Embed Size (px)
Citation preview

A survey on luteal‐phase support:An IVF Worldwide Survey results
I have no conflict of interest!

The reason why luteal phase support is needed:
The normal physiological support of the corpus luteum—the pulsatile secretion of LH by the anterior pituitary—is disrupted during controlled ovarian stimulation
Mid‐luteal LH levels
~ 6.0 IU/l in natural cycle (Tavaniotou and Devroey 2003)
~ 1.5 IU/l ‐ GnRHa trigger (Humaidan et al. 2005)
~ 0.2 IU/l – HCG trigger (Humaidan et al. 2005)
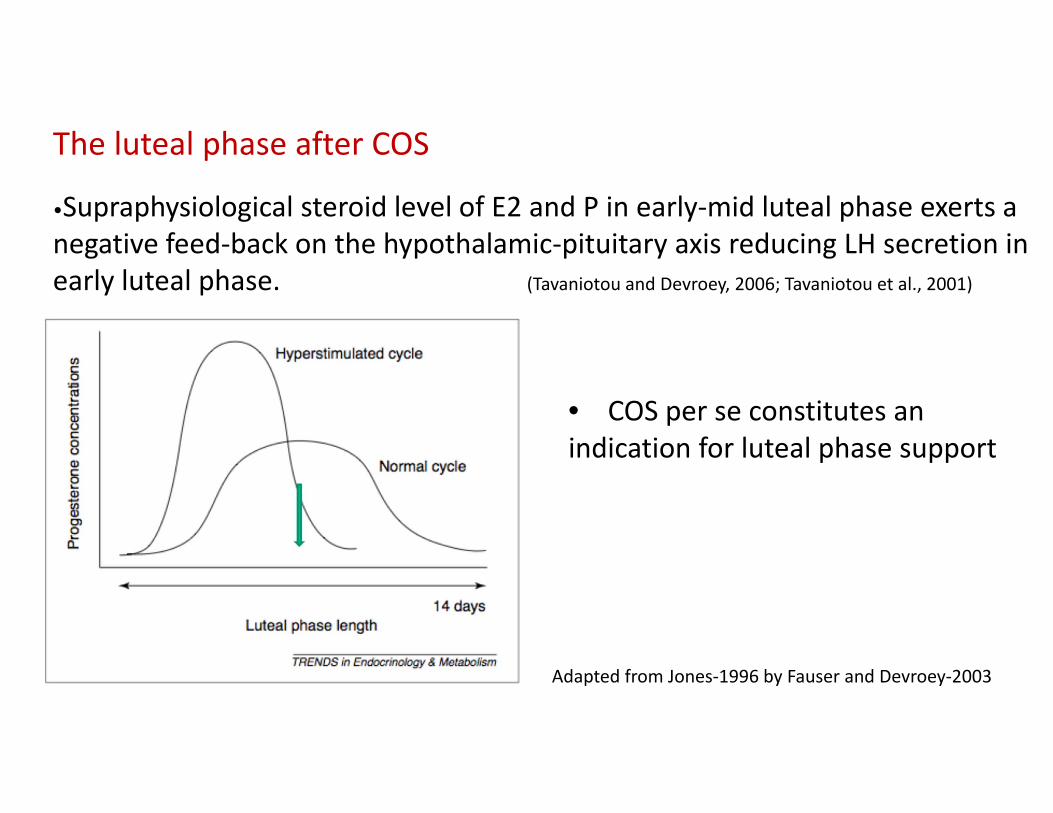
The luteal phase after COS
•Supraphysiological steroid level of E2 and P in early‐mid luteal phase exerts a negative feed‐back on the hypothalamic‐pituitary axis reducing LH secretion in early luteal phase. (Tavaniotou and Devroey, 2006; Tavaniotou et al., 2001)
Adapted from Jones‐1996 by Fauser and Devroey‐2003
• COS per se constitutes anindication for luteal phase support

Weissman et al., Gynecol Endocrinol 10; 273‐6: 1996.
Pharmacokinetics of hCG administration

Figure 1
De Ziegler et al., Fertility and Sterility 2018 109, 749-755
Chronologic characteristics of the effects of exogenous hCG and hCG produced by the conceptus

Luteal phase support in ART
• Formulation and route of administration
• When to start?
• When to stop?
• What should be included?
• Should LPS in ART be individualized?

Evidence Based Medicine
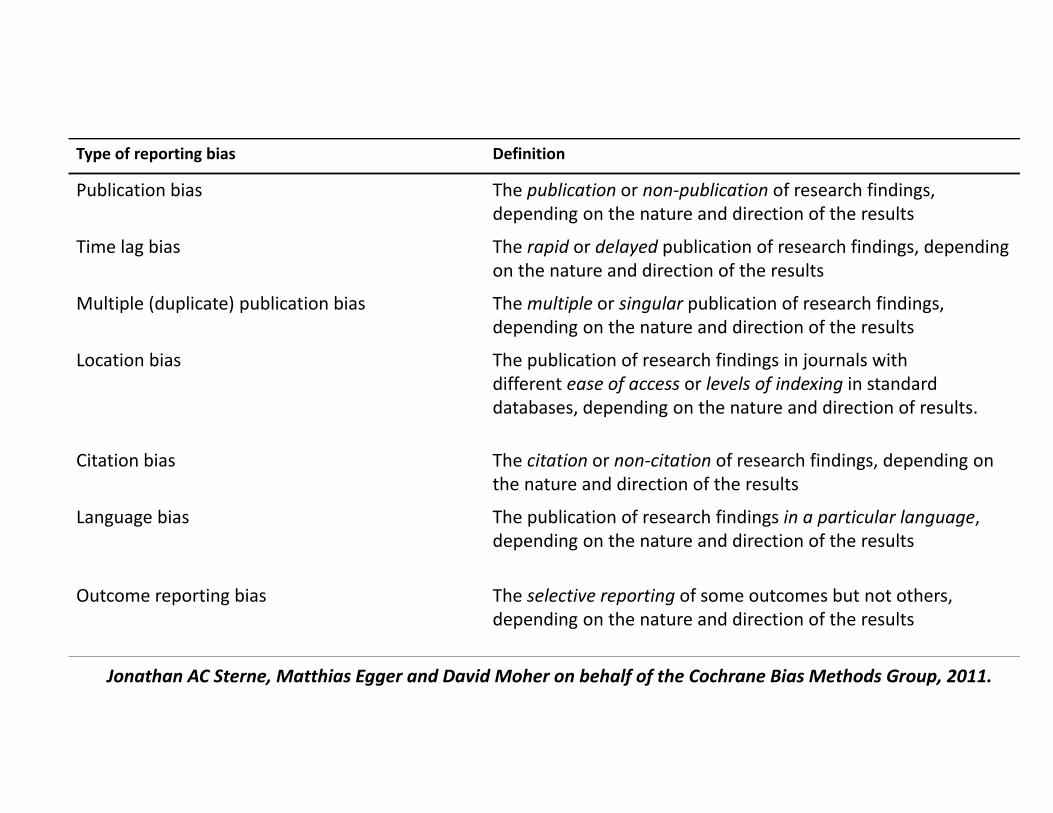
Type of reporting bias Definition
Publication bias The publication or non‐publication of research findings, depending on the nature and direction of the results
Time lag bias The rapid or delayed publication of research findings, depending on the nature and direction of the results
Multiple (duplicate) publication bias Themultiple or singular publication of research findings, depending on the nature and direction of the results
Location bias The publication of research findings in journals with different ease of access or levels of indexing in standard databases, depending on the nature and direction of results.
Citation bias The citation or non‐citation of research findings, depending on the nature and direction of the results
Language bias The publication of research findings in a particular language, depending on the nature and direction of the results
Outcome reporting bias The selective reporting of some outcomes but not others, depending on the nature and direction of the results
Jonathan AC Sterne, Matthias Egger and David Moher on behalf of the Cochrane Bias Methods Group, 2011.

Ties with the industry:
87% of authors have ties to industry
58% receive financial support for research
38% serves as employs or consultants
Roger Collier, CMAJ, 2011:183;3

IVF‐WorldwideClinic Locator
Education Center
News‐letters
Surveys
Blogs / Forums
Genetics Virtual
Academy Physicians consulting physicians
Online Journal
Online Informed Consent
Virtual university
Focus on professional education
IVF Worldwide surveys
• Large number of units (over 3,800)
• All 6 continents
• Data from academic and non‐academic practices
• A global scale
The Wisdom of the Crowds
Why the many are smarter than the few and how collective wisdom shapes business,
economies, societies and nations
James Surowiecki 2004

The SurveysAnti‐Mullerian hormone (AMH) and antral follicular count (AFC)
Minimising the risk of infection and bleeding at trans‐vaginal ultrasound guided ovum pick‐up
Vitrification, GnRH trigger and differed ET
Mechanical Infertility
Oocyte Donation
Reproductive Immunology Practice in IVF
Embryo Culture and Catheter Loading
Egg Collection and Embryo Transfer Techniques
PCOS – Definition, Diagnosis and Treatment
Poor Responders
The use of GnRH agonist in IVF protocols
Metformin Use In IVF Patients
Frozen‐Thawed Embryo Transfer
Updated survey on the use of progesterone for luteal phase support in stimulated IVF cycles
Progesterone Support In IVF
1st ‐ 20092nd ‐ 2012

Continent IVF Cycles % of cycles IVF units % of IVF units
USA & Canada 44900 13.9 52 11.9
South America 31100 9.6 59 13.5Australia & New Zealand 15400 4.8 12 2.7
Asia 64900 20.2 90 20.6
Europe 153400 47.6 200 45.8
Africa 12700 3.9 24 5.5
Total 322400 100 437 100
Geographic distribution of IVF units participating in the survey

Which factor is most important to you when deciding which luteal support regimen to use?
%
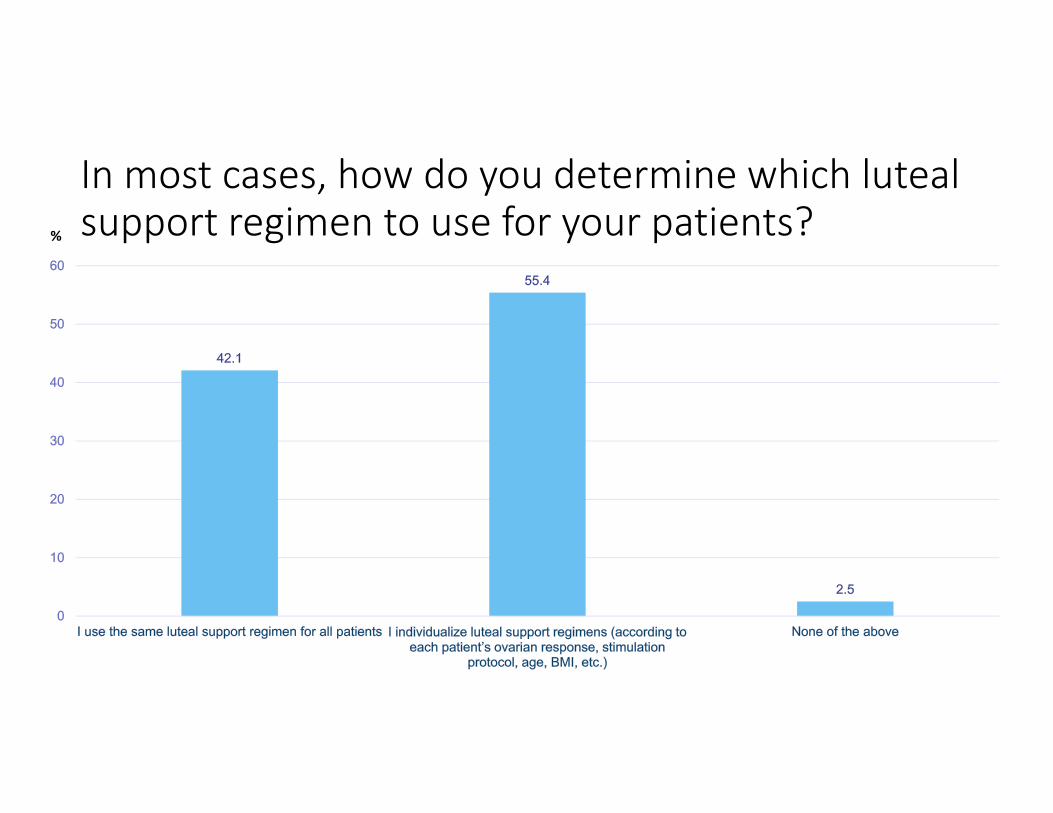
In most cases, how do you determine which luteal support regimen to use for your patients?%

