Embed Size (px)
Citation preview
P1: VENDOR/FNV P2: GCQ/FLK QC: FTK
Journal of Genetic Counseling [jgc] PH011-292577 January 5, 2001 10:15 Style file version Nov. 19th, 1999
Journal of Genetic Counseling, Vol. 10, No. 1, 2001
A Survey of Genetic Counselors’ Use of InformedConsent Documents for Prenatal GeneticCounseling Sessions
Gretchen M. Jacobson,1 Patricia McCarthy Veach,2,4 and Bonnie S. LeRoy3
Thirty six members of the Prenatal Diagnosis Special Interest Group of the Na-tional Society of Genetic Counselors were interviewed about their use of informedconsent documents for the genetic counseling component of their prenatal geneticcounseling sessions and their perceptions of the utility and feasibility of such doc-uments. Major findings include (1) None of the genetic counselors currently useda consent document describing the genetic counseling component of the sessionitself; (2) Only three participants stated that they had ever used an informed con-sent document for this component of the session; (3) They disagreed about theimportance and usefulness of such a document; (4) There was variability in theirreported likelihood of using a document if one were available; (5) There was afair amount of agreement about the types of information to include on an informedconsent document for genetic counseling; over half of the sample endorsed 8 of10 topics; and (6) Participants identified 10 obstacles to using such a document.Recommendations for genetic counseling practice, policy, and research are given.
KEY WORDS: informed consent; prenatal genetic counseling.
DEFINITION OF INFORMED CONSENT
Informed consent is an ethical and legal concept concerning an individual’sright to be made aware of the services and activities in which she or he could
1Children’s Hospital Regional Genetics Center, Columbus, Ohio.2Department of Educational Psychology, University of Minnesota, Minneapolis, Minnesota.3Department of Genetics, Cell Biology and Development, Institute of Human Genetics, University ofMinnesota, Minneapolis, Minnesota.
4Correspondence should be directed to Dr. Patricia McCarthy Veach, Department of Educational Psy-chology, University of Minnesota, 139 Burton Hall, 178 Pillsbury Drive, S.E., Minneapolis, Minnesota55455; e-mail: [email protected].
3
1059-7700/01/0200-0003$19.50/1C© 2001 National Society of Genetic Counselors, Inc.

P1: VENDOR/FNV P2: GCQ/FLK QC: FTK
Journal of Genetic Counseling [jgc] PH011-292577 January 5, 2001 10:15 Style file version Nov. 19th, 1999
4 Jacobson, Veach, and LeRoy
participate and to have input into decisions regarding those services (Coreyet al.,1993). Beauchamp and Childress (1994) define informed consent as an individual’sautonomous authorization of a medical intervention or of involvement in research;this type of informed consent refers only to a legally effective authorization as de-termined by prevailing rules (institutional or legal). Schmerler (1998) describes in-formed consent as a process consisting of an information component and a consentcomponent. The information component refers to the disclosure of pertinent in-formation and comprehension of this information whereas the consent componentrefers to a voluntary decision and agreement to undergo a recommended procedure.
According to Beauchamp and Childress (1994), five elements must be presentfor consent to be truly informed: disclosure (of relevant information); competence(to understand and decide); understanding (of the disclosed information and rec-ommendation); voluntariness (in deciding); and consent (decision making andauthorization). Informed consent constitutes a major goal of patient–provider in-teractions and is an important part of the process of shared health care decisionmaking (Schmerler, 1998).
HISTORY OF INFORMED CONSENT IN MEDICINE
Since the Nuremburg trials, the issue of informed consent has been at the fore-front of biomedical ethics (Beauchamp and Childress, 1994). Although the earlyuse of informed consent was to protect research subjects from harm, in recentyears the primary justification for requiring informed consent has been to providethe subject with the knowledge needed to make a rational, autonomous choice(Reilly et al., 1997). Thus, the focus has shifted from the health care provider’sor researcher’s obligation to disclose information, to the quality of a patient’sunderstanding and consent (Beauchamp and Childress, 1994). Today, virtually allmedical and research codes and institutional rules of ethics hold that physicians andinvestigators must procure the informed consent of patients and research subjectsbefore intervention. Consent documents and practices are intended to enable au-tonomous choice, protect patients and research subjects from harm, and encouragemedical professionals to act responsibly.
Although the primary ethical justification for informed consent, as it evolvedhistorically, was to enable autonomous choice by recipients of medical treat-ment and by research subjects, not all authors agree that it is the primary vehicle(Churchillet al., 1998). Katz (1984) argues that in the clinical setting, physicianshave never embraced informed consent as a means of achieving patient autonomy,but have tolerated it only as a necessary legal obligation or, at times, as a formof protective beneficence. Additionally, others (e.g., Robinson and Merav, 1976)found that patients often poorly appreciate the procedure of obtaining “informedconsent,” that they recall little of the interview, and they think that the primary goalis to provide legal protection for the doctor. On the other hand, Daweset al.(1993)found that their sample of 135 patients wanted to know more about their conditions
P1: VENDOR/FNV P2: GCQ/FLK QC: FTK
Journal of Genetic Counseling [jgc] PH011-292577 January 5, 2001 10:15 Style file version Nov. 19th, 1999
A Survey of Genetic Counselors 5
and the proposed treatments. Furthermore, when the patients received this informa-tion in a structured fashion, they remembered more of the potential complicationsof their proposed procedures without increased anxiety. These authors concludedthat gaining the patients’ confidence before treatment greatly reduces the chancesof their seeking legal redress for an unexpected outcome.
Although somewhat controversial, the use of informed consent appears towork well for invasive medical procedures, but not all health care fields involve suchprocedures. An important question concerns the relevance of informed consent asa vehicle for preserving patient rights when the potential risks are less obvious.In order to address this question we examine another area of health care, mentalhealth, to see how practitioners implement informed consent.
HISTORY OF INFORMED CONSENT IN THE MENTALHEALTH FIELD
Mental health professionals have used informed consent documents for manyyears (Coreyet al., 1993). Weinrach (1989) argues that because it is impossible topredict who will need to know what information and when, it makes sense to ensurethat all clients are informed equally from the outset, and advocates the use of writ-ten informed consent documents for psychological counseling and psychotherapy.Benefits include providing clients with “ground rules” and helping clients andcounselors operate from a “common frame of reference”; stimulating discussionof important process and outcome issues; and providing a basis for conflict res-olution. Mental health informed consent documents describe a variety of issuesthat may be relevant during routine care including counselor credentials; how tocontact the counselor; confidentiality and its limits; who to contact in the eventof an emergency; when and how to end treatment; financial concerns; descriptionof services, including potential risks and benefits; alternatives to counseling ser-vices; and due process (an established course of judicial proceedings designed tosafeguard the individual’s legal rights). Weinrach stresses that the guidelines area flexible agreement as opposed to a legally binding contract because there is nopractical way to prepare a set of guidelines that will provide for all contingen-cies. He further suggests that counselors should be willing to discuss, explain, andnegotiate the guidelines with their clients.
