Embed Size (px)
Citation preview

IEEE JOURNAL OF BIOMEDICAL AND HEALTH INFORMATICS, VOL. 18, NO. 6, NOVEMBER 2014 1839
A Smartphone-Centric System for the Rangeof Motion Assessment in Stroke Patients
Wang Wei Lee, Shih-Cheng Yen, Arthur Tay, Ziyi Zhao, Tian Ma Xu, Karen Koh Mui Ling,Yee-Sien Ng, Effie Chew, Angela Lou Kuen Cheong, and Gerald Koh Choon Huat
Abstract—The range of motion (ROM) in stroke patients is of-ten severely affected. Poststroke rehabilitation is guided throughthe use of clinical assessment scales for the rROM. Unfortunately,these scales are not widely utilized in clinical practice as they areexcessively time-consuming. Although commercial motion-capturesystems are capable of providing the information required forthe assessments, most systems are either too costly or lack theconvenience required for assessments to be conducted on a dailybasis. This paper presents the design and implementation of asmartphone-based system for automated motor assessment usinglow-cost off-the-shelf inertial sensors. The system was used to au-tomate a portion of the upper-extremity Fugl–Meyer assessment(FMA), which is widely used to quantify motor deficits in strokesurvivors. Twelve out of 33 items were selected, focusing mainlyon joint angle measurements of the upper body. The system hasthe ability to automatically identify the assessment item being con-ducted, and calculate the maximum respective joint angle achieved.Preliminary results show the ability of this system to achieve com-parable results to goniometer measurements, while significantlyreducing the time required to conduct the assessments. The porta-bility and ease-of-use of the system would simplify the task ofconducting range-of-motion assessments.
Index Terms—Body sensor networks, mobile nodes, patient re-habilitation, wearable sensors.
I. BACKGROUND
S TROKE is the fourth leading cause of death in the UnitedStates, with about 795 000 people experiencing stroke each
year [1]. Globally, an estimated 15 million people suffer strokeyearly [2]. In Singapore, stroke is a major cause of death, with
Manuscript received August 30, 2013; accepted January 10, 2014. Date ofpublication January 20, 2014; date of current version November 3, 2014. Thiswork was supported in part by the Singapore Millennium Foundation and inpart by NUS MOE Tier 1 Grant R263-000-A42-112.
W. W. Lee, S.-C. Yen, A. Tay, and Z. Zhao are with the Department ofElectrical and Computer Engineering, National University of Singapore, Singa-pore (e-mail: [email protected]; [email protected]; [email protected]; [email protected]).
K. K. M. Ling, A. L. K. Cheong, and G. K. C. Huat are with theSaw Swee Hock School of Public Health, National University of Singa-pore, Singapore (e-mail: [email protected]; [email protected];[email protected]).
T. M. Xu is with the Ang Moh Kio-Thye Hwa Kwan Community Hospital,Singapore (e-mail: [email protected]).
Y.-S. Ng is with the Singapore General Hospital, Singapore (e-mail:[email protected]).
E. Chew is with the Division of Neurology, University Medicine Cluster,National University Hospital, Singapore (e-mail: [email protected]).
Color versions of one or more of the figures in this paper are available onlineat http://ieeexplore.ieee.org.
Digital Object Identifier 10.1109/JBHI.2014.2301449
more than 10 000 new patients being hospitalized due to strokeeach year [3]. Stroke affects a person’s cognitive, language, per-ceptual, sensory, and motor abilities [4]. The recovery processis very long, extending beyond the hospital stay and into thehome setting, and are guided by clinical assessments such astheir range of motion. Accurate assessment of their ranges ishence crucial in selecting the best therapies for stroke patients.
The Fugl–Meyer assessment of sensorimotor recovery afterstroke (FMA) is widely used in clinical trials to quantify motordeficits in patients after stroke [5]. The main evaluation aspectsof the FMA include motor movements, balance, sensation, jointROM and pain, thus providing a concise scale to quantify strokeseverity with sound psychometric properties. However, the FMAis rarely used in clinics due to its lengthy administration time, asit consists of a 33-item upper extremity subscale and a 17-itemlower extremity subscale [6]. A typical full-scale assessmentwould require more than an hour to conduct. A shorter versionof the FMA (S-FM) was developed by Hsieh et al. [7] to reduceits administration time. Despite the reduction in items, the S-FMis still not very widely used. One of the reasons is that theS-FM is still based on observations of subjects’ motor behavior,and measurements are conducted manually using a goniometeror visual estimation. As a result, the accuracy and consistencymay vary greatly across clinicians [8]. A precise, reliable, yetconvenient method of performing such assessments is thus im-perative, and this is where the use of electronic tools may beuseful.
The first step to such an effective electronic assessment tool isthe ability to accurately measure joint ROM. Traditionally, elec-tronic assessments of ROM are performed using multicameravision systems, which are often too elaborate, expensive, andinconvenient to perform on large numbers of patients. Othervision-based systems such as Microsoft Kinect have seen sig-nificant adoption in applications for posture and gesture detec-tion. However, such systems suffer from skeletal merging [9]and thus do not work reliably when the caregiver is withinthe field of view of the camera, or if the subject were to siton a wheelchair/bed. In recent years, there have been a grow-ing number of attempts to track movements in humans usingwearable devices instead [10]. Methods such as e-textiles [11],optical linear encoders [12], and fiber optics [13] have beeninvestigated with the aim of providing accurate joint angle mea-surements. However, these approaches require the calibration ofequipment for individual patients, due to the variations in jointsizes and skin elasticity. Inertial measurement units (IMU) areless sensitive to such variations, since they work by compar-ing orientation between limbs, instead of measuring the amount
2168-2194 © 2014 IEEE. Personal use is permitted, but republication/redistribution requires IEEE permission.See http://www.ieee.org/publications standards/publications/rights/index.html for more information.