If you support the luteal phase, when do you start the regimen you use?
•At the time of hCG admin.
•At the time OPU
•One day post OPU
•At the time of ET
•6 days post OPU
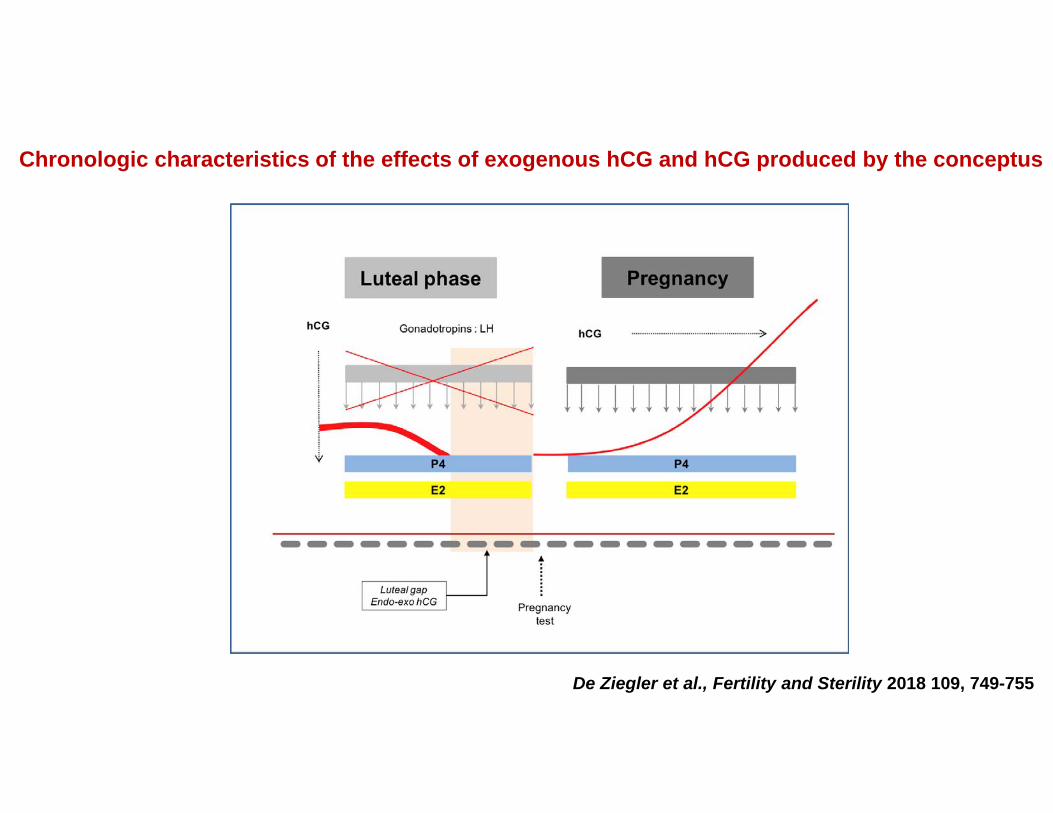
Figure 1
De Ziegler et al., Fertility and Sterility 2018 109, 749-755
Chronologic characteristics of the effects of exogenous hCG and hCG produced by the conceptus
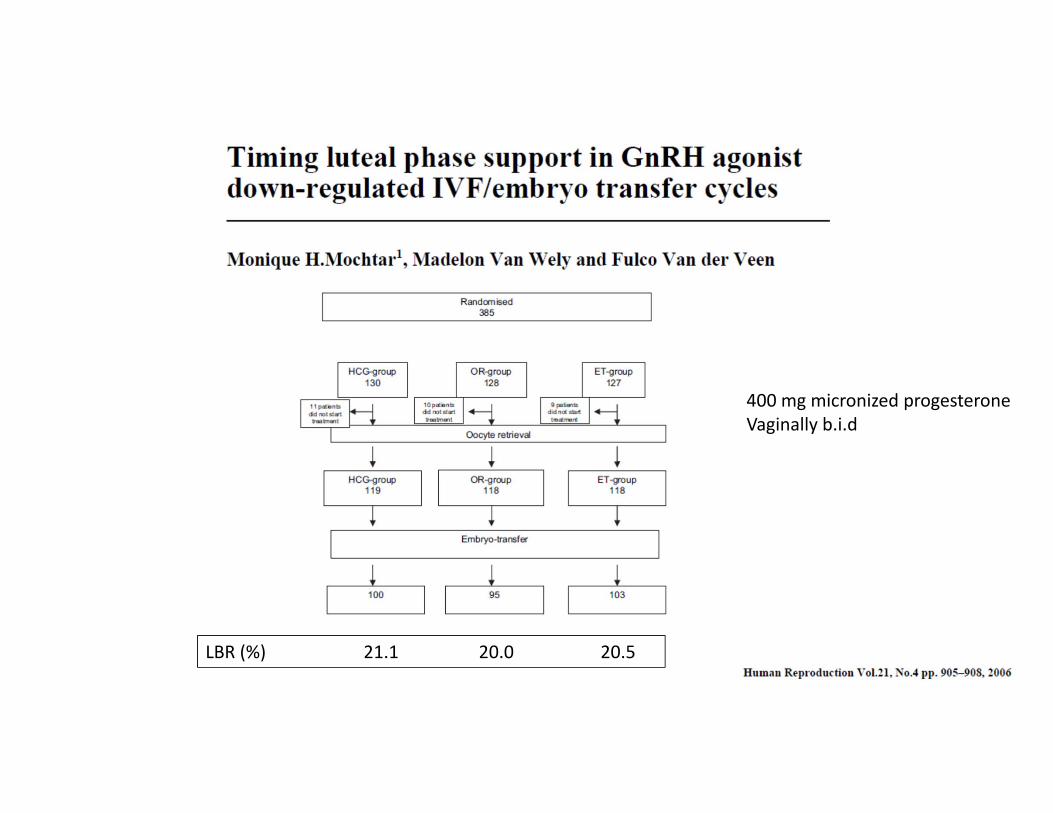
LBR (%) 21.1 20.0 20.5
400 mg micronized progesterone Vaginally b.i.d

RCT

RCTLPS: Uterogestan 400 mg/d Group A: from the evening of the day of oocyte retrievalGroup B: from the evening of embryo transfer (2nd day).
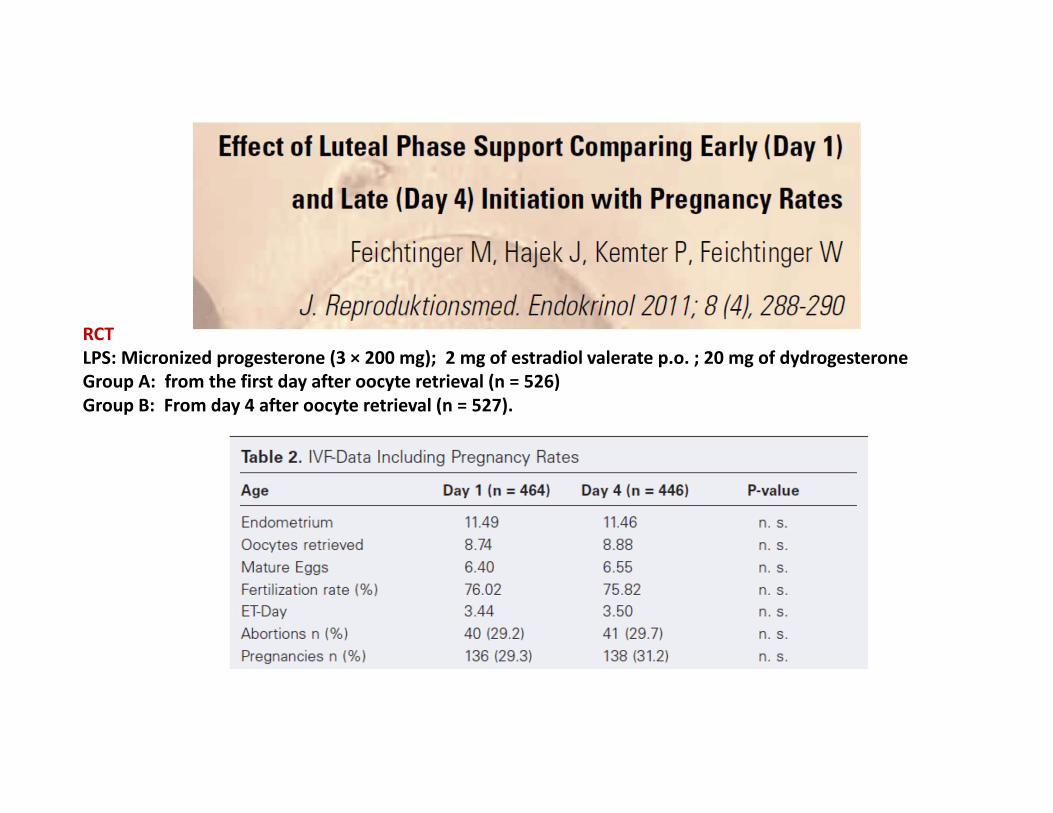
RCTLPS: Micronized progesterone (3 × 200 mg); 2 mg of estradiol valerate p.o. ; 20 mg of dydrogesteroneGroup A: from the first day after oocyte retrieval (n = 526)Group B: From day 4 after oocyte retrieval (n = 527).

RCTLPS: Prometrium, 200 mg intravaginally t.i.d.Group A: from the morning of the 3rd day after oocyte retrievalGroup B: from the morning of the 6th day after oocyte retrieval
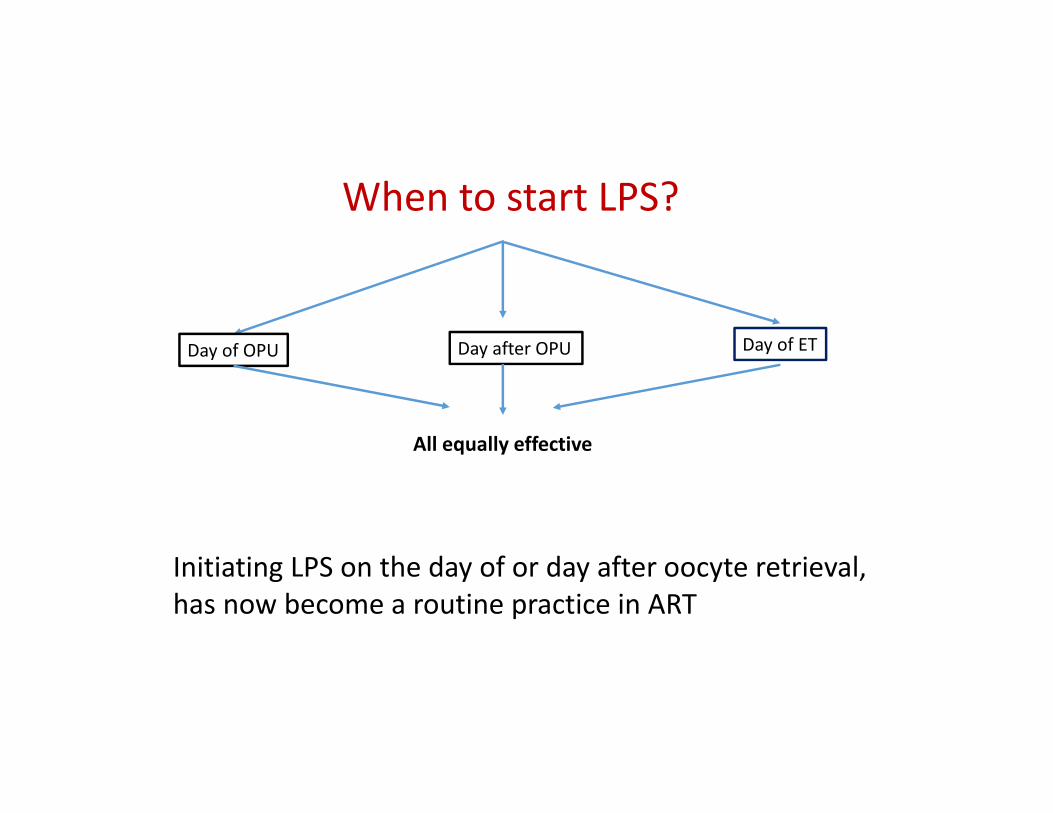
Initiating LPS on the day of or day after oocyte retrieval, has now become a routine practice in ART
When to start LPS?
Day of OPU Day after OPU Day of ET
All equally effective

If you support the luteal phase, when do you start the regimen you use?%
How long do you continue progesterone supplementation if the patient conceives?
•At the time of pregnancy test
•At the time of 1st US (6W)
•At 8 W
•At 10‐12 W

