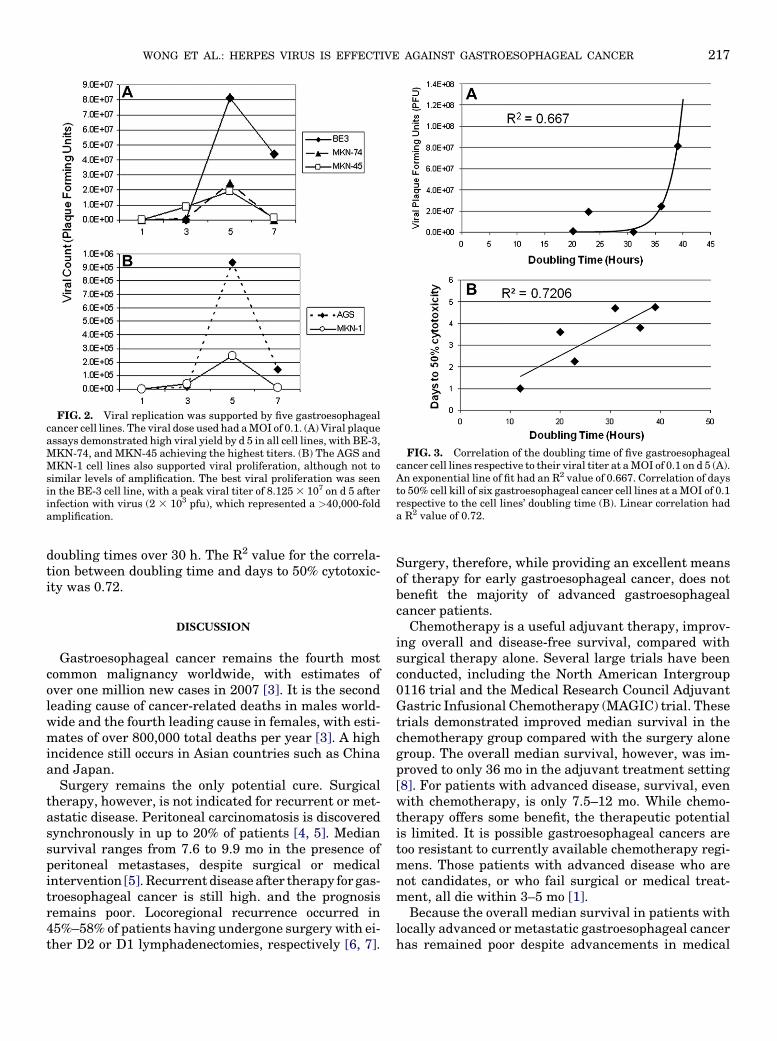
FIG. 2. Viral replication was supported by five gastroesophagealcancer cell lines. The viral dose used had a MOI of 0.1. (A) Viral plaqueassays demonstrated high viral yield by d 5 in all cell lines, with BE-3,MKN-74, and MKN-45 achieving the highest titers. (B) The AGS andMKN-1 cell lines also supported viral proliferation, although not tosimilar levels of amplification. The best viral proliferation was seenin the BE-3 cell line, with a peak viral titer of 8.125 3 107 on d 5 afterinfection with virus (2 3 103 pfu), which represented a >40,000-foldamplification.
FIG. 3. Correlation of the doubling time of five gastroesophagealcancer cell lines respective to their viral titer at a MOI of 0.1 on d 5 (A).An exponential line of fit had an R2 value of 0.667. Correlation of daysto 50% cell kill of six gastroesophageal cancer cell lines at a MOI of 0.1respective to the cell lines’ doubling time (B). Linear correlation hada R2 value of 0.72.
WONG ET AL.: HERPES VIRUS IS EFFECTIVE AGAINST GASTROESOPHAGEAL CANCER 217
doubling times over 30 h. The R2 value for the correla-tion between doubling time and days to 50% cytotoxic-ity was 0.72.
DISCUSSION
Gastroesophageal cancer remains the fourth mostcommon malignancy worldwide, with estimates ofover one million new cases in 2007 [3]. It is the secondleading cause of cancer-related deaths in males world-wide and the fourth leading cause in females, with esti-mates of over 800,000 total deaths per year [3]. A highincidence still occurs in Asian countries such as Chinaand Japan.
