Embed Size (px)
Citation preview

Duration of drug action, which we define as thetime during which a pharmacodynamic effect
(or response) exceeds a nominal threshold, isan important concept in drug therapy. It provides a basisfor guiding dosing schedules, for predicting recoverytime (eg, for drugs in anesthesia), and for monitoringtherapeutic outcomes. However, despite this, attentionhas largely focused on quantifying or predicting phar-
macodynamic responses at specified intervals after dos-ing. Pharmacokinetic–pharmacodynamic models, forinstance, describe relations between dosage regimens,concentrations, and effects with time.1-4 Although suitedfor the purpose, they have not been used specifically toquantify the duration of drug action.It has been generally assumed that there is a log-
linear relation between the dose of drug and itsduration of action.5 This assumption is based onearly theoretical and empirical pharmacodynamicanalyses by Levy and colleagues,6-9 which werefocused on a few drugs with direct, reversible, mech-anisms of action that have single compartment phar-macokinetics. Mathematical derivations of therelation between dose and duration of action haveassumed plasma concentrations to decline monoex-ponentially for drugs with direct modes of action.5
For a bolus injection, the plasma concentration, C, is
From the Institute of Medical and Social Care Research, Bangor University,Bangor, North Wales, United Kingdom (Dr Hughes) and the Departmentof Primary Health Care, University of Oxford, Oxford, United Kingdom(Dr Aronson). Submitted for publication August 6, 2008; revised versionaccepted November 6, 2008. Address for correspondence: Dyfrig AHughes, Institute of Medical and Social Care Research, Dean Street, BangorUniversity, Bangor, North Wales LL57 1UT, United Kingdom; e-mail:[email protected]: 10.1177/0091270008329555
A Systematic Review and Empirical Analysisof the Relation Between Dose and Duration
of Drug Action
Dyfrig A. Hughes, PhD, MRPharmS, and Jeffrey K. Aronson, DPhil, FRCP
There is a log-linear relation between the dose and dura-tion of action of drugs with single-compartment pharma-cokinetics and direct, reversible mechanisms of action.However, it has been suggested that this relation does notextend to drugs whose metabolites are active or slowlyeliminated, drugs with saturable kinetics, and drugs withhit-and-run effects. The purpose of this study is to test thishypothesis and to quantify the relationship by way of asystematic review coupled to an empirical analysis. Allissues of 4 clinical pharmacology journals from 1980 to2005 are hand-searched for articles that present pharma-codynamic response versus time curves for 4 or more dif-ferent doses. Data on duration of action, dose, and areaunder the plasma concentration versus time curve fromzero to infinity (AUC) are abstracted and analyzed bypanel data regression modeling, with within-study fixedeffects. Duration of drug action is defined as the time dur-ing which a pharmacodynamic effect (or response)
exceeds a nominal threshold. The generalized models ofall observations from 33 publications, with duration ofaction as the dependent variable and the logarithm of thedose (or AUC) as the explanatory variable, yield signifi-cant log-linear relationships. The regressions for individ-ual studies are correctly specified in 27 cases; there areinsufficient data for analysis in 10 studies, and a log-linear specification is deemed inappropriate in 6.Analysis of published dose-ranging studies shows that theduration of action of a drug is directly proportional to thelogarithm of dose across a wide range of different drugs,extending a result that was previously documented forvery few compounds.
Keywords: Duration of drug action; pharmacokinetics;pharmacodynamics
Journal of Clinical Pharmacology, 2010;50:17-26© 2010 the American College of Clinical Pharmacology
J Clin Pharmacol 2010;50:17-26 17
REVIEW

a function of dose, the volume of distribution (V)and the elimination rate constant, k, and time, t:
C =Dose.e−kt
V
The duration of action, ∆, is defined as the timetaken for the concentration to decline to some mini-mally effective value, Cmin:
Cmin =Dose. e−k∆
V
Rearranging and taking the logarithms, we obtainan expression for ∆:
∆ =1K[In(Dose) – In(Cmin . V )] (1)
According to this expression, the duration ofaction is proportional to the reciprocal of the elimi-nation rate constant. However, for many drugs thereis a temporal dissociation between the pharmacoki-netic and pharmacodynamic profiles, which sug-gests that duration of action might not be readilypredicted from dose.1,3 In such cases, the relationbetween duration of action and dose is a complexfunction of pharmacodynamic as well as pharmacoki-netic parameters, which cannot be solved explicitly inpurely pharmacokinetic terms. Notable examplesof pronounced differences between the time-courseof plasma concentration and pharmacologicaleffect include drugs that act irreversibly, such asthe antiplatelet effects of acetylsalicylic acid10 andthe anti-acid secretory effect of H+/K+-adenosinetriphosphatase inhibitors,11 and drugs whose pharma-codynamic effects are indirect outcomes of theirpharmacologic mechanisms of action, such as the anti-coagulant effects of warfarin12 and adrenal suppressionby corticosteroids.4
The aim of the present analysis was to perform asystematic review of dose-ranging studies to deter-mine whether the hypothesis that the logarithm ofdose is related to duration of response can be gener-alized to a wide range of drugs.