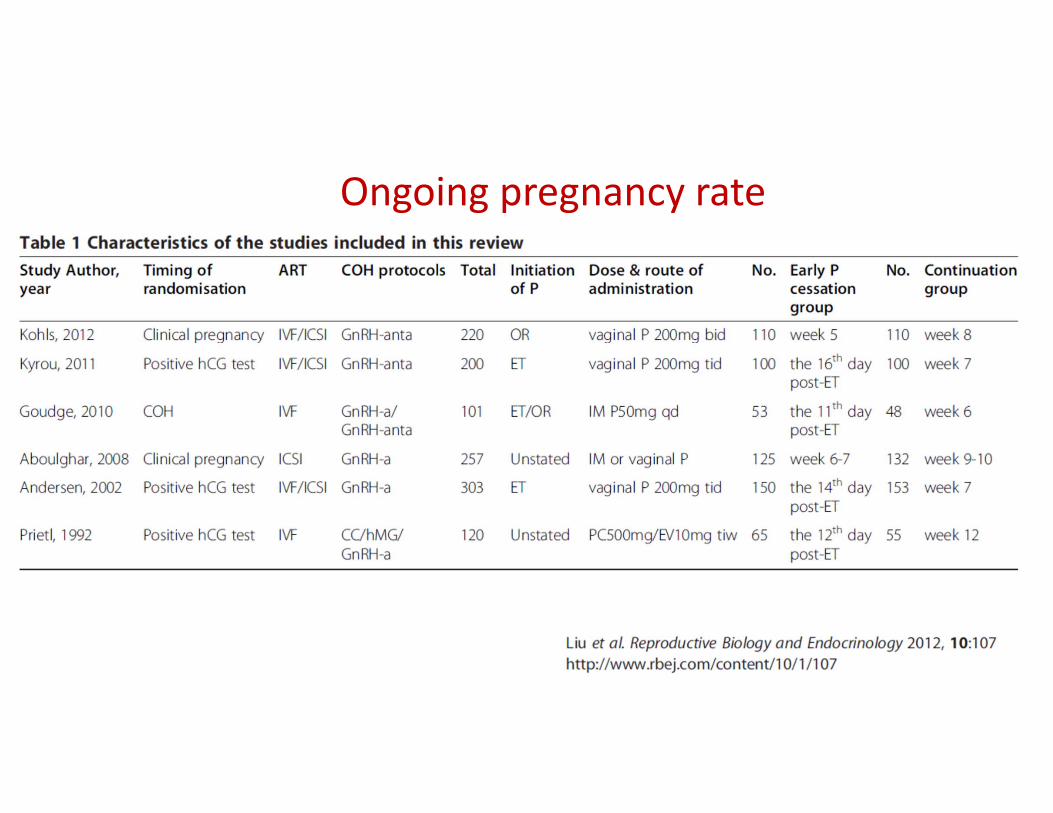
Ongoing pregnancy rate

Ongoing pregnancy rate
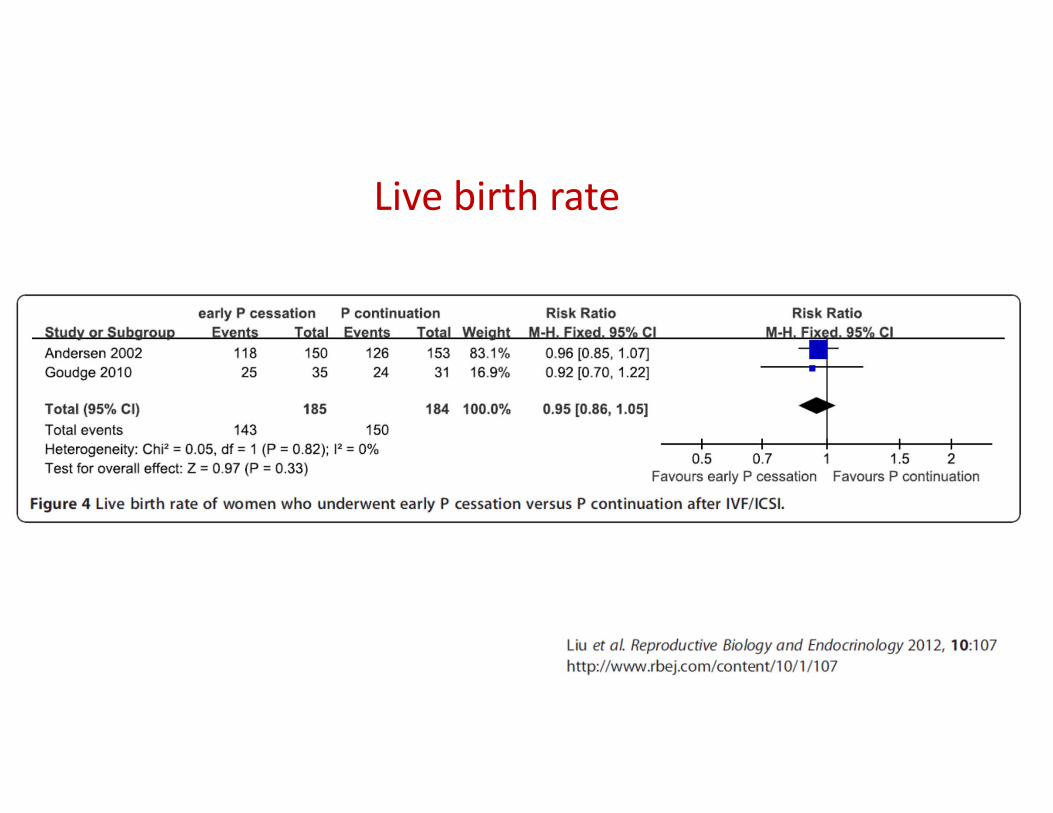
Live birth rate

Miscarriage rate
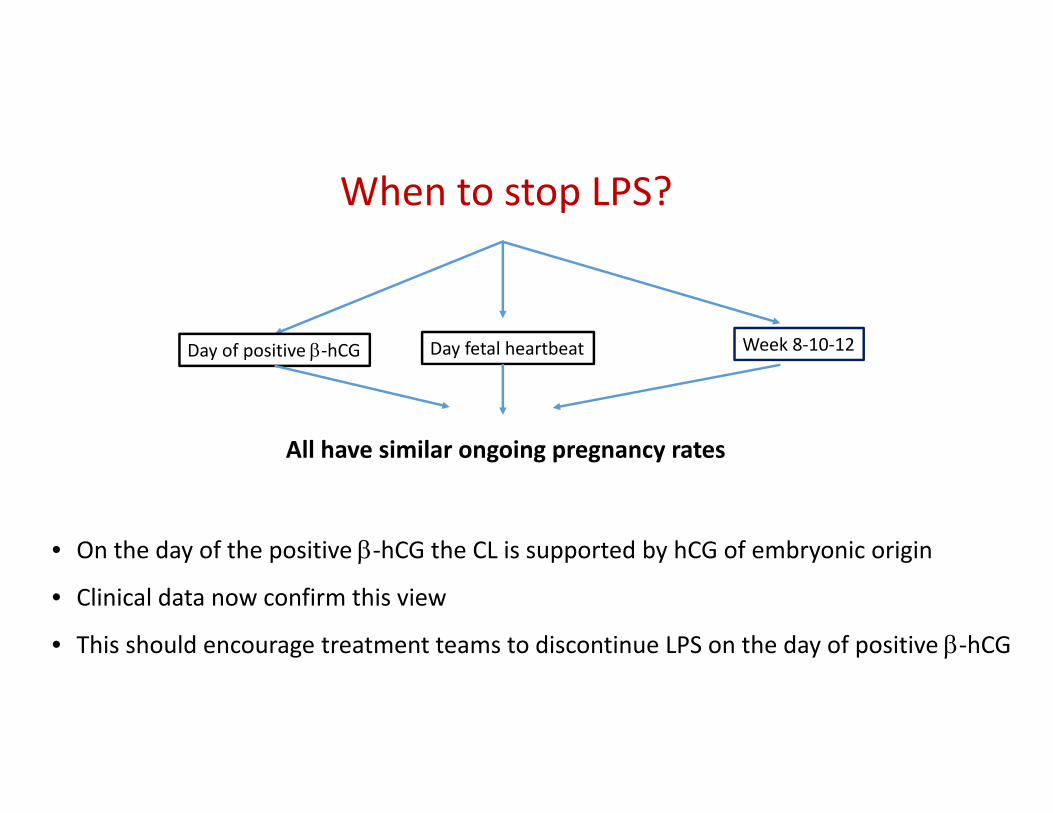
• On the day of the positive ‐hCG the CL is supported by hCG of embryonic origin
• Clinical data now confirm this view
• This should encourage treatment teams to discontinue LPS on the day of positive ‐hCG
When to stop LPS?
Day of positive ‐hCG Day fetal heartbeat Week 8‐10‐12
All have similar ongoing pregnancy rates