1840 IEEE JOURNAL OF BIOMEDICAL AND HEALTH INFORMATICS, VOL. 18, NO. 6, NOVEMBER 2014
Fig. 1. General system architecture.
of bend at a joint. In IMU systems, MEMS (microelectrome-chanical systems) sensors such as accelerometers, gyroscopes,magnetometers or a combination of them are used to estimatethe orientation of the limbs the sensors are attached to. Estima-tion of joint angles and joint kinematics using IMUs have beenextensively studied [14]–[18]. The accuracy and reliability ofIMU-based systems have since improved to the point where ap-plications in motion capture, gait, and posture analysis are alsopossible [19], [20], and commercial motion capture systems arenow readily available [21], [22].
Despite the availability of technology for accurate joint mo-tion capture, a convenient, user-friendly and cost-effective motorability assessment tool has yet to appear. Many of the systemsmentioned are rather complicated, requiring skilled personel tooperate. In addition, these systems often require a PC to processthe data from the sensors, which translates to reduced portabilityand convenience.
The aim of this paper is to introduce a new joint-angle mea-surement system, designed specifically for physicians to con-duct ROM assessments quickly and easily within the hospital.Although it is also based on IMUs, the system is operated froma smartphone instead, thus improving its mobility. As a start, 12simple assessment activities from the upper extremity FMA thatdo not involve muscle-group synergies were selected and im-plemented in the system. These activities can be automaticallyidentified and measured by the system, thus ensuring that theinterface remains simple and user friendly. Developed in collab-oration with healthcare professionals from Singapore GeneralHospital (SGH) and Ang Moh Kio-Thye Hwa Kwan commu-nity Hospital (AMKH), the system aims to provide doctors andtherapists with a practical tool to perform ROM measurements.
Section II will elaborate on the design and implementationconsiderations of the system. Section III focuses on validat-ing the accuracy of the system against the goniometer, whileSections IV and V present the discussion and conclusions,respectively.
II. DESIGN AND DEVELOPMENT
A. System Architecture
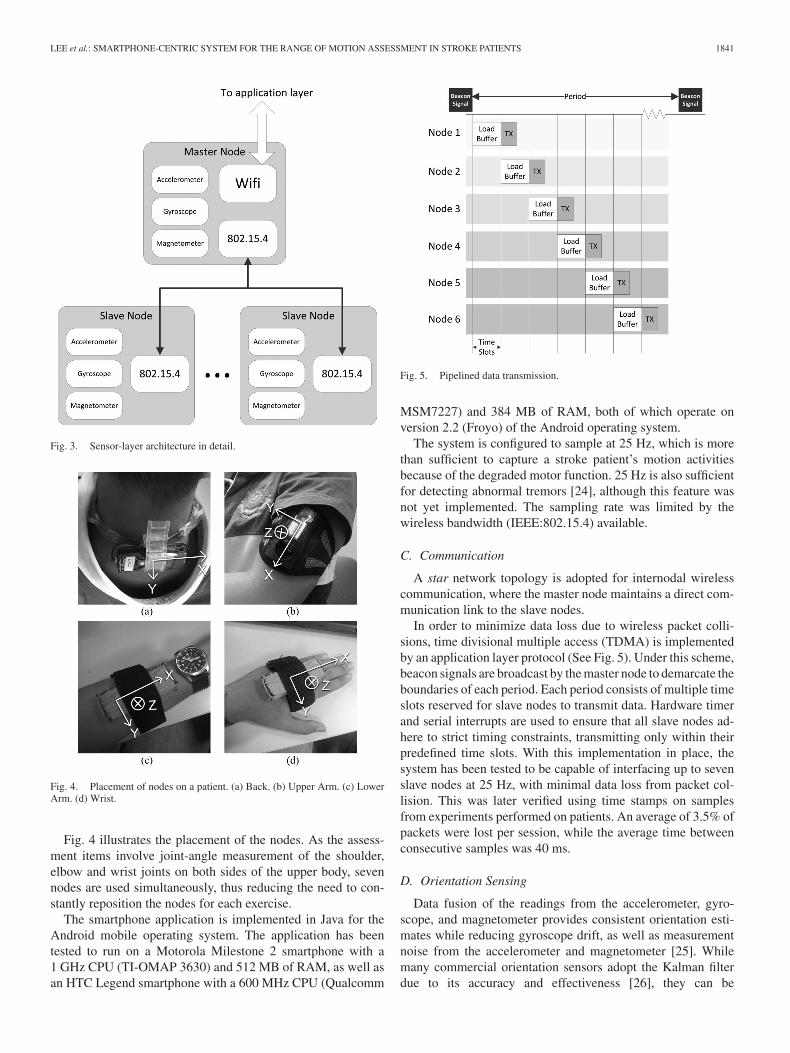
There are two main parts to the system (see Fig. 1)—the sen-sor nodes (see Fig. 2) and the application. The sensor nodes
Fig. 2. Sensor node.
are responsible for acquiring data on the orientation and move-ment of the patient’s limbs. A total of seven sensor nodes areused. Each node includes tri-axial accelerometer, gyroscope, andmagnetometer sensors that are polled by an on-board microcon-troller. Also included is a wireless communication module andbattery. Each node measures 66.6 mm × 28.2 mm × 18.1 mmand weighs 22 g. When used with a fully charged battery, eachnode lasts 179 min on average.