METHODS
Data Collection
All issues published between January 1980 andOctober 2005 of 4 journals, Clinical Pharmacologyand Therapeutics, the British Journal of Clinical
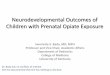
Pharmacology, Clinical Pharmacokinetics, and theEuropean Journal of Clinical Pharmacology, werehand-searched for articles that presented pharma-codynamic response versus time curves for 4 ormore different doses. This represented more than18 000 articles in 189 volumes. Studies wereincluded for analysis only if both the onset and off-set of response were measured. Figures werescanned electronically, and the data points weredigitized for determination of (x, y) coordinates,using TechDig 2.0 software (Jones, Mundelein, Ill).Duration of action was defined as above, and thevalue of the threshold effect was chosen such thatresponses for all doses intersected it during theonset and offset of effect. When possible, 3 suchthresholds were selected, to test whether the choiceof threshold influenced the result. This is illus-trated in Figure 1.When they were available, values of AUC (the
area under the plasma concentration versus timecurve from zero to infinity) for each dose werenoted. In other cases, figures were scanned electron-ically and digitized, and the linear trapezoidalmethod was used to calculate AUCt, the area fromzero to the last reported concentration, with extrap-olation to infinity by dividing the last concentrationby the terminal rate constant.
Statistical Analyses
To test the hypothesis that the duration of action waslinearly related to the logarithm of the dose, a panel
Figure 1. Depiction of pharmacodynamic response versus timecurves for a range of doses. For analytical purposes, the durationof response above a threshold response was determined, and 3such thresholds were selected when possible (eg, at a response of2, 4, and 6 units).
Duration of action (hours)
Pha
rmac
odyn
amic
resp
onse
Threshold response
110
1001000mg
0
2
4
6
8
10
0 10 20 30 40 50
HUGHES, ARONSON
18 • J Clin Pharmacol 2010;50:17-26

REVIEW 19
RELATION BETWEEN DOSE AND DURATION OF ACTION
data analysis was performed in Stata 10.0 (StataCorporation, Tex). The Hausman specification testwas used to test the appropriateness of a fixed orrandom-effects model.13 To standardize units, weconverted all doses, values of AUC, and durations ofaction to percentages of the lowest values in eachstudy. When more than 1 outcome measure was pre-sented for a given study drug, data on only 1 mea-sure were included in the regression analysis toavoid correlation between observations. This wasbased on selecting (1) outcomes that were objectivein their assessment (in preference to those that weremeasured subjectively) and (2) data for which morethan 1 threshold value could be determined. If morethan 1 set of observations per study remained, theoutcome for inclusion in the analysis was selected atrandom. However, a separate analysis in which alloutcome measures were included did not give a dif-ferent result.We tested 3 regression models, each founded on
equation 1:
1. For Model 1, all observations were included, usingduration of action (∆) as the dependent variable andthe natural logarithm of the dose, ln(dose), as theexplanatory variable (regression Model 1).
2. For Model 2, a second regression was used to testwhether the coefficient of ln(dose) was sensitive tothe choice of threshold. This was accomplished byintroducing dummy variables and interaction termsof ln(dose) with each threshold value.
3. Because data on AUC were not available for all stud-ies, for Model 3 ln(AUC) was used as the explana-tory variable for 1 threshold value only (the middleof 3 thresholds, when applicable).
Regressions were estimated by ordinary leastsquare, with 95% confidence intervals (CIs) basedon robust standard errors.For study i and threshold j, the models were spec-
ified as follows:Regression Model 1:
∆i = β1 In(dose)i + αi + εi
Regression Model 2 (multiple thresholds):
∆ij = β1In(dose)ij + β2Threshold1i + β3Threshold2i +β4In(dose).Threshold1i + β5In(dose).Threshold2i+ αi + εij
Regression Model 3 (single threshold):
∆i = β1 In (AUC)i + αi + εji
where β1 to β5 represent the coefficients to be esti-mated, αi represents the intercept, ε is the error term,and Threshold1 and Threshold2 are dummy vari-ables that represent the lower and middle thresholdsrespectively.In the simple pharmacokinetic expression repre-
sented by equation 1, β1 fromModel 1 is the reciprocalof the elimination rate constant, and –αi multipliedby the elimination rate constant and exponentiatedrepresents the total amount of drug needed in thebody to elicit the threshold response. However, inmore complex cases, β1 and αi represent functionsof pharmacokinetic and pharmacodynamic parame-ters that cannot be solved explicitly in standardpharmacokinetic terms.In Model 2, the intercepts and slopes are allowed
to vary by threshold. The intercept for the highest (ofthe 3) thresholds is given by αi, the intercept for themiddle threshold is αi + β3, and the intercept for thelower threshold is αi + β2. The null hypothesis is thatthe estimated coefficients β4 and β5 for the interactionterms equal zero. Rejecting the null hypothesis isinterpreted as meaning that the slope of duration ofaction with respect to ln(dose) is independent ofthreshold value.Separate regression analyses, which included
dummy variables and interaction terms, as specifiedin regression Model 2, were also conducted for eachindividual study. For these regressions, variableswere kept in their native units and not converted topercentages. The Ramsey RESET F test for modelspecification was used to test for differences of R2
under linear versus nonlinear assumptions.