How long do you continue progesterone supplementation if the patient conceives?%

0
10
20
30
40
50
60
70
80
Positive bhCG Clinical preg Week 8‐12
2009 2012 2018
How long do you continue progesterone supplementation if the patient conceives?
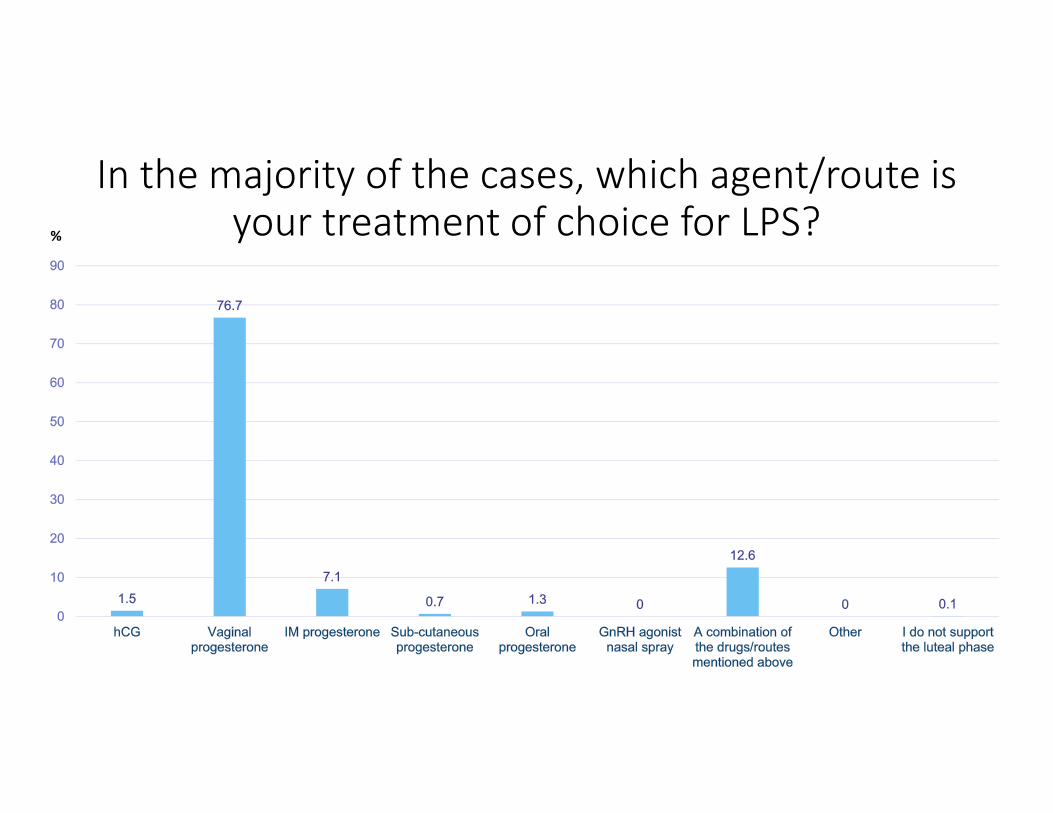
In the majority of the cases, which agent/route is your treatment of choice for LPS? %
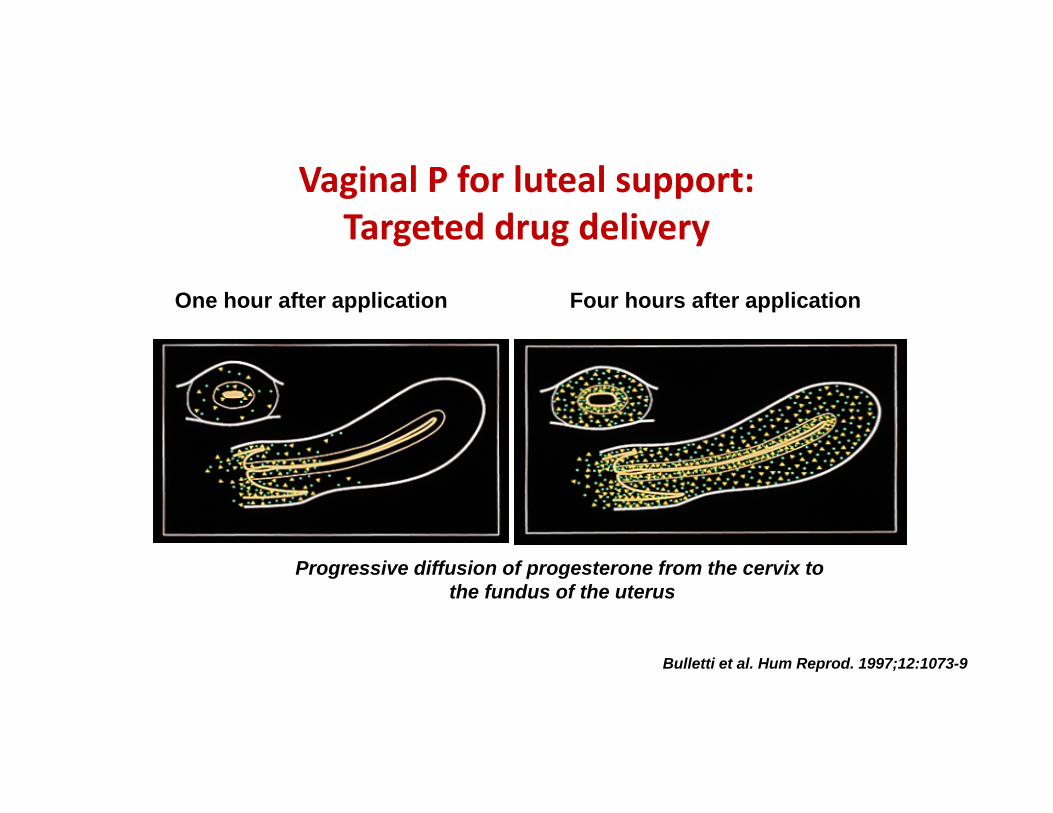
Vaginal P for luteal support:Targeted drug delivery
One hour after application Four hours after application
Progressive diffusion of progesterone from the cervix tothe fundus of the uterus
Bulletti et al. Hum Reprod. 1997;12:1073-9
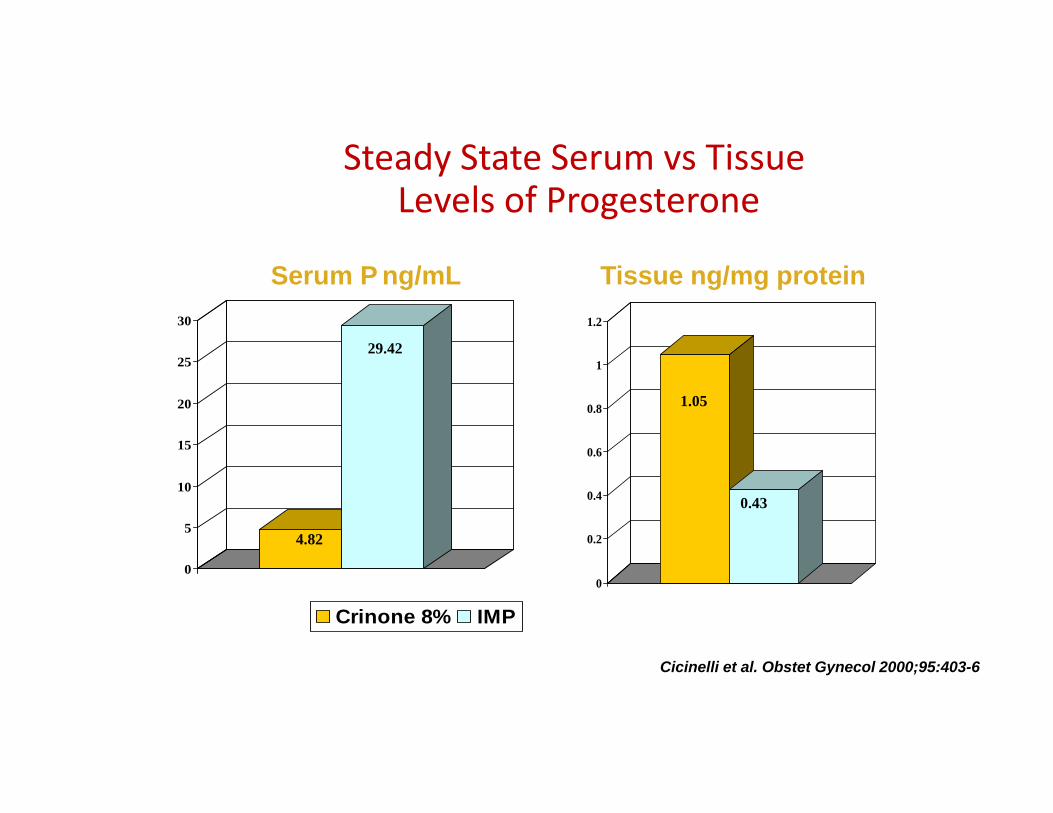
Steady State Serum vs TissueLevels of Progesterone
0
0.2
0.4
0.6
0.8
1
1.2
0
5
10
15
20
25
30
Crinone 8% IMP
Serum P ng/mL Tissue ng/mg protein
29.42
4.82
1.05
0.43
Cicinelli et al. Obstet Gynecol 2000;95:403-6
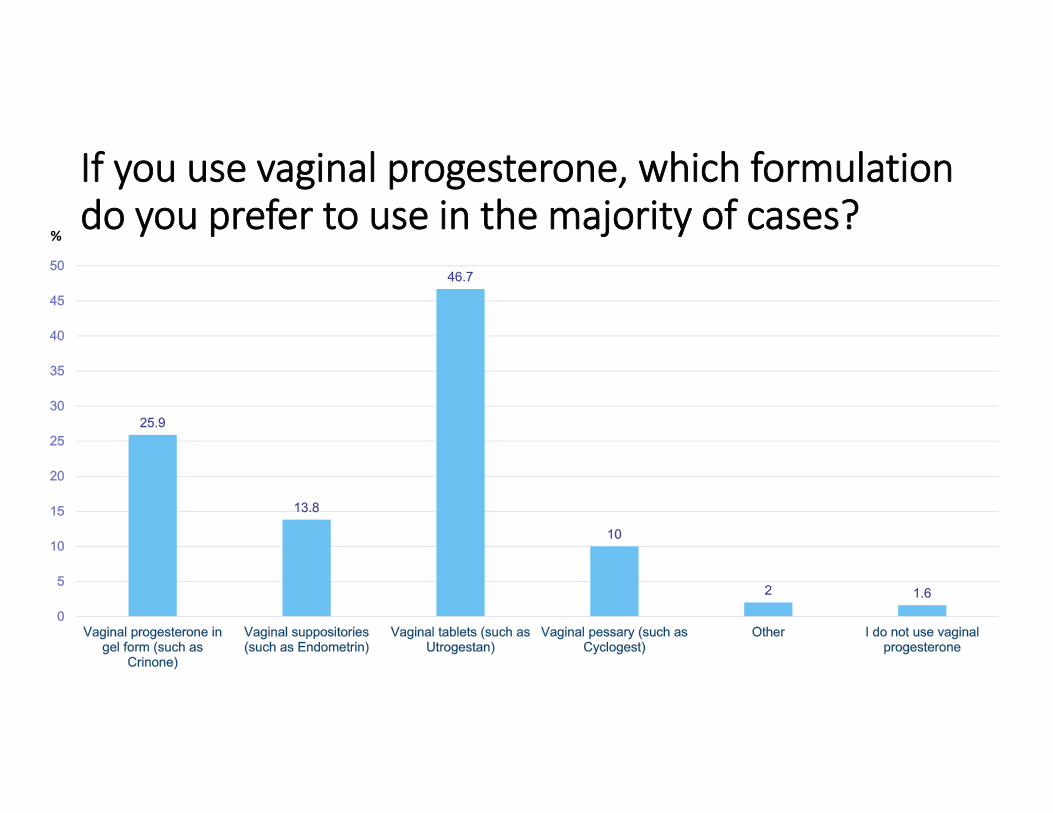
If you use vaginal progesterone, which formulation do you prefer to use in the majority of cases?
%
Child et al., RBM Online, in press
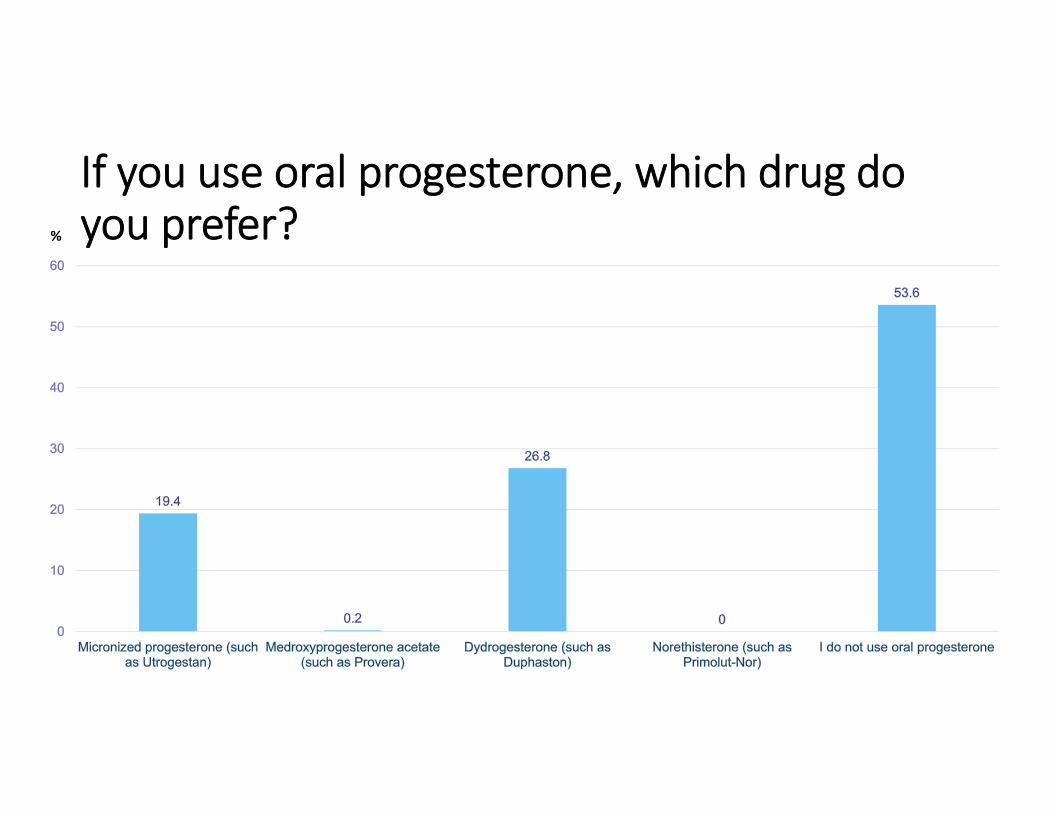
If you use oral progesterone, which drug do you prefer?%

Oral Micronized Progesterone

Progesterone for luteal support: the oral route
Micronization: improved absorption of oral P
Poor bioavailability
Circulating levels are too low for adequate support
Liver first pass leads to massive metabolism
At best 10% circulates as active P
Inadequate secretory transformation
Dose increase: unacceptable somnolence
Nahoul and de Ziegler D. Fertil Steril 1994;61:790–2.Bourgain et al., Hum Reprod 1990;5:537–43.
0
2
4
6
8
10
12
14
16
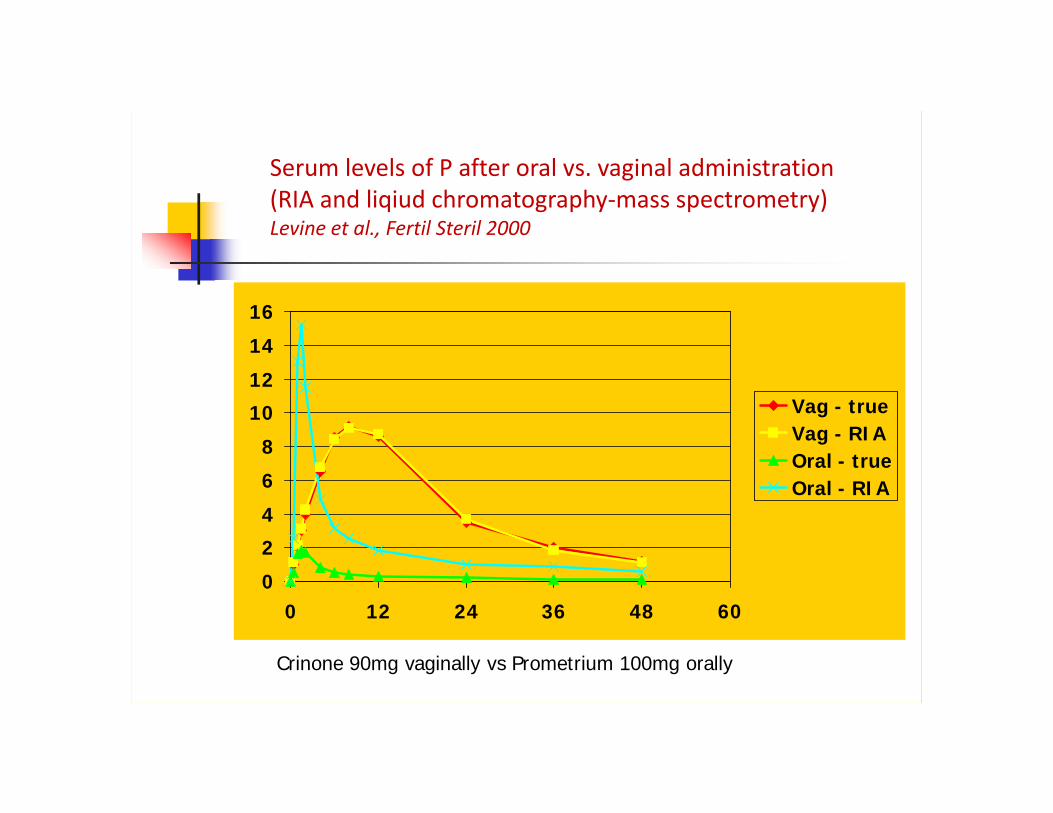
0 12 24 36 48 60
Vag - trueVag - RIAOral - trueOral - RIA
Crinone 90mg vaginally vs Prometrium 100mg orally
Serum levels of P after oral vs. vaginal administration(RIA and liqiud chromatography‐mass spectrometry)Levine et al., Fertil Steril 2000

0
10
20
30
40
50
60
70
CPR IR
IM P PO P
Outcome with oral P administration
0
5
10
15
20
25
30
35
40
45
50
CPR IR Miscarriage
Vag P PO P* P<0.05
Licciardi et al. 1999 Friedler et al. 1999
**

Oral dydrogesterone
Oral dydrogesterone for luteal phase support in IVFAn oral retroprogesterone – progesterone agonistApproved for: Threatened and recurrent miscarriage (associated with proven progesterone deficiency) Infertility due to luteal phase insufficiency
It has been extensively used for a variety of indications since 1960
Compared with progesterone:• Greater affinity for the progesterone receptors • Can be used at lower oral doses to promote endometrial proliferation owing to its better bioavailability and to the progestogenic activity of its metabolites
Schindler AE et al., Maturitas 2008;61:171–180.