A sensor-fusion algorithm runs on each node, where rawsensor readings are combined to continuously update the 3-Dorientation of the sensor. Compared to implementing the fu-sion algorithm on the smartphone, calculations performed onindividual nodes greatly reduce the computational load on thesmartphone, while improving reliability of the orientation esti-mates since it does not have to deal with the possible loss ofsensor readings during wireless transmission.
The IEEE 802.15.4 [23] standard for wireless communica-tion is used for all nodes, in order to reduce size and powerconsumption. A single larger node capable of communicatingon both WiFi and the IEEE 802.15.4 standard is included in thesystem. Known as the master node, it acts as a bridge betweenthe other (slave) nodes and the smartphone, while at the sametime collecting data from its on-board sensors. This eliminatesthe need for a separate network adapter for the phone. Anotheradvantage of this solution is the distribution of processing load,as the master node encapsulates the network protocol needed tocommunicate with the rest of the slave nodes. The architectureof the sensor layer is illustrated in Fig. 3.
The application layer runs on an Android smartphone. It re-ceives the orientation of all nodes from the master node viaWiFi, from which the posture of the subject can then be derived.The computation of joint angles and the identification of assess-ment exercises are performed at this stage. The application alsoserves as the user interface of the system.
B. System Configuration
The system is built using commercially available compo-nents. Each slave node consists of an 8 bit microprocessor(ATMEGA328, Atmel), a triaxial accelerometer (ADXL345,Analog Devices), a triaxial gyroscope (ITG3200, InvenSense),a triaxial magnetometer (HMC5883L, Honeywell), as well as aIEEE 802.15.4 compliant wireless module (XB24-A, Digi). Themaster node uses a different microprocessor (LPC1768, NXP),and also includes a WiFi module (RN-131C, Roving Networks)in addition to the sensors used on the slave nodes.
LEE et al.: SMARTPHONE-CENTRIC SYSTEM FOR THE RANGE OF MOTION ASSESSMENT IN STROKE PATIENTS 1841
Fig. 3. Sensor-layer architecture in detail.
Fig. 4. Placement of nodes on a patient. (a) Back. (b) Upper Arm. (c) LowerArm. (d) Wrist.
Fig. 4 illustrates the placement of the nodes. As the assess-ment items involve joint-angle measurement of the shoulder,elbow and wrist joints on both sides of the upper body, sevennodes are used simultaneously, thus reducing the need to con-stantly reposition the nodes for each exercise.
The smartphone application is implemented in Java for theAndroid mobile operating system. The application has beentested to run on a Motorola Milestone 2 smartphone with a1 GHz CPU (TI-OMAP 3630) and 512 MB of RAM, as well asan HTC Legend smartphone with a 600 MHz CPU (Qualcomm
Fig. 5. Pipelined data transmission.
MSM7227) and 384 MB of RAM, both of which operate onversion 2.2 (Froyo) of the Android operating system.
The system is configured to sample at 25 Hz, which is morethan sufficient to capture a stroke patient’s motion activitiesbecause of the degraded motor function. 25 Hz is also sufficientfor detecting abnormal tremors [24], although this feature wasnot yet implemented. The sampling rate was limited by thewireless bandwidth (IEEE:802.15.4) available.
C. Communication
A star network topology is adopted for internodal wirelesscommunication, where the master node maintains a direct com-munication link to the slave nodes.
In order to minimize data loss due to wireless packet colli-sions, time divisional multiple access (TDMA) is implementedby an application layer protocol (See Fig. 5). Under this scheme,beacon signals are broadcast by the master node to demarcate theboundaries of each period. Each period consists of multiple timeslots reserved for slave nodes to transmit data. Hardware timerand serial interrupts are used to ensure that all slave nodes ad-here to strict timing constraints, transmitting only within theirpredefined time slots. With this implementation in place, thesystem has been tested to be capable of interfacing up to sevenslave nodes at 25 Hz, with minimal data loss from packet col-lision. This was later verified using time stamps on samplesfrom experiments performed on patients. An average of 3.5% ofpackets were lost per session, while the average time betweenconsecutive samples was 40 ms.