RESULTS
We identified 33 articles that satisfied the inclusion cri-teria.14-46 Some articles presented more than 1 pharma-codynamic response,14-19 whereas others includeddifferent populations,20,21 or more than 1 drug,22
making 43 studies available for analysis (Table I). Ofthese, 9 studies were subsequently excluded from thepooled analysis (indicated in Table I) to eliminate cor-relation between outcome measures. In 32 studies, itwas possible to measure 3 pharmacodynamic thresh-olds. Values of AUC relating to parent compound, orfigures depicting the concentration–time profiles, fromwhich AUC values were estimated, were available for

Table I Summary of the Evidence on Duration of Drug Action, Together Withthe Results of Individual Regressions Specified by Model 2
No. of Dosesb (Route Parameter RamseyDrug Subjectsa of Administration) Observed R2 β1 (95% CI) F (P Value) Referencec
Midazolam 12 5,10,15,20 mg Leeds psychomotor 0.89 4.10 h NA 14(po) tester—reaction (–0.2, 8.4)
time (ms)Midazolamd 12 5, 10, 15, 20 mg Leeds psychomotor 0.92 2.83 h NA 14
(po) tester—critical (0.3, 5.4)flicker fusion (Hz)
Midazolamd 12 5, 10, 15, 20 mg Drowsiness—visual 0.15 1.06 h NA 14(po) analogue rating (–6.7, 8.9)
scale (mm)Ro 48-6791 10 0.3, 1, 2, 3 mg Saccadic peak 0.94 1.48 h 2.09 15
(iv) velocity (°/s) (0.8, 2.2) (.2801)Ro 48-6791d 10 0.3, 1, 2, 3 mg (iv) EEGβ power (µV) 0.90 1.11 h NA 15
(–0.0, 2.2)Sibrafiban 49 5, 7, 10, 12 mg ADP-induced platelet 0.97 9.32 h 0.13 16
(po) aggregation (4.3, 14.3) (.9359)(% inhibition)
Sibrafiband 49 5, 7, 10, 12 mg TRAP-induced 0.97 9.74 h 0.07 (.97) 16(po) platelet aggregation (6.8, 12.7)
(% inhibition)Milnaciprand 12 50, 100, 200, 400 5-HT uptake (% 0.88 9.53 h 0.19 17
mg (po) inhibition) (2.0, 17.1) (.8959)Milnacipran 12 100, 200, 300, Noradrenaline 0.93 6.88 h 0.84 17
400 mg (po) (norepinephrine) (1.9, 11.8) (.5537)uptake (%inhibition)
Formoterold 20 12, 24, 48, 96 µg QTc interval (ms) 0.82 3.44 h NA 18(inh) (–1.5, 8.4)
Formoterol 20 12, 24, 48, 96 µg Blood glucose 0.96 0.90 h 28.03 18(inh) (mmol/L) (0.6, 1.2) (.0107)
Isosorbide 12 15, 30, 60, Systolic blood 0.75 2.56 h NA 19dinitrated 120 mg (po) pressure (mm Hg) (–1.9, 7.1)
Isosorbide 12 15, 30, 60, 120 Pulse rate (/min) 0.94 0.50 h NA 19dinitrate mg (po) (0.1, 0.9)
Recombinant 32 450, 900, 1350, Reticulocytes (%) 0.96 4.04 days 3.55 20erythropoietind 1800 IU/kg (sc) (2.1, 6.0) (.1627)
Recombinant 30 300, 600, 1200, Reticulocytes (%) 0.81 2.07 days 3.88 20erythropoietin 2400 IU/kg (sc) (–0.6, 4.7) (.1476)
MK-0434 8 0.1, 1, 10, 50 Testosterone 0.58 –0.46 h 0.73 21mg (po) concentration (–2.8, 1.9) (.5976)
(% change frombaseline)
MK-0434d 8 0.5, 5, 25, 100 Testosterone 0.07 –0.90 h NA 21mg (po) concentration (–11.2, 9.4)
(% change frombaseline)
Buprenorphine 4 1, 2, 4, 8, 16, Pupillary 0.92 20.35 h ) 23.39 2232 mg (sl) constriction (mm) (11.9, 28.8) (.0003)
Methadone 5 15, 30, 45, 60 Pupillary 0.94 25.10 h 18.96 22hydrochloride mg (po) constriction (mm) (12.5, 37.7) (.0187)
(continued)
20 • J Clin Pharmacol 2010;50:17-26
HUGHES, ARONSON

Table I (continued)
No. of Dosesb (Route Parameter RamseyDrug Subjectsa of Administration) Observed R2 β1 (95% CI) F (P Value) Referencec
Alfentanil 10 23, 30, 43, Pupil diameter 0.99 2.67 h 2.61 2375 µg/kg (po) change (mm) (2.1, 3.3) (.2261)
Tolcapone 48 5, 10, 25, 50, 100, COMT activity 0.94 2.83 h 1.87 24200, 400, 800 mg (po) (% baseline) (2.2, 3.5) (.1936)
SQ 28,668 56 25, 50, 100, 200, 400, Fractional inhibition 0.88 2.72 h 0.23 25800, 1200 mg (po) of TxA2 (1.2, 4.3) (.873)
Zilfrosilone 54 10, 30, 60, 90, 120, Erythrocyte 0.91 4.24 h 1.18 26150, 200, 250, acetylcholinesterase (2.3, 6.2) (.3558)300 mg (po) activity (%
inhibition)Ibuprofen 40 8, 10, 12, 14 Basal TxB2 0.84 2.34 h 7.97 27
mg/kg (po) concentration (–0.6, 5.3) (.061)(pg/mL)
Z13752A 8 50, 100, 200, 400, Serum ACE activity 0.95 12.99 h 0.80 (.527) 28600, 800 mg (po) (% predose values) (9.8, 16.2)