Remly (1993) discusses the benefits of written documents for psychologi-cal consultation. He argues that they decrease the likelihood of future conflicts orlegal issues due to misperceptions, and they may help to clarify the complexities ofthe consultation relationship. Written documents force practitioners to commit topolicies on how they conduct their practice. Counselors have the primary responsi-bility for structuring the therapeutic relationship, and clients benefit from knowing,rather than guessing, the structure of this relationship. Remley further argues thatproviding clients with a written description of the most frequently addressed is-sues serves to facilitate the therapeutic relationship and reduces the likelihood that
P1: VENDOR/FNV P2: GCQ/FLK QC: FTK
Journal of Genetic Counseling [jgc] PH011-292577 January 5, 2001 10:15 Style file version Nov. 19th, 1999
6 Jacobson, Veach, and LeRoy
nontherapeutic issues will become a source of unhappiness and conflict. Becauseconsultations may be most effective when patient perceptions match counselorinterventions (Conoleyet al., 1991), written consultation documents may benefitboth parties.
Informed consent appears to be a prevalent component of mental health coun-seling and psychological consultations. Written consent documents may help toestablish guidelines for effective working relationships, and provide clients withpertinent information that allows them to make informed, autonomous decisionsto enter into these relationships.
INFORMED CONSENT IN GENETIC COUNSELING
Genetic counseling which is a service sharing aspect of both the medical andmental health fields, is nevertheless a distinct and unique professional health careservice. An important question concerns the potential role of informed consent inthe genetic counseling arena. The Code of Ethics for Genetic Counseling statesthat genetic counselors provide relevant information for informed decision-makingwhile “respecting client’s beliefs, cultural traditions, inclinations, circumstancesand feelings” (National Society of Genetic Counselors [NSGC], 1992, p. 42).The counselor–patient relationship is based on “values of care and respect for theclient’s autonomy, individuality, welfare and freedom” (NSGC, 1992, p. 42). TheAmerican Society of Human Genetics (ASHG, 1975) defines genetic counseling as“a communication process which deals with the human problems associated withthe occurrence or risk of occurrence, of a genetic disorder in a family” (p. 241),and states that genetic counseling involves “communicating facts to families in away they can understand so that they can choose one course of action appropriatefor them” (p. 241).
An important aspect of genetic counseling involves providing complicatedinformation that patients can understand in order to consent to a plan of action(Elias and Annas, 1994). Ironically, although this is a primary aim for geneticcounselors, there appear to be few mechanisms in place to determine if patientstruly understand the nature of genetic counseling, who their genetic counselor is,the information presented during the session, and the limitations of their patient–counselor relationship. Additionally, because many patients are referred to a ge-netic counselor without full knowledge of what the counselor can provide, therelationship becomes complicated even before it begins.
The process of informed consent would appear to be an essential part of thegenetic counseling relationship. Not only can it increase the likelihood that geneticcounselors maintain a standard of care, but it may promote basic genetic counselinggoals of helping patients understand their options and associated benefits and risksand help them make informed, self-determined decisions. The Council of RegionalNetworks Committee on Ethics (1996) states that “the genetics professional has anobligation to assess the extent of the patient’s knowledge and understanding and to
P1: VENDOR/FNV P2: GCQ/FLK QC: FTK
Journal of Genetic Counseling [jgc] PH011-292577 January 5, 2001 10:15 Style file version Nov. 19th, 1999
A Survey of Genetic Counselors 7
communicate with the patient in appropriate language and levels of complexity”(p. 180).
Adequately assessing the level of a patient’s understanding can be challeng-ing. Typically, genetic counseling services, especially in the prenatal arena, relyupon a 50–60-min session for imparting a great deal of information. Genetic coun-selors are limited in the extent to which they can adequately cover many aspectsof informed consent in this session. Additionally, depending on the focus of thegenetic counseling, there may be differences in the informed consent issues empha-sized. For instance, informed consent for genetic counseling for presymptomaticgenetic testing typically focuses on psychosocial factors and insurance risks inaddition to the implications of test results (Durfyet al., 1998). Informed consentfor genetic screening measures involves decisions about what information shouldbe given to which patients, when it should be presented, who should present it,and how and by whom the results should be conveyed (Elias and Annas, 1994).
Based on a survey of 126 prenatal genetic counselors, Matloff (1994) foundthat the content of prenatal counseling sessions varies significantly from counselorto counselor. She further found a discrepancy between respondents’ interpreta-tions of which issues were important for informed consent and which issues theyconsidered to be applicable to the session. Matloff’s findings raise a number ofissues about informed consent in prenatal counseling: Are patients really gettingall of the pertinent information? Is patient autonomy and informed independentdecision-making fully supported? Are genetic counselors fully fulfilling their roleas described in the Code of Ethics? Are genetic counselors protecting themselveslegally? Matloff concluded that although every session and patient is unique, thereare certain issues that counselors should include in every prenatal session. Shefurther suggested that as a profession, we examine the content of prenatal sessionsand decide if we need quality assurance provisions. Rhodes (1987) argues that“standards which will govern the field of genetic counseling will be based on thedegree of uniformity of conduct that can be expected of practitioners” (p. 13),and Matloff cautions that the courts may have a substantial role in setting thesestandards if the profession does not do so.
SUMMARY OF BACKGROUND
In summary, the literature indicates that informed consent is an importantprocess within the fields of medicine and mental health. Despite some criticisms,theory and research generally support the potential benefits of providing writtendocuments that describe the process and outcome of helping relationships withinthese fields. After reviewing the literature from these fields it is our belief thatgenetic counseling might benefit from a more formal informed consent process tofacilitate effective relationships.
Within genetic counseling, the informed consent process is an essential andvalued tenet of the professional code of ethics. However, no research to date has

P1: VENDOR/FNV P2: GCQ/FLK QC: FTK
Journal of Genetic Counseling [jgc] PH011-292577 January 5, 2001 10:15 Style file version Nov. 19th, 1999
8 Jacobson, Veach, and LeRoy
examined the extent to which provision of informed consent about the nature ofthe genetic counseling process itself is an explicit part of the genetic counselor–patient relationship. In addition, no one has assessed genetic counselors’ percep-tions of informed consent documents. Recognizing the complexity of the geneticcounselor–patient relationship, and using the mental health and medical fields asguides, we investigated the use of informed consent documents in genetic counsel-ing. We interviewed 36 genetic counselors regarding their use of written informedconsent documents describing the prenatal genetic counseling session; their at-titudes about the importance of using written documents; perceived benefits fortheir patients; topics which should be included in such a document; and obstaclesto using such documents within their practice.
The goals of our study were to investigate genetic counselors’ attitudes toward,and use of, informed consent documents for the genetic counseling component.To address these goals, we investigated the following questions: (1) What typesof information do prenatal genetic counselors typically provide during a prenatalgenetic counseling session? (2) Do prenatal genetic counselors currently use aninformed consent document for the genetic counseling component of the session?(3) Have they used such a document in the past? (4) How important would it be touse an informed consent document for the genetic counseling component of theprenatal session? (5) How useful would such a document be for patients? (6) Whattypes of information should be in such a document? (7) How likely would theybe to use a document if it were available? (8) What are the obstacles to usingan informed consent document? (9) What percentage of prenatal patients asksquestions about informed consent issues?
METHODS
Participants
The population of interest is prenatal genetic counselors. We selected thisgroup because prenatal genetic counseling presently encompasses a majority ofgenetic counseling cases (Schneider and Kalkbrenner [1998] found that 70% oftheir 816 respondents to an NSGC professional status survey are prenatal geneticcounselors), and because these counselors generally work with a limited numberof conditions. We solicited potential participants via a letter of invitation mailed toall genetic counselors who were members of the Prenatal Special Interest Groupof the NSGC in 1998 (N = 123). They represented a cross-section of counselorswith special interest and expertise in prenatal genetic counseling. We invited themto participate in a confidential telephone survey investigating the use of informedconsent documents by prenatal genetic counselors. Those willing to be interviewedreturned an enclosed letter of intent by fax, and we scheduled an appointment fora telephonic interview.
P1: VENDOR/FNV P2: GCQ/FLK QC: FTK
Journal of Genetic Counseling [jgc] PH011-292577 January 5, 2001 10:15 Style file version Nov. 19th, 1999
A Survey of Genetic Counselors 9
Data Collection
Instrument
We developed a 14-item interview tool, shown in Appendix, to use in semi-structured telephone interviews. A semistructured interview invites participants torespond to the same questions, which allows for comparison of responses (Patton,1990). We based the questions on our combined clinical experience in geneticcounseling and mental health counseling and on the informed consent literaturefrom the mental health field. After several iterations, we piloted the interviewtool on an advanced genetic counseling student and a prenatal genetic counselorwho were not familiar with the project’s purposes, to determine if they couldunderstand the questions and to be sure that the interviewer clarified in the intro-duction that this was a study of consent for the genetic counseling session. Wemade minor changes in wording based on their feedback. The items include ques-tions about the nature of a participant’s prenatal intake sessions, use of and opin-ions about an informed consent document for genetic counseling, and participantdemographics.
Procedures
G. J. conducted all of the interviews over the telephone, either at each partic-ipant’s office or home. The structured interviews averaged 10 min in length (range5–15 min). G. J. recorded all responses on paper and also took notes during theinterviews to assist in content analysis.
Design and Analysis
G. J., in consultation with B. L. and P. MV, used a “cross-case analysisand pattern matching method” (Patton, 1990) in which she studied each of theinterview questions separately and made comparisons across all interviews. Shecategorized common individual responses and then tallied them. For open-endeditems, she used an inductive analysis procedure (Patton, 1990) to identify patternsin the form of themes. In this approach, researchers immerse themselves in thedetails and specifics of responses to discover important dimensions. They do notbegin with preexisting hypotheses. After each theme, she recorded the participantnumber for each individual who discussed that theme, and then tallied responsesacross the sample.
During the analysis G. J. analyzed variation in participant responses due toprimary focus, work setting, and experience. Because no patterns emerged, wereport the findings for the sample as a whole. We calculated descriptive statisticsfor responses to each of the interview questions (means and standard deviations
P1: VENDOR/FNV P2: GCQ/FLK QC: FTK
Journal of Genetic Counseling [jgc] PH011-292577 January 5, 2001 10:15 Style file version Nov. 19th, 1999
10 Jacobson, Veach, and LeRoy
for continuous data and frequencies for categorical data). In the following section,the results are organized according to interview questions.
This project received human subjects approval from the University ofMinnesota IRB.
RESULTS
Sample Characteristics
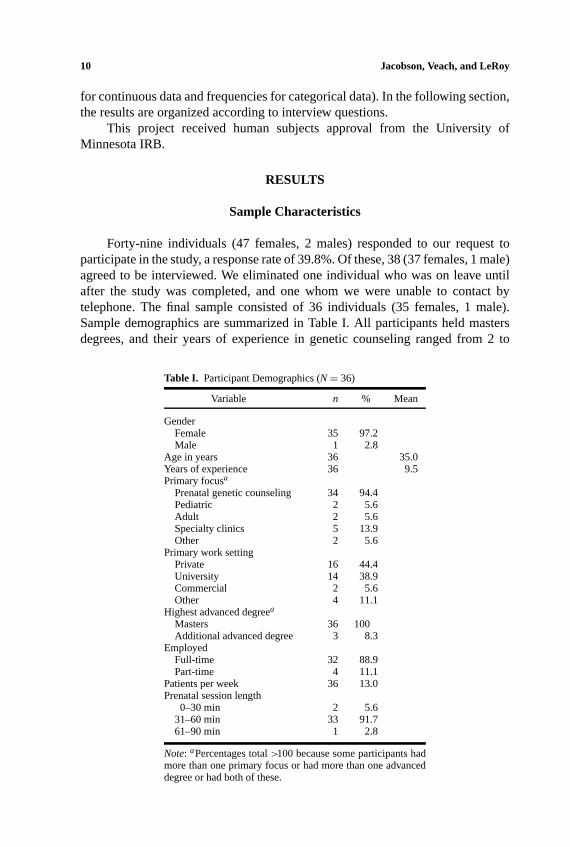
Forty-nine individuals (47 females, 2 males) responded to our request toparticipate in the study, a response rate of 39.8%. Of these, 38 (37 females, 1 male)agreed to be interviewed. We eliminated one individual who was on leave untilafter the study was completed, and one whom we were unable to contact bytelephone. The final sample consisted of 36 individuals (35 females, 1 male).Sample demographics are summarized in Table I. All participants held mastersdegrees, and their years of experience in genetic counseling ranged from 2 to
Table I. Participant Demographics (N= 36)
Variable n % Mean
GenderFemale 35 97.2Male 1 2.8
Age in years 36 35.0Years of experience 36 9.5Primary focusa
Prenatal genetic counseling 34 94.4Pediatric 2 5.6Adult 2 5.6Specialty clinics 5 13.9Other 2 5.6
Primary work settingPrivate 16 44.4University 14 38.9Commercial 2 5.6Other 4 11.1
Highest advanced degreea
Masters 36 100Additional advanced degree 3 8.3
EmployedFull-time 32 88.9Part-time 4 11.1
Patients per week 36 13.0Prenatal session length
0–30 min 2 5.631–60 min 33 91.761–90 min 1 2.8
Note: aPercentages total>100 because some participants hadmore than one primary focus or had more than one advanceddegree or had both of these.

P1: VENDOR/FNV P2: GCQ/FLK QC: FTK
Journal of Genetic Counseling [jgc] PH011-292577 January 5, 2001 10:15 Style file version Nov. 19th, 1999
A Survey of Genetic Counselors 11
20 years (mean= 9.5 years). They came from 24 different states and representedall 6 of the NSGC geographical regions. The majority reported prenatal geneticcounseling as their primary focus, and most worked full-time in either a private oruniversity setting. They saw an average of 13 patients per week, and the majorityreported spending between 31–60 min with a standard prenatal patient.
What Types of Information Do Genetic Counselors Providein a Prenatal Intake Session?
Participants were given nine options for the types of information they coverin a prenatal intake session. As shown in Table II, all of the participants routinelycover five of these topics: genetic risk information specific to a given patient’ssituation; basic genetic information (e.g., genes, chromosomes); family, medical,and social history; agenda for the session; and procedure information. In addition,most reported discussing decision making and patient options if test results areabnormal. Only one participant reported routinely discussing her/his credentialswith patients. About 61% (n = 22) of the participants gave responses that werecategorized as “other,” for example, information about cystic fibrosis testing forCaucasians, AFP testing, time for results, counselor/staff responsibilities for ses-sion, limits to testing, insurance issues, agreement between couples, and mentalhealth issues.
Do Genetic Counselors Currently Use an Informed Consent Document forthe Genetic Counseling Component of the Prenatal Counseling Session?
We determined that none of the participants currently used an informed con-sent document for the genetic counseling component of their prenatal counselingsessions. Although seven of the participants (19%) indicated that they used aconsent document, on further discussion, it was apparent that these are testing
Table II. Types of Information Covered During RoutinePrenatal Intake Sessions (N = 36)
Topic n %
Genetic risk information 36 100Basic genetic information 36 100Family, medical, social history 36 100Agenda for the session 36 100Procedure information 36 100Decision-making process 34 94.4Options if abnormal results obtained 32 88.9Counselor credentials 1 2.8Othera 22 61.1
aFollow-up information; additional testing information; lo-gistical information; psychosocial issues.

P1: VENDOR/FNV P2: GCQ/FLK QC: FTK
Journal of Genetic Counseling [jgc] PH011-292577 January 5, 2001 10:15 Style file version Nov. 19th, 1999
12 Jacobson, Veach, and LeRoy
procedure-related consent forms. One individual stated that a letter is sent priorto the session describing the purpose of genetic counseling, costs, and so forth;another individual reported using a form that describes genetic counseling forpersons who deny genetic counseling services.
Have Genetic Counselors Ever Used an Informed Consent Documentfor the Genetic Counseling Session?
Three individuals (8%) reported using an informed consent document forthe genetic counseling component of genetic counseling in the past, two during agraduate training program, and one at her/his current clinic. The majority of partic-ipants, 92% (n = 33), stated that they had never used such a document. The threeparticipants who used a document in the past indicated that the patients receivedit after the session as a summary of the session. These documents contained riskfigures specific to the patient (e.g., advanced maternal age risk, abnormal triplescreen risk), information pertinent to the patient’s family history (e.g., high riskethnic groups, family history of genetic disease), procedure risks and benefits,description of the counseling session, alternatives to prenatal testing, and patientand counselor signatures. The participants reported that they reviewed the consentdocument with their patients at the end of a session, a process which took lessthan 1 min. They stated that few of their patients (between 0–10%) asked themquestions about these issues after reviewing the form.
How Important Do Genetic Counselors Think it Would be to Use anInformed Consent Document for the Prenatal Genetic Counseling Session?
Participants rated their opinion as to the importance of using an informedconsent document for prenatal genetic counseling on a 5-point, Likert type scale(1= not important at all, 5= very important). The mean importance rating was2.86 (SD=1.17) with both a median and a mode of 3. Approximately 31% (n = 11)gave a rating of “3”; 25% (n = 9) a rating of “2”; and 22% (n = 8) a rating of“4.” Another 14% (n = 5) rated the importance as “1,” while 8% (n = 3) rated theimportance as “5.” It should be noted that seven participants responded betweentwo numbers. Their ratings were adjusted so that they were divided equally betweenthe whole numbers on either side. We used this procedure whenever participantsresponded between two numbers to a question.
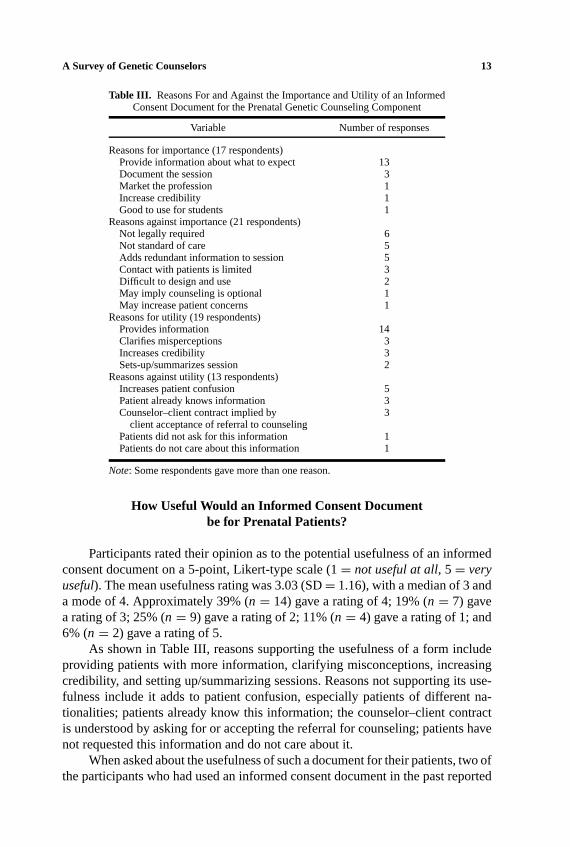
Participants also gave reasons to support their ratings. As shown in Table III,a form would be important because it could provide more information and docu-mentation (e.g., what is/is not covered, limits, etc.), promote genetic counselingand its credibility, and be useful for students. A document might not be importantbecause it is not required; is not a standard of care in genetic counseling; is redun-dant; would be difficult to design and use; might imply that counseling is optional;and could raise patient concerns.
P1: VENDOR/FNV P2: GCQ/FLK QC: FTK
Journal of Genetic Counseling [jgc] PH011-292577 January 5, 2001 10:15 Style file version Nov. 19th, 1999
A Survey of Genetic Counselors 13
Table III. Reasons For and Against the Importance and Utility of an InformedConsent Document for the Prenatal Genetic Counseling Component
Variable Number of responses
Reasons for importance (17 respondents)Provide information about what to expect 13Document the session 3Market the profession 1Increase credibility 1Good to use for students 1
Reasons against importance (21 respondents)Not legally required 6Not standard of care 5Adds redundant information to session 5Contact with patients is limited 3Difficult to design and use 2May imply counseling is optional 1May increase patient concerns 1
Reasons for utility (19 respondents)Provides information 14Clarifies misperceptions 3Increases credibility 3Sets-up/summarizes session 2
Reasons against utility (13 respondents)Increases patient confusion 5Patient already knows information 3Counselor–client contract implied by 3
client acceptance of referral to counselingPatients did not ask for this information 1Patients do not care about this information 1
Note: Some respondents gave more than one reason.
How Useful Would an Informed Consent Documentbe for Prenatal Patients?
Participants rated their opinion as to the potential usefulness of an informedconsent document on a 5-point, Likert-type scale (1= not useful at all, 5= veryuseful). The mean usefulness rating was 3.03 (SD= 1.16), with a median of 3 anda mode of 4. Approximately 39% (n = 14) gave a rating of 4; 19% (n = 7) gavea rating of 3; 25% (n = 9) gave a rating of 2; 11% (n = 4) gave a rating of 1; and6% (n = 2) gave a rating of 5.
As shown in Table III, reasons supporting the usefulness of a form includeproviding patients with more information, clarifying misconceptions, increasingcredibility, and setting up/summarizing sessions. Reasons not supporting its use-fulness include it adds to patient confusion, especially patients of different na-tionalities; patients already know this information; the counselor–client contractis understood by asking for or accepting the referral for counseling; patients havenot requested this information and do not care about it.
When asked about the usefulness of such a document for their patients, two ofthe participants who had used an informed consent document in the past reported
P1: VENDOR/FNV P2: GCQ/FLK QC: FTK
Journal of Genetic Counseling [jgc] PH011-292577 January 5, 2001 10:15 Style file version Nov. 19th, 1999
14 Jacobson, Veach, and LeRoy
that it was useful. One participant stated that at the time of use, ultrasound was notperformed in the same office, and the patient had to decide about the procedurebefore having the ultrasound. However, because this is often not the case now, theparticipant was unsure if the informed consent document would still be as useful.Additionally, one participant indicated that it was more useful for the counselor asa legal document rather than of use to the patient, and that the agency eventuallyreplaced the form with a summary letter.
What Types of Information Should be Included in an InformedConsent Document?
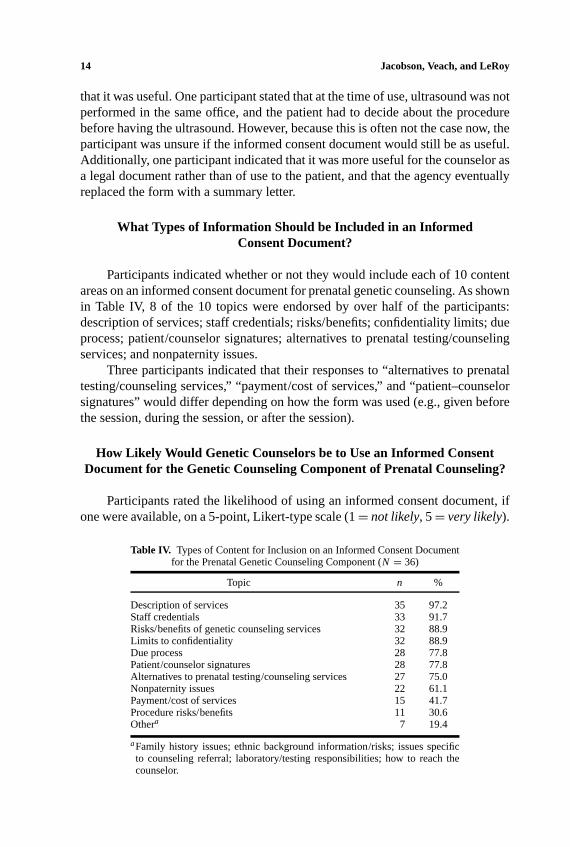
Participants indicated whether or not they would include each of 10 contentareas on an informed consent document for prenatal genetic counseling. As shownin Table IV, 8 of the 10 topics were endorsed by over half of the participants:description of services; staff credentials; risks/benefits; confidentiality limits; dueprocess; patient/counselor signatures; alternatives to prenatal testing/counselingservices; and nonpaternity issues.
Three participants indicated that their responses to “alternatives to prenataltesting/counseling services,” “payment/cost of services,” and “patient–counselorsignatures” would differ depending on how the form was used (e.g., given beforethe session, during the session, or after the session).
How Likely Would Genetic Counselors be to Use an Informed ConsentDocument for the Genetic Counseling Component of Prenatal Counseling?
Participants rated the likelihood of using an informed consent document, ifone were available, on a 5-point, Likert-type scale (1= not likely, 5= very likely).
Table IV. Types of Content for Inclusion on an Informed Consent Documentfor the Prenatal Genetic Counseling Component (N = 36)
Topic n %
Description of services 35 97.2Staff credentials 33 91.7Risks/benefits of genetic counseling services 32 88.9Limits to confidentiality 32 88.9Due process 28 77.8Patient/counselor signatures 28 77.8Alternatives to prenatal testing/counseling services 27 75.0Nonpaternity issues 22 61.1Payment/cost of services 15 41.7Procedure risks/benefits 11 30.6Othera 7 19.4
aFamily history issues; ethnic background information/risks; issues specificto counseling referral; laboratory/testing responsibilities; how to reach thecounselor.

P1: VENDOR/FNV P2: GCQ/FLK QC: FTK
Journal of Genetic Counseling [jgc] PH011-292577 January 5, 2001 10:15 Style file version Nov. 19th, 1999
A Survey of Genetic Counselors 15
Table V. Reasons For and Against Using an Informed Consent Document for the PrenatalGenetic Counseling Component
Variable Number of reasons
Reasons for using (12 respondents)Provide patients with more information 7Help cover liability 4Would use if standard of care 3Allows patients to decline counseling 2Prevents patients from receiving counseling 1
from untrained individualsReasons against using (13 respondents)
Not standard of care 4No need for a document 3Time constraints 3Information covered elsewhere 1Movement away from consent forms to information sheets 1
Note: Some respondents gave more than one reason.
The mean likelihood rating was 3.19 (SD= 1.41), with both a median and modeof 3. Approximately 28% (n = 10) gave a rating of 3; 25% (n = 9) gave a ratingof 5; 17% (n = 6) gave a rating of 4; 17% (n = 6) gave a rating of 1; and 14%(n = 5) gave a rating of 2. As shown in Table V, reasons why they would belikely to use a document include it would provide more information; help coverliability; they would use it if it were the standard of care; it would allow patientsto decline genetic counseling; and it might prevent people from receiving geneticcounseling from untrained individuals. Reasons why they would be unlikely touse a document include it is not the standard of care; there is no apparent needfor such documents; time constraints; information is covered elsewhere; it addsto the amount of paper; and hospitals are moving toward informational sheets.Several participants (n = 5) stated that they would have to receive approval fromtheir supervisors, legal departments, and so forth, in order to use a form; and threeparticipants stated that they would try the form and see how it worked for theirpatients.
What Are the Obstacles to Using an Informed Consent Documentfor the Genetic Counseling Component of Prenatal Counseling?
As shown in Table VI, 34 individuals identified 10 different obstacles: timeconstraints (e.g., a document would use time, which is limited); difficulties devel-oping a standardized form (e.g., due to differences in opinion about content, clarity,and distribution of the document, and the need for the document to be in multiplelanguages); patient negative reactions (e.g., intimidates patients, increases anxi-ety, makes sessions less personal); utility of a form (e.g., too many forms already;redundant with information in other forms); legal issues (e.g., need to be approved

P1: VENDOR/FNV P2: GCQ/FLK QC: FTK
Journal of Genetic Counseling [jgc] PH011-292577 January 5, 2001 10:15 Style file version Nov. 19th, 1999
16 Jacobson, Veach, and LeRoy
Table VI. Types of Obstacles to Using an Informed ConsentDocument for the Prenatal Genetic Counseling Component
(n = 34)
Obstacle n %
Time constraints 16 47.1Difficulties developing a standardized form 12 35.3Patient negative reactions 11 32.4Utility of a form 8 23.5Legal issues 4 11.8Depends on when/how used 3 8.8Unavailability 1 2.9Implies genetic counseling is optional 1 2.9Negative professional reactions 1 2.9Ethical consistency 1 2.9
Note: Percentages total>100 because some participants iden-tified more than one obstacle.
by legal department); depends on how/when used; lack of availability of a form;makes genetic counseling appear to be optional; professional negative reactions(e.g., physicians and genetic counselors might not accept their use); and ethicalconsistency (e.g., not sure an informed consent document is consistent with thegenetic counseling code).
What Percentage of Prenatal Patients Asks Questions About InformedConsent Issues?
Participants were asked to indicate the percentage of their patients who askthem questions about informed consent issues. Approximately 61% (n = 22) indi-cated that 10% or less of their patients ask them questions about informed consentissues. However, 14% (n = 5) reported that over half of their patients ask suchquestions. Another 11% (n = 4) stated that 11%–20% of their patients ask ques-tions, 8% (n = 3) indicated that 21%–30% ask questions, one participant (3%)said that 31%–40% ask such questions, and another participant (3%) reported that41%–50% of patients ask these types of questions.
DISCUSSION
The purposes of this study were to investigate genetic counselors’ use of andattitudes toward informed consent documents that describe the prenatal geneticcounseling process. Thirty-six individuals participated in interviews from whichseveral themes emerged.
Informed consent documents that focus on the genetic counseling componenttypically are not used in prenatal genetic counseling.None of the participants

P1: VENDOR/FNV P2: GCQ/FLK QC: FTK
Journal of Genetic Counseling [jgc] PH011-292577 January 5, 2001 10:15 Style file version Nov. 19th, 1999
A Survey of Genetic Counselors 17
reported currently using a consent form that addresses the genetic counselingcomponent itself. Only three individuals indicated that they had ever used sucha document. These results raise important questions about the degree to whichpatients are informed about the content and process of the prenatal genetic coun-seling session. It appears that prenatal counselors may provide verbal informationabout some aspects of the process. Indeed, the entire sample reported that theyroutinely cover the agenda for the session, almost all of the participants reportedlydiscuss the decision making process, and one individual describes her/his cre-dentials. However, there is variability in the topics covered. In addition, becausecounselors present the information verbally, there is a question about the extent towhich the information is standardized.
Historically, genetic counseling informed consent has concerned testing andassociated procedures, and not the counseling itself. The present results suggestthat this is the case for prenatal genetic counselors. For example, several partic-ipants reported using consent to treat forms. Also, typical discussion topics dur-ing prenatal genetic counseling included genetic risk information and procedureinformation, options if abnormal results are obtained, additional testing informa-tion, and logistical information such as limits to testing.
Genetic counselors disagree about the importance and usefulness of an in-formed consent document for prenatal genetic counseling and about their like-lihood of using such a document. When asked to rate their opinions as to theimportance of informed consent documents, the sample was distributed acrossthe 5-point scale, suggesting that their opinions were quite varied. Their varyingopinions may be partially explained by the fact that about half of the participantsanecdotally indicated never having thought about or considered the use of in-formed consent documentation for the prenatal genetic counseling session prior tothis investigation. Additionally, most of the participants had no experience usingsuch a document. It seems as though it would be difficult during a 10-min inter-view to effectively rate the importance of a consent document that one has neitherconsidered nor used before.
There was slightly greater agreement about the utility of such a document.About half of the sample stated that it would be useful or very useful for their pa-tients because it could describe the process, clarify expectations, and enhance thecredibility of services. These reasons are supported by McCarthy Veachet al.’sstudy (McCarthy Veachet al., 1999) of 28 former clients’ perceptions of theimpact of genetic counseling. One-third of their sample reported experiencing ob-stacles that included confusion and misperceptions about the process. The authorsrecommended addressing these with either an informed consent document or aprecounseling information sheet.
Some of the reasons participants gave against the usefulness of an informedconsent document suggest that patients do not need or desire this type of docu-mentation. These reasons are inconsistent with the results of Shilohet al. (1990)
P1: VENDOR/FNV P2: GCQ/FLK QC: FTK
Journal of Genetic Counseling [jgc] PH011-292577 January 5, 2001 10:15 Style file version Nov. 19th, 1999
18 Jacobson, Veach, and LeRoy
and Hallowellet al.(1997) who found that genetic counseling patients respondedfavorably to a written summary of their sessions. This inconsistency may be duein part to the samples—we surveyed geneticcounselorswhereas these authorsassessed genetic counselingpatientsdirectly. Moreover, some of our sample’s re-sponses may reflect a lack of experience using informed consent documents forthe session itself.
Close to half of the sample stated that they would be either likely or verylikely to use an informed consent document if it were available, for reasons thatincluded providing information to patients and covering liability, while almostone-third reported that they would be unlikely to use such a document, because itis not a standard of care and is not needed. The remaining participants rated theirlikelihood a “3,” which suggests a certain degree of ambivalence.
In our opinion, some of the reasons given against informed documents “begthe question,” for example, “a document is hard to design.” The present resultssuggest that it may not be that hard to design. Over three-fourths of the sampleagreed upon 8 of 10 topics to include on such a document. Furthermore, informedconsent documents developed for use in the mental health profession could serve asmodels. Another reason given is that a document “might raise concerns about whatis discussed.” We would argue that a documentshouldraise concerns for somepatients in certain situations (e.g., who has access to medical records). Anotherreason given is that contact with patients is limited. When considered broadly,contact typically involves one genetic counseling session, follow-up calls, and thepossibility of another session if test results are abnormal. Also, the issues thatare covered can be quite intense, despite the restricted amount of time spent onthem. Therefore, genetic counseling is not necessarily a limited relationship. Iftime constraints are an issue, a document could be mailed to patients before theirappointment and reviewed at the beginning of the session.
We also question participant beliefs that a document would not be useful. Forexample, it could be informative for individuals whose reading skills are betterthan their listening skills. In addition, not all patients have accurate information;McCarthy Veachet al.(in press) found that many genetic counseling patients havemisperceptions (e.g., that the genetic counselor can conduct medical procedures).Moreover, it is an empirical question whether patients “understand the contract byaccepting a referral”; in our experience many patients say, “I don’t know why I’mhere; my doctor told me to come.” We need to survey patients to see whether theywould prefer to receive a document, would care about it, and/or whether it wouldconfuse them.
We take issue with the belief that “presumptive consent is sufficient.” Becausemany patients come through referral, we cannot assume that their decision isnecessarily informed, nor completely voluntary. Some participants claimed thatthe information is “covered elsewhere.” But, can we assume that consent is obtainedverbally? A comparison of what the present sample reportedly discusses with whatthey stated should be part of an informed consent document indicates little overlap.

P1: VENDOR/FNV P2: GCQ/FLK QC: FTK
Journal of Genetic Counseling [jgc] PH011-292577 January 5, 2001 10:15 Style file version Nov. 19th, 1999
A Survey of Genetic Counselors 19
Informed consent does involve more paperwork, but does not necessarily “take toomuch time” as the participants who used a document in the past reported needingabout l min to review with patients.
There is a fairly consistent body of information that genetic counselors believeshould be included on an informed consent document. Over half of the sampleendorsed eight topics for inclusion on an informed consent document for prenatalgenetic counseling. These findings suggest that although prenatal counselors differin their opinions about the importance and utility of informed consent documents,they are in close agreement about the types of issues to include in such a document.These topics generally were not covered in the genetic counseling sessions. Forexample, only one participant reported actually discussing her/his credentials aspart of a session, and none of the sample reported verbally providing a descriptionof genetic counseling, risks/benefits of this service, confidentiality limits, dueprocess, testing/counseling alternatives, and nonpaternity. These results supportthose of Mattloff (1994) and Burke and Kolker (1994) who found variability inthe types of issues discussed by genetic counselors in prenatal genetic counselingsessions. They also raise the possibility that patients are not aware of the natureof genetic counseling, and therefore cannot provide consent for a service that theydo not understand.
It is our belief that patients are not well informed about confidentiality limits(e.g., access to medical records, duty to warn/report, etc.). In addition, they maynot consider other potential risks such as the emotional reactions precipitated bygenetic counseling. McCarthy Veachet al.(1999) found that almost two-thirds ofthe emotions experienced by their sample during genetic counseling were negative,including anxiety, anger, confusion, and sadness.
Genetic counselors perceive several barriers to using an informed consentdocument for the genetic counseling component of prenatal counseling. The mostfrequently mentioned barrier was time. Time constraints could be addressed bymailing the document in advance to the patient and then discussing another copyof the document at the beginning of the session.
A number of participants expressed concerned about the form itself (e.g.,content, clarity, distribution, language, negative patient reactions). Preparing aform in advance, distributing it to referring physicians, and/or utilizing translationservices are all methods to alleviate these obstacles. Remly (1993) found that inpsychological consultation some individuals complain that contracts are too legal-istic and they signify distrust between the consultant and consultee. Nevertheless,he argues that consultation is a business arrangement and should be entered intoin a businesslike fashion. A written document can identify misunderstandings andresolve problems before they arise. In genetic counseling, if the form is designedto provide patients with more information and to ensure that they gain the mostfrom their sessions, it is possible that patients would view a document positively.Research is needed to investigate the impact of informed consent documents ongenetic counseling patients.

P1: VENDOR/FNV P2: GCQ/FLK QC: FTK
Journal of Genetic Counseling [jgc] PH011-292577 January 5, 2001 10:15 Style file version Nov. 19th, 1999
20 Jacobson, Veach, and LeRoy
Limitations of the Study
The primary limitation of this study is the sample size and modest responserate, which limit generalizability. It is not known whether those individuals who didnot participate would respond in some significantly different way from the presentsample. For instance, the individuals who responded may have had a particularinterest in the topic. Also, a larger sample could yield greater clarity of the issues.Another limitation is that the participants may have inaccurate perceptions aboutpatient reactions to informed consent. Researchers should survey prenatal geneticcounseling patients in order to directly assess their attitudes.
Additionally, the interviewer noticed anecdotally that some participants ap-peared confused or surprised by the topic, despite the information provided in theletter inviting their participation. For example, some participants believed that thistype of informed consent could be obtained by giving patients a written docu-ment at the end of the counseling session. Informed consent cannot be obtained“after the fact.” Some individuals appeared to be ambivalent about this issue be-cause their responses vacillated between favorable and unfavorable ratings. Thisraises the possibility that their self-reported behaviors would not match their actualbehaviors if informed consent documents were available.
Finally, only prenatal genetic counselors were surveyed in this study. Addi-tional research should be done to determine how other types of genetic counselorsview the use of informed consent documents, whether any use such forms, andwhat they believe should be included in these types of documents.
Suggestions for Practice and Policy
Despite the limitations of this study, the results raise some considerationsfor practice. The process of prenatal genetic counseling involve risks that includeincreased anxiety and other intense negative affect due to the provision of certaininformation (McCarthy Veachet al., 1999), tension and conflict among familymembers, especially when they disagree (e.g., over prenatal testing; McCarthyVeachet al., in press; Sorensonet al., 1981); feelings that the discussion of someoptions such as abortion are “forced upon” patients who regard these options ascompletely untenable (McCarthy Veachet al., 1999); unanticipated information(e.g., nonpaternity); and limits to confidentiality (e.g., women who come for pre-natal genetic counseling and testing may not realize that the results of genetictesting cannot be given to other family members without their permission). In ad-dition, as demonstrated in the present study, at least some patients have questionsabout informed consent issues. Increasingly authors are calling for the provisionof informed consent for genetic counseling (Elias and Annas, 1994; Matloff, 1994;McCarthy Veachet al., 1999). A written document would standardize the infor-mation provided, and it might mitigate problems before they occur.
P1: VENDOR/FNV P2: GCQ/FLK QC: FTK
Journal of Genetic Counseling [jgc] PH011-292577 January 5, 2001 10:15 Style file version Nov. 19th, 1999
A Survey of Genetic Counselors 21
A written document is intended to educate clients about the genetic counselingprocess, reduce misperceptions or confusion, identify potential risks and benefits,and clarify procedures for due process. Hallowellet al. (1997) found that clientswho are appropriately prepared for genetic counseling may benefit more from thesession. Informed consent documents could also benefit the genetic counselingprofession by promoting the profession and its goals, and by providing some legalprotection in the event of a dispute over the information presented during a session(Matloff et al., 1994; Rhodes, 1987).
Recently, Dunne and Warren (1998) claimed that prenatal genetic counselors“sometimes provide one-sided negative information to women undergoing prenataldiagnosis which promotes abortion of what are considered ‘defective’ fetuses”(p. 198). The authors equate the misleading information provided by geneticcounselors, and the subsequent termination of pregnancies, with the eugenicsmovement. These are disturbing accusations that might be partially addressedthrough the use of informed consent documents.
One possible direction for policy based on the present results is a recom-mendation that the NSGC Professional Issues Committee examine the issue ofusing informed consent documents for genetic counseling. This group could pro-vide guidance about whether genetic counselors should use such documents intheir practice and help to clarify the nature of informed consent about the geneticcounseling process.
Recommendations for Future Research
The present results suggest that genetic counseling may be “caught in themiddle” between the medical and mental health models of service provision. Be-cause genetic counseling is a service that involves both aspects of standard medicalcare and mental health care, there may be a need to develop an informed consentprocess unique to the profession. To determine whether informed consent docu-ments should be a standard of care in genetic counseling, additional research isneeded. Researchers could design a prototypical document for prenatal geneticcounseling, using the topics identified by the present sample, and implement theform in several prenatal genetic counseling centers. Studies comparing the per-ceptions of counselors and patients who used the consent forms and those whodid not would be helpful in determining the efficacy of this type of document forgenetic counseling. For example, do informed consent documents decrease patientmisperceptions? Do they increase, decrease, or have no effect on patient anxietyand proactivity during a session? A study comparing informed consent documentswith informational sheets could determine which is more effective for increas-ing client satisfaction and knowledge. Informed consent is not unique to prenatalgenetic counseling. Researchers should design, implement, and evaluate consentforms for each specialty area. This type of research would help to determine the
P1: VENDOR/FNV P2: GCQ/FLK QC: FTK
Journal of Genetic Counseling [jgc] PH011-292577 January 5, 2001 10:15 Style file version Nov. 19th, 1999
22 Jacobson, Veach, and LeRoy
extent to which genetic counseling patients receive sufficient information to makeinformed and voluntary decisions to participate in genetic counseling.