D. Orientation Sensing
Data fusion of the readings from the accelerometer, gyro-scope, and magnetometer provides consistent orientation esti-mates while reducing gyroscope drift, as well as measurementnoise from the accelerometer and magnetometer [25]. Whilemany commercial orientation sensors adopt the Kalman filterdue to its accuracy and effectiveness [26], they can be
1842 IEEE JOURNAL OF BIOMEDICAL AND HEALTH INFORMATICS, VOL. 18, NO. 6, NOVEMBER 2014
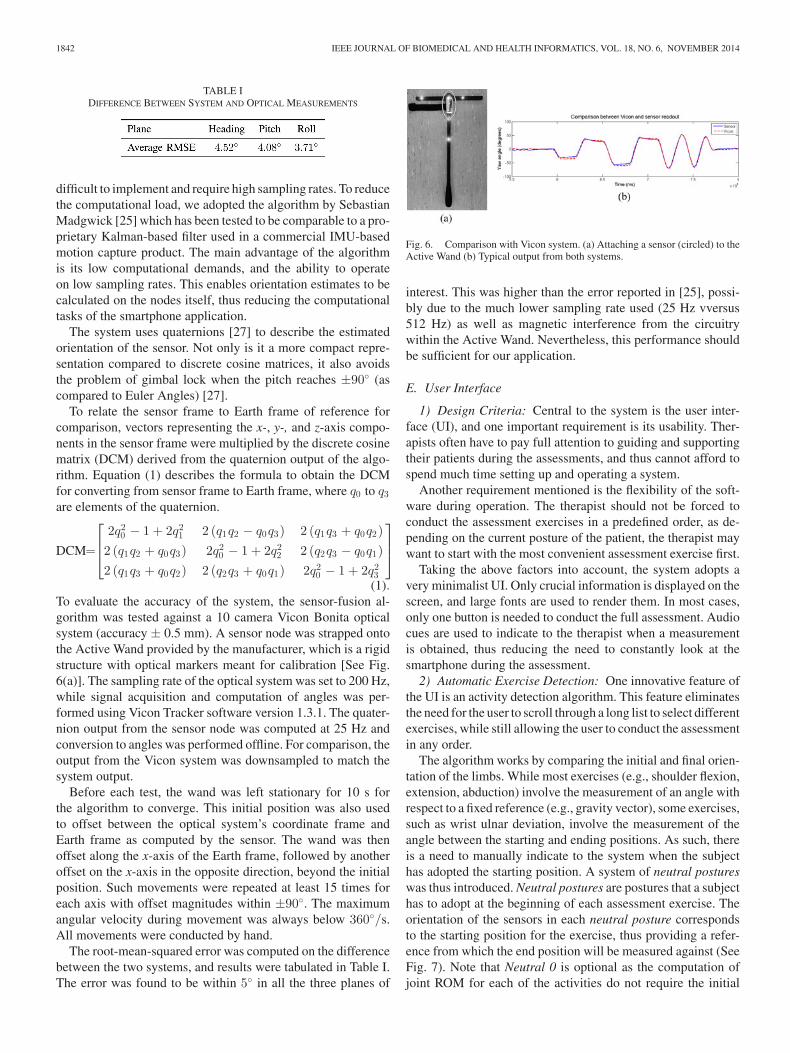
TABLE IDIFFERENCE BETWEEN SYSTEM AND OPTICAL MEASUREMENTS
difficult to implement and require high sampling rates. To reducethe computational load, we adopted the algorithm by SebastianMadgwick [25] which has been tested to be comparable to a pro-prietary Kalman-based filter used in a commercial IMU-basedmotion capture product. The main advantage of the algorithmis its low computational demands, and the ability to operateon low sampling rates. This enables orientation estimates to becalculated on the nodes itself, thus reducing the computationaltasks of the smartphone application.
The system uses quaternions [27] to describe the estimatedorientation of the sensor. Not only is it a more compact repre-sentation compared to discrete cosine matrices, it also avoidsthe problem of gimbal lock when the pitch reaches ±90◦ (ascompared to Euler Angles) [27].
To relate the sensor frame to Earth frame of reference forcomparison, vectors representing the x-, y-, and z-axis compo-nents in the sensor frame were multiplied by the discrete cosinematrix (DCM) derived from the quaternion output of the algo-rithm. Equation (1) describes the formula to obtain the DCMfor converting from sensor frame to Earth frame, where q0 to q3are elements of the quaternion.
DCM=
⎡⎢⎣
2q20 − 1 + 2q2
1 2 (q1q2 − q0q3) 2 (q1q3 + q0q2)2 (q1q2 + q0q3) 2q2
0 − 1 + 2q22 2 (q2q3 − q0q1)
2 (q1q3 + q0q2) 2 (q2q3 + q0q1) 2q20 − 1 + 2q2
3
⎤⎥⎦
(1).To evaluate the accuracy of the system, the sensor-fusion al-gorithm was tested against a 10 camera Vicon Bonita opticalsystem (accuracy ± 0.5 mm). A sensor node was strapped ontothe Active Wand provided by the manufacturer, which is a rigidstructure with optical markers meant for calibration [See Fig.6(a)]. The sampling rate of the optical system was set to 200 Hz,while signal acquisition and computation of angles was per-formed using Vicon Tracker software version 1.3.1. The quater-nion output from the sensor node was computed at 25 Hz andconversion to angles was performed offline. For comparison, theoutput from the Vicon system was downsampled to match thesystem output.
Before each test, the wand was left stationary for 10 s forthe algorithm to converge. This initial position was also usedto offset between the optical system’s coordinate frame andEarth frame as computed by the sensor. The wand was thenoffset along the x-axis of the Earth frame, followed by anotheroffset on the x-axis in the opposite direction, beyond the initialposition. Such movements were repeated at least 15 times foreach axis with offset magnitudes within ±90◦. The maximumangular velocity during movement was always below 360◦/s.All movements were conducted by hand.
The root-mean-squared error was computed on the differencebetween the two systems, and results were tabulated in Table I.The error was found to be within 5◦ in all the three planes of
Fig. 6. Comparison with Vicon system. (a) Attaching a sensor (circled) to theActive Wand (b) Typical output from both systems.
interest. This was higher than the error reported in [25], possi-bly due to the much lower sampling rate used (25 Hz vversus512 Hz) as well as magnetic interference from the circuitrywithin the Active Wand. Nevertheless, this performance shouldbe sufficient for our application.
E. User Interface
1) Design Criteria: Central to the system is the user inter-face (UI), and one important requirement is its usability. Ther-apists often have to pay full attention to guiding and supportingtheir patients during the assessments, and thus cannot afford tospend much time setting up and operating a system.