Surgery remains the only potential cure. Surgicaltherapy, however, is not indicated for recurrent or met-astatic disease. Peritoneal carcinomatosis is discoveredsynchronously in up to 20% of patients [4, 5]. Mediansurvival ranges from 7.6 to 9.9 mo in the presence ofperitoneal metastases, despite surgical or medicalintervention [5]. Recurrent disease after therapy for gas-troesophageal cancer is still high. and the prognosisremains poor. Locoregional recurrence occurred in45%–58% of patients having undergone surgery with ei-ther D2 or D1 lymphadenectomies, respectively [6, 7].
Surgery, therefore, while providing an excellent meansof therapy for early gastroesophageal cancer, does notbenefit the majority of advanced gastroesophagealcancer patients.
Chemotherapy is a useful adjuvant therapy, improv-ing overall and disease-free survival, compared withsurgical therapy alone. Several large trials have beenconducted, including the North American Intergroup0116 trial and the Medical Research Council AdjuvantGastric Infusional Chemotherapy (MAGIC) trial. Thesetrials demonstrated improved median survival in thechemotherapy group compared with the surgery alonegroup. The overall median survival, however, was im-proved to only 36 mo in the adjuvant treatment setting[8]. For patients with advanced disease, survival, evenwith chemotherapy, is only 7.5–12 mo. While chemo-therapy offers some benefit, the therapeutic potentialis limited. It is possible gastroesophageal cancers aretoo resistant to currently available chemotherapy regi-mens. Those patients with advanced disease who arenot candidates, or who fail surgical or medical treat-ment, all die within 3–5 mo [1].
Because the overall median survival in patients withlocally advanced or metastatic gastroesophageal cancerhas remained poor despite advancements in medical

JOURNAL OF SURGICAL RESEARCH: VOL. 163, NO. 2, OCTOBER 2010218
and surgical therapies, novel therapies are being inves-tigated in preclinical studies. Adenovirus vectors havebeen used for gene transfer in mediating apoptosis ingastric cancer and are a hopeful therapeutic agent butare not yet clinically available [9]. Attenuated oncolyticherpesviruses have been widely investigated for vari-ous types of cancer, including glioma, melanoma, meso-thelioma, breast, bladder, colorectal, hepatocellular,and salivary gland tumors [10, 11]. Several clinicaltrials are being conducted to determine efficacy andapplicability of various herpesviruses toward differenttypes of cancer [2, 12].
Oncolytic herpesvirus therapy has great promise ascancer therapy from many respects. The genome hasbeen sequenced and characterized so that nonessentialgenes may be deleted [13]. As much as 30 kb of thegenome may be deleted for insertion of genes tailoredfor cancer therapy [14]. Oncolytic herpesviruses havebeen genetically attenuated to be tumor specific andnon-neurovirulent. Double deletion of the g134.5 geneattenuates the virus to make it less neurotoxic, and de-letion of ICP47 increases antigen presentation withininfected tumor cells [15]. Importantly, antiherpes treat-ments such as acyclovir and ganciclovir make oncolyticherpes a clinically useful and safe vector [16].
Previous preclinical studies have been conductedevaluating the use of two oncolytic herpesviruses,G207 and NV1020, in relation to gastric cancer and car-cinomatosis. The G207 virus contains a double deletionof the g134.5 gene and an inactivation of the UL39 gene,which encodes ICP 6, a large subunit of ribonucleotidereductase. NV1020 contains only 1 deletion of theg134.5 gene. These studies found that both G207 andNV1020 were tumor specific with a significant thera-peutic benefit [17–19].
Several phases I and II clinical trials have evaluatedthe clinical efficacy of second-generation oncolytic her-pesviruses against melanoma and metastatic coloncancer, among others [12, 20]. Both intratumoral andintra-arterial injections of virus were performed, withlow toxicity effects observed. Local inflammation, ery-thema, and a transient febrile response were the mostcommonly observed effects from intratumoral injection[12]. Intraarterial injection produced more severeeffects, including transient rise in liver enzymes, diar-rhea, and leukocytosis, although these symptoms allcleared by 1 mo after administration. Additionally, nopatient demonstrated evidence of viral reactivation inblood, saliva, rectal, or vaginal swabs in close follow-up. Furthermore, the patients with high response tovirus administration had clinical response and sur-vived well past expected for disease prognosis [21].
These clinical trials were all performed with second-generation oncolytic herpesvirus and clearly demonstratedsafety and clinical benefits in human administration,
with low toxicity to healthy human cells. Successivegenerations of oncolytic herpesviruses have been en-gineered to further increase antitumor efficacy aswell as the safety and immunogenic profile of theseviruses [16].
