Embed Size (px)
Citation preview

A study on etiology and risk factorsassociated with fatal outcome of childhoodpneumonia in the Philippines from 2008 to 2016
著者 Bindongo Price Polycarpe Dembele学位授与機関 Tohoku University学位授与番号 11301甲第18541号URL http://hdl.handle.net/10097/00126062

PhD Dissertation
博士論文
A study on etiology and risk factors associated with fatal outcome of
childhood pneumonia in the Philippines from 2008 to 2016
( 2008年から 2016年までのフィリピンにおける小児肺炎の死亡転帰に関連する病因および
危険因子に関する研究)
Tohoku University Graduate School of Medicine
東北大学大学院医学系研究科
Disaster Medical Science Division
災害医学研究部門
Department of International Cooperation for Disaster Medicine
災害医療国際協力学分野
Dembele Bindongo Price Polycarpe
ビンドンゴ プリス ポリカープ ダンビリ

Table of contents
1. Summary:………………………………………………………………..1
2. Abbreviations:……………………………………………………………4
3. Introduction :……………………………………………………………6
4. Objectives:……………………………………………………………….9
5. Materials and methods: ………………………………………………..10
5.1 Study designs ……………………………………………………….10
5.2 Study sites…………………………………………………………...10
5.3 Study patients………………………………………………………11
5.4 Collection of patient information…………………...………………...….12
5.5 Assessment of chest X-ray………………………………………….14
5.6 Detection of viruses………………………………………………....14
5.7 Detection of bacteria …………………………………………….…16
5.8 Data analysis………………………………………………………..17
5.9 Ethical considerations………………………………………………19
6. Results ………………………………………………………………….19
6.1 Demographic, clinical and radiographic findings………………...20
6.2 Pathogens detected………………………………………………….23
6 2 1 Viruses detected from nasopharyngeal swabs………………….23
6. 2 2 Bacteria detection in blood………………………………………24
6 3 Factors associated with deaths…………………………………….25
6 3 1 Univariate logistic regression analysis of factors associated with
death…………………………………...………………………………..25
6 3 2 Multivariate logistic regression analysis of factors associated
with death…………………………………………………………….…26
6 3 3 Multivariate logistic regression analysis of factors associated
with deaths tested positive for different pathogens......................…...26
7. Discussion………………………………………………………….……27
8. Conclusion………………………………………………………………37
References……………………………………………………………….38
List of Tables of Figures
Figure 1: Map depicting the location of study sites participating in the
childhood pneumonia study in the Philippines, 2008-
2016…………….......................................................................................46
Figure 2: Periods of study according to different hospitals……….……47
Figure 3: Flowchart of the selection of eligible study participants in the
childhood pneumonia study in Philippines, from 2008- 2016...................48
Table 1:Yearly Distribution of Children with Severe Pneumonia Stratified
According to the Hospital and Outcome……………………...49
Table 2: Demographic, Socio-economic and Environmental
Characteristics of Children hospitalised with Severe Pneumonia, Stratified
by Age Group and Outcome………………………………………...…...50
Table 3 : Clinical and Laboratory Findings of Children hospitalised with
Severe Pneumonia, Stratified by Age Group and Outcome……………. 52
Table 4: Factors Associated With Death Among Children hospitalised
With Severe Pneumonia, Stratified By Age Group……………………...54
Table 5: Pathogen Detected And Clinical Outcome In <2months Old
Children hospitalised With Pneumonia, Philippines, 2008 to 2016.…55

Table 6: Pathogen Detected And Clinical Outcome In Children 2−59
Months Old Children hospitalised With Pneumonia, Philippines, 2008-
2016……………………………………………………………………...56
Table 7: Clinical Signs and Symptoms Associated With Death among
Less 59 Months Old Children hospitalised With Pneumonia and Tested
Positive for Different Pathogens, Philippines, 2008-2016…………….57
Table 8: Demographic Characteristics Of Children hospitalised With
Severe Pneumonia, Stratified By Age Group And Outcome…………58.
Appendix:
Hospital admission data collection form……………………..…….59

1 | P a g e
1. Summary 1
Pneumonia remains the leading cause of hospitalizations and deaths in children 2
<5 years. A variety of respiratory pathogens cause acute respiratory infections 3
including pneumonia. However, their associations with death are still not well 4
defined. I analyzed viral and bacterial pathogens and other risk factors associated 5
with fatal outcomes among children hospitalised in the Philippines. 6
Children aged <5 years with a clinical diagnosis of severe pneumonia were 7
recruited in four hospitals in the Philippines from 2008-2016. Nasopharyngeal 8
swabs were collected for virus identification by polymerase chain reaction 9
(PCR), and venous blood samples were collected for bacterial culture. 10
Demographic information, clinical data, and laboratory findings were also 11
collected at the admission. Univariate and multivariate logistic regression 12
analyses were performed to identify the factors associated with death. 13
A total of 5,054 pneumonia cases were recruited, and 68.9% of them were aged 14
less than one year, 55% of death cases were malnourished, and 13% were 15
hypoxemic (SpO2 <90%). Children aged <24 months accounted for 87.0% of the 16

2 | P a g e
fatal cases with the age group of 2-5 months having the highest CFR of 7.0%. A 17
significant decreasing trend of CFR was observed during the 9-year study period 18
with the highest CFR of 12.5% in 2008 and the lowest CFR of 2.0% in 2013 (p 19
<0.001). At least one virus was detected in 61.0% cases; respiratory syncytial 20
virus (RSV) (27.0%) and rhinovirus (RV) (23.0 %) were the most common 21
viruses. In children aged 2-59 months, risk factors significantly associated with 22
death included sensorial changes, severe malnutrition, grunting, central cyanosis, 23
decreased breath sounds, tachypnea, wheeze, fever (≥ 38.5°C), SpO2<90%, 24
infiltration, consolidation and pleural effusion on chest radiograph. Among 25
pathogens, adenovirus (ADV), particularly ADV-7, seasonal influenza A (H1N1) 26
and blood culture positive for invasive bacteria were significantly associated with 27
deaths, while RSV (AOR: 95% CI 0.31;0.19-0.5) and RV (AOR: 95% CI 0.99; 28
0.68-1.41) were not associated with death. Similar patterns were observed 29
between death cases and these aforementioned factors in children <2 months. 30
Hypoxemia was associated with death in RSV, RV, enteroviruses positive 31
patients. 32
Malnutrition was the most common factor associated with death and addressing 33

3 | P a g e
this issue may decrease the case fatality rate. Since 13% of patients were 34
hypoxemic, evaluation of hypoxemia by a pulse oximeter should be promoted. 35
Oxygen therapy should be administered in patients with hypoxia, since it appears 36
that hypoxia is one of the driving factors for fatal outcome especially in children 37
with viral infections. In general, viral infections did not increase the risk of fatal 38
outcomes except for ADV and seasonal influenza A (H1N1). Appropriate 39
measures including early detection and early treatment for bacterial pneumonia 40
should be taken considering high CFR among blood culture positive cases. 41
42
Key words: childhood pneumonia; death; association; oxygen; saturation; 43
viruses; bacteria; chest radiograph. 44
45
46
47
48
49
50
4 | P a g e
Abbreviations 51
AOR: adjusted odds ratio. 52
OR: odds ratio. 53
CFR: case fatality rate. 54
ADV: Adenovirus; 55
PCR: Polymerase chain reaction. 56
RT-PCR: Real-time polymerase chain reaction. 57
RSV: Respiratory syncytial virus. 58
RV: Rhinovirus. 59
HMPV: Human Metapneumovirus. 60
PIV: Parainfluenza virus. 61
IFV: Influenza virus. 62
EV: Enterovirus 63
EV-D68: Enterovirus-68 64
LMIC: Low and middle-income countries. 65
WHO: World Health Organization. 66
IMCI: Integrated Management of Childhood Illness. 67
ALRI: Acute lower respiratory infection. 68

5 | P a g e
BPH: Biliran Provincial Hospital. 69
EVRMC: Eastern Visayas Regional Medical Center. 70
ONP: Ospital ng Palawan. 71
RITM: Research Institute for Tropical Medicine. 72
RR: Respiratory rate. 73
SpO2: Blood oxygen saturation. 74
SES: socio-economic status 75
76
77
78
79
80
81

6 | P a g e
3. Introduction 82
Globally, pneumonia accounts for a substantial burden of disease and mortality 83
among children less than 5 years. Around 120 million pneumonia episodes 84
occurred every year, of which 14 million (12%) progress to severe pneumonia1. It 85
is estimated that 5.6 million children died in 2016 before their fifth birthday. 86
Pneumonia accounted for 896,000 of these deaths2 and 81% of them occurred 87
among children aged less than 2 years. Around 99% of childhood pneumonia 88
deaths occur in low and middle-income countries (LMIC) 1. In the Philippines, a 89
community-based study conducted from June 2011 to May 2012 reported 90
incidence rates of pneumonia-like episodes, severe pneumonia-like episodes, and 91
pneumonia-associated deaths were 105, 61 and 0.9 per 1,000 person-years, 92
respectively 3. 93
There are several challenges for tackling childhood pneumonia mortality in 94
resource-limited settings. Risk factors such as poverty 4, household crowding, 95
malnutrition, and solid fuel use for cooking 3 5-7
, and HIV-AIDS mainly in sub-96
Saharan 8 are associated with childhood pneumonia mortality. Despite the high 97
burden of childhood pneumonia, its diagnosis remains difficult and largely based 98

7 | P a g e
on clinical signs and symptoms [9]. Integrated Management of Childhood Illness 99
(IMCI), which was developed by the World Health Organization (WHO) and 100
UNICEF has been widely used for better management of common childhood 101
illnesses including pneumonia in LMIC and was modified in 20149 10
. However, 102
IMCI and other cases definitions use clinical signs and symptoms that are not 103
specific to pneumonia. Several other conditions such as bronchiolitis, measles, 104
and malaria may have similar clinical features11-15
. Determining the etiology of 105
pneumonia is also challenging in the absence reliable laboratories 16
, and lack of 106
access to any form of diagnostic imaging in most of primary care settings in 107
LMIC 17
, although chest radiograph is an important tool for diagnosis of 108
pneumonia. 109
Several groups of pathogens can cause pneumonia. Bacteria are considered to be 110
an important aetiology for childhood pneumonia, and bacterial infections have 111
been shown to be associated with mortality 18 19
. One of the main strategies for 112
pneumonia treatment of IMCI is to treat a patient presenting severe or very 113
severe pneumonia with appropriate antibiotics9 10
. Vaccines against Haemophilus 114
influenzae type b and Streptococcus pneumonia have been introduced in many 115
8 | P a g e
LMIC, which are shown to have reduced morbidity and mortality of childhood 116
pneumonia 2 20-23
, and has decreased the incidence of radiologic pneumonia. 117
24. 118
Viruses are the most common group of pathogens identified from children with 119
acute lower respiratory infection (ALRI) including pneumonia25
. Findings of 120
previous studies, in which conventional virological diagnostic techniques such as 121
virus isolation and immunofluorescence staining were used, are likely to 122
underestimate the role of viruses as a cause of pneumonia 26
. It is known that at 123
least 26 viruses can cause childhood pneumonia 25
and respiratory syncytial virus 124
(RSV) is one of the most common viruses detected from children with ALRI. 125
Most recent estimates on the global burden of RSV indicated that 33.1 million 126
episodes of RSV associated ALRI (RSV-ALRI) with 59,600 in-hospital deaths 127
among children less than five years in 201527
. About 45% of hospital admissions 128
and in-hospital deaths due to RSV-ALRI occur in children younger than 6 129
months. In high-income countries, most deaths associated with RSV occur in 130
children with comorbidities 28 29
. Influenza virus (IFV) infection has also been 131
shown to have a significant impact on children worldwide with estimated 28,000-132
9 | P a g e
111,500 deaths in children younger than five years 30
. Other common viruses 133
identified from ALRI include rhinovirus (RV), human metapneumovirus 134
(HMPV), parainfluenza virus (PIV), and adenovirus (ADV) 31-33
. More recently, 135
enterovirus D68 (EV-D68) was shown to be associated with ALRI 34
. However, 136
the impact of these viral infections on childhood pneumonia mortality in a 137
hospital setting is still not well characterized. 138
Some risk factors and clinical signs including nutritional status1 35
, low 139
birth weight 36
, cyanosis and grunting 37
, and radiological findings such as chest 140
X-ray consolidation 38
are well described as predictors of death in childhood 141
pneumonia. Nonetheless, further reduction of childhood pneumonia mortality 142
requires a better understanding of the association between death and viral 143
infections as well as an update of all factors associated with death in general. 144
3. Objectives 145
The objective of this study was to define the etiological, demographic and 146
environmental factors and clinical findings associated with mortality among 147
children hospitalised with pneumonia in the Philippines. 148
5 .Material and methods 149

10 | P a g e
5.1 Study design: This is a case series study of hospitalised pneumonia cases, 150
which is a part of the large comprehensive epidemiological and etiological study 151
on acute respiratory infections in children. 152
5.2 Study sites 153
Paediatric pneumonia cases were enrolled between May 2008 and March 2016. 154
This study was done in the following 4 hospitals in the Philippines: Biliran 155
Provincial Hospital; Eastern Visayas Regional Medical Center; Ospital ng 156
Palawan; and Research Institute for Tropical Medicine. Biliran Provincial 157
Hospital (BPH) is the main hospital in Biliran Island with 50 pediatrics beds. 158
Eastern Visayas Regional Medical Center (EVRMC) is a tertiary care 159
government hospital in Central Philippines with a 250-bed capacity including 50 160
paediatric beds. Ospital ng Palawan (ONP) is a secondary referral government 161
hospital in Western Philippines with 40 beds in the paediatric department. ONP 162
has around 500 patients in the paediatric department each year. Research Institute 163
for Tropical Medicine (RITM), which is located in Metro Manila, has a 164
specialized tertiary care hospital with 50 beds, 28 doctors and 62 nurses. RITM 165
has around 500 patients per year. The study periods varied among hospitals with 166
BPH from September 2012 to March 2016, EVRMC from June 2008 to Jan 2015, 167
ONP from August 2012 to February 2015, and RITM from September 2012 to 168
January 2015 (Figure 2). 169

11 | P a g e
5.3 Study patients 170
Children aged from 8 days to less than 5 years who were hospitalised in the 171
above facilities with acute respiratory symptoms were assessed by using the 172
IMCI algorithm by trained study physicians9. Patients who were assessed to have 173
severe pneumonia or very severe disease by the IMCI algorithm were recruited 174
for the study. In 2014, the IMCI algorithm for acute respiratory infection was 175
revised, and children with chest indrawing are no longer diagnosed as severe 176
pneumonia and do not require hospitalization. However, this new algorithm had 177
not been widely implemented in the study sites during the study period, and 178
patients with chest indrawing and those with danger signs continued to be 179
recruited based on the previous IMCI algorithm. Exclusion criteria included 180
children aged less than 7 days old or 5 years or more, children admitted for 181
another illness and who had developed symptoms of pneumonia during 182
hosipitalization, children who had been admitted to another hospital within the 183
last 3 days prior to present admission and children who had prior hospital 184
admission without one week symptom free period when readmitted to the 185
hospital. 186

12 | P a g e
Patient outcomes were grouped into two categories, survived and deceased. 187
Survived group included discharged cases and discharged against medical advice 188
with improved conditions. The deceased group included those who deceased 189
during the hospitalization and discharged against medical advice with a 190
deteriorated condition on their last clinical assessment. Congenital abnormalities 191
included congenital heart disease, trisomy 21 syndrome, cerebral palsy or other 192
neurodevelopmental conditions, and inherited haemolytic anaemia. Tachypnea 193
was defined as follows: respiratory rate (RR) ≥60 breaths per minute (min) in 194
children <2 months, RR ≥50 breaths per min in children 2‒11 months, and RR 195
≥40 breaths per min in children ≥12 months 39
. Tachycardia was defined heart 196
rate ≥180 beats per minute (bpm) for children <12 months old and ≥140 bpm for 197
children older than ≥12 months. The WHO child growth standards were used to 198
evaluate the nutritional status of the child by computing the Z-scores of weight-199
for-age and height-for-age40
. Blood oxygen saturation (SpO2) was measured on 200
admission by using a pulse oximeter (Handheld Pulse Oximeter PalmSAT 2500A 201
with Finger Clip Sensor (Paediatrics), Nonin Medical, Inc.). Venous blood 202
samples were also collected. The level of hemoglobin <8g/dL was classified as 203
severe anemia. 204
13 | P a g e
5.4 Collection of patient information 205
A standardized questionnaire was used to collect the socio-demographic and 206
environmental data of households only for children recruited from February 2014 207
to March 2016. A Simple Poverty Scorecard for the Philippines developed by 208
Mark Schreiner3 was used to assess the socio-ecomonic status (SES) of the 209
household. This score uses 10 simple questions (the number of children per 210
household, school attendance of the children, female head’s education level, 211
employment salary, material of the house’s roof and walls, the type of toilet 212
facility, and possession of a refrigerator, television, or washing machine), and the 213
scores range from 0 to 100. Households with an SES score <30 were defined as 214
being in extreme poverty. A physical examination was conducted by a trained 215
study physician, which included an examination of neck rigidity, sensorial 216
changes, grunting, decreased breath sounds, chest indrawing, rales, central 217
cyanosis, and nasal flaring. The following signs were considered as sensorial 218
change: irritability, drowsiness, and stupor. The Glasgow coma scale was used 219
for the assessment of coma and impaired consciousness41
. Glasgow coma scale 220

14 | P a g e
<9 was considered to indicate severe condition, while the scale of 9–12 was 221
considered to indicate moderate condition. 222
5.5 Assessment of chest X-ray 223
Anteroposterior and lateral chest radiographs were obtained. The image was 224
interpreted by a designated radiologist trained for the standard interpretation of 225
chest radiographs for the diagnosis of childhood pneumonia, as developed by the 226
WHO Pneumonia Vaccine Trial Investigators’ Group42
. The chest X-ray findings 227
included end-point consolidation, other infiltrates and pleural effusion, and end-228
point pneumonia was defined as the presence of end-point consolidation or 229
pleural effusion. 230
5.6 Detection of viruses 231
After the sample collection, nasopharyngeal swabs (NPS) in viral transport 232
medium were stored at 4°C in different sites and transported with ice packs to 233
RITM in Manila for further analysis twice a week. Viral RNA and DNA were 234
purified using the QIAamp MinElute Virus Spin Kit. Viral RNA was reverse 235
transcribed to complementary DNA by the Moloney Murine Leukaemia Virus 236
Reverse Transcriptase with random hexamer primers. RSV, HMPV and PIV 237

15 | P a g e
were detected in the samples by multiplex polymerase chain reaction (PCR) 238
using two systems. The first system was for detection of RSV and HMPV. The 239
second system was for detection of PIV-1, -2, -3 and -4. RSV positive samples 240
were further subtyped into RSV-A and RSV-B by performing the nested PCR43-46
. 241
RV and enterovirus (EV) were detected from clinical samples by targeting 5’ 242
Noncoding Region (NCR). The RV species (A, B, C) and serotypes of EV 243
including EV-D68 were further identified by sequencing and phylogenetic 244
analysis of 5’ NCR. RT-PCR was performed for the detection of IFV 245
A(H1N1)pdm09, IFV A(H3N2) and IFV B47
. ADV detection was performed by 246
combining viral isolation and neutralization test as well as PCR and serotyping 247
by sequencing48-50
. 248
5.7 Detection of bacteria 249
Blood drawing for bacterial identification was done after obtaining consent from 250
caregivers. One mL of venous blood was aseptically collected from patients on 251
admission, and inoculated into a bottle containing 20 mL of brain-heart infusion 252
broth with 1% gelatin, 0.125% sodium polyanethol sulfonate, and 0.1% agar. 253
Samples were incubated at 36°C for seven days and subcultures were conducted 254
16 | P a g e
on sheep blood, chocolate, and MacConkey agar plates after 18 hours and 3, 5, 255
and 7 days of inoculation. Plates were cultured at 36°C in a candle jar for 2 days. 256
All isolates were stored in the skim milk at −20°C and transported to RITM for 257
confirmatory tests. For confirmatory test for Burkholderia cepacia group, isolates 258
were sent to Miroku Medical Laboratory in Nagano, Japan, and underwent 259
sequencing for 16S rRNA. It was considered bacterial culture positive if at least 260
one of the following 12 bacteria was identified; Acinetobacter baumannii (A. 261
baumannii), Burkholderia cepacia (B. cepacia), Enterobacter aerogenes (E. 262
aerogenes), Haemophilus influenzae (H. influenzae), Klebsiella pneumoniae (K. 263
pneumoniae), Staphylococcus aureus (S. aureus), Pseudomonas aeruginosa (P. 264
aeruginosa), Pseudomonas stutzeri (P. stutzeri), other Pseudomonas species (P. 265
spp.), Streptococcus pneumoniae (S. pneumoniae), and Onchrobactrum anthropi 266
(O. anthropi). 31
. Due to the high carriage rates of certain bactearia in the upper 267
respiratory tract and low diagnostic value of bacterial culture using NPS, bacteria 268
were not tested for NPS 51
. 269
Virus-bacteria co-detection was defined positive for at least one virus and one 270
pathogenic bacterium and virus-virus co-detection was defined as patient with 271
two or more viruses detected. Patients whose samples were negative for any of 272
17 | P a g e
the target viruses and bacteria by blood culture were considered negative for all 273
pathogens. 274
275
5.8 Data analysis 276
Outcome: 277
Patient outcomes were grouped into two categories: survived and deceased. The 278
survived group comprised of patients who were discharged, including those 279
discharged against medical advice but with improved conditions. The deceased 280
group comprised of patients who deceased during the hospitalisation period or 281
were discharged against medical advice (DAMA)with a deteriorated condition on 282
their last clinical assessment. We considered the worse cases scenarios by 283
assuming that patients who were DAMA with deteriorated condition were all 284
going to die. 285
The survived group included who were discharged and observed cured and those 286
who were DAMA cases but with improved condition at their last examination. 287