Barbosa Et al., Ultrasound Obstet Gynecol 2016; 48: 161‐170
RCTLPS: From the day of oocyte retrievalGroup A: MVP 200 mg capsules TID with oral placebo tablets TIDGroup B: Oral dydrogesterone 10 mg tablets TID with placebo intravaginal capsules TID

Fertility and Sterility 2018 109, 756-762DOI: (10.1016/j.fertnstert.2018.03.034)
Ongoing pregnancy rates and live birth ratesin the (total n = 974) LOTUS I trial.
Fertility and Sterility 2018 109, 756-762DOI: (10.1016/j.fertnstert.2018.03.034)
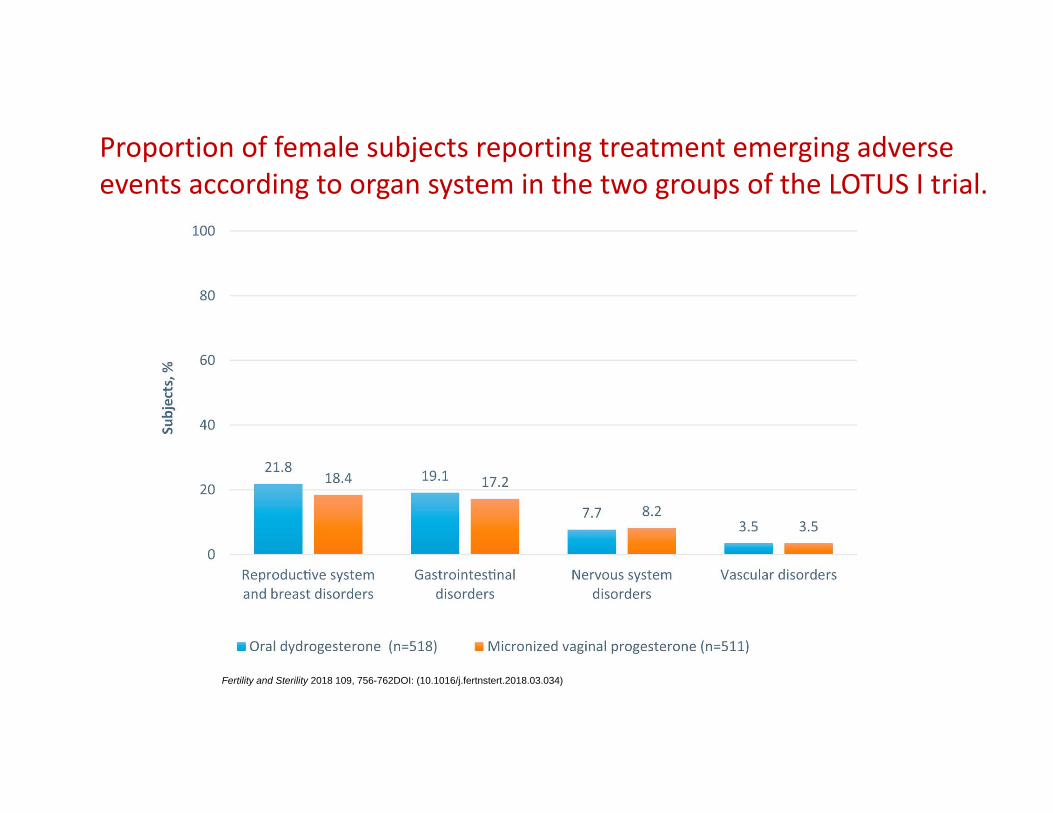
Proportion of female subjects reporting treatment emerging adverse events according to organ system in the two groups of the LOTUS I trial.
• Noninferiority of daily 30 mg oral dydrogesterone for luteal phase support • Well tolerated as vaginal progesterone in safety analyses • No new fetal safety concerns
• Widespread preference of women for an oral compound • Dydrogesterone may well become the new standard for LPS in fresh IVF‐ET cycles

IM Progesterone
P is highly water insolubleP in oilStandard route of P delivery High efficiency: avoids hepatic “first pass”
Several drawbacks: *Painful and uncomfortable* Preservatives (benzyl alcohol)*Sterile abscess formation*Allergic response *Time and cost
Progesterone for luteal support: The intramuscular route

Progesterone for luteal support: The intramuscular route
IM dosing: 25‐100 mg daily
Long acting formulations
Mean production rate of progesterone of 25 mg/24 h
“Gold standard” of LPS
“in phase” endometrial architecture
Satisfactory pregnancy/miscarriage rates
Able to delay menses in most women
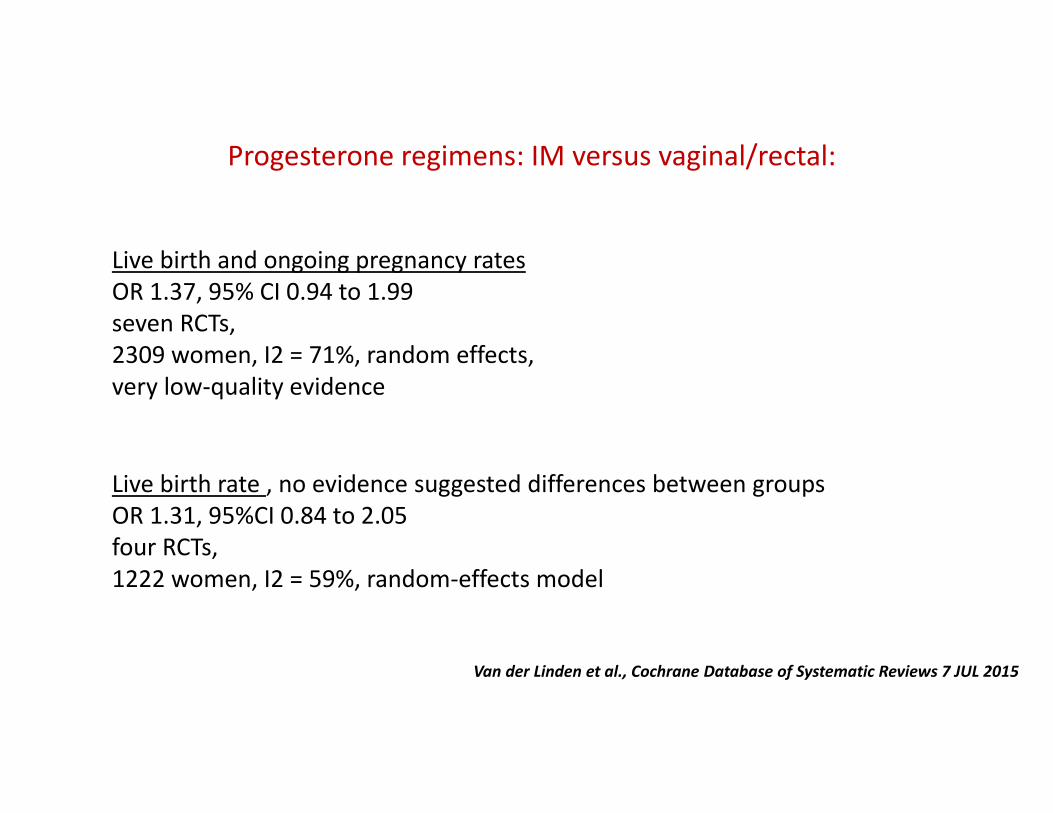
Progesterone regimens: IM versus vaginal/rectal:
Live birth rate , no evidence suggested differences between groups OR 1.31, 95%CI 0.84 to 2.05 four RCTs, 1222 women, I2 = 59%, random‐effects model
Live birth and ongoing pregnancy ratesOR 1.37, 95% CI 0.94 to 1.99 seven RCTs, 2309 women, I2 = 71%, random effects, very low‐quality evidence
Van der Linden et al., Cochrane Database of Systematic Reviews 7 JUL 2015
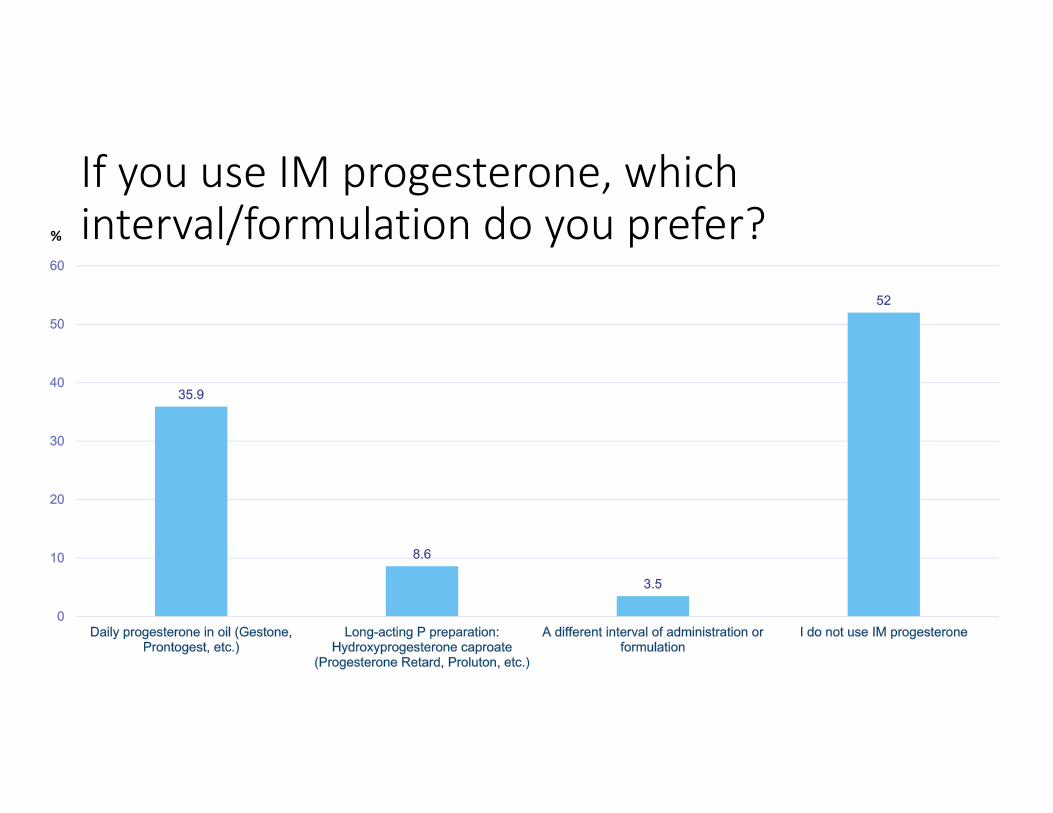
If you use IM progesterone, which interval/formulation do you prefer?%

SC Progesterone

• Water insolubility of P: an aqueous preparation of P was seemingly impossible
• Enhancing polarity by encapsulation of P molecules in a starch residue, cyclodextrine
• On reaching bodily fluids, cyclodextrine is readily digested
• This liberates native P, which reaches the general circulation
• Prolutex—is available in single‐use preparations
• Contains no preservatives
de Ziegler et al., Fertil Steril 2013
Aqueous subcutaneous progesterone

Non‐inferiority of SC P versus vaginal P
95% CICrinoneProlutex
‐ 9.91‐3.37330.527.4Ongoing PR (10 wks) (%)
‐9.87‐3‐3.5829.926.8Live birth rate (%)
Lockwood et al. Fertil Steril 2013
95% CIEndometrinProlutex
‐ 9.7‐4.244.441.6Ongoing PR (10 wks) (%)
‐8.9‐4.943.141.1Live birth rate (%)
Baker VL et al. Hum Reprod 2014
95% CIORProlutex vs. Vag P (n=1435)
0.694‐1.0770.865Ongoing PR (10 wks) (%)
0.714‐1.1060.889Live birth rate (%)
Doblinger et al. Plos One 2016