Lamivudine 24 5, 20, 100, 300, Hepatitis B DNA (% 0.63 3.1 days 15.46 29600 mg/day (po) change from (–2.1, 8.3) (.00031)
baseline)Cilazapril 24 0.5, 1, 2.5, 5 mg (po) Plasma ACE activity 0.98 7.87 h 0.8 30
(% inhibition) (4.1, 11.7) (.5692)Tolcapone 42 50, 100, 200, 400, COMT activity 0.94 3.85 h 3.2 31
800 mg (po) (% baseline) (3.0, 4.7) (.0764)
AMD3100 29 40, 80, 160, 240 White blood cell 0.97 8.12 h 1.73 32µg/kg (sc) count (cells/µL) (5.7, 10.5) (.3315)
Ibandronate 124 0.25, 0.5, 1, uCTX (% change) 0.93 24.39 days NA 332 mg (iv) (4.0, 44.8)
Entacapone 12 5, 25, 50, 100, 200, COMT activity 0.91 0.92 h 38.21 34400, 800 mg (po) (% inhibition) (0.4, 1.4) (.0000)
h-GRF-I-44-NH2 7 10, 20, 40, 80 µg (iv) Plasma growth 0.97 0.35 h 8.04 35hormone (0.2, 0.5) (.0603)concentration (µg/L)
Cicaprost 6 5, 10, 15, 20 µg (po) ADP-induced 0.98 0.95 h 1.25 36platelet aggregation (0.6, 1.3) (.4295)(% inhibition)
BIA 3-202e 18 50, 100, 200, COMT activity 0.96 1.66 h 1.64 37400 mg (po) (pmol/mg/protein/h) (0.8, 2.5) (.3468)
Dexmedetomidine 5 12.5, 25, 50, 75 µg (iv) Growth hormone 0.98 0.96 h 0.47 38secretion (µg/L) (0.7, 1.2) (.7242)
Bradykinin 23 1, 10, 100, 1000, Normalized pain 0.99 8.22 s 0.74 3910000 pmol (id) ratings (6.9, 9.5) (.5744)
Perindopril 18 2, 4, 8, 16 mg (po) Plasma ACE 0.91 9.05 h 0.98 40activity (% control) (0.3, 17.7) (.5073)
Benazepril 74 5, 10, 20, 40 Diastolic blood 0.72 –3.69 h 0.11 41hydrochloride mg (po) pressure (mm Hg) (–10.0, 2.6) (.947)
Dexmedetomidine 5 12.5, 25, 50, 75 µg (iv) Growth hormone 0.98 0.96 h 0.47 38secretion (µg/L) (0.7, 1.2) (.7242)
Bradykinin 23 1, 10, 100, 1000, Normalized pain 0.99 8.22 s 0.74 3910000 pmol (id) ratings (6.9, 9.5) (.5744)
Perindopril 18 2, 4, 8, 16 mg (po) Plasma ACE 0.91 9.05 h 0.98 40activity (% control) (0.3, 17.7) (.5073)
(continued)
RELATION BETWEEN DOSE AND DURATION OF ACTION
REVIEW 21

22 • J Clin Pharmacol 2010;50:17-26
HUGHES, ARONSON
Table I (continued)
No. of Dosesb (Route Parameter RamseyDrug Subjectsa of Administration) Observed R2 β1 (95% CI) F (P Value) Referencec
Benazepril 74 5, 10, 20, 40 Diastolic blood 0.72 –3.69 h 0.11 41hydrochloride mg (po) pressure (mm Hg) (–10.0, 2.6) (.947)
RHC3659 15 5, 10, 20, 40, Plasma ACE 0.98 1.79 h 1.92 4280 mg (po) activity (1.5, 2.1) (.2274)
(nmol/mL/min)Meptazinol 10 50, 100, 150, Pain threshold 0.95 2.04 h NA 43
200 mg (po) (mA change (0.5, 3.5)from placebo)
Dobutamine 6 3.2, 4.8, 6, 7.2, Systolic blood 0.97 3.97 min 6.71 449, 10.8, 12.2 pressure (mm Hg) (2.5, 5.5) (.0113)µg/kg (iv)
Bisoprolol 36 5, 10, 20, Pulse rate (% change 0.90 3.23 h NA 4540 mg (po) from baseline) (–0.0, 6.5)
Cilazapril 14 1.25, 2.5, 5, Plasma ACE activity 1.00 0.68 h 0.32 (.8157) 4610 mg (po) (nmol/mL/min) (–1.7, 3.0)
CI, confidence interval; po, orally; NA, not applicable; iv, intravenously; EEGβ, Electroencephalographic beta waves; ADP, adenosine 5′-diphosphate; TRAP,thrombin receptor agonist peptide; inh, inhaled; sc, subcutaneously; sl, sublingually; COMT, catechol-O-methyltransferase; TxA2, thromboxane A2; TxB2,thromboxane B2; ACE, angiotensin-converting enzyme; uCTX, urinary excretion of the C-telopeptide of the α chain of type I collagen; id, intradermally.a. All studies, other than Burgess et al,18 Thadani et al,19 Johnson et al,29 Pillai et al,33 and Weinberger et al,41 were conducted in healthy volunteers.b. In all studies, other than Johnson et al,29 single doses of drugs were administered; lamivudine was administered daily for 4 weeks.29
c. Some articles have more than 1 entry, to include different pharmacodynamic responses, different drugs, or different populations.d. These studies were excluded from the pooled analyses on the basis that other outcome measures are likely to be highly correlatede. BIA 3-202 was given in addition to levodopa 100 mg and benserazide 25 mg.