We studied a third-generation, attenuated,replication-competent oncolytic herpesvirus containingtransgenes encoding GALV and Fcy::Fur to determineif it could play a therapeutic role in gastroesophagealcancer. It has already been shown to be cytotoxic invitro to human fibrosarcoma, colorectal and pancreaticcarcinoma, glioblastoma, astrocytoma, and lung epider-moid carcinoma cell lines [22]. The virus construct isunique in that it contains a double deletion of theg134.5 gene as well as a single deletion of the US12gene, making it tumor-specific and immune responsestimulating, respectively. In place of these genes, thegene coding for the GALV fusogenic protein and geneFcy::Fur were inserted. Expression of the GALV proteincaused the infected cells to form large syncytia and hasbeen shown to potentiate spread of virus and efficacy ofviral therapy [23].
Table 1 illustrates characteristics of the six gastro-esophageal cancer cell lines studied. All cell lines werederived from human gastroesophageal tumors or metas-tases from primary gastric cancer. The OCUM-2MD3,MKN-45, and MKN-74 cell lines, especially, are usedfrequently in animal models of peritoneal carcinomato-sis, having a predilection for peritoneal dissemination.Adhesion characteristics have been studied, and lossof expression of E-cadherin has been implicated in tu-mor progression and metastasis. All of the cell linesexcept for BE-3 and MKN-74 have a low level or down-regulation of E-cadherin. Further genetic characteriza-tions are listed for each cell line [24–27].
All of the gastroesophageal cancer cell lines studiedwere susceptible to viral oncolysis. While the OCUM-2MD3, MKN-74, and AGS cell lines proved to be partic-ularly susceptible with a MOI as low as 0.01, a MOI of1.0 was cytotoxic in the less sensitive cell lines BE3,MKN-1, and MKN-45. It is evident then that thisthird-generation, modified, oncolytic herpesvirus wouldbe a useful therapy as a single agent against gastro-esophageal cancer, as all cell lines are susceptible toviral oncolysis.
Cell lines with shorter doubling times were more sus-ceptible to viral oncolysis and demonstrated faster cyto-toxicity. OCUM-2MD3, MKN-45, and AGS cell lines, themost sensitive of the gastroesophageal cancer cell lines,had doubling times under 30 h, while the other three celllines, MKN-74, MKN-1, and BE3, had doubling timesover 30 h [28–31]. This oncolytic herpesvirus wouldtherefore be particularly useful against gastric cancerswith fast growth rates, as there is enhanced in vitrosensitivity of cell lines with doubling times under 30 h.
TA
BL
E1
Ch
ara
cte
ris
tics
of
Ga
stro
eso
ph
ag
ea
lC
an
cer
Cell
Lin
es
Cel
ln
am
eT
yp
ean
dd
eriv
ati
onT
urn
orfo
rmati
onM
ouse
mod
elA
dh
esio
nst
atu
sG
enet
icch
ara
cter
izati
ons
AG
SM
oder
ate
lyd
iffe
ren
tiate
dad
enoc
arc
inom
aE
BV
-F
lan
ktu
mor
Nu
de
mic
eL
owle
vel
ofE
-cad
her
inex
pre
sses
LI-
cad
her
inE
xp
ress
es:vil
lin
1L
GA
LS
4
OC
UM
-2M
D3
Sci
rrh
ous
poo
rly
dif
fere
nti
ate
dca
rcin
oma
ad
eriv
edfr
omO
CU
M-2
M
Per
iton
eal
dis
sem
inati
onN
ud
em
ice
Dow
n-r
egu
lati
onof
E-c
ad
her
inan
din
tegri
nb4
Dow
n-r
egu
lati
onof
squ
am
ous
cell
dif
fere
nti
ati
onm
ark
ergen
ecl
ust
erB
E3
Barr
ett’
ses
oph
agu
sass
ocia
ted
esop
hagea
lad
enoc
arc
inom
afr
omd
ista
les
oph
agu
s
Fla
nk
tum
orN
ud
em
ice
Un
kn
own
Exp
ress
es:p
Ikkb
(S181)
pT
SC
1(S
511)
p36K
1(T
389)
mem
ber
sof
the
infl
am
mati
onass
ocia
ted
sign
ali
ng
path
way
MK
N-1
Ad
enos
qu
am
ous
carc
inom
aes
tabli