Another requirement mentioned is the flexibility of the soft-ware during operation. The therapist should not be forced toconduct the assessment exercises in a predefined order, as de-pending on the current posture of the patient, the therapist maywant to start with the most convenient assessment exercise first.
Taking the above factors into account, the system adopts avery minimalist UI. Only crucial information is displayed on thescreen, and large fonts are used to render them. In most cases,only one button is needed to conduct the full assessment. Audiocues are used to indicate to the therapist when a measurementis obtained, thus reducing the need to constantly look at thesmartphone during the assessment.
2) Automatic Exercise Detection: One innovative feature ofthe UI is an activity detection algorithm. This feature eliminatesthe need for the user to scroll through a long list to select differentexercises, while still allowing the user to conduct the assessmentin any order.
The algorithm works by comparing the initial and final orien-tation of the limbs. While most exercises (e.g., shoulder flexion,extension, abduction) involve the measurement of an angle withrespect to a fixed reference (e.g., gravity vector), some exercises,such as wrist ulnar deviation, involve the measurement of theangle between the starting and ending positions. As such, thereis a need to manually indicate to the system when the subjecthas adopted the starting position. A system of neutral postureswas thus introduced. Neutral postures are postures that a subjecthas to adopt at the beginning of each assessment exercise. Theorientation of the sensors in each neutral posture correspondsto the starting position for the exercise, thus providing a refer-ence from which the end position will be measured against (SeeFig. 7). Note that Neutral 0 is optional as the computation ofjoint ROM for each of the activities do not require the initial

LEE et al.: SMARTPHONE-CENTRIC SYSTEM FOR THE RANGE OF MOTION ASSESSMENT IN STROKE PATIENTS 1843
Fig. 7. Neutral postures at start of assessment. Postures 1 and 2 differ in thepositions of the palms.
Fig. 8. Flowchart for activity detection. Neutral 0 is not explicitly checked.
angle to be known. However, adopting Neutral 0 at the begin-ning of an activity would still improve detection accuracy, asthe number of possible activities would be reduced. Note thatthe neutral positions adopted here are not the ones that are com-monly used in the FMA [5], [7]. These neutral positions wereadopted primarily to make it easier for us to measure the rangeof motion of different joints.
The logic used in activity detection is based on a set of experi-mentally derived thresholds, and guided by the patient’s postureat the start of the activity. Fig. 8 illustrates the logic flow. For ex-ample, a patient starting in neutral posture 2 who flexes his/herwrist downward would be recognized as performing the wrist-flexion assessment.
The algorithm has been kept intentionally simple consideringthe limited processing capability of mobile phones, althoughthe accuracy should improve with further refinement and betterhardware.
3) Operation: The smartphone has to enable WiFi hotspotmode to connect to the master node. The master node searchesfor the pre-defined SSID of the hotspot when turned on. Toestablish the connection, the user has to press the Connect buttonafter the application is launched [See Fig. 9(a)].
Fig. 9. Screenshots of User Interface. (a) Landing page. (b) Connected tomaster node. (c) During assessment. (d) Summary Table.
Before the assessment begins, the user has to enter the iden-tification of the patient. The user is then taken to the assessmentinterface once the ID is entered. Within the assessment interface,there is only a single toggle button to start and stop the activity.The subject should adopt the respective neutral posture beforethe start button is pressed. Automatic activity detection beginsonce the start button is pressed. Once the application recognizesthe activity, a ‘beep’ sound is played, while it continuously cal-culates the respective joint angle [see Fig. 9(c)]. When the samebutton is depressed again to stop the activity, the maximum jointangle is recorded. The application is capable of recognizing twodifferent activities simultaneously, one on each side of the body.A checklist of measurements is presented in between activi-ties to indicate to the therapists which measurements have beenperformed [see Fig. 9(d)].
Although much effort has been invested to ensure that the ac-tivity detection algorithm identifies the correct activity, theremay be instances when the subject may not be capable ofadopting the right neutral posture, or when the subject is notcapable of moving enough to trigger the detection. In such sit-uations, a manual override can be invoked by tapping on thename of the activity. The user will then be presented with a listof activities to choose from.
1844 IEEE JOURNAL OF BIOMEDICAL AND HEALTH INFORMATICS, VOL. 18, NO. 6, NOVEMBER 2014
TABLE IIACTIVITIES AND THEIR RESPECTIVE NEUTRAL POSTURES
III. DATA COLLECTION
A. Methodology
A preliminary study was conducted, where the system wastested on five subjects undergoing rehabilitation at AMKH (2males and 3 females, mean age of 68 years). All participantswere newly disabled in-patients (less than 3 months) undergoingrehabilitation for a wide variety of diagnoses. Research ethicsapproval was obtained from the NUS Institutional Review Board(Reference Code 11-013 and Approval Number NUS-1270). Allsubjects provided informed consent, and participation was vol-untary. The purpose of the study was to determine the agreementbetween existing goniometric measurements and measurementsby the system. Feedback on the usability of the system was alsogathered from therapists and patients during the study.
Two therapists, each with more than ten years of experi-ence in neuro-rehabilitation of stroke patients were recruitedto perform manual measurements using goniometers. The go-niometers used were from HighRes (Baseline©, ±1◦), as theseare the standard instruments used by the therapists. Maximualactive ROM measurements were taken when the subject wear-ing the sensor system has achieved the maximal excursion ofa particular movement in a specific joint by a therapist follow-ing protocols described by Clarkson [28]. The equivalent anglemeasured by the sensor was recorded by an independent engi-neering research assistant.
