Embed Size (px)
Citation preview
A STUDY ON THE HEALTH STATUS OF ADOLESCENT
GIRLS RESIDING IN SOCIAL WELFARE HOSTELS OF
NELLORE CITY, A.P.
Dissertation submitted toDr. NTR UNIVERSITY OF HEALTH SCIENCES
VIJAYAWADA (A.P.)
In partial fulfillment of the requirement for the
DOCTOR OF MEDICINE
IN
COMMUNITY MEDICINE
To be held in April –May, 2010
By
Dr. K. MUNI SUSMITHA M.B;B.S.,
DEPARTMENT OF COMMUNITY MEDICINENARAYANA MEDICAL COLLEGE
NELLORE-524 002ANDHRA PRADESH
INDIA
2010
CERTIFICATE
THIS IS TO CERTIFY THAT THIS DISSERTATION TITLED
“A STUDY ON THE HEALTH STATUS OF ADOLESCENT
GIRLS RESIDING IN SOCIAL WELFARE HOSTELS OF
NELLORE CITY, A.P.”IS THE ORIGINAL INVESTIGATIVE
WORK DONE BY Dr. K. MUNISUSMITHA, M.B.B.S., UNDER MY
SUPERVISION AND GUIDANCE.
DR.N.ANANTHAIAH CHETTY, M.D.,PROFESSOR & H.O.D,DEPARMENT OF COMMUNITY MEDICINE,NARAYANA MEDICAL COLLEGE,
PLACE: NELLORE NELLORE. (A.P.)DATE: 24 .11.2009
PROFESSOR OF COMMUNITY MEDICINE,NARAYANA MEDICAL COLLEGE,
NELLORE, (A.P.)
Dr. N.T.R. UNIVERSITY OF HEALTH SCIENCESVIJAYAWADA (A.P.)
DECLARATION BY THE CANDIDATE
I, Dr. K. Muni Susmitha, hereby declare that, this dissertation titled
“A Study On The Health Status Of Adolescent Girls Residing In Social
Welfare Hostels Of Nellore City, A.P.” has been prepared by me is being
submitted to the Dr. N. T. R. University of Health Sciences, Vijayawada,
Andhra Pradesh in partial fulfillment of the regulations for the award of
degree of Doctor of Medicine (Community Medicine), examination to be
held in April 2010.
Date : 24.11.2009
Place: Nellore (Dr. K. Muni Susmitha)
3
I am greatly indebted to my respected Professor and Head of the
department, Dr.N.Ananthaiah Chetty for his valuable guidance in
shaping up this dissertation work.
I thank Dr.V.VenugopalReddy, Professor, department of
community medicine for his invaluable suggestions. I also thank
immensely Dr. G. Sreenath, former Professor and Head of the department
for his invaluable guidance.
I sincerely thank Dr.Abhay B.Mane and Dr.R.Rajkumar and
Dr.C.Kumar Associate Professors of the department for their valuable
help and guidance.
I express my deep sense of gratitude to Dr.E.Venkat Rao and Dr.
C.Jyothi Assistant professors of the department for helping me constantly
throughout the work.
I am extremely thankful to my colleague post graduates and other
staff members of the department for their moral support and help
whenever sought.
I sincerely thank the Hostel Welfare Officers of social welfare
hostels, Nellore, for the kind help extended. I also thank the other
4
members of social welfare hostels involved in the study for the help
extended.
Last but not the least; I am extremely thankful to the study subjects
enrolled in the study for their participation and cooperation in
successfully carrying out this study.
Dr. K. MUNISUSMITHA
5
LIST OF ABBREVIATIONS USED
ARI – Acute Respiratory Infections
BMI – Body Mass Index
Ht – Height
ICMR – Indian Council of Medical Research
ICRW - International Center for Research on Women
NCHS – National Centre for Health Statistics
NFHS – National Family and Health Survey
NHANES - National Health and Nutrition Examination Survey
NNMB – National Nutrition Monitoring Bureau
RCH – Reproductive and Child Health
STI/RTI – Sexual Transmitted / Reproductive Tract Infections
SC and ST – Scheduled Caste and Scheduled Tribes
UTI – Urinary Tract Infections
WHO – World Health Organization
Wt – Weight
6
CONTENTS
S.NO TITLE PAGE NO.
1) INTRODUCTION 01- 05
2) AIMS AND OBJECTIVES 06
3) REVIEW OF LITERATURE 07- 40
4) MATERIALS AND METHODS 41 - 47
5) RESULTS 48 - 73
6) DISCUSSION 74 - 85
7) SUMMARY & CONCLUSIONS 86- 87
8) RECOMMENDATIONS 88 -89
9) LIMITATIONS 90
10) BIBLIOGRAPHY 91 – 100
11) ANNEXURES
7
INTRODUCTION
INTRODUCTION
8
WHO defines adolescence as the segment of life between the ages of
10-19 years. Adolescence is a transition phase through which a child
becomes an adult. It is characterized by rapid growth and development;
physiologically, psychologically and socially.1
There are 1-2 billion adolescents in the world, 85% of them live in
developing countries.2 The adolescent population constitutes about 18-25%
of the total population of the South East Asia Region.1
About one-fifth of India’s population is in the adolescent age group of
10–19 years. Adolescents constitute a sizeable proportion of the Indian
mothers. However, despite adolescents being a huge segment of the
population, policies and programs in India have focused very little on the
adolescent group.
Adolescents constitute perhaps the healthiest group in the population,
having the lowest mortality and morbidity compared with other population
age groups. Adolescents are an “in between group”, with some nutrition
problem, some common with children and some with adults. In addition,
there are adolescent-specific issues that call for specific strategies and
interventions.1 However, the period of adolescence, beginning with the onset
of puberty, is a crucial to healthy transition into adulthood. Most adolescents
9
go through adolescence with little or no knowledge of the body’s impending
physical and physiological changes, health issues and problems. Early
marriages, high fertility rates, high rates of teenage pregnancy, high risk of
STI/RTI, and poor nutritional status are the main health problems among the
adolescent population in India.3
The newer focus on RCH also has been invigorated by the continuing
realization of the importance of women’s health; it is now widely accepted
that if the health of women is to be improved, the health of adolescents must
be given high priority in Indian policy and programme development and
implementation.3
Girls are deprived of nutrition, access to health care, and opportunities
for education and employment. They are taken out of schools when they
reach menarche. From the very beginning of life, girls are groomed to
accommodate the male-dominated, patriarchal society. Girl children grow
into adulthood without being able to experience the important period of
adolescence. Nearly 46.6 % of adolescent girls are illiterate when compared
with males (25.5 %).3
Anaemia is a widely prevalent health problem among adolescent girls.
Both the 1992 ICMR study on Iron and Folic Acid supplementation and
UNICEF have reported low mean hemoglobin levels and low nutritional
10
intake of proteins, calories, and macro/micronutrients among adolescent
girls and pregnant mothers. Poor physical growth and stunting are the
primary outcomes of poor nutrition. The 1998–99 NFHS-2 reported that the
prevalence of anaemia was highest (56 %) among adolescents (ages 15–19)
compared with other group of women of reproductive age.3
Adolescent health is the domain of the Ministry of Health and Family
Welfare at central level and the Department of Health and Family Welfare at
state level. The Ministry of Women and Child Development is significantly
involved in the issues of nutrition and development of children, particularly
girl children. The major thrust to adolescent health, however, was given in
the National Population Policy 2000. The National Youth Policy, 1986 (New
Draft National Youth Policy, 2000) placed adolescent health as a subsection
under the health sector.3
In Andhra Pradesh, this segment constitutes approximately 5.03% of
the population. The importance of this target group lies in the fact that they
are going to be the mothers of tomorrow – whose well being is critically
important for improving the nutritional, health and educational status of
women in the State. Various base line surveys also revealed that the health,
nutritional and educational status of adolescent girls are at sub-optimal
level.4
11
The scheduled castes and scheduled tribes have been identified as two
most disadvantaged groups of Indian society needing special attention.5
As per 2001 census, Scheduled Castes constitute about 16.2% and
Scheduled Tribes about 8.1% of the Indian population, and in Andhra
Pradesh they constitute about 16.2% and 6.6 % of population.6
The school age children from poor Scheduled Castes families are not
being sent to school because of the tendency of some parents to utilize the
services of their children at their tender age, in order to augment their family
income. A provision for educational opportunities forms a very important
part of the programme for the welfare of the SCs and the STs.
Empowerment of the Adolescent Girl is necessary to help her cope
with the changes and promote awareness of health, hygiene and nutrition so
as to break the intergenerational life cycle of nutritional and gender
disadvantage and provide an enabling and supporting environment for self
development.4
The main mission of the social welfare department is educational,
socio-economic development, welfare and protection of scheduled castes.
This department, with respect to the socioeconomic status of SC population
and socio academic profile of the scheduled caste children, has been
12
maintaining hostels as a pro-educational measure. These hostels serve as
homes away from homes at places where schooling facilities are available.
The girls stay more than 8 years in these hostels. Health care of the
girls in the hostels is of utmost importance because the children in the school
age (5-15years) are in a period of growth and development when optimum
nutritional and health care is essential. Good health and nutrition are
necessary for proper learning at school. Inculcation of healthful habits
among these adolescents will have permanent benefit in their lives and also
the ideas and practices will influence their families and communities. As
these girls have come out of their environment and are living in groups, they
face special risks and need extra care for the maintenance and improvement
of their health and nutrition.
The data regarding the nutritional status, morbidity status and sanitary
conditions of the social welfare hostels for the scheduled castes are sparse,
despite the usefulness of such information in the management of hostels and
upliftment of these groups.7
In this context, the present study was taken up among adolescent girls
residing in the social welfare hostels for scheduled castes in Nellore city.
This study focuses on health and nutritional status of adolescent girls and the
environmental conditions in the hostels.
13
AIMS AND
OBJECTIVES14
AIM
To study the health status of adolescent girls residing in social welfare
hostels of Nellore city, A.P.
OBJECTIVES
1. To assess the Nutritional status of the adolescent girls residing in the
hostel.
2. To study the Morbidity pattern among the adolescent girls in the
social welfare hostels for scheduled castes.
3. To describe the menstrual health problems of the adolescent girls in
the social welfare hostels.
4. To describe the environmental conditions of the hostels.
15
REVIEW OF LITERATURE
16
REVIEW OF LITERATURE
Adolescence definition
No longer children, not yet adults. Adolescence is a period of rapid
development when young people acquire new capacities and are faced with
many new situations.8
The World Health Organization defines adolescents as young people
aged 10-19 years.9
As they grow they feel a sense of independence, but depend on adults
for their material needs. And as they change, so do their needs change with
them.
Phases in adolescence
1. Early adolescence (10-13yrs): It is characterised by a spurt of
growth, and the beginning of sexual maturation. Young people start to
think abstractly.
2. Mid-adolescence(14-15yrs):The main physical changes are
completed, while the individual develops a stronger sense of identity,
and relates more strongly to his or her peer group, although families
usually remain important. Thinking becomes more reflective.
17
3. Late adolescence (16-19yrs): The body fills out and takes its adult
form, while the individual now has a distinct identity and have more
settled ideas and opinions.
Special characteristics
Over 80% of adolescent growth (attained weight and height) is
completed in early adolescence (10-15 years), with a marked deceleration in
weight and height velocity in the post-pubertal phase. This adolescent
growth spurt is also associated with cognitive, emotional and hormonal
changes.1
This phase of life cycle is marked by special characteristics which include
1. Rapid physical growth and development.
2. Physical, social and psychological maturity.
3. Sexual maturity and onset of sexual activity.
4. Beginning of menstruation in girls and onset of reproduction
cycle.
5. Experimentation.
6. Development of adult mental processes and adult identity.
7. Transition. 10
18
Numerical facts
There are about 1.2 billion adolescents, a fifth of the world’s
population and their number is increasing. Four out of five live in
developing countries.9
Adolescents constitute about 23% of population in India. In India,
girls constitute 5.1% of adolescents in 10 - 14 years age group and 4.8% in
15 – 19 years age group.1
Factors affecting health status of adolescents
The lives of millions of adolescents are marred by poverty,
inadequate education and work opportunities, exploitation, war, civil unrest
and ethnic and gender discrimination. Rapid urbanization,
telecommunication, travel and migration bring both new possibilities and
new risks to young people. These conditions may directly jeopardize health.8
Health problems of adolescents are interrelated. Many of the factors
that underlie unhealthy development in adolescents are decreasing influence
of family and culture, earlier puberty and late marriage - all these extend the
risks of unprotected sexual activity in unmarried adolescents in many parts
of the world. In some countries, early marriage and childbearing lead to high
maternal and infant mortality rates. In others, sexually transmitted diseases,
including HIV/AIDs, pose enormous health risks to adolescents.8
19
Potentially harmful substances - tobacco, alcohol and other drugs - are
now more readily available to adolescents and threaten their health in both
the short and long term. Violence inflicted by and on young people is a
growing phenomenon. Young men frequently take part in acts of violence,
including wars. Suicide attempts appear to be on the increase among the
young.8
Importance of Adolescent Health
Adolescent girl's health covers morbidity, mortality, nutritional status
and reproductive health and linked to these are environmental degradations,
violence and occupational hazards, all of which have implications for
adolescent girl health.3
Adolescent girl’s health plays an important role in determining the
health of future population, because adolescent girl’s health has an
intergenerational effect. The cumulative impact of the low health situation of
girls is reflected in the high MMR, the incidence of low birth weight babies,
high perinatal mortality and foetal wastage and consequent high fertility
rates.
20
A transitional period between childhood and adulthood, adolescence
provides an opportunity to prepare for a healthy productive and reproductive
life, and also to prevent the onset of nutrition related chronic diseases in
adult life, while addressing adolescence-specific nutrition issues and
possibly also correcting some nutritional problems originating in the past.11
Nutrition influences growth and development throughout infancy,
childhood and adolescence; it is, however, during the period of adolescence
that nutrient needs are the greatest.11
Nutritional and health needs of the adolescents are more because of
more requirements for growth spurt and increase in physical activity. They
need more of all nutrients particularly calcium, iron and iodine. The need for
more of iron in adolescents is due to growth spurt and the onset of
menstruation. Inadequate iron stored during adolescence and before
conception is a major cause of iron deficiency anaemia during pregnancy,
which aggravates the risk of pregnancy.12
Poor nutrition starts before birth, and generally continues into
adolescence and adult life and can span generations. Chronically
malnourished girls are more likely to remain undernourished during
21
adolescence and adulthood, and when pregnant, are more likely to deliver
low birth-weight babies.1
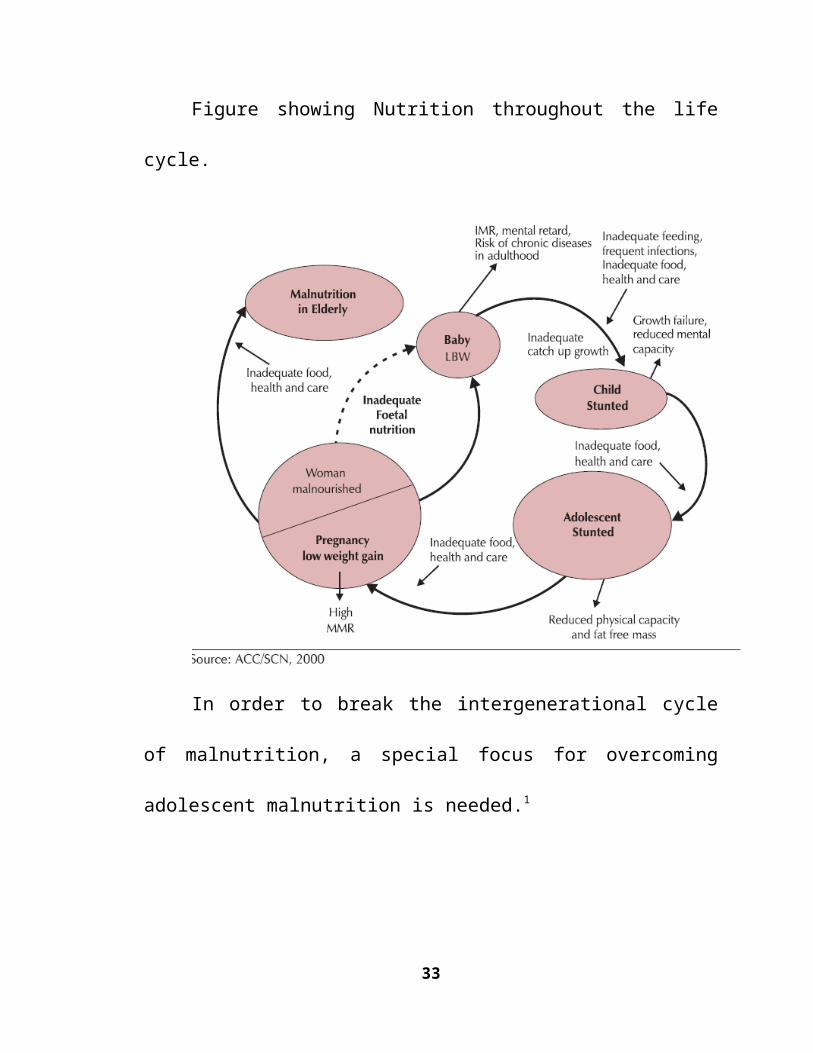
Figure showing Nutrition throughout the life cycle.
In order to break the intergenerational cycle of malnutrition, a special
focus for overcoming adolescent malnutrition is needed.1
22
Health Status of Adolescents
World
For a number of years, the health of adolescents has not been a major
concern and research has consequently been limited, as they are less
susceptible to disease and suffer from fewer life-threatening conditions than
children and elderly people. Indeed, adolescence is generally described as a
period of relatively good health with low prevalence of infection and chronic
disease. Mortality and morbidity trends among adolescents are quite similar
in developing and developed countries. It is noteworthy that health services
in developing countries focus on preschool-age children and pregnant
women, with the consequence that health needs of adolescents may not be
adequately met.11
A general profile of adolescent girl’s nutritional status was sketched in
the South-East Asia Region: “They are undernourished, indicating a chronic
energy deficiency. Most often, the BMI of adolescent girls of 13years and
above is below 18.5. The girls are usually physically stunted, a manifestation
of chronic protein energy malnutrition. Iron deficiency anaemia is the most
glaring nutritional deficiency, with not less than 25-40% of adolescent girls
as victims of moderate and sometimes severe anaemia. In all countries of the
region, at least 40-50% of adolescent pregnant girls are anaemic”.
23
Under nutrition was highly prevalent in three of the 11 studies of
ICRW: 53% in India, 36% in Nepal.11
India
The health of adolescent girl is intricately related to the socio-
economic status of the households to which they belong and their age and
kinship status within the households. India has traditionally been a male
dominated society; so there is a strong son preference in most parts of India,
and girls tend to be discriminated by their families. It is not enough,
therefore, to highlight adolescence in general; a larger focus of the girl child
also must be addressed. Demographic trends indicate deep-rooted gender
discrimination which begins with female feticide and prenatal sex
determination.3
Given the predominantly patriarchal setup, girls get a lesser share in
the household distribution of health, goods and services compared to men
and boys. There is data to show that in a situation of extreme food and
scarcity, the adverse effect on the nutritional status is greater on girls than on
boys. Girls in the 13 to 16 years of age group consume less food than boys.
However, in the intra-household distribution of labour, adolescent girls get
the major share of economic, procreative and family responsibilities. Due to
the competing demands on their time and energy as well as their
24
socialization, girls tend to neglect their health. The lesser access to food
coupled with neglect invariably leads to a poor nutritional status and a state
of ill health for most of the adolescent girls' health.13
As malnutrition among the child population in the country is widely
prevalent, it follows that a moderate to severe degree of malnutrition would
persist among girl child too. As a consequence, the malnutrition persists
throughout adolescence and in pregnancy. As a result, the growth and
development of unborn child is affected, giving rise to low birth weight.
About 30 % of the total births in the country constitute low birth weight and
this in turn leads to high infant and child mortality and morbidity. According
to the NNMB data (National Nutrition Monitoring Bureau), a very high
proportion of girls are at obstetric risk as they enter the 14th -15th year of life
with a height less than 145 cm and weight less than 38 Kg.13 However, not
much attention has been paid to adolescents by nutrition-related programmes
in developing countries.1
In order to break the intergenerational transfer of anaemia and cycle
of malnutrition, anaemia control will find a high place in the action plan for
the Adolescent Girls year.1 Women Development & Child Welfare
Department declared the year 2003 as the “Year of the Adolescent Girl.”4
25
The collaborative study done in Hyderabad, New Delhi, Calcutta and
Madras showed that amongst girls between 6-14 years of age, the prevalence
of anaemia was 63.8%, 65.7%, and 98.7% respectively. A study in rural area
showed that 65.5% parents of adolescent girls never spoke about the
physical changes during puberty, like menarche, with their daughters.13
Special problems of adolescent girls
Unfortunately, the special needs of adolescents are rarely addressed
by the educational, health, and family welfare programs in India. The
commitment of the national government to the reproductive health approach
forged at the International Conference on Population and Development
(ICPD) in 1994 has reshaped the family welfare program into a broad-based
Reproductive and Child Health (RCH) Services Program in India.
Policymakers and planners have now realized that the adolescent population
group has specific health and developmental needs. There is a growing
understanding that adolescence is a bridge between childhood and
adulthood.3
The 1998–99 National Family Health Survey-2 (NFHS-2) reported
that among young female adolescents (ages 10–14 years), 67 % attended
school. The corresponding figure for male adolescents was 80.2 %. Location
26
had a significant influence on the schooling of females. In rural areas, only
32.7% of female adolescents (ages 15–17) attended school compared with
60.5% of female adolescents in urban areas. More than one-quarter of girls’
lack of education was ascribed to their responsibilities for caring for siblings
at home and other household responsibilities.3
A large proportion of adolescent girls suffer from various
gynecological problems, particularly menstrual irregularities such as
menorrhagia, polymenorrhea, oligomenorrhea, and dysmenorrhea. As many
as 40–45% of adolescent girls report menstrual problems. These are mainly
due to psychosocial stress and emotional changes.3
Indian culture promotes universal marriage. Of importance to
Adolescent Reproductive Health is the traditional young marriage age of
girls - referred to as early marriage. The national average age at marriage for
women in India is 16.4 years, although there are vast regional variations.3
NFHS-2 reports that in states like Rajasthan, Bihar, Uttar Pradesh,
Madhya Pradesh, and Andhra Pradesh, girls are married at around age of
15years. According to NFHS-2, about one-third of women were married by
age 15 and two-thirds (64.6 percent) by age 18.3
27
Teenage pregnancy is the major cause of poor reproductive health and
health outcomes among adolescents. About 15 % of pregnancies are among
teenage girls under age 18 and they have a 2-5 times higher risk of maternal
death. Adolescent pregnant mothers, who are often already poorly nourished
before becoming pregnant, run a high obstetric risk for premature delivery,
giving birth to a low birth weight baby, prolonged and obstructed labour,
and severe intrapartum and postpartum hemorrhage. 3
Programmes and Schemes for adolescent girls implemented by
Government of India
Important relevant policies and plans that have been developed in
India over the past 25 years include, RCH Services Program, Integrated
Child Development Services (ICDS) Scheme, Adolescent Girl Scheme,
State Plans of Action for the Girl Child, District Primary Education
Program, Balika Samriddhi Yojana, 1997, National Plan of Action for the
SAARC Decade of the Girl Child (1991–2000), International Center for
Research on Women (ICRW)3, The Children’s Code Bill, 2000,National
Health Policy, 1983,National Nutrition Policy, 1993, The National Youth
Policy, 1986 (New Draft NationalYouth Policy, 2000) placed adolescent
28
health as a subsection under the health sector. Youth empowerment and
gender justice were recognized as the major thrust areas of the policy.3.