shed
from
lym
ph
nod
em
etast
ase
s
Fla
nk
tum
orN
ud
em
ice
E-c
ad
her
insi
len
ced
by
pro
mot
erh
yp
erm
eth
yla
tion
Mis
sen
sem
uta
tion
ofp
53
MK
N-4
JP
oorl
yd
iffe
ren
tiate
dad
enoc
arc
inom
a,d
iffu
sety
pe
Per
iton
eal
dis
sem
inati
onN
ud
eS
CID
mic
eW
ild
typ
eall
ele
ofE
-cad
her
inlo
stC
EAþ
am
pli
fica
tion
ofc-
met
pro
to-o
nco
gen
ew
ild
typ
ep
53
exp
ress
eslo
wle
vel
sbcl
-2M
KN
-74
Inte
stin
al
typ
em
oder
ate
lyd
iffe
ren
tiate
dtu
bu
lar
ad
enoc
arc
inom
ad
eriv
edfr
omli
ver
met
ast
ase
s
Per
iton
eal
dis
sem
inati
onN
ud
eS
CID
mic
eN
ogen
etic
alt
erati
onto
E-c
ad
her
inC
EA
-wil
dty
pe
p53
doe
sn
otex
pre
ssbcl
-2
WONG ET AL.: HERPES VIRUS IS EFFECTIVE AGAINST GASTROESOPHAGEAL CANCER 219
Paradoxically, higher viral titers were achieved in thosecell lines with longer doubling times, indicating thatimmediate cytotoxicity may be detrimental to ultimateviral replication. It also indicates that while somereplication is important for viral spread and furtherinfection, a very high level of replication is notnecessary for complete killing of cancer.
Additionally, for cell lines with a predisposition forperitoneal dissemination, in particular the OCUM-2MD3 and MKN74 cell lines, this virus appears to beparticularly effective in killing. This may prove to beimportant clinically, as those patients with peritonealseeding have a high likelihood of recurrence.
CONCLUSION
This study demonstrates that a third-generation,modified, oncolytic herpesvirus can effectively infect,replicate within, and lyse gastroesophageal cancer cells.Cell lines that are fast growing with short doublingtimes, and cell lines that are particularly tumorigenicin the peritoneum proved to be the most susceptible.For those unfortunate patients who have metastatic dis-ease or recurrence from gastric cancer, this virus mayoffer a new therapeutic approach. These data would en-courage future clinical trials of this agent as palliativeand adjuvant therapies for gastroesophageal cancer.
REFERENCES
1. Alberts SR, Cervantes A, van de Velde CJH. Gastric cancer:Epidemiology, pathology and treatment. Ann Oncol 2003;14.ii31.
2. Kasuya H, Takeda S, Nomoto S, et al. The potential of oncolyticvirus therapy for pancreatic cancer. Cancer Gene Ther 2005;12:725.
3. Garcia M, Jemal A, Ward EM, et al. Global Cancer facts and fig-ures 2007. Atlanta, GA: American Cancer Society, 2007.
4. Yonemura Y, Bandou E, Kawamura T. Quantitative prognosticindicators of peritoneal dissemination of gastric cancer. Eur JSurg Oncol 2006;32:602.
5. Gretschel S, Siegel R, Estevez-Schwarz L, et al. Surgical Strate-gies for gastric cancer with synchronous peritoneal carcinomato-sis. Br J Surg 2006;93:1530.
6. Bonenkamp JJ, Hermans J, Sasako M, et al. Extended lymph-node dissection for gastric cancer. N Engl J Med 1999;340:908.
7. Hartgrink HH, van de Velde CJH, Putter H, et al. Extendedlymph node dissection for gastric cancer: Who may benefit? Finalresults of the randomized Dutch gastric cancer group trial. J ClinOncol 2004;22:2069.
8. Khan FA, Shukla AN. Pathogenesis and treatment of gastric car-cinoma: An up-date with brief review. J Cancer Res Ther 2006;2:196.
9. Ohashi M, Ueno H, Tanaka T, et al. Adenovirus mediated p53tumor suppressor gene therapy for human gastric cells in vitroand in vivo. Gut 1999;44:366.
10. Song TJ, Eisenberg DP, Adusumilli PS, et al. Oncolytic herpesviral therapy is effective in the treatment of hepatocellularcarcinoma cell lines. J Gastrointestinal Surg 2006;10:532.