A typical assessment consists of the 12 activities listed inTable II . The activities were performed sequentially, whilethe order of the activities were not fixed. Each subject wassubjected to two consecutive assessments on the same day, eachtime by a different therapist, but with minimal change in nodeplacement between the assessments. The therapists performedthe measurements independently. Only one set of measurementswas taken per activity per therapist, as it was too tiring forthe patient to perform repeated assessments. The correlationcoefficient between the values obtained by our system and thetherapists were computed to quantify the similarity between thetwo measurements.
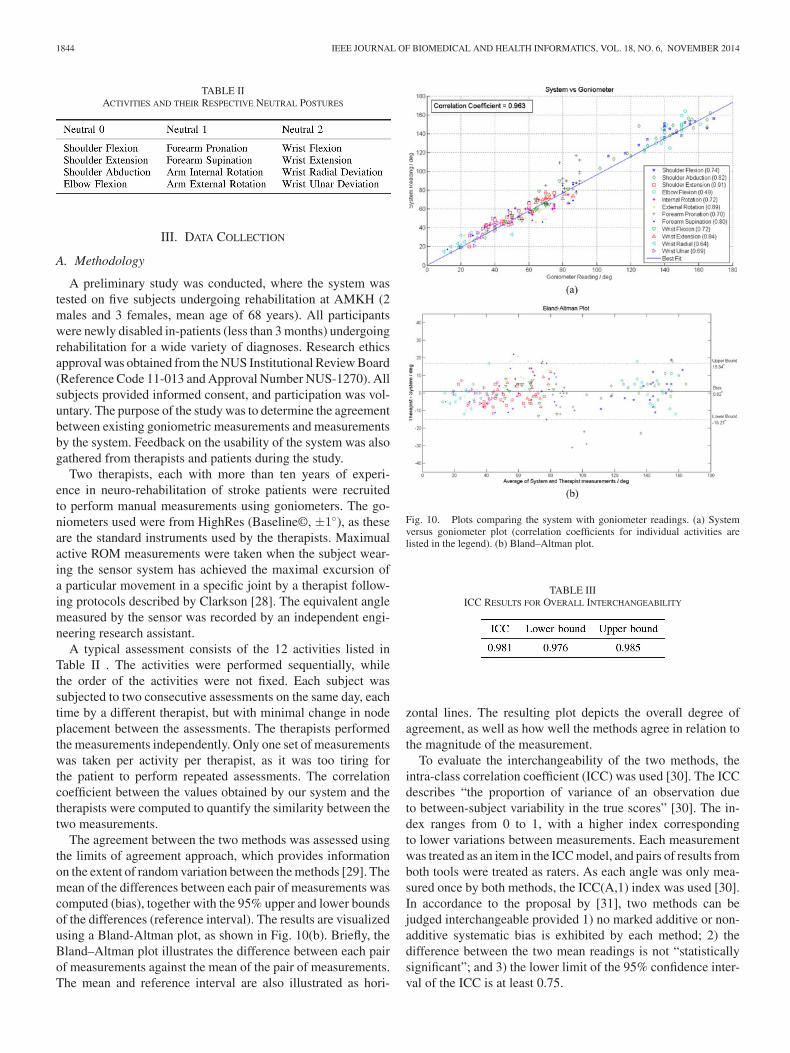
The agreement between the two methods was assessed usingthe limits of agreement approach, which provides informationon the extent of random variation between the methods [29]. Themean of the differences between each pair of measurements wascomputed (bias), together with the 95% upper and lower boundsof the differences (reference interval). The results are visualizedusing a Bland-Altman plot, as shown in Fig. 10(b). Briefly, theBland–Altman plot illustrates the difference between each pairof measurements against the mean of the pair of measurements.The mean and reference interval are also illustrated as hori-
Fig. 10. Plots comparing the system with goniometer readings. (a) Systemversus goniometer plot (correlation coefficients for individual activities arelisted in the legend). (b) Bland–Altman plot.
TABLE IIIICC RESULTS FOR OVERALL INTERCHANGEABILITY
zontal lines. The resulting plot depicts the overall degree ofagreement, as well as how well the methods agree in relation tothe magnitude of the measurement.
To evaluate the interchangeability of the two methods, theintra-class correlation coefficient (ICC) was used [30]. The ICCdescribes “the proportion of variance of an observation dueto between-subject variability in the true scores” [30]. The in-dex ranges from 0 to 1, with a higher index correspondingto lower variations between measurements. Each measurementwas treated as an item in the ICC model, and pairs of results fromboth tools were treated as raters. As each angle was only mea-sured once by both methods, the ICC(A,1) index was used [30].In accordance to the proposal by [31], two methods can bejudged interchangeable provided 1) no marked additive or non-additive systematic bias is exhibited by each method; 2) thedifference between the two mean readings is not “statisticallysignificant”; and 3) the lower limit of the 95% confidence inter-val of the ICC is at least 0.75.

LEE et al.: SMARTPHONE-CENTRIC SYSTEM FOR THE RANGE OF MOTION ASSESSMENT IN STROKE PATIENTS 1845
TABLE IVBA PLOT STATISTICS FOR EACH OF THE ACTIVITIES PERFORMED BY THE TWO THERAPISTS
B. Results
The data collected during our study are shown in Fig. 10(a).Each data point indicates a measurement that was collectedsimultaneously by our system and by one of the therapists.Overall, we found the correlation coefficient between the twomeasurements to be 0.963, with individual activities exhibitingcorrelation coefficients that ranged from 0.49 (for elbow flexion)to 0.91 (for shoulder extension). This showed that the measure-ments provided by our system were similar to those obtained bytherapists, but could be obtained much more easily and quickly.