APPENDIX: INTERVIEW QUESTIONS
Introduction: Informed consent has been used in the mental health field formany years. Informed consent is an ethical and legal concept that concerns anindividual’s right to be apprised of the types of services s/he will receive andto participate in the decisions pertaining to these services. Informed consent ingenetic counseling involves the provision of an appropriate amount and type ofinformation to allow clients to make autonomous decisions about genetic screeningand its results. In this project, we are attempting to determine if there is a need forinformed consent in prenatal genetic counseling.
1. Approximately how many prenatal patients do you see per week?2. How much time do you spend with a standard prenatal patient?
0–30 min 31–60 min 61–90 min >90 min3. Which of the following types of information do you cover in a routine
prenatal intake session? (See Table I for list of topics presented to partic-ipants.)
4. Do you currently use an informed consent statement for your prenatalcounseling session? Is this form designed for the procedure/the geneticcounseling session/or both?
5. Have you ever used an informed consent statement that covers the geneticcounseling session at any other prenatal clinic besides your current setting?
6. On a scale from 1–5, 1 beingnot important at alland 5 beingvery impor-tant, how important do you think it is to use an informed consent statementabout genetic counseling in a prenatal setting? Why/Why not?
IF yes to #4 or 5:
7a. Do you send this form to the patient in advance? Give them the form atcheck in? Or give during the session?
7b. Does your consent form cover the following? (See Table II for list of topicspresented to participants.)
7c. Do you review the consent form with the patient?7d. If yes, how much time does it take you to review the consent?7e. What percentage of your patients ask you questions about informed consent
issues?7f. Do you think this form is helpful/useful to your patients? Why?7g. Could you send us a copy of your forms?
P1: VENDOR/FNV P2: GCQ/FLK QC: FTK
Journal of Genetic Counseling [jgc] PH011-292577 January 5, 2001 10:15 Style file version Nov. 19th, 1999
A Survey of Genetic Counselors 23
IF no to #4 and 55
8a. On a scale of 1–5, 1 beingnot useful at all, 5 beingvery useful, do you thinkan informed consent form would be useful for your patients? Why/Why not?
8b. If a statement were to be used in your setting, what types of informationwould you include on an informed consent form? (See Table II for a list oftopics presented to participants.)
8c. On a scale of 1–5, 1 beingnot very likelyand 5 beingvery likely, how likelywould you be to use a consent form if it were available to you?
8d. What percentage of your patients ask you questions about informed consentissues?
9. What do you perceive to be barriers/obstacles to using an informed consentform?
10–14. Participants demographics.
REFERENCES
American Society of Human Genetics (1975) Genetic counseling.Am J Hum Genet27: 240–242.Beauchamp TL, Childress JF (1994)Principles of Biomedical Ethics: Fourth Edition. New York:
Oxford University Press, pp 120–189.Burke MB, Kolker A (1994) Variation in content in prenatal genetic counseling interviews.J Genet
Counsel3: 23–38.Churchill LR, Collins ML, King N, Pemberton SG, Wailoo KA (1998) Genetic research as therapy:
Implications of gene therapy for informed consent.J Law, Med Ethics26: 38–47.Conoley CW, Conoley JC, Ivey DC, Scheel MJ (1991) Enhancing consultation by matching the coun-
selees’ perspectives.J Counsel Dev69: 546–549.Corey G, Corey MS, Callanan P (1993)Issues and Ethics in the Helping Professions(4th Ed). Pacific
Grove, CA: Brooks/Cole.Council of Regional Networks Committee on Ethics (1996) Code of ethics and principles for genetics
professionals.Am J Med Genet65: 179–183.Dawes PJD, O’Keefe L, Adcock S (1993) Informed consent: Using a structured interview changes
patients’ attitudes toward informed consent.J Laryn Otol107: 775–779.Dunne C, Warren C (1998) Lethal autonomy—the malfunction of the informed consent mechanism
within the context of prenatal diagnosis of genetic variants.Issues Law Med14: 165–202.Durfy S, Buchanan T, Burke W (1998) Testing for inherited susceptibility to breast cancer: A survey
of informed consent forms for BRCA 1 and BRCA 2 mutation testing.Am J Med Genet75: 82–87.
Elias S, Annas GJ (1994) Generic consent for genetic screening.New Engl J Med330: 1611–1613.Hallowell N, Murton F, Statham H, Green JM, Richards, MPM (1997) Women’s need for informa-
tion before attending genetic counseling for familial breast or ovarian cancer: A questionnaire,interview, and observational study (1997)Br Med J314: 281–283.
Katz J (1984)The Silent World of Doctor and Patient. New York: Free Press.Matloff ET (1994) Practice variability in prenatal genetic counseling.J Genet Counsel3: 215–231.McCarthy Veach P, Bartels DM, LeRoy BS (in press) Ethical and professional challenges posed by
patients with genetic concerns: A report of focus group discussions with genetic counselors,physicians, and nurses.J Genet Counsel
5Since no one currently used an informed consent document for the genetic counseling component, allparticipants responded to questions 8–9.
P1: VENDOR/FNV P2: GCQ/FLK QC: FTK
Journal of Genetic Counseling [jgc] PH011-292577 January 5, 2001 10:15 Style file version Nov. 19th, 1999
24 Jacobson, Veach, and LeRoy
McCarthy Veach P, Truesdell SE, LeRoy BS, Bartels DM (1999) Client perceptions of the impact ofgenetic counseling: An exploratory study.J Genet Counsel8: 191–216.
National Society of Genetic Counselors, Inc. (1992) NSGC code of ethics.J Genet Counsel1: 41–43.
Patton MQ (1990)Qualitative Evaluation and Research Methods. Newbury Park, CA: Sage Publica-tions.
Reilly P, Boshar M, Holtzman N (1997) Ethical issues in genetic research: Disclosure and informedconsent.Nat Genet15: 16–20.
Remly TP Jr. (1993) Consultation contracts.J Counsel Dev72: 157–158.Rhodes A (1987) Legal issues in perinatal care.Birth Def: Orig Art SerXXIII: 1–15.Robinson G, Merav A (1976) Informed consent recall by patients tested post-operatively.Ann Thor
Surg22: 209–212.Schmerler S (1998) Ethical and legal issues. In: Baker DL, Schuette JL, Uhlmann WR (eds),A Guide
to Genetic Counseling. New York: Wiley-Liss, pp 249–276.Schneider KA, Kalkbrenner KJ (1998) National Society of Genetic Counselors Professional Status
Survey.Perspect Genet Counsel Suppl20: S1–S8.Shiloh S, Avdor O, Goodman RM (1990) Satisfaction with genetic counseling: Dimensions and mea-
surement.Am J Med Genet37: 522–529.Sorenson JR, Swazey J, Scotch N (1981) Reproductive pasts, reproductive futures: Genetic counseling
and its effectiveness.Birth Def: Orig Art SerXVII: 1–192.Weinrach SG (1989) Guidelines for clients of private practitioners: Committing the structure to print.
J Counsel Dev67: 299–300.





