28 studies in 21 articles.15-17,19-20,22-37 For 1 study the con-centrations used to calculate AUC were those of theactive metabolite.16
Significance of the Hausman test confirmed theappropriateness of specifying the panel data regres-sion models with within-study fixed effects. Thegeneralized model (Model 1) of all pooled observa-tions, specified with the logarithm of the dose as theexplanatory variable, yielded a positive and significantβ coefficient of 1.06 (95% CI = 0.90, 1.23) (Table II).This suggests that there is, on average, a positiverelation between duration of action and the loga-rithm of the dose. However, it does not indicatewhether this relation is linear in nature or whetherit is applicable to all of the investigated drugs.After restricting the analysis to those studies in
which 3 threshold values were available (Model 2),we found that neither the differential interceptnor any of the differential slope coefficients werestatistically significant (Table II), suggesting thatthe coefficient of ln(dose), β1, is independent of thethreshold value. The regression coefficient for thelogarithm of AUC in Model 3 was positive and sig-nificant: 2.12 (95% CI = 1.69, 2.55).The pooled analyses, although allowing us to test
for a general hypothesis, do not allow for testing ofmodel specification error, nor do they result in
meaningful values of the beta coefficients. Theresults of the individual study regressions are pre-sented in Table I. Twenty-seven studies were speci-fied correctly (nonsignificant Ramsey RESET test).Insufficient data points precluded application of thetest in 10 studies, and the use of a linear regressionmodel was deemed inappropriate in 6 studies. Thewide confidence intervals around the β coefficientsreflect the limited number of data points for eachstudy, which is dictated by the number of dosesassessed. Plots of individual weighted residuals ver-sus predictions, and observed versus predicteddurations of action, are shown in Figure 2.
DISCUSSION
It has been more than 40 years since Levy et al6-9
showed that duration of action is directly propor-tional to the logarithm of dose for drugs that areadministered intravenously and have direct andreversible pharmacological effects. However, theiranalyses were limited to a handful of drugs. We havebeen unable to identify any subsequent systematicanalyses or model-based analyses that documentthis relation. We therefore tested this hypothesis fora larger number of drugs. Our analysis extends thenotion that duration of action is proportional to the

RELATION BETWEEN DOSE AND DURATION OF ACTION
REVIEW 23
logarithm of dose to a wide range of drugs with vary-ing mechanisms of action.The studies identified from the literature review
included a range of routes of administration, drugsthat are metabolized to pharmacologically activecompounds, drugs that are associated with nonlin-ear and/or multicompartmental pharmacokinetics,and drugs that have indirect mechanisms of action.Cilazapril and benazepril, for instance, have biexpo-nential kinetics and are metabolized to active com-pounds,30,47 benazepril being a prodrug.41 The 5α-reductase inhibitor MK-0434 and SQ 28,668, astructural analogue of thromboxane A2, both havenonlinear kinetics.21,24 Methadone not only inducesits own metabolism48 but also is subject to tolerance,as is buprenorphine.22 In all these cases there was alog-linear relation between dose and duration ofaction. These observations contradict Levy and col-leagues’ original view that such relationships wouldnot be seen with drugs whose metabolites are activeor are slowly eliminated, drugs with saturable kinet-ics, and drugs with hit-and-run effects.9
We recognize a distinction between pharmacologicaleffects (the actions of drugs at the molecular level)and pharmacodynamic outcomes (effects at higher lev-els, such as cellular, organ, or whole-body effects).However, we have not distinguished between the vari-ous hierarchical levels of these effects. Orders of magni-tude of differences in the rates of change of responsewould be expected at the various levels. A subgroupanalysis for the various pharmacodynamic levels ofeffect might have provided further insight into theobserved relation; however, there were too few studiesto allow this.Our analysis suggests that proportionality between
duration of action and the logarithm of dose is main-tained, irrespective of the choice of pharmacodynamicthreshold. However, the model was misspecified in 6
Table II Results of Fixed-Effect, Panel Regression Models
Regression 1 Regression 2 Regression 3
Constant –3.134 (–4.021, –2.246) –3.212 (–4.426, –1.999) –7.641 (–9.917, –5.366)ln(dose) 1.002 (0.856, 1.148) 1.007 (0.809, 1.204)ln(AUC) 1.971 (1.560, 2.383)Threshold1 0.801 (–0.735, 2.338)Threshold2 0.120 (–1.433, 1.673)ln(dose)·threshold1 –0.163 (–0.412, 0.087)ln(dose)·threshold2 –0.050 (–0.301, 0.202)Overall R2 0.165 0.208 0.025F 182 (P < .0000) 40 (P < .0000) 91 (P < .0000)
Regression Models 1 to 3 are described in the Methods section. The dependent variable is specified as the duration of drug action in each case. Thecoefficients for each explanatory variable are presented with the 95% confidence interval.
Figure 2. Individual predictions versus observed durations ofaction (the line is the line of identity) and individual standardresiduals versus individual predictions.
0
25
50
75
100
0 25 50 75 100
Observations (hr)
Ind
ivid
ual
pre
dic
tio
ns
(hr)
–3
–2
–1
0
1
2
3
0 25 50 75 100
Individual predictions (hr)
Ind
ivid
ual
stan
dar
dre
sid
ual
s

24 • J Clin Pharmacol 2010;50:17-26
HUGHES, ARONSON
studies.18,22,29,34,44 In 3 cases, the duration of action at thehighest dose appeared to deviate from the log-linearrelationship.18,34,44 In the remainder, the data wereinconsistent with a dose-response relation, in that forcertain levels of response, a lower dose yielded a moresustained effect than a higher dose.24,29
The use of panel data regression models with fixedeffects was appropriate for assessing the generalizedhypothesis, because these models take into account thefact that the error termsmay be correlatedwith the indi-vidual study effects.13 Fixed-effects regression modelsassume that the unobserved variables (eg, subject-specific characteristics) differ between studies but areconstant across doses within each study. The pooledanalyses, however, result in sample-averaged estimatorsthat may not be readily interpreted. Furthermore, thereis no statistical test for specification for panel dataanalysis. Hence, separate regressions for individualstudies were conducted to provide both relevant coeffi-cient estimators and an indication of model misspecifi-cation. In some instances, however, the test for modelspecification would not operate because of low num-bers of observations. This was a consequence of notbeing able to quantify duration of action for more than1 threshold in some cases.The overall R2 for each regression model appears
to suggest that only a small proportion of the vari-ability in duration of drug action is explained by thelogarithm of dose (or AUC). However, in panel datamodels, the explanatory effects of the interceptterms are removed, thereby resulting in low valuesof R2. By way of comparison, a linear regressionspecified in the same way as Model 1 but withdummy variables for each study results in an R2 of0.62. Here the explanatory effects of the intercept arepreserved.Some limitations to the empirical analysis will
have affected the robustness of these findings. Forpractical reasons, articles were selected from only 4journals, albeit major ones. We may therefore havemissed other studies that would have satisfied theinclusion criteria. However, it was not possible toidentify appropriate studies through electronicmeans, which posed a major constraint on the iden-tification of evidence. A limit of 4 journals wastherefore imposed. We believe that in surveying18 000 articles we are likely to have detected a largeenough corpus of data to allow our findings to begeneralized.The method used to quantify duration of action and
the nature of the data generated were also potentialsources of bias. Analysis of time points from digitizedimages may result in systematic error, although it is
more likely to reduce precision than accuracy, andanalysis of mean values is less robust than analysis ofindividual data points.These limitations could have been mitigated had
it been possible to conduct a complete systematicreview of all articles and a meta-analysis of individ-ual patient data. Clearly that was not feasible.The evaluated studies were not designed to mea-
sure duration of drug action. Pharmacological effectsor responses were reported at prespecified timepoints, rather than time being reported at prespeci-fied thresholds of effect. This represents a weaknessin the published literature; effect- or biomarker-controlled trials48 would be more appropriate for thepurposes of this type of analysis.Despite its limitations, this is to our knowledge the
first systematic review of dose-ranging studies thatreported pharmacodynamic effects versus time sincethe work of Levy and Gibaldi in 1972.9 One practicaloutcome of the relation that is described is in guidingdosage selection according to the desired intensity andduration of action. If the duration of action of the dosethat produces a specified effect is ∆s, the dose requiredto produce this duration of action, Ds, is given by Ds =exp[( ∆s − αs)/β1]. Because we have shown that β1 isconstant for a given drug and is independent of dose orchoice of threshold response, comparison of valuesof β1 among drugs with common pharmacodynamicend points provides a useful measure of the allowablemargin of effective dosing interval. It represents theabsolute change in duration of action per percentageunit change in dose. The β1 value for the activity ofplasma angiotensin-converting enzyme (ACE) (percent-age inhibition) associated with cilazapril, for instance,is 7.9 hours, compared with 9.1 hours with perindo-pril. This suggests that the relative increase in durationof action per percentage unit increase in dose is higherfor perindopril, and this is supported by evidence onACE inhibition and blood pressure control from a com-parative study of the 2 agents.49
We have confirmed that there is a good relationbetween the duration of action of a drug and the loga-rithm of dose and have shown that this relationshipextends beyond drugs with the characteristics that Levyspecified. This suggests that during drug development,these relationships might be of use in establishingdosing regimens and predicting, by extrapolation, thedurations of action of specific doses. This work demon-strates the usefulness of studying the time courses ofeffects of drugs—an aspect of pharmacology that islargely neglected.
Financial disclosure: None declared.