The Bland–Altman plot is shown in Fig. 10(b). We foundthe mean difference between the two methods to be 0.82◦, sug-gesting that there was minimal bias between the methods. The95% reference interval was from −15.21◦ to 16.84◦, which rep-resented the extent to which the methods differed. This wasnot unexpected as goniometry is known to have a reliability of±10◦ [32].
The ICC for the two methods was computed to be 0.981,with the lower bound of the 95% confidence interval at 0.976.This demonstrates strong interchangeability, as it far exceedsthe criteria of 0.75 set by Lee et al. in [31].
Breaking down the results into individual activities yieldedmixed results (see Table IV). It is apparent that activities suchas shoulder flexion, shoulder abduction, internal rotation of thearm, elbow flexion, and forearm pronation all exhibited sig-nificant differences in biases between the two therapists. Asthe nodes were not shifted between the two readings taken bythe therapists, the difference in bias may be considered as asign of intertherapist inconsistency. This is not surprising, asresearch has shown that in the absence of standardized mea-surement procedures, interrater reliability for goniometry tendsto be poor [33], [34]. However, this is not enough to concludethat the proposed system is more precise, since no replicatemeasurements were performed for each joint angle [35]. Thisis because it was not possible for patients to replicate the samejoint angle across assessments. In addition, there may have beensome errors introduced in the system’s readings as the strapsused to mount the nodes may not have been secure enough.For example, during activities such as elbow flexion or shoulderflexion, bulging of muscles or movement of clothing beneath
the straps can affect the alignment of the node on the limbs.Further improvement is hence required to minimize such errors.
As therapist and system measurements were taken from thesame assessments, we could not directly compare the amount oftime saved from using the system. Nevertheless, time taken foreach activity was logged by the system. On average, measure-ment of a single activity took 18 s by the therapist, while thesystem took only 2 s. This does not include the time needed toassist and guide the patient to perform the activities. A typicalcomplete assessment took 54 min on average. It should be notedthat the system is capable of recording from both sides simul-taneously, but this feature was not exploited in our experiment.Further time savings could potentially be achieved if that werethe case.
IV. DISCUSSION
As a proof of concept, the system has demonstrated the abil-ity of mobile platforms to perform real-time data acquisitionand interpretation, in the form of measuring joint angles anddetecting the type of activity. The system has also shown com-parable levels of accuracy in measuring a range of joint angleswhen compared to the goniometer. More importantly, the timerequired to conduct the assessment has been dramatically re-duced through the use of the system. However, to conclusivelyaccess accuracy and reproducibility of the devices, multiple setsof testing need to be done, and we are currently in the processof doing so.
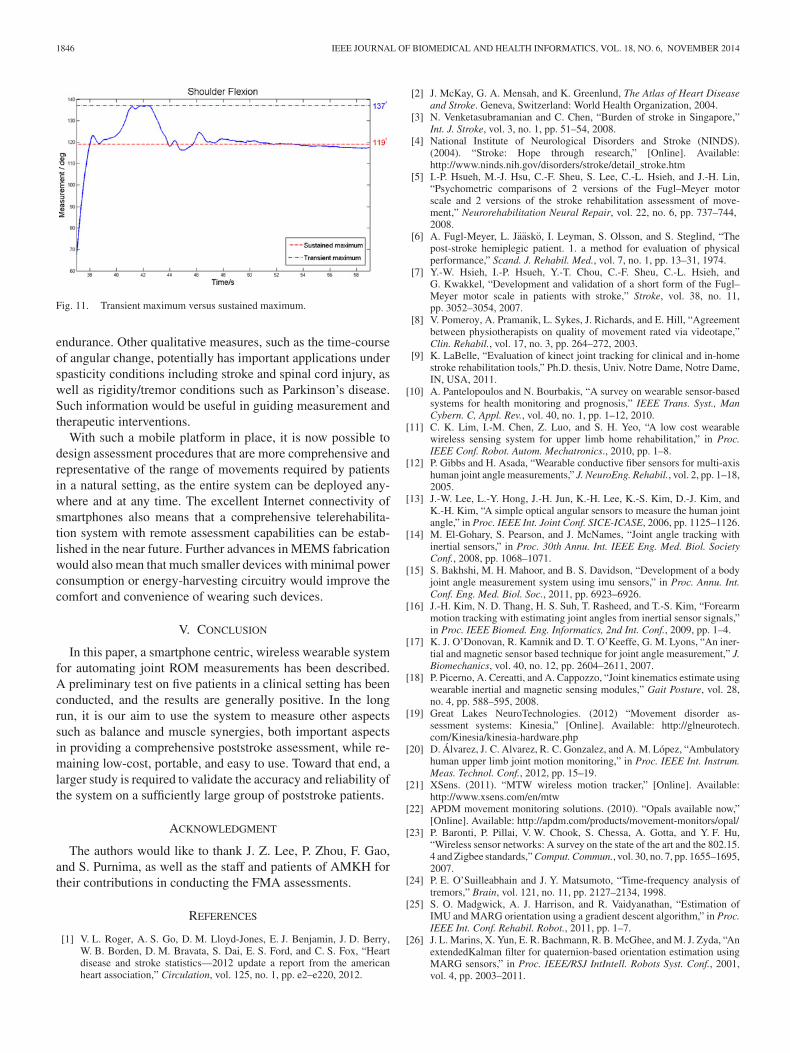
Due to the continuous nature of the data acquisition, the sys-tem is able to capture additional information not easily availablecurrently. For example, the system is able to capture transientmaximum joint angles, which are maximum joint angles that asubject can achieve, but is unable to sustain. Therapists, how-ever, can only measure sustained angles, as the subject needs tohold the angle for a period long enough for the measurement tobe taken. Fig. 11 illustrates one such situation.