If you use a combination of progesterone treatments, which do you prefer?%

Do you include estradiol in your luteal support regimen?
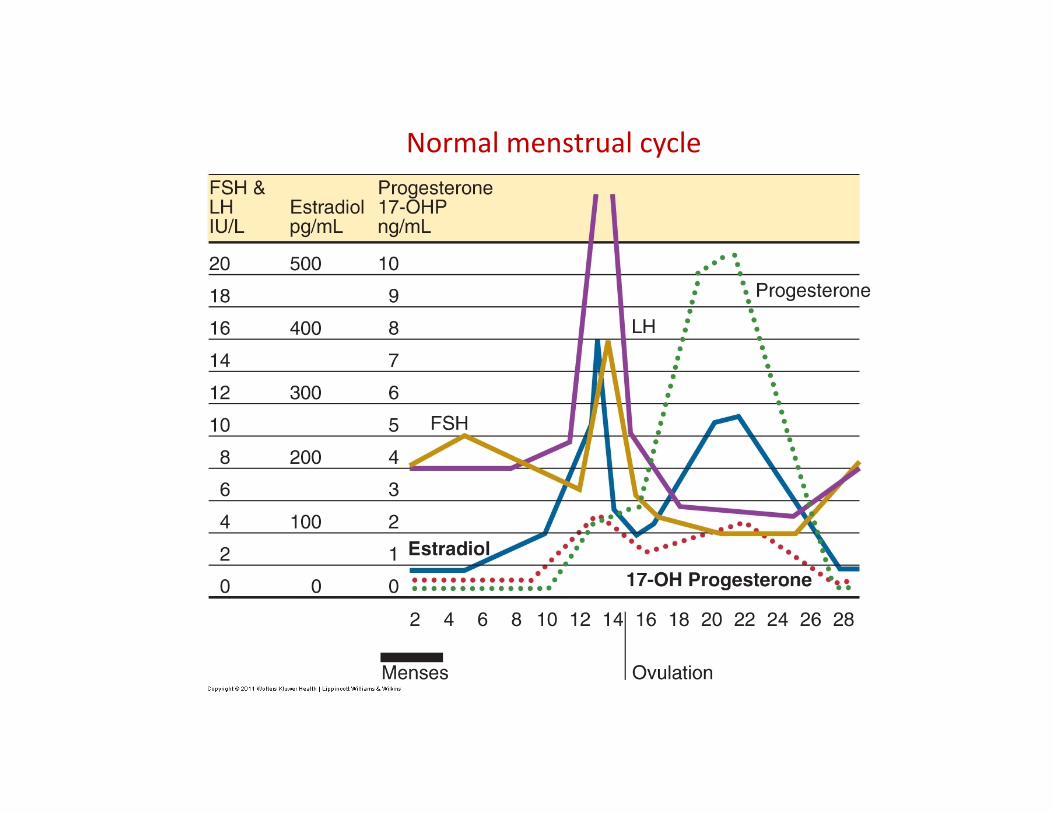
Normal menstrual cycle
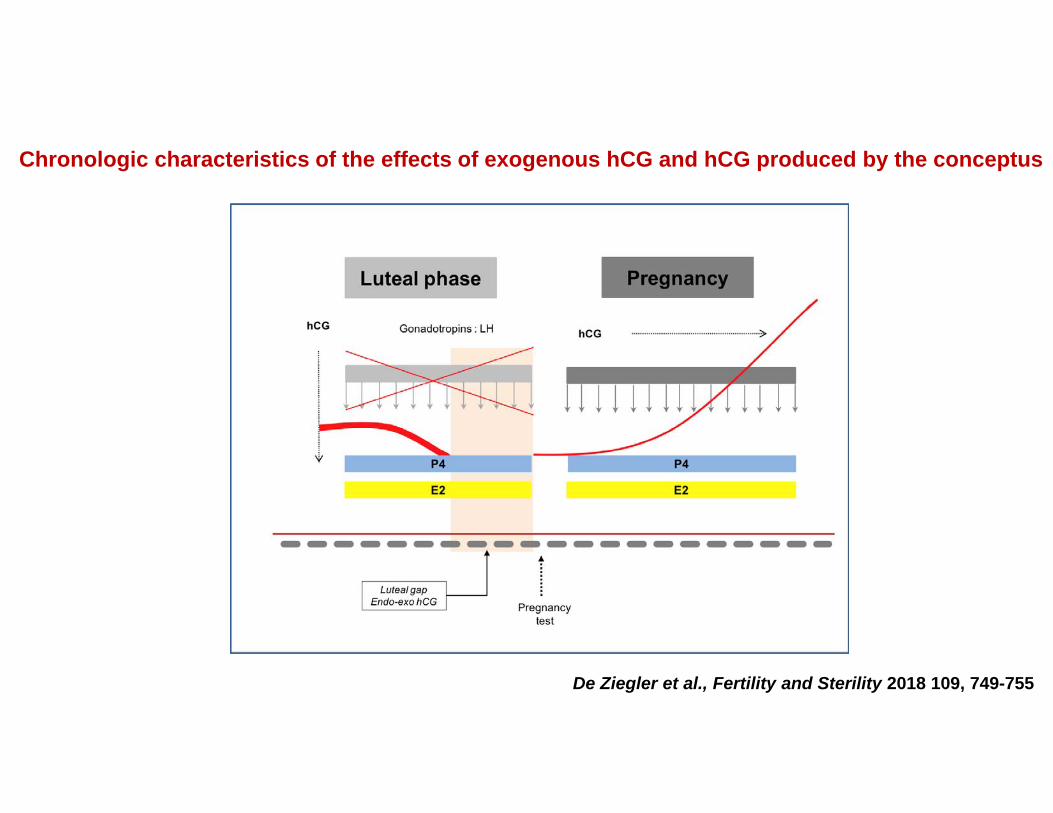
Figure 1
De Ziegler et al., Fertility and Sterility 2018 109, 749-755
Chronologic characteristics of the effects of exogenous hCG and hCG produced by the conceptus
RCT – Patients with E2 >2500 pg/mL on hCG dayLPS: IM + Vag P Group A: 2 mg of E2 (Estrofem) p.o. b.i.d. starting on day 7 after ET (n=136)Group B: P only (n=149)
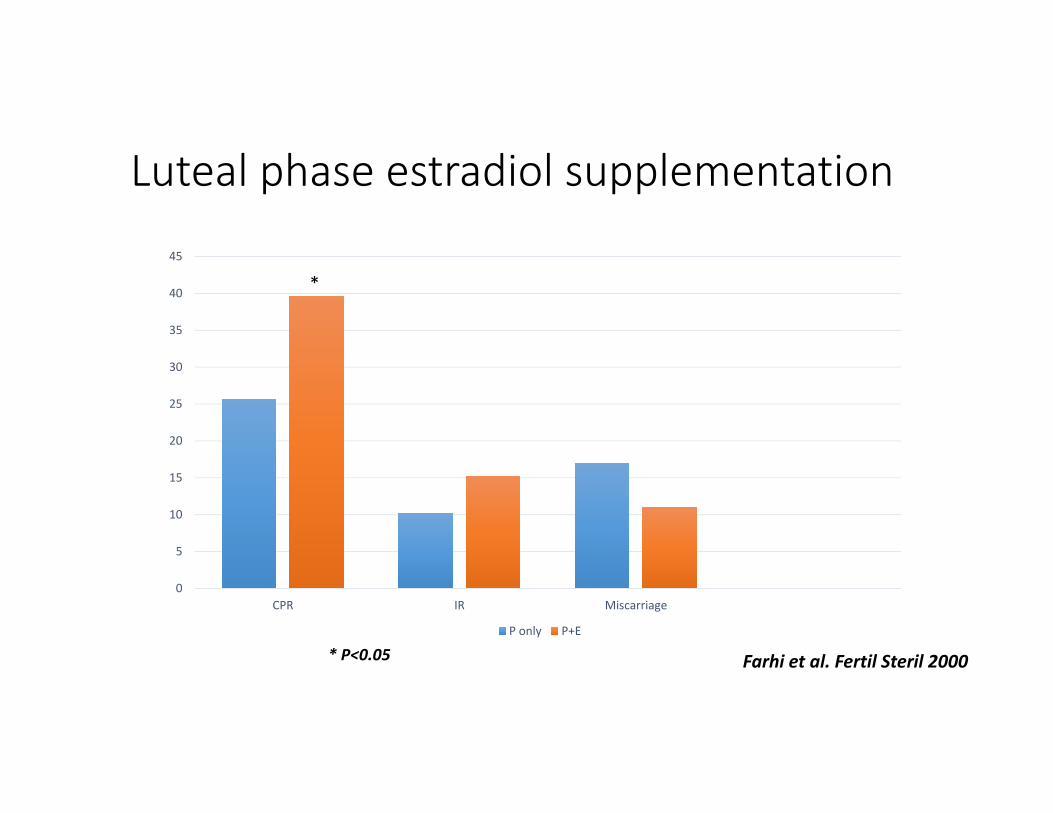
Luteal phase estradiol supplementation
0
5
10
15
20
25
30
35
40
45
CPR IR Miscarriage
P only P+E
Farhi et al. Fertil Steril 2000
*
* P<0.05
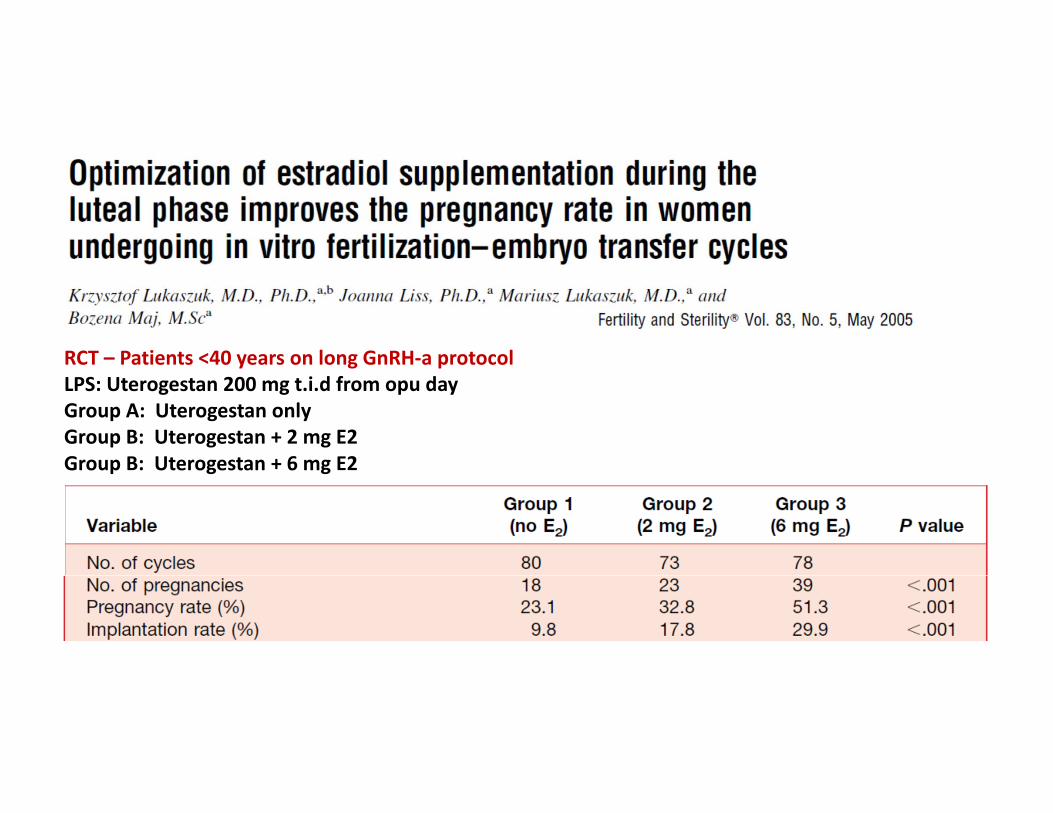
RCT – Patients <40 years on long GnRH‐a protocolLPS: Uterogestan 200 mg t.i.d from opu dayGroup A: Uterogestan onlyGroup B: Uterogestan + 2 mg E2Group B: Uterogestan + 6 mg E2
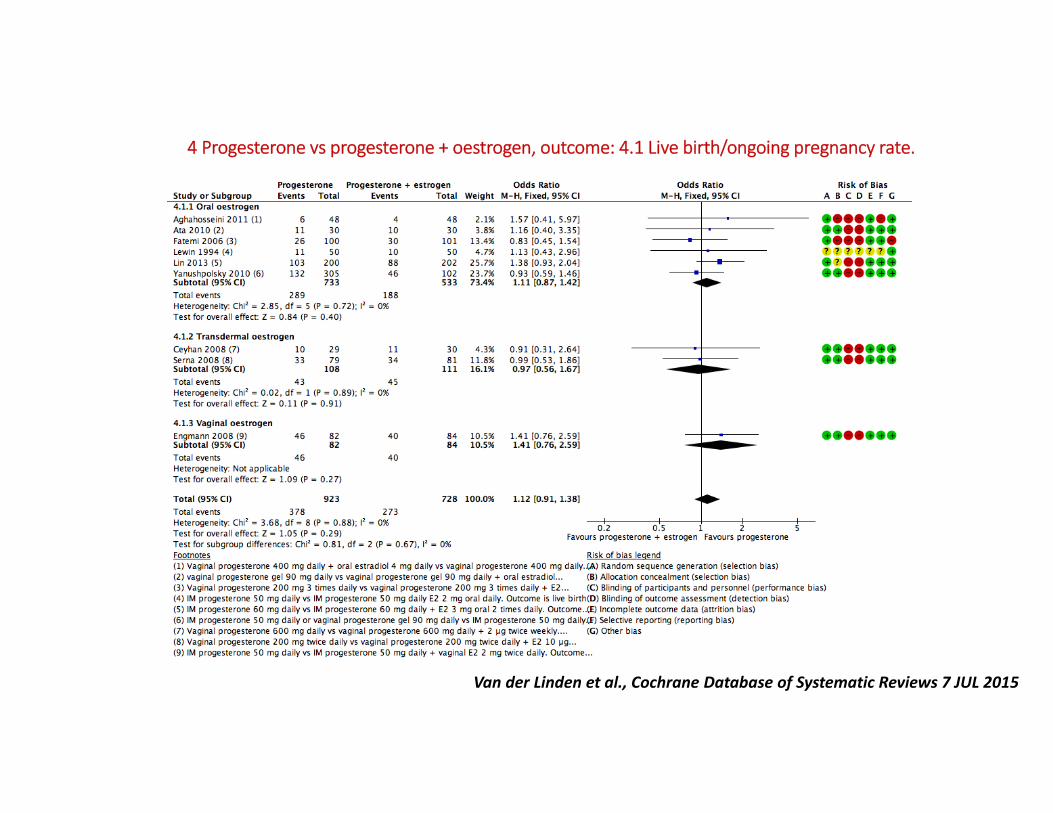
4 Progesterone vs progesterone + oestrogen, outcome: 4.1 Live birth/ongoing pregnancy rate.
Van der Linden et al., Cochrane Database of Systematic Reviews 7 JUL 2015
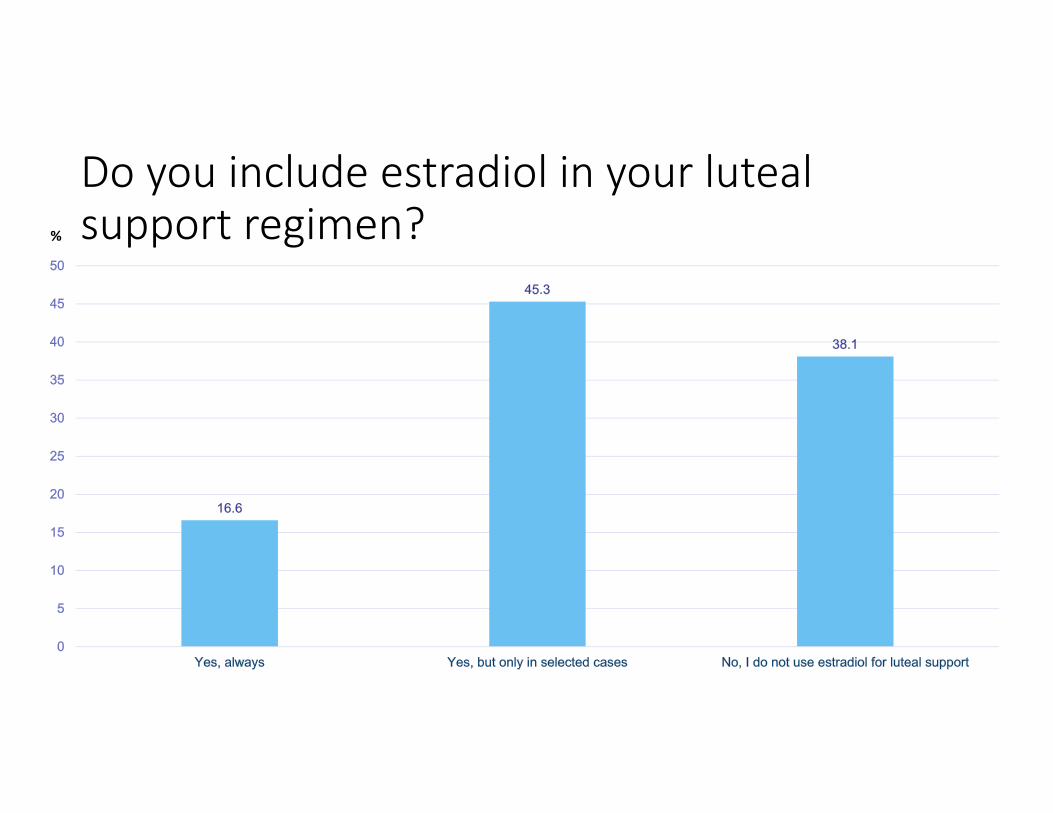
Do you include estradiol in your luteal support regimen?%
When triggering ovulation with a GnRHagonist, which luteal support do you use?
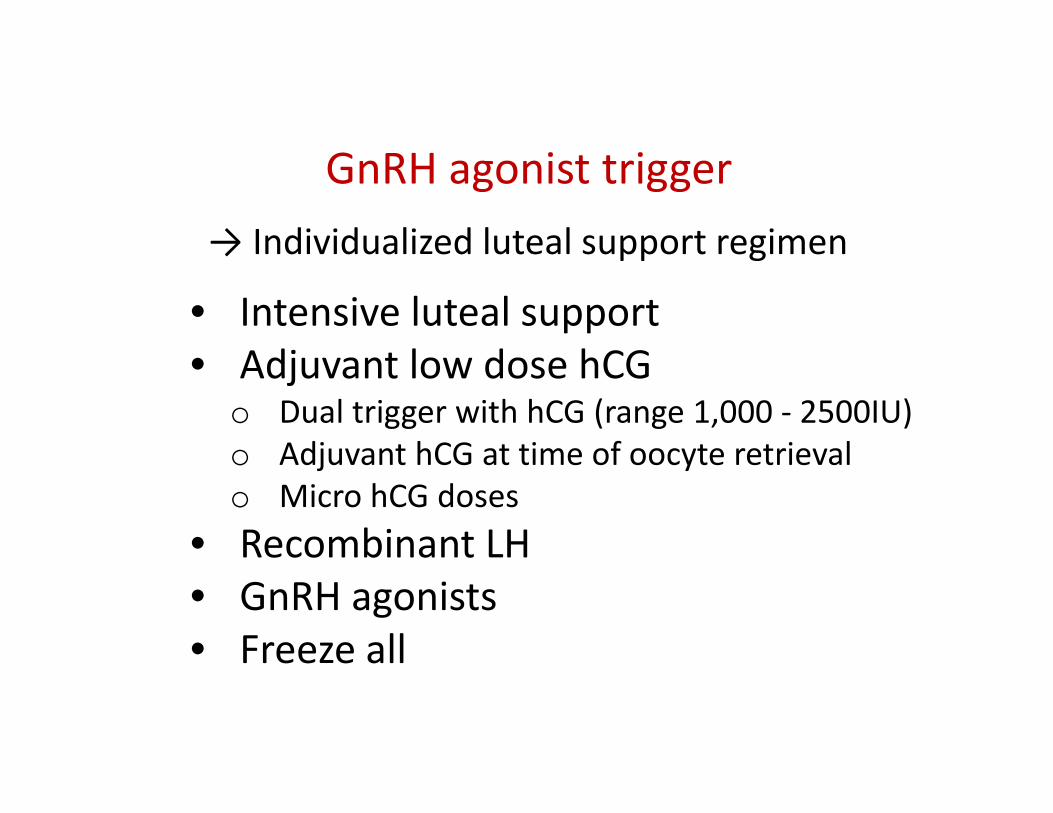
GnRH agonist trigger→ Individualized luteal support regimen
• Intensive luteal support• Adjuvant low dose hCG
o Dual trigger with hCG (range 1,000 ‐ 2500IU)o Adjuvant hCG at time of oocyte retrievalo Micro hCG doses
• Recombinant LH• GnRH agonists• Freeze all

Mid‐luteal LH levels
~ 6.0 IU/l in natural cycle
~ 1.5 IU/l ‐ GnRHa trigger
~ 0.2 IU/l – HCG trigger
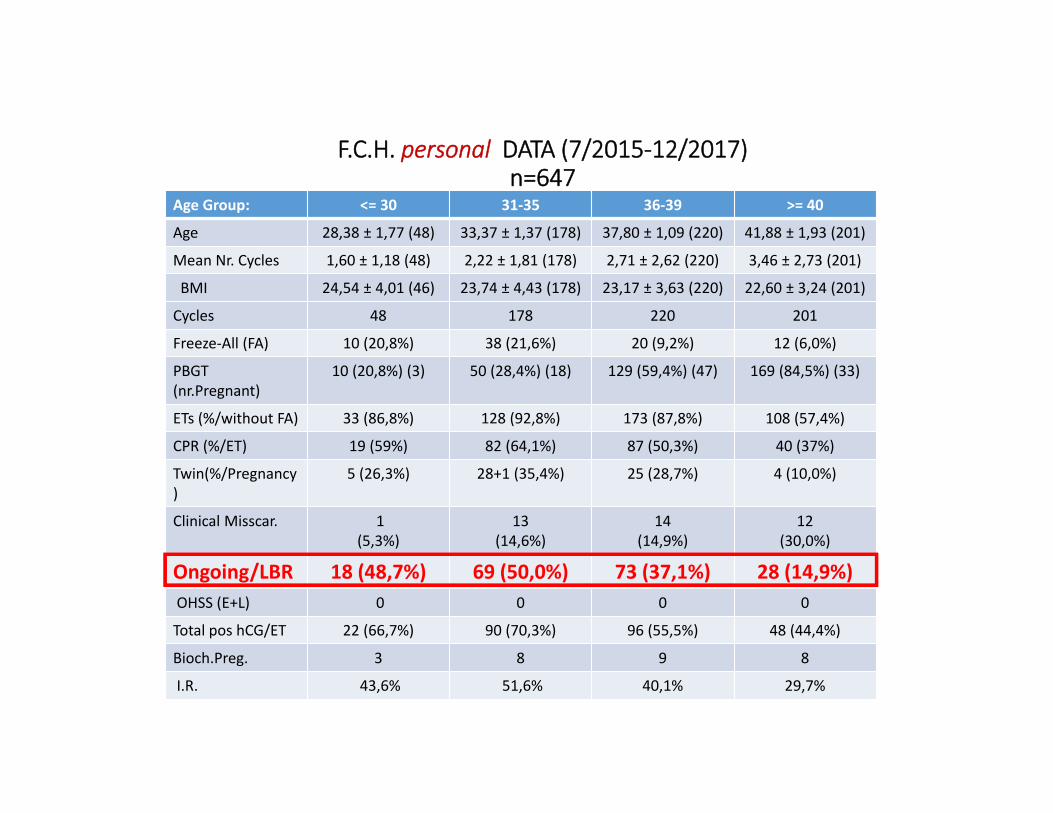
F.C.H. personal DATA (7/2015‐12/2017)n=647
Age Group: <= 30 31‐35 36‐39 >= 40
Age 28,38 ± 1,77 (48) 33,37 ± 1,37 (178) 37,80 ± 1,09 (220) 41,88 ± 1,93 (201)
Mean Nr. Cycles 1,60 ± 1,18 (48) 2,22 ± 1,81 (178) 2,71 ± 2,62 (220) 3,46 ± 2,73 (201)
BMI 24,54 ± 4,01 (46) 23,74 ± 4,43 (178) 23,17 ± 3,63 (220) 22,60 ± 3,24 (201)
Cycles 48 178 220 201
Freeze‐All (FA) 10 (20,8%) 38 (21,6%) 20 (9,2%) 12 (6,0%)
PBGT (nr.Pregnant)
10 (20,8%) (3) 50 (28,4%) (18) 129 (59,4%) (47) 169 (84,5%) (33)
ETs (%/without FA) 33 (86,8%) 128 (92,8%) 173 (87,8%) 108 (57,4%)
CPR (%/ET) 19 (59%) 82 (64,1%) 87 (50,3%) 40 (37%)
Twin(%/Pregnancy)
5 (26,3%) 28+1 (35,4%) 25 (28,7%) 4 (10,0%)
Clinical Misscar. 1 (5,3%)
13(14,6%)
14(14,9%)
12 (30,0%)
Ongoing/LBR 18 (48,7%) 69 (50,0%) 73 (37,1%) 28 (14,9%)OHSS (E+L) 0 0 0 0
Total pos hCG/ET 22 (66,7%) 90 (70,3%) 96 (55,5%) 48 (44,4%)
Bioch.Preg. 3 8 9 8
I.R. 43,6% 51,6% 40,1% 29,7%
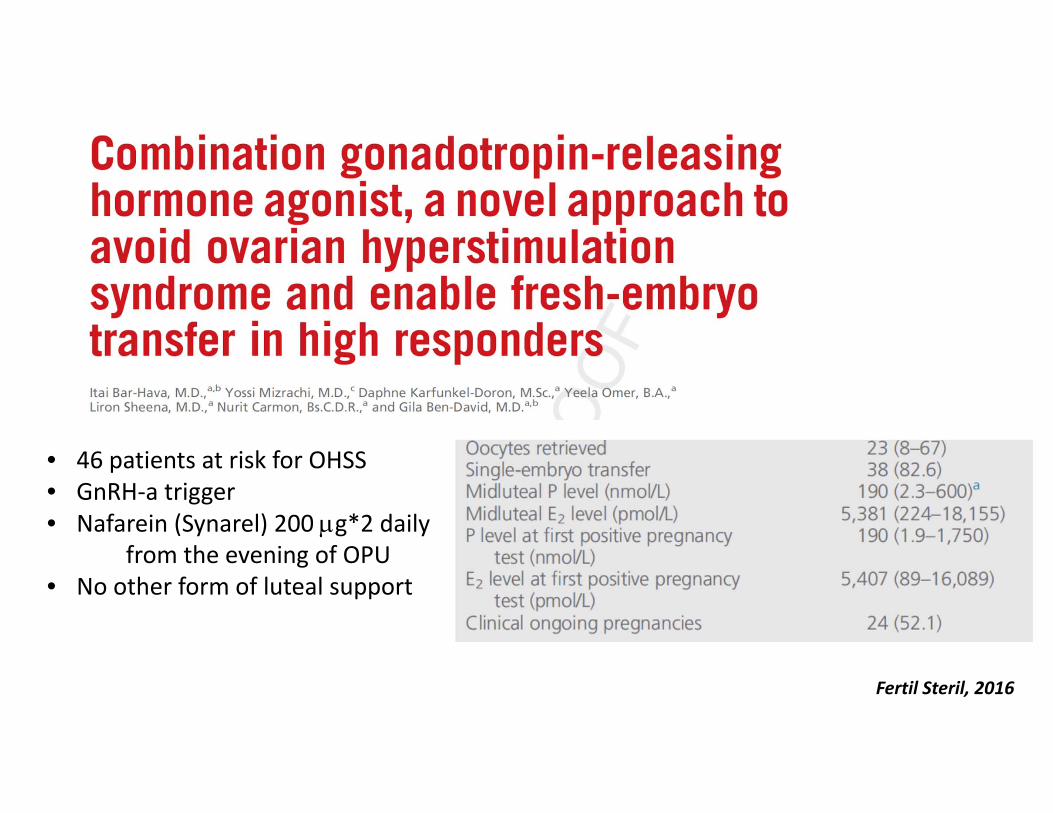
Fertil Steril, 2016
• 46 patients at risk for OHSS• GnRH‐a trigger• Nafarein (Synarel) 200 g*2 daily
from the evening of OPU• No other form of luteal support
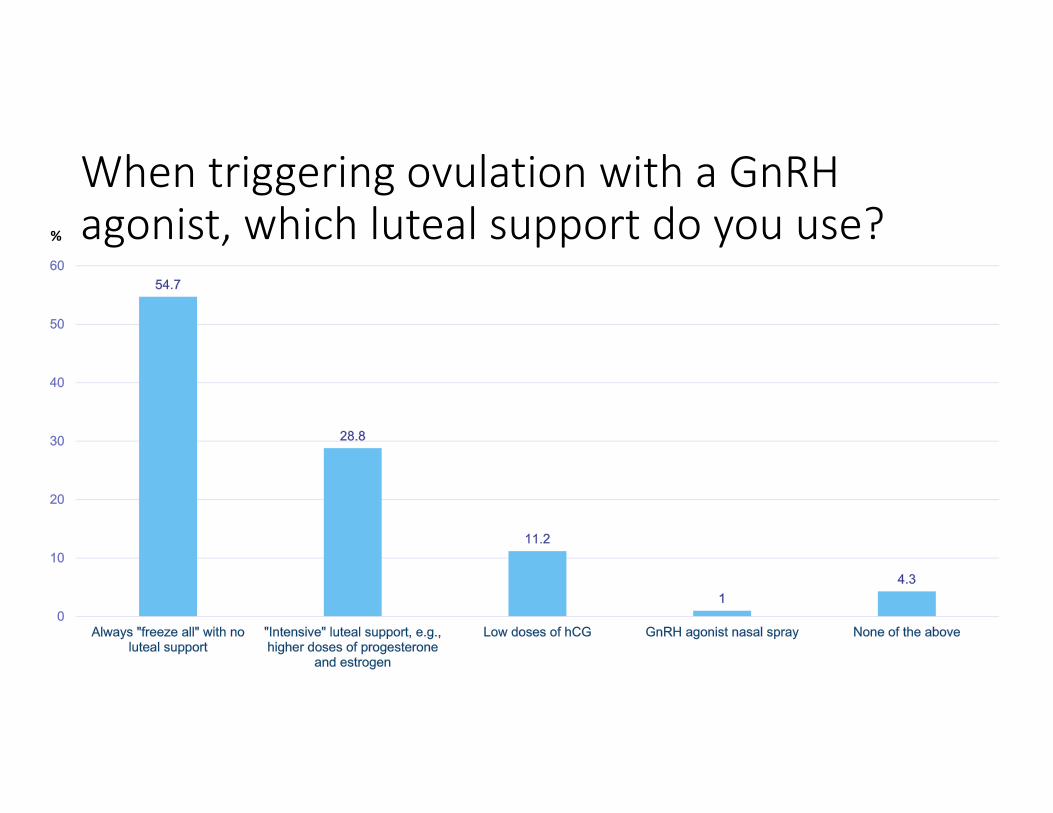
When triggering ovulation with a GnRHagonist, which luteal support do you use?%
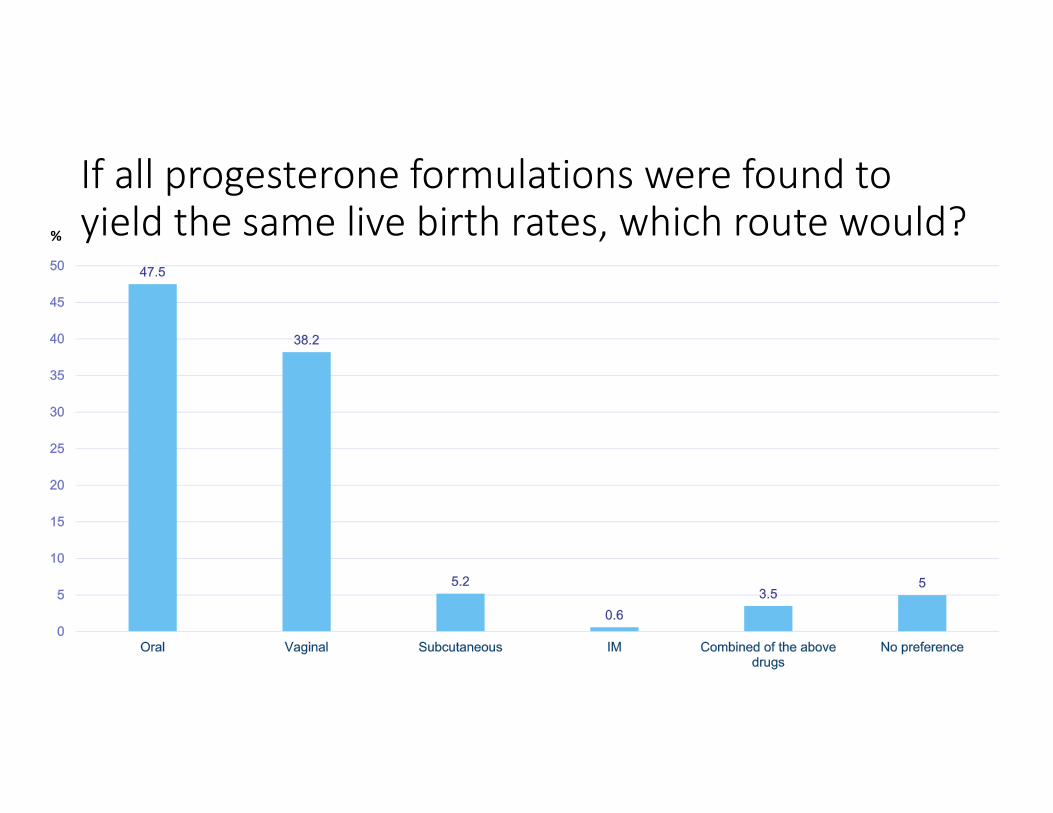
If all progesterone formulations were found to yield the same live birth rates, which route would? %
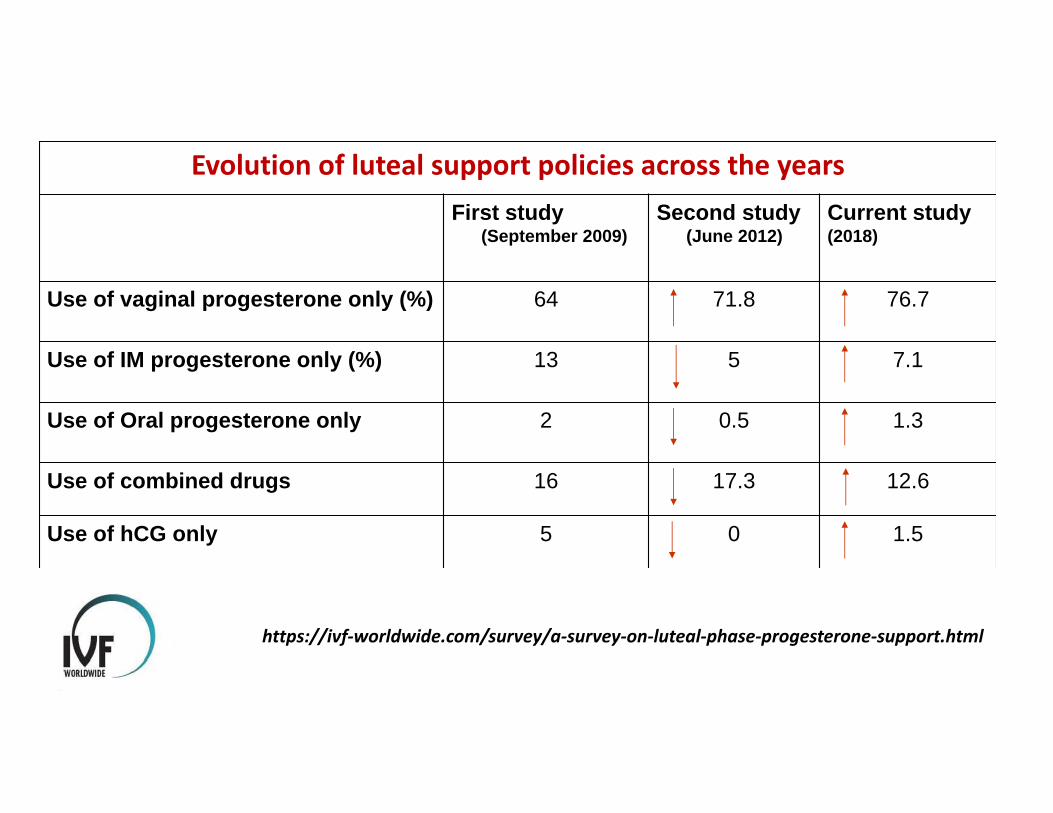
Evolution of luteal support policies across the yearsCurrent study(2018)
Second study (June 2012)
First study (September 2009)
76.771.864Use of vaginal progesterone only (%)
7.1513Use of IM progesterone only (%)
1.30.52Use of Oral progesterone only
12.617.316Use of combined drugs
1.505Use of hCG only
https://ivf‐worldwide.com/survey/a‐survey‐on‐luteal‐phase‐progesterone‐support.html
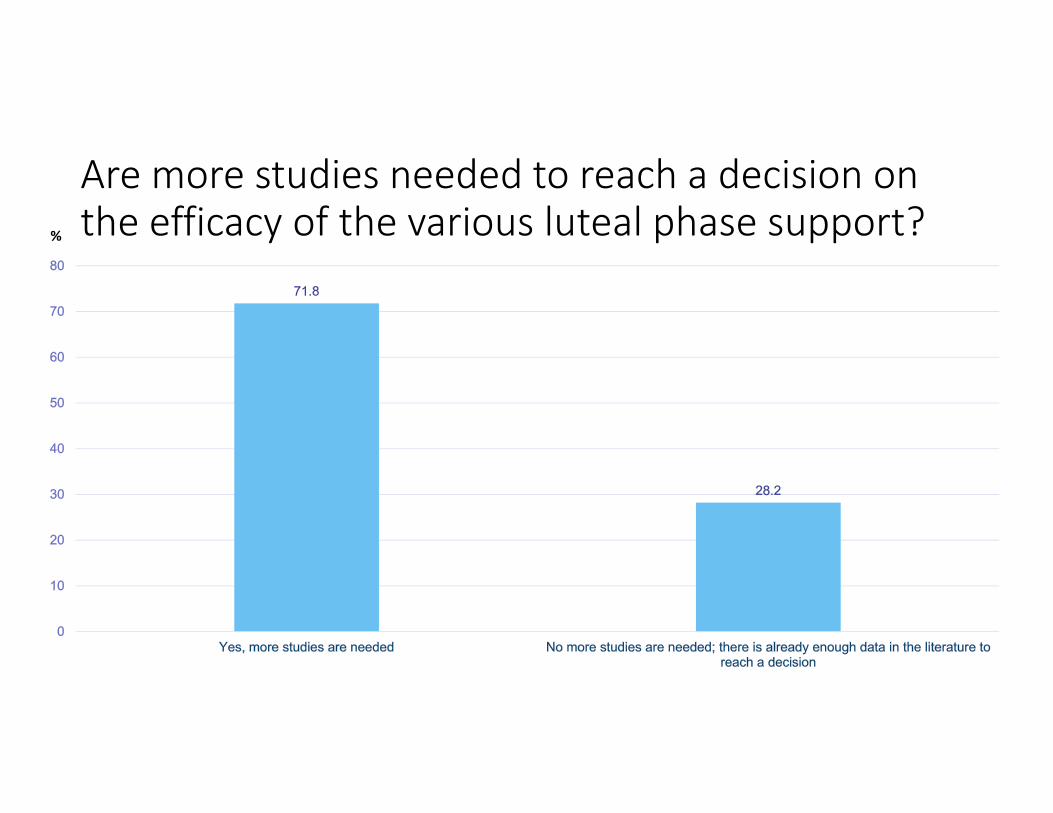
Are more studies needed to reach a decision on the efficacy of the various luteal phase support? %

I would like to see more research data about the following routes/formulations:%

Team

Amount of information generated by meta‐analyses. PubMed search of the words “meta‐analysis” in the published literature.
Greco et al., Heart Lung Vessel. 2013; 5): 219–225.

Van der Linden et al., Cochrane Database of Systematic Reviews 7 JUL 2015