Apart from various policies, several legislative provisions have also
been introduced that directly or indirectly protect the rights of adolescents.
Besides constitutional provisions, some other legislative acts have been
promulgated to safeguard the health and social protection of children, such
as the Immoral Traffic (Prevention) Act, 1956; the Child Marriage Restraint
Act, 1976; the Juvenile Justice Act, 1986; and the Child Labour (Prohibition
and Regulation) Act, 1986. More recently, the Prenatal Diagnostic
Techniques (Regulation and Prevention of Misuse) Act of 1994 has been
promulgated to prevent selective female feticide.3
In view of the above it is felt necessary to bring in greater synergy
between the resources and programmes of all agencies both Governmental
as well as Non-Governmental, achieve a higher degree of convergence with
other programmes of similar nature in the education, rural development and
health sectors and evolve a strategy for the growth and development of the
Adolescent Girls so that they can be productive and useful members of
society. While there are inter-state and inter-regional variations in the status
of the Adolescent girls, one common threat faced by the Adolescent girls is
29
the low levels of iron and folic acid, leading to nutritional anaemia and low
health status.4
Overview of Education in India and the Extent of Social exclusion in
Scheduled Caste Children
“Social exclusion reflects the multiple and overlapping nature of the
disadvantages experienced by certain groups and categories of the
population, with social identity as the central axis of their exclusion.”
Constitutional amendment recognizes education as a fundamental right of all
Indian citizens. Even after 60 years of independence disparities continue to
be pronounced between the various castes.14
People from the Scheduled Castes, previously referred to as the
“untouchables”, make up 16% of the population and consistently fare poorer
across various indicators related to primary education. Development
approaches from the 1950s to the 1980s primarily focused on social and
economic development as an outcome of the development process and were
less concerned with civil and political rights. In contrast, the human rights
based approach to development recognizes both the achievement of a
desirable outcome and the establishment of an adequate process to achieve
and sustain that outcome.14
30
A rights perspective is based on principles that emphasize
accountability of those with obligations to realize the rights of children. The
state and the other ‘duty-bearers’ (eg. parents and teachers) have obligations
to fulfill these rights. As rights-holders, children are entitled to demand that
the duty-bearers meet their respective obligation to respect, protect and
fulfill their rights.14
This global shift in development towards a human rights perspective
has important implications for addressing social exclusion in education as it
encourages one to take a broader, systemic and more holistic view of the
issue. Poverty is not merely a lack of income but rather a condition of living
in various forms of deprivation, social exclusion is not only a development
issue, but is also a human rights issue and therefore requires a more
comprehensive and process-oriented response.
As per the Census 2001, the total population of the Scheduled Castes
(SC) in India is 166,635,700, which is 16.3% of the total population
(Registrar General, 2005).14
The population of SCs is unevenly distributed among the states in
India, with nearly 60% of all SC children of primary school-going age (6-10
years) residing in the following six states: Andhra Pradesh, Bihar, Madhya
Pradesh, Orissa, Rajasthan and Uttar Pradesh. The latter five states are
31
among the most disadvantaged states in India across most social indicators.
15 In an average for India, 27.09% of the population live below the poverty
line in rural areas, compared to 36.25% of the SC population and 23.62% in
urban areas compared to 38.47% of the SC population. These provisions
need to be fully utilised for the benefit of these weaker sections in our
society.14
However, the gap between upper and lower castes children with
respect to completion of primary education is still persisting due to various
socio economic factors. Scheduled caste (SC) children remain disadvantaged
across many social indicators. Estimates from the National Family Health
Survey III (2005-06) suggest that 28 % of the SC population belong to
lowest wealth quintile households. The disadvantaged children have suffered
from multiple forms of disadvantages, example being SC, girls, poor, living
in a poor and/or remote location, etc. Just 21% of SC children have
completed primary education compared to 70% of children belonging to
other castes.15
Only 65.7% of SC children of age 7-17 are currently attending school
compared to 81.3% of higher caste groups. Furthermore, 20.8% of SC
children never attended school compared to 7.6% of children from high
caste.14
32
Evolution of social welfare services
With the attainment of freedom in 1947 and adoption of constitution
in 1950, India became a welfare state. The constitution makers drew up a
preamble which states specifically, that state shall secure for all citizens,
justice, social, economic and political, liberty of thought and expression,
faith and worship, equality of status and opportunity. The fundamental
principles of state policy in the Indian constitution became the basis of social
services / welfare programmes.
The Central Social Welfare Board came into existence in 1953 with a
main purpose of assisting voluntary organizations with requisite grants. The
Department of Social Welfare was setup for first time in 1966. In pursuit of
the goal, the government distinguished between the social service needs of
the general population and the special needs of the large groups who have
traditionally suffered social disabilities such as SCs and STs. The central
Government therefore appointed a special commissioner for SCs and STs. It
has also created organizational infrastructure for the welfare of the SCs and
33
STs in the ministry of home affairs. A commission for SCs and STs was also
set up. 7
There has been a significant increase in overall literacy rates and
school participation rates across the country since the early 1990s. Gender
and social disparities have also declined with an overall increase in school
attendance. The country is approaching near universalisation of enrolment at
the primary stage.
A number of factors have contributed to the rising enrollment rate
including the introduction of mid-day meals, opening of alternate schools,
promoting the participation of Parent Teacher Associations (PTAs) and
massive enrolment drives.
Special provisions: After independence, the Government of India has
taken number of steps to strengthen the educational base of the persons
belonging to the Scheduled Castes and Scheduled Tribes. Pursuant to the
National Policy on Education (1986) and the Programme of Action (POA)-
1992, the following special provisions for SCs and STs have been
incorporated in the existing schemes of the Departments of Elementary
Education and Literacy and Secondary and Higher Education.
34
Sarva Shiksha Abhiyan (SSA): Is a historic stride towards achieving
the long cherished goal of Universalisation of Elementary Education (UEE).
SSA aims to provide useful and quality elementary education to all children
in the 6-14 age groups by 2010.16 Some of the main features of the
programme are:
Focus on girls, especially belonging to SC/ST communities and
minority groups.
Back to school campus for out of school girls.
Free textbooks for girls.16
District Primary Education Programme (DPEP) –
The thrust of the scheme is on disadvantaged groups like girls,
SCs/STs, working children, urban deprived children, disabled children, etc.
There are specific strategies for girls and SCs/STs; as well. According to a
study conducted in schools of DPEP districts, more than 60% students
belonged to SC/ST communities.16
Administration of social welfare hostels in Andhrapradesh
35
In Andhrapradesh, the welfare programmes for the Scheduled Castes
are looked after by the Education and Social welfare department. On the
executive side, there is a Director of social welfare who is ex-officio Deputy
Secretary to the department of education and social welfare. At the district
level a Deputy Director of social welfare will implement the programmes for
the SCs including the hostels. The District Collector as the administrative
head of the district looks after the welfare programmes. Assistant social
welfare officer will look after the management of the hostels in his region.
One hostel welfare officer (warden) and one care taker will look after the
needs of the children in each hostel. Composition of children in social
welfare hostels is as follows
Scheduled castes - 70%
Christians converted from SC - 12%
Backward classes - 9%
Scheduled tribes - 5%
Others - 4%
At present there are 2210 hostels (Boys 1677 and Girls 533) in the
state with sanctioned strength of 2.46 lakhs at the rate of 100 per each
hostel.17
36
The aim of these hostels is to give the triple dimension of the teacher,
the taught and the parent (Wardens, Matrons in place of the parents) and to
promote and level up the SC children’s education on par with other castes.18
Hostel Facilities for SC Students
The hostels function for 10 1/2 months and even further in the
summer for implementing various educational schemes.
There is uniform time schedule for all these hostels for the day to day
programme of academic and other routine of the boarders.
Also, there is uniform menu for all the hostels at the rate of Rs. 270/-
per month for the classes I to VII and Rs. 330/- per month per boarder
for the classes VIII to X.
The boarders are also provided with facilities like soaps, hair oil, text
books, note books, bedding material, trunk boxes plates and glasses
etc. free of cost. Cosmetic charges are enhanced from Rs. 10/-per
month to Rs. 20/- per month for boys and from Rs. 12/- and Rs. 17/-
per month to Rs. 25/-per month for girls.
Necessary provision is also made towards purchase of medicines to
the boarders in the Government hostels. Individual Health cards (HAI
37
cards) to each boarder have been introduced to facilitate the visiting
medical officer to record his findings in respect of sick boarders for
taking up necessary follow up action (Department of social welfare,
Hyderabad, 2000).
There are 79 Ananda Nilayams functioning to accommodate the
children of those engaged in unclean occupation and orphan children
in the ratio of 50:50. These institutions run on par with hostels and are
being run in summer vacation also.18
Review of studies on Adolescent Health
Health Status:
In a study conducted in social welfare hostels of Tirupati town
on 598 children aged 6-17 years, the common morbid conditions found were
skin disorders 25.7%,dental caries 21.5%, history of passing worms in stool
21.6% , vitamin B deficiency3.2% ,ARI 1.7% and diarrhea 1.2%. The
prevalence of anaemia and helminthiasis was found to be 79.6% and 39.3%
respectively. In the follow up study, the major health problems reported
were ARI, skin disease, injuries, vitamin .B complex deficiency, diarrhoea
and eye diseases.7
38
In a study conducted in slums of Lucknow on 400 adolescent girls
aged 10-19 years. 233 (58.2%) girls had attained menarche and the mean age
at menarche was 13.3 years. The mean height and mean weight in all age
groups was less than ICMR standards. The mean hemoglobin was 10 gm%.
Deficiency signs of vitamins were found in 28.7%; 22.2% showed Iron
deficiency signs and 3% had signs of vitamin A deficiency. The various
morbid conditions found among girls were inadequate oral hygiene (55.4%),
pediculosis (39.2%), cold & cough (25.8%), lymphadenopathy (22.2%),
scabies (16.2%), inflamed tonsils (7.8%) and ear discharge (7%).19
In a study on Health Status of School Children in Ludhiana City 776
students of both sexes (462 boys and 314 girls), in the age group 5-16 years,
from a secondary school in Ludhiana were examined. The health and
nutritional standards of the school children were found to be low, more so in
girls than in boys. The extent of malnutrition in this group was high, with the
children in nearly all ages, both boys and girls, being deficient in both
weight and height as compared to the ICMR standards. The prevalence of
wasting and stunting in these children was high (52.2% wasted and 26.3%
stunted) with boys and girls suffering almost equally. The prevalence of
anaemia was high in both sexes of adolescents, though significantly more so
39
in girls (30.5%) than in boys (22.9%). Malnutrition and anaemia make the
adolescents more susceptible to infection.20
In a Study of Health Problems of Adolescents in Urban Field Practice
Area of Nagpur, in the 10-20 years age group, 700 adolescents were studied.
Age of menarche in females ranged from 10 - 17 years, with majority having
attained it at the age of 13years. Menstrual problems, including
oligomenorrhoea were present in 30% adolescents. 439 (62.71%)
adolescents were suffering from acute nasopharyngitis / acute tonsillitis and
401 (57.28%) from anaemia. 379 (54.14%) were having acne, 259 (37.0%)
were having dental caries, 240 (34.28%) were having nicotine stains on
teeth. 184 (26.28%) adolescents were having signs of vitamin B complex
deficiency, 136 (19.42%) had history of passing worms in stools, 45 (6.43%)
adolescents had scabies, 52 (7.43%) pediculosis, 25 (3.57%) obesity and 2
(0.28%) were known cases of congenital heart diseases (CHD). Out of 700
adolescents, 401 (57.28%) were anaemic, with 117 (16.71%) having
moderate and 284 (40.57%) having mild anaemia. Higher prevalence of
anaemia was seen in female adolescents 219 (60.16%) as compared to male
adolescents182 (54.16%). The percentage of morbid conditions were higher
in joint families (82.42%) as compared to nuclear families (61.08%), due to
overcrowding and poor sanitation.21
40
In a study in rural Tamil Nadu, the prevalence of cold and headache
was 16.62 % and 10.23% respectively. About 7.67% of the girls surveyed
had non-specific fever and another 8% had digestive problems. 12% of the
girls reported body pains and backache. The prevalence of general morbidity
increased with age and it was high among illiterate than literates. 46% had
reproductive morbidity, 5% had general illness and 37 % had both general
and reproductive illness.22
In a study conducted in Mumbai among 1,144 girls of 5-15 years age,
630 of primary section and 514 of secondary section of affluent population,
the commonest health problems noted in these girls were related to hygiene
(62.2%). While dental caries and helminthiasis were commoner in younger
girls, pediculosis was most frequently seen in older girls of secondary
section. Nutritional disorders were present in 29.0%.Other important health
problems included asthma (6.6%), hypertension (2.2%), otitis media (2.0%),
splenomegaly (1.6%), ocular infections (1.5%), cervical lymphadenopathy
(1.1 %), tuberculosis (0.8%), cardiac disease (0.5%), deafness (0.4%),
epilepsy (0.4%) and UTI (0.4%). Among the six cardiac lesions, two were
rheumatic in origin.23
In a study done in the Kaniyambadi Block of North Arcot District of
Tamil Nadu, a total of 190 adolescents were studied. The five leading
41
general complaints were general fatigue, palpitations, frequent headaches,
backaches and abdominal pain (not related to menstruation). Over 20%
seemed to suffer from joint pains, weight loss, poor appetite and recurrent
respiratory problems. Sleep disturbances, loss of weight, frequent headaches
and dermatological problems were more common among those who had
attained menarche. Heights of adolescent girls varied from 140 to 151 cm
and weights from 31 to 43 kg. Pubertal spurts were seen between 13 to 14
years. The heights and weights were less than the 5th percentile of National
center for Health statistics. The body mass index varied from 16 to 19 and
generally depicts an undernourished population. One hundred and twenty
four of the girls had attained menarche, the mean age being 13.9 years.24
In a study conducted in Pondicherry, the morbidity of 5,602
adolescents aged 10-19 years was studied; diseases of the eye, ear, nose,
throat and skin, and upper respiratory infections were found in 70%. Injuries
seem to be the next important cause of morbidity amongst adolescents.
Dysentery seems to occupy a less important place in the morbidity figures of
adolescents in comparison with that of infants and children. Accidents seem
to be the leading cause of death amongst the adolescent population of all
countries. Malignant neoplasms, including neoplasms of tissues seems to be
42
the second most important cause of death amongst the adolescent population
of the developed countries.25
In a clinical survey of 916 school children in a rural area in Western
Orissa for B.C.G. immunization coverage; coverage was found as 69.5 per
cent. Anthropometric measurements revealed that the height of these
children was more than the ICMR standard while weight was lower than the
ICMR standard. Chest circumference was more or less similar to the ICMR
standard. Common causes of morbidity were vitamin B complex deficiency
(42.9%), vitamin A deficiency (28.6%), anaemia (25.7%), upper respiratory
tract infections (22.1%), gastro-intestinal tract disorders (8.7%), scabies
(16%) and dental diseases (8.5%).26
A cross sectional study was undertaken on 640 Relli boys and 671
Relli girls aged between 10 to 18 years in urban schools situated in
Visakhapatnam The study revealed that Relli girls attained maximum mean
annual increase between 10 and 12 years and boys between 14 and 16 years.
The Relli boys and girls were taller and heavier than ICMR (1984) National
standards.27
In a cross-sectional study conducted in Boileaugang, Shimla during
June 2002 to January 2003 among 870 adolescents of age 10-19 years (480
males and 390 females), anaemia was diagnosed clinically in 62 (12.9%)
43
males and 52 (13.3%) females with an overall prevalence of 13.1%. 48
(77.4%) anaemic males and 33 (63.5%) anaemic females had poor personal
hygiene. Among females, 44 (84.6%) anaemic subjects had history of worm
infestation as compared to 147(43.8%) non-anaemic females (p<0.001). It
was also seen that, 30 (53.6%) anaemic females had menstrual problems like
menorrhagia, polymenorrhea, or irregular menstrual cycle as compared to 22
(6.6%) non-anaemic females. Prevalence of anaemia was 14.9% (15.5% in
males and 14.3% in females).28
Nutritional Status
In a cross sectional study carried out in tea gardens of Dibrugarh
district of Assam, in 605 adolescents aged 10-18years, the prevalence of
thinness in boys was 59.49% and in girls 41.32%. Mean BMI values of both
boys and girls were far below the NCHS median. Over weight was present
in 0.33%.29
In a study conducted in two PHC areas of Wardha district in
adolescents, 53.8% were thin, 44% were normal, and 2.2% were over
weight. The mean BMI for boys and girls was 16.88kg/m² and 15.44 kg/m²
respectively.30
44
In a study conducted by NNMB (1996-97) in 120 villages from each
state, overall prevalence of stunting (< median height-2 SD) was similar in
both the sexes, boys: 39.5% and girls: 39.1%. Under nutrition (< median-
2SD of NCHS weight for age) in males was more (53.1%) as compared to
females (39.5%) in case of body weight. The mean daily intake of different
foods according to sex were almost similar in both the sexes. The percentage
of under nutrition was less in adolescents belonging to extended families
(40.7%) as compared to joint families (48.6%).31
In a study conducted in adolescent rural girls of Varanasi, two-third of
study subjects were undernourished (BMI < 18.5 kg/m2), nearly one-third
had chronic energy deficiency grade-III (BMI<16 kg/m2).53.33%
adolescent girls had normal built. Vitamin A, B, C and D deficiencies were
present in 13.70%, 4.07%, 15.92% and 10% study subjects respectively.
Bitot’s spots were seen in 3.33% subjects and 25.90%, 13.33% and 4.44 %
girls had anaemia, dental caries and Iodine Deficiency Disorders (IDDs)
respectively. Nearly one-third girls were anaemic (Hb < 12 g/dl). Anaemia
was significantly more in non-menstruating girls and subjects not using
footwear during defecation.32
In a community-based survey carried out by NNMB (2000) on rural
males and females, up to 22 years of age from eight states, showed the
45
prevalence of Bitot’s spot in females (12-21 years) declined from 1.8 to
1.3%. The prevalence of goitre reduced from 5.8% to 3.0% during 1998-99
when compared to 1985-87 surveys in respect of all states, as revealed by
the pooled data. Overall dietary intake of iron had declined in all age groups
(1-3, 4-6, 7-9, 10-12 and 13-15 years) as per 1998-99 surveys when
compared with 1985-87 surveys.33
In a Study of growth parameters and prevalence of overweight and
obesity in school children from Delhi, total of 21,485 children in the age
group 5 to 18 years were evaluated for height, weight and BMI. The
prevalence of overweight and obesity among the lower socio economic
status school girls was 2.14% and 0.28% as compared to 19.01% and 5.73%
respectively among girls from upper socio economic status. There is a
significant disparity in anthropometric parameters of children belonging to
the upper and lower socioeconomic strata, with upper socio economic status
children being significantly taller and heavier.34
In a study conducted in adolescent girls between 10 and 15 years of
age, studying in 6th to 10th standards in 16 high schools located in two
randomly selected Mandals of Medak district, signs and symptoms of
anaemia like pallor (eyes, tongue nails), fatigue, breathlessness, poor
appetite and lack of concentration in studies were reported by 12.5%, 14.1%,
46
9.2%, 26.5% and 86% of girls respectively. Iron deficiency anaemia was
found in 81% of respondents. Mild, moderate and severe grades of anaemia
were observed in 63.2%, 12.5% and 5.3% of respondents respectively. The
heights and weights of study subjects at any given point of age were far
below the NCHS standards. Haemoglobin level improved in 45.6% while it
remained static in 49.4 % and declined in only 5 % of subjects.35
In a study among 504 adolescent Girls in rural Areas of District
Meerut (UP), 174 (34.5%) adolescent girls were anaemic. The prevalence of
mild, moderate and severe anaemia among adolescent girls was 19%, 14.1%
and 1.4%, respectively. The proportion of mild, moderate and severe
anaemia was 55.2%, 40.8% and 4.0% respectively. The significant
association of anaemia with socio-economic status, type of family, father’s
occupation, mother’s education and family size stressed the need to develop
strategies for intensive adult education, nutrition education and dietary
supplementation, including anaemia prophylaxis.36
In a study conducted in orphanages located in Udaipur city, the
average amount of cereals consumed by the boys of different age group was
76.2% - 91.5% of the requirements, whereas intake of pulses was only 30%
of the suggested quantities. The leafy vegetables were rarely supplied to the
children but intake of other vegetables was more than the recommended.
47
Intake of fats and oils was observed to be 30-45% less than what it is
suggested. The milk intake by children was insufficient. Food items like
fruits, meat, fish and eggs were never included in the diet provided in the
orphanages. All the children received significantly less than the
recommended intake of iron.37
Indian Council of Medical Research (ICMR) had undertaken a
multicentre, Community-based study “District Nutrition Project” in 18
districts from 13 states of the country including rural and urban children
(< 12 years), adolescent girls (11-18 years) and pregnant women. Prevalence
of anaemia among 4,332 non-pregnant adolescent girls from 16 districts was
90.1%. The range was 58.2 % to 100% .Average prevalence of anaemia in
the eight districts of northern India was 89.4 % and in the six districts of
eastern (including north-east) India, it was 91.7%. Mild and moderate
anaemia is more prevalent than severe anaemia.38
In a study carried out among 1295 girls of school going age (6-18
years) residing in 15 randomly selected slums of the north Ahmedabad city,
81.8% of girls were anaemic, out of which 55.2 % were mildly anaemic,
0.6% severely anaemic and the rest were moderately anaemic No significant
relationship of anaemia was observed with socio-economic class, knowledge
about anaemia, and parent’s education, status of menstruation and daily
48
consumption of lemon/ sour fruits. Anaemia was found to be significantly
higher among girls with a habit of post meal consumption of tea / coffee
(94.4%), whose fathers were working as semi-skilled/skilled workers (77%),
those having a BMI of 18.5 or lower (82.4%), as compared to those with
BMI more than 18.5(79.7%). The prevalence of anaemia was significantly
lower in girls consuming green leafy vegetables.39
In the study conducted by ICRW on the Nutrition of Adolescent Girls
in five developing countries including India, which was done in Bombay
urban slums in 69 Males and 69 Females of 10-19 years, 55% were anaemic,
32% were stunted and 53% were under nourished.40
In a study conducted in a rural area of West Bengal, in 143 adolescent
girls of 10-19 years, prevalence of thinness was 14.7%, 37.8% were stunted,
44.8% were anaemic, dental caries in 25.9% and 15.4% with angular
stomatitis, goiter in 1.4%. The prevalence of stunting was significantly
higher among the late adolescent age group than in early adolescent age
group.41
In a study conducted in 360 school going adolescent girls of 13-18
years age group of Raipur city, the prevalence of anaemia was 82%. The
subjects of the experimental group were provided with different types of
supplementation. The study revealed that role of Iron and Folic acid twice a
49
week supplementation is important in improving the level of anaemic
adolescent girls.42
In a study conducted in 454 girls, of 11-18 years age group in Delhi, it
was observed that 35.5% were under nourished, 3.1% were obese. Anaemia
was found in 56% and dental caries in 23.3%.43
50
MATERIAL AND
METHODS
51
Municipal Corporation Map of Nellore Showing Social Welfare Hostels
52
MATERIAL AND METHODS
Description of the study area
Nellore District is one of the 23 districts of Andhra Pradesh. Nellore is
famous for high paddy field, and so it got its name from the word (paddy)
"nelli".44 The population of the district was 2,668,564 of which 22.45% were
urban as of 2001. Nellore city is its administrative headquarters. The major
cities in the district are Nellore, Kavali and Gudur.
The study was conducted in five social welfare hostels and Ananda
Nilayam located near Madras bus stand within a radius of half a kilometer.
All the hostels except one are housed in Government buildings. Three
hostels are located in a single building but having kitchen and storage room
in separate blocks in the same compound. The other two girl’s hostels are
located as separate unit. The staffing pattern of hostel consists of one
warden, one care taker and three kitchen staff in addition to one sweeper and
one watchman.
The girls in the hostels are attending three primary schools, one high
school and three colleges in the neighbourhood. The medical officer of the
school health clinic provides medical checkup and treatment for children
53
once in a month. Those requiring specialist treatments will be referred to
district hospital. There is a provision for reimbursement of the amount
incurred for the purchase of medical aids like spectacles prescribed by the
specialist for the children.
Study setting: Social welfare hostels for scheduled caste girls in
Nellore city.
Study design: Descriptive cross sectional study.
Study period: June 2008 –May 2009.
Study population: All the girls aged between 11-19 years residing in
the social welfare hostels of Nellore city.
Inclusion criteria: 1.All adolescent girls aged 11-19 years.
2. A minimum of not less than one year stay in the
hostel.
Exclusion criteria: Absentees and drop outs of the subjects from the hostel
during the period of survey.
Sample size: 562 adolescent girls were registered at the time of study in
social welfare hostels out of which 542 are recruited in this study.
54
Study instruments: Pre-designed, pre-tested, semi-structured questionnaire,
stethoscope, sphygmomanometer, Snellen chart, Weighing machine,
stadiometer etc.
Study methodology: The study was conducted among adolescent girls
residing in six social welfare hostels for scheduled caste students in Nellore.
Among these six hostels four are for school children, one is Anandanilayam
(orphanage) and one for college girls. Written permission was obtained from
the Deputy Director of social welfare hostels of Nellore district. The study
was conducted with the co-operation of the hostel welfare officers.
Morbidity Status
Data regarding morbidity status was collected using a pre-designed,
pre- tested proforma (Annexure-1).Every girl was examined physically from
head to toe and deviations from normal were recorded. Enquiry was made
about the education and occupation of the parents, duration of stay in the
hostel, practices regarding personal hygiene, menstrual history, menstrual
hygiene and occurrence of any ailment during previous two weeks.
55
Nutritional Status
Nutritional status of girls was assessed by:
Anthropometric measurements viz height, weight, BMI.
Biochemical markers viz haemoglobin estimation.
Diet survey.
Anthropometry45
Height- Stadiometer (measuring rod) capable of measuring to an
accuracy of 0.1 cm was used to assess height of the subjects. The subject
was made to stand without foot wear with the feet parallel and with heels,
buttocks, shoulders, and occiput touching the measuring rod, hands hanging
by the sides. The head was held comfortably upright with the top the head
making firm contact with the horizontal head piece.
Weight- A portable weighing machine with an accuracy of 100gms
was used to record the weight of the girls. Checking the scale with a known
weight was done frequently and adjustment to zero was done every time for
accurate reading. Girls were instructed to stand on the weighing machine
with light clothing and without footwear and with feet apart and looking
straight and weight was recorded to the nearest value.
56
Body Mass Index (BMI) – BMI was calculated using the formula
Weight in kg/height in m²
The subjects were categorized into four groups based on BMI according to
WHO Asian Pacific46 standards as
<18.5 kg/m2 - Chronic energy deficiency or under weight
18.5-22.99 kg/m2 - Normal
23 – 24.99 kg/m2 - Over weight
> 25 kg/m2 - Obese
Thinness- WHO defines thinness in adolescents as BMI below the 5th
centile for age.47 In this study, 5th percentile of NCHS standards of BMI for
age were considered as thin.
Wasting - Height for age less than 3rd percentile of NCHS/WHO standards.48
In this study, 5th percentile of NCHS standards of height for age were
considered as stunted or wasted.
Diet survey – A diet survey as a part of nutritional assessment was
conducted by weighment of raw foods. This method is widely employed, as
it is practicable, fairly accurate and specially suited to institutions. Diet
survey was carried out for one dietary cycle of seven days in two hostels
randomly. Weighment of raw foods was done three times in a day (6.00AM,
10.00AM and 4.30 PM) preceding breakfast, lunch and dinner. The weights
57
of bulk items like rice, pulses etc.were recorded by an Avery weighing scale.
For any item below 1 kg, a small weighing scale was used. The number of
children who dined that day and their ages were recorded.
Daily consumption of calories and important nutrients were calculated
using “Nutritive value of Indian Foods” (ICMR) 49 and compared with
recommended balanced diets.
Environmental conditions:
All hostels were visited and information was collected regarding
environmental conditions by inspection using a proforma (Annexure-II).
Laboratory Tests:
Haemoglobin estimation was done by Sahli’s method (Annexure-III)
on a 20% subsample of subjects, drawn by systemic random sampling. The
WHO cut off levels were taken as standards to classify the haemoglobin
status.
58
Table showing stages of anaemia50
Analysis:
Data collected was entered in Microsoft Office Excel and analysed by using
SPSS Version 12.0.
Proportions were calculated for different study variables.
Chi-square test was used for analysis of categorical variables.
Criteria of significance used in the study was p < 0.05.
Listing and Citing of References:
Vancouver’s style was used for listing and citing of references.
59
RESULTS
60
RESULTS
I. Socio-Demographic Profile
Table1: Demographic background of study subjects (n=542)
Socio-demographic
factors
Urban
(%)
Rural
(%)
Total
(%)
Significance
Age group (Years)
11 – 13 60(18.81) 259(81.19) 319(100) χ² = 1.88
df = 2
p = 0.39
14 – 15 21(12.88) 142(87.22) 163(100)
16 – 19 8(13.33) 52(86.67) 60(100)
Total 89(16.42) 453(83.58) 542(100)
Type of family
Nuclear 64(14.95) 364(85.05) 428(100) χ² = 3.21
df = 2
p = 0.2
Joint 24(21.82) 86(78.18) 110(100)
Three – generation 1(25) 3(75) 4(100)
Total 89(16.42) 453(83.58) 542(100)
Family size
< 4 members 31(18.23) 139(81.77) 170(100) χ² = 1.7
df = 2
p = 0.43
4-6 members 42(14.29) 252(85.71) 294(100)
>6 members 16(20.51) 62(79.49) 78(100
Total 89(16.42) 453(83.58) 542(100)
Majority of the girls were from rural background (83.58%). The
present study revealed that irrespective of the area majority belonged to
nuclear families (78.97%). Majority of the study subjects are having a
61
average family size of 4-6 (54.2%). There is no significant difference
between urban and rural areas for the above Socio-demographic factors.
Table2: Educational background of parents of study subjects (n=542)
Urban (%)Rural
(%)Total (%)
Significance
Mother’s education
Illiterate 41(15.59) 222(84.41
)
263(100) χ² = 3.12
df = 2
p = 0.2School educated 44(16.73) 219(83.27
)
263(100)
College
educated
4 (25) 12(75) 16(100)
Total 89(16.42) 453(83.58
)
542 (100)
Father’s education
Illiterate 41(15.59) 222(84.41
)
263(100) χ² = 25.92
df = 2
p = 0.00School educated 42(15.85) 223(84.15
)
265(100)
College
educated
6(42.86) 8(57.14) 14(100)
Total 89(16.42) 453(83.58
)
542 (100)
62
Majority of mothers from rural areas were illiterate (41%) and in
urban areas majority were school educated (8.1%). On the other hand
nearly41.1% fathers from rural areas were educated up to school level
followed by illiterates (41%).In case of urban areas number of fathers with
illiterate and school educated were almost equal. When compared with
mothers and fathers, maximum numbers of fathers were school educated
where as equal numbers of mothers were illiterate and school educated.
There is significant difference between urban and rural areas for father’s
education.
Table3: Occupational background of parents of study subjects (n=542)
Mother’s
occupation
Urban (%) Rural (%) Total (%) Significance
Home maker 35(26.51) 97(73.49) 132(100) χ² = 63.73
df = 3
p = 0.00
Labour 32(9.64) 300(90.36) 332(100)
Service 16(23.53) 52(76.47) 68(100)
Others 6(60) 4(40) 10(100)
Total 89(16.42) 453(83.58) 542 (100)
Father’s occupation
Farming 20(6.87) 271(93.13) 291(100) Χ² = 33.27
df = 3
p =0.00
Labour 26(21.67) 94(78.33) 120(100)
Service 31(41.33) 44(58.67) 75(100)
Others 12(21.43) 44(78.57) 56(100)
63
Total 89(16.42) 453(83.58) 542 (100)
When considered in terms of mother’s occupation 61.25 % were
labourers followed by home maker (17.9%) in rural areas. 72.14% of
father’s were farmers followed by 22.14% labourers, 13.84% service and
10.32% others. There is significant difference between urban and rural
areas for mother’s and father’s occupation.
64
Table4: Educational status of study subjects (n=542)
Educational status Frequenc
y
Percentage
Middle school 194 35.79
High school 304 56.08
College education 44 8.11
Total 542 100
On the whole 35.79% were in middle school, 56.08% were in high school,
8.11%were in college education.
Table5: Duration of Stay of study subjects in the hostel (n=542)
Period of stay
(years)
Total (%)
<5 466 (85.97)
>5 76 (14.03)
Total 542 (100)
The study shows that majority of girls stayed less than five years in
the hostel.
65
II. MORBIDITY STATUS
Table 6: Current morbidity profile of study subjects (n = 542)
Morbidity Frequency Percentage
1 Pediculosis 451 83.21
2 Dysmenorrhea (n=273) 119 43.6
3 Pallor 223 41.14
4 Dental caries 152 28.04
5 Skin disorders 143 26.4
6 Vitamin deficiency 117 21.57
7 Passing worms in the stools 72 13.28
8 Defective vision 67 12.36
9 ENT disorders 38 7.01
1
0
Inflamed Gums 25 4.61
1
1
Respiratory infections 26 4.85
1
2
Diarrhoea 14 2.58
1
3
Cardiovascular disorders 6 1.11
1
4
Musculoskelet al. disorders 5 0.9
1
5
Lymphadenopathy 4 0.73
1
6
Having one or more morbid conditions 482 88.93
66
The major prevalent morbid conditions among girls were Pediculosis
83.21%, Dysmenorrhea 43.6% Dental caries 28.04%, Skin disorders 26.4%
(scabies-20.84%, eczema-2%, ulcers-2%, warts-1.56%) Vitamin deficiency
21.57%(vitamin A - 0.74%, vitamin B- 7.93%, vitamin C- 11.44%, vitamin
B&C- 1.46%), clinical anaemia 41.14% and defective vision 12.36% .On the
whole 88.93% of the girls were having one or more morbid conditions,
11.07% were free from any recognizable morbidity.
Table7: Morbidity pattern of study subjects across age groups (n=542)
Morbidity
Age group in years
P value
11-13
(n=319)
14-15
(n=163)
16-19
(n=60)Frequency
(%)
Frequency
(%)
Frequency
(%)
Pediculosis 281(88.1) 132(81) 38(63.3) 0.00(HS)*
Poor personal
hygiene
159(49.8) 69(42.3) 19(31.7) 0.04 (S)#
Pallor 141(44.2) 56(34.3) 26(43.3) 0.28(NS)§
Skin disorders 97(30.4) 36(22.1) 10(16.7) 0.09(NS)§
Vitamin deficiency 73(22.8) 27(16.5) 15(25) 0.36(NS)§
Defective vision 30(9.4) 31(19) 8(13.3) 0.11(NS)§
ENT disorders 19(5.9) 15(9.2) 4(15) 0.01 (S)#
Respiratory
disorders
16(5) 8(5) 2(3.33) 0.72(NS)§
Dysmenorrhea 27(35.5) 52(37.96) 40(66.7) 0.00(HS)*
67
(n=76) (n=137) (n=60)
S#-significant; NS§-not significant; HS*-highly significant.
Pediculosis, poor personal hygiene and dysmenorrhea were found to
have significance across the age groups. High morbidity was found in 11-13
year age group.
Table 8: Illness of study subjects in past two weeks (n = 542)
Illness in last 2 weeks Frequency Percentage
Pyrexia 229 42.25
Scabies 91 16.79
Diarrohea 60 11.07
Acute respiratory infections 36 6.64
Exanthematous fever 21 3.87
Dysmenorrhea 18 3.32
Having one or more illness 446 82.3
In 542 subjects, 17.7% did not report any illness in the past two
weeks, 446 (82.3%) reported illness in the past two weeks. 42.25% suffered
from pyrexia, followed by 16.79% scabies, 11.07% diarrohea and 6.64%
acute respiratory infections.
68
III. Menstrual Health
Table 9: Age at Menarche of study subjects (n = 273)
Age
(years)
Frequency Percentage
10 2 0.7
11 5 1.8
12 81 29.7
13 91 33.3
14 70 25.6
15 23 8.4
16 1 0.4
Total 273 100
Out of 542 girls, 273 (50.36%) attained menarche. Majority of them
attained menarche at the age of 13 years (33.3%) followed by 12 years
(29.7%) and 14 years (25.6%).
69
Table10: Menstrual pattern of study subjects (n=273)
Menstrual cycle Frequency Percentag
e
Regular 171 62.6
Irregular 102 37.4
Bleeding during menstruation
<3 days 18 6.6
3-5 days 211 77.3
6-7 days 36 13.2
>7 days 8 2.9
Dysmenorrhea
Never 154 56.4
Occasionally 30 11
Frequently 12 4.4
Always 77 28.2
PreMenstrualTension
Never 231 84.6
Occasionally 14 5.1
Frequently 2 0.7
Always 26 9.5
Breast pain during menstruation
Never 255 93.4
Occasionally 6 2.2
Frequently 2 0.7
Always 10 3.7
70
This table shows the menstrual pattern in 273 girls who attained
menarche. 62.2% had regular menstrual cycle, 77.3% had an average of 3-5
days of menstrual bleeding. 28.2% always suffered from dysmenorrhea .
9.5% always suffered from premenstrual tension. 3.7% always suffered from
breast pain during menstruation.
Table 11: Menstrual hygiene in study subjects (n=273)
Method of disposal Frequency Percentage
Cloth pieces reused 46 16.9
Pads / cloths disposed properly 200 73.3
Pads / cloths disposed
improperly
27 9.9
No. of pads used per day
<2 97 35.5
>2 176 64.5
64.5% used more than two pads per day during menstruation.
Majority of them (73.3%) were using sanitary pads or cloths which are
disposed properly.
71
III. NUTRITIONAL STATUS
Anthropometric Measurements
Table 12: Age wise distribution of Median weight of study subjects (n=542)
Age(yrs
)
Number
of girls
Median wt(kg) S.D
.
NCHS(50th percentile)
Weight( kg)
11 78 30 4.69 37
12 102 34 4.85 42
13 139 36 5.18 46
14 112 39 4.67 49
15 51 40 4.84 52
16 22 41.5 8.63 54
17 10 44 4.92 55.30
18 8 45.5 2.10 56.20
19 20 45 2.94 57.20
The median weight of the girl ranged from 30 ± 4.69 Kg to 45.5 ±
2.10 Kg. The median weight increased as the age increased. When compared
to 50th percentile of NCHS standards the mean weights of girls in the present
study were very low. This was significant with a t value of 0.002.
72
Figure1: Line chart showing Weight for Age
Figure2: Line chart showing Height for Age
73
11 1213 1415 1617 18 1930354045505560
Weight for Age
NCHS StandardsPresent study
Age in years
Wt in kg
Table 13: Median Height compared with NCHS standards in study
Subjects (n=542)
Age
(years)
Number
of girls
Median height(cm) S.D. NCHS(50th percentile)
Height(cm )
11 78 131 6.24 144
12 102 138 6.28 151
13 139 143 5.68 157.5
14 112 147 6.04 161
15 51 149 5.15 162
16 22 154 6.25 162.5
17 10 153.50 2.46 163
18 8 154.5 4.06 163.2
19 20 153.5 4.10 163.5
The median height of the girls ranged from 131 ± 6.24 cm to 154.50 ±
4.06cm. When compared to 50th percentile of NCHS the median height of
74
11 12 13 14 15 16 17 18 19130135140145150155160165
Height for age
NCHS StandardsPresent study
Age in years
Ht in cm
girls in the present study were very low. This was significant with a t value
of 0.005.
75
Table14: Prevalence of Stunting in study subjects (n=542)
Age group
(Years)
Number
of girls
Stunting
Frequency Percentage
11 - 13 319 28 8.8
14 – 15 163 24 14.7
16 – 19 60 8 13.3
Total 542 60 11.07
χ²=0.97, df=2, p>0.05
Stunting was highest 14.7% in 14-15 year age group, followed by
13.3% in 16-19 years and 8.8% in 11-13 year age group.
Figure3: Bar diagram showing Prevalence of Thinning and Stunting
11-13 14-15 16-190
20
40
60
80
50.8
74.8
46.7
8.814.7 13.3
Prevalence of Thinning and Stunting
ThinningStunting
Age group (years)
Percentage
76
Table15: Prevalence of Thinness in study subjects (n=542)
Age group
(Years)
Number
of girls
Thinness
Frequency Percentage
11 - 13 319 162 50.8
14 – 15 163 122 74.8
16 – 19 60 28 46.7
Total 542 312 57.56
χ²=0.62, df=2, p>0.05 The prevalence of thinness in the study subjects was 57.56%. Thinness
was highest in the age group of 14-15 year i.e., 46.7%, followed by 50.8 %
in 11-13 years and 46.7% in 16 – 19 year age group.
Table 16: Distribution of study subjects according to BMI staging (n=542)
BMI staging Frequency Percentage
1 <18.5(under weight) 350 64.6
2 18.5-22.99(normal) 188 34. 7
3 23-24.99(pre-obese) 2 0.4
4 >25(obese) 2 0.4
Total 542 100
According to WHO BMI staging 64.6% were underweight, 0.4% were
pre-obese and 0.4% were obese.
77
Figure4: Histogram showing Age and Mean Haemoglobin
11 12 13 14 15 16 17 18 190
4
8
12 10.22 10.87 11.01 11.23 10.6 11.26 11.512.6
10.92
Age and Mean Haemoglobin
Age in years
Mean haemoglobin gm/dl
The mean haemoglobin of the girls ranged from 10.22±0.5 to
12.6±0.11 gm/dl. The mean haemoglobin level was highest in 18 year age
group.
78
Table 17: Grading of Haemoglobin of study subjects according to WHO criteria (n=135)
Haemoglobin(gm/dl) Frequency Percentage
1 Normal (>12) 68 50.4
2 Mild Anaemia (7-9.99) 22 16.3
3 Moderate Anaemia (10-11.99) 39 28.9
4 Severe Anaemia (<7) 6 4.4
Total 135 100
A 20% sub-sample of 542 subjects i.e. 135 subjects were examined
for Haemoglobin estimation. 49.6% were found to be anaemic.
Figure5: Pie diagram showing Grading of Haemoglobin
50.4
16.3
28.9
4.4
Grading of Haemoglobin
NormalMildModerateSevere
79
Table 18: Mean Haemoglobin of study subjects according to Menstrual Status (n=135)
Menstrual Status Number (%)
Mean Hb (gm/dl)
S.D 95% CI
Menstruating 78 (57.77) 11.06 1.59 10.7-11.42Non-menstruating 57 (42.33) 10.69 2.20 10.11-11.27
(z=1.12)Out of 135 girls in whom haemoglobin estimation was done, the mean
haemoglobin in menstruating girls (11.06 ± 1.59 gm/dl) was more than in
non-menstruating girls (10.69 ± 2.20 gm/dl) .The mean difference between
these two groups was found to be not significant. (z=1.12).
Table 19: Duration of stay of study subjects in the hostel and Anaemia (n=135)
Period of
stay
(years)
Anaemia
Total
(%)
Present
(%)
Absent
(%)
<5 40(52) 37(48) 77(100)
>5 27(46.55) 31(53.45) 58(100)
Total 67(49.63) 68(50.37) 135(100)
(χ ²=0.2,df = 1, p = 0.65)
Out of 77 girls who stayed less than five years in the hostel, anaemia
was present in 52% where as in those who stayed more than five years
anaemia was present in 46.55% and this was found to be statistically
insignificant. (χ ²=0.2,df = 1, p = 0.68)
80
Table 20: Prevalence of Anaemia and Passing worms (n=135)
Passing wormsin the stool
Anaemia
Present (%)Absent
(%)Total (%)
Present 27(84.38) 5(15.62) 32(100)
Absent 40(38.84) 63(61.16) 103(100)
Total (%) 67(49.62) 68(50.38) 135(100)
(df = 1, χ² = 18.474, p <0.001)In 49.62% of girls who were anaemic 84.38% had the history of
passing worms, where as in 50.38% of girls who were not anaemic,15.62%
have the history of passing worms. This was found to be statistically
significant. (df = 1, χ² = 18.474, p < 0.001)
IV. Diet Survey:
The diet survey, as apart of nutritional assessment was carried out in
two girl’s hostels. The finding of the survey in terms of intake of nutrients
and intake of food articles compared with recommended allowances are
presented here. The requirements of nutrients and food items were computed
by multiplying number of children in each group and the recommended
values for children of corresponding ages.
81
CaloriesProteins
(gm)
Fats
(gm)
Calcium
(mg)
Iron
(mg)
Vitamin-
A
Carotene
(µg)
Vitamin-
B1 (mg)
Vitamin-
B2 (mg)
Nicotinic
acid (mg)
Vitamin-
C (mg)
Requirements 1,70,680 5,100 1,870 51,000 1,955 2,04,000 85 102 1,139 3,400
Actual
consumption
1,96,628 5,343 2,643 41,800 3,422 6,13,624 279 5,002 899 5,302
Excess 25,948 243 773 - - 4,09,624 - 654 240 1,902
Deficit - 9,200 1,467 - 194 4,900 -
Table 21: Estimated daily intake of calories and nutrients compared with requirements (n=85)
Calories, proteins, Fats, vitamin-A, vitamin- B2, vitamin- C intake was adequate. The intake of other nutrients
was below the actual requirement
Table 22: Daily intake of food items compared with requirements in terms of recommended balanced diets
82
(n=85)
Cereals
(gm)
Pulses
(gm)
Green leafy
vegetables
(gm)
Other
vegetables,
roots and
nuts (gm)
Fruits
(gm)
Milk
(gm)
Fats
and
oils
(gm)
Eggs
(gm)
Sugar
and
jaggery
(gm)
Requirements 28,305 5,465.5 10,336 9,095 3,519 18,836 4,080 2,550 3,519
Actual
consumption
32,300 6,375 3,400 8920 7,650 1,530 1,275 5,100 867
Excess 3,995 909.5 - - 4,131 - - 2,550 -
Deficit - - 6,936 175 - 17,306 2,805 - 2,652
Cereals, pulses, fruits and egg intake was adequate whereas the intake of all other food items were
below the recommended levels.
Table 23: Estimated daily intake of calories and nutrients compared with requirements. (n=140)
83
Calories Proteins
(gm)
Fats
(gm)
Calcium
(mg)
Iron
(mg)
Vitamin
- A
Carotene
(µg)
Vitamin
- B1
(mg)
Vitamin
-B2
(mg)
Nicotinic
acid
(mg)
Vitamin
- C
(mg)
Requirements 2,88,400 9,100 3,080 84,000 3,920 3,36,000 168 140 1960 5,600
Actual
consumption
4,40,600 4,248 5,300.15 1,65,320 7,899 4,85,241 986.96 7,280 2,725 7,900
Excess 1,52,200 - 2,220.15 81,320 3,979 1,49,241 818.96 7,140 765 2,300
Deficit - 4,852 - - - - - - - -
The intake of all nutrients was adequate except the proteins which was less than the recommended values.
Table 24: Daily intake of food items compared with requirements in terms of recommended balanced diets.
84
(n=140)
Cereals
(gm)
Pulses
(gm)
Green
leafy
vegetables
(gm)
Other
vegetables,
roots and nuts
(gm)
Fruits
(gm)
Milk
(gm)
Fats
and
oils
(gm)
Eggs
(gm)
Sugar
and
Jaggery
(gm)
Requirements 49,000 7,000 21,000 21,000 4,200 21,000 5,600 8,400 4,200
Actual
consumption
80,000 8,100 2,000 12,500 15,000 16,000 2,200 4,200 6,700
Excess 31,000 1,100 - - 10,300 - - - 2,500
Deficit - - 19,000 8,500 - 5,000 3,400 4,200 -
The intake of cereals, pulses, fruits, sugar and Jaggery were adequate, whereas the intake of all other
food items were below the recommended levels
85
Table26: Environmental Conditions of Social Welfare Hostels
Sl.No
Environmental conditionsGirls hostel
I(n=165)
Girls hostel II
(n=140)
Girls hostelIII
(n=104)
Girls hostel IV
(n=165)
College hostel(n=65)
Ananda nilayam(n=77)
1 Distance from road (mts) 50 50 134 64 64 502 Source of noise and dust Present Present Absent Absent Absent Present 3 Floor area per girl (sq.ft) 9.8 11 6 6.4 12 9.74 Ventilation (window area) Inadequate
(18%)Adequate (21%)
Inadequate (15%)
Adequate (21%)
Adequate 42%
Adequate 45%
5 Indoor lighting Insufficient Sufficient Insufficient Sufficient sufficient sufficient6 Furniture Not provided Not
providedNot provided Not
providedNot provided Not provided
7 Reading facilities Inadequate Inadequate Inadequate Inadequate Inadequate Inadequate8 a. Water supply
b. Storage of drinking water
c. Drawal of drinking water
InadequateSatisfactory
Satisfactory
InadequateSatisfactory
Satisfactory
AdequateSatisfactory
Satisfactory
Inadequate Not SatisfactoryNot Satisfactory
InadequateSatisfactory
Satisfactory
InadequateSatisfactory
Satisfactory
9a. No. of toilets b. Toilet : pupil ratioc. Maintenance
61:27Bad
61:23 Bad
81:13Good
71:23Bad
21:32 Good
61:13 Bad
86
10a. No. of bathroomsb. Bathroom : pupil ratioc. Maintenance
61:27 Bad
61:23 Bad
61:17 Good
71:23Bad
21:32Good
61:13Bad
11Facilities for collection and disposal of refuse and garbage
Adequate Adequate Adequate Adequate Adequate Adequate
12
a. Physical condition of the kitchenb. Fuelc. Storage of raw food
d. Rodent infestation
Bad
LPGSeparate room
Absent
Bad
LPGSeparate roomAbsent
Good
LPGSeparate roomAbsent
Good
LPG Separate roomPresent
Bad
FirewoodSeparate roomPresent
Bad
LPGSeparate roomAbsent
13 Dining hall Absent Absent Absent Absent Absent Absent
14 Food handler’s hygiene(physical examination)
Good Good Good Good Bad Good
87
The per capita floor area for the hostel children ranged from 6 sq.ft -
12 sq.ft in girls’ hostels which was well below the prescribed norm of
20sq.ft per child. The number of toilets provided was inadequate which
ranged from 1 for 32 girls in one hostel and 1 for13 in another hostel. Water
supply and storage of drinking water are not satisfactory. The inmates of all
the hostels are falling short of prescribed sanitary requirement of 1 sanitary
facility for 10 children. The condition of the kitchen was bad in college
hostel and two hostels have rodent infestation. Dining hall provision is
absent in all hostels and indoor lighting was found to be inadequate in two
hostels.
88
DISCUSSION
89
Discussion
The results of the study done at Social welfare hostels, Nellore among
adolescent girls aged 11-19 years are discussed below.
Morbidity profile:-
The health problems of adolescent girls vary from place to place and
several studies conducted in India and abroad revealed that the main
morbidity conditions include infectious diseases, malnutrition, pediculosis,
dental caries, helminthiasis, and diseases of skin, and ear.
In the present study, the leading causes of morbidity were pediculosis
(83.2%), pallor (41%), dysmenorrhoea (43.6%), dental caries (28%), skin
diseases (26.4%), vitamin deficiency (21.5%), and passing worms in stools
(13.2%) and defective vision (12%).
In a study conducted by Srinivasan7 (2000), in Tirupati in 598 children
aged 6-17 years, the common morbid conditions found were skin disorders
25.7%, dental caries 21.5%, history of passing worms in stool 21.6%,
vitamin B deficiency 3.2%, ARI 1.7% and diarrohea 1.2%.The morbidity
conditions are of similar pattern but the study included boys also.
In a study conducted in urban slums of Lucknow by Singh et
al..19(2006) on 400 adolescent girls aged 10 – 19years, the various morbid
90
conditions found were inadequate oral hygiene (55.4%), pediculosis
(39.2%), cold & cough (25.8%) , lymphadenopathy (22.2%) , scabies
(16.2%) , inflamed tonsils (7.8%) and ear discharge (7%) of girls.
A study conducted by Satapathy et al.51(2008) in tribal children of
Orissa of age up to 15years, the different types of morbidities were fever
24.4%, acute respiratory infections 35.4%, goiter 14.4%, diarrhea 5%,
44.1% splenomegaly. As it is a tribal area, 14.4% suffered from malaria.
Similar study conducted by Geetha et al.24(1997) in Kaniyambadi
Block of North Arcot district of Tamil Nadu, the leading general complaints
were general fatigue, palpitations, backache and abdominal pain. The study
was conducted in rural community; girls were not educated and are more
involved in household chores leading to more musculoskelet al. disorders.
In a study conducted by Balasubramanian22 in rural Tamil Nadu,
prevalence of cold and headache was 16.62% and 10.23% respectively.
Prevalence of general morbidity increased with age and it was high among
illiterate than literates.
In a study conducted by Agarwal et al.23(1999) in Mumbai among
1,144 girls of 5–15 years age group common health problems were hygiene
related (62.2%). Dental caries and helminthiasis were common in younger
91
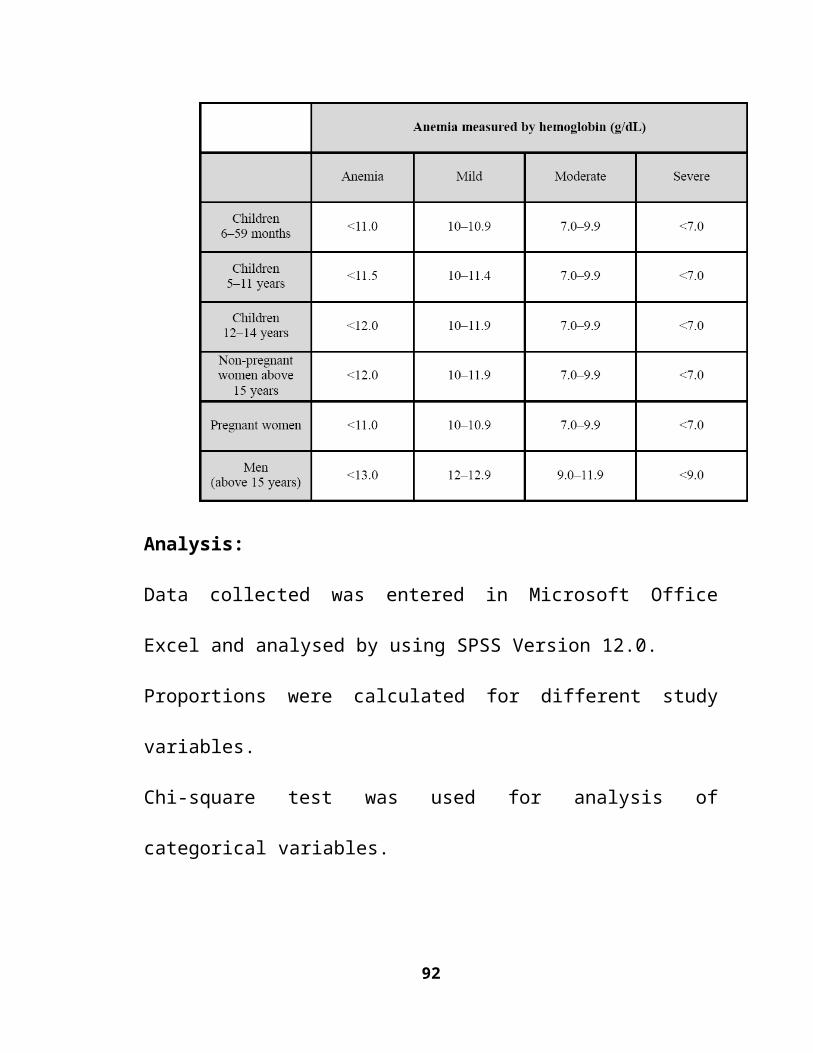
girls; pediculosis was most frequently seen in older girls, 6.6% asthma, 0.5%
cardiac diseases.
In the present study, the morbidity due to skin diseases is 24.4%. In
the study by Srinivasan7, scabies accounted for 29.9%. In a study by Singh et
al.19 scabies accounted for 16.2%. In a study by Satapathy51 scabies
accounted for 15%. The high prevalence of pediculosis and scabies in
present study can be attributed to the over crowding, poor personal hygiene.
In the present study, the prevalence of dental caries is found to be
28.04%. In the study by Srinivasan dental caries was 21.5%. 13.33% of
dental caries was seen in the study conducted by Choudhary et al.32 in
adolescent girls of rural area of Varanasi. The high prevalence of dental
caries in the present study may be due to poor oral hygiene.
In the present study, the history of passing worms in stool is 13%. In
the study by Srinivasan7 the percentage of history of passing worms was
reported to be 21%. 19.4% had history of passing worms in study by
Kalamka (2001) in Nagpur.21
In the present study, 21.5% of study subjects suffered from vitamin
deficiency , among them vitamin C deficiency accounts to 11.44%. In the
study conducted by Srinivasan, the prevalence of vitamin B deficiency was
92
1.6%7 and another study from Western Orissa26 showed a prevalence of
28.6% of vitamin A and 42.9% vitamin B deficiency respectively.
In a study in Lucknow, the prevalence of vitamin A deficiency was
22.2%.19 When compared to other studies the vitamin deficiencies found in
the present study were low as they are in social welfare hostels and are
provided balanced diet when compared to Orissa and Lucknow studies
which were done in general community. The prevalence of angular
stomatitis in study conducted by Dilip kumar Das et al. in West Bengal was
15.4%.41
In the present study defective vision was 12.36%, whereas in other
studies7,19 the prevalence of defective vision was 4.7% and 4.5%
respectively. This difference may be due to inadequate indoor lighting.
Menstrual Pattern
In the present study, the mean age at menarche is 13 years. The age of
menarche among Indian girls, ranges from 11.5–14.5 years, with the current
average age being 13.5 years3.Singh et al..19, in his study found the age of
menarche to be 13.7 years. The results of two studies are comparable to each
other. In the present study dysmenorrhea is present in 43% of study subjects.
In a study conducted by Deo et al.52 dysmenorrhea was present in 31.64%. In
a study conducted by Srinivasan dysmenorrhea was noted in 3.5%. The low
93
prevalence of dysmenorrhea in the other studies may be due to the reason
the study subjects comprised of different age groups.
In a study by Geetha24 in rural south India, the mean age of menarche
was found to be 13.9 years and dysmenorrhea was noted in 21%.
Nutritional status
In the present study, the median weight of subjects ranged from 30 ±
4.69kg to 45.5 ± 2.1kg and the median height ranged from 131 ± 6.24cm to
154.5 ± 4.06cm. These are very low when compared to NCHS standards.53
In the study conducted by Srinivasan7 the mean weights and heights of
both boys and girls were below NCHS standards, reason being both the
studies were conducted in social welfare hostels similar to present study. In a
study by Varsha Zanvar et al.54 of Marathwada region, weights, heights and
BMI were below the NCHS standards. In a study by Banerjee55 in school
children, the heights and weights were below NCHS (50th percentile) and
Indian (50th percentile) standards, 31.7% were under weight and 7.02% were
of short stature when compared to 5th and 3rd percentiles of NCHS. In the
present study 46.7% are having thinness and 13.3% are stunted. This high
prevalence of thinness and stunting may be due to inadequate food intake.
In the study conducted by Srinivasan7 in Tirupati, prevalence of
malnutrition was 78.4%.This high value may be due to lower age group.
94
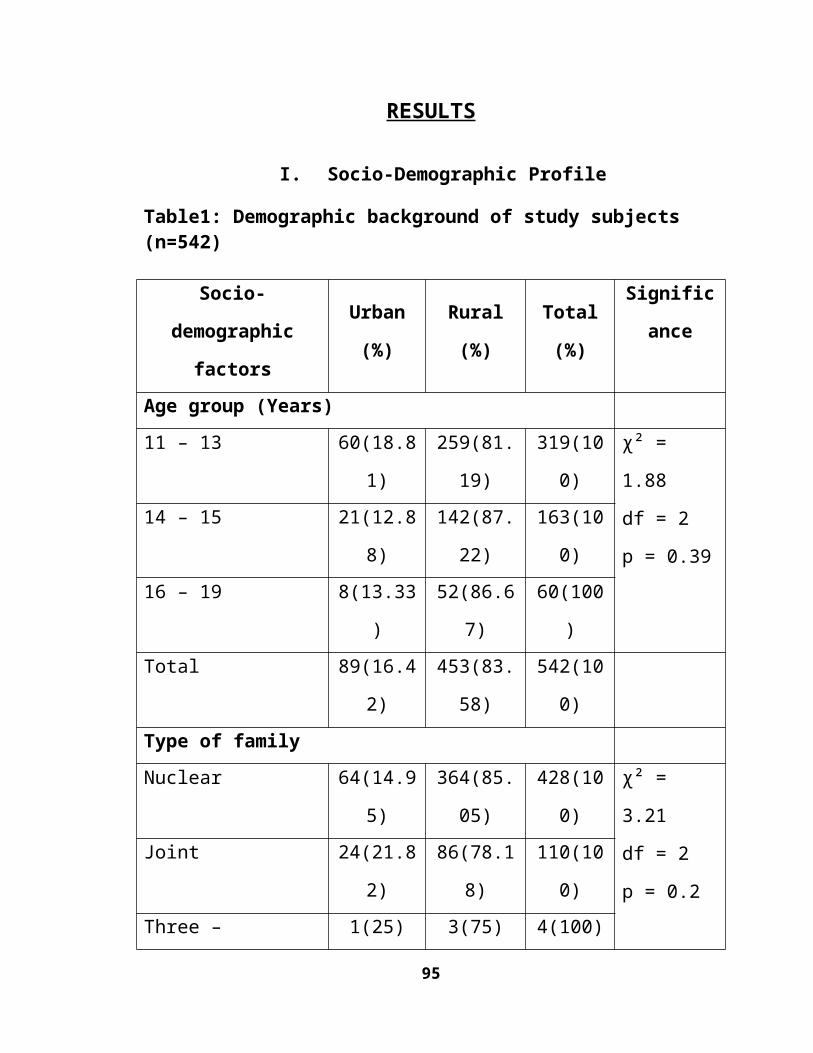
Chabbra35 et al. noted 36.7% of malnutrition in children observation home in
Delhi.
In the study by Deshmukh30 thinness was higher in early adolescence
(57%) than in late adolescence (48.5%) whereas in my study thinness is
highly prevalent in mid adolescence (74.8%) than in early adolescence
(50.8%). This may be due to growth spurt. In a study conducted by Dilip
kumar das41 in West Bengal were 37.8% stunted and 14.7% were thin.
In another study by Medhi et al.29 52% of girls were stunted and 41%
were thin when compared to NHANES standards.
Studies by Geetha24 in rural south India, Raheena Begum56 in
Thiruvanathapuram reported heights and weights less than NCHS standards,
whereas Singh et al.19 in Lucknow in his study reported less than ICMR
standards.
95
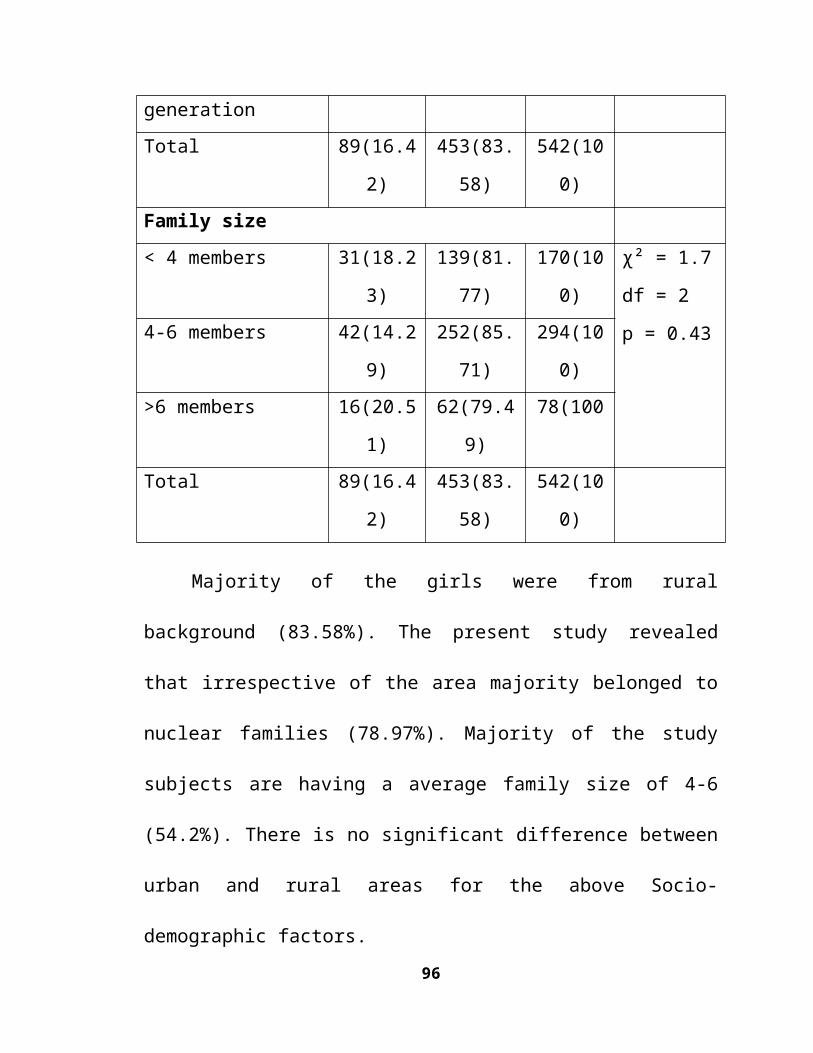
Table: Comparative frequency of under nutrition among Adolescents of different countries57
Reference study Area/ Population
Sex Date of survey
Under Nutrition
Kurz, 1996 Bombay, India Both 1992-93 53.00%
Kurz, 1996 Nepal, Both 1992-93 36.00%Kurz, 1996 Benin,
WestAfricaBoth 1992-93 23%
Cookson et al., 1998
Dadaab, Kenya Both 1998 61%
Woodruff et al.., 1998
Kakuma, Kenya
Both 1998 57%
Woodruff et al.., 1999
Nepal Both 1999 34%
Mukhopadhyay.Aet al.,
Kolkata, India Both 2000 36.49%
de Onis et al., 2001
India Boys 1982-83 50.50%
Venkaiah et al., 2002
India Boys 1996-97 67%
I R C, 1997 Kakuma, Kenya
Boys 1997 75%
Present Study Kolkata, India Girls 2000 30.61%Venkaiah et al., 2002
India Girls 1996-97 40%
I R C, 1997 Kakuma, Kenya
Girls 1997 55%
Ahmed et al., 1998
Dhaka, Bangladesh
Girls 1995 16%
Present Study Nellore,A.P., India
Girls 2009 64.6%
96
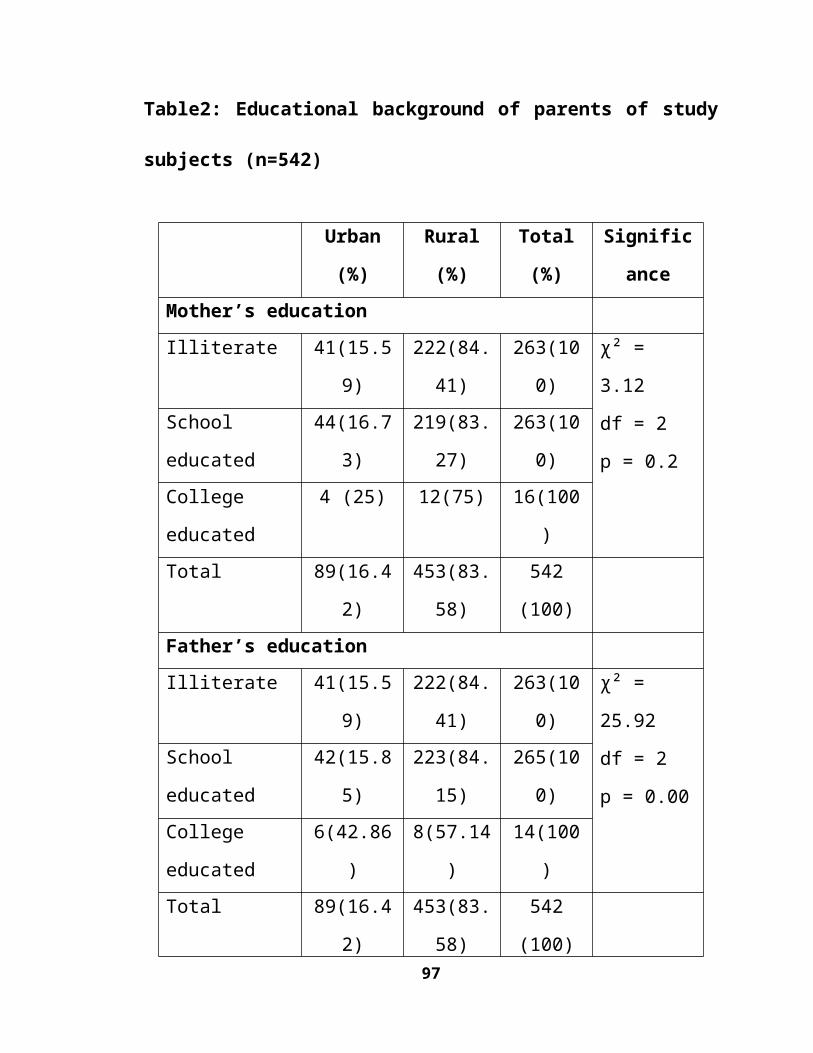
In study by Patil58 in Maharashtra according to WHO Asian Pacific BMI
criteria, 67.8% were under weight.
In the present study according to WHO BMI staging 64.6% were having
chronic energy deficiency (CED), 34.7% were normal, 0.4% obese and 0.4%
preobese. In a study by Kapil et al.59 8.1% were CED grade I, 6.65 were CED
grade II and 78.8% were CED grade III.
In a study by Raheena Begum56 in Kerala, 53% in 14 years age group and
33% in 15 years age group were having BMI <18.5.
In a study by Medhi et al.29 in adolescents of tea garden workers, median
BMI was far below NCHS median and over weight was detected in only 2
adolescents (0.33%) which is similar to the present study.
In a study by Deshmukh et al.30, CED was found to be 75.3%. This high
prevalence of CED in other studies when compared to present study may be due to
fact that they are conducted in communities and most of them have included both
boys and girls.
In the present study 49% of girls suffered from anaemia, 16.3% from mild,
29% from moderate, 4.4% from severe anaemia. The mean haemoglobin ranges
from 10.22 to 12.6gm/dl. Similar prevalence of anaemia was noted in studies by
Dilip kumar et al.41 (44.8%), Varsha Zanvar54 (46.6%), Aneja et al.43 (47%), Singh
et al.19 (56%) and Patel58 in Maharashtra (42%).
97
High prevalence of anaemia was found in studies by Srinivasan7 (80.4%),
Chaturvedi et al.59 (73.7%), Pooja Trivedi42 (82%) and Satapathy et al. 51 (72.7%).
This high prevalence when compared to present study may be due to inadequate
iron intake and relatively high incidence of worm infestation.
In the present study the mean haemoglobin in menstruating girls (11.06 ±
1.59 gm/dl) is more than that of non-menstruating girls (10.69 ± 2.20 gm/dl), this
is similar to the study by Choudhary et al.32 who reported average haemoglobin of
menstruating girls (12.65 ± 1.3 g/dl) more than that of non-menstruating girls
(12.10 ± 1.21 g/dl).This may be attributed to awareness of girls regarding
menstrual blood loss and better intake of nutrients.
In a study by Goel et al. (2007)28 13.3% had anaemia, 84.6% anaemic
subjects had history of worm infestation, similar to the present study where
84.38% anaemic subjects had history of passing worms in stools.
Prevalence of anaemia among adolescents in India according to severity11
Study Country No of subjects /
Year Anaemia prevalence (%)Mild Modera Severe Total
98
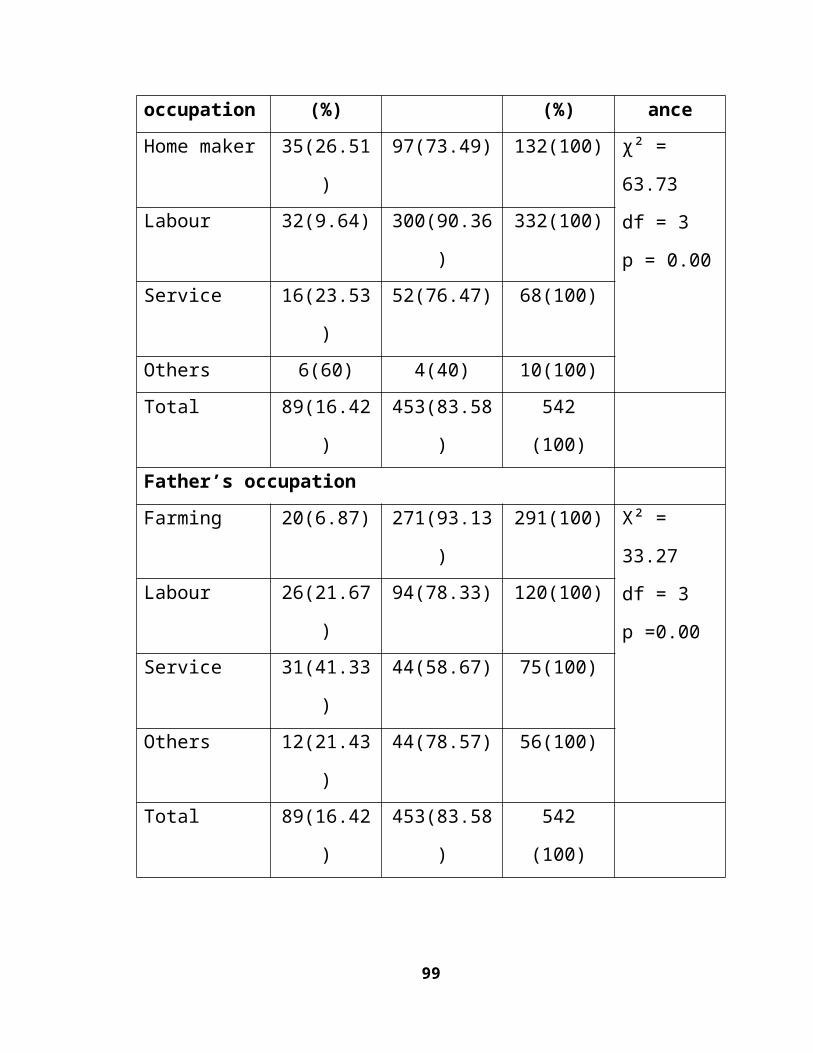
settings te SWACH Foundation
India
(Haryana)
218/206 SGAG/ NSGAG rural
2001 SGAG*-21.9
NSGAG-17.0
SGAG-56.1
NSGAG-61.6
SGAG-7.3
NSGAG -11.7
SGAG-85.3
NSGAG-90.3
ICMR
(Toteja et al.)
India 4337girls/ 16 districts
2001 32.1 50.9 7.1 90.1
Rajarathnam et al.
India
(Tamil Nadu)
316, 13-19 years old girls/rural
2000 36.5 6.3 2.1 44.8
Kotech et al. baseline survey; adolescent girls
India
(Vadodara district)
2860, 12-19 years old girls tribal, rural and urban areas
2000 58.0 15.1 1.6 74.7
*SGAG: School Going Adolescent Girls
NSAG: Non- School Going Adolescent Girls
Diet survey
A study of the consumption of the food items revealed that among the 13-15
years age group the intake of all nutrients was adequate except the proteins, green
leafy vegetables, other vegetables, milk, fats and eggs which were below the
recommended levels. In the 10-12 years age group, the intake of all nutrients was
adequate except milk, fats, iron, green leafy vegetables and other vegetables which
were below the actual requirement.
The diet survey results are comparable to the studies among children in
social welfare hostels of Tirupati town by Srinivasan which revealed deficit intake
99
of pulses, green leafy vegetables, milk, fats and oils, sugar, and jaggery in boys and
girls hostels which was below the recommended levels.
In a study by Swapna et al.59 in Rajasthan adolescent girls had basically a
cereal based diet. The intake of legumes, animal foods, green leafy vegetables and
other vegetables were inadequate.
In the study by Raheena Begum56 in Kerala showed deficit intake of energy,
proteins, green leafy vegetables, other vegetables and iron in a sub sample. In the
study by Varsha et.al in Marathwada54 region showed decreased intake of proteins,
energy, iron, green leafy vegetables, milk and calcium.
Environmental conditions:
The per capita floor area for the hostel children ranged from
6-12sq.ft in girls’ hostels which was well below the prescribed norm of
20sq.ft per child.60 Thus there was over crowding present in all the six hostels
which might be responsible for the high prevalence of skin disorders, pediculosis.
The number of toilets provided was inadequate which ranged from 1 for 32 girls in
one hostel and 1 for13 in another hostel. Dubey and Murdia61 (1976) in a study on
the administration of backward class hostels in Andhrapradesh found that there
was over crowding in the hostels and the sanitary facilities were grossly
inadequate.
100
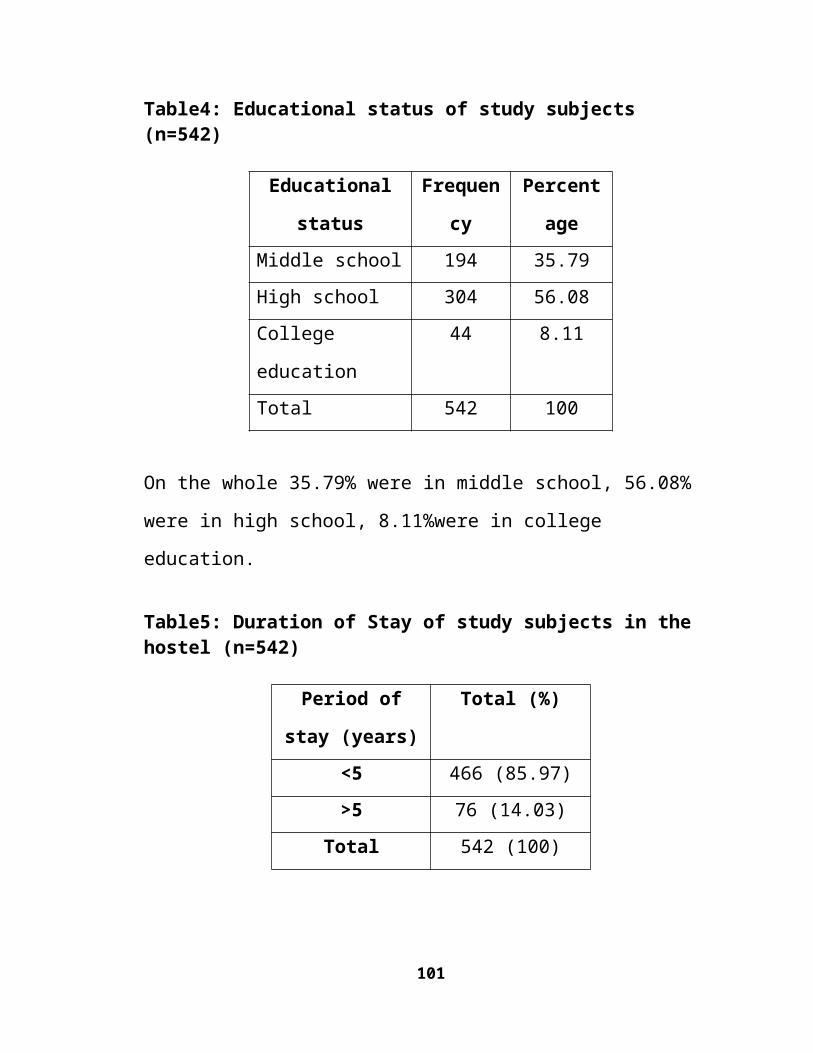
The bad environmental conditions may also account for the high prevalence
of morbid conditions. This observation was supported by the findings of Rajashree
et al.62 (1994) in Kerala which revealed that owing to the environmental
deprivation, the rural coastal children exhibited poorer nutritional status in spite of
better food intake compared to non-coastal children.
101
SUMMARY&
CONCLUSIONS
102
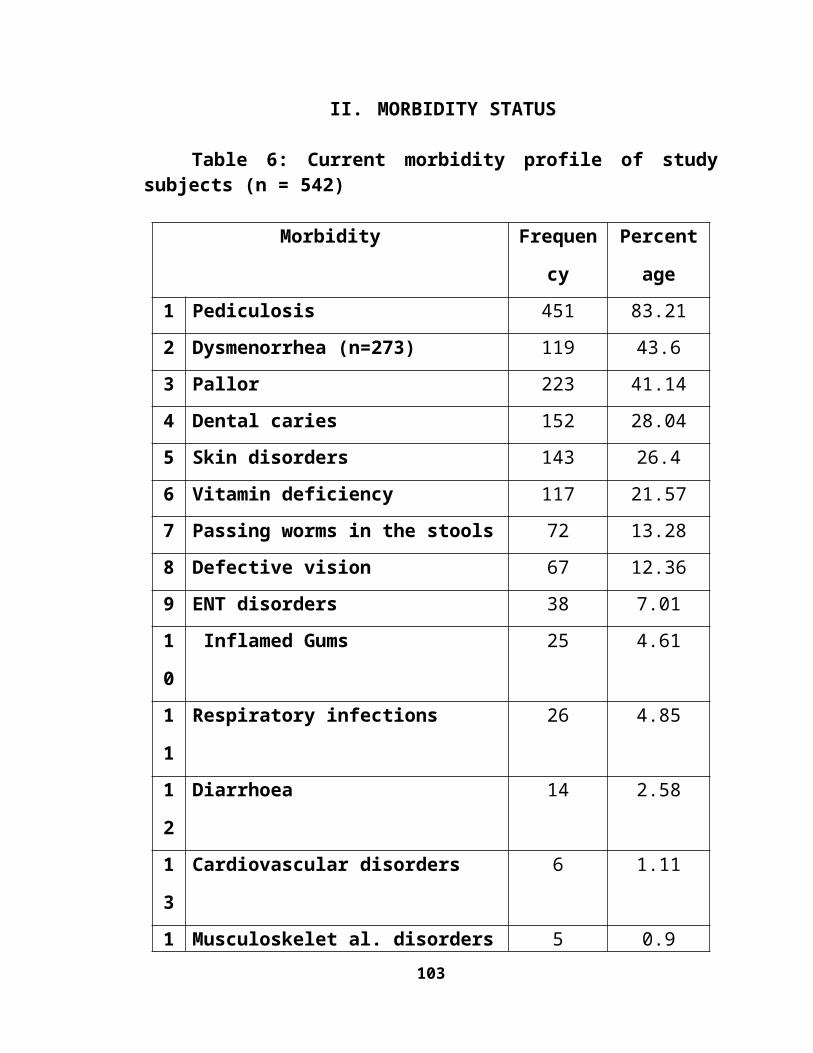
SUMMARY AND CONCLUSIONS
The following are the conclusions from the present study:
1. Majority of the girls were from rural background (83.58%).35.79% were in
middle school, 56.08% were in high school, 8.11%were in college
education. Majority of girls stayed less than five years in the hostel.
2. The major prevalent morbid conditions among girls were Pediculosis
(83.21%), Dysmenorrhea (43.6%), Dental caries (28.04%), Skin disorders
(26.4%), Vitamin deficiency (21.57%), clinical anaemia (41.14%) and
defective vision (12.36%).
3. Pediculosis, poor personal hygiene and dysmenorrhea were found to have
significance across the age groups. High morbidity was found in 11-13 year
age group. 82.3% reported illness in the past two weeks.
4. 50.36% attained menarche, majority at the age of 13 years the mean
hemoglobin of non menstruating girls was more than that of menstruating
girls.
5. The median weight of the girls ranged from 30 ± 4.69 Kg to 45.5 ± 2.10 Kg
and it was very low when compared to 50th percentile of NCHS standards.
The median height of the girls ranged from 131 ± 6.24 cm to 154.50 ±
4.06cm.
103
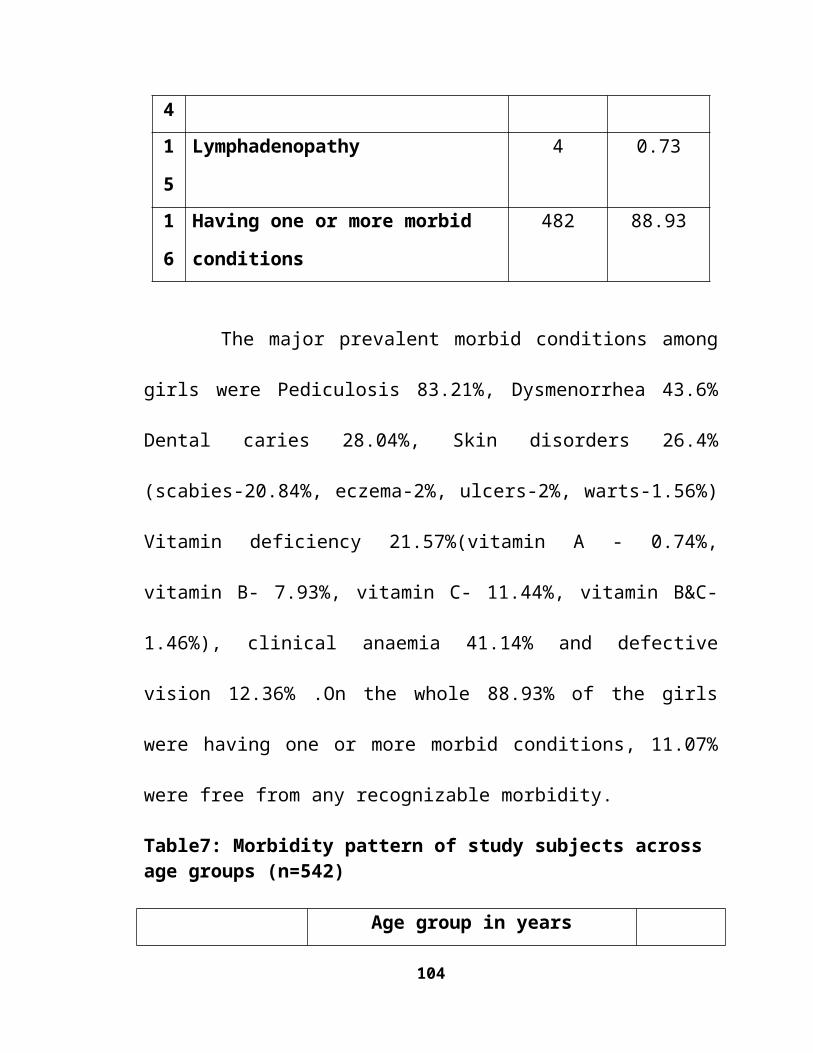
6. Stunting was highest (14.7%) in 14-15 year age group. The prevalence of
thinness was 57.56%. According to WHO BMI staging 64.6% were
underweight.
7. The mean haemoglobin of the girls ranged from 10.22±0.5 to 12.6±0.11
gm/dl. In 135 subjects examined for Haemoglobin estimation, 49.6% were
found to be anaemic, among them 84.38% had the history of passing worms.
8. A study of the consumption of the food items revealed that among 13-15
years age group and 10-12 years age group, green leafy vegetables, other
vegetables, milk, fats and eggs were below the recommended levels.
9. There was over crowding in all the six hostels which might be responsible
for the high prevalence of skin disorders, pediculosis. Number of toilets
provided were inadequate.
104
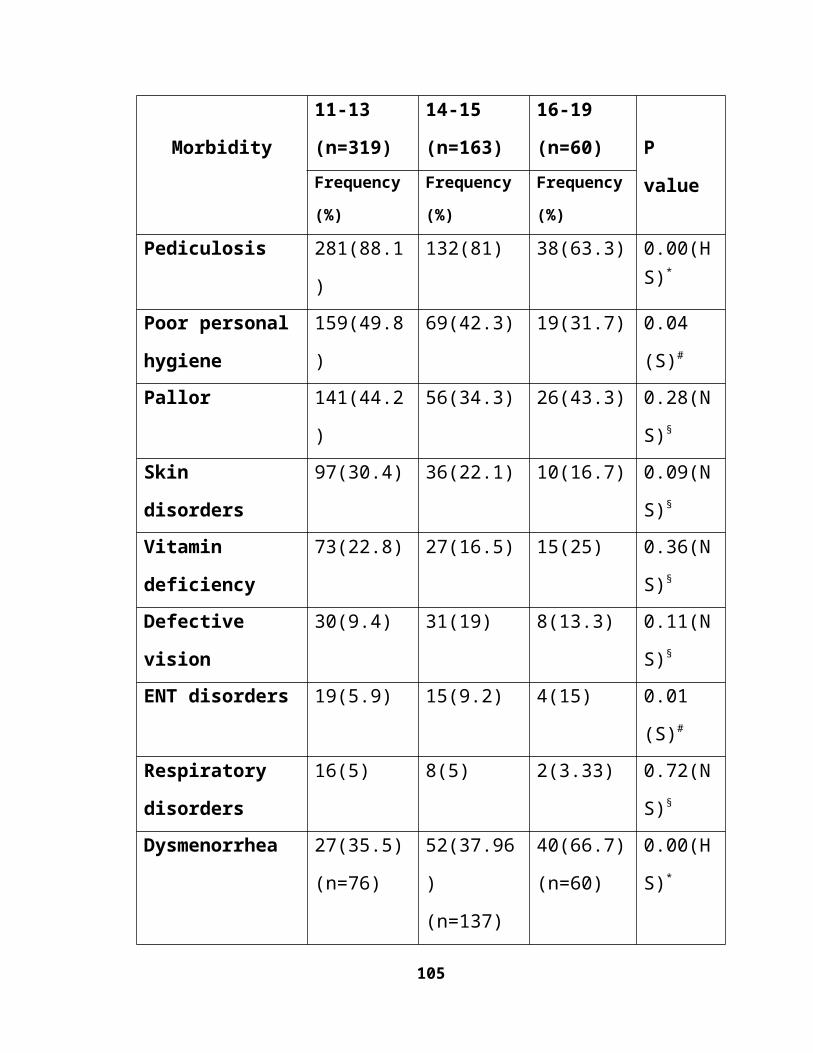
RECOMMENDATIONS
105
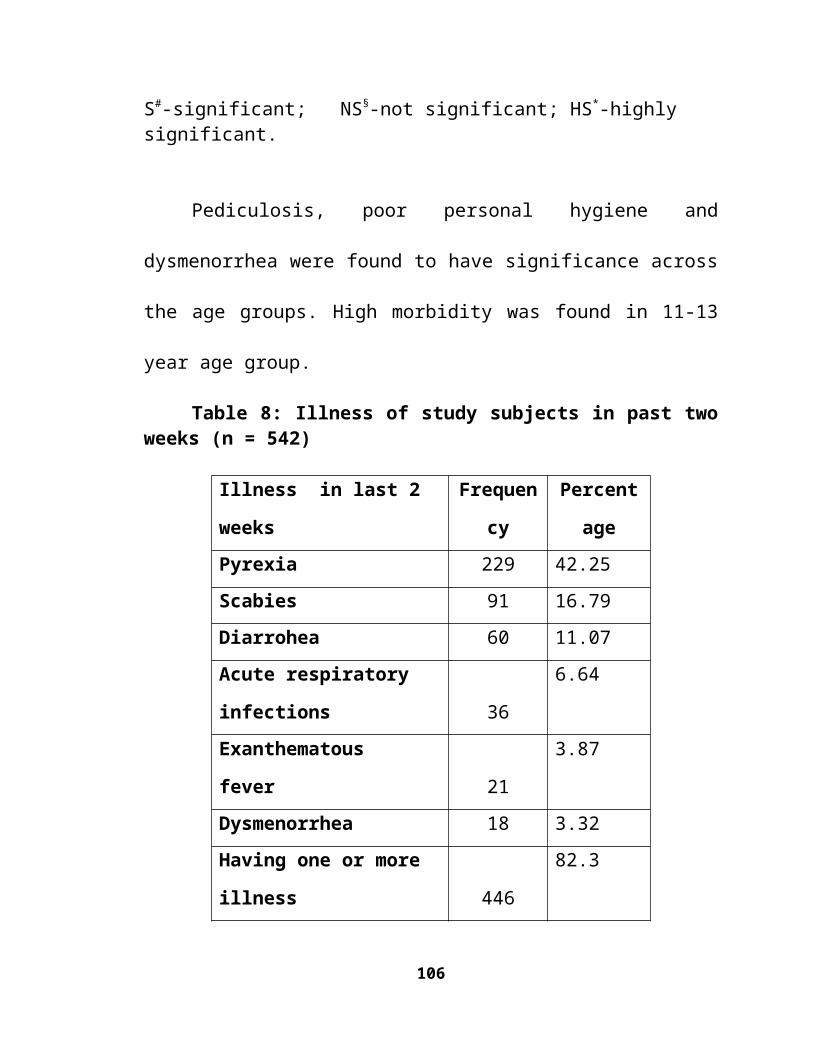
RECOMMENDATIONS
In view of the high prevalence and incidence of morbidity among adolescent
girls in the hostels, regular periodic medical examination and haemoglobin
estimation of inmates and facilities for treatment on the spot at school health clinic
and referral services should be organized and monitored systematically.
Special attention must be paid to the treatment and prevention of certain
diseases like skin diseases, anaemia, worm infestation and menstrual problems etc.
which are recurring in nature. In view of the high prevalence of anaemia, Iron and
Folate supplementation and Deworming must be done periodically.
In view of high prevalence of diseases associated with poor personal
hygiene, instruction to students in respect of personal hygiene, providing necessary
materials like sanitary napkins, soaps and oils etc. in kind and regular supervision
by hostel staff will go a long way in controlling these conditions.
It is very necessary to inculcate hygienic habits among adolescent girls.
Health education programmes on hygiene and common diseases have to be carried
out regularly both at school and in hostels in consultation with health authorities.
The hostel menus need to be modified suitably to provide balanced diet for
intake of various dietary articles sufficient in quantity and quality.
106
The physical conditions of the kitchen should be improved in terms of laying
wash proof tiles and daily cleaning. Proper storage facilities are to be improved to
prevent infestation by rodents and other vermin. Separate furnished dining hall to
be provided for all the hostels.
In view of the existing overcrowding, additional living accommodation has
to be created to satisfy the norms of 20 sq.ft. for each student. Sufficient facilities
for reading and writing have to be provided in terms of space, lighting and sitting
arrangements at all hostels. So necessary provision should be made to construct
new hostel buildings with all these provisions.
Similarly additional bathrooms and toilets have to be provided and
maintained in order to improve the sanitary conditions. Hence a separate post
should be created to look after the sanitary conditions of the hostel.
107
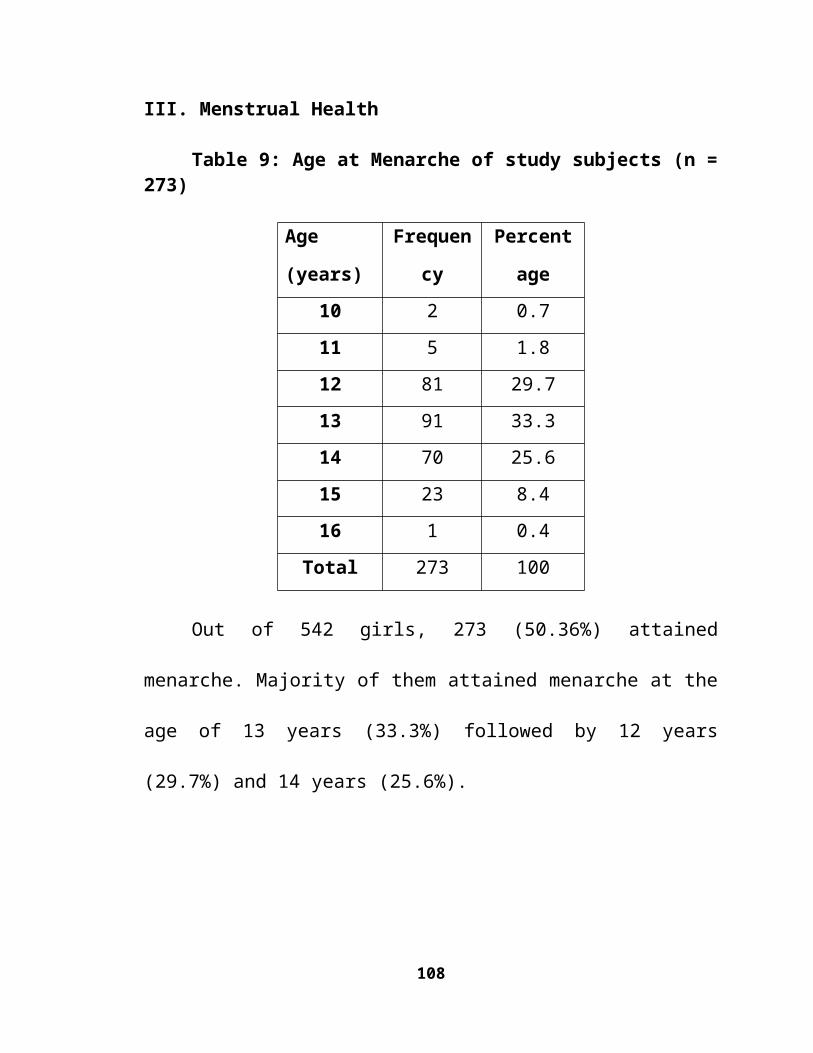
LIMITATIONS
108
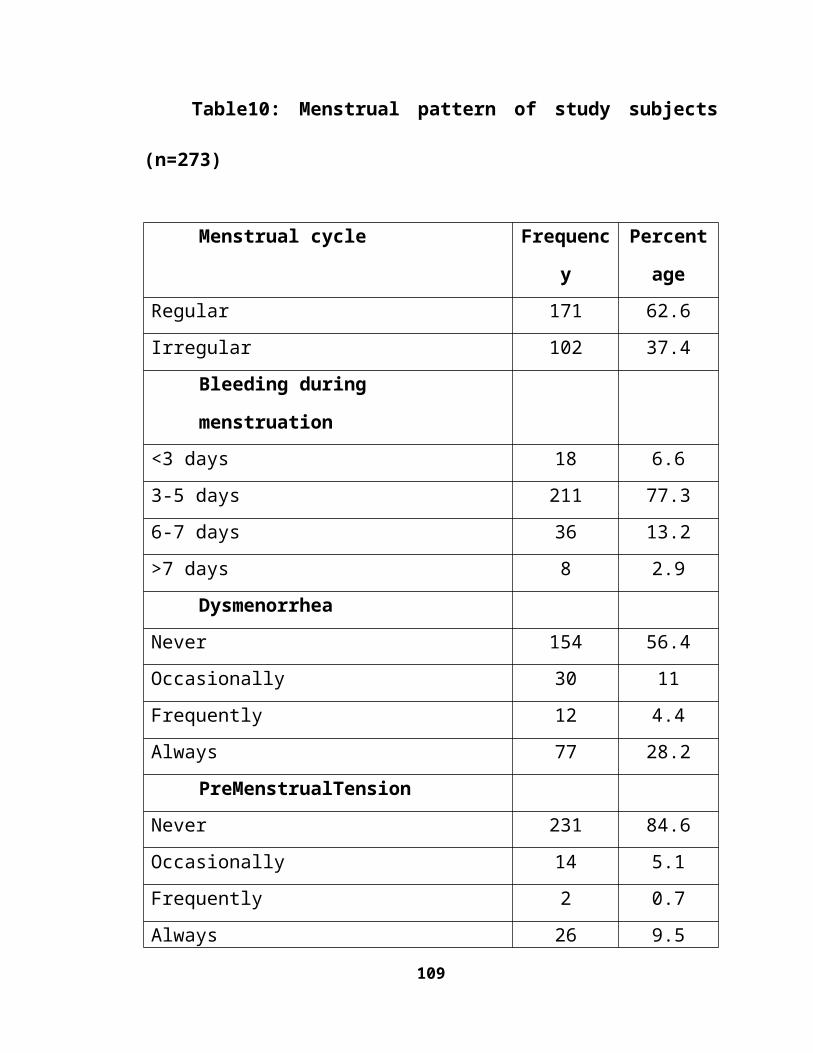
LIMITATIONS
1. Haemoglobin estimation was carried out only on a sub sample of 135
girls and stool examination for worm infestation could not be carried out due
to logistic reasons.
2. In the present study, NCHS standards were used for comparison of mean
heights and weights as IAP standards were not available for 18 and 19 year
age groups.
3. Diet survey was conducted in only two girl’s hostels, due to constraint of
time and resources.
4. Since the hostel authorities were informed about the study, the conditions
observed with regard to the diet and environment may not reflect the true
picture.
109
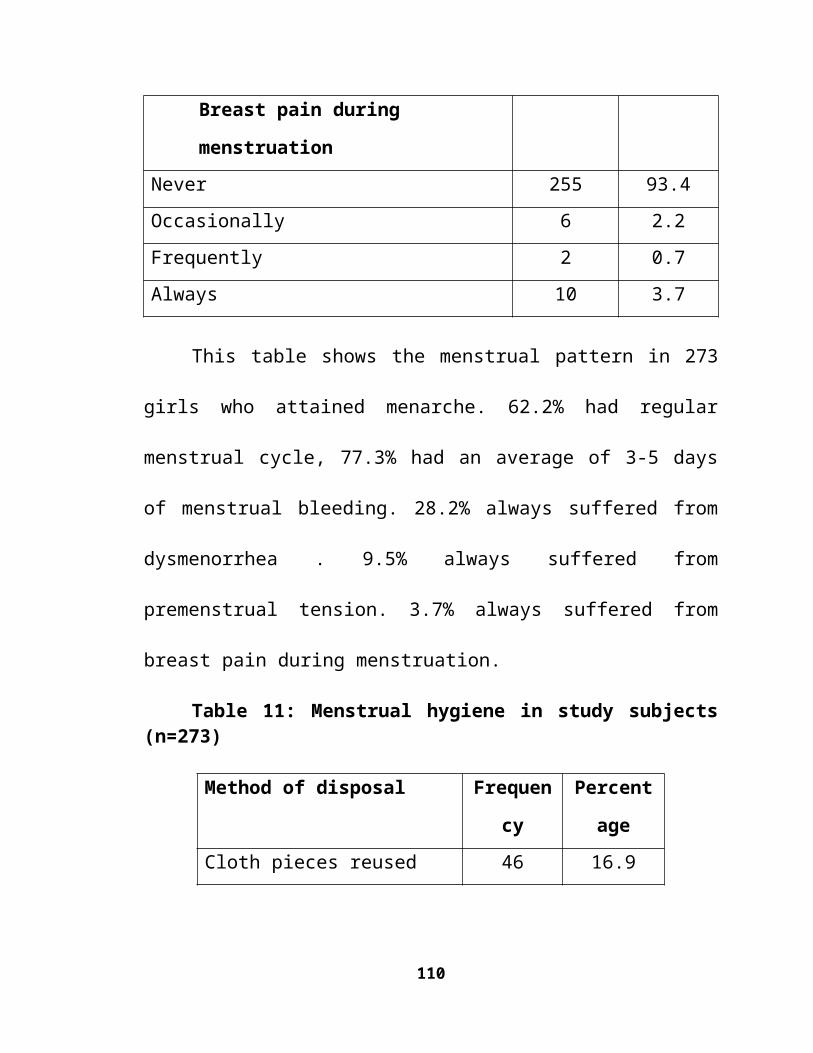
BIBLIOGRAPHY
110
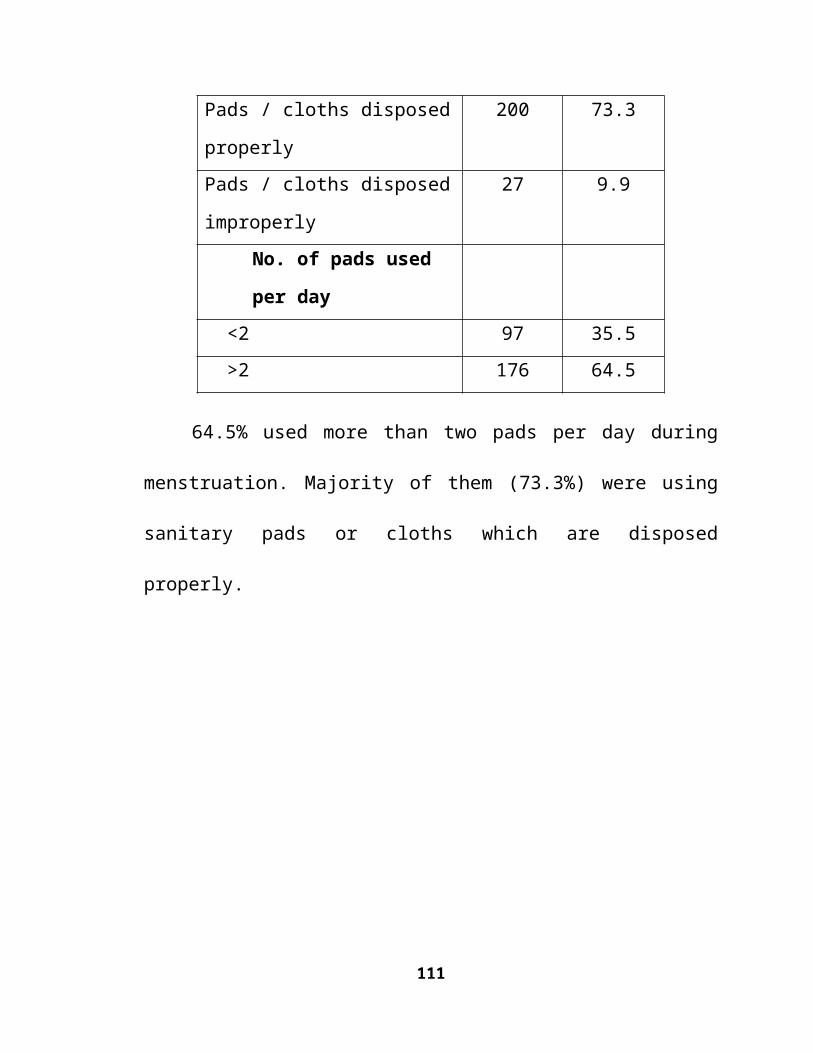
Bibliography
1. WHO. Adolescent Nutrition: A Review of the Situation in Selected
South-East Asian Countries, 2006.
2. WHO. The reproductive health of adolescents: A strategy for action, A
joint WHO/ UNFPA/ UNICEF statement, 1989.
3. USAID. Adolescent and youth reproductive health in India, status,
issues, policies and programs: policy project.
4. Govt of AndhraPradesh.2003. Declaring the year 2003 as the year of
the adolescent girl. Department of women development and child
welfare, Government of Andhra Pradesh.
5. Introduction of scheduled caste education; f ile:// H :/introduction of sc
educ.htm (Accessed on 21-10-08).
6. Registrar general and census commissioner. 2001. Scheduled castes and
scheduled tribe’s population census – India, 2001.
7. Srinivasan K., Prabhu.G.R. A study of the morbidity status of the
children in social welfare hostels in Tirupati town, Indian Journal of
Community Medicine, 2006; 31(3):25-30.
8. WHO. Action for Adolescent Health: Towards a Common Agenda,
Recommendations from a joint Study Group.WHO,UNFPA,
UNICEF1997.
111
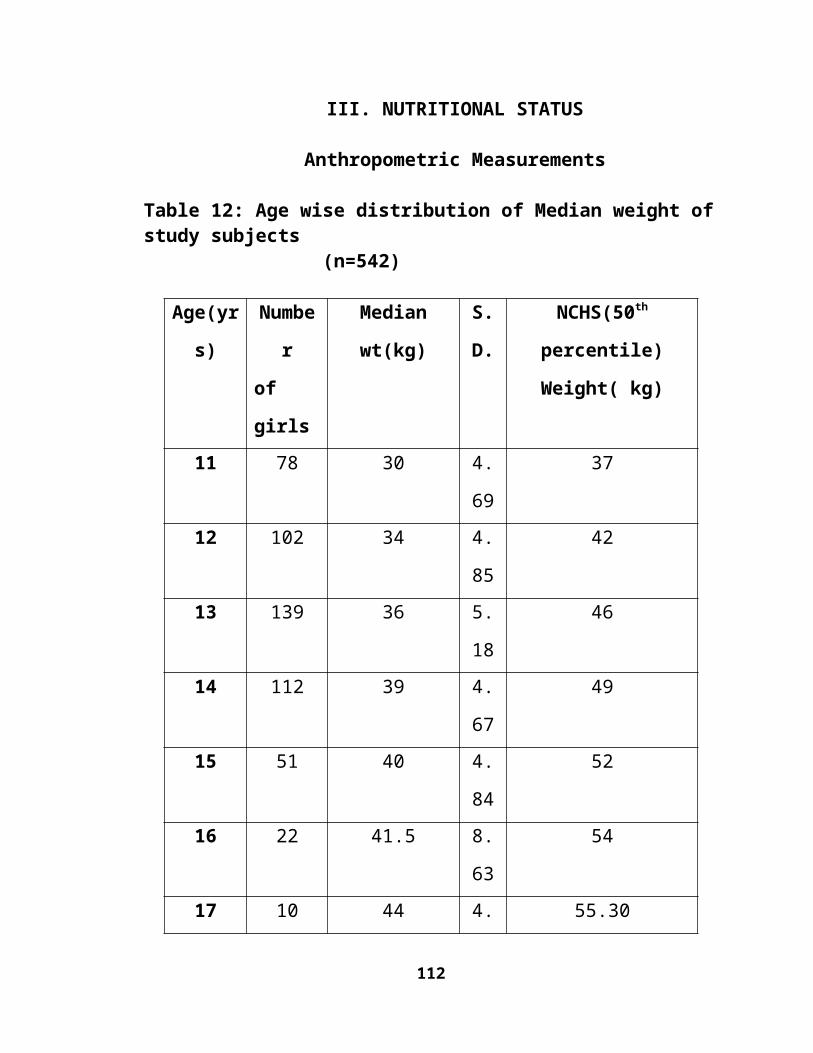
9. WHO. Adolescent Friendly Health Services – An Agenda for Change;
2002.
10.Sunderlal, Adarsh, Pankaj. Textbook of community medicine. 1st
edition, CBS publishers and distributors, New Delhi, 2007, 128.
11.WHO.Nutrition in adolescence: Issues and challenges for the health
sector: Issues in adolescent health and development, 2005.
12.Kishore. J. National Health Programs of India, National Policies and
Legislation Related to Health. 8th edition, Century publications; 2009,
162.
13.Anant Kumar, Poverty and adolescent girl health: A passage
toBihar.TheBihartimes;www.bihartimes.com/Poverty/anant_
pandey.html (Accessed on 2-12-08).
14.Social exclusion of scheduled caste children from primary education in
India, Draft. New Delhi, India: UNICEF; 2006.
15.Lakhan Singh. Deprivation of India’s Scheduled Caste Children from
primary education: Evidence from NFHS-3.
http://iussP2009.princeton.edu/download. (Accessed on 24-12-08)
16.National portal of India: Education of scheduled caste and
scheduledtribes:http://india.gov.in/sectors/transport/index.php.
(Accessed on 24-12-08).
112
17.Government of Andhra Pradesh. Department of Social
welfare,Hyderabad.http://apsocialwelfare.apgov.in/sc_st
commission.asp (Accessed on 25-12-08).
18.Department Of Social Welfare: Commissionerate of Social Welfare:G:\
downloads\APonlineorganisation_schostels.2.mht. (Accessed on 25-12-
08).
19.Singh.J, Singh.V, Srivastava.A.K, Suryakant. Health status of
adolescent girls in slums of Lucknow – Indian Journal of Community
Medicine.2006, 31(2):11-15.
20.Panda P. Benjamin. Health status of school children in Ludhiana city –
Indian Journal of Community Medicine.2000, 25(4):150-155.
21. Kalamka.H.S, Study of health problems of adolescent in urban field
practice area. A thesis submitted for the Degree of Doctor of Medicine
(M.D), Nagpur University, Nagpur, 2001.
22.Balasubramanian P. Health Needs of Poor Unmarried Adolescent Girls:
A Community-Based Study in Rural Tamil Nadu, Indian Journal of
Population Education, 2005, March-June: 18-33.
23.Agrawal.M, Ghildyal.R, Khopkar.S. Health status of school girls from
affluent population of Mumbai. Indian Journal of Pediatrics. 1999, 36:
75-78
113
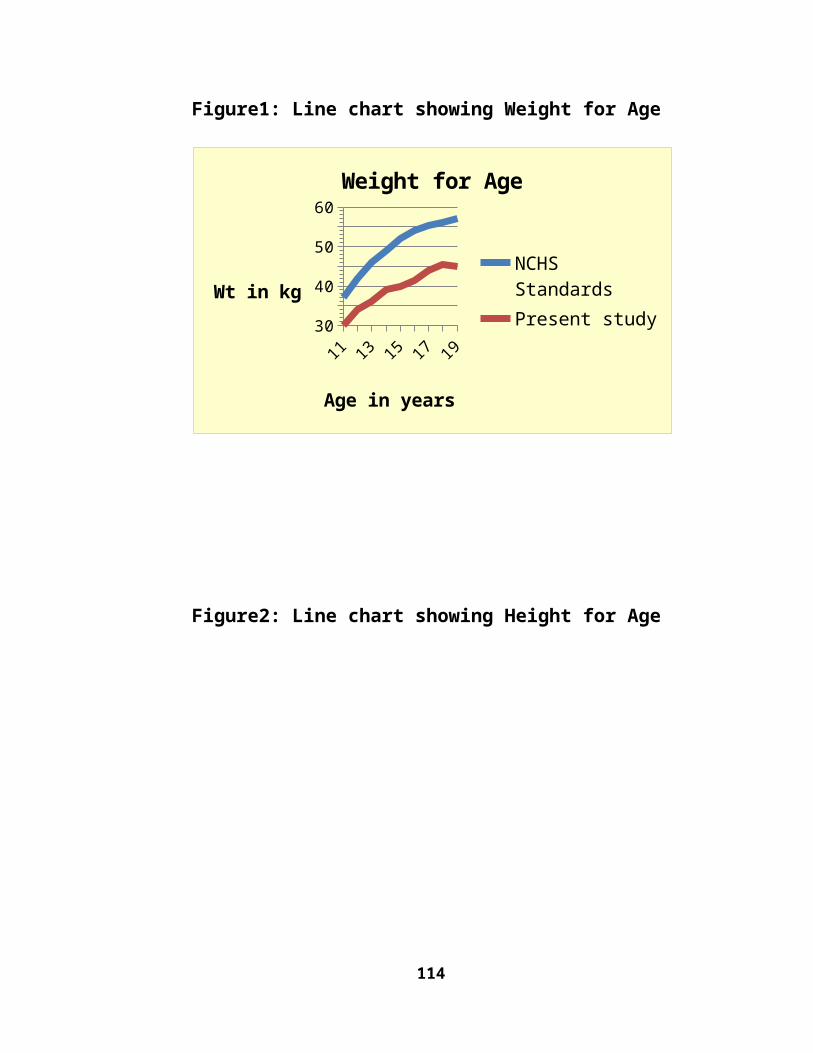
24.Geetha.A, Sara Bhattarcharji, Abraham Joseph, Rao.P.S.S. General and
reproductive health of adolescent girls in rural south India. Indian
Journal of Pediatrics. 1997, March, 34; 242-245.
25.Gosh.B.N. Dhikpathy. Morbidity pattern of the south Indian
adolescents. Indian Journal of Pediatrics. 1966, June. 33:.221.
26.Arunachopdar, Mishra P.K. Health status of rural school children in
Western Orissa. Indian Journal of Pediatrics. May 1980, 47(3): 203-
206.
27.Bhaskara Rao Busi, Dharmarao.B. Rao.V.L.N. Girija Vani.D.S.
Himabindu.D. Growth progression in physical and physiological
variables among Relli's: A scheduled caste of Andhra Pradesh. Man in
India ISSN 0025-1569. 2003, 83: 89-107.
28.Goel.S. Gupta.B.P. Low Anaemia Prevalence among Adolescents of an
Urban Hilly Community. Indian Journal of Community Medicine.
2007, 32(1).
29.Medhi.G.K. Hazarika.N.C. Mahanta.J. Nutritional status of adolescents
among tea garden workers – Indian Journal of Pediatrics. 2007 April,
74:343-347.
114
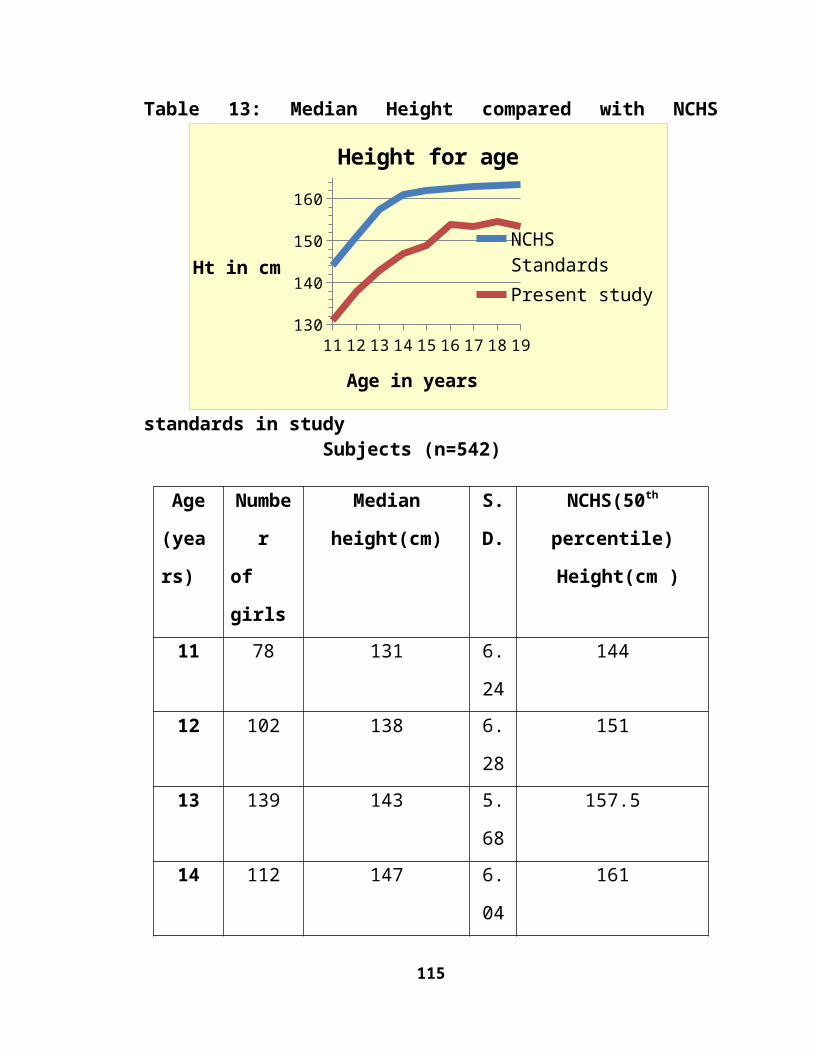
30.Deshmukh.P.R.Guptha.S.S.Bharambe.M.S.Dongre.A.R. Maliye.C.
Kaur.S. et al.. Nutritional status of adolescents in rural Wardha. Indian
Journal of Pediatrics. 2006 Feb, 73: 139-141.
31.Diet and nutritional status of adolescent: NNMB, 20th Report, NIN
ICMR Hyderabad 2000; 20: 1-25.
32.Choudhary.S. Mishra.C.P. Shukla.K.P. Nutritional status of adolescent
girls in rural area of Varanasi. Indian Journal of Preventive and Social
Medicine, 2003:34 (1): 54-61.
33.Diet and nutritional status of tribal population. Report on first repeat
survey (NNMB) Hyderabad: National Institute of Nutrition; 2000.
34.Marwaha.R.K. Tandon.N. Singh.Y. Aggrawal.R. Grewal.K. Mani.K. A
Study of Growth Parameters and Prevalence of Overweight and Obesity
in School Children from Delhi. Indian Journal of Pediatrics, November
2006: 43(11):943-952.
35.Prevention and Control of Anemia in Rural Adolescent Girls through
School System. Annual Report, AndhraPradesh .Indian Institute of
Health and Family Welfare; 2001-2002.
36.Rawat.C.M.S. Garg.S.K. Singh.J.V. Bhatnagar.M. Socio Demographic
Correlates of Anemia among Adolescent Girls in Rural Areas of
115
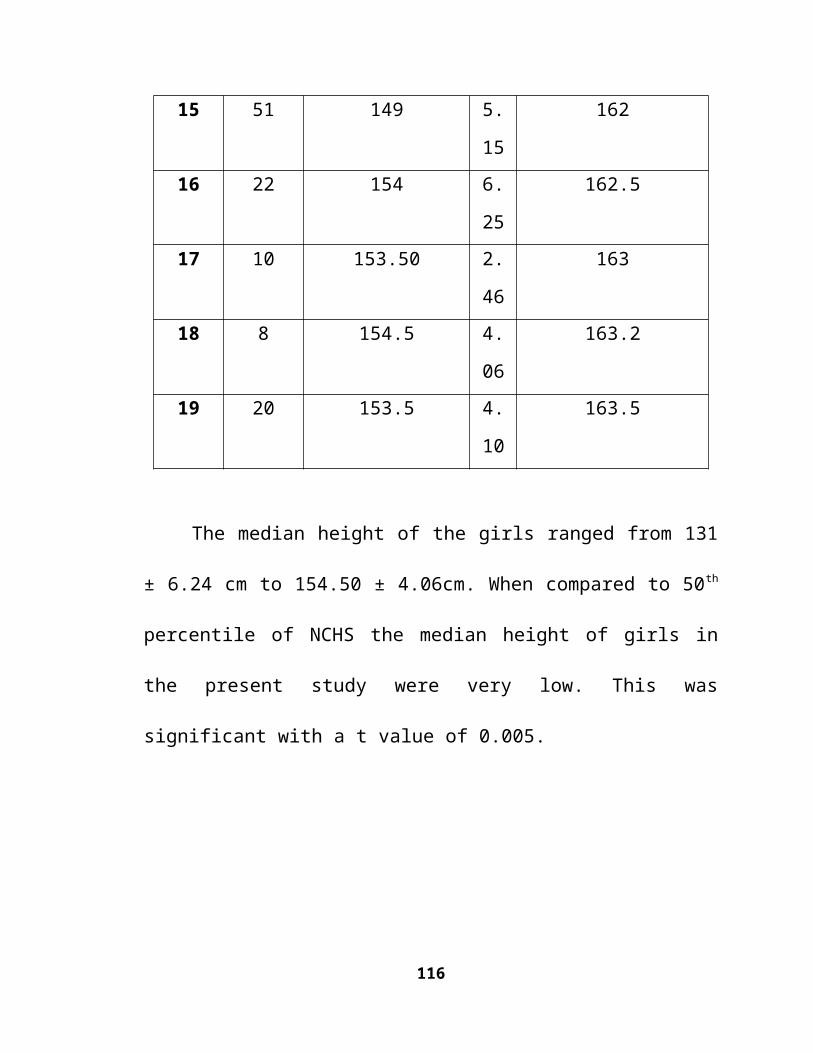
District Meerut (UP) Indian Journal of Community Medicine, 2001
October-December; 25(4): 173-175.
37.Shahnaz Khan, Aarti Sankhla.P.K. Dashora. Nutritional Adequacy of
Boys in Orphanages Indian Journal of Pediatrics, March 1996:33: 226-
228.
38.Micronutrient Deficiency Disorders in 16 Districts of India – Part 1
Report of an ICMR Task Force Study: District Nutrition Project, 2001.
39.Verma.A. Rawal.V.S. Kedia.G. Kumar.D. Chauhan.J. Factors
Influencing Anemia among Girls of School Going Age (6-18 years)
from the Slums of Ahmadabad City. Indian Journal of Community
Medicine, 2004 January – March. 29(1): 25-26.
40.Kathleen M. Kurz. Adolescent Nutritional status in developing
countries. Proceedings of nutrition society. 1996; 55: 321-331.
41.Dilp kumar Das, Ranadeb Biswas. Nutritional status of adolescent girls
in a rural area of North 24 Paraganas District, W.Bengal. Indian Journal
of Public Health, Jan-Mar 2005, 49(1):18-21.
42.Pooja Trivedi , Aruna Palta . Prevalence of anemia and impact of Iron
supplementation on anemic adolescent school girls. Health and
population. Perspectives and issues: 2007, 30(1)45-55.
116
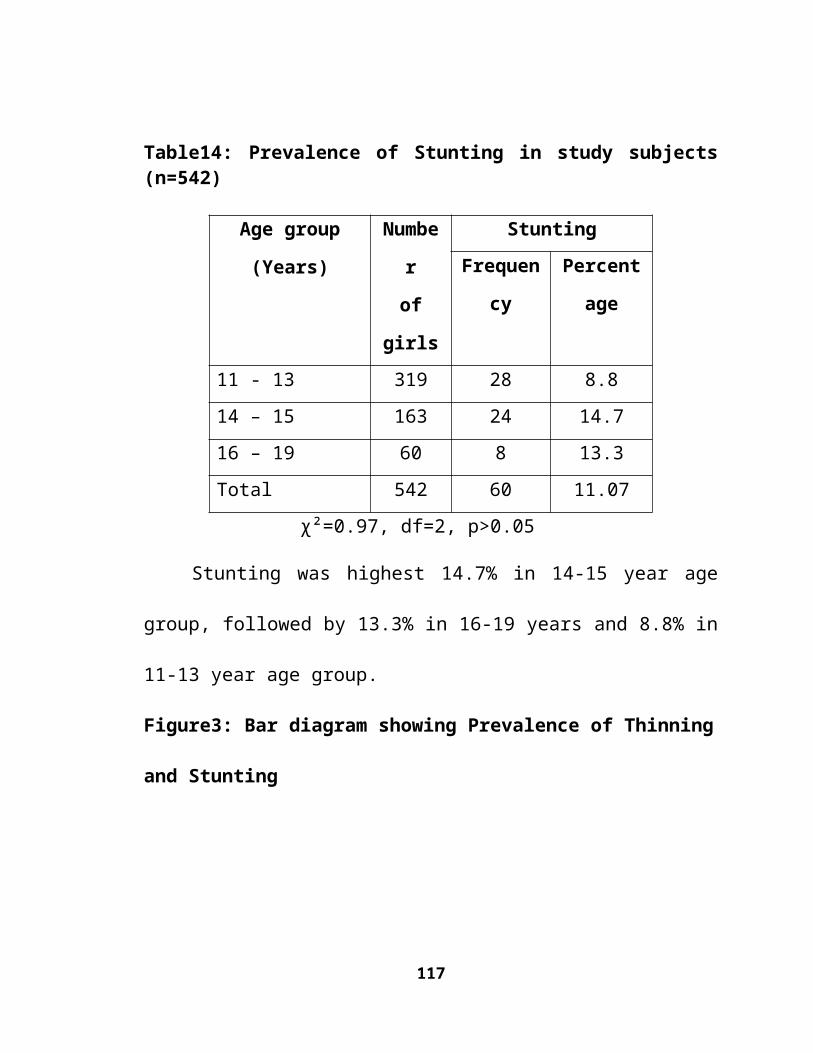
43.Kapoor.G. Aneja.S. Nutritional disorders in adolescent girls. Indian
Journal of Pediatrics, August 1992, 29:969-973.
44.Chief planning officer Nellore. Hand book of statistics. 2007-2008. P1
45.Bodysizemeasurementprocedures.www.cardia.dopm.uab.edu/pdf D
10689. (Accessed on 20-9-08).
46.Mohan.V. Deepa.R. Obesity and abdominal obesity in Asian Indians,
Indian Journal of Medical Research 2006 May, 123: 593-596.
47.Tim J Col, Katherine M Flegal, Dasha Nicholis, Alan A Jacson. BMI
cut offs to define thinness in children and adolescents: International
survey; BMJ 2007; 335(7612): 194, doi:10.1136/bmj.39238.399444.55
48.Physical status: the use and interpretation of anthropometry. Technical
report series. Report no: 854. Geneva: WHO, 1995.
49.Gopalan.C. Ramasastri. B.V. Balasubramanian .S.C.Narasinga
Rao .B.S. Deosthale .Y.G. Pant .K.C. Nutritive Value of Indian
Foods.1st ed.NIN, ICMR, Hyderabad; 2004.
50.Klaus kraemer, Michael Zimmermann.B. Nutritional anaemia. Sight
and life press, Switzerland, 2007, 47.
51.Behera T.R., Satapathy, D.M. Sahani, N.C. and Sahu.T. Nutritional
deficiency status among tribal children in a hard to reach area of
117
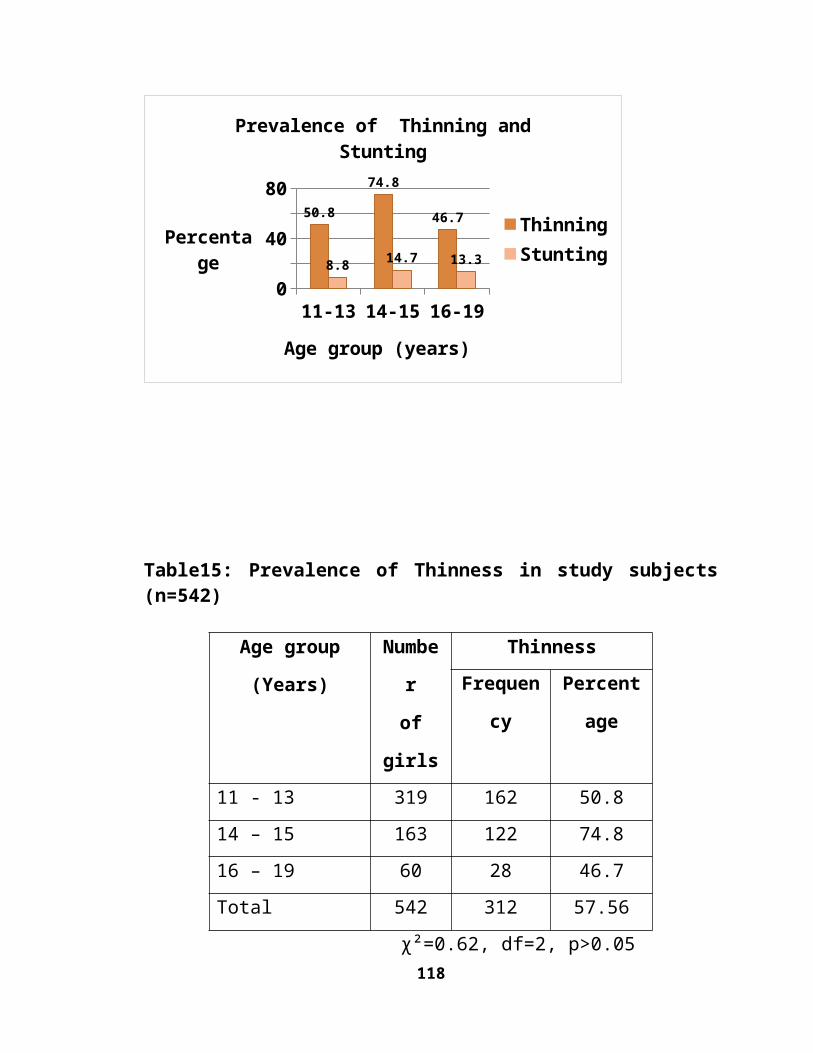
Malkangiri Dist in Orissa, Indian journal of nutrition and dietetics,
2009:46:106-111.
52.Deepali Deo.S. And Ghattargi.C.H. Menstrual problems in Adolescent
school girls: A comparative study in urban and rural area, Indian
Journal of Preventive and Social Medicine, 2007: 38(1):64-66.
53.National Centre for Health Statistics: CDC growth charts. United
States: National Centre for Chronic Disease Prevention and Health
Promotion; 2000.
54.Varsha zanvar, Rohini Devi, Asha Arya, Nerlekar. Prevalence of
anaemia among selected Adolescent girls of Marathwada region. Indian
Journal of Nutrition and Dietetics, 2007: 44: 559-571.
55.Lt Col Benarjee.A. Height and Weight patterns as indicators of growth
among school children in an air force station: A cross-sectional study.
Medical Journal Armed Forces India. 2001: 57(1).
56.Raheena Begum.M. Prevalence of malnutrition among adolescent girls:
A case study in Kalliyoor panchayat, Thiruvananthapuram. Kerala
research programme on local level development; centre for
development studies. 2001.
118
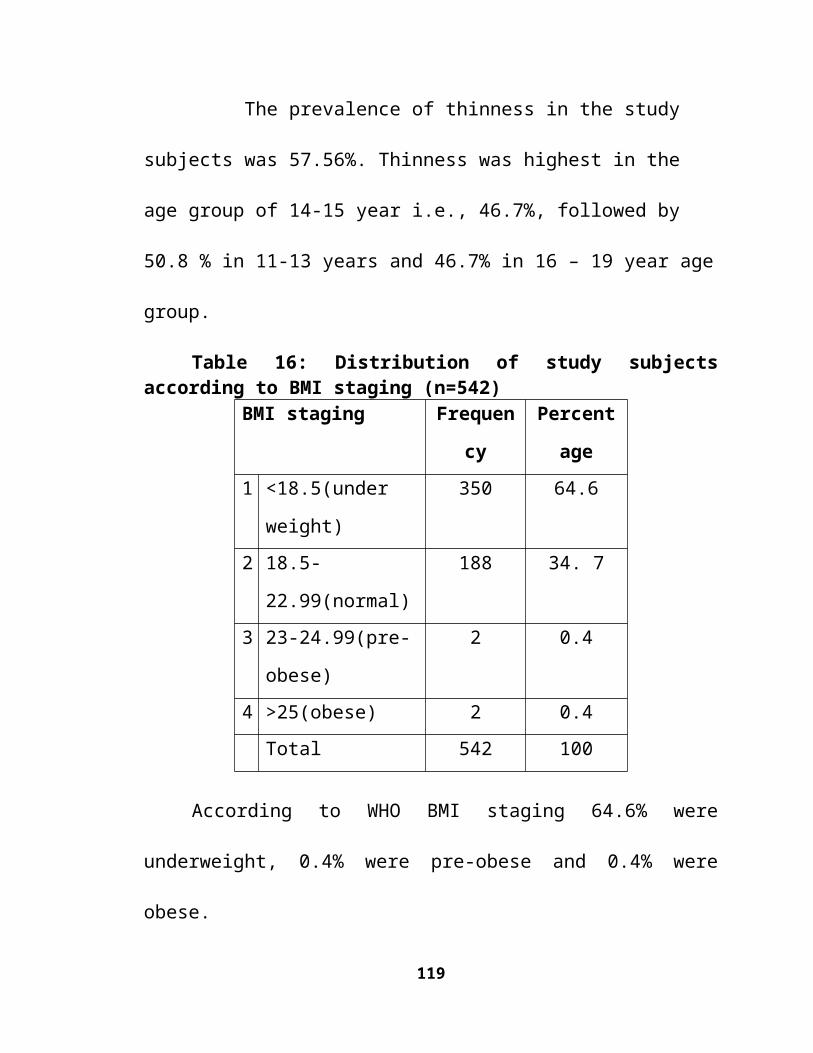
57.Ashish Mukhopadhyay, Meethu Bhadra and Kaushik Bose.
Anthropometric Assessment of Nutritional Status of Adolescents of
Kolkata, West Bengal –– J.Hum.Ecol. 2005, 18(3):213-216.
58.Patil.S.N. Wasnik.V. Wadke.R. Health problems among adolescent
girls in rural areas of Rathnagiri District of Maharashtra, India. Journal
of Clinical and Diagnostic Research. 2009, 3(5): 1784-1790.
59.Swapnachathurvedi, Kapil.U. Gnanasekharan.N. Sachdev.H.P.S.
Pandey.R.M. Bhanti.T. Nutrient intake amongst Adolescent girls
belonging to poor socioeconomic group of rural area of Rajasthan.
Indian Journal of pediatrics. 1996 March: 33(3):197-201.
60.http://164.100.24.208/ls/committeeR/EMPOWERMENT/10rep.pdf
(Accessed on 10-1-2009).
61.Dubey.S.N. Murdia.R. Administration of policy and programmes for
backward classes in India. Soumya publications private limited. 1976,
53, 204-215.
62.Rajashree.S. Soman.R. Nutritional status of school children in kerala.
Indian Journal of pediatrics.1996:31:651-655.
119
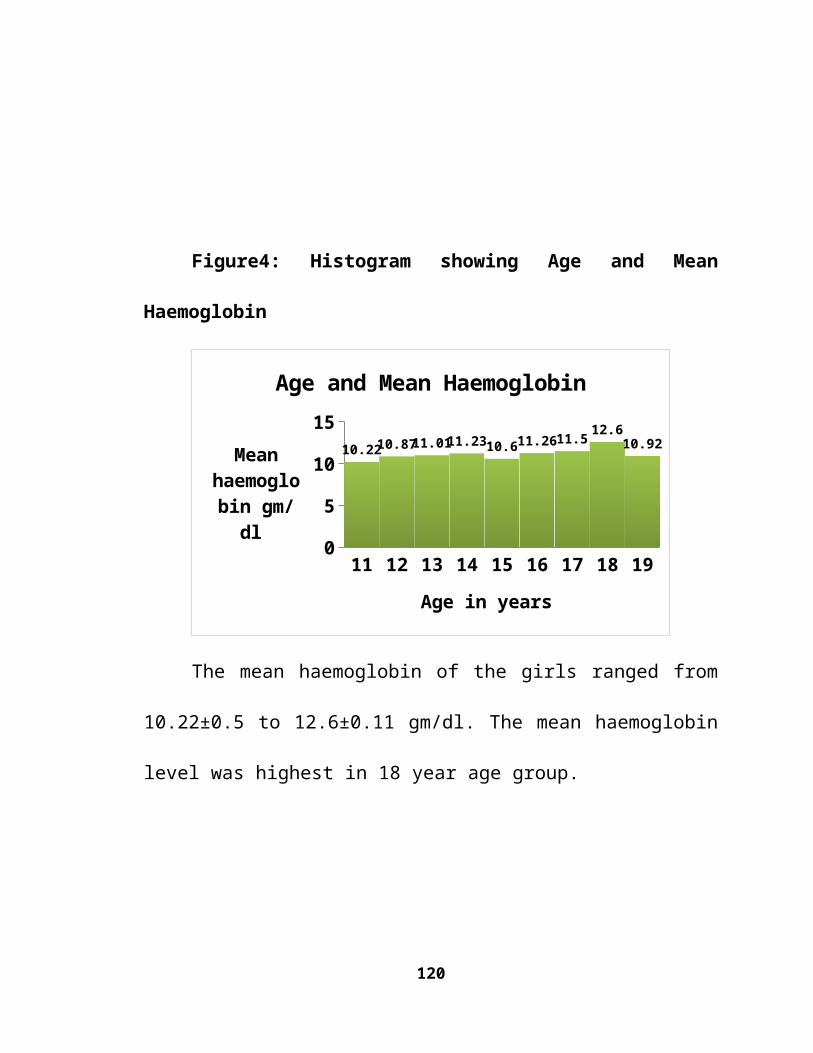
ANNEXURES
120
ANNEXURE – I
A STUDY ON THE HEALTH STATUS OF ADOLESCENT GIRLS RESIDING IN SOCIAL WELFARE HOSTELS OF NELLORE CITY, A.P.
1. SOCIO DEMOGRAPHIC DATA.1. S.no:2. Name of the hostel: 3. Name of the student: 4. Class:5. Age in years :6. Residential address7. Duration of stay in the hostel(years, months)8. Type of family : nuclear / joint / extended9. Total number of family members: 10.No of brothers : No of sisters:11.Occupation of father : farmer / labourer / service / others 12.Literacy status of father : illiterate/ school educated / college educated13.Occupation of mother : homemaker / labourer / service / others 14.Literacy status of mother : illiterate/school educated / college educated
II.PHYSICAL EXAMINATION :15.Anthropometry : Ht(cms): Wt(kgs): BMI(kg/m²):16.pulse rate : 18. BP:
III.GENERAL EXAMINATION :19.Built – Thin /normal 20.Pallor,Icterus,Clubbing,Kyphosis,Lymphadenopathy,Edema - 21. Eye vision – refractive errors – present / absent
22. Signs of vitamin deficiency: 23. ENT disorders: 24.Congenital abnormalities: present/absent
25.BCG scar : present/absent26.Habits and Behavioural problems if any :
121
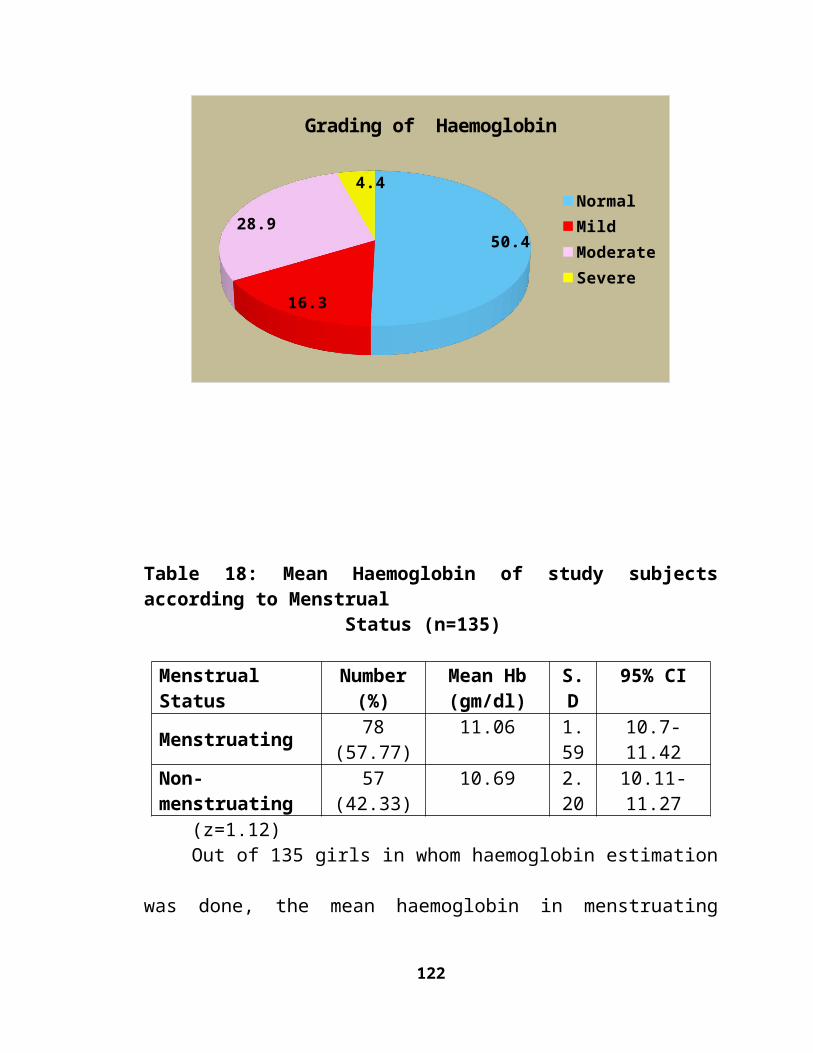
IV. SYSTEMIC EXAMINATION:27.CVS:28.RESPIRATORY SYSTEM:29.PER ABDOMEN:30.CNS:
V.INVESTIGATIONS: 31. Haemoglobin (gm/dl): 32. H/O Passing worms in the stools: present /absent
VI. PERSONAL HYGIENE:33. Hair: dull and lusterless /healthy/clean and groomed/louse infested34. Oral hygiene: brushing teeth daily-once/twice34. Gums: normal / inflammation / bleeding / ulcers /others 35. Teeth: normal / caries / mottling / others 36. Nose: normal / nasal discharge / epistaxis / others 37. Bathing daily – once / twice 38. Nails: trimmed / filled with dirt 39. Washing hands with soap and water: Before eating – yes /no
After defecation – yes / no 40. Skin: normal/scabies/ pyoderma / ulcers / patches / others 41. Clothes – clean and tidy – yes / no; change daily – yes / no 42. Wearing foot wear: yes / no
VII. REPRODUCTIVE HEALTH 43. Age at menarche:44. Menstrual cycle: regular / irregular 45. Bleeding during menstruation (days) : <3 / 3-5 / 6-7 / >7 46. Dysmenorrhoea: never / occasionally / frequently / always 47. Periods more than once a month: yes / no 48. White discharge per vaginum: never / occasionally / frequently /
always49. Breast pain during menstruation: never / occasionally / frequently /
always
122
50. Pre-menstrual tension during menstruation: never /occasionally/ frequently/always Menstrual hygiene:
51. Material used during menstruation: sanitary pads / new cloth / old cloth / all 52. No. of pads used per day: 53. Method of disposal: cloth pieces reused / sanitary pads or clothes disposed properly
VIII . HEALTH STATUS 54. Health status of the students – normal / sick 55. Any illness during the last two weeks:
H/O Diarrohea – present / absent H/O ARI – present / absent H/O Pyrexia present / absent H/O Dermatitis, scabies - present / absent
56. Mode of treatment of this student – Govt.hospital / Pvt.hospital / NGO / Home Medication.
123
ANNEXURE – II
SCHEDULE FOR ENVIRONMENT CONDITIONS
Name of the hostel: Date of visit:No. of children in Register:
1. Location of the hostel / distance from the road (mts) - ---------------2. Any source of noise (Traffic) __________________Present / Absent 3. Any source of nuisance ________________Present / Absent 4. Premises of Hostels :
a) Un-necessary vegetation - Present / Absent b) Pools of Water / Ditches - Present / Absent c) Kept clean - Yes / No
5. Compound wall - Present / Absent 6. No. of living rooms available in the hostel ___________________ 7. No. of students per each room _________________ 8. Floor Area per student ______________ 9. Ventilation of rooms - Good / Bad 10. No. of windows in each room ________________ 11. Measurements of windows __________________ 12. Tube lights / Bulbs - Present / Absent 13. Lighting - Sufficient / Non Sufficient 14. Verandah - Present / Absent 15. Furniture - Provided / Not Provided 16. Nature of Furniture - 17. Drinking water supply a) Source of water - Sanitary well / piped water supply / Well maintained hand pump . b) Nature of storage of water _______________________ c) Method of drawing water-Taps / ladles- provided/Not Provided 18. Toilets provided - Yes / No 19. No. of latrines provided ___________ 20. Maintenance of toilets - Good / Bad 21. Urinals Provided - Yes / No 22. No. of urinals provided - ---------------------
124
23. Maintenance of urinals - Good / Bad 24. No. of bathrooms provided - ---------------------- 25. Maintenance of bathrooms - Good / Bad 26. Disposal of refuse (Description of methods of collection and disposal)
a) Pits with in the premises b) Thrown outside the hostel c) Collected and burnt d) Municipal services to collect e) Others specify
27. Disposal of garbage ______________28. Disposal of waste water _______________29. Mosquito / fly breeding if any - Yes / No 30. White washing of the walls _____________________31. Kitchen a) Structural condition Good / Bad b) Kept clean Yes / No c) Rodent infestation of kitchen Present / Absent d) Dimensions of Kitchen _________________ e) Ventilators Provided / Not Provided f) Lighting Sufficient / Not Sufficient g) Smoke outlet facility provided / not provided 32. Storage of food grains – separate room - Present / Absent 33. Dining Hall – provided/not provided . 34. Utensils - Steel / Brass / German Silver / Aluminium. 35. Washing method of vessels ____________________ 36. If brass vessel present - Tinned / Not Tinned 37. No. of chairs and tablets in dining hall ___________________ 38. Food handler’s hygiene a) Personal hygiene - Good / Bad b) History of passing of worms in stools -Yes / No c) Soap and Towel provided separately-Yes / No
125
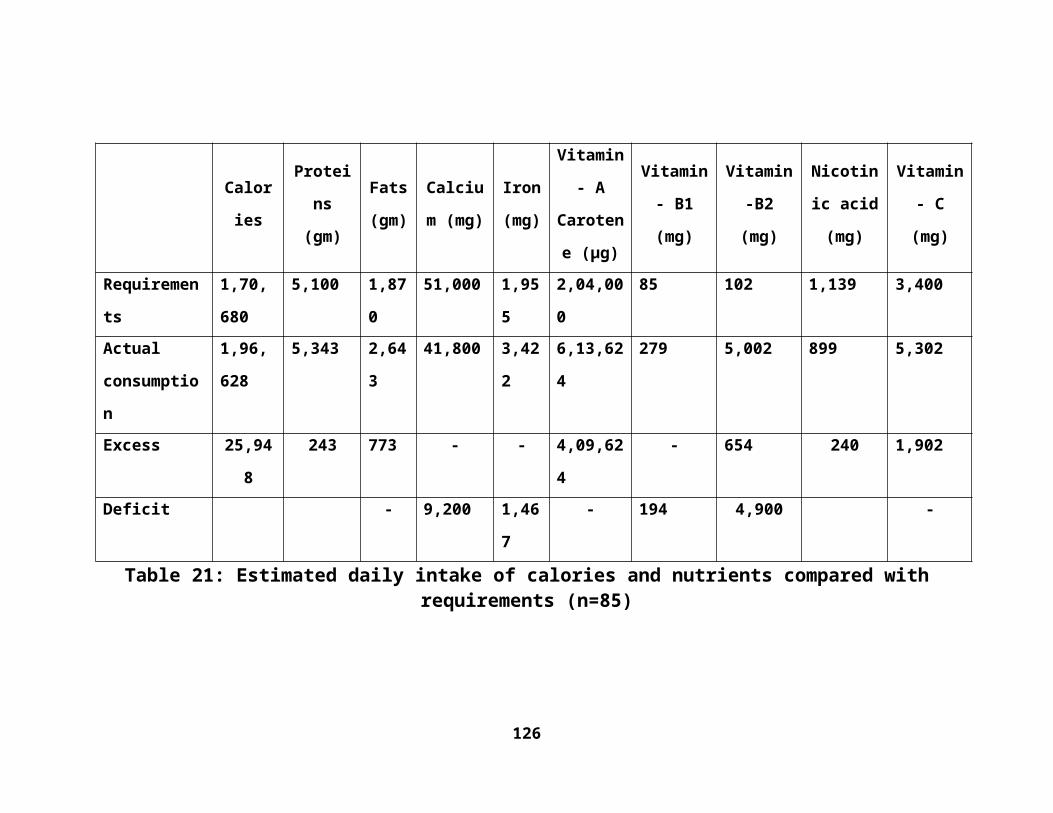
ANNEXURE-III
OPERATIONAL DEFINITIONS USED IN THIS STUDY
Socio Demographic Factors
Illiterate - Who cannot read and write in any language were labelled as illiterate.
School educated –Subject’s education from 1st to 10th class.
College educated- Subject’s education above 10th class including post graduation,
professional.
Middle school - Subjects studying class 6-7.
High school - Subjects studying class 8-10.
Type of Family
a) Nuclear: A married couple and their children while they are still regarded as
dependent.
b) Joint family: Number of married couples and their children who live
together in the same household.
c) Three generation: This tends to be a household with representatives of
three generations.
Menstrual pattern
Menstrual cycle – Regular- subject’s having 28-30 day cycle.
Irregular - subject’s having any deviation from 28-30 day cycle.
Dysmenorrhea - the occurrence of painful cramps during menstruation.
Frequently - >5 times in one year.
Occasionally -<5 times in one year.
Always - on every menstrual cycle.
Morbidity profile
126
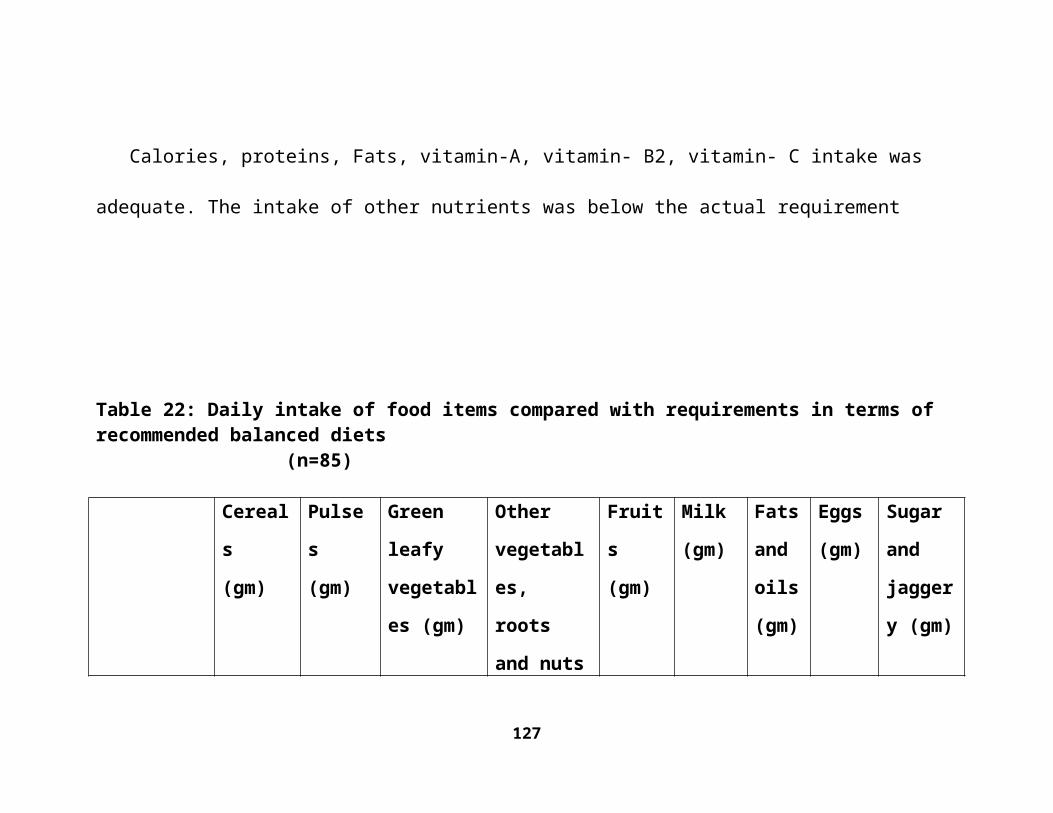
Current Morbidity status- Any morbidity present at the time of examination by
the investigator.
Fever-A body temperature (oral) that is higher than normal (98.4ºF) recorded by
mercury thermometer.
Exanthematous fever – Fever accompanied by different types of rash.
Scabies- A contagious skin disease caused by a parasitic mite (Sarcoptes scabiei)
and characterized by intense itching.
Pediculosis - An infestation with head louse.
Hygiene- Refers to practices associated with ensuring good health and cleanliness.
Poor personal hygiene- Refers to practices associated with: hair with lost luster,
nails not trimmed and filled with dirt, brushing teeth only once daily, teeth with
caries/mottling, swollen, inflamed / bleeding gums, skin with diseases, clothes not
changed after bath, not bathing daily, not wearing foot wear etc.
Vitamin deficiency- Is any disease caused by chronic or long-term vitamin
deficiency or caused by a defect in metabolic conversion with clinical features of
angular stomatitis, cheilosis, bitots spots, bleeding gums etc.
Defective vision - WHO criteria of visual acuity ≤6/18 in better eye detected by
Snellen chart is taken as defective vision,
Pallor - Paleness of mucosal membranes, conjunctiva, palms.
Method of haemoglobin estimation-Sahli’s haemoglobinometer
Principle- Amount of Hb can be estimated by conversion of known volume of
blood in to acid haematin by addition of dilute Hcl and subsequent calorimetric
comparison with a suitable standard.
127
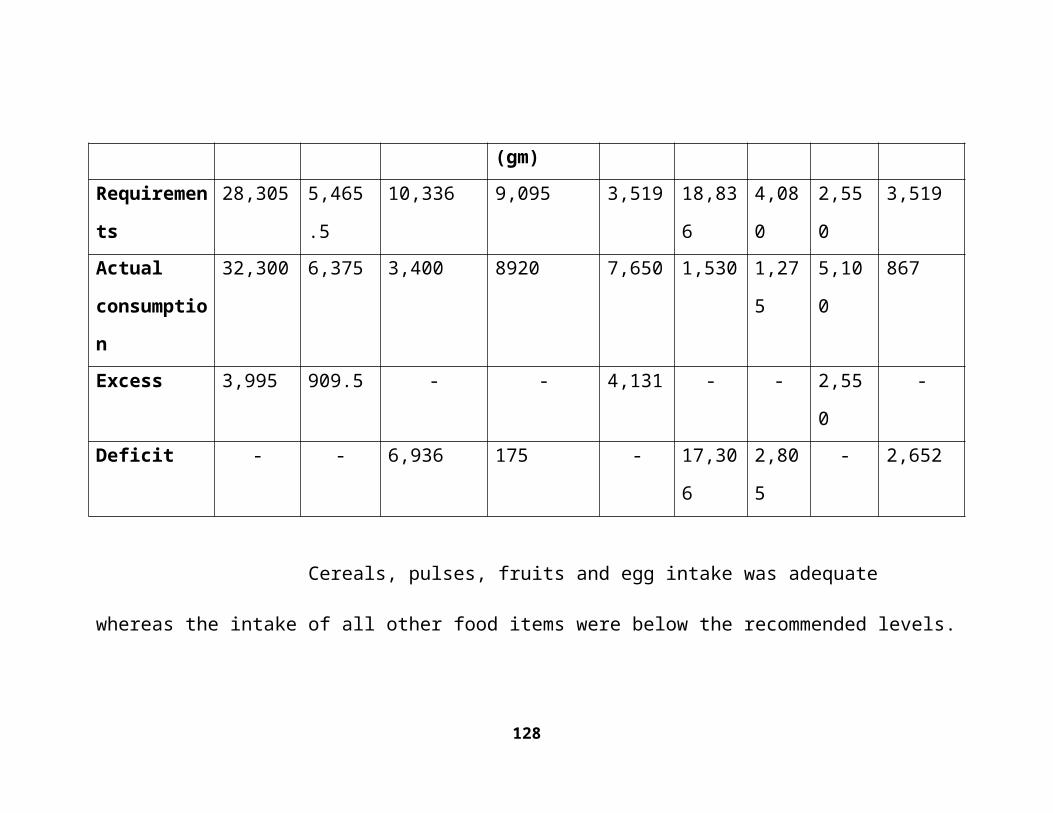
128





