Feedback from the clinicians was that the transient maximumangles are important, as they represent the actual maximumrange of motion of a joint. The period of time in which thesubject can hold a transient maximum is also a sign of muscle
1846 IEEE JOURNAL OF BIOMEDICAL AND HEALTH INFORMATICS, VOL. 18, NO. 6, NOVEMBER 2014
Fig. 11. Transient maximum versus sustained maximum.
endurance. Other qualitative measures, such as the time-courseof angular change, potentially has important applications underspasticity conditions including stroke and spinal cord injury, aswell as rigidity/tremor conditions such as Parkinson’s disease.Such information would be useful in guiding measurement andtherapeutic interventions.
With such a mobile platform in place, it is now possible todesign assessment procedures that are more comprehensive andrepresentative of the range of movements required by patientsin a natural setting, as the entire system can be deployed any-where and at any time. The excellent Internet connectivity ofsmartphones also means that a comprehensive telerehabilita-tion system with remote assessment capabilities can be estab-lished in the near future. Further advances in MEMS fabricationwould also mean that much smaller devices with minimal powerconsumption or energy-harvesting circuitry would improve thecomfort and convenience of wearing such devices.
V. CONCLUSION
In this paper, a smartphone centric, wireless wearable systemfor automating joint ROM measurements has been described.A preliminary test on five patients in a clinical setting has beenconducted, and the results are generally positive. In the longrun, it is our aim to use the system to measure other aspectssuch as balance and muscle synergies, both important aspectsin providing a comprehensive poststroke assessment, while re-maining low-cost, portable, and easy to use. Toward that end, alarger study is required to validate the accuracy and reliability ofthe system on a sufficiently large group of poststroke patients.
ACKNOWLEDGMENT
The authors would like to thank J. Z. Lee, P. Zhou, F. Gao,and S. Purnima, as well as the staff and patients of AMKH fortheir contributions in conducting the FMA assessments.
REFERENCES
[1] V. L. Roger, A. S. Go, D. M. Lloyd-Jones, E. J. Benjamin, J. D. Berry,W. B. Borden, D. M. Bravata, S. Dai, E. S. Ford, and C. S. Fox, “Heartdisease and stroke statistics—2012 update a report from the americanheart association,” Circulation, vol. 125, no. 1, pp. e2–e220, 2012.
[2] J. McKay, G. A. Mensah, and K. Greenlund, The Atlas of Heart Diseaseand Stroke. Geneva, Switzerland: World Health Organization, 2004.
[3] N. Venketasubramanian and C. Chen, “Burden of stroke in Singapore,”Int. J. Stroke, vol. 3, no. 1, pp. 51–54, 2008.
[4] National Institute of Neurological Disorders and Stroke (NINDS).(2004). “Stroke: Hope through research,” [Online]. Available:http://www.ninds.nih.gov/disorders/stroke/detail_stroke.htm
[5] I.-P. Hsueh, M.-J. Hsu, C.-F. Sheu, S. Lee, C.-L. Hsieh, and J.-H. Lin,“Psychometric comparisons of 2 versions of the Fugl–Meyer motorscale and 2 versions of the stroke rehabilitation assessment of move-ment,” Neurorehabilitation Neural Repair, vol. 22, no. 6, pp. 737–744,2008.
[6] A. Fugl-Meyer, L. Jaasko, I. Leyman, S. Olsson, and S. Steglind, “Thepost-stroke hemiplegic patient. 1. a method for evaluation of physicalperformance,” Scand. J. Rehabil. Med., vol. 7, no. 1, pp. 13–31, 1974.
[7] Y.-W. Hsieh, I.-P. Hsueh, Y.-T. Chou, C.-F. Sheu, C.-L. Hsieh, andG. Kwakkel, “Development and validation of a short form of the Fugl–Meyer motor scale in patients with stroke,” Stroke, vol. 38, no. 11,pp. 3052–3054, 2007.
[8] V. Pomeroy, A. Pramanik, L. Sykes, J. Richards, and E. Hill, “Agreementbetween physiotherapists on quality of movement rated via videotape,”Clin. Rehabil., vol. 17, no. 3, pp. 264–272, 2003.
[9] K. LaBelle, “Evaluation of kinect joint tracking for clinical and in-homestroke rehabilitation tools,” Ph.D. thesis, Univ. Notre Dame, Notre Dame,IN, USA, 2011.
[10] A. Pantelopoulos and N. Bourbakis, “A survey on wearable sensor-basedsystems for health monitoring and prognosis,” IEEE Trans. Syst., ManCybern. C, Appl. Rev., vol. 40, no. 1, pp. 1–12, 2010.
[11] C. K. Lim, I.-M. Chen, Z. Luo, and S. H. Yeo, “A low cost wearablewireless sensing system for upper limb home rehabilitation,” in Proc.IEