-
7/27/2019 A Study of the Clinical Test of Sensory Interaction
and Balance.
1/6
Research ReportA Study of the Clinical Test of Sensory
Interactionand Balance
Key Words: Balance, Equilibrium, Posture, Tests and
measurements, Vestibularsystem.
Background and Purpose. The ability to maintain an upright
position dun'ngquiet standing is a usefil motor skill. The Clinical
Test of Sensory Interaction andBalance is an inexpensive, easily
administered test that provides informationabout the ability to
stand upright under several sensory conditions. Subjects.
Successful performance of some dailylife tasks, such as reading
the titles ofbooks on a shelf, requires the abilityto maintain an
upright position. Forthis reason, many physical therapistsare
concerned with their patients'ability to perform this motor skill.
Wewill refer to the ability to maintain anupright position during
quiet standingas "balance." Force platforms, electro-myography, and
motion analysis sys-tems have all been used for assess-
Helen CohenCathleen A BlatchlyLaurle L Gombash
ment of balance.' These sophisticatedsystems, however, are
expensive andoften impractical for use by a thera-pist in a typical
hospital or privatepractice. They require considerablefloor space,
special training, and com-puters. These resources may be
un-available to the clinician who wouldlike to be able to test
patients' bal-ance, but who lacks funds to purchasesophisticated
equipment or who mustcarry equipment from place to place.
Three groups of neurologically asymptomatic (AS) adults, divided
by age intoyounger, middle-aged, and older groups, participated in
the study.A fourth groupcomprked subjects diagnosed with vestibular
disorders. M et b o d s . Timed perjor-mances under six dzrerent
conditions were compared across groups. Results.Subjects with
vestibular disorders were signifcantly impaired on perjormancewhen
compared with age-matched AS subjects. OlderAS and vestibularly
impairedsubjecrs had greater variation in their scores than did
younger AS subjects. Con-cluston and Dlscussfon. This test is a
usehl screening tool for examiningstatic standing balance. [CobenH,
Blatchly GI, ombash LL. A study of the Clini-cal Test o f Sensory
Interaction and Balance. Phys Ther. 1993;73:346354..]
H Co hen, EdD, OTR, is Assistant Professor, Department o f O
torhinolaryngology and Comm unica-tive Sciences, Baylor College of
Medicine, One Baylor Plaza, Houston,TX 77030 (USA). She
wasAssistant Professor, Program in Rehabilitation Science, and
Assistant Professor, Departrnent of Oto-laryngology, Medical
College of Ohio, Toledo, OH 43699, at the time of this study.
Address allcorrespondence to Dr Cohen.CA Blatchly, PT, is Assistant
Professor, Program in Physical Therapy, Medical College of OhioLL
Gombash, PT, is Physical Therapist, Medical College Hospital, and
Clinical Lecturer, Departrnentof Otolaryngology, Medical College of
Ohio .This study was approved by the Institutional Rwiew Board of
the Medical College of Ohio.This article wa s submitted February 18
, 199 2, and wa s accepted January 29 , 1 993.
Therefore, a simpler, less expensivvalid, and reliable test is
needed.The Clinical Test of Sensoq Interaction and Balance (CTSIB)
is a timedtest that was developed for systemacally testing the
influence of visual,vestibular, and somatosensoq inpustanding
balance.2 This test is inexpsive, requires minimal equipment, is
currently in use by some cliniciaConditions 1,2,and 3 involve
standon the floor with eyes open, eyesclosed, and wearing a
visualconflicdome. The dome provides a sensoconflict by depriving
the subject ofperipheral vision and introducing asway-referenced
image. Use of theconflict dome results in a discrepanbetween
vestibular input stimulatedpostural sway and visual flow.'
Thuconditions 2 and 3 should examinedifferent aspects of sensoq
organiztion of visual information that may
Physical Therapy/Volume 73, Number 6/June 1993 34
-
7/27/2019 A Study of the Clinical Test of Sensory Interaction
and Balance.
2/6
require different postural adjustments.3That is, condition 2
exam ines howwell subjects maintain balance in theabsence of any
vision, and condition 3examines how well subjects maintainbalance
wh en vision is present bu t thatinforma tion conflicts with v
estibularinformation.Conditions 4, 5, and 6 involve stand-ing on
foam and repeating the visualconditions described for conditions
1through 3. For each condition, thelength of time the subject can
main-tain standrng and the amount of bodysway that occurs a re
assessed.Although no rms fo r this test havebee n established for
children andyoung adults, norms fo r performanceon the CTSIB have
not been estab-lished for older adults and patientswith vestibular
deficits.4.5 Currently,the CTSIB requi res perform ance of atleast
on e trial on each of the six con-ditions. Some investigators have
ques-tioned whether the eyes-closed an dth e
visuab'vestibular-conflict condi-tions produce different
performance.Billek-Sawhney5 foun d n o differenceson m easures of
duration and swayamplitude in the eyes-closed andvisual-conflict
condition s in neurolo gi-cally asym ptom atic (AS) y oung
adults.No studies in the literature addressthese issues in older
adults and indi-viduals with vestibular disorde rs.It is unclear
whether patients improveo n re peated trials on the CTSIB, be-cause
different investigator+ haveused d ifferent methods for
calculatingperformance times and am ount ofsway. Physical
therapists have a dvo-cated the use of balance retrainingthat
involves repeated exposure todifferent sensory conditions
whenstanding,7 but n o studie s have distin-guished between motor
performanceon this test and motor learning as aresult of practice.
Determ ining theneed for repeated trials during assess-ment would
be useful.
'Alimed Inc, 68 HarrisonAve, Boston,MA 02111.
These findings suggest that the CTSIBshould b e studied further.
Previousfindings suggest that therapists usingthe CTSIB should
expect performanceon this test to vary with respect to ageand
health status.6.S10This study hadseveral goals: (1) to de term
inewhether healthy adults of differentages had different timed
balancescores o n the CTSIB, (2) to deter min ewhether healthy
subjects performeddifferently on each of the six condi-tions, (3)
to learn whether individualsdiagnosed with vestibular
disordersperform ed differently than AS sub -jects, and (4) to
determine whethersubjects' performance im proved o
vertrials.MethodSubjectsPilot data were collected from 22 sen-ior
physical therapy students (9 m en ,13 wome n), aged 20 to 24
years@= 21.3 , SD=0.85). Subjects in theexperiment were divided
into fourgroups. Groups 1,2, and 3 each com-prised 15 AS subjects.
G ro up 1 com-prised 5 men a nd 10 wom en, aged 25to 44 years @
=39.3, SD=5.5). Gr oup2 comprised 4 me n and 11women,aged 45 to 64
years @=52.1, SD=6.2).Group 3 comprised 1man and 14wom en, aged 65
to 84 years @=75 .1,SD=5.9). No subjects we re ob ese.Subjects were
screened for majorhealth problems, and only individualswith n o
history of "dizziness," balancedisorders, or recent o rthopedic
prob-lems we re included. Subjects ingroups 1 and 2 w ere recruited
fromamo ng th e physical therapy students,SUE, an d faculty at the
Medical Collegeof Ohio, Toledo, Ohio. Group 3 sub-jects were
retired elderly people livingin the community.Gro up 4 comprised 17
patients (7me n, 10 wom en), aged 30 to 87 years@ =59 .8, SD=
18.9), diagnosed w ithvestibular disorders by a board-certified
otolaryngologist specializingin vestibular disorders. In addition
to
the clinical evaluation, diagnostic testsincluded computerized
harmonicacceleration tests of the vestibulo-ocular reflex,
optokinetic nystagmus,ocular pursuit and saccades, and ca-loric
tests, duri ng which eye m ove-ments were recorded with
electroocu-lography. Patients' diagnoses inc ludedbenign paroxysmal
positional vertigo,vestibular n euronitis, cupu
lolithiasis,labyrinthitis, and vestibular disorde rof idiopathic
origin. Their initial com-plaints included vertigo, disequili-brium
, and blurred vision. The physi-cian referred all patients for
physicaltherapy at th e M edical College Hospi-tal. All subjects
gave informed consentbefo re participating in this
study.EquipmentThe materials for this test included a40.64x 40.64x
7.62-cm piece ofmedium-density Sunm ate* foam,2
avisuaUvestibular-conflict d o m e m a defrom a Chinese lantern
attached to aplastic su n visor, and a stopwatch. (Asun visor is a
hatless brim attached toan elastic band covered in terry
cloth,which holds th e brim over the fore-head to shade the eyes.)
We used asun visor that could be detached fromits elastic band, s o
that ditferent bandscould b e used w ith each subject.Between test
sessions, the elasticbands we re w ashed. This detail elimi-nated
any concerns subjects mighthave had about hygiene. The domewas
constructed according to thedescription by Shumway-Cook andHorak2
so that the subject saw a fixa-tion point, a larg e black cross,
cen-tered in visual field. The total cost formaterials was
approximately $40.Because the materials needed for thistest are
inexpen sive, even clinics withsmall budgets can afford to obtain
thenecessary equipm ent.ProcedureAll subjects we re tested for th
ree trialon each of the six conditions, instocking feet. The
conditions were(1) quiet standing on the floo r, look-ing straight
ahead; (2) quiet standingon the floor with eyes closed; (3)quiet
standing on the floor wearingthe conflict dome; (4) quiet
standmg
10 / 347 Physical Therapy /Volum e 73, Number 6/June 199
-
7/27/2019 A Study of the Clinical Test of Sensory Interaction
and Balance.
3/6
on the foam, with eyes open ; ( 5 )quiet standing on the foam,
with eyesclosed; and ( 6 ) quiet standing o n thefoam wearing the
conflict dome. Be-tween trials for conditions 4 through6 , the foam
was turned over androtated 90 degrees to prevent thefoam from
wearing unevenly overmany trials. Subjects rested betw eentrials,
fo r 30 to 60 seconds, to elimi-nate the confounding effect of
fatigue.Pilot work showed no effect of orderof conditions, with
subjects who u n-derstooci the n ature of the task, whe nconditions
1 through 3 were givenbefore o r after conditions 4 through6 .
Similarly, no dae renc es werefound when the orde rs of conditions2
an d 3 and conditions 5 and 6 werereversed. Performance is known to
beaEected by the performer's level ofunderstanding of the skd l.ll
Althoughthe postural control aspect of the testis presumably
automatic, assumingthe correct position of the feet andhands could
require som e practice tounderstand the nature of the
task.Therefore, the experimental paradigmwas always administered
using co ndi-tions 1 through 3 first t o give th esubjects the idea
of the po sition re-quired. For that reason, condition 1,the least
complicated con dition, al-ways preceded all other conditions,and
condition 4 always precede d
b conditions 5 and 6 .- Prior to testing in each condition,
theinvestigator demonstrated the task.The test was administered
with theconditions in the same ord er eachtime. For all conditions,
the subjectwas instructed to stand quietly, witharms co mfortably
across the waist,feet togethe r, for as long as possible,up to 30
seconds. This period of timehad been specified in the
originaldescription of the test.2 Th e instruc-tions given by all
investigators we restandardized and were chang edslightly for each
condtion.Prior to starting the test, subjects weretold that each
trial would last for upto 30 seconds. For condition 1 , th
einvestigator told the subject, "Standwith your feet together,
hands acrossyou r waist, and look straight ahead.
Do this until I tell you to stop." Theinstructional set for the
other condi-tions included the instruction to"close your eyes" for
condition 2 an d"Now I'd like you to wear this hat andlook at the
cross" for condition 3. Fo rconditions 4 through 6 , subjects w
eregiven the same instruction regardingvisual conditions and were
also askedto stand on the cente r of the foam.The length of time
the subject couldmaintain balance was rec ord ed. A trialwas
terminated when the subject'sarms o r feet changed position.
Forsubjects wh o were able to perform all18 trials for 30 seconds,
the test tookapproximately 20 minutes. All subjectswere tested in a
quiet, well-lightedroom with a linoleum floor.Data AnalysisThe data
were analyzed using themean time performing the test, overthe thre
e trials for each condition.Test-retest reliability a nd
interraterreliability were determ ined usingPearson Product-Moment
CorrelationCoefficients. Differences am ong expe r-imental groups
were determinedusing an analysis of variance (ANOVA)for repeated
measures. Significantdifferences were then subjected topost hoc
Tukey's tests. Differencesbetween AS subjects and
age-matchedvestibularly impaired subjects wereexamined with t tests
using the Bon-ferroni correction.ResultsBoth test-retest and
interrater reliabil-ity were high (r=.99, Pc.01).Thesemeasures we
re taken with the pilotgro up . Interrater reliability was
evalu-ated by having two investigators at atime test five subjects
simultaneously,using identical digital stopwatches.Values were
round ed to th e nearesthalf secon d. T est-retest reliability
wastested by having the same investigatortest five subjects
twice.Th e ANOVA sho we d n o significantdifferences among grou ps
fo r condi-tions 1 through 3 . That is, all subjectscould stand on
the floor for 30 sec-onds with eyes ope n, eyes closed, and
wearing the conflict do me , for althree trials.The results were
somewhat diffefor conditions 4 , 5 , and 6 (eyes oeyes closed, and
wearing the condo me , respectively, while standinthe foam). As
shown in Figure 1,co nfirm ed w ith the ANOVA, subjein groups 1 , 2
, an d 3 performed dition 4 for significantly longer thcondition 5
(F[16,34] 11.35, P
-
7/27/2019 A Study of the Clinical Test of Sensory Interaction
and Balance.
4/6
40 Condition
n 30J8-n 2085mm
10
0 1 2 3 4
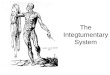
GroupFigure 1. Mean duration of balance in each group, by
condition. Error bars repre-sent standard deviations. Condition
4=standing onfoam with eyes open, condition5=standing on foam with
eyes closed, condition 6=standing on foam wearing
visual/vestibular-conflictdome. Group I =asymptomatic subjects aged
25 to 44 years, group2=asymptomatic subjects aged 45 to M years,
group 3=asymptomatic subjects aged 65to 84 years, group
4=uestibukarly impaired subjects.
Group40 1
8 2
30 3n42C . 4040 20853 10
0 4 5 6
Condition
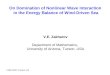
Figure2. Mean duration of balance in each condition, by group.
Error bars repre-sent standard deviations. See Fig. I legend for
desn'ptons of groups and conditions.
g r ou p s 1 , 2 , and 3 performed signifi-cantly better than
grou p 4 on condi-tions 5 and 6 (condition 5: t[l6]=4.17 ,P
-
7/27/2019 A Study of the Clinical Test of Sensory Interaction
and Balance.
5/6
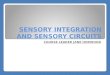
VesUbuladyImpaired Subjects
1 Condition 1Flgure 3. Dz$wences in balance duration between
vestibularly impaired subjectsand age-matched asymptomatic
subjects. Ewor bars represent standard deviations. SeeFig. 1 legend
for descriptions of conditions.
-able 1. Mean Balance Scores (in Seconds)" for Each Group by
TrialCondttlon 4' Condltlon 5" Condttlon6.Groupb Trlal 1 Trlal 2
Trlal 3 Trlal 1 Trlal 2 Trlal 3 Trlal 1 Trlal 2 Trlal 3*Standard
deviations shown in parenthesesb ~ r o u p=asymptomatic subjects
(n=15) aged 25 to 44 years, group 2=asymptomatic subjects(n=15)
aged 45 to 64 years, group 3=asymptomatic subjects (n=15) aged 65
to 84 years, group4=vestibularly impaired subjects
(n=17).'Condition 4=standing on foam with eyes opend~ on dit ion
=standing on foam with eyes closed.
ular diso rders canno t. Therefore,condition may serve as a
useful bline, particularly when assessing patients with vestibular
disordersothe r balance problems.On condit ion 5, both the older
gand the vestibularly impaired g roperformed more poorly than
didyounger AS groups . These findinare consistent with th ose of
previwork.10 The vestibularly impairedgro up performed at the sam e
levthe older AS group, regardless ofOn the measure reported in
thisstudy, youn ger subjects with vestlar impairments perfor med as
if twere o lder people.O n condition 6, although the eldAS subjects
had lower score s thantheir younger counterparts, they better able
to perform this condithan sub jects with vestibular disoders. These
data suggest that a scof 20 seconds o n condit ions 4, 5,6 with the
feet together is withinnorm al limits for o lder subjects. Cdition
6 may also be useful in discriminating between older peoplwith and
without vestibular disorWhen a therapist suspects a vestibdisorder
in a patient without suchdiagnosis, these data may h elp thphysical
therapist make a referralthe approp riate physician for evation.
Such a difference may also buseful in reassessing patients
aftecourse of physical therapy.Older AS and vestibularly
impairesubjects tended to show higher swith successive trials o n
the two ditions in which vision was elimino r not useful. This
finding suggesthat these subjects may have usedunsuccessful
movement strategy itially, but were able to mod* themotor plans
with practice. This fiing may indicate that these subjectook longer
than younger AS subto understand the motor require-ments of the
task. Because the sujects with vestibular lesions had mvariability
than o the r subjects, andbecause those subjects did improove r
trials, it might b e useful to aminister this test using three or
m
"Condition 6=standing on foam wearing
visuaVvestibular-conflictdome.Physical Therap y/Volu me 73, Number
64une 1993
-
7/27/2019 A Study of the Clinical Test of Sensory Interaction
and Balance.
6/6
trials and take the mean of thosetrials.This study examined
subjects' abilityto maintain quiet upright standingwhe n sensory
inputs were systemati-cally altered. Measures of sway c ouldprovide
further insight into perfor-mance abilities of individuals in
differ-ent age gro ups, but that issue was notexamined in this
study because ob-semin g sway in the clinic would haverequired two
observers or m ore so-phisticated, expensive equipment.On e purpo
se of this study was tomake it easy for a single physicaltherapist
to adm inister this test.
Although the CTSIB does not spec@the exact nature of a subject's
balanceproblem , it is u seful in difFerentiatingbetween
individuals with and w ithoutvestibular disorders. Th e test is
alsouseful for obtaining data abou t pa-tients' performance before
and aftertherapy, and thus in documenting theefficacy of treatm
ent, for the benefit of
Commentary
third-par ty payers . Because the CTSIBis inexpensive, it is a
useful option forclinics in which expensive dynam icposturography
testing equipm ent isunavailable, but w here the therapistsstill
need objective data ab out balance.AcknowledgmentsWe thank Rebecca
Koch, FT, and Milli-cent Branch, FT, or their assistance.
References1 Horak FB. Clinical measurement of pos-tural control
in adults. Phys Ther 1987;67:1881-1885.2 Shumway-Cook A, Horak FB.
Assessing theinfluence of sensory interaction on balance:suggestion
from the field. Phys Ther 1986;66:1548-1550.3 Nashner LM,McCollum
G. The organizationof human postural movements: a formal basisand
experimental synthesis. Behav Brain Sci.1985;8:135-172.4 Crowe TK,
Deitz JC, Richardson PK, AtwaterSW. Interrater reliability of the
pediatric clini-cal test of sensory interaction for
balance.Physical and Occupational Therapy in Pediat-rics.
