Embed Size (px)
Citation preview
Nurse Education in Practice (2009) 9, 61–71
Nurse
www.elsevier.com/nepr
Educationin Practice
A survey of first year student nurses’ experiencesof learning blood pressure measurement
Lesley Baillie *, Joan Curzio 1
Faculty of Health and Social Care, London South Bank University, 103 Borough Road, London SE1 0AA,United Kingdom
Accepted 11 May 2008
14do
1
KEYWORDSBlood pressuremeasurement;Student nurses;Clinical skills;Supervision
71-5953/$ - see front mattei:10.1016/j.nepr.2008.05.00
* Corresponding author. Tel.E-mail address: baillilj@lsbTel.: +44 207 815 5901; fa
r �c 2003
: +44 20u.ac.ukx: +44 20
Summary Blood pressure (BP) measurement is an important clinical nursing skill.Informal evaluation triggered concerns about first year student nurses’ opportuni-ties to practise it. Therefore 447 first year pre-registration nursing students com-pleted evaluative questionnaires following two 6-week clinical placements. Thedata were analysed using SPSS v.13 for analysis; open comments were analysed the-matically. A third of the respondents (n = 137) had pre-course experience in measur-ing BP. Ninety-five percent (n = 425) attended the university skills laboratorysession. Only 36% (n = 158) of students measured BP using both electronic and man-ual equipment in both placements and 6% (n = 27) did not practise this skill in eitherplacement. Students undergoing non-hospital placements reported fewer practiceopportunities. A large number of students reported never having been supervisedwhile measuring BP; they were more likely to be supervised while measuring BPmanually than electronically. Students’ self-confidence in BP measurementincreased over the first year but larger number of students were confident in elec-tronic BP. To conclude, experiences of learning BP measurement varied in terms ofopportunities to practise, equipment used, supervision levels and self-confidence.Students’ experiences of learning other clinical skills may also differ, which hasimplications for healthcare education generally.
�c 2008 Elsevier Ltd. All rights reserved.
Introduction
As educators we are chargedwith preparing pre-reg-istration nursing students to be fit for purpose and fit
8 Elsevier Ltd. All rights rese
7 815 8457.
7 815 5907.
for practice. In the United Kingdom (UK), 50% of stu-dents’ learning occurs in clinical placements (NMC,2004) where it is expected that mentors will super-vise students and provide constructive feedback(NMC, 2006). However, there have been concernsabout the variability of students’ skills learning intheir clinical placements which have affected com-petence levels at registration (NMC, 2005). Carlisle
rved.

62 L. Baillie, J. Curzio
et al. (1999) study highlighted a practical skills def-icit in newly qualified nurses.
Blood pressure (BP) measurement is an impor-tant nursing skill and it is commonly assumed thatstudent nurses can easily learn BP measurementearly in their education (O’Brien and Davison,1994). However, studies have indicated a generallypoor level of training in BP measurement for nursesand doctors (Bove et al., 1989; Gleichmann et al.,1989; Feher et al., 1992; Kemp et al., 1994; Pietz,1994) and deficits in both performance (Cienki etal., 2004; Drevenhorn et al., 2001; Feher et al.,1992; Bogan et al., 1993; Torrance and Serginson,1996a) and knowledge (Feher et al., 1992; Kempet al., 1994; McVicker, 2001; Carney et al., 1999;Armstrong, 2002; Kennedy and Curzio, 1996; Boganet al., 1993; Torrance and Serginson, 1996b; Nolanand Nolan, 1993; Bagir and Ahmed, 1997; Gleich-mann et al., 1989; Markandu et al., 2000). At theauthors’ university, in a pilot of a manual bloodpressure measurement Objective Structured Clini-cal Examination (OSCE), only 51% passed. Students’informal evaluative comments following this OSCEindicated varied placement opportunities to learnBP measurement which students perceived im-pacted on their confidence and ability. In particu-lar, practice with manual BP equipment(sphygmomanometer and auscultation with stetho-scope) was limited, while practice with electronicequipment using oscillometry was more frequent.As only a few studies have focused on student nurseeducation, none of which addressed students’placement experiences of BP measurement, therewas a need for further investigation.
Therefore in 2006, an anonymous educationalaudit survey of first year pre-registration nursingstudents was undertaken to systematically evalu-ate students’ BP measurement experience. Theaims were to explore:
(1) Students’ pre-course BP measurementexperience,
(2) Students’ pre-placement skills laboratory BPmeasurement learning,
(3) Students’ opportunities to practise BP mea-surement during placements with manualand electronic equipment and frequency ofsupervision,
(4) How levels of self-confidence in BP measure-ment over the first year of the pre-registra-tion nursing programme varied withdifferent placement experiences.
This paper’s focus is on students’ experiences oflearning to measure BP, including skills laboratory
practice and opportunities to rehearse the skillduring placements.
Background/literature
Context for skills acquisition inpre-registration nurse education
TheNursing andMidwifery Council (NMC),which reg-ulates the nursing profession in the UK, identifiesthat all student nurses need to be able to performclinical skills safely (NMC, 2004, 2007a). UK studentnurses must achieve proficiencies within four do-mains of practice (professional and ethical practice,care delivery, care management, and personal andprofessional development) to enter the nursing reg-ister (NMC, 2004). These proficiencies include skillsbut the NMC (2007a) recently published more spe-cific guidance about certain groups of skills to bedeveloped during pre-registration nursing pro-grammes. The ability to measure and record vitalsigns accurately, including blood pressure,was iden-tified as an essential skill for student nurses toachieve prior to commencing the second year oftheir pre-registration nursing programme.
Development of skills competence andself-confidence
Knowing how to do a practical skill (or motor skill)can be termed ‘know-how’ type of knowledge –practical expertise and skill that is acquiredthrough practice and experience (Manley, 1997).Lack of a skilled performance can jeopardise bothsafety and comfort for patients. Learning motorskills, such as BP measurement, requires practice:the opportunity to repeat the skill and gain feed-back (Quinn and Hughes, 2007). Therefore, studentnurses need opportunities to practise skills andlearn from their experience.