11. Reid V, Yu Z, Schuman T, et al. Herpes oncolytic therapy ofsalivary gland tumors. Int J Cancer 2007;122:202.

JOURNAL OF SURGICAL RESEARCH: VOL. 163, NO. 2, OCTOBER 2010220
12. Kemeny N, Brown K, Covey A, et al. Phase I, open-label, dose-escalating study of a genetically engineered herpes simplexvirus, NV1020, in subjects with metastatic colorectal carcinomato the liver. Human Gene Ther 2006;17:1214.
13. Roizman B. The function of herpes simplex virus genes: A primerfor genetic engineering of novel vectors. Proc Natl Acad Sci USA1996;93:11307.
14. Everts B, Van der Poel HG. Replication-selective oncolytic vi-ruses in the treatment of cancer. Cancer Gene Ther 2005;12:141.
15. Liu BL, Robinson M, Han Z-Q, et al. ICP34.5 deleted herpes sim-plex virus with enhanced in colitic, immune stimulating, andanti-tumor properties. Gene Ther 2003;10:292.
16. Varghese S, Rabkin S. Oncolytic herpes simplex virus vectors forcancer virotherapy. Cancer Gene Ther 2002;9:967.
17. Bennett JJ, Kooby DA, Delman K, et al. Antitumor efficacy of re-gional oncolytic viral therapy for peritoneally disseminated can-cer. J Mol Med 2000;78:166.
18. Bennett JJ, Delman KA, Burt B, et al. Comparison of safety, de-livery, and efficacy of two oncolytic herpes viruses (G207 andNV1020) for peritoneal cancer. Cancer Gene Ther 2002;9:935.
19. Stanziale SF, Stiles BM, Bhargava A, et al. Oncolytic herpes sim-plex virus-1 mutant expressing green fluorescent protein can de-tect and treat peritoneal cancer. Human Gene Ther 2004;15:609.
20. Kaufman HL, Kim DW, Deraffele G, et al. Local and distant im-munity induced by intralesional vaccination with an oncolyticherpes virus encoding GM-CSF in patients with stage IIIc andIV melanoma. Ann Surg Oncol 2009;17:718.
21. Fong Y, Kim T, Bhargava A, et al. A herpes oncolytic virus can bedelivered via the vasculature to produce biologic changes inhuman colorectal cancer. Mol Ther 2009;17:389.
22. Simpson GR, Han Z, Wang Y, et al. Combination of a fusogenicglycoprotein, prodrug activation, and oncolytic herpes simplex
virus for enhanced local tumor control. Cancer Res 2006;66:4835.
23. Fu X, Tao L, Jin A, et al. Expression of a fusogenic membraneglycoprotein by an oncolytic herpes simplex virus potentiatesthe viral antitumor effect. Mol Ther 2003;7:748.
24. Hippo Y, Yashiro M, Ishii M, et al. Differential gene expressionprofiles of scirrhous gastric cancer cells with high metastatic po-tential to peritoneum or lymph nodes. Cancer Res 2001;61:889.
25. Ji J, Chen X, Leung SY, et al. Comprehensive analysis of thegene expression profiles in human gastric cancer cell lines.Oncogene 2002;21:6549.
26. Yen CJ, Izzo JG, Lee DF, et al. Bile acid exposure up-regulatestuberous sclerosis complex 1/mammalian target of rapamycinpathway in Barrett’s-associated esophageal adenocarcinoma.Cancer Res 2008;68:2632.
27. Yokozaki H. Molecular characteristics of eight gastric cancer celllines established in Japan. Pathol Int 2000;50:767.
28. Mitsuhashi Y, Inaba M, Sugiyama Y, et al. In vitro measurementof chemosensitivity of human small cell lung and gastric cancercell lines toward cell cycle phase-nonspecific agents under theclinically equivalent area under the curve. Cancer 2006;70:2540.
29. Altorki N, Schwartz GK, Blundell M, et al. Characterization ofcell lines established from human gastric-esophageal adenocar-cinomas biologic phenotype and invasion potential. Cancer 1993;72:649.
30. Feng RH, Zhu ZG, Li JF, et al. Inhibition of human telomerase inMKN-45 cell line by antisense hTR expression vector induces cellapoptosis and growth arrest. World J Gastroenterol 2002;8:436.
31. Nakamura K, Yashiro M, Matsuoka T, et al. A novel moleculartargeting compound as K-samII/FGF-R2 phosphorylation inhib-itor, Ki23057, for scirrhous gastric cancer. Gastroenterology2006;131:1530.