RELATION BETWEEN DOSE AND DURATION OF ACTION
REVIEW 25
REFERENCES
1. Gabrielsson J, Weiner D. Pharmacokinetics and Pharmacody-namic Data Analysis: Concepts and Applications. Stockholm:Swedish Pharmaceutical Press; 2002.2. Derendorf H, Hochhaus G. Handbook of Pharmacokinetic/Pharmacodynamic Correlation. Boca Raton, FL: CRC Press; 1995.3. Mager DE, Wyska E, Jusko WJ. Diversity of mechanism-based pharmacodynamic models. Drug Metab Dispos. 2003;31:501-508.4. Jusko WJ, Ko HC. Physiologic indirect response models charac-terize diverse types of pharmacodynamic effects. Clin PharmacolTher. 1994;56:406-419.5. Rowland M, Tozer TN. Clinical Pharmacokinetics: Conceptsand Applications. 3rd ed. Media, PA: Lippincott Williams &Wilkins; 1995.6. Levy G, Nelson E. Theoretical relationship between dose, elim-ination rate, and duration of pharmacological effect of drugs.J Pharm Sci. 1965;54:812.7. Levy G. Kinetics of pharmacologic effects. Clin PharmacolTher. 1966;7:362-372.8. Levy G. Relationship between elimination rate of drugs andrate of decline of their pharmacologic effects. J Pharm Sci. 1964;53:342-343.9. Levy G, Gibaldi M. Pharmacokinetics of drug action. Annu RevPharmacol. 1972;12:85-98.10. Cahill RA, McGreal GT, Crowe BH, et al. Duration of increasedbleeding tendency after cessation of aspirin therapy. J Am CollSurg. 2005;200:564-573.11. Bell N, Karol MD, Sachs G, Greski-Rose P, Jennings DE, HuntRH. Duration of effect of lansoprazole on gastric pH and acidsecretion in normal male volunteers. Aliment Pharmacol Ther.2001;15:105-113.12.Nagashima R, O’Reilly RA, Levy G. Kinetics of pharmacologiceffects in man: the anticoagulant action of warfarin. Clin PharmacolTher. 1969;10:22-35.13.Wooldridge JM. Econometric Analysis of Cross Section andPanel Data. Cambridge, MA: MIT Press; 2002.14. Gudgeon AC, Hindmarch I. Midazolam: effects on psychomotorperformance and subjective aspects of sleep and sedation in normalvolunteers. Br J Clin Pharmacol. 1983;16(suppl 1):121S-126S.15. Dingemanse J, van Gerven JM, Schoemaker RC, et al.Integrated pharmacokinetics and pharmacodynamics of Ro 48-6791, a new benzodiazepine, in comparison with midazolam dur-ing first administration to healthy male subjects. Br J ClinPharmacol. 1997;44:477-486.16.Wittke B, Mackie IJ, Machin SJ, Timm U, Zell M, Goggin T.Pharmacokinetics and pharmacodynamics of Ro 44-3888 aftersingle ascending oral doses of sibrafiban, an oral platelet aggrega-tion inhibitor, in healthy male volunteers. Br J Clin Pharmacol.1999;47:521-530.17. Palmier C, Puozzo C, Lenehan T, Briley M. Monoamine uptakeinhibition by plasma from healthy volunteers after single oraldoses of the antidepressant milnacipran. Eur J Clin Pharmacol.1989;37:235-238.18. Burgess C, Ayson M, Rajasingham S, Crane J, Della Cioppa G,Till MD. The extrapulmonary effects of increasing doses of for-moterol in patients with asthma. Eur J Clin Pharmacol. 1998;54:141-147.
19. Thadani U, Fung HL, Darke AC, Parker JO. Oral isosorbidedinitrate in angina pectoris: comparison of duration of action anddose-response relation during acute and sustained therapy. Am JCardiol. 1982;49:411-419. Cited in Thadani U, Whitsett T.Relationship of pharmacokinetic and pharmacodynamic proper-ties of the organic nitrates. Clin Pharmacokinet. 1988;15:32-43.20. Cheung WK, Goon BL, Guilfoyle MC, Wacholtz MC. Pharma-cokinetics and pharmacodynamics of recombinant human ery-thropoietin after single and multiple subcutaneous doses tohealthy subjects. Clin Pharmacol Ther. 1998;64:412-423.21. Van Hecken A, Depre M, Schwartz JI, et al. Plasma concentra-tions and effect on testosterone metabolism after single dosesof MK-0434, a steroid 5 alpha-reductase inhibitor, in healthysubjects. Eur J Clin Pharmacol. 1994;46:123-126.22.Walsh SL, Preston KL, Stitzer ML, Cone EJ, Bigelow GE.Clinical pharmacology of buprenorphine: ceiling effects at highdoses. Clin Pharmacol Ther. 1994;55:569-580.23. Kharasch ED, Hoffer C, Walker A, Sheffels P. Disposition andmiotic effects of oral alfentanil: a potential noninvasive probe forfirst-pass cytochrome P450 3A activity. Clin Pharmacol Ther.2003;73:199-208.24. Dingemanse J, Jorga KM, Schmitt M, et al. Integrated pharma-cokinetics and pharmacodynamics of the novel catechol-O-methyltransferase inhibitor tolcapone during first administra-tion to humans. Clin Pharmacol Ther. 1995;57:508-517.
25. Friedhoff LT, Manning J, Funke PT, et al. Quantitation of druglevels and platelet receptor blockade caused by a thromboxaneantagonist. Clin Pharmacol Ther. 1986;40:634-642.
26. Cutler NR, Seifert RD, Schleman MM, et al. Acetyl-cholinesterase inhibition by zilfrosilone: pharmacokinetics andpharmacodynamics. Clin Pharmacol Ther. 1995;58:54-61.
27. Longenecker GL, Swift IA, Bowen RJ, Beyers BJ, Shah AK.Kinetics of ibuprofen effect on platelet and endothelial prostanoidrelease. Clin Pharmacol Ther. 1985;37:343-349.
28. Bani M, Colantoni A, Guillaume M, Macchi F, Moroni G,Persiani S. A double-blind, placebo-controlled study to assess tol-erability, pharmacokinetics and preliminary pharmacodynamicsof single escalating doses of Z13752A, a novel dual inhibitor ofthe metalloproteases ACE and NEP, in healthy volunteers. Br JClin Pharmacol. 2000;50:338-349.