Student assessment of their self-confidence inregards to clinical skill acquisition has been usedpreviously as an outcome measure assessing curric-ulum (Clark et al., 2004) and curriculum change(Farrand et al., 2006). Adequate practice withand without supervision should lead to competencyand a resultant sense of self-confidence. Kissinger(1998) concept analysis recognises that overconfi-dence in nursing practice exists. However, she fo-cuses on clinical decision making rather thanclinical skills performance. With a curriculumbased on student self-directed learning (O’Shea,2003), students assessing their self-confidence in
A survey of first year student nurses’ experiences of learning blood pressure measurement 63
carrying out a skill can trigger more self-study,practice and request for supervised practice.
Learning skills in skills laboratories
Jefferies (2005) defines simulations as activitiesmimicking the reality of clinical environments.Skills laboratories can provide the opportunity forstudents to learn through simulation, with studentsdeveloping their skills in a controlled, safe environ-ment (Knight, 1998). In simulation students practiseskills without risk of harming patients and then ap-ply these skills in the clinical setting (Wilford andDoyle, 2006). Thus students can practise blood pres-sure measurement on their peers in skills laborato-ries prior to practising with patients in placementsettings. Studies evaluating simulation based onstudents’ perceptions are overwhelmingly positive(Hogg et al., 2006; Johnson et al., 1999; Weller,2004; Ker et al., 2003; Mole and McLafferty, 2004;Robertson, 2006). It is argued that simulation canimprove health professionals’ competency and pro-mote safe practice (Hogg et al., 2006; Ziv et al.,2000). Simulation is increasingly commonplace inhealthcare education (Bradley, 2003; Feingold etal., 2003) and the benefits of simulation have beenrecognised by the NMC (2007b). However, whileskills laboratory learning clearly has benefits andcan ease pressure on clinically based learning (Fre-eth and Fry, 2005) it does not replace skills practicewithin clinical placements.
Learning clinical skills in placement
The clinical learning environment is an essentialelement of nurse education (Midgley, 2006) andthe NMC (2006) details how students’ effectivelearning and assessment in practice placementscan be facilitated. However, while quality clinicalplacements are central in nursing education (Lev-ett-Jones et al., 2006; Hartigan-Rogers et al.,2007), variability in students’ placement experi-ences has been reported (Andrews et al., 2006).
In Morgan (2002) phenomenological study of sixstudent nurses’ experiences on their first place-ments, students reported that being shown howto carry out skills was helpful but in a further re-lated paper, Morgan (2006) suggested that staffbusyness led to students seeing skills performeddifferently and that students should therefore betaught correct procedures in the skills laboratory.Clearly this was a very small study but it gave in-sights into a little explored topic. Astin et al.(2005) conducted focus groups with a purposivesample of 16 registered nurses, identifying that
their expectations of first year students’ clinicalskills and knowledge were not consistently met.They emphasised the need for a range of funda-mental skills, including recording vital signs, butexpected expertise which the authors argue wasunrealistic. The participants also questionedwhether laboratory taught sessions were beneficialand whether lecturers were clinically credible,thus inferring that placement learning was morerelevant.
Savage (1999) studied the influence of staffnurses in creating a ward learning environmentfor student nurses. A minority of students reportedthat staff nurses repeatedly demonstrated newprocedures to them. Wards which were viewed ashaving favourable learning environments weremost likely to be associated with providing satisfac-tory levels of supervision. However, almost half thestudents (44%, n = 44) reported too little supervi-sion. A key factor inhibiting learning was studentsbeing left to work on their own instead of workingwith qualified staff. Sixty-one percent of studentsidentified an unwillingness of staff nurses to teach,which hindered their learning. Nevertheless, thereis an expectation that student nurses will developtheir competence in clinical skills, such as BP mea-surement, under the supervision of placementstaff.
Teaching and learning of BP measurement
While it is important that student nurses developaccurate BP measurement skills, Kemp et al.(1994) concluded that little importance is givento BP measurement training and that healthcarestaff knowledge is inadequate. A few studies haveinvestigated student nurses’ BP measurement skillsand knowledge (Baldwin et al., 1991; Beeson andKring, 1999; Bogan et al., 1993; Torrance and Serg-inson, 1996a, 1996b). However there were no stud-ies identified which explored students’opportunities to practise BP measurement duringpractice placements.
Of the studies examining student nurses’ BPmeasurement performance, only Bogan et al.(1993) study focused on assessing performance inpractice. The majority of the senior students stud-ied failed to comply with the American Heart Asso-ciation’s (AHA) recommended steps for measuringBP (including proper placement of the cuff, estima-tion of the systolic pressure by palpation, calcula-tion of the maximum inflation level, properplacement of the stethoscope). Students cited bar-riers to compliance as lack of time and the physicalenvironment. In one of the few UK studies,
64 L. Baillie, J. Curzio
Torrance and Serginson (1996a) observed 50 firstyear pre-registration nursing students’ BP measure-ment. They provided no information about the stu-dents’ learning, either in the university or inplacement. The results indicated that the studentslacked the knowledge and skills to accurately mea-sure blood pressure using a sphygmomanometerand auscultation and the authors recommendedthat the teaching and practice of BP measurementshould be reviewed.
A general lack of training of healthcare staff inBP measurement has been identified (Kemp etal., 1994). Pietz (1994) surveyed US nursing schoolsand found that most nurse education programmesdid not follow the AHA guidelines exactly; time,lack of proper equipment and lack of training werethe main barriers. Gleichmann et al. (1989) identi-fied that both nurses and doctors had inadequatetraining in BP measurement at pre-registration le-vel. Bove et al. (1989) surveyed fifty US educa-tional institutions, finding that all taught BP inthe first year of study using various methods: lec-ture, laboratory practice, monitoring students ina simulated setting, reading, self-instruction andvideo tapes. Students did not receive adequatepractice using sphygmomanometers, only half theinstitutions used dual-headed stethoscopes to eval-uate accuracy and there was generally a casual ap-proach to evaluating students’ accuracy. No similarUK studies were identified. Various university-based methods of teaching BP measurement havebeen evaluated, including use of instructional vid-eos (Beeson and Kring, 1999; Baldwin et al.,1991; Grim and Grim, 1995) and a CD-ROM (Baueret al., 2001). The results indicated that these re-sources can complement traditional methods butnot replace lecturer contact.
Regarding the equipment with which studentslearn to measure BP, studies almost exclusively fo-cus on the use of manual equipment. Increasingly,electronic equipment is used to measure BPthrough oscillometry and the Medicines and Health-care products Regulatory Agency (MHRA) (2006)identified that clinical staff are therefore losingskills in manual BP measurement. Such a situationdisadvantages student nurses as they too will havereduced opportunities to measure BP with manualequipment and the staff supervising them may havebecome deskilled themselves. However, the Inde-pendent Advisory Group on Blood Pressure Monitor-ing in Clinical Practice (2005) recommended thatauscultation should continue to be taught tohealthcare workers as appropriate, highlightingthat in certain clinical conditions, oscillometry isinappropriate. In addition, electronic devices arenot available in all clinical settings, particularly
non-acute areas, and there remains concern aboutthe accuracy of BP measurement equipment(Carney et al., 1999). However, Markandu et al.(2000) argue that validated automatic devices,being less liable to measurement and observererror, should replace manual equipment.
In summary, student nurses must have opportu-nity to develop skills such as BP measurement un-der supervision with initial skills laboratorylearning and opportunities to practise in placementwith patients/clients. However there is a generallack of research relating to student nurses’ experi-ences of learning clinical skills in placement andspecifically BP measurement. Studies relating tolearning BP measurement have focused almostexclusively on use of manual equipment despiteelectronic equipment being used increasingly.Overall, there was a need to investigate students’experiences of learning to measure BP using differ-ent equipment in both skills laboratory and prac-tice placement settings, hence the audit wasconducted.
Methods
Four hundred and forty-seven students from onepre-registration nursing cohort completed ques-tionnaires anonymously in the classroom towardsthe end of their first year. The students had re-ceived one skills laboratory session on BP measure-ment of 1.5 h prior to placement, with somestudents undergoing additional practice in a prepa-ration for practice day. Students had then under-gone two 6-week placements in their chosenspecialty: adult nursing (n = 251), children’s nurs-ing (n = 90), mental health nursing (n = 90) or learn-ing disability nursing/social work (n = 16).Placements were provided by a wide range of Na-tional Health Service acute and primary caretrusts, social care, educational and charitableorganisations.
The questionnaire content was identified fromlecturers’ experience and knowledge and refinedseveral times. The tool aimed to elicit quantitativedata regarding students’ opportunities to practisemeasuring BP with manual and electronic equip-ment, and the frequency with which they weresupervised. They were also asked to rate theirself-confidence in measuring BP prior to thecourse, after they attended a university skills labo-ratory session and at the end of their first year.Two open questions invited students’ views abouthow learning BP measurement could be enhancedand any other comments. The data were enteredinto SPSS v.13 for analysis and percentages and

A survey of first year student nurses’ experiences of learning blood pressure measurement 65
frequencies calculated. The open comments wereanalysed thematically.
As not all students responded to every questionand some questions were only answered if theyhad replied positively to another, percentageswere calculated on the basis of the proportionwho replied to a particular question. These dataare given in the results.
As this was an educational audit utilising ananonymous questionnaire, formal ethical approvalwas not required. Approval to access students wasobtained from the Head of Department and CourseDirector. Students were informed it was voluntaryand that consent to participation was assumed bycompletion and return of the questionnaire. Thequestionnaire was distributed and collected by anacademic outside of the auditing team.
Results
The 447 students represented 79% of the cohort’s565 students. A third of the respondents (n = 137)had prior experience in measuring BP. Ninety-fivepercent (n = 425) of those responding attendedthe university skills laboratory session and nearlyall of those (98%; n = 416) had practised the BritishHypertension Society recommended manual BP(MBP) measurement technique (www.bhsoc.org).Unfortunately, 50% (n = 214) did so only once andonly 43% (n = 182) practised with a lecturer usinga double headed stethoscope. Thirty-seven percent(n = 157) of the students practised electronic BP(EBP) with only 12% (n = 50) practising EBP morethan once. One hundred and fourteen students(26%) made suggestions about the university’s in-put, the vast majority requesting more skills labo-ratory practice. Students requested more time tolearn, particularly prior to first placements, withsmaller groups, less noise in the room and higherlevels of supervision from lecturers.
Overall only about a third of students reportedmeasuring BP using both electronic and manualequipment in both placements and 6% reportedthey did not practise this skill in either of theirplacements (Table 1). Some students wrote com-ments about their lack of opportunity to practiseBP:‘Practice does make perfect but some of us do nothave opportunity to practise at all which I think is abit unfair’. (Student 45)
It is interesting to note that 71 (16%) studentspractised measuring BP using electronic equipmentin both placements but did not practise manuallymeasuring BP in either. In comparison, only 14 stu-
dents (3%) practised MBP on both placements butnot EBP. Twenty-four students wrote specific com-ments about MBP measurement in placement, mostrelating to lack of availability of manual equipmentbut also supervision issues:‘Many students have not had the opportunity topractise manual BP on the wards for many reasonse.g. lack of equipment, lack of motivation fromstaff’. (Student 238)
Some students commented that wards were toobusy to allow time to practise MBP and others ex-pressed that learning to measure BP on placementcaused anxiety to patients. In addition, the BHStechnique taught in the university (in particular,initial systolic estimation by palpation) was notnecessarily encountered in practice causing confu-sion:‘Confusion about technique taught in skills labcompared to way done in ward i.e. don’t have topump cuff twice in reality’. (Student 49)
However some students had more positive expe-riences:‘On my clinical placement I was not allowed to useelectronic equipment, that [was] why I developedmy confidence using the manual blood pressureequipment’. (Student 290)
Table 1 also indicates that opportunities to prac-tise BP measurement were affected by type of clin-ical placements with students undergoing non-hospital placements being disadvantaged in termsof practice opportunities, illustrated by this com-ment:‘Being in the community for both placements did notleave room for practice. I had a chat withmymentorand discussed the procedure but not practice’. (Stu-dent 21)
Further examination of BP practice opportunitiesrevealed that type of hospital placements affectedpractice: 58% (n = 113) of students who had twoacute hospital placements practised MBP and EBPin both placements, compared with only 16%(n = 6) of students whose placements were both inmental health wards. One student commented:‘Iwish I had the opportunity to practisemore skills asmental health students are at a disadvantage’. (Stu-dent 59)
Those students who had opportunity to practiseBP experienced variable levels of supervision butthey were more likely to be supervised while mea-suring BP manually than electronically (Table 2). Asurprisingly large number of students reportednever having been supervised while measuring BP.There were occasional comments regarding the
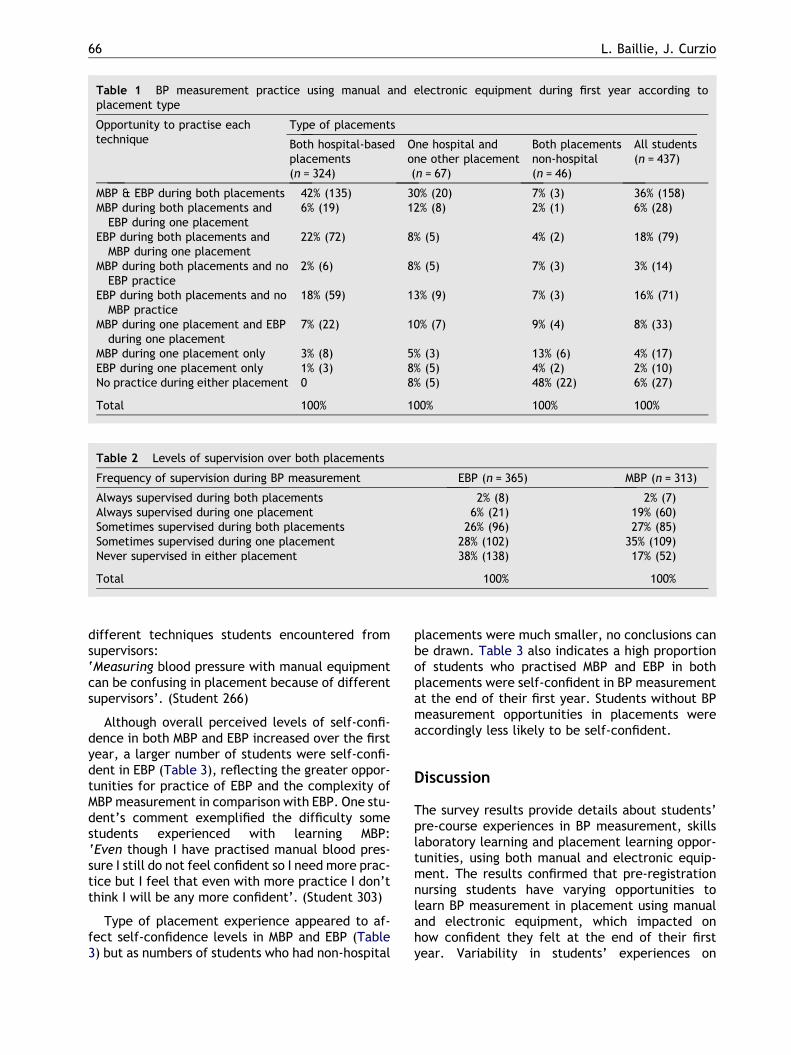
Table 1 BP measurement practice using manual and electronic equipment during first year according toplacement type
Opportunity to practise eachtechnique
Type of placements
Both hospital-basedplacements(n = 324)
One hospital andone other placement(n = 67)
Both placementsnon-hospital(n = 46)
All students(n = 437)
MBP & EBP during both placements 42% (135) 30% (20) 7% (3) 36% (158)MBP during both placements andEBP during one placement
6% (19) 12% (8) 2% (1) 6% (28)
EBP during both placements andMBP during one placement
22% (72) 8% (5) 4% (2) 18% (79)
MBP during both placements and noEBP practice
2% (6) 8% (5) 7% (3) 3% (14)
EBP during both placements and noMBP practice
18% (59) 13% (9) 7% (3) 16% (71)
MBP during one placement and EBPduring one placement
7% (22) 10% (7) 9% (4) 8% (33)
MBP during one placement only 3% (8) 5% (3) 13% (6) 4% (17)EBP during one placement only 1% (3) 8% (5) 4% (2) 2% (10)No practice during either placement 0 8% (5) 48% (22) 6% (27)
Total 100% 100% 100% 100%
Table 2 Levels of supervision over both placements
Frequency of supervision during BP measurement EBP (n = 365) MBP (n = 313)
Always supervised during both placements 2% (8) 2% (7)Always supervised during one placement 6% (21) 19% (60)Sometimes supervised during both placements 26% (96) 27% (85)Sometimes supervised during one placement 28% (102) 35% (109)Never supervised in either placement 38% (138) 17% (52)
Total 100% 100%
66 L. Baillie, J. Curzio
different techniques students encountered fromsupervisors:‘Measuring blood pressure with manual equipmentcan be confusing in placement because of differentsupervisors’. (Student 266)
Although overall perceived levels of self-confi-dence in both MBP and EBP increased over the firstyear, a larger number of students were self-confi-dent in EBP (Table 3), reflecting the greater oppor-tunities for practice of EBP and the complexity ofMBP measurement in comparison with EBP. One stu-dent’s comment exemplified the difficulty somestudents experienced with learning MBP:‘Even though I have practised manual blood pres-sure I still do not feel confident so I need more prac-tice but I feel that even with more practice I don’tthink I will be any more confident’. (Student 303)
Type of placement experience appeared to af-fect self-confidence levels in MBP and EBP (Table3) but as numbers of students who had non-hospital
placements were much smaller, no conclusions canbe drawn. Table 3 also indicates a high proportionof students who practised MBP and EBP in bothplacements were self-confident in BP measurementat the end of their first year. Students without BPmeasurement opportunities in placements wereaccordingly less likely to be self-confident.
Discussion
The survey results provide details about students’pre-course experiences in BP measurement, skillslaboratory learning and placement learning oppor-tunities, using both manual and electronic equip-ment. The results confirmed that pre-registrationnursing students have varying opportunities tolearn BP measurement in placement using manualand electronic equipment, which impacted onhow confident they felt at the end of their firstyear. Variability in students’ experiences on
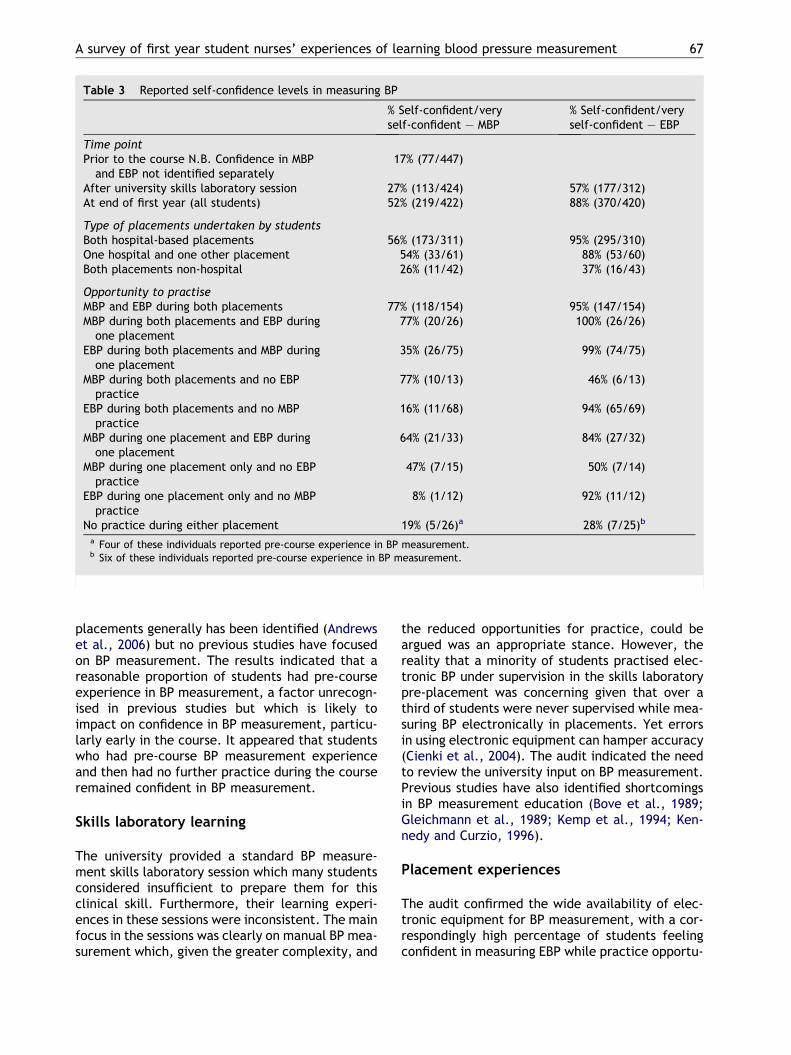
Table 3 Reported self-confidence levels in measuring BP
% Self-confident/veryself-confident – MBP
% Self-confident/veryself-confident – EBP
Time pointPrior to the course N.B. Confidence in MBP
and EBP not identified separately17% (77/447)
After university skills laboratory session 27% (113/424) 57% (177/312)At end of first year (all students) 52% (219/422) 88% (370/420)
Type of placements undertaken by studentsBoth hospital-based placements 56% (173/311) 95% (295/310)One hospital and one other placement 54% (33/61) 88% (53/60)Both placements non-hospital 26% (11/42) 37% (16/43)
Opportunity to practiseMBP and EBP during both placements 77% (118/154) 95% (147/154)MBP during both placements and EBP during
one placement77% (20/26) 100% (26/26)
EBP during both placements and MBP duringone placement
35% (26/75) 99% (74/75)
MBP during both placements and no EBPpractice
77% (10/13) 46% (6/13)
EBP during both placements and no MBPpractice
16% (11/68) 94% (65/69)
MBP during one placement and EBP duringone placement
64% (21/33) 84% (27/32)
MBP during one placement only and no EBPpractice
47% (7/15) 50% (7/14)
EBP during one placement only and no MBPpractice
8% (1/12) 92% (11/12)
No practice during either placement 19% (5/26)a 28% (7/25)b
a Four of these individuals reported pre-course experience in BP measurement.b Six of these individuals reported pre-course experience in BP measurement.
A survey of first year student nurses’ experiences of learning blood pressure measurement 67
placements generally has been identified (Andrewset al., 2006) but no previous studies have focusedon BP measurement. The results indicated that areasonable proportion of students had pre-courseexperience in BP measurement, a factor unrecogn-ised in previous studies but which is likely toimpact on confidence in BP measurement, particu-larly early in the course. It appeared that studentswho had pre-course BP measurement experienceand then had no further practice during the courseremained confident in BP measurement.
Skills laboratory learning
The university provided a standard BP measure-ment skills laboratory session which many studentsconsidered insufficient to prepare them for thisclinical skill. Furthermore, their learning experi-ences in these sessions were inconsistent. The mainfocus in the sessions was clearly on manual BP mea-surement which, given the greater complexity, and
the reduced opportunities for practice, could beargued was an appropriate stance. However, thereality that a minority of students practised elec-tronic BP under supervision in the skills laboratorypre-placement was concerning given that over athird of students were never supervised while mea-suring BP electronically in placements. Yet errorsin using electronic equipment can hamper accuracy(Cienki et al., 2004). The audit indicated the needto review the university input on BP measurement.Previous studies have also identified shortcomingsin BP measurement education (Bove et al., 1989;Gleichmann et al., 1989; Kemp et al., 1994; Ken-nedy and Curzio, 1996).
Placement experiences
The audit confirmed the wide availability of elec-tronic equipment for BP measurement, with a cor-respondingly high percentage of students feelingconfident in measuring EBP while practice opportu-

68 L. Baillie, J. Curzio
nities and confidence using manual equipment waslower. The findings thus supported the MHRA (2006)concerns about loss of skills in manual BP measure-ment. However, the Independent Advisory Groupon Blood Pressure Monitoring in Clinical Practice(2005) highlighted that there is still a need for com-petence in manual BP measurement. Inaccuraciesin electronic BP equipment have been identified(Carney et al., 1999) and furthermore, most ofthe university’s local placement providers hadexplicitly expressed that manual BP was an essen-tial skill for nurses. Yet the students’ allocatedclinical placements clearly impacted on opportuni-ties to practise BP measurement with manual andelectronic equipment. Most students in acute hos-pital wards gained experience in BP measurementusing both manual and electronic equipment. How-ever, fewer students on placements in mentalhealth wards and community placements gainedthese opportunities. As there are concerns aboutthe physical health of people with learning disabil-ities (Department of Health, 2001) and mentalhealth problems (Department of Health, 2006),students need to acquire physical health assess-ment skills, such as BP measurement.
Supervision of students in practice andimplications for patient care
It was expected that such junior students wouldhave been initially supervised during BP measure-ment on their clinical placements so that mentorscould ensure their technique was correct and givefeedback on their performance. Indeed, the NMC(2006) identifies that the mentor’s role includes‘supervising students in learning situations and pro-viding them with constructive feedback on theirachievements’. Saarikoski and Leino-Kilpi (2002)indicated the importance of quality supervision tostudent satisfaction with their clinical placements.Students must have feedback in order to improvetheir performance (Quinn and Hughes, 2007),which would normally be given during or aftersupervised practice. Thus the survey’s findings,that 38% of students had never been supervised inmeasuring BP electronically, and 17% had neverbeen supervised during manual BP measurement,during either of their first year placements, givecause for concern. Savage (1999) also identifiedlow supervision levels of student nurses in place-ments. Reasons why students were not supervisedwere not explicitly explored but some students’comments supported Morgan (2006) findings thatthe busy clinical environment had a negative im-pact on learning skills in practice. Astin et al.
(2005) found high expectations of students in termsof their skills performance but students cannot be-come competent in their clinical skills withoutsupervised practice opportunities.
If students are unsupervised during BP measure-ment, errors in BP measurement technique, com-monly identified in previous research, may gouncorrected. Common errors include arm positionfor sitting measurement and cuff size assessment(Armstrong, 2002; Kennedy and Curzio, 1996),which are relevant whether manual or electronicequipment is used. Accurate BP measurement isessential as important clinical decisions are madeon the basis of BP measurement results (Bogan etal., 1993; Kemp et al., 1994); errors can lead tomisdiagnosis and incorrect treatment (Armstrong,2002; Bagir and Ahmed, 1997; Pietz, 1994). Therecould be detrimental effects on patient outcomestherefore if junior students measure BP unsuper-vised and inaccurate recordings are obtained. Inaddition, if errors are not corrected due to unsu-pervised practice, any deficits in technique arelikely to become embedded. Andrews et al.(1998) suggested that continued repetition of skillsmay lead to merely habitual behaviour. The auditonly identified whether students had been super-vised; quality of supervision, if present, was notexplored. As studies have indicated poor BP mea-surement techniques among qualified nurses de-spite high levels of confidence (Carney et al.,1999; Kennedy and Curzio, 1996; Nolan and Nolan,1993), the quality of supervision could in any casebe questionable.
Self-assessment of confidence andimplications
Newly qualified staff nurses have cited lack of self-confidence as an issue for them (Clark and Holmes,2007). However, within medical education it hasbeen highlighted that self assessment of confi-dence should not be used as a means to judge‘accuracy’, but can assist individuals in reflectingon their practice (Stewart et al., 2000). In thisaudit, the assessment of self-confidence has beenused as an outcome measure, as lack of self-confi-dence was an issue raised by the students whofailed to adequately demonstrate this clinical skillduring a pilot manual blood pressure measurementOSCE the previous year.
Although the percentage of students who wereself-confident in BP measurement increased aftertwo clinical placements, only about half the stu-dents were self-confident in manual BP measure-ment. A higher percentage of students who had

A survey of first year student nurses’ experiences of learning blood pressure measurement 69
practised manual BP on both their placements wereconfident in this skill. Self-confidence in electronicBP however developed more readily, with a veryhigh percentage of students feeling self-confidenteven if they practised it in only one placement.Clearly, if manual BP measurement is a desiredand expected skill for nurses, all student nursesneed equitable opportunities for sufficient prac-tice. If these cannot be guaranteed during place-ments for all students, then universities need toprovide additional opportunities in skills laborato-ries. However, consolidating skills laboratory prac-tice by measuring manual BP in actual clinicalsettings is preferable for developing confidence.Morgan (2002) highlighted how active participationin patient care in conjunction with experiencednurses, develops students’ self-confidence. It mustbe recognised however that while opportunities topractise may increase students’ self-confidence,their performance may not improve if they areunsupervised.
Dissemination and action
The survey’s results were disseminated to the uni-versity’s pre-registration nursing lecturers and toall practice placement providers (hospitals andcommunity settings). Each of the latter was pro-vided with individualised reports, presenting howtheir allocated students evaluated their opportuni-ties to learn BP measurement, their supervisionlevels and confidence. This feedback has led to sev-eral initiatives to enhance BP measurement learn-ing opportunities, including follow-up audits beingconducted by several placement providers. Theuniversity has reviewed the input on BP measure-ment for first year students, and has increasedpractice time, skills laboratory equipment andstaff: student ratios, and developed further re-sources to complement laboratory-based learning.As part of their practice-based assessment, stu-dents are now required to be directly observedand assessed on vital signs measurement on place-ment using standardised assessment criteria, priorto the midpoint and final assessments.
Strengths, limitations and recommendationsfor further study
The audit illuminated the reality of first year stu-dents’ experiences of learning to measure BP inthe university and placement setting. While previ-ous studies indicated deficits in health care profes-sionals’ BP performance, no previous studies wereidentified that had examined practice-based learn-
ing of this fundamental skill. This is an importantarea as it gives insight into reasons why theremay be skills deficits and how therefore, thesemight be addressed.
A key limitation was that although we had datafrom a previous cohort indicating limited abilitiesto demonstrate MBP, there was no direct observa-tion of BP measurement technique as a componentof this audit. Results relied on the accuracy ofrespondents’ recollections of their experiences ofBP measurement. It would be useful to conduct fur-ther studies which include observation of studentsin practice, and the supervision they encounterwhile practising clinical skills, such as BP measure-ment. It would also be illuminating to measure therelationship between perceived confidence in BPmeasurement and actual performance.
Conclusions
To conclude, an audit of first year nursing students’experiences of learning BP measurement indicatedvariability in terms of opportunities to practise,equipment used and supervision levels. Studentswere more likely to practise electronic BP in clini-cal placements leading to higher levels of confi-dence with this equipment but there is a generalexpectation currently that nurses will be able tomeasure BP with manual equipment. Students inmental health and community placements weredisadvantaged in their opportunities to practiseBP measurement. Supervision during skills perfor-mance is necessary to ensure good practice devel-ops but frequency was surprisingly low for first yearstudents. While many students’ confidence im-proved due to practice in placements, their abilityto measure BP accurately may not have done so.More supervised skills laboratory practice timecould compensate for lack of supervised opportuni-ties during placements, but placement allocationand supervision of first year students in practicealso needs review.
While this survey focused solely on BP measure-ment, it is likely that students’ experiences oflearning other clinical skills may also vary. TheNMC has identified a range of essential skills whichstudents must achieve, of which BP measurementis just one example, and emphasises that assess-ment should take place in practice wherever possi-ble (NMC, 2007a). To promote effective, safepatient/client care, it is essential that studentnurses experience effective initial skills laboratorypreparation, followed by supervised practice andfeedback during placements and assessment to

70 L. Baillie, J. Curzio
ensure skills are being performed safely andeffectively.
References
Andrews, G.J., Brodie, D.A., Andrews, J.P., et al., 2006.Professional roles and communications in clinical place-ments: a qualitative study of nursing students’ perceptionsand some models for practice. International Journal ofNursing Studies 43 (7), 861–874.
Andrews, M., Gidman, J., Humphreys, A., 1998. Reflection: doesit enhance professional nursing practice?. British Journal ofNursing 7 413–417.
Armstrong, R.S., 2002. Nurses’ knowledge of error in bloodpressure measurement technique. International Journal ofNursing Practice 8 (3), 118–126.
Astin, F., McKenna, L., Newton, J., Moore-Coulson, L., 2005.Registered nurses’ expectations and experiences of first yearstudents’ clinical skills and knowledge. Contemporary Nurse18 (3), 279–291.
Bagir, M., Ahmed, K., 1997. Knowledge of blood pressuremeasurement among a teaching hospital staff in a developingnation. Journal of Human Hypertension 11 (8), 495–499.
Baldwin, D., Hill, P., Hanson, G., 1991. Performance ofpsychomotor skills: comparison of two teaching strategies.Journal of Nursing Education 30 (8), 367–370.
Bauer, M., Geront, M., Huynh, M., 2001. Teaching bloodpressure measurement: CD-ROM versus conventional class-room instruction. Journal of Nursing Education 40 (3), 138–141.
Beeson, S.A., Kring, D.L., 1999. The effects of two teachingmethods on nursing students’ factual knowledge and perfor-mance of psychomotor skills. Journal of Nursing Education 38(8), 357–359.
Bogan, B., Kritzer, S., Deane, D., 1993. Nursing studentcompliance to standards for blood pressure measurement.Journal of Nursing Education 32 (2), 90–92.
Bove, P.A., Owen, L., Ekelman, F.P., 1989. Investigation of themethods used to teach blood pressure measurement tech-niques. Health Values 13 (3), 36–42.
Bradley, P., 2003. Simulation in clinical learning. MedicationEducation 37 (Suppl 1), 1–5.
Carlisle, C., Luker, K.A., Davies, C., et al., 1999. Skills compe-tency in nurse education: nurse managers’ perceptions ofdiploma level preparation. Journal of Advanced Nursing 29(5), 1256–1264.
Carney, S., Gillies, A., Green, S., et al., 1999. Hospital bloodpressure measurement: staff and device assessment. Journalof Quality in Clinical Practice 19 (2), 95–98.
Cienki, J., DeLuca, L., Daniel, N., 2004. The validity ofemergency department triage blood pressure measurements.Academic Emergency Medicine 11 (3), 237–243.
Clark, M.C., Owen, S.V., Tholcken, M.A., 2004. Measuringstudent perceptions of clinical competence. Journal ofNursing Education 43 (12), 548–554.
Clark, T., Holmes, S., 2007. Fit for practice? An exploration ofthe development of newly qualified nurses using focusgroups. International Journal of Nursing Studies 44, 1210–1220.
Department of Health, 2001. ValuingPeople: A New Strategy forLearning Disability for the 21St Century. DH, London.
Department of Health, 2006. From Values to Action: The ChiefNursing Officer’s Review of Mental Health Nursing. DH,London.
Drevenhorn, E., Hakansson, A., Petersson, K., 2001. Bloodpressure measurement – an observational study of 21 publichealth nurses. Journal of Clinical Nursing 10, 189–194.
Farrand, P., McMullan, M., Jowett, R., Humphreys, A., 2006.Implementing competency recommendations into pre-regis-tration nursing curricula: effects upon levels of confidence inclinical skills. Nurse Education Today 26, 97–103.
Feher, M., Harris-St. John, K., Lant, A., 1992. Blood pressuremeasurement by junior doctors– a gap in medical education?Health Trends 24 (2), 59–61.
Feingold, C.E., Calaluce, M., Kallen, M.A., 2003. Computerizedpatient model and simulated clinical experiences: evaluationwith baccalaureate nursing students. Journal of NursingEducation 43 (4), 156–163.
Freeth, D., Fry, H., 2005. Nursing students’ and tutors’ percep-tions of learning and teaching in a clinical skill centre. NurseEducation Today 25, 272–282.
Gleichmann, S., Gleichmann, U., Mannebach, H., et al., 1989.Educating nurses in blood pressure and hypertension control.Journal of Hypertension 7 (Suppl. 3), S99–S102.
Grim, C.M., Grim, C.E., 1995. A curriculum for the training andcertification of blood pressure measurement for health careproviders. Canadian Journal of Cardiology 11 ( Suppl. H),38H–42H.
Hartigan-Rogers, J.A., Cobbett, S.L., Amirault, M.A., Muise-Davis, M.E., 2007. Nursing graduates’ perceptions of theirundergraduate clinical placement. International Journal ofNursing Education Scholarship 4 (1), 1–12.
Hogg, G., Pirie, E., Ker, J., 2006. The use of simulated learningto promote safe blood transfusion practice. Nurse Educationin Practice 6, 214–223.
Independent Advisory Group on Blood Pressure Monitoring inClinical Practice, 2005. Report of the Independent AdvisoryGroup on Blood Pressure Monitoring in Clinical Practice.Available from: <http://www.mhra.gov.uk>.
Jefferies, P.R., 2005. A framework for designing, implementingand evaluating simulations used as teaching strategies innursing. Nursing Education Perspectives 26 (2), 96–103.
Johnson, J.H., Johnson, J., Theis, S.L., 1999. Clinical simulationlaboratory: an adjunct to clinical teaching. Nurse Educator24 (5), 37–41.
Kemp, F., Foster, C., McKinlay, S., 1994. How effective istraining for blood pressure measurement? Professional Nurse9 (8), 521–522, 524.
Kennedy, S., Curzio, J., 1996. Blood pressure points. PracticeNurse 11 (1), 25–28.
Ker, J., Mole, L., Bradley, P., 2003. Early introduction tointerprofessional learning: a simulated ward environment.Medical Education 37, 248–255.
Kissinger, J.A., 1998. Overconfidence: a concept analysis.Nursing Forum 33, 18–19.
Knight, C., 1998. Evaluating a skills centre: the acquisition ofpsychomotor skills in nursing – a review of the literature.Nurse Education Today 18, 441–447.
Levett-Jones, T., Fahy, K., Parsons, K., Mitchell, A., 2006.Enhancing nursing students’ clinical placement experiences:a quality improvement project. Contemporary Nurse 23 (1),58–71.
McVicker, J., 2001. Blood pressure measurement – does anyonedo it right? An assessment of the reliability of equipment inuse and the measurement techniques of clinicians. Journal ofFamily Planning and Reproductive Health 27 (3), 163–164.
Manley, K., 1997. Knowledge for nursing practice. In: Perry, A.,Jolley, M. (Eds.), Nursing: A Knowledge Base for Practice,second ed. Arnold, London, pp. 301–333.
Markandu, N.D., Whitcher, F., Arnold, A., Carney, C., 2000.The mercury sphygmomanometer should be abandoned
A survey of first year student nurses’ experiences of learning blood pressure measurement 71
before it is proscribed. Journal of Human Hypertension 14(1), 31–36.
Medicines andHealthcareproductsRegulatoryAgency,2006.BloodPressure Measurement Devices. DH, London, DB2006(03).
Midgley, K., 2006. Pre-registration student nurses’ perception ofthe hospital-learning environment during clinical place-ments. Nurse Education Today 26 (4), 338–345.
Mole, L.J., McLafferty, I.H., 2004. Evaluating a simulated wardexercise for third year student nurses. Nurse Education inPractice 4, 91–99.
Morgan, R., 2002. Giving students the confidence to take part.Nursing Times 98 (36), 36–37.
Morgan, R., 2006. Using clinical skills laboratories to promotetheory–practice integration during first practice place-ments: an Irish perspective. Journal of Clinical Nursing 15(2), 155–161.
Nolan, J., Nolan, M., 1993. Can nurses take an accurate bloodpressure? British Journal of Nursing 2 (14), 724–729.
Nursing and Midwifery Council, 2004. Standards for Proficiencyfor Pre-registration Nursing Education. NMC, London.
Nursing and Midwifery Council, 2005. Proposals Arising From aReview of Fitness for Practice at the Point of Registration.NMC, London.
Nursing and Midwifery Council, 2006. Standards to SupportLearning and Assessment in Practice: NMC Standards forMentors, Practice Teachers and Teachers. NMC, London.
NMC., 2007a. Introduction of Essential Skills Clusters for Pre-registration Nursing Programmes. NMC circular 07/2007.
NMC., 2007b. SupportingDirect Care Through Simulated PracticeLearning in the Pre-registration Nursing Programme. NMCcircular 36/2007.
O’Brien, D., Davison, M., 1994. Blood pressure measurement:rational and ritual actions. British Journal of Nursing 3 (8),393–396.
O’Shea, E., 2003. Self-directed learning in nurse education: areviewof the literature. Journal ofAdvancedNursing43,62–70.
Pietz, L., 1994. Variations in teaching and practices of bloodpressure measurement. Nurse Educator 19 (5), 9–14.
Quinn, F., Hughes, S.J., 2007. Quinn’s Principles and Practice ofNurse Education, fifth ed. Nelson Thornes Ltd., Cheltenham.
Robertson, B., 2006. An obstetric simulation experience in anundergraduate nursing curriculum. Nurse Educator 31 (2),74–78.
Saarikoski, M., Leino-Kilpi, H., 2002. The clinical learningenvironment and supervision by staff nurses: developingthe instrument. International Journal of Nursing Studies 39,259–267.
Savage, E.B., 1999. The ward learning environment for studentnurses: a study to determine the influence of staff nurses.Part 2. Nursing Review 17 (3), 57–63.
Stewart, J., O’Halloran, C., Barton, J.R., Singleton, S.J.,Harrigan, P., Spencer, J., 2000. Clarifying the concepts ofconfidence and competence to produce appropriate self-evaluation measurement scales. Medical Education 34 (11),903–909.
Torrance, C., Serginson, E., 1996a. An observational study ofstudent nurses’ measurement of arterial blood pressure bysphygmomanometry and auscultation. Nurse EducationToday 16 (4), 282–286.
Torrance, C., Serginson, E., 1996b. Student nurses’ knowledgein relation to blood pressure measurement by sphygmoma-nometry and auscultation. Nurse Education Today 16 (6),397–402.
Weller, J., 2004. Simulation in undergraduate medical educa-tion: bridging the gap between theory and practice. MedicalEducation 38, 32–38.
Wilford, A., Doyle, T.J., 2006. Integrating simulation traininginto the nursing curriculum. British Journal of Nursing 15(11), 604–607.
Ziv, A., Small, S., Wolpe, P., 2000. Patient safety and simula-tion-based medical education. Medical Teacher 22 (5), 489–495.
Available online at www.sciencedirect.com





