199O;lO:l-27.5 Billek-Sawhney B. Clinical and ObjectiveAssessment
of Postural Stabilify. Pittsburgh, Pa:University of Pittsburgh;
1990. Thesis.
6 Di Fabio RP, Badke MB. Relationship of sen-sory organization
to balance function in pa-tients with hemiplegia. Phys Ther.
1990;70:542-548.7 Toal Tangeman P, Wheeler J. Inner ear con-cussion
syndrome: vestibular implications andphysical therapy treatment. ~
o p i i sn AcuteCare Trauma Rehabilitation. 1986;1:72-83.8 Pyykko
I, Aalto H, Hytonen M, et al. Effect ofage on posture control. In:
Amblard B,Benhoz A, Clarack E, eds. Posture and Gait:Development,
Adaptation, a nd M odulation.Amsterdam, the Netherlands: Elsevier;
1988:95-104.9 Straube A, Botzel K, Hawken M , et al. Pos-tural
control in the elderly: differential effectsof visual, vestibular
and somatosensory input.In: Amblard B. Benhoz A Clarack E, eds.
Pos-ture an d Gait:'~ e v e l o ~ m t k z t ,daptation, an
dModulation. Amsterdam, the Netherlands: El-sevier; 1988:105-114.10
Woollacott MH. Aging, posture control andmovement preparation. In:
Woollacott MH,Shumway-CookA, eds. Posture an d GaitAcross the
LiJespan. Columbia, SC: University ofSouth Carolina Press;
1989:155-175.11 Gentile AM. A working model of skill ac-quisition
with application to teaching. Quest,1972;17:%23.12 Norre ME, Forrez
G, Beckers A. Vestibularhabituation training and posturography on
be-nign paroxysmal positioning vertigo. ORLJOtorhino laryngo l
Relat Spec. 1987,4922-25.
The developm ent of effective metho dsfor assessing and treating
adults withvestibular deficits is a p romin ent issuefor physical
therapists and occupa-tional therapists involved with "vestibu-lar
rehabilitation." The article by Co-hen et al provides a vehicle for
thekind of dialogue that is need ed aboutthis important topic. I
would conside rtheir study preliminary, however, inview of several
issues related to thebroad generalization of their results,the
inconsistency of age-m atched com-parisons, the recommendation to
de-lete various aspects of t he Clinical Testof Sensory Interaction
o n Balance(CTSIB), and the absen ce of a do cu-mented relationship
between stanceduration an d functional status in pa-tients with
vestibular impairments.
Generallzatlon of FlndlngsThe primary conclusion reported
byCohen a nd colleagues was that theCTSIB ". . . is useful in
differentiatingbetween individuals with and withoutvestibular
disorders." I believe thatthis conclusion is potentially
mislead-ing for several reasons:1. Su bjects with a nd witho ut
activevertigo have equivalent scores ontests of sen sory
interaction ac-quir ed with posturography.' Theconditions used for
evaluatingbalance with posturography andthe CTSIB are essentially
the sam e.Posturography, however, incorpo-rates a forc e platform
an d a visualenclosure that can be referenced
to spontaneous displacements ofthe subject's center of force.2
Pos-turography provides a mo re sensi-tive measu re of balance
comparedwith th e CTSIB becau se manipula-tion of the sensory
environmen t isprecisely controlled and equilib-rium scores are
derived from verti-cal floor reaction forces. It is un-likely,
therefore, that the CTSIBwill identify sensory integrationdeficits
in m any patients with ver-tigo, because m ore sensitive mea-sures
d o not detect deficits relatedto this symptom.Subjects with
compensated (chron-ic) unilateral peripheral vestibularimpairments
often have normalbalance responses when tested
14 / 351 Physical Therapy /Volum e 73, Number G/June 1993