29. Johnson MA, Moore KH, Yuen GJ, Bye A, Pakes GE. Clinicalpharmacokinetics of lamivudine. Clin Pharmacokinet. 1999;36:41-66.
30.Massarella J, DeFeo T, Lin A, Limjuco R, Brown A. The phar-macokinetics and dose proportionality of cilazapril. Br J ClinPharmacol. 1989;27(suppl 2):199S-204S.
31. Dingemanse J, Jorga K, Zurcher G, et al. Pharmacokinetic–pharmacodynamic interaction between the COMT inhibitor tol-capone and single-dose levodopa. Br J Clin Pharmacol. 1995;40:253-262.
32. Lack NA, Green B, Dale DC, et al. A pharmacokinetic–pharmacodynamic model for the mobilization of CD34+ hematopoi-etic progenitor cells by AMD3100. Clin Pharmacol Ther. 2005;77:427-436.
33. Pillai G, Gieschke R, Goggin T, Jacqmin P, Schimmer RC,Steimer JL. A semimechanistic and mechanistic populationPK-PD model for biomarker response to ibandronate, a newbisphosphonate for the treatment of osteoporosis. Br J ClinPharmacol. 2004;58:618-631.

26 • J Clin Pharmacol 2010;50:17-26
HUGHES, ARONSON
34. Keranen T, Gordin A, Karlsson M, et al. Inhibition of solublecatechol-O-methyltransferase and single-dose pharmacokineticsafter oral and intravenous administration of entacapone. Eur JClin Pharmacol. 1994;46:151-157.35. Boissel JP, Cohen R, Biot-Laporte S, et al. Synthetic humangrowth hormone releasing factor (h-GRF-I-44-NH2) dose responseeffect on growth hormone and prolactin secretion in healthy adultmen. Eur J Clin Pharmacol. 1986;29:609-614.36. Hildebrand M, Staks T, Nieuweboer B. Pharmacokinetics andpharmacodynamics of cicaprost in healthy volunteers after oraladministration of 5 to 20 micrograms. Eur J Clin Pharmacol.1990;39:149-153.37. Silveira P, Vaz-da-Silva M, Almeida L, et al. Pharmacokinetic–pharmacodynamic interaction between BIA 3-202, a novel COMTinhibitor, and levodopa/benserazide. Eur J Clin Pharmacol. 2003;59:603-609.38. Kallio A, Scheinin M, Koulu M, et al. Effects of dexmedeto-midine, a selective α2-adrenoceptor agonist, on haemodynamiccontrol mechanisms. Clin Pharmacol Ther. 1989;46:33-42.39.Manning DC, Raja SN, Meyer RA, Campbell JN. Pain andhyperalgesia after intradermal injection of bradykinin in humans.Clin Pharmacol Ther. 1991;50:721-729.40. Bussien JP, d’Amore TF, Perret L, et al. Single and repeateddosing of the converting enzyme inhibitor perindopril to normalsubjects. Clin Pharmacol Ther. 1986;39:554-558.41.Weinberger MH, Black HR, Lasseter KC, et al. Diurnal bloodpressure in patients with mild-to-moderate hypertension treatedwith once daily benazepril hydrochloride. Clin Pharmacol Ther.1990;47:608-617.
42. Burnier M, Turini GA, Brunner HR, et al. RHC 3659: a neworally active angiotensin converting enzyme inhibitor in normalvolunteers. Br J Clin Pharmacol. 1981;12:893-899.43. Gabka J, Price RK. Tooth pulp stimulation: a method of deter-mining the analgesic efficacy of meptazinol in man. Br J ClinPharmacol. 1982;14:104-106.44. Pousset F, Chalon S, Thomare P, Diquet B, Lechat P. Evaluationof cardiac beta 1-adrenergic sensitivity with dobutamine in healthyvolunteers. Br J Clin Pharmacol. 1995;39:633-639.45. Leopold G, Ungethum W, Pabst J, Simane Z, Buhring KU,Wiemann H. Pharmacodynamic profile of bisoprolol, a new beta1-selective adrenoceptor antagonist. Br J Clin Pharmacol. 1986;22:293-300.46. Burnier M, Mooser V, Nussberger J, Waeber B, Brunner HR.Correlation between plasma concentration of cilazapril andhaemodynamic and hormonal effects in healthy man. Br J ClinPharmacol. 1989;27(suppl 2):189S-197S.47. Garrido MJ, Troconiz IF. Methadone: a review of its pharma-cokinetic/pharmacodynamic properties. J Pharmacol ToxicolMethods. 1999;42:61-66.48. Grahnen A, Karlsson MO. Concentration-controlled or effect-controlled trials: useful alternatives to conventional dose-controlled trials? Clin Pharmacokinet. 2001;40:317-325.49. Louis WJ, Conway EL, Krum H, et al. Comparison of the phar-macokinetics and pharmacodynamics of perindopril, cilazapriland enalapril. Clin Exp Pharmacol Physiol. 1992;19(suppl):55-60.


















![Frequency of Prolonged Remission Duration after High-Dose ......[CANCER RESEARCH 58. 4173-4179. September 15. 1998] Frequency of Prolonged Remission Duration after High-Dose Cytarabine](https://img.pdfslide.us/doc/110x75/5ff130819dc4c84faf6cc524/frequency-of-prolonged-remission-duration-after-high-dose-cancer-research.jpg)