18 | P a g e
The data were analysed based on two age groups, children <2 months and 2-59 288
months according to the IMCI guidelines.10 52
. 289
To investigate the etiologic and clinical factors associated with fatal outcomes, a 290
generalized linear model was applied. This model was adjusted for the age of 291
patients, the year of sampling, and the hospitals where patients were admitted. A 292
second model was also applied where the association of death was evaluated in 293
the context of the clinical and radiological findings in 6 separate groups of 294
children including those positive for RSV, RV, ADV, EV, bacteria in blood and 295
negative for any viruses. The second model was adjusted for the age of patients, 296
the year of sampling, and the hospitals after matching with the age groups. The 297
extent of association with the fatal outcome in both models was evaluated by 298
calculating the odd ratios (ORs) and 95% confidence interval (C.I.) using a 299
simple exact binomial calculation. Fisher exact test was applied to compare the 300
frequencies and Welch’s t-test or Brunner-Munzel test was used to compare the 301
means and medians of variables between the two groups. P-value <0.05 indicated 302
statistical significance. The comparison of CFRs by the year was examined using 303
the Cochran-Armitage Test for Trend. Missing data were not included in analysis. 304
19 | P a g e
All statistical analyses were performed using Microsoft R Open 3.2.4 and Dplyr 305
package53
. 306
307
5.8 Ethical considerations 308
The study protocol was approved by the Ethics Committee of Tohoku University 309
Graduate School of Medicine and the Institutional Review Board of RITM. 310
Written informed consent was obtained from the parents or guardians of children 311
who participated in the study. 312
313
6. Results 314
6.1 Demographic, clinical and radiographic findings. 315
From 2008 to 2016, 5,128 children were enrolled in the study (Fig. 2). Of these, 316
the outcome was available for 5,054 (98.6%) children, while 74 (1.4%) children 317
were excluded from the analysis due to loss to follow-up, unknown outcome, or 318
transferred to another hospital. Out of the 5,054 patients analysed, 749 (14.8%) 319
were <2 months and 4,305 (85.2%) were aged 2-59 months old. 320
20 | P a g e
The case fatality rate (CFR) was slightly higher in patients aged <2 321
months than in those aged 2-59 months (5.3% vs. 4.6%) and declined as the age 322
of children increased. Children aged <24 months accounted for 87.0% of the fatal 323
cases with the age group of 2-5 months having the highest CFR of 7.0% (Table 324
2). Similar patterns were also observed when analysis was done without 325
including DAMA cases (Table 8). 326
There were more male patients (n=2876, 56.9%) than female patients 327
(n=2178, 43.1%), although there was no significant association between the 328
gender and outcome in both age groups (Table 2). A significant decreasing trend 329
of CFR was observed during the 9-year study period, with the highest CFR of 330
12.5% in 2008 and the lowest CFR of 2.0% in 2013 (p <0.001) (Table 1). 331
EVRMC showed the highest CFR among the hospitals in both age groups (<2 332
months, 7.8% and 2-59 months, 5.7%) and presented its highest CFR (12.5%) in 333
2008 and the lowest in 2013(1.1%). 334
CFRs were lower in BPH (3.2%) and ONP (2.1%). The median days of 335
hospitalization was longer in patients aged <2 months than those aged 2-59 336
months (7 vs 4 days) (Table 2). The presence of congenital abnormalities was 337

21 | P a g e
associated with the fatal outcome for both age groups (p <0.05). Severe 338
underweight for age (<-3SD) was observed in 41.2% of the fatal cases in patients 339
aged <2 months, and in 39.2% of the fatal cases in patients aged 2-59 months. 340
The history of child loss in the family was more frequent in fatal cases than in the 341
survived group for children aged 2-59 months (33.3% vs 10.2%, p =0.003). 342
Charcoal and wood were used as the cooking fuels by 86.5% of patient’s 343
families; however, there was no significant association between the type of 344
cooking fuels and outcomes (Table 2). 345
Among the findings of physical examination, rales and chest indrawing 346
were the most common signs in both age groups (Table 3). On admission, 19.1% 347
(968/5054) of fatal patients had fever (>38.5°C), and fever was significantly 348
more frequent in the deceased group than in the survived group of both age 349
groups. Sensorial changes were present in 28.0% of the fatal cases; these changes 350
were more frequent in the deceased group than the survived group of both age 351
groups (p <0.001). Glasgow coma scale <9 was also associated with fatal 352
outcome in children aged 2-59 months (p <0.001). The prevalence rate of 353
hypoxemia was 13.0% (654/5023). Among the respiratory signs, grunting, 354

22 | P a g e
decreased breath sounds, central cyanosis, apnoeic episode and SpO2 <90% were 355
more commonly observed in the deceased group than in the survived group of 356
both age groups (Table 3). 357
The proportion of patients with severe anaemia (<8g/dL) was higher in the 358
deceased group of both age groups (p <0.01), while the mean hemoglobin level 359
was lower only in the patients aged 2-59 months (10.3 vs 11.2 g/L, p <0.001). 360
WBC counts were significantly higher in the deceased cases than in the survived 361
cases in both age groups, while neutrophil cell count was higher in the deceased 362
cases than in the survived cases in both age groups, but statistical significance 363
was only observed in patients aged 2-59 months (9.86 vs 7.17 103/μL, p =0.01) 364
(Table 3). 365
A total of 4,498 children had chest radiographs; of these, 4,452 showed 366
interpretable results. At least one abnormal finding was noted in 1,711 (38.4%) 367
chest radiographs. Among the deceased cases, 41.6% patients showed end-point 368
pneumonia, 5% had consolidation, 35% had infiltrations, and 3.4 % had pleural 369
effusion These findings were significantly more common in the deceased cases 370
23 | P a g e
than in the survived cases except for pleural effusion in children aged <2 months 371
age (Table 3). 372
6 2 Pathogens detected 373
6 2 1 Viruses detected from nasopharyngeal swabs 374
Of the 5,054 nasopharyngeal swabs, 61.0 % were tested positive for at least one 375
virus. RSV was the most common viral pathogen, which was found in 27.0% 376
(1352/5054), of which, 135(10.0%) of them had co-infection with other viruses. 377
RV was the second most common viral pathogen, which was detected in 23.0% 378
(1156/5054) of the cases, of which 173(17.6 %) had co-infection infections with 379
other viruses. The RSV positive rate was significantly lower in the deceased 380
cases among patients aged 2-59 months. A similar trend was also observed in 381
patients aged <2 months; however, the difference was not statistically significant. 382
The positive rates of RSV-A, RSV-B, and HMPV were also significantly lower 383
in the cases than in the survived cases among those aged 2-59 months. On the 384
other hand, the positive rate of ADV, specifically for ADV-7 was significantly 385
higher in the deceased cases than in the survived cases for patients aged 2-59 386
months, while the CFRs of ADV and ADV-7 were 10.7% and 24.0%, 387

24 | P a g e
respectively. The positive rate for EV-D68 was higher in the deceased cases than 388
in the survived cases, although the difference was not statistically significant 389
(Table 5 and 6). 390
6 2 2 Bacteria detection in blood. 391
A total of 3,000 blood samples were tested for bacterial culture. The overall 392
positivity rate for any pathogenic bacteria in the blood samples was 1.6% 393
(49/3,000) and the CFR among blood culture-positive cases was 18.3% (9/49). 394
The most commonly identified bacterial pathogen was B. cepacia (26.5%, n=13), 395
followed by S. pneumoniae (22.4%, n=11), and A. baumannii (n=5) (Tables 5 396
and 6). The positive rates for blood culture were significantly higher in the 397
deceased cases than in the survived cases in both age groups. Among the 398
deceased cases in the patients aged 2-59 months, the identified bacteria included 399
P. aeruginosa (n=2), S. pneumoniae (n=2), MRSA (n=2), A. baumannii (n=1), B. 400
cepacia (n=1), and K. pneumoniae (n=1) while A. baumannii and K. pneumoniae 401
were identified in the deceased cases aged <2 months (Table 5 and 6). 402
403
6 3 Factors associated with deaths 404
25 | P a g e
6 3 1 Univariate logistic regression analysis of factors associated with death 405
In the univariate analysis, the demographic, clinical and laboratory findings 406
significantly associated with death in both age groups included severe 407
underweight (weight-for-age <-3SD), presence of congenital abnormalities, 408
decreased breath sounds, grunting, sensorial changes, central cyanosis, fever 409
(>38.5°C), SpO2<90%, anaemia (<8g/dL), endpoint pneumonia and blood culture 410
positive for bacteria (Tables 3 and 4). In addition, past experiences of child loss, 411
tachypnea, and pleural effusion were associated with death in patients aged 2-59 412
months. Infection with RSV [OR: 0.33(95%CI 0.2-0.52)], and HMPV [OR: 0.25 413
(95%CI: 0.04-0.79)] were negatively associated with death in patients aged 2 -59 414
months (Table 3 and 4). In contrast ADV [OR: 4.18(1.79-8.57)], particularly 415
ADV-7 [OR: 10.66 (95%CI: 3.68-27.77)] was positively associated with death in 416
children aged 2 -59 months (Tables 5 and 6). 417
6 3 2 Multivariate logistic regression analysis of factors associated with 418
death 419
After adjusting for age in months, the year of sampling, and the hospital in the 420
multivariate analysis, the following factors were found to be associated with 421
26 | P a g e
death in both age groups: severe underweight, presence of congenital 422
abnormalities, decreased breath sounds, grunting, sensorial changes, central 423
cyanosis, SpO2 (<90%,) fever (>38.5C), anaemia (<8 g/dL), consolidation, 424
infiltration, blood culture positive for bacteria (Tables 3 and 4). Moreover, past 425
experience of child loss, mild underweight (-3SD ≤ w<-2SD), tachypnea, 426
tachycardia, ADV, ADV-7 and seasonal IFV A (H1N1) were found to be 427
associated with death in children 2-59 months. In contrast, RSV, HMPV and RV-428
C infections decreased the odds of death in children aged 2-59 months (Tables 4, 429
5, 6). 430
431
6 3 3 Multivariate logistic regression analysis of factors associated with 432
deaths tested positive for different pathogens. 433
The factors with the deceased cases were analysed for those positive for RSV, 434
RV, ADV, EV, blood culture for bacteria, and negative for all viruses (Table 7). 435
The presence of fever >38.5°C increased the odds of death in patients infected 436
with RV, ADV, EV, and bacteria and in patients who were tested negative for all 437
viruses. The presence of hypoxemia increased the odds of death in patients 438
27 | P a g e
infected with RSV, RV and ADV. The presence of infiltration increased the odds 439
of death in patients infected by RSV, ADV and EV. Interestingly, pleural 440
effusion was associated with death in the group of patients who are negative to 441
all viruses (Table 7). 442
443
7 Discussion 444
The overall CFR of children hospitalised with severe pneumonia in the 445
present study was 4.7%. This value is similar to those reported in other LMIC35 54
446
55. A significant decreasing trend of mortality was observed during the study 447
period; however, this trend essentially reflected the trend of EVRMC, and could 448
be attributed to the improved access to health-care facilities and the improved 449
management of childhood pneumonia in the past decade. Another possible reason 450
may be the introduction of new vaccines such as H. influenzae type b (Hib) 451
vaccines and pneumococcal conjugate vaccines (PCV). These vaccines have been 452
shown to reduce the mortality due to childhood pneumonia 22 23
. However, in the 453
Philippines, Hib vaccines were introduced in 2010 and PCVs were introduced in 454
201456
. Vaccination coverage for Hib and PCV were estimated to be 67% and 455

28 | P a g e
35%, respectively in 2014 56
. Since a decreasing trend in CFR was observed 456
before the introduction of these vaccines, other factors such as improved access 457
to health-care facilities and improved quality of care are more likely to have 458
contributed to the reduction of CFR. 459
Children aged <24 months accounted for 87.0% of total deaths, which is 460
comparable with the global estimate of 81.0% of pneumonia-related deaths 461
occurring in children aged < 2 years57
. Patients aged 2-5 months showed the 462
highest CFR of 7.0 %. Similar results have also been reported in a previous study 463
conducted in the Philippines, wherein children of this age group were at risk for 464
pneumonia-associated mortality18
. The immune system of patients in this age 465
group is not fully functional 58
and children aged 2-5 months have a lower level 466
of circulating IgG in the blood than in other age groups59
. 467
Moreover, an association between the history of child loss in the family 468
and deaths was found in children aged <2-59 months, which may be due to the 469
lack of financial resources in the family, limited access to health-care facilities, 470
or inappropriate health-seeking behaviour of the caretakers such as self-471
medication, which may result in delayed commencement of proper care for 472
children with pneumonia60
. Another contributing factor can be the higher number 473

29 | P a g e
of children per family among families in which the history of child loss was 474
observed. In the present study, CFR was higher in families with the number of 475
children ≥4, although it was not significant. The increased risk of pneumonia in 476
households using solid cooking fuel and low SES has been well characterised in 477
the past 3 5-7
. However, their role in the fatal outcome of childhood pneumonia 478
remains to be established in hospital settings. 479
More than half of the patients (55.0%) who died were moderate or severe 480
underweight (weight-for-age <-3SD). A similar rate of 52.5% has been reported 481
among undernourished patients who died of infectious diseases in LMIC among 482
children <5 years61
. In a hospital-based study conducted in Malawi, the CFR-483
attributed to pneumonia was high among patients with severe malnutrition, 484
despite the general trend of decreasing CFR among patients with pneumonia35
, 485
which suggests that severely malnourished children with pneumonia require 486
intensive inpatient care 62
. Furthermore, malnutrition and HIV are endemically 487
present in many areas in the world63-65
. The underlying mechanisms explaining the 488
association between infections and malnutrition are not well established. 489
Deficiencies of some micronutrients have been found to be associated with some 490
conditions. Vitamin D deficiency has been reported to increase the risk of RSV 491

30 | P a g e
infection 66
, and zinc deficiency was found to be associated with acute respiratory 492
diseases 67
. Additionally, impairment of intracellular bacterial digestion 68
, and an 493
increase of risk of bacterial resistance to β-lactam by increasing exchange of ß-494
lactamase encoding genes between bacteria, were reported among severely 495
malnourished patients 69
. Guidelines for the management of pneumonia in 496
children with malnutrition should consider this strong association with mortality. 497
498
Several clinical factors have been found to be associated with death including 499
decreased breath sounds, grunting, severe anaemia, central cyanosis, and fever 500
(>38.5°C), which are consistent with those reported previously 35 37
. In children 501
<2 months particular attention needs to be given to patients with fever > 38.5°C 502
because of the high CFR of 32.5%. A bacterial infection should be considered in 503
pneumonia cases with fever >38.5°C as reported elsewhere70
. However, in 504
malaria endemic areas, fever >38.5°C can be confused with malaria. Several 505
other conditions can present similar clinical features, and patients can have 506
multiple conditions simultaneously11-14
. 507
508
Hypoxemia (SpO2<90%) prevalence was 13.0% in this study, which is 509
compatible to the mean rate of hypoxemia among severe and very severe 510
31 | P a g e
pneumonia cases in a review study71
, but lower than the reported hypoxemic 511
cases of 20% in Bohol Island in the Philippines 72
. Some patients had received 512
the oxygen supply before SpO2 measurement in this study, which might 513
underestimate the prevalence of hypoxia. Hypoxemia was associated with death 514
in this study, in concordance with earlier findings73-77
. In a multicentre study that 515
included five LMIC, the CFR among the hypoxemic patients was 8.5%78
, which 516
is lower than the range of CFRs (12.6%-15.7%) among the hypoxemic patients in 517
this study. Hypoxemia was associated with viral infections such as RV and RSV 518
and with poor outcome particularly in ADV infection79-83
. In this study, 519
hypoxemia was significantly associated with death in patients infected with RV, 520
RSV and ADV, and adjusted OR was particularly high for ADV. Central 521
cyanosis was also significantly associated with death for RSV and RV, which 522
suggests that hypoxia, is particularly important in viral infections (Table 5). The 523
use of pulse oximeter for detection of hypoxemia in the management of 524
community-acquired pneumonia has been proven to be useful, and it is able to 525
increase the referral of patients and reduce the rate of improper treatment with 526
antibiotics 84 85
. 527
528

32 | P a g e
The presence of a positive chest radiograph findings generally increase 529
CFR. CFR among the cases with consolidation was 13.0%, which is the same as 530
the reported mean CFR of 13% in a multicentre study on childhood pneumonia 38
. 531
The positivity rates for abnormal findings of chest radiograph varied across 532
countries with the type of population and the presence of comorbidities38
but the 533
association of endpoint pneumonia and consolidation with death or treatment 534
failure have been consistently reported 18 76 77
. In addition, patients positive for 535
RV and bacteria and negative for any viruses were more likely to die if they had 536
abnormal findings by chest radiograph. These findings suggest that among 537
patients positive for RV and negative for any viruses, a subset of these patients 538
may have bacterial pneumonia. 539
Seasonal IFV A (H1N1) had a CFR of 40% in children aged 2-59 months, which 540
was in contrast with the CRF of 0% for IFV A (H1N1) pdm09. The reason why 541
seasonal IFV A(H1N1) had such a high CFR remains unclear, however it should 542
be noted that all seasonal IFV A(H1N1) occurred during the period of 2008 to 543
2009, which was marked by an overall high CFR. ADV-7 had CFR of 24.0% in 544
patients aged 2-59 months, which concurs with a similar finding in China86
. Most 545
cases of ADV-7 in this study occurred between 2008 and 2011, which coincided 546
33 | P a g e
with the ADV-7 outbreaks in China 86 87
. CFR associated with EV-68 (8.5%) was 547
also higher than the average value. The association of EV-68 with severe ALRI, 548
including pneumonia, has been well reported across several studies, including 549
those reporting fatal cases 34 88-90
. RSV was the most common virus identified in 550
the present study, which is in agreement with some previous reports 31-33
. 551
However, RSV was negatively associated with death. Similar findings were also 552
observed in other studies conducted in hospital settings even in high-risk 553
populations such as HIV positive patients and cases with comorbidities91-94
. 554
RV presented with the highest number of deaths in this study. In contrast 555
to RSV, which was significantly and inversely associated with death in children 556
aged 2−59 months, RV did not have any positive or negative associations with 557
death. RV is classified into three species, RV-A, B and C. CFRs for RV-A and B 558
were higher than average, but the difference was not statistically significant. The 559
CFR of RV-C was lower in patients aged 2-59 months, which was statistically 560
significant in the univariate analysis. Some studies revealed that RV-C is 561
associated with severe respiratory infections, including deaths95
. However, the 562
data from this study does not support this association. As mentioned earlier, 563
some RV positive cases, especially those positive for RV-A and B may include 564

34 | P a g e
bacterial pneumonia cases. Further studies are required to determine the 565
association of different RVs with pneumonia and deaths due to pneumonia. I also 566
did not observe an increase of the risk of death in patients with multiple viral 567
infections, which is consistent with an earlier report96
. However, the majority of 568
multiple infections that occurred due to RV, RSV, and both of the viruses did not 569
increase the risk of death. Additionally, it is also possible that some of these 570
viruses were not the cause of symptoms as they can be found in asymptomatic 571
patients 97 98
. 572
573
Blood culture positive for bacteria was associated with death as reported 574
elsewhere 99 100
. CFR among the patients positive for bacteria was 5 times higher 575
than the overall CFR in children aged < 2 months old. 576
Methicillin-resistant Staphylococcus aureus was identified in 2 patients 577
with fatal outcome. This bacterium is known to cause nosocomial infection101
. 578
Similarly for B. cepacia and A. baumannii can be identified as a result of 579
nosocomial infection or environmental contamination102-104
. Since blood samples 580
were collected immediately after admission, the possibility of nosocomial 581
transmission of these bacteria is low. However, a possibility of environmental 582

35 | P a g e
contamination cannot be ruled out. Furthermore, a study done among childhood 583
pneumonia cases in the Philippines in Bohol Island did not report either B. 584
cepacia nor A. baumannii suggesting a possibility of environmental 585
contamination105
. 586
A proper diagnosis of bacterial infection and early treatment with 587
antibiotics are particularly important in this group of patients. However, there 588
were no specific signs and symptoms that could differentiate the patients with 589
bacterial infections and those with viral infections. Furthermore, the detection 590
rate of bacteria was low, which is similar to the findings of previously published 591
reports106 107
, particulary with those conducted in the Phillipines, which reported 592
a positivity rate of 1.1% 105
. The possibility of an antimicrobial treatment before 593
admission in hospital may play a role in low positivity rate since the 4 hospitals 594
in studies are all secondary of teriary referal centers. 595
Although the sensitivity of blood culture for childhood pneumonia is 596
extremely low, there is no alternative to the gold standard in the diagnosis of 597
bacterial pneumonia in children. The difficulty in obtaining proper sputum 598
samples from children also prevented us from identifying the pathogens in 599
patients 108
. 600

36 | P a g e
The positive rate for at least one pathogen was 68% for all patients and 601
54.4% for fatal cases. Although the availability of molecular diagnostic assays 602
such as PCR has greatly increased the ability to detect respiratory viruses, 603
detection of other pathogens remains a challenge in childhood pneumonia as 604
observed in others studies 109 110
. 605
606
This study has some limitations. IMCI algorithm was used as diagnosis 607
criteria; however, these criteria are not able to distinguish pneumonia from other 608
acute lower respiratory infections, such as bronchitis and bronchiolitis 10 52
. 609
Inclusion of the DAMA-deteriorated cases as deaths could have increased the 610
CFR. Data collection on social factors started from 2014 onward, and limited 611
analysis was possible for risk factors. And finally, some clinical and laboratory 612
data were missing, especially in fatal cases because several deaths occurred 613
immediately after hospital admission. Similarly, the sampling rate for blood 614
culture was lower for fatal cases because the patients died before their samples 615
could be obtained. Despite these limitations, this study had a large sample size of 616
more than 5,000 patients and studies over a long duration of 9 years in a lower-617
middle income country, which provided a comprehensive data on the 618

37 | P a g e
demographics, clinical characteristics, mortality and aetiology of hospitalised 619
children with severe pneumonia in the Philippines that can be generalised not 620
only in the Philippines but also in other LMICs with high level of malnutrition. 621
However, in areas with high HIV-AIDS prevalence, the possibility of 622
Pneumocystis jiroveci 111
and other opportunistic infections should be considered. 623
8 Conclusion 624
Underweight (malnutrition) remains the most common factor associated with 625
death among childhood pneumonia cases. Therefore, reinforcing measures to 626
improve nutritional status will probably reduce the mortality rate of childhood 627
pneumonia. SpO2<90% was also an important predictor for fatal outcome. 628
Monitoring of oxygen saturation should be promoted not only in severe but also 629
in non-severe childhood-pneumonia cases and supplementary oxygen therapy 630
should be administered in these patients. Due to the association of chest 631
radiograph findings with death, a chest radiograph should be required in all 632
hospitalised patients with signs of pneumonia and health workers should be 633
trained to read the chest radiograph. The adequate measure should be taken to 634
diagnose or eliminate the presence of bacterial infections. Continuous detection 635
38 | P a g e
of EV-D68 and ADV-7 infections should be performed for monitoring and 636
control of future outbreaks. 637
638
9 References 639
1. Walker CL, Rudan I, Liu L, et al. Global burden of childhood pneumonia and diarrhoea. 640 Lancet 2013;381(9875):1405-16. doi: 10.1016/S0140-6736(13)60222-6 641
2. UNICEF. Levels & Trends in Child Mortality Report 2017 Estimates Developed by theUN 642 Inter-agency Group for Child Mortality Estimation 2017. 643
3. Kosai H, Tamaki R, Saito M, et al. Incidence and Risk Factors of Childhood Pneumonia-Like 644 Episodes in Biliran Island, Philippines--A Community-Based Study. PloS one 645 2015;10(5):e0125009. doi: 10.1371/journal.pone.0125009 646
4. Thorn LK, Minamisava R, Nouer SS, et al. Pneumonia and poverty: a prospective population-647 based study among children in Brazil. BMC Infect Dis 2011;11:180. doi: 10.1186/1471-648 2334-11-180 649
5. Fonseca Lima EJ, Mello MJ, Albuquerque MF, et al. Risk factors for community-acquired 650 pneumonia in children under five years of age in the post-pneumococcal conjugate 651 vaccine era in Brazil: a case control study. BMC Pediatr 2016;16(1):157. doi: 652 10.1186/s12887-016-0695-6 653
6. Mahalanabis D, Gupta S, Paul D, et al. Risk factors for pneumonia in infants and young 654 children and the role of solid fuel for cooking: a case-control study. Epidemiol Infect 655 2002;129(1):65-71. 656
7. Ezeh OK, Agho KE, Dibley MJ, et al. The effect of solid fuel use on childhood mortality in 657 Nigeria: evidence from the 2013 cross-sectional household survey. Environmental 658 health : a global access science source 2014;13:113. doi: 10.1186/1476-069X-13-113 659
8. Byass P. Interplay between childhood pneumonia and HIV infection. Lancet Infect Dis 660 2014;14(12):1172-3. doi: 10.1016/S1473-3099(14)71006-0 661
9. WHO. Handbook : IMCI integrated management of childhood illness. 662 10. WHO. Revised WHO classification and treatment of childhood pneumonia at health 663
facilities EVIDENCE SUMMARIES 2014 664 11. English M, Punt J, Mwangi I, et al. Clinical overlap between malaria and severe pneumonia 665
in Africa children in hospital. Transactions of the Royal Society of Tropical Medicine and 666 Hygiene 1996;90(6):658-62. 667
12. O'Dempsey TJ, McArdle TF, Laurence BE, et al. Overlap in the clinical features of 668 pneumonia and malaria in African children. Transactions of the Royal Society of 669 Tropical Medicine and Hygiene 1993;87(6):662-5. 670
13. Redd SC, Vreuls R, Metsing M, et al. Clinical signs of pneumonia in children attending a 671 hospital outpatient department in Lesotho. Bulletin of the World Health Organization 672 1994;72(1):113-8. 673
14. D'Acremont V, Kilowoko M, Kyungu E, et al. Beyond malaria--causes of fever in outpatient 674 Tanzanian children. The New England journal of medicine 2014;370(9):809-17. doi: 675 10.1056/NEJMoa1214482 676

39 | P a g e
15. Perry RT, Halsey NA. The clinical significance of measles: a review. J Infect Dis 2004;189 677 Suppl 1:S4-16. doi: 10.1086/377712 678
16. Olmsted SS, Moore M, Meili RC, et al. Strengthening laboratory systems in resource-limited 679 settings. American journal of clinical pathology 2010;134(3):374-80. doi: 680 10.1309/AJCPDQOSB7QR5GLR 681
17. Maru DS, Schwarz R, Jason A, et al. Turning a blind eye: the mobilization of radiology 682 services in resource-poor regions. Globalization and health 2010;6:18. doi: 683 10.1186/1744-8603-6-18 684
18. Lupisan SP, Ruutu P, Erma Abucejo-Ladesma P, et al. Predictors of death from severe 685 pneumonia among children 2-59 months old hospitalized in Bohol, Philippines: 686 implications for referral criteria at a first-level health facility. Trop Med Int Health 687 2007;12(8):962-71. doi: 10.1111/j.1365-3156.2007.01872.x 688
19. Johnson AW, Osinusi K, Aderele WI, et al. Etiologic agents and outcome determinants of 689 community-acquired pneumonia in urban children: a hospital-based study. Journal of 690 the National Medical Association 2008;100(4):370-85. 691
20. Black RE, Cousens S, Johnson HL, et al. Global, regional, and national causes of child 692 mortality in 2008: a systematic analysis. Lancet 2010;375(9730):1969-87. doi: 693 10.1016/S0140-6736(10)60549-1 694
21. Garcia Gabarrot G, Lopez Vega M, Perez Giffoni G, et al. Effect of pneumococcal conjugate 695 vaccination in Uruguay, a middle-income country. PLoS One 2014;9(11):e112337. doi: 696 10.1371/journal.pone.0112337 697
22. Theodoratou E, Johnson S, Jhass A, et al. The effect of Haemophilus influenzae type b and 698 pneumococcal conjugate vaccines on childhood pneumonia incidence, severe 699 morbidity and mortality. Int J Epidemiol 2010;39 Suppl 1:i172-85. doi: 700 10.1093/ije/dyq033 701
23. Becker-Dreps S, Amaya E, Liu L, et al. Changes in childhood pneumonia and infant mortality 702 rates following introduction of the 13-valent pneumococcal conjugate vaccine in 703 Nicaragua. Pediatr Infect Dis J 2014;33(6):637-42. doi: 704 10.1097/INF.0000000000000269 705
24. le Roux DM, Zar HJ. Community-acquired pneumonia in children - a changing spectrum of 706 disease. Pediatric radiology 2017;47(11):1392-98. doi: 10.1007/s00247-017-3827-8 707
25. Ruuskanen O, Lahti E, Jennings LC, et al. Viral pneumonia. Lancet 2011;377(9773):1264-75. 708 doi: 10.1016/S0140-6736(10)61459-6 709
26. McIntosh K. Community-acquired pneumonia in children. N Engl J Med 2002;346(6):429-37. 710 doi: 10.1056/NEJMra011994 711
27. Shi T, McAllister DA, O'Brien KL, et al. Global, regional, and national disease burden 712 estimates of acute lower respiratory infections due to respiratory syncytial virus in 713 young children in 2015: a systematic review and modelling study. Lancet 714 2017;390(10098):946-58. doi: 10.1016/S0140-6736(17)30938-8 715
28. Shay DK, Holman RC, Roosevelt GE, et al. Bronchiolitis-associated mortality and estimates 716 of respiratory syncytial virus-associated deaths among US children, 1979-1997. J Infect 717 Dis 2001;183(1):16-22. doi: 10.1086/317655 718
29. El Kholy AA, Mostafa NA, El-Sherbini SA, et al. Morbidity and outcome of severe respiratory 719 syncytial virus infection. Pediatrics international : official journal of the Japan Pediatric 720 Society 2013;55(3):283-8. doi: 10.1111/ped.12051 721
30. Nair H, Brooks WA, Katz M, et al. Global burden of respiratory infections due to seasonal 722 influenza in young children: a systematic review and meta-analysis. Lancet 723 2011;378(9807):1917-30. doi: 10.1016/S0140-6736(11)61051-9 724

40 | P a g e
31. Suzuki A, Lupisan S, Furuse Y, et al. Respiratory viruses from hospitalized children with 725 severe pneumonia in the Philippines. BMC infectious diseases 2012;12:267. doi: 726 10.1186/1471-2334-12-267 727
32. Jain S, Williams DJ, Arnold SR, et al. Community-acquired pneumonia requiring 728 hospitalization among U.S. children. N Engl J Med 2015;372(9):835-45. doi: 729 10.1056/NEJMoa1405870 730
33. Garcia-Garcia ML, Calvo C, Pozo F, et al. Spectrum of respiratory viruses in children with 731 community-acquired pneumonia. Pediatr Infect Dis J 2012;31(8):808-13. doi: 732 10.1097/INF.0b013e3182568c67 733
34. Martin G, Li R, Cook VE, et al. Respiratory Presentation of Pediatric Patients in the 2014 734 Enterovirus D68 Outbreak. Canadian respiratory journal 2016;2016:8302179. doi: 735 10.1155/2016/8302179 736
35. Lazzerini M, Seward N, Lufesi N, et al. Mortality and its risk factors in Malawian children 737 admitted to hospital with clinical pneumonia, 2001-12: a retrospective observational 738 study. The Lancet Global health 2016;4(1):e57-68. doi: 10.1016/S2214-109X(15)00215-739 6 740
36. Barton L, Hodgman JE, Pavlova Z. Causes of death in the extremely low birth weight infant. 741 Pediatrics 1999;103(2):446-51. 742
37. Spooner V, Barker J, Tulloch S, et al. Clinical signs and risk factors associated with 743 pneumonia in children admitted to Goroka Hospital, Papua New Guinea. Journal of 744 tropical pediatrics 1989;35(6):295-300. doi: 10.1093/tropej/35.6.295 745
38. Fancourt N, Deloria Knoll M, Baggett HC, et al. Chest Radiograph Findings in Childhood 746 Pneumonia Cases From the Multisite PERCH Study. Clinical infectious diseases : an 747 official publication of the Infectious Diseases Society of America 748 2017;64(suppl_3):S262-S70. doi: 10.1093/cid/cix089 749
39. Moschovis PP, Banajeh S, MacLeod WB, et al. Childhood anemia at high altitude: risk 750 factors for poor outcomes in severe pneumonia. Pediatrics 2013;132(5):e1156-62. doi: 751 10.1542/peds.2013-0761 752
40. Cole TJ, Green PJ. Smoothing reference centile curves: the LMS method and penalized 753 likelihood. Statistics in medicine 1992;11(10):1305-19. 754
41. Jennett B, Teasdale G. Aspects of coma after severe head injury. Lancet 1977;1(8017):878-755 81. 756
42. WHO. Standardization of interpretation of chest radiographs for the diagnosis of 757 pneumonia in children2001. 758
43. Bonroy C, Vankeerberghen A, Boel A, et al. Use of a multiplex real-time PCR to study the 759 incidence of human metapneumovirus and human respiratory syncytial virus infections 760 during two winter seasons in a Belgian paediatric hospital. Clin Microbiol Infect 761 2007;13(5):504-9. doi: 10.1111/j.1469-0691.2007.01682.x 762
44. Matsuzaki Y, Mizuta K, Takashita E, et al. Comparison of virus isolation using the Vero E6 763 cell line with real-time RT-PCR assay for the detection of human metapneumovirus. 764 BMC Infect Dis 2010;10:170. doi: 10.1186/1471-2334-10-170 765
45. Bellau-Pujol S, Vabret A, Legrand L, et al. Development of three multiplex RT-PCR assays for 766 the detection of 12 respiratory RNA viruses. J Virol Methods 2005;126(1-2):53-63. doi: 767 10.1016/j.jviromet.2005.01.020 768
46. Ohno A, Suzuki A, Lupisan S, et al. Genetic characterization of human respiratory syncytial 769 virus detected in hospitalized children in the Philippines from 2008 to 2012. Journal of 770 clinical virology : the official publication of the Pan American Society for Clinical 771 Virology 2013;57(1):59-65. doi: 10.1016/j.jcv.2013.01.001 772

41 | P a g e
47. NIID. https://www.niid.go.jp/niid/images/lab-manual/Influenza2014.pdf 773
2014:36-45. 774 48. Yamamoto D, Okamoto M, Lupisan S, et al. Impact of human adenovirus serotype 7 in 775
hospitalized children with severe fatal pneumonia in the Philippines. Jpn J Infect Dis 776 2014;67(2):105-10. 777
49. Heim A, Ebnet C, Harste G, et al. Rapid and quantitative detection of human adenovirus 778 DNA by real-time PCR. J Med Virol 2003;70(2):228-39. doi: 10.1002/jmv.10382 779
50. Casas I, Avellon A, Mosquera M, et al. Molecular identification of adenoviruses in clinical 780 samples by analyzing a partial hexon genomic region. J Clin Microbiol 781 2005;43(12):6176-82. doi: 10.1128/JCM.43.12.6176-6182.2005 782
51. Gunnarsson RK, Holm SE, Soderstrom M. The prevalence of potential pathogenic bacteria 783 in nasopharyngeal samples from healthy children and adults. Scandinavian journal of 784 primary health care 1998;16(1):13-7. 785
52. WHO. Handbook : IMCI integrated management of childhood illness2005:173. 786 53. Wickham H, François R, Henry L, et al. A Grammar of Data Manipulation. 2018 787 54. Ayieko P, Okiro EA, Edwards T, et al. Variations in mortality in children admitted with 788
pneumonia to Kenyan hospitals. PLoS One 2012;7(11):e47622. doi: 789 10.1371/journal.pone.0047622 790
55. Naheed A, Saha SK, Breiman RF, et al. Multihospital surveillance of pneumonia burden 791 among children aged <5 years hospitalized for pneumonia in Bangladesh. Clin Infect Dis 792 2009;48 Suppl 2:S82-9. doi: 10.1086/596485 793
56. WHO. http://www.who.int/immunization/monitoring_surveillance/data/en/, 2018. 794 57. Walker CLF, Rudan I, Liu L, et al. Global burden of childhood pneumonia and diarrhoea. 795
Lancet 2013;381(9875):1405-16. doi: 10.1016/S0140-6736(13)60222-6 796 58. Simon AK, Hollander GA, McMichael A. Evolution of the immune system in humans from 797
infancy to old age. Proceedings Biological sciences 2015;282(1821):20143085. doi: 798 10.1098/rspb.2014.3085 799
59. Agarwal S, Cunningham-Rundles C. Assessment and clinical interpretation of reduced IgG 800 values. Annals of allergy, asthma & immunology : official publication of the American 801 College of Allergy, Asthma, & Immunology 2007;99(3):281-3. doi: 10.1016/S1081-802 1206(10)60665-5 803
60. Kim SA, Capeding MR, Kilgore PE. Factors influencing healthcare utilization among children 804 with pneumonia in Muntinlupa City, the Philippines. The Southeast Asian journal of 805 tropical medicine and public health 2014;45(3):727-35. 806
61. Caulfield LE, de Onis M, Blossner M, et al. Undernutrition as an underlying cause of child 807 deaths associated with diarrhea, pneumonia, malaria, and measles. Am J Clin Nutr 808 2004;80(1):193-8. doi: 10.1093/ajcn/80.1.193 809
62. Agweyu A, Lilford RJ, English M, et al. Appropriateness of clinical severity classification of 810 new WHO childhood pneumonia guidance: a multi-hospital, retrospective, cohort 811 study. The Lancet Global health 2018;6(1):e74-e83. doi: 10.1016/S2214-812 109X(17)30448-5 813
63. Ahmed T, Mahfuz M, Ireen S, et al. Nutrition of children and women in Bangladesh: trends 814 and directions for the future. Journal of health, population, and nutrition 2012;30(1):1-815 11. 816
64. Akombi BJ, Agho KE, Merom D, et al. Child malnutrition in sub-Saharan Africa: A meta-817 analysis of demographic and health surveys (2006-2016). PLoS One 818 2017;12(5):e0177338. doi: 10.1371/journal.pone.0177338 819
42 | P a g e
65. Kharsany AB, Karim QA. HIV Infection and AIDS in Sub-Saharan Africa: Current Status, 820 Challenges and Opportunities. The open AIDS journal 2016;10:34-48. doi: 821 10.2174/1874613601610010034 822
66. Belderbos ME, Houben ML, Wilbrink B, et al. Cord blood vitamin D deficiency is associated 823 with respiratory syncytial virus bronchiolitis. Pediatrics 2011;127(6):e1513-20. doi: 824 10.1542/peds.2010-3054 825
67. Shakur MS, Malek MA, Bano N, et al. Serum and hair zinc in severely malnourished 826 Bangladeshi children associated with or without acute lower respiratory infection. 827 Indian journal of pediatrics 2009;76(6):609-14. doi: 10.1007/s12098-009-0109-y 828
68. Seth V, Chandra RK. Opsonic activity, phagocytosis, and bactericidal capacity of polymorphs 829 in undernutrition. Arch Dis Child 1972;47(252):282-4. 830
69. Woerther PL, Angebault C, Jacquier H, et al. Massive increase, spread, and exchange of 831 extended spectrum beta-lactamase-encoding genes among intestinal 832 Enterobacteriaceae in hospitalized children with severe acute malnutrition in Niger. 833 Clin Infect Dis 2011;53(7):677-85. doi: 10.1093/cid/cir522 834
70. Michelow IC, Olsen K, Lozano J, et al. Epidemiology and clinical characteristics of 835 community-acquired pneumonia in hospitalized children. Pediatrics 2004;113(4):701-7. 836
71. Subhi R, Adamson M, Campbell H, et al. The prevalence of hypoxaemia among ill children 837 in developing countries: a systematic review. Lancet Infect Dis 2009;9(4):219-27. doi: 838 10.1016/S1473-3099(09)70071-4 839
72. Thomas DS, Anthamatten P, Root ED, et al. Disease mapping for informing targeted health 840 interventions: childhood pneumonia in Bohol, Philippines. Trop Med Int Health 841 2015;20(11):1525-33. doi: 10.1111/tmi.12561 842
73. Duke T, Mgone J, Frank D. Hypoxaemia in children with severe pneumonia in Papua New 843 Guinea. The international journal of tuberculosis and lung disease : the official journal 844 of the International Union against Tuberculosis and Lung Disease 2001;5(6):511-9. 845
74. Onyango FE, Steinhoff MC, Wafula EM, et al. Hypoxaemia in young Kenyan children with 846 acute lower respiratory infection. BMJ 1993;306(6878):612-5. 847
75. Asghar R, Banajeh S, Egas J, et al. Chloramphenicol versus ampicillin plus gentamicin for 848 community acquired very severe pneumonia among children aged 2-59 months in low 849 resource settings: multicentre randomised controlled trial (SPEAR study). BMJ 850 2008;336(7635):80-4. doi: 10.1136/bmj.39421.435949.BE 851
76. Kelly MS, Crotty EJ, Rattan MS, et al. Chest Radiographic Findings and Outcomes of 852 Pneumonia Among Children in Botswana. Pediatr Infect Dis J 2016;35(3):257-62. doi: 853 10.1097/INF.0000000000000990 854
77. Basnet S, Sharma A, Mathisen M, et al. Predictors of duration and treatment failure of 855 severe pneumonia in hospitalized young Nepalese children. PLoS One 856 2015;10(3):e0122052. doi: 10.1371/journal.pone.0122052 857
78. Benet T, Picot VS, Awasthi S, et al. Severity of Pneumonia in Under 5-Year-Old Children 858 from Developing Countries: A Multicenter, Prospective, Observational Study. Am J 859 Trop Med Hyg 2017;97(1):68-76. doi: 10.4269/ajtmh.16-0733 860
79. Peled N, Nakar C, Huberman H, et al. Adenovirus infection in hospitalized 861 immunocompetent children. Clinical pediatrics 2004;43(3):223-9. doi: 862 10.1177/000992280404300303 863
80. Wu PQ, Li X, Jiang WH, et al. Hypoxemia is an independent predictor of bronchiolitis 864 obliterans following respiratory adenoviral infection in children. SpringerPlus 865 2016;5(1):1622. doi: 10.1186/s40064-016-3237-7 866

43 | P a g e
81. Ghanaiem H, Averbuch D, Koplewitz BZ, et al. An outbreak of adenovirus type 7 in a 867 residential facility for severely disabled children. Pediatr Infect Dis J 2011;30(11):948-868 52. doi: 10.1097/INF.0b013e31822702fe 869
82. Tran DN, Trinh QD, Pham NT, et al. Clinical and epidemiological characteristics of acute 870 respiratory virus infections in Vietnamese children. Epidemiol Infect 2016;144(3):527-871 36. doi: 10.1017/S095026881500134X 872
83. Riccetto AG, Ribeiro JD, Silva MT, et al. Respiratory syncytial virus (RSV) in infants 873 hospitalized for acute lower respiratory tract disease: incidence and associated risks. 874 The Brazilian journal of infectious diseases : an official publication of the Brazilian 875 Society of Infectious Diseases 2006;10(5):357-61. 876
84. Floyd J, Wu L, Hay Burgess D, et al. Evaluating the impact of pulse oximetry on childhood 877 pneumonia mortality in resource-poor settings. Nature 2015;528(7580):S53-9. doi: 878 10.1038/nature16043 879
85. McCollum ED, King C, Deula R, et al. Pulse oximetry for children with pneumonia treated as 880 outpatients in rural Malawi. Bulletin of the World Health Organization 881 2016;94(12):893-902. doi: 10.2471/BLT.16.173401 882
86. Yu Z, Zeng Z, Zhang J, et al. Fatal Community-acquired Pneumonia in Children Caused by 883 Re-emergent Human Adenovirus 7d Associated with Higher Severity of Illness and 884 Fatality Rate. Sci Rep 2016;6:37216. doi: 10.1038/srep37216 885
87. Shen CF, Wang SM, Ho TS, et al. Clinical features of community acquired adenovirus 886 pneumonia during the 2011 community outbreak in Southern Taiwan: role of host 887 immune response. BMC Infect Dis 2017;17(1):196. doi: 10.1186/s12879-017-2272-5 888
88. Rao S, Messacar K, Torok MR, et al. Enterovirus D68 in Critically Ill Children: A Comparison 889 With Pandemic H1N1 Influenza. Pediatric critical care medicine : a journal of the 890 Society of Critical Care Medicine and the World Federation of Pediatric Intensive and 891 Critical Care Societies 2016;17(11):1023-31. doi: 10.1097/PCC.0000000000000922 892
89. Midgley CM, Watson JT, Nix WA, et al. Severe respiratory illness associated with a 893 nationwide outbreak of enterovirus D68 in the USA (2014): a descriptive 894 epidemiological investigation. The Lancet Respiratory medicine 2015;3(11):879-87. doi: 895 10.1016/S2213-2600(15)00335-5 896
90. Imamura T, Oshitani H. Global reemergence of enterovirus D68 as an important pathogen 897 for acute respiratory infections. Rev Med Virol 2015;25(2):102-14. doi: 898 10.1002/rmv.1820 899
91. Kelly MS, Smieja M, Luinstra K, et al. Association of respiratory viruses with outcomes of 900 severe childhood pneumonia in Botswana. PloS one 2015;10(5):e0126593. doi: 901 10.1371/journal.pone.0126593 902
92. Szabo SM, Gooch KL, Bibby MM, et al. The risk of mortality among young children 903 hospitalized for severe respiratory syncytial virus infection. Paediatric respiratory 904 reviews 2013;13 Suppl 2:S1-8. doi: 10.1016/S1526-0542(12)00095-4 905
93. Welliver RC, Sr., Checchia PA, Bauman JH, et al. Fatality rates in published reports of RSV 906 hospitalizations among high-risk and otherwise healthy children. Current medical 907 research and opinion 2010;26(9):2175-81. doi: 10.1185/03007995.2010.505126 908
94. Oladokun R, Muloiwa R, Hsiao NY, et al. Clinical characterisation and phylogeny of 909 respiratory syncytial virus infection in hospitalised children at Red Cross War Memorial 910 Children's Hospital, Cape Town. BMC infectious diseases 2016;16:236. doi: 911 10.1186/s12879-016-1572-5 912
95. Kiang D, Yagi S, Kantardjieff KA, et al. Molecular characterization of a variant rhinovirus 913 from an outbreak associated with uncommonly high mortality. Journal of clinical 914

44 | P a g e
virology : the official publication of the Pan American Society for Clinical Virology 915 2007;38(3):227-37. doi: 10.1016/j.jcv.2006.12.016 916
96. Cebey-Lopez M, Herberg J, Pardo-Seco J, et al. Does Viral Co-Infection Influence the 917 Severity of Acute Respiratory Infection in Children? PLoS One 2016;11(4):e0152481. 918 doi: 10.1371/journal.pone.0152481 919
97. Toivonen L, Schuez-Havupalo L, Karppinen S, et al. Rhinovirus Infections in the First 2 Years 920 of Life. Pediatrics 2016;138(3) doi: 10.1542/peds.2016-1309 921
98. Munywoki PK, Koech DC, Agoti CN, et al. Frequent Asymptomatic Respiratory Syncytial 922 Virus Infections During an Epidemic in a Rural Kenyan Household Cohort. J Infect Dis 923 2015;212(11):1711-8. doi: 10.1093/infdis/jiv263 924
99. McMullan BJ, Bowen A, Blyth CC, et al. Epidemiology and Mortality of Staphylococcus 925 aureus Bacteremia in Australian and New Zealand Children. JAMA Pediatr 926 2016;170(10):979-86. doi: 10.1001/jamapediatrics.2016.1477 927
100. McGowan JE, Jr., Bratton L, Klein JO, et al. Bacteremia in febrile children seen in a "walk-928 in" pediatric clinic. N Engl J Med 1973;288(25):1309-12. doi: 929 10.1056/NEJM197306212882501 930
101. Al-Talib HI, Yean CY, Al-Jashamy K, et al. Methicillin-resistant Staphylococcus aureus 931 nosocomial infection trends in Hospital Universiti Sains Malaysia during 2002-2007. 932 Annals of Saudi medicine 2010;30(5):358-63. doi: 10.4103/0256-4947.67077 933
102. Doit C, Loukil C, Simon AM, et al. Outbreak of Burkholderia cepacia bacteremia in a 934 pediatric hospital due to contamination of lipid emulsion stoppers. J Clin Microbiol 935 2004;42(5):2227-30. 936
103. Srinivasan S, Arora NC, Sahai K. Report on the newly emerging nosocomial Burkholderia 937 cepacia in a tertiary hospital. Medical journal, Armed Forces India 2016;72(Suppl 938 1):S50-S53. doi: 10.1016/j.mjafi.2016.03.003 939
104. Howard A, O'Donoghue M, Feeney A, et al. Acinetobacter baumannii: an emerging 940 opportunistic pathogen. Virulence 2012;3(3):243-50. doi: 10.4161/viru.19700 941
105. Puumalainen T, Quiambao B, Abucejo-Ladesma E, et al. Clinical case review: a method to 942 improve identification of true clinical and radiographic pneumonia in children meeting 943 the World Health Organization definition for pneumonia. BMC Infect Dis 2008;8:95. 944 doi: 10.1186/1471-2334-8-95 945
106. Murdoch DR, O'Brien KL, Driscoll AJ, et al. Laboratory methods for determining 946 pneumonia etiology in children. Clinical infectious diseases : an official publication of 947 the Infectious Diseases Society of America 2012;54 Suppl 2:S146-52. doi: 948 10.1093/cid/cir1073 949
107. Shah SS, Dugan MH, Bell LM, et al. Blood cultures in the emergency department 950 evaluation of childhood pneumonia. Pediatr Infect Dis J 2011;30(6):475-9. doi: 951 10.1097/INF.0b013e31820a5adb 952
108. Rodrigues CMC, Groves H. Community-Acquired Pneumonia in Children: the Challenges of 953 Microbiological Diagnosis. J Clin Microbiol 2018;56(3) doi: 10.1128/JCM.01318-17 954
109. Liu P, Xu M, He L, et al. Epidemiology of Respiratory Pathogens in Children with Lower 955 Respiratory Tract Infections in Shanghai, China, from 2013 to 2015. Jpn J Infect Dis 956 2018;71(1):39-44. doi: 10.7883/yoken.JJID.2017.323 957
110. Iroh Tam PY, Bernstein E, Ma X, et al. Blood Culture in Evaluation of Pediatric Community-958 Acquired Pneumonia: A Systematic Review and Meta-analysis. Hospital pediatrics 959 2015;5(6):324-36. doi: 10.1542/hpeds.2014-0138 960
111. Leibovitz E, Rigaud M, Pollack H, et al. Pneumocystis carinii pneumonia in infants infected 961 with the human immunodeficiency virus with more than 450 CD4 T lymphocytes per 962
45 | P a g e
cubic millimeter. N Engl J Med 1990;323(8):531-3. doi: 963 10.1056/NEJM199008233230807 964
965
966
967
968
969

46 | P a g e
970
Figure1. Map depicting the location of study sites participating in the childhood pneumonia 971 study in the Philippines, 2008-2016. A dot indicates hospital location and the color refers to 972 hospital name. hospital coordinates were recorded by using google maps and mapped the 973 geographical distribution of hospital with ArcGIS 10.4 (ESRI, Redlands, CA, USA). This study 974 used the administrative boundaries of The Philippines from the PhilGIS website 975 (http://philgis.org/ and then we overlaid the administrative boundaries layer with openstreetmap 976 tool in ArcGIS 10.4 (ESRI, Redlands, CA, USA)). 977
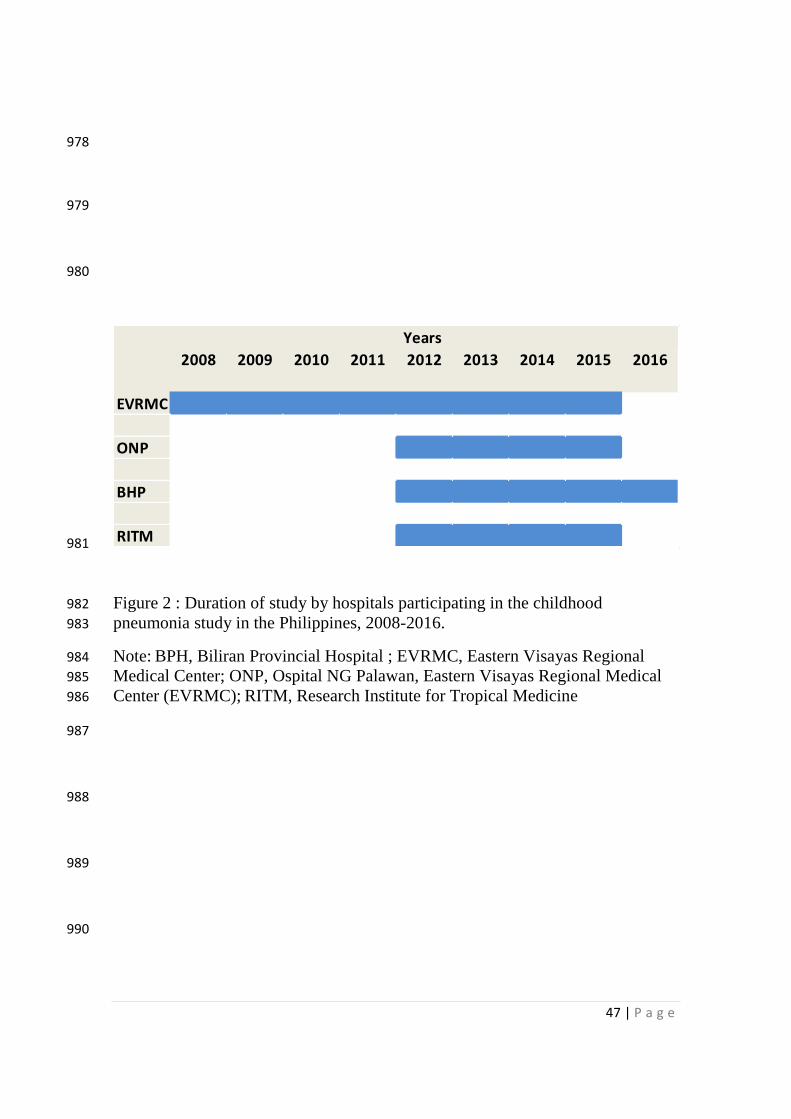
47 | P a g e
978
979
980
981
Figure 2 : Duration of study by hospitals participating in the childhood 982
pneumonia study in the Philippines, 2008-2016. 983
Note: BPH, Biliran Provincial Hospital ; EVRMC, Eastern Visayas Regional 984
Medical Center; ONP, Ospital NG Palawan, Eastern Visayas Regional Medical 985
Center (EVRMC); RITM, Research Institute for Tropical Medicine 986
987
988
989
990
2008 2009 2010 2011 2012 2013 2014 2015 2016
EVRMC
ONP
BHP
RITM
Years

48 | P a g e
991
992
993
994
995
996
997
998
999
1000
1001
1002
DAMA, discharged against medical advice 1003
Figure 3: Flowchart of study participants in the childhood pneumonia study 1004
in Philippines, 2008-2016. 1005
Loss to follow up, unknown
outcome, transferred to
another hospital (n=74)
Were included in analysis
1112 (22%) patients in sociodemographic and economic status study
5054 patients with medical records
4336(85.8%) measurement of saturation of oxygen
5054 nasopharyngeal result tested for different viruses 4452 (88 %) of chest radiographs 3018 (60%) of blood culture for identification of bacteria done (49 bacteria were diagnosed)
Children <2month
Survived (n: 709) made of
Survived observed in hospital (n: 605)
DAMA improved (n: 104)
Fatal outcomes (n: 40) made of:
Deaths observed in hospital (n= 28)
And DAMA Deteriorated (n=12).
Study period: 2008-2016
Enrolled patients
Severe and very severe pneumonia cases
(N= 5128)
Children 2-59 months
Survived: (n: 4107) made of
Survived observed in hospital (n: 3722)
DAMA improved (n: 385)
Fatal outcomes (n: 198), made of:
Deaths observed in hospital (n= 165)
And DAMA Deteriorated (n=33).
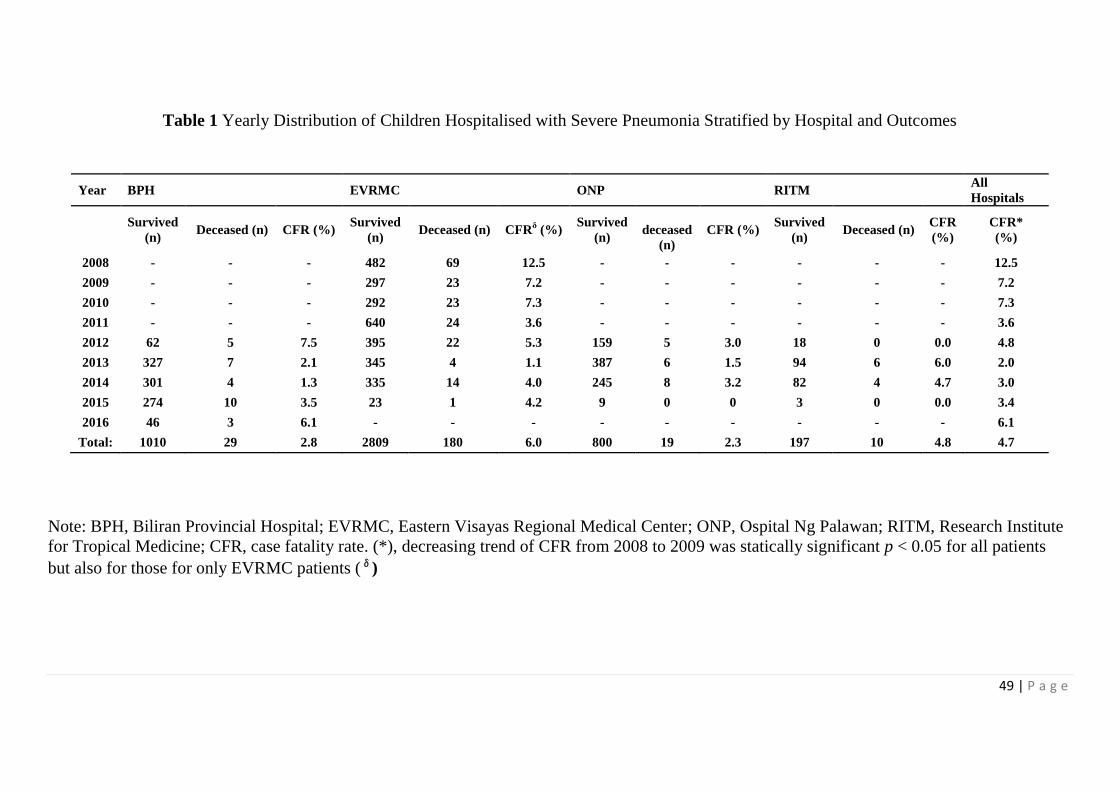
49 | P a g e
Table 1 Yearly Distribution of Children Hospitalised with Severe Pneumonia Stratified by Hospital and Outcomes
Year BPH EVRMC ONP RITM All
Hospitals
Survived
(n) Deceased (n) CFR (%)
Survived
(n) Deceased (n) CFR
δ (%)
Survived
(n)
deceased
(n)
CFR (%) Survived
(n) Deceased (n)
CFR
(%)
CFR*
(%)
2008 - - - 482 69 12.5 - - - - - - 12.5
2009 - - - 297 23 7.2 - - - - - - 7.2
2010 - - - 292 23 7.3 - - - - - - 7.3
2011 - - - 640 24 3.6 - - - - - - 3.6
2012 62 5 7.5 395 22 5.3 159 5 3.0 18 0 0.0 4.8
2013 327 7 2.1 345 4 1.1 387 6 1.5 94 6 6.0 2.0
2014 301 4 1.3 335 14 4.0 245 8 3.2 82 4 4.7 3.0
2015 274 10 3.5 23 1 4.2 9 0 0 3 0 0.0 3.4
2016 46 3 6.1 - - - - - - - - - 6.1
Total: 1010 29 2.8 2809 180 6.0 800 19 2.3 197 10 4.8 4.7
Note: BPH, Biliran Provincial Hospital; EVRMC, Eastern Visayas Regional Medical Center; ONP, Ospital Ng Palawan; RITM, Research Institute
for Tropical Medicine; CFR, case fatality rate. (*), decreasing trend of CFR from 2008 to 2009 was statically significant p < 0.05 for all patients
but also for those for only EVRMC patients (δ)
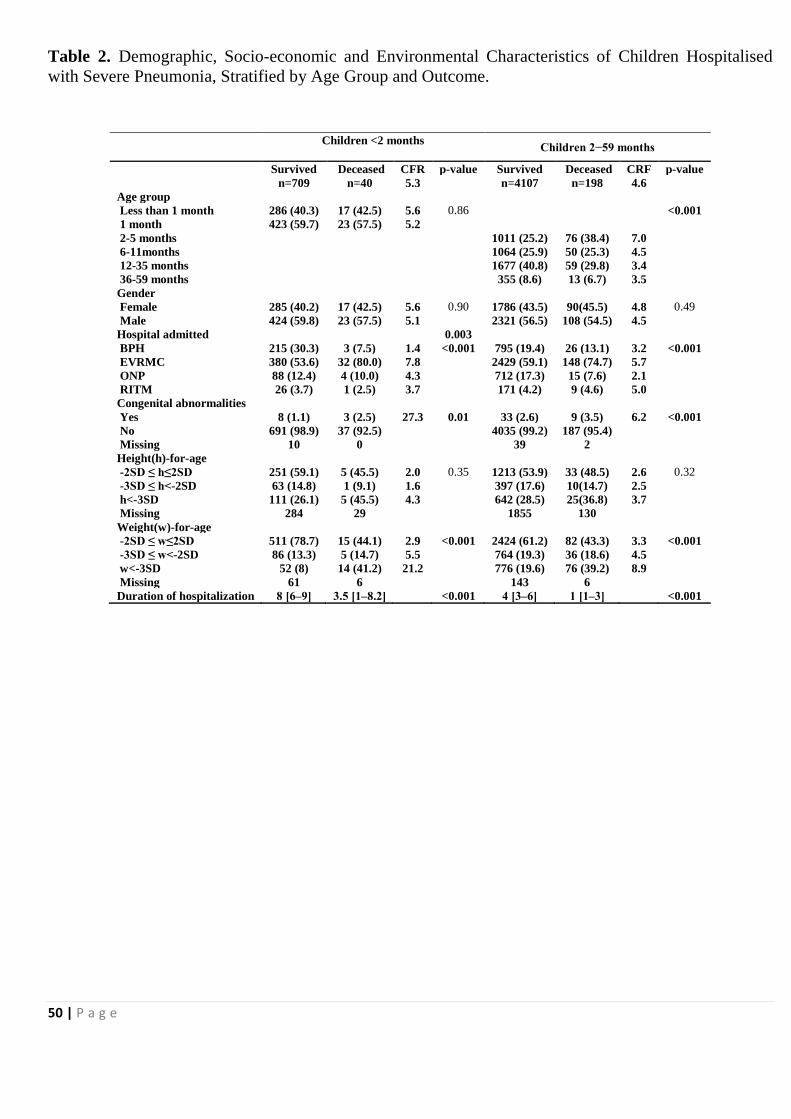
50 | P a g e
Table 2. Demographic, Socio-economic and Environmental Characteristics of Children Hospitalised
with Severe Pneumonia, Stratified by Age Group and Outcome.
Children <2 months
Children 2−59 months
Survived Deceased CFR p-value Survived Deceased CRF p-value
n=709 n=40 5.3 n=4107 n=198 4.6
Age group
Less than 1 month 286 (40.3) 17 (42.5) 5.6 0.86 <0.001
1 month 423 (59.7) 23 (57.5) 5.2
2-5 months 1011 (25.2) 76 (38.4) 7.0
6-11months
1064 (25.9) 50 (25.3) 4.5
12-35 months
1677 (40.8) 59 (29.8) 3.4
36-59 months
355 (8.6) 13 (6.7) 3.5 Gender
Female 285 (40.2) 17 (42.5) 5.6 0.90 1786 (43.5) 90(45.5) 4.8 0.49
Male 424 (59.8) 23 (57.5) 5.1 2321 (56.5) 108 (54.5) 4.5
Hospital admitted
0.003
BPH 215 (30.3) 3 (7.5) 1.4 <0.001 795 (19.4) 26 (13.1) 3.2 <0.001
EVRMC 380 (53.6) 32 (80.0) 7.8
2429 (59.1) 148 (74.7) 5.7
ONP 88 (12.4) 4 (10.0) 4.3
712 (17.3) 15 (7.6) 2.1
RITM 26 (3.7) 1 (2.5) 3.7
171 (4.2) 9 (4.6) 5.0 Congenital abnormalities
Yes 8 (1.1) 3 (2.5) 27.3 0.01 33 (2.6) 9 (3.5) 6.2 <0.001
No 691 (98.9) 37 (92.5) 4035 (99.2) 187 (95.4)
Missing 10 0 39 2
Height(h)-for-age
-2SD ≤ h≤2SD 251 (59.1) 5 (45.5) 2.0 0.35 1213 (53.9) 33 (48.5) 2.6 0.32
-3SD ≤ h<-2SD 63 (14.8) 1 (9.1) 1.6 397 (17.6) 10(14.7) 2.5
h<-3SD 111 (26.1) 5 (45.5) 4.3 642 (28.5) 25(36.8) 3.7
Missing 284 29 1855 130
Weight(w)-for-age
-2SD ≤ w≤2SD 511 (78.7) 15 (44.1) 2.9 <0.001 2424 (61.2) 82 (43.3) 3.3 <0.001
-3SD ≤ w<-2SD 86 (13.3) 5 (14.7) 5.5 764 (19.3) 36 (18.6) 4.5
w<-3SD 52 (8) 14 (41.2) 21.2 776 (19.6) 76 (39.2) 8.9
Missing 61 6 143 6
Duration of hospitalization 8 [6‒9] 3.5 [1‒8.2] <0.001 4 [3‒6] 1 [1‒3] <0.001
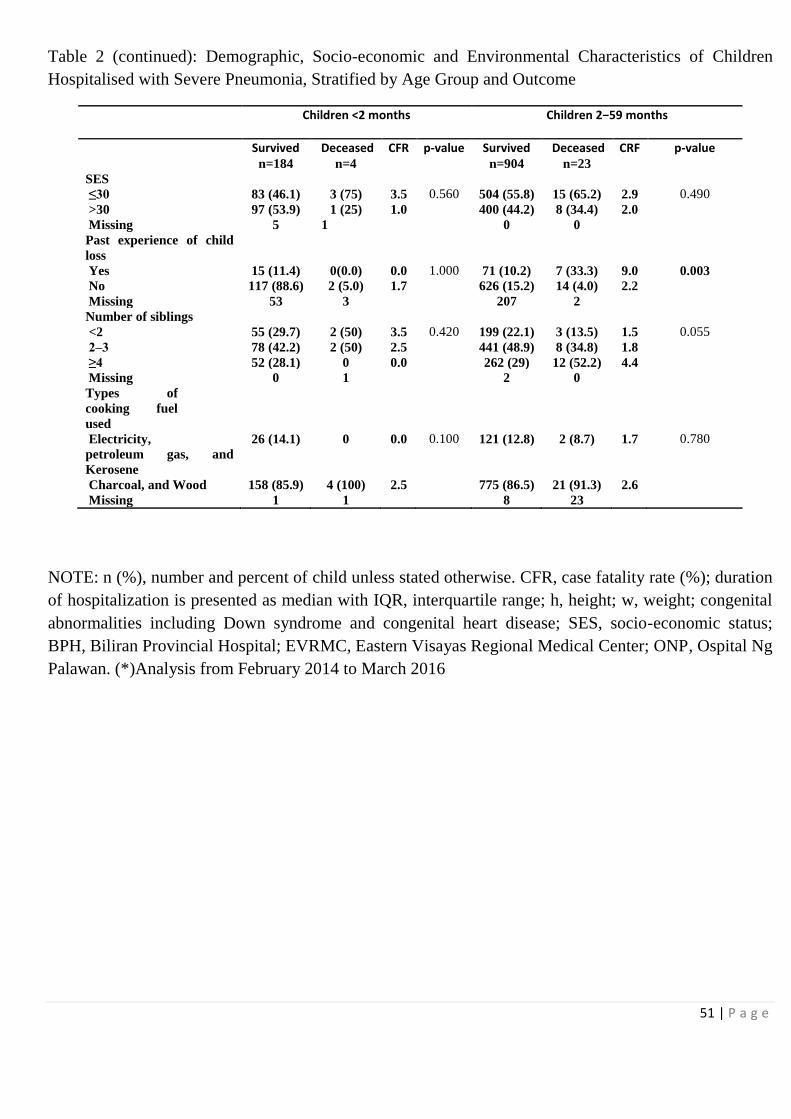
51 | P a g e
Table 2 (continued): Demographic, Socio-economic and Environmental Characteristics of Children
Hospitalised with Severe Pneumonia, Stratified by Age Group and Outcome
Children <2 months
Children 2−59 months
Survived Deceased CFR p-value Survived Deceased CRF p-value
n=184 n=4 n=904 n=23
SES ≤30 83 (46.1) 3 (75) 3.5 0.560 504 (55.8) 15 (65.2) 2.9 0.490
>30 97 (53.9) 1 (25) 1.0 400 (44.2) 8 (34.4) 2.0
Missing 5 1 0 0
Past experience of child
loss
Yes 15 (11.4) 0(0.0) 0.0 1.000 71 (10.2) 7 (33.3) 9.0 0.003
No 117 (88.6) 2 (5.0) 1.7 626 (15.2) 14 (4.0) 2.2
Missing 53 3 207 2
Number of siblings <2 55 (29.7) 2 (50) 3.5 0.420 199 (22.1) 3 (13.5) 1.5 0.055
2‒3 78 (42.2) 2 (50) 2.5 441 (48.9) 8 (34.8) 1.8
≥4 52 (28.1) 0 0.0 262 (29) 12 (52.2) 4.4
Missing 0 1 2 0
Types of
cooking fuel
used
Electricity,
petroleum gas, and
Kerosene
26 (14.1) 0 0.0 0.100 121 (12.8) 2 (8.7) 1.7 0.780
Charcoal, and Wood 158 (85.9) 4 (100) 2.5 775 (86.5) 21 (91.3) 2.6
Missing 1 1 8 23
NOTE: n (%), number and percent of child unless stated otherwise. CFR, case fatality rate (%); duration
of hospitalization is presented as median with IQR, interquartile range; h, height; w, weight; congenital
abnormalities including Down syndrome and congenital heart disease; SES, socio-economic status;
BPH, Biliran Provincial Hospital; EVRMC, Eastern Visayas Regional Medical Center; ONP, Ospital Ng
Palawan. (*)Analysis from February 2014 to March 2016

52 | P a g e
Table 3. Clinical and Laboratory Findings of Children Hospitalised with Severe Pneumonia, Stratified
by Age Group and Outcome
Children < 2 months
Children-2−59 months
Survived Deceased CFR p-value Survived Deceased CFR p-value Clinical findings n=709 n=40 5.3 n=4107 n=198 4.6 Neck rigidity Yes 2 (0.4) 0(0.0) 0.0 1.000 6 (0.1) 2 ( 2.7) 25.0 0.008 No 457 (99.6) 12 (100) 2433 (99.8) 71 (97.3) Missing 250 28 1668 125 Sensorial changes Yes 26 (3.7) 10 (25.0) 27.8 <0.001 146 (4.0) 51 (28.8) 25.9 <0.001 No 608 (95.9) 28 (73.7) 3466 (96) 126 (71.2) Missing 75 2 495 21 Glasgow coma scale Severe 1 (14.3) 1 (50.0) 50.0 0.140 2 (3.6) 5 (62.5) 71.4 <0.001 Moderate 6 (85.7) 1(50) 54 (96.4) 4 (50) Missing 702 38 4051 31 Grunting Yes 4 (0.9) 2 (18.2) 33.3 <0.001 13 (0.5) 6 (8.2) 31.6 <0.001 No 455 (99.1) 9(81.8) 2427 (99.5) 67 (91.8) Missing 250 29 1667 125 Decreased breath sounds Yes 15 (2.1) 4 (10.0) 21.1 0.010 81 (2.0) 12 (6.1) 12.9 <0.001 No 694 (97.9) 36 (90.0) 4022 (98.0) 186 (93.9) Missing 0 0 4 0 Wheezing Yes 91 (12.8) 9 (22.5) 9.0 0.130 1454 (35.4) 84 (42.4) 5.5 0.040 No 618 (87.2) 31(77.5) 2650 (64.6) 113 (57.4) Missing 0 0 0 1 Chest indrawing Yes 704 (99.3) 38 (95) 5.1 0.050 4080 (99.4) 196 (99.0) 4.6 0.730 No 5 (0.7) 2 (5) 23 (0.6) 2 (1) Missing 0 0 4 0 Rales Yes 693 (97.7) 39 (97.5) 5.3 1.000 4083 (99.5) 197 (99.5) 4.6 1.000 No 16 (2.3) 1(2.5) 21 (0.5) 1 (0.5) Missing 0 0 3 1 Central cyanosis Yes 22 (3.1) 8 (20.0) 26.7 <0.001 45 (1.1) 47 (23.9) 51.1 <0.001 No 687 (96.9) 32 (80) 4056 (98.9) 150 (76.1) Missing 0 0 6 1 Apnoeic episode Yes 3 (0.4) 3 (7.5) 50.0 <0.001 2 (0.04) 14 (7.1) 87.5 <0.001 No 706 (99.6) 37 (92.5) 4098 (99.06) 183 (92.9) Missing 0 0 7 1 Nasal flaring Yes 183 (39.9) 8 (66.1) 4.2 0.110 996 (40.8) 39 (53.4) 3.8 0.040 No 276 (60.1) 4 (33.3) 1444 (59.2) 34 (46.6) Missing 250 28 1667 125 Tachypnea Yes 594 (84.4) 35 (92.1) 5.6 0.250 3428 (83.8) 169 (91.4) 4.7 <0.001 No 110 (15.6) 3 (7.9) 663 (16.2) 16 (8.6) Missing 5 2 16 13 SpO2<90% Yes 75 (10.7) 14 (35.0) 15.7 <0.001 494 (12.1) 71 (36.0) 12.6 0.005 No 629 (89.3) 26 (65.0) 3588 (87.9) 126 (64.0) Missing 5 0 25 1
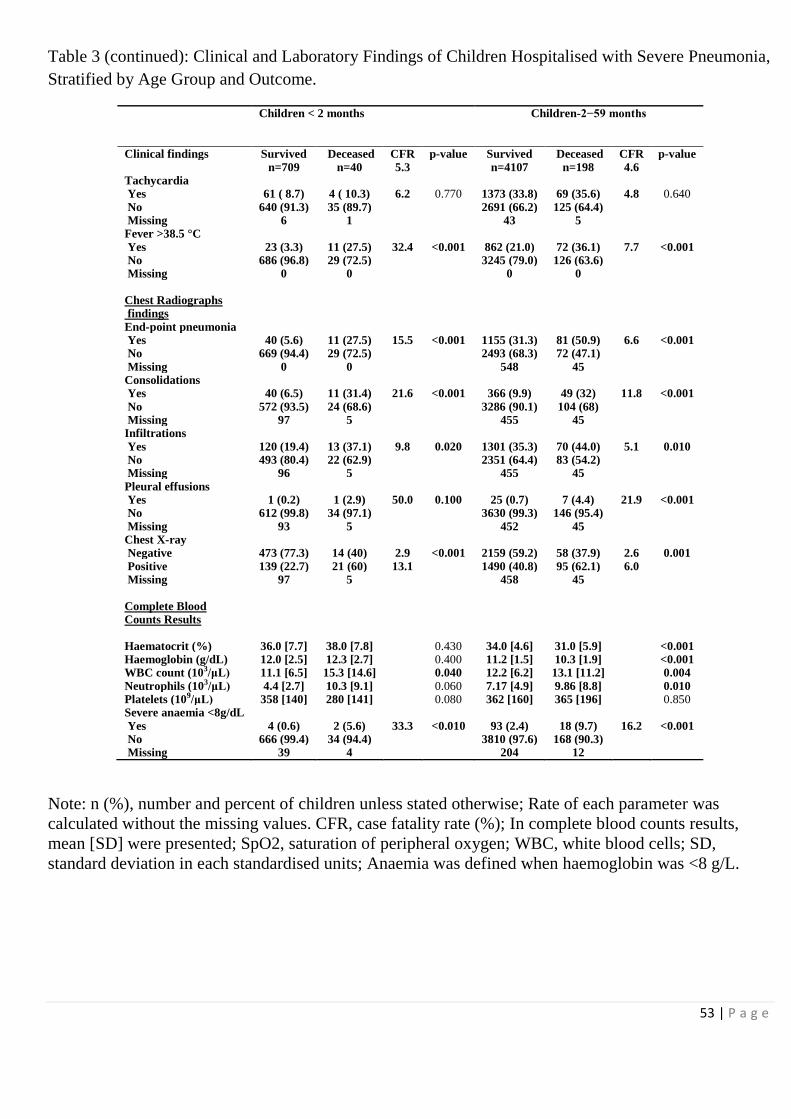
53 | P a g e
Table 3 (continued): Clinical and Laboratory Findings of Children Hospitalised with Severe Pneumonia,
Stratified by Age Group and Outcome.
Children < 2 months
Children-2−59 months
Clinical findings Survived Deceased CFR p-value Survived Deceased CFR p-value
n=709 n=40 5.3 n=4107 n=198 4.6 Tachycardia Yes 61 ( 8.7) 4 ( 10.3) 6.2 0.770 1373 (33.8) 69 (35.6) 4.8 0.640 No 640 (91.3) 35 (89.7) 2691 (66.2) 125 (64.4) Missing 6 1 43 5 Fever >38.5 °C
Yes 23 (3.3) 11 (27.5) 32.4 <0.001 862 (21.0) 72 (36.1) 7.7 <0.001 No 686 (96.8) 29 (72.5) 3245 (79.0) 126 (63.6) Missing 0 0 0 0
Chest Radiographs findings
End-point pneumonia Yes 40 (5.6) 11 (27.5) 15.5 <0.001 1155 (31.3) 81 (50.9) 6.6 <0.001 No 669 (94.4) 29 (72.5) 2493 (68.3) 72 (47.1)
Missing 0 0 548 45 Consolidations Yes 40 (6.5) 11 (31.4) 21.6 <0.001 366 (9.9) 49 (32) 11.8 <0.001
No 572 (93.5) 24 (68.6) 3286 (90.1) 104 (68) Missing 97 5 455 45 Infiltrations
Yes 120 (19.4) 13 (37.1) 9.8 0.020 1301 (35.3) 70 (44.0) 5.1 0.010 No 493 (80.4) 22 (62.9) 2351 (64.4) 83 (54.2) Missing 96 5 455 45
Pleural effusions Yes 1 (0.2) 1 (2.9) 50.0 0.100 25 (0.7) 7 (4.4) 21.9 <0.001 No 612 (99.8) 34 (97.1) 3630 (99.3) 146 (95.4)
Missing 93 5 452 45 Chest X-ray Negative 473 (77.3) 14 (40) 2.9 <0.001 2159 (59.2) 58 (37.9) 2.6 0.001
Positive 139 (22.7) 21 (60) 13.1 1490 (40.8) 95 (62.1) 6.0 Missing 97 5 458 45
Complete Blood Counts Results
Haematocrit (%) 36.0 [7.7] 38.0 [7.8] 0.430 34.0 [4.6] 31.0 [5.9] <0.001 Haemoglobin (g/dL) 12.0 [2.5] 12.3 [2.7] 0.400 11.2 [1.5] 10.3 [1.9] <0.001 WBC count (103/μL) 11.1 [6.5] 15.3 [14.6] 0.040 12.2 [6.2] 13.1 [11.2] 0.004
Neutrophils (103/μL) 4.4 [2.7] 10.3 [9.1] 0.060 7.17 [4.9] 9.86 [8.8] 0.010 Platelets (109/μL) 358 [140] 280 [141] 0.080 362 [160] 365 [196] 0.850 Severe anaemia <8g/dL
Yes 4 (0.6) 2 (5.6) 33.3 <0.010 93 (2.4) 18 (9.7) 16.2 <0.001 No 666 (99.4) 34 (94.4) 3810 (97.6) 168 (90.3) Missing 39 4 204 12
Note: n (%), number and percent of children unless stated otherwise; Rate of each parameter was
calculated without the missing values. CFR, case fatality rate (%); In complete blood counts results,
mean [SD] were presented; SpO2, saturation of peripheral oxygen; WBC, white blood cells; SD,
standard deviation in each standardised units; Anaemia was defined when haemoglobin was <8 g/L.

54 | P a g e
Table 4 Factors Associated With Death Among Children Hospitalised With Severe Pneumonia,
Stratified By Age Group.
Children <2 months Children -2−59 months
Factors Crude OR (95% C.I.)
Adjusted OR (95% C.I.)
Crude OR (95% C.I.)
Adjusted OR (95% C.I.)
Age group
Less than 1 month Ref. Ref. - -
1 month 0.93 (0.6-1.5) 0.9 (0.57-1.44) - -
2 - 5 months - - 1.73 (1.17-2.69) 1.77 (1.19-2.75)
6-11months - - 1.29 (0.89-1.82) 1.29 (0.89-1.82)
12-35 months - - 0.97 (0.72-1.3) 0.96 (0.72-1.29)
36-59 months - - Ref Ref
Past experience of child loss NA NA 4.9 (1.83-11.87) 5.42 (1.99-13.51)
Weight(w)-for-age
-2SD ≤ w≤2SD Ref. Ref. Ref Ref
-3SD ≤ w<-2SD 1.98 (0.63-5.25) 1.98 (0.62-5.33) 1.41 (0.93-2.1) 1.58 (1.04-2.35)
w<-3SD 9.15 (4.15-20.12) 9.59 (4.22-21.88) 2.93 (2.12-4.05) 3.22 (2.3-4.51)
Presence of
congenital abnormalities 7.0(1.49-25.35) 1.96 (0.08-2.43) 5.88 (2.62-11.97) 3.12 (1.08-8.62)
Decreased breath sounds 5.14 (1.41-15.03) 9.81 (2.11-46.49) 3.2 (1.64-5.76) 5.36 (2.6-10.38)
Grunting 25.28 (3.22-148.64) 28.65 (2.89-259.6) 16.72 (5.73-43.71) 14.27 (4.64-39.86)
Sensorial changes 1.59 (1.01-3.3) 1.79 (1.13-3.22) 9.61 (6.63-13.78) 8.31 (5.68-12.0)
Glasgow coma scale<9 6.0 (0.15-321.95) - 45.0 (6.92-437.72) -
Central cyanosis 7.81 (3.07-18.33) 6.49 (2.50-15.63) 28.24 (18.19-43.95) 27.58 (17.55-43.5)
Tachypnea 1.20 (0.35-3.13) 2.03 (0.7-8.6) 2.04 (1.25-3.57) 1.89 (1.15-3.34)
Tachycardia 2.16 (0.76-9.07) 2.03 (0.56-5.84) 1.08 (0.8-1.46) 2.09 (1.42-3.07)
SpO2<90% 4.52 (2.21-8.91) 4.69 (2.23-9.56) 4.09 (3.0-5.54) 5.06 (3.67-6.94)
Wheeze 1.97 (0.86-4.12) 2.87 (1.11-6.87) 1.35 (1.01-1.81) 1.55 (1.15-2.08)
Fever (>38.5 °C) 11.31 (4.9-25.07) 11.98 (5.03-27.87) 2.15 (1.59-2.89) 2.5(1.83-3.38)
Severe anaemia (<8 g/dL) 9.79 (1.32-52.0) 9.18 (1.18-54.0) 4.39 (2.51-7.27) 4.04 (2.29-6.8)
Endpoint pneumonia 5.55 (2.76-11.24) 5.64 (2.74-11.68) 2.43 (1.75-3.36) 2.67 (1.92-3.73)
Consolidation 6.55 (2.91-14.08) 5.37 (2.34-11.77) 4.23 (2.94-6.0) 4.11 (2.84-5.88)
Infiltration 2.43 (1.16-4.9) 2.70 (1.26-5.57) 1.52 (1.1-2.11) 1.71 (1.23-2.38)
Pleural effusion 18.0 (0.7-461.79) 23.0 (0.76-949.37) 6.96 (2.74-15.54) 6.85 (2.66-15.63)
Note: SpO2, saturation of peripheral oxygen; OR, odds ratio; CI, confidence interval.
Multivariate logistic models were adjusted by age in month, year of sampling and hospitals.
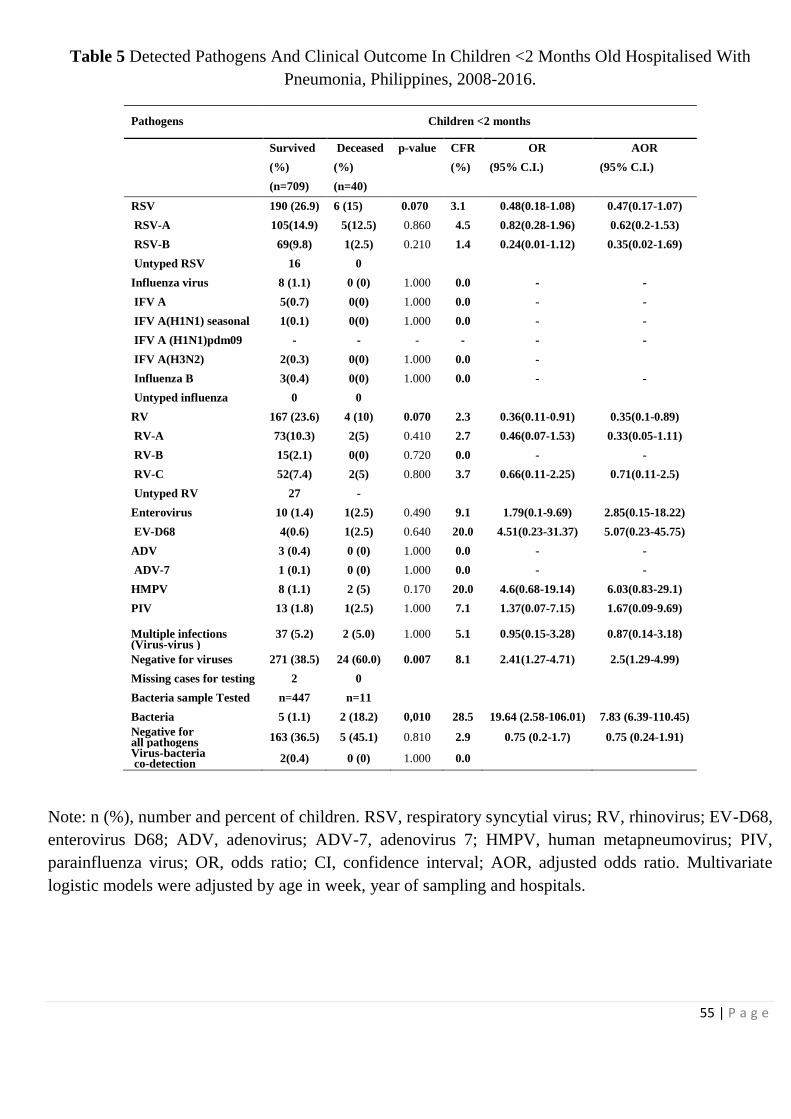
55 | P a g e
Table 5 Detected Pathogens And Clinical Outcome In Children <2 Months Old Hospitalised With
Pneumonia, Philippines, 2008-2016.
Pathogens
Children <2 months
Survived Deceased p-value CFR OR AOR
(%) (%)
(%) (95% C.I.) (95% C.I.)
(n=709) (n=40)
RSV 190 (26.9) 6 (15) 0.070 3.1 0.48(0.18-1.08) 0.47(0.17-1.07)
RSV-A 105(14.9) 5(12.5) 0.860 4.5 0.82(0.28-1.96) 0.62(0.2-1.53)
RSV-B 69(9.8) 1(2.5) 0.210 1.4 0.24(0.01-1.12) 0.35(0.02-1.69)
Untyped RSV 16 0
Influenza virus 8 (1.1) 0 (0) 1.000 0.0 - -
IFV A 5(0.7) 0(0) 1.000 0.0 - -
IFV A(H1N1) seasonal 1(0.1) 0(0) 1.000 0.0 - -
IFV A (H1N1)pdm09 - - - - - -
IFV A(H3N2) 2(0.3) 0(0) 1.000 0.0 -
Influenza B 3(0.4) 0(0) 1.000 0.0 - -
Untyped influenza 0 0
RV 167 (23.6) 4 (10) 0.070 2.3 0.36(0.11-0.91) 0.35(0.1-0.89)
RV-A 73(10.3) 2(5) 0.410 2.7 0.46(0.07-1.53) 0.33(0.05-1.11)
RV-B 15(2.1) 0(0) 0.720 0.0 - -
RV-C 52(7.4) 2(5) 0.800 3.7 0.66(0.11-2.25) 0.71(0.11-2.5)
Untyped RV 27 -
Enterovirus 10 (1.4) 1(2.5) 0.490 9.1 1.79(0.1-9.69) 2.85(0.15-18.22)
EV-D68 4(0.6) 1(2.5) 0.640 20.0 4.51(0.23-31.37) 5.07(0.23-45.75)
ADV 3 (0.4) 0 (0) 1.000 0.0 - -
ADV-7 1 (0.1) 0 (0) 1.000 0.0 - -
HMPV 8 (1.1) 2 (5) 0.170 20.0 4.6(0.68-19.14) 6.03(0.83-29.1)
PIV 13 (1.8) 1(2.5) 1.000 7.1 1.37(0.07-7.15) 1.67(0.09-9.69)
Multiple infections (Virus-virus )
37 (5.2) 2 (5.0) 1.000 5.1 0.95(0.15-3.28) 0.87(0.14-3.18)
Negative for viruses 271 (38.5) 24 (60.0) 0.007 8.1 2.41(1.27-4.71) 2.5(1.29-4.99)
Missing cases for testing 2 0
Bacteria sample Tested n=447 n=11
Bacteria 5 (1.1) 2 (18.2) 0,010 28.5 19.64 (2.58-106.01) 7.83 (6.39-110.45)
Negative for all pathogens 163 (36.5) 5 (45.1) 0.810 2.9 0.75 (0.2-1.7) 0.75 (0.24-1.91)
Virus-bacteria co-detection 2(0.4) 0 (0) 1.000 0.0
Note: n (%), number and percent of children. RSV, respiratory syncytial virus; RV, rhinovirus; EV-D68,
enterovirus D68; ADV, adenovirus; ADV-7, adenovirus 7; HMPV, human metapneumovirus; PIV,
parainfluenza virus; OR, odds ratio; CI, confidence interval; AOR, adjusted odds ratio. Multivariate
logistic models were adjusted by age in week, year of sampling and hospitals.
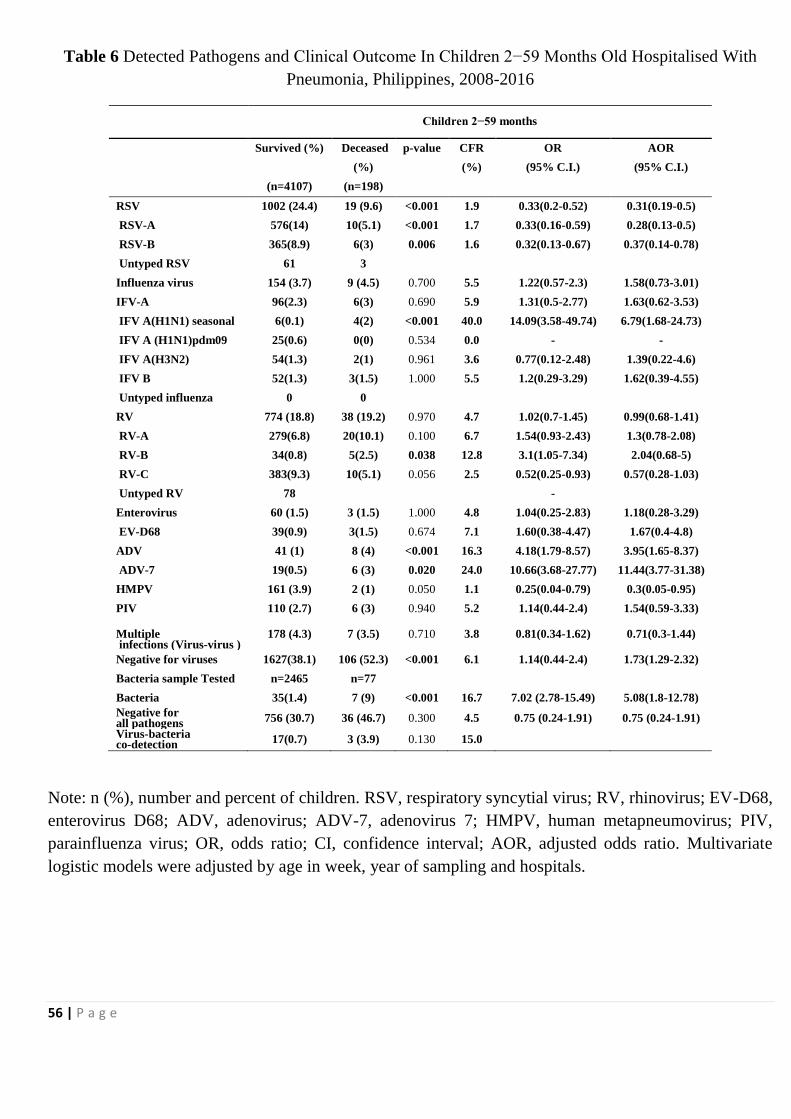
56 | P a g e
Table 6 Detected Pathogens and Clinical Outcome In Children 2−59 Months Old Hospitalised With
Pneumonia, Philippines, 2008-2016
Children 2−59 months
Survived (%) Deceased p-value CFR OR AOR
(%)
(%) (95% C.I.) (95% C.I.)
(n=4107) (n=198)
RSV 1002 (24.4) 19 (9.6) <0.001 1.9 0.33(0.2-0.52) 0.31(0.19-0.5)
RSV-A 576(14) 10(5.1) <0.001 1.7 0.33(0.16-0.59) 0.28(0.13-0.5)
RSV-B 365(8.9) 6(3) 0.006 1.6 0.32(0.13-0.67) 0.37(0.14-0.78)
Untyped RSV 61 3
Influenza virus 154 (3.7) 9 (4.5) 0.700 5.5 1.22(0.57-2.3) 1.58(0.73-3.01)
IFV-A 96(2.3) 6(3) 0.690 5.9 1.31(0.5-2.77) 1.63(0.62-3.53)
IFV A(H1N1) seasonal 6(0.1) 4(2) <0.001 40.0 14.09(3.58-49.74) 6.79(1.68-24.73)
IFV A (H1N1)pdm09 25(0.6) 0(0) 0.534 0.0 - -
IFV A(H3N2) 54(1.3) 2(1) 0.961 3.6 0.77(0.12-2.48) 1.39(0.22-4.6)
IFV B 52(1.3) 3(1.5) 1.000 5.5 1.2(0.29-3.29) 1.62(0.39-4.55)
Untyped influenza 0 0
RV 774 (18.8) 38 (19.2) 0.970 4.7 1.02(0.7-1.45) 0.99(0.68-1.41)
RV-A 279(6.8) 20(10.1) 0.100 6.7 1.54(0.93-2.43) 1.3(0.78-2.08)
RV-B 34(0.8) 5(2.5) 0.038 12.8 3.1(1.05-7.34) 2.04(0.68-5)
RV-C 383(9.3) 10(5.1) 0.056 2.5 0.52(0.25-0.93) 0.57(0.28-1.03)
Untyped RV 78
-
Enterovirus 60 (1.5) 3 (1.5) 1.000 4.8 1.04(0.25-2.83) 1.18(0.28-3.29)
EV-D68 39(0.9) 3(1.5) 0.674 7.1 1.60(0.38-4.47) 1.67(0.4-4.8)
ADV 41 (1) 8 (4) <0.001 16.3 4.18(1.79-8.57) 3.95(1.65-8.37)
ADV-7 19(0.5) 6 (3) 0.020 24.0 10.66(3.68-27.77) 11.44(3.77-31.38)
HMPV 161 (3.9) 2 (1) 0.050 1.1 0.25(0.04-0.79) 0.3(0.05-0.95)
PIV 110 (2.7) 6 (3) 0.940 5.2 1.14(0.44-2.4) 1.54(0.59-3.33)
Multiple infections (Virus-virus )
178 (4.3) 7 (3.5) 0.710 3.8 0.81(0.34-1.62) 0.71(0.3-1.44)
Negative for viruses 1627(38.1) 106 (52.3) <0.001 6.1 1.14(0.44-2.4) 1.73(1.29-2.32)
Bacteria sample Tested n=2465 n=77
Bacteria 35(1.4) 7 (9) <0.001 16.7 7.02 (2.78-15.49) 5.08(1.8-12.78)
Negative for all pathogens 756 (30.7) 36 (46.7) 0.300 4.5 0.75 (0.24-1.91) 0.75 (0.24-1.91)
Virus-bacteria co-detection 17(0.7) 3 (3.9) 0.130 15.0
Note: n (%), number and percent of children. RSV, respiratory syncytial virus; RV, rhinovirus; EV-D68,
enterovirus D68; ADV, adenovirus; ADV-7, adenovirus 7; HMPV, human metapneumovirus; PIV,
parainfluenza virus; OR, odds ratio; CI, confidence interval; AOR, adjusted odds ratio. Multivariate
logistic models were adjusted by age in week, year of sampling and hospitals.

57 | P a g e
Table 7 Clinical Signs And Symptoms Associated With Death Among Children <59 Months Old Hospitalised With Pneumonia Who Were
Tested Positive For Different Pathogens, Philippines, 2008-2016.
Factors RSV
AOR (95% C.I.)
RV
AOR (95% C.I.)
ADV
AOR (95% C.I.)
EV
AOR (95% C.I.)
Bacteria
AOR (95% C.I.)
Negative for viruses
AOR (95% C.I.)
Grunting 1.00 (0.71-1.43) 0.91(0.63-1.32) - 2.79( 1.81- 4.31) 0.91 (0.47-1.79) 4.36 (1.91-9.98)
Sensorial changes 2.11 (1.74-2.57) 1.19 (0.92-1.53) 1.09 (0.87-1.35) 1.46 (1.13 -1.89) 2.11 (1.41-3.17) 0.78 (0.69-0.87)
Central cyanosis 1.21 (1.02-1.45) 1.62 (1.2-2.19) 1.25 (0.84 - 1.88) 1.27(0.91- 1.76) 1.61 (0.66-3.91) 0.81 (0.61-1.08)
Alar flaring 1.04 (0.98-1.11) 1.01 (0.91-1.13) 0.99 (0.79 -1.25) 1.79(0.96- 3.33) 1.1 (0.7-1.73) 1.07 (0.94-1.23)
Decreased breath sound 0.90 (0.71-1.15) 1.46 (0.97-2.2) 0.87 (0.54-1.40) 0.94(0.67- 1.33) 0.68 (0.29-1.61) 1.57(1.05-2.35)
Wheezing 0.99 (0.89-1.10) 1.12 (0.96-1.3) 1.01 (0.84- 1.19) 8.27(2.83-24.15) 1.04 (0.79-1.39) 1.18 (0.98-1.42)
Fever (>38.5 °C) 1.16 (0.96-1.4) 1.95 (1.51-2.51) 6.30 (1.57-25.21) 7.07(2.44- 20.48) 9.48 (1.91-47.0) 1.57 (1.22-2.03)
Tachypnea 0.99 (0.88-1.1) 1.04 (0.91-1.2) - - 7.4 (1.06-51.67) 1.01(0.85-1.18)
Tachycardia 1.16 (1.02-1.33) 1.07 (0.89-1.28) 1.41 (0.30 -6.48) 2.55( 1.10-5.89) 0.1 (0.01-0.81) 0.82 (0.65-1.02)
SpO2<90% 1.27 (1.14-1.4) 1.29 (1.07-1.54) 6.17 (1.49 -25.42) 1.12 ( 0.93- 1.34) 1.17 (0.79-1.75) 0.95 (0.78-1.14)
Severe anaemia (<8 g/dL) 0.86 (0.48-1.51) 0.68 (0.38-1.2) - - 2.58 (1.51-4.4) 5.71 (2.92-11.17)
Consolidation 1.02 (0.9-1.16) 1.13 (0.94-1.37) 6.69 (2.11-21.22) 1.53( 1.29- 1.82) 0.97 (0.69-1.35) 2.2 (1.69-2.88)
Infiltration 1.13 (1.03-1.23) 1.07 (0.92-1.24) 6.22 (1.98-19.51) 1.17(1.03- 1.34) 7.84 (1.4-44.0) 1.13 (0.98-1.32)
Pleural effusion - 1.33 (1.18-1.51) 0.93 (0.57- 1.50) 0.97(0.56-1.71) 1.05(0.59-1.84) 2.05 (1.07-3.95)
Note: RSV, respiratory syncytial virus; RV, rhinovirus; ADV, adenovirus; EV, enterovirus, OR, odds ratio; CI, confidence interval. Multivariate
logistic models were matched with age groups and adjusted by patients age, year of sampling and hospitals

58 | P a g e
Table 8: Demographic Characteristics Of Children Hospitalised With Severe
Pneumonia, Stratified By Age Group And Outcome Excluding Children Who
Were Discharged Against Medical Advice
Children <2 months
Children 2−59 months
Survived Deceased CFR p-value Survived Deceased CRF p-value
n= 605 n=28 4.4 n=3722 n=165 4.2
Age group
Less than 1 month 239 ( 39.5) 15 ( 53.6) 5.9
- - <0.001
1 month 366 ( 60.5) 13 ( 46.4) 3.4 - -
2-5 months - - - 903 (24.3) 68 (41.2) 7
6-11months - - -
964 (25.9) 43 (26.1) 4.3
12-35 months - - -
1530 (41.1) 45 (27.3) 2.9
36-59 months - - -
325 ( 8.7) 9 ( 5.5) 2.7 Gender
Female 361 ( 59.7) 16 ( 57.1) 4.7 0.940 2100 (56.4) 91 (55.2) 4.4 Male 244 ( 40.3) 12 ( 42.9) 4.2 1622 (43.6) 74 (44.8) 4.2 0.8
Hospital admitted
BPH 181 ( 29.9) 2 (7.1) 1.1 0.050 662 (17.8) 17 (10.3) 2.5 <0.001
EVRMC 312 ( 51.6) 21 ( 75.0) 6.3
2210 (59.4) 125 (75.8) 5.4
ONP 86 ( 14.2) 4 ( 14.3) 4.4
681 (18.3) 15 ( 9.1) 2.2
RITM 26 ( 4.3) 1 ( 3.6) 3.7
169 ( 4.5) 8 ( 4.8) 4.5
Note: CRF, Case Fatality rate, BPH, Biliran Provincial Hospital; EVRMC,
Eastern Visayas Regional Medical Center; ONP, Ospital Ng Palawan; RITM,
Research Institute for Tropical Medicine; for only EVRMC patients.
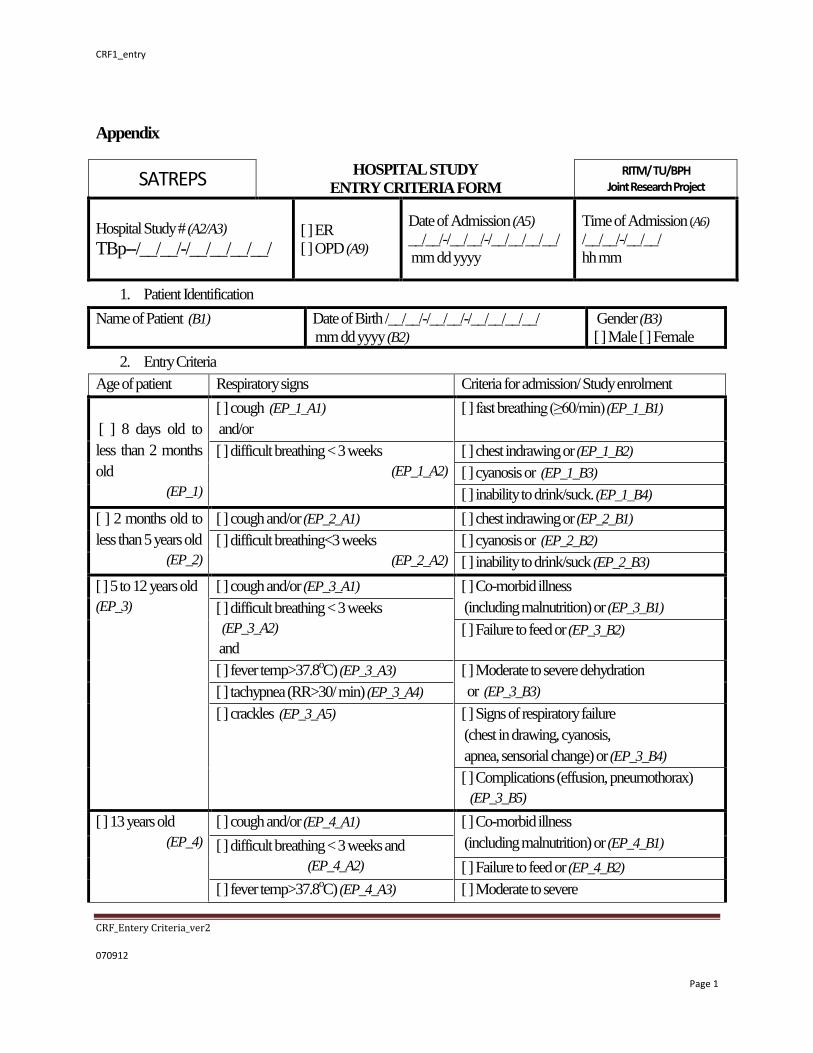
CRF1_entry
CRF_Entery Criteria_ver2
070912
Page 1
Appendix
SATREPS HOSPITAL STUDY
ENTRY CRITERIA FORM
RITM/ TU/BPH Joint Research Project
Hospital Study # (A2/A3)
TBp--/__/__/-/__/__/__/__/ [ ] ER
[ ] OPD (A9)
Date of Admission (A5)
__/__/-/__/__/-/__/__/__/__/
mm dd yyyy
Time of Admission (A6)
/__/__/-/__/__/
hh mm
1. Patient Identification
Name of Patient (B1) Date of Birth /__/__/-/__/__/-/__/__/__/__/
mm dd yyyy (B2)
Gender (B3)
[ ] Male [ ] Female
2. Entry Criteria
Age of patient Respiratory signs Criteria for admission/ Study enrolment
[ ] 8 days old to
less than 2 months
old
(EP_1)
[ ] cough (EP_1_A1)
and/or
[ ] fast breathing (≥60/min) (EP_1_B1)
[ ] difficult breathing < 3 weeks
(EP_1_A2)
[ ] chest indrawing or (EP_1_B2)
[ ] cyanosis or (EP_1_B3)
[ ] inability to drink/suck. (EP_1_B4)
[ ] 2 months old to
less than 5 years old
(EP_2)
[ ] cough and/or (EP_2_A1) [ ] chest indrawing or (EP_2_B1)
[ ] difficult breathing<3 weeks
(EP_2_A2)
[ ] cyanosis or (EP_2_B2)
[ ] inability to drink/suck (EP_2_B3)
[ ] 5 to 12 years old
(EP_3)
[ ] cough and/or (EP_3_A1) [ ] Co-morbid illness
(including malnutrition) or (EP_3_B1) [ ] difficult breathing < 3 weeks
(EP_3_A2)
and
[ ] Failure to feed or (EP_3_B2)
[ ] fever temp>37.8oC) (EP_3_A3) [ ] Moderate to severe dehydration
or (EP_3_B3) [ ] tachypnea (RR>30/ min) (EP_3_A4)
[ ] crackles (EP_3_A5) [ ] Signs of respiratory failure
(chest in drawing, cyanosis,
apnea, sensorial change) or (EP_3_B4)
[ ] Complications (effusion, pneumothorax)
(EP_3_B5)
[ ] 13 years old
(EP_4)
[ ] cough and/or (EP_4_A1) [ ] Co-morbid illness
(including malnutrition) or (EP_4_B1) [ ] difficult breathing < 3 weeks and
(EP_4_A2) [ ] Failure to feed or (EP_4_B2)
[ ] fever temp>37.8oC) (EP_4_A3) [ ] Moderate to severe

60 | P a g e
[ ] tachypnea (RR>30/ min) (EP_4_A4) dehydration or (EP_4_B3)
[ ] tachycardia (HR> 100/min) and
(EP_4_A5)
[ ] Signs of respiratory failure
(chest in drawing, cyanosis,
apnea, sensorial change) or (EP_4_B4) [ ] abnormal chest finding (diminished
breath sounds, rhonchi, crackles, or
wheezes) ( EP_4_A6)
[ ] Complications (effusion, pneumothorax)
(EP_4_B5)
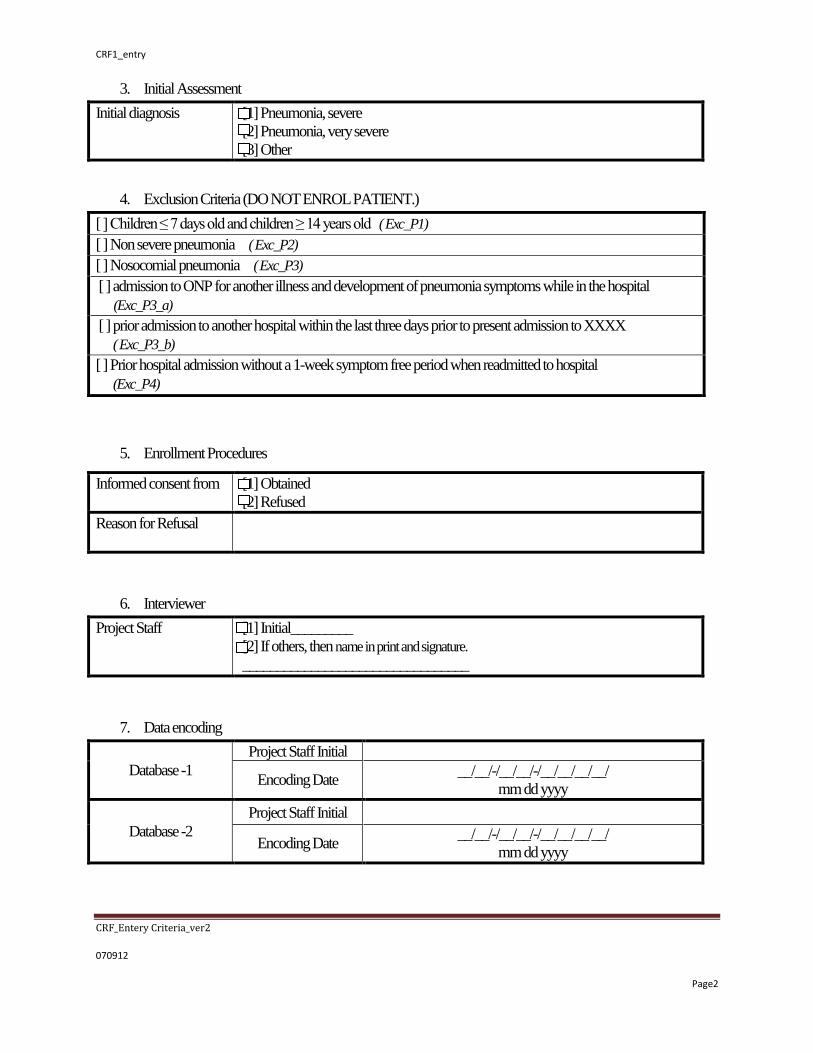
CRF1_entry
CRF_Entery Criteria_ver2
070912
Page2
3. Initial Assessment
Initial diagnosis [1] Pneumonia, severe
[2] Pneumonia, very severe
[3] Other
4. Exclusion Criteria (DO NOT ENROL PATIENT.)
[ ] Children ≤ 7 days old and children ≥ 14 years old ( Exc_P1)
[ ] Non severe pneumonia ( Exc_P2)
[ ] Nosocomial pneumonia ( Exc_P3)
[ ] admission to ONP for another illness and development of pneumonia symptoms while in the hospital
(Exc_P3_a)
[ ] prior admission to another hospital within the last three days prior to present admission to XXXX
( Exc_P3_b)
[ ] Prior hospital admission without a 1-week symptom free period when readmitted to hospital
(Exc_P4)
5. Enrollment Procedures
Informed consent from [1] Obtained
[2] Refused
Reason for Refusal
6. Interviewer
Project Staff [1] Initial_________
[2] If others, then name in print and signature.
_________________________________
7. Data encoding
Database -1
Project Staff Initial
Encoding Date __/__/-/__/__/-/__/__/__/__/
mm dd yyyy
Database -2
Project Staff Initial
Encoding Date __/__/-/__/__/-/__/__/__/__/
mm dd yyyy

62 | P a g e
SATREPS HOSPITAL ADMISSION
DATA COLLECTION FORM RITM/ TU / BPH
Joint Research Project
Hospital Study # (A2/A3)
TBp--/__/__/-/__/__/__/__/
Date of Admission (A5) /__/__/-/__/__/- /__/__/__/__/
mm dd yyyy
1. Patient Identification
Name of Patient
06 Patient initials /__/__/__/ - /__/__/ 3 letters in FIRST name and 2 letters in FAMILY name Example: Akira Y. Suzuki *akisu*
07 Date of Birth /__/__/-/__/__/-/__/__/__/__/ (mm-dd-yyyy)
08 Gender [ ] Male [ ] Female
2. Chief Complaint
01 Chief complaint
3. Illness History (Caregiver* observed during the course of this episode OR interviewer observed).
01 Fever □[1] Yes □ [2] No □[99] DK If yes, duration /__/__/days
02 Nasal Discharge □[1] Yes □ [2] No □[99] DK If yes, duration /__/__/days
02-a →If yes, what is the characteristic? ______________________________________
03 Cough □[1] Yes □ [2] No □[99] DK If yes, duration /__/__/days
04 Wheeze □[1] Yes □ [2] No □[99] DK If yes, duration /__/__/days
05 Difficult Breathing □[1] Yes □ [2] No □[99] DK If yes, duration /__/__/days
06 Inability to drink or feed □[1] Yes □ [2] No □[99] DK If yes, duration /__/__/days
07 Sleeping most of the time, or
difficult to wake#
□[1] Yes □ [2] No □[99] DK If yes, duration /__/__/days
08 Convulsion □[1] Yes □ [2] No □[99] DK

CRF1_entry
CRF_Entery Criteria_ver2
070912
Page2
09 Pallor □[1] Yes □ [2] No □[99] DK
*Caregiver is defined as person who takes care of the child more than 1 year or since birth.
4. Medication History
01 Antibiotic given (within the last three days prior to hospital admission for this episode)
□[1] Yes □ [2] No □[99] DK If yes, specify______________
Other medications given 48 hours before the admission for this episode
02 Antipyretics □[1] Yes □ [2] No □[99] DK If yes, specify______________
03 Bronchodilator □[1] Yes □ [2] No □[99] DK If yes, specify______________
04 Traditional Medicine □[1] Yes □ [2] No □[99] DK If yes, specify______________
5. Vital Signs/ Pulse oximetry /Anthropometry
01 Axillary temperature
02 Respiratory rate
03 Heart rate
/__/__/./__/ o C /__/__/__/ per minute /__/__/__/ per minute
04 Weight
05 Height/Length
/__/__/./__/ kg /__/__/./__/ cm
06 Blood Pressure (3 years old and above)
Diastolic Systolic
06-D /__/__/__/ mmHg 06-S /__/__/__/ mmHg
07
Oximetry
08 Oximetry pulse
09
Oximetry measurement
/__/__/./__/ % □ [1] before oxygen / bronchodilator therapy □[2] during or after oxygen or □[8] not measured /__/__/./__/ per min

64 | P a g e
6. Physical Examination (to be completed on admission by MD)
01 Grunting □[1] Yes □ [2] No
02
Decreased breath
sounds
Right Lobe 02-R □[1] Yes □ [2] No
Left Lobe 02-L □[1] Yes □ [2] No
03 Wheeze Right Lobe 03-R □[1] Yes □ [2] No
Left Lobe 03-L □[1] Yes □ [2] No
04 Rales/Crepitation Right Lobe 04-R □[1] Yes □ [2] No
Left Lobe 04-L □[1] Yes □ [2] No
05 Alar Flaring □[1] Yes □ [2] No
06 Chest indrawing □[1] Yes □ [2] No
07 Central Cyanosis □[1] Yes □ [2] No
08 Apneic episodes □[1] Yes □ [2] No
09 Neck rigidity# □[1] Yes □ [2] No
10 Sensorial change #
(irritability, restlessness, drowsy, stupor or coma)
□[1] Yes □ [2] No
For those who answered yes on 3-07(Sleeping/Difficult to wake)#, 6-09#, or 6-10#
11.1 Glasgow Coma Scale* Eye opening response □[1] □[2] □[3] □[4]
11.2 Glasgow Coma Scale* Verbal response □[1] □[2] □[3] □[4] □[5]
11.3 Glasgow Coma Scale* Motor response □[1] □[2] □[3] □[4] □[5] □[6]
- Glasgow Coma Scale* Total Score (No need to encode data)
12 Ear pain/tenderness (for 3 years and older) □[1] Yes □ [2] No □[99] NA
13 Ear discharge □[1] Yes □ [2] No
14 Poor skin turgor □[1] Yes □ [2] No
15 Organomegaly □[1] Yes □ [2] No □[99] NA

CRF1_entry
CRF_Entery Criteria_ver2
070912
Page2
16 Other significant finding (s)
7. Clinical Assessment
01 Initial diagnosis
[1] Pneumonia, severe [2] Pneumonia, very severe [3] Others, specify _____________________________ _____________________________
8. Project Staff
01 Attending physician [1] Project MD (initial) _________ [2] Resident on duty (name in print/signature)
_________________________________
9. Data encoding
Database -1 Project Staff Initial
Encoding Date __/__/-/__/__/-/__/__/__/__/
mm dd yyyy
Database -2 Project Staff Initial
Encoding Date __/__/-/__/__/-/__/__/__/__/
mm dd yyyy
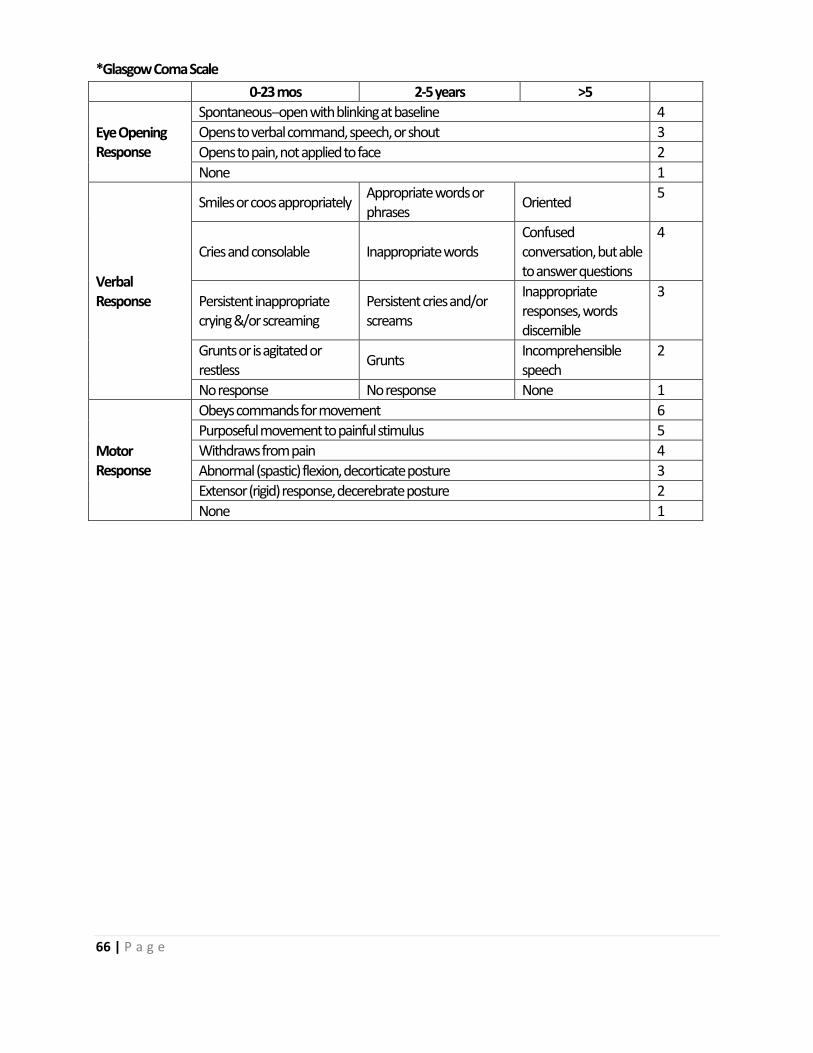
66 | P a g e
*Glasgow Coma Scale
0-23 mos 2-5 years >5
Eye Opening Response
Spontaneous--open with blinking at baseline 4
Opens to verbal command, speech, or shout 3
Opens to pain, not applied to face 2
None 1
Verbal Response
Smiles or coos appropriately Appropriate words or phrases
Oriented 5
Cries and consolable Inappropriate words Confused conversation, but able to answer questions
4
Persistent inappropriate crying &/or screaming
Persistent cries and/or screams
Inappropriate responses, words discernible
3
Grunts or is agitated or restless
Grunts Incomprehensible speech
2
No response No response None 1
Motor Response
Obeys commands for movement 6
Purposeful movement to painful stimulus 5
Withdraws from pain 4
Abnormal (spastic) flexion, decorticate posture 3
Extensor (rigid) response, decerebrate posture 2
None 1
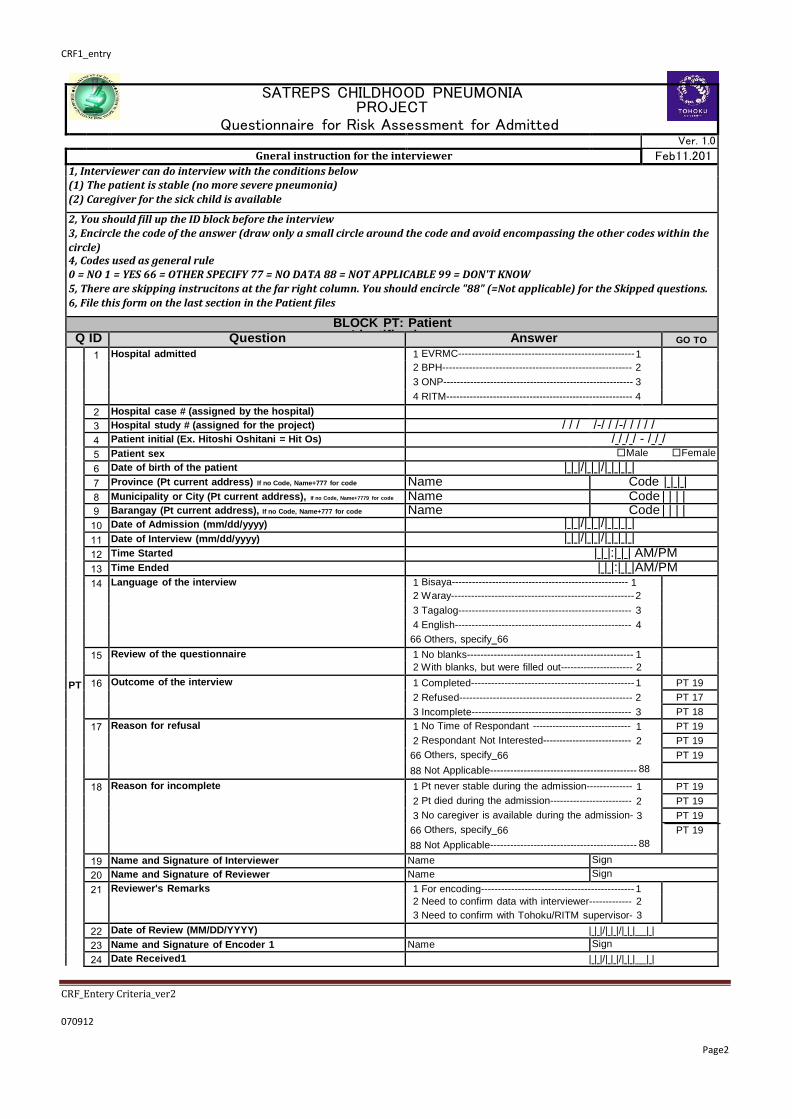
CRF1_entry
CRF_Entery Criteria_ver2
070912
Page2
SATREPS CHILDHOOD PNEUMONIA PROJECT
Questionnaire for Risk Assessment for Admitted Patient
RESEARCH INSTITUTE FOR TROPICAL MEDICINE AND TOHOKU UNIVERSITY Ver. 1.0
Gneral instruction for the interviewer Feb11.2014 1, Interviewer can do interview with the conditions below
(1) The patient is stable (no more severe pneumonia)
(2) Caregiver for the sick child is available
2, You should fill up the ID block before the interview 3, Encircle the code of the answer (draw only a small circle around the code and avoid encompassing the other codes within the
circle) 4, Codes used as general rule 0 = NO 1 = YES 66 = OTHER SPECIFY 77 = NO DATA 88 = NOT APPLICABLE 99 = DON'T KNOW
5, There are skipping instrucitons at the far right column. You should encircle "88" (=Not applicable) for the Skipped questions.
6, File this form on the last section in the Patient files
BLOCK PT: Patient Identification Q ID Question Answer GO TO
PT
1 Hospital admitted 1 EVRMC----------------------------------------------------- 1 2 BPH--------------------------------------------------------- 2 3 ONP--------------------------------------------------------- 3 4 RITM-------------------------------------------------------- 4
2 Hospital case # (assigned by the hospital) 3 Hospital study # (assigned for the project) / / / /-/ / /-/ / / / /
4 Patient initial (Ex. Hitoshi Oshitani = Hit Os) / / / / - / / /
5 Patient sex □Male □Female
6 Date of birth of the patient | | |/| | |/| | | | |
7 Province (Pt current address) If no Code, Name+777 for code Name Code | | | |
8 Municipality or City (Pt current address), If no Code, Name+7779 for code Name Code | | | | 9 Barangay (Pt current address), If no Code, Name+777 for code Name Code | | | |
10 Date of Admission (mm/dd/yyyy) | | |/| | |/| | | | |
11 Date of Interview (mm/dd/yyyy) | | |/| | |/| | | | |
12 Time Started | | |:| | | AM/PM
13 Time Ended | | |:| | |AM/PM
14 Language of the interview 1 Bisaya----------------------------------------------------- 1 2 Waray------------------------------------------------------- 2 3 Tagalog---------------------------------------------------- 3 4 English----------------------------------------------------- 4
66 Others, specify 66 15 Review of the questionnaire 1 No blanks-------------------------------------------------- 1
2 With blanks, but were filled out---------------------- 2 16 Outcome of the interview 1 Completed------------------------------------------------- 1 PT 19
2 Refused---------------------------------------------------- 2 PT 17
3 Incomplete------------------------------------------------ 3 PT 18
17 Reason for refusal 1 No Time of Respondant ------------------------------ 1 PT 19
2 Respondant Not Interested--------------------------- 2 PT 19
66 Others, specify 66 PT 19
88 Not Applicable-------------------------------------------- 88
18 Reason for incomplete 1 Pt never stable during the admission-------------- 1 PT 19
2 Pt died during the admission------------------------- 2 PT 19
3 No caregiver is available during the admission- 3 PT 19
66 Others, specify 66
88 Not Applicable-------------------------------------------- 88
PT 19
19 Name and Signature of Interviewer Name Sign
20 Name and Signature of Reviewer Name Sign
21 Reviewer's Remarks 1 For encoding---------------------------------------------- 1 2 Need to confirm data with interviewer------------- 2
3 Need to confirm with Tohoku/RITM supervisor- 3
22 Date of Review (MM/DD/YYYY) | | |/| | |/| | |__| |
23 Name and Signature of Encoder 1 Name Sign
24 Date Received1 | | |/| | |/| | |__| |

68 | P a g e
25 Date Encoded1 | | |/| | |/| | |__| |
26 Name and Signature of Encoder 2 Name Sign
27 Date Received 2 | | |/| | |/| | |__| |
28 Date Encoded 2 | | |/| | |/| | |__| |

CRF1_entry
CRF_Entery Criteria_ver2
070912
Page2
BLOCK HR: HOUSEHOLD ROSTER
HR 1 2 3 4 5 6 7 8 9 10 11 12 13
ID
What is the relationsh ip to the head of HH?
Age
Birth Date
Sex
Caregive r ID
Status of the biological mother
Highest Level of Education for household member
Has (ID No)
had asthma?
Does (ID
No) smoke?
Does (ID
No) sleep in the same room with this sick child?
Does (ID No) sleep besides sick child?
Does (ID No) usually wash hand when get back home
Start with
H/head
(01 printed) then from elderies
USE CODE
Enter the number and encircle Y, M or D
Y= year for >=1yo
M = month for <1yo D = day for <30days
MM/DD/YYYY
Only for the Under 5 children
Male
=1 Female
=2
Only for
<5yo
Use ID
in HR1
Only for
<15yo
USE CODE
USE CODE
Yes=1
No =0 DK=99
Yes=1
No =0
For the sick child, encircle both 1 /0
For the sick child, encircle both 1 /0
Yes=1
No =0
01 0 | 1 | | | Y / M / D | | |/| | |/| | | | | 1 / 2 | 1 / 0 / 99 1 / 0 1 / 0 1 / 0 1 / 0
02 | | | | Y / M / D | | |/| | |/| | | | | 1 / 2 | 1 / 0 / 99 1 / 0 1 / 0 1 / 0 1 / 0
03 | | | | Y / M / D | | |/| | |/| | | | | 1 / 2 | 1 / 0 / 99 1 / 0 1 / 0 1 / 0 1 / 0
04 | | | | Y / M / D | | |/| | |/| | | | | 1 / 2 | 1 / 0 / 99 1 / 0 1 / 0 1 / 0 1 / 0
05 | | | | Y / M / D | | |/| | |/| | | | | 1 / 2 | 1 / 0 / 99 1 / 0 1 / 0 1 / 0 1 / 0
06 | | | | Y / M / D | | |/| | |/| | | | | 1 / 2 | 1 / 0 / 99 1 / 0 1 / 0 1 / 0 1 / 0
07 | | | | Y / M / D | | |/| | |/| | | | | 1 / 2 | 1 / 0 / 99 1 / 0 1 / 0 1 / 0 1 / 0
08 | | | | Y / M / D | | |/| | |/| | | | | 1 / 2 | 1 / 0 / 99 1 / 0 1 / 0 1 / 0 1 / 0
09 | | | | Y / M / D | | |/| | |/| | | | | 1 / 2 | 1 / 0 / 99 1 / 0 1 / 0 1 / 0 1 / 0
10 | | | | Y / M / D | | |/| | |/| | | | | 1 / 2 | 1 / 0 / 99 1 / 0 1 / 0 1 / 0 1 / 0
11 | | | | Y / M / D | | |/| | |/| | | | | 1 / 2 | 1 / 0 / 99 1 / 0 1 / 0 1 / 0 1 / 0
12 | | | | Y / M / D | | |/| | |/| | | | | 1 / 2 | 1 / 0 / 99 1 / 0 1 / 0 1 / 0 1 / 0
13 | | | | Y / M / D | | |/| | |/| | | | | 1 / 2 | 1 / 0 / 99 1 / 0 1 / 0 1 / 0 1 / 0
14 | | | | Y / M / D | | |/| | |/| | | | | 1 / 2 | 1 / 0 / 99 1 / 0 1 / 0 1 / 0 1 / 0
15 | | | | Y / M / D | | |/| | |/| | | | | 1 / 2 | 1 / 0 / 99 1 / 0 1 / 0 1 / 0 1 / 0

70 | P a g e
HR 2 01 Head 04 Son-In-Law / Daughter-In-Law 08 Brother / Sister 12 Other relative Specify
02 Wife / Husband
03 Son / Daughter
05 Grandchild
06 Parent
09 Brother-In-Law / Sister-In-Law
10 Uncle / Aunt
13 Adopted / Foster / Stepchild
14 Not related
HR7 1.Alive and live in the household 07 Parent-In-Law 11 Niece / Nephew 99 DK
2.Alive and live out of household HR8 0 = None 3 = Graduate Elementary 6 = Vocational
3.Died 1 = Pre-school 4 = First- to fourth-year high school 7 = College or higher
4.DK 2 = Elementary student 5 = High school graduate 99 = DK

CRF1_entry
CRF_Entery Criteria_ver2
070912
Page2
BLOCK HH: Household
Q ID
Question
Answer Skip
1
How many people in the family are aged 0 to 14? 0 None--------------------------------------------------------------- 0 1 One-----------------------------------------------------------------1 2 Two-----------------------------------------------------------------2 3 Three---------------------------------------------------------------3 4 Four---------------------------------------------------------------- 4 5 Five or more------------------------------------------------------5
2
Do all children in the family of ages 6 to 14 go to school?
0 None--------------------------------------------------------------- 0 1 Yes----------------------------------------------------------------- 1 2 No children ages 6 to 14-------------------------------------- 2
3
What is the education level of the female head/spouse? 1 Graduate primary or less--------------------------------------1 2 First- to fourth-year secondary-------------------------------2 3 Graduate secondary------------------------------------------- 3 4 First-year college or higher----------------------------------- 4
4 Do any family members have salaried employed? (not
self employed)
0 No------------------------------------------------------------------ 0 1 Yes----------------------------------------------------------------- 1
5
What are the house’s outer walls made of, mainly? Light materials (Salvaged, makeshift, cogon, nipa, or
1 anahaw)--------------------------------------
1
Strong materials (iron, aluminum, tile, concrete, 2
brick, stone, wood, asbestos)------------------------------- 2
6
What is the house’s roof made of, mainly? Light materials (Salvaged, makeshift, cogon, nipa, or
1 anahaw)--------------------------------------
1
Strong materials (iron, aluminum, tile, concrete, 2
brick, stone, wood, asbestos)------------------------------- 2
7 What kind of toilet facility does the family have? 1 Water sealed ---------------------------------------------------- 1
2 None, open pit, closed pit, or other------------------------- 2
8 Does the family own a refrigerator? 0 No------------------------------------------------------------------ 0
1 Yes----------------------------------------------------------------- 1
9
How many television sets does the family have? 0 None--------------------------------------------------------------- 0 1 One-----------------------------------------------------------------1 2 Two or more------------------------------------------------------2
10 Does the family own a washing machine? 0 No------------------------------------------------------------------ 0
1 Yes----------------------------------------------------------------- 1
11 How many of the following pets does this
household have?
Write the number of pets in the boxes. If its Zero, Encircle
the pets name and Write zero at the corresponding Box
1 Dog----------------------------------------------------------| || |
2 Cat-----------------------------------------------------------| || |
66 Others Specify | || |
12 How many rooms in the house? Write number of rooms in the boxes |__|__| 13 How many rooms in the house are used for sleeping? Write number of rooms in the boxes |__|__| 14 Where is the kitchen located? 1 In a separate room used as kitchen------------------------ 1
2 Elsewhere in the house----------------------------------------2
3 In a separate building------------------------------------------ 3
HH16
4 Outdoors---------------------------------------------------------- 4 HH16
5 No cooking done in the household (ig. eat other
palce always)--------------------------------------------------- 5
HH17
66 Other (specify ) 66 15 Is/are there window(s) in the kitchen? 0 No------------------------------------------------------------------ 0 1 Yes----------------------------------------------------------------- 1 88 Not applicable----------------------------------------------------
88
16 What type of fuel does your household mainly use
for cooking?
1 Electricity----------------------------------------------------------1 2 Liquefied Petroleum Gas (LPG)----------------------------- 2 3 Kerosene----------------------------------------------------------3 4 Charcoal---------------------------------------------------------- 4 5 Wood-------------------------------------------------------------- 5 6 No food cooked in household-------------------------------- 6 66 Others, specify 66
17 FOR CAREGIVER 0 No------------------------------------------------------------------ 0 Next
Do you usually wash your hand before taking care of the
baby/child?
1 Yes----------------------------------------------------------------- 1
Blk

72 | P a g e
18 What is used for hand washing? 1 Only water-------------------------------------------------------- 1 2 Water With soap /detergent---------------------------------- 2 3 Alcohol or hand sanitizer-------------------------------------- 3

CRF1_entry
CRF_Entery Criteria_ver2
070912
Page2
BLOCK TY: Typhoon related questions
Q ID
Question
Answer Go
to
TY
1
Level of damage to your house after the typhoon
1 No damage------------------------------------------------------------------------------- 1
TY3
walls, some minor damages(s) such as hole
2 Moderately damaged------------------------------------------------------------------- 2
walls are still there
3 Severely damaged---------------------------------------------------------------------- 3
4 Total damage---------------------------------------------------------------------------- 4 walls,
2
Current staus of the damage of the original house 1 All fixed already-------------------------------------------------------------------------- 1
2 Use of temporary materials as roof (blue sheet etc)--------------------------- 2
3 Use of temporary materials for whole house ------------------------------------ 3
4 Abandoned-------------------------------------------------------------------------------- 4
66 Others, Specify
66
88 Not applicable---------------------------------------------------------------------------- 88
3
Where do you stay now? 1 Same address with same family---------------------------------------------------- 1
2 Same address with additional family----------------------------------------------- 2
3 Different address with same family------------------------------------------------- 3
4 Different address with additional family------------------------------------------- 4
4
Have you ever lived in the evacuation center? 0 NO------------------------------------------------------------------------------------------- 0 TY6
1 YES----------------------------------------------------------------------------------------- 1
5
How long had you lived in the evacuation center? 1 1day----------------------------------------------------------------------------------------- 1
2 2-5days------------------------------------------------------------------------------------ 2
3 1 week-2weeks-------------------------------------------------------------------------- 3
4 More than 2weeks, Specify weeks ------------------------------ 4
88 Not applicable---------------------------------------------------------------------------- 88
6
What was your primary source of income before the
Typhoon ? 1 Farming------------------------------------------------------------------------------------ 1
2 Fishery------------------------------------------------------------------------------------- 2
3 Transport driver-------------------------------------------------------------------------- 3
4 Others (Specify 4
7
How is your household income affected by the typhoon ?
1 Not affected------------------------------------------------------------------------------- 1
Ask how long they probably will not have normal income
because of the effect of the typhoon.
2 Moderately (3 months at most after the typhoon)------------------------------- 2
3 Severely (more than 3 months after the typhoon)------------------------------ 3

74 | P a g e
BLOCK HB: Health seeking
behavior Q ID Question Answer GO TO
HB
1
What symptoms made you decide to bring the child to this 1 Cough--------------------------------------- YES NO
2 Colds---------------------------------------- YES NO Ask this question, and the respondant immedately answer
"Don’t Know, just referred or told to consult", then encircle
3 Chest indrwaing-------------------------- YES NO "YES" in "7" and "NO" for the rest of the questions. If they can
tell you any symptoms, start to read each item and encircle the
4 Inabitity to dirink/be fed----------------- YES NO
answer YES or NO 5 Fast breathing----------------------------- YES NO
6 Fever---------------------------------------- YES NO
7 Don’t know, just told (referred) ------ YES NO
8 Others1, specify here
YES NO
9 Others2, specify here
YES NO
10 Others3, specify here
YES NO
2
How soon did you leave for the hospital after you decided 1 Within 30min----------------------------------------------------- 1 HB4
to bring the child or told to go to this hospital? 2 On the day-------------------------------------------------------- 2 3 1 day later-------------------------------------------------------- 3 Time to take action, NOT reaching the health facility 4 2 days later------------------------------------------------------- 4 5 3 dyas later------------------------------------------------------- 5 6 4 days later------------------------------------------------------- 6 7 5 dyas late or more-------------------------------------------- 7
3
Why were you unable to take the child to the hospital
immediately?
Multiple answers are allowed. For all answers mentioned
by the respondent, encircle the code.
If the respondent gives an answer that is not on the list, encircle
it on the space for Others
1 Look for Finalcial support to pay transport-------------- 1
2 Look for Finalcial support to pay hospital fee----------- 2
3 Cannot leave work at that time----------------------------- 3 4 Cannot leave other children at that time----------------- 4
66 Others, specify 66 88 Not applicable--------------------------------------------------- 88
4
Tell me your action(s) taken for the child between the point Noticed your child was unwell you seek for help outside and reaching this hospital by
1st
Vis
it
1, BHS------------------------------------------------------------- 1 chronological order? 2, RHU------------------------------------------------------------- 2 3, Sattelite clinic------------------------------------------------- 3 You should say "Where did you go first?" And continue to say 4, Traditional healer------------------------------------------- 4 "Then" until the child reached this hospital.
5, Pharmacy --------------------------------------------------- 5 6, Private Clinic------------------------------------------------- 6 7, Hospital other than this hospital------------------------ 7 Encircle a cohice chronologically from 1st to 4th visit. 66, Others, specify 66
88Not applicable------------------------------------------------ 88
You should encircle 88 for "not applicalbe" if the item(s) not
2nd V
isit
1, BHS------------------------------------------------------------- 1 used. 2, RHU------------------------------------------------------------- 2 3, Sattelite clinic------------------------------------------------- 3 4, Traditional healer------------------------------------------- 4 5, Pharmacy --------------------------------------------------- 5 6, Private Clinic------------------------------------------------- 6 7, Hospital other than this hospital------------------------ 7 66, Others, specify 66 88Not applicable------------------------------------------------ 88
3rd
Vis
it
1, BHS------------------------------------------------------------- 1 2, RHU------------------------------------------------------------- 2 3, Sattelite clinic------------------------------------------------- 3 4, Traditional healer------------------------------------------- 4 5, Pharmacy --------------------------------------------------- 5 6, Private Clinic------------------------------------------------- 6 7, Hospital other than this hospital------------------------ 7 66, Others, specify 66 88Not applicable------------------------------------------------ 88
4th
Vis
it
1, BHS------------------------------------------------------------- 1 2, RHU------------------------------------------------------------- 2 3, Sattelite clinic------------------------------------------------- 3 4, Traditional healer------------------------------------------- 4 5, Pharmacy --------------------------------------------------- 5 6, Private Clinic------------------------------------------------- 6 7, Hospital other than this hospital------------------------ 7 66, Others, specify 66 88Not applicable------------------------------------------------ 88 Reached this hospital
hospital?
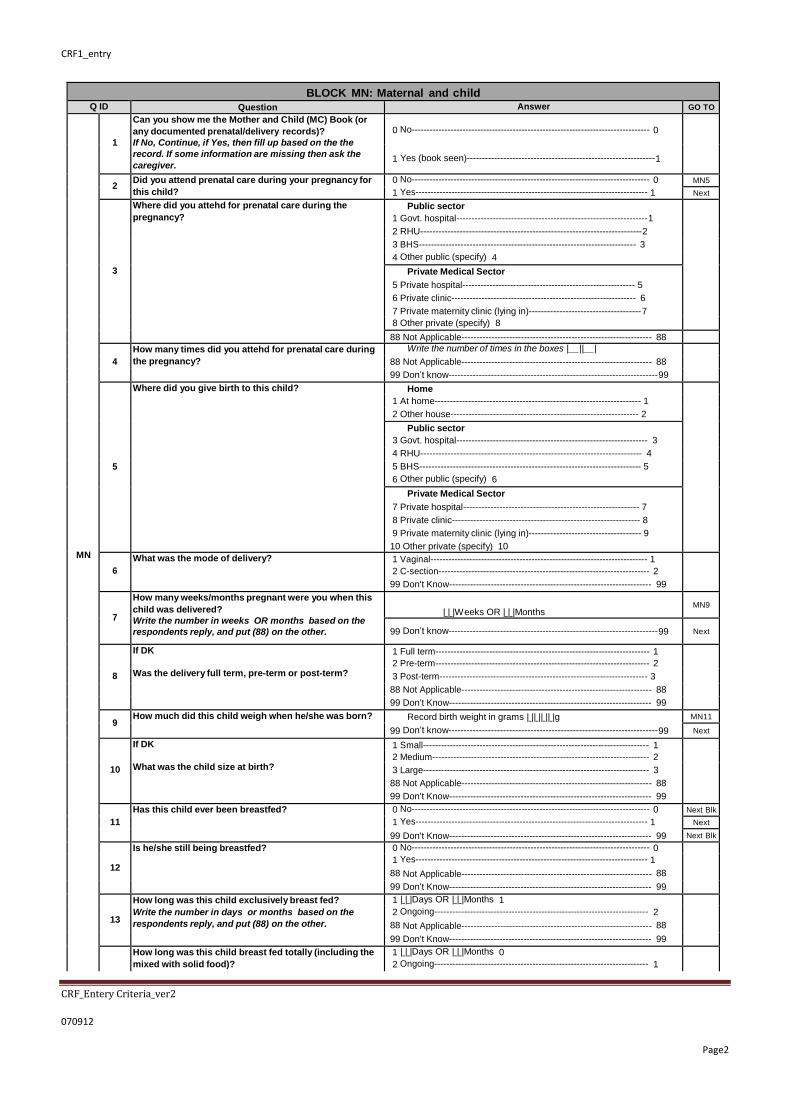
CRF1_entry
CRF_Entery Criteria_ver2
070912
Page2
BLOCK MN: Maternal and child health Q ID Question Answer GO TO
MN
1
Can you show me the Mother and Child (MC) Book (or
any documented prenatal/delivery records)?
If No, Continue, if Yes, then fill up based on the the
record. If some information are missing then ask the
caregiver.
0 No-------------------------------------------------------------------------------- 0
1 Yes (book seen)--------------------------------------------------------------1
2 Did you attend prenatal care during your pregnancy for
this child?
0 No-------------------------------------------------------------------------------- 0 MN5
1 Yes------------------------------------------------------------------------------ 1 Next
3
Where did you attehd for prenatal care during the
pregnancy?
Public sector 1 Govt. hospital---------------------------------------------------------------1 2 RHU-------------------------------------------------------------------------2 3 BHS------------------------------------------------------------------------- 3 4 Other public (specify) 4
Private Medical Sector
5 Private hospital---------------------------------------------------------- 5
6 Private clinic-------------------------------------------------------------- 6
7 Private maternity clinic (lying in)-------------------------------------7
8 Other private (specify) 8 88 Not Applicable---------------------------------------------------------------- 88
4
How many times did you attehd for prenatal care during
the pregnancy?
Write the number of times in the boxes |__||__| 88 Not Applicable---------------------------------------------------------------- 88 99 Don’t know---------------------------------------------------------------------99
5
Where did you give birth to this child? Home 1 At home-------------------------------------------------------------------- 1 2 Other house-------------------------------------------------------------- 2
Public sector 3 Govt. hospital--------------------------------------------------------------- 3 4 RHU------------------------------------------------------------------------- 4 5 BHS------------------------------------------------------------------------- 5 6 Other public (specify) 6
Private Medical Sector
7 Private hospital---------------------------------------------------------- 7
8 Private clinic-------------------------------------------------------------- 8
9 Private maternity clinic (lying in)------------------------------------- 9
10 Other private (specify) 10
6
What was the mode of delivery? 1 Vaginal------------------------------------------------------------------------- 1 2 C-section----------------------------------------------------------------------- 2 99 Don't Know-------------------------------------------------------------------- 99
7
How many weeks/months pregnant were you when this
child was delivered?
Write the number in weeks OR months based on the
respondents reply, and put (88) on the other.
| | |Weeks OR | | |Months
MN9
99 Don’t know---------------------------------------------------------------------99
Next
8
If DK 1 Full term------------------------------------------------------------------------ 1 2 Pre-term------------------------------------------------------------------------ 2 Was the delivery full term, pre-term or post-term? 3 Post-term---------------------------------------------------------------------- 3 88 Not Applicable---------------------------------------------------------------- 88 99 Don't Know-------------------------------------------------------------------- 99
9 How much did this child weigh when he/she was born? Record birth weight in grams | || || || |g MN11
99 Don’t know---------------------------------------------------------------------99 Next
10
If DK 1 Small---------------------------------------------------------------------------- 1 2 Medium------------------------------------------------------------------------- 2 What was the child size at birth? 3 Large---------------------------------------------------------------------------- 3 88 Not Applicable---------------------------------------------------------------- 88 99 Don't Know-------------------------------------------------------------------- 99
11
Has this child ever been breastfed? 0 No-------------------------------------------------------------------------------- 0 Next Blk
1 Yes------------------------------------------------------------------------------ 1 Next
99 Don't Know-------------------------------------------------------------------- 99 Next Blk
12
Is he/she still being breastfed? 0 No-------------------------------------------------------------------------------- 0 1 Yes------------------------------------------------------------------------------ 1 88 Not Applicable---------------------------------------------------------------- 88 99 Don't Know-------------------------------------------------------------------- 99
13
How long was this child exclusively breast fed?
Write the number in days or months based on the
respondents reply, and put (88) on the other.
1 | | |Days OR | | |Months 1 2 Ongoing------------------------------------------------------------------------ 2 88 Not Applicable---------------------------------------------------------------- 88 99 Don't Know-------------------------------------------------------------------- 99
How long was this child breast fed totally (including the
mixed with solid food)?
1 | | |Days OR | | |Months 0 2 Ongoing------------------------------------------------------------------------ 1

76 | P a g e
14 Write the number in days or months based on the
respondents reply, and put (88) on the other. 88 Not Applicable---------------------------------------------------------------- 88 99 Don't Know-------------------------------------------------------------------- 99

CRF1_entry
CRF_Entery Criteria_ver2
070912
Page2
BLOCK UD: Underlying disease
UD
1
Does child have any congenital abnormality?
(abnormality compared to other baby, such as down
sysdrom)
0 No---------------- ------------------------------ ---------------------------------- 0 UD 3
1 Yes------------------------------------------------------------------------------ 1 Next
99 Don't Know-------------------------------------------------------------------- 99 UD 3
2
What is the congenital abnormality? 1 Trisomy 21----------------------------------- ----------------------------------1 2 Congenital heart disease-------------------------------------------------- 2 3 Hydrocephalous---------------------------- ---------------------------------- 3 66 Others, Specify
88 Not Applicable------------------------------
99 Don't Know-------------------------------------------------------------------- 99
3
Has the child been diagnosed to have TB? 0 No---------------- ------------------------------ ---------------------------------- 0 UD 5
1 Yes------------------------------------------------------------------------------ 1 Next
99 Don't Know-------------------------------------------------------------------- 99 UD 5
4
Has the child been treated with completeing TB drug
therapy?
0 No---------------- ------------------------------ ---------------------------------- 0 1 Yes------------------------------------------------------------------------------ 1 2 Ongoing-------- ---------------------------------------------------------------- 2 88 Not Applicable------------------------------ ---------------------------------- 88 99 Don't Know-------------------------------------------------------------------- 99
5
Has the child been diagnosed to have asthma? 0 No---------------- ------------------------------ ---------------------------------- 0 UD 7
1 Yes------------------------------------------------------------------------------ 1 Next
99 Don't Know-------------------------------------------------------------------- 99 UD 7
6
Is the child under any medication for asthma? 0 No---------------- ------------------------------ ---------------------------------- 0 1 Yes------------------------------------------------------------------------------ 1 88 Not Applicable------------------------------ ---------------------------------- 88 99 Don't Know-------------------------------------------------------------------- 99
7
Has s/he had chronic cough for 2 weeks in the past one
year?
0 No---------------- ------------------------------ ---------------------------------- 0 1 Yes------------------------------------------------------------------------------ 1 99 Don't Know-------------------------------------------------------------------- 99
8
Has the child ever been diagnosed with atopic dermatitis? 0 No---------------- ------------------------------ ---------------------------------- 0 1 Yes------------------------------------------------------------------------------ 1 99 Don't Know-------------------------------------------------------------------- 99
9
Does the child have chronic redness or dry skin? 0 No---------------- ------------------------------ ---------------------------------- 0 1 Yes------------------------------------------------------------------------------ 1 99 Don't Know-------------------------------------------------------------------- 99
10
Does child have other disease(s) now, diagnosed by a
physician? 0 No---------------- ------------------------------ ---------------------------------- 0 Next Blk
1 Yes------------------------------------------------------------------------------ 1 Next
99 Don't Know-------------------------------------------------------------------- 99 Next Blk
11
What is/are this/these disease(s)?
List down all
88 Not Applicable---------------------------------------------------------------- 88
99 Don't Know-------------------------------------------------------------------- 99 BLOCK HA: Hospital
admission
HA
1
has your child ever been confined in hospital for whatever reason - from the time s/he was born until now ?
0 No---------------- ------------------------------ ---------------------------------- 0 Next Blk
1 Yes------------------------------------------------------------------------------ 1 Next
99 Don't Know--------------------------------------------- 99 Next Blk
2
How many times has the child been confined in the hospital ? Record the number of times on the boxes and write the details of the confinement on the table below
If recalled, write the number -------------------------| | | Next
88 Not Applicable---------------------------------------------------------------- 88 Next Blk
99 Don't Know-------------------------------------------------------------------- 99 Next Blk
Ask about th past admission history from the latest admission (except for the current admission). 3 4 5 6 7 8
No o f N a m e of H os pi ta l
Month/ YEAR
Duration betw een
date of the onset and
date of the adm ission
If recalled (in DAYS)
Duration of stay in
hosp
If recalled (in DAYS)
D i a g nos i s
h o spit al admissio n
01, E V R MC If NOT recalled
in Month,
encode 99 in MM
if not in Year
encode 9999 in YYYY
If not recalled
encode 999
If not recalled
encode 999
01, Pneum oi na Fr o m 02, B PH
lat e st t o 03, ON P 02, Sev ere Pneum oni a
o lde r 04, R ITM
03, V ery Sev ere Pneum oni a 66, Others Spec i f y
66, Others s pec i f y
1 | | | Specify |__|__| / |__|__|__|__| |__|__|__| |__|__|__| | | | Specify 2 | | | Specify |__|__| / |__|__|__|__| |__|__|__| |__|__|__| | | | Specify 3 | | | Specify |__|__| / |__|__|__|__| |__|__|__| |__|__|__| | | | Specify 4 | | | Specify |__|__| / |__|__|__|__| |__|__|__| |__|__|__| | | | Specify 5 | | | Specify |__|__| / |__|__|__|__| |__|__|__| |__|__|__| | | | Specify 6 | | | Specify |__|__| / |__|__|__|__| |__|__|__| |__|__|__| | | | Specify

78 | P a g e
7 | | | Specify |__|__| / |__|__|__|__| |__|__|__| |__|__|__| | | | Specify

CRF1_entry
CRF_Entery Criteria_ver2
070912
Page2
BLOCK IM: Immunization stutus
IM1 Can you show me a vaccination record for this child? No record shown------------------------------- 0 Yes, record was shown to interviewer----- 1
If any record shown, use the information to complete the table of vaccination below. If no record given, or lacking information in the record, interview the caregiver.
Follow this
Column 1 Column 2 Column 3
Q ID
Vaccines
Given to the child?
Can you remember Month
and/or Year?
Date
NO YES DK NO YES NA MM/YYYY NA
IM2 BCG 0 1 99 0 1 88 | _|_ |/| _|_ | | | 88
IM3_1 DPT (1st) 0 1 99 0 1 88 | _|_ |/| _|_ | | | 88
IM3_2 DPT (2nd) 0 1 99 0 1 88 | _|_ |/| _|_ | | | 88
IM3_3 DPT (3rd) 0 1 99 0 1 88 | _|_ |/| _|_ | | | 88
IM4_1 OPV (1st) 0 1 99 0 1 88 | _|_ |/| _|_ | | | 88
IM4_2 OPV (2nd) 0 1 99 0 1 88 | _|_ |/| _|_ | | | 88
IM4_3 OPV (3rd) 0 1 99 0 1 88 | _|_ |/| _|_ | | | 88
IM5_1 HBV(1st) 0 1 99 0 1 88 | _|_ |/| _|_ | | | 88
IM5_2 HBV(2nd) 0 1 99 0 1 88 | _|_ |/| _|_ | | | 88
IM5_3 HBV(3rd) 0 1 99 0 1 88 | _|_ |/| _|_ | | | 88
IM5_4 HBV(4th) 0 1 99 0 1 88 | _|_ |/| _|_ | | | 88
IM6 AMV(9Months) 0 1 99 0 1 88 | _|_ |/| _|_ | | | 88
IM7 MMR 0 1 99 0 1 88 | _|_ |/| _|_ | | | 88
IM8 Vitamin A 0 1 99 0 1 88 | _|_ |/| _|_ | | | 88
IM9 Deworming 0 1 99 0 1 88 | _|_ |/| _|_ | | | 88
IM10_1 Hib(1st) 0 1 99 0 1 88 | _|_ |/| _|_ | | | 88
IM10_2 Hib(2nd) 0 1 99 0 1 88 | _|_ |/| _|_ | | | 88
IM10_3 Hib(3rd) 0 1 99 0 1 88 | _|_ |/| _|_ | | | 88
IM10_4 Hib(4th) 0 1 99 0 1 88 | _|_ |/| _|_ | | | 88
IM11_1 Rota(1st) 0 1 99 0 1 88 | _|_ |/| _|_ | | | 88
IM11_2 Rota(2nd) 0 1 99 0 1 88 | _|_ |/| _|_ | | | 88
IM11_3 Rota(3rd) 0 1 99 0 1 88 | _|_ |/| _|_ | | | 88
IM12 Others Specify:- 0 1 99 0 1 88 | _|_ |/| _|_ | | | 88
IM13 Others Specify:- 0 1 99 0 1 88 | _|_ |/| _|_ | | | 88
IM14 Others Specify:- 0 1 99 0 1 88 | _|_ |/| _|_ | | | 88
IM15 Others Specify:- 0 1 99 0 1 88 | _|_ |/| _|_ | | | 88

80 | P a g e
BLOCK MT: Mortality
Q No. Question Answer Go To
MT
1
Have you ever given birth to a boy or girl who was born alive but later died before
the birthday of 5 years of age?
If “No” probe by asking:
I m ean, to a child w ho ever breathed or cried or show ed other signs of life – even if he
or she lived only a few m inutes or hours?
0
No------------------------------------------------------------------
0
End
1
Yes----------------------------------------------------------------
1
CM 2
99
Don’t know------------------------------------------------------
99
End
2 How many boys have died? Boys -------------------------------------- I__I I__I Next
If none, record ‘00’. 88 Not applicable-------------------------------------------------- 88
3 How many girls have died? Girls -------------------------------------- I__I I__I End
If none, record ‘00’ . 88 Not applicable-------------------------------------------------- 88

CRF1_entry
CRF_Entery Criteria_ver2
070912
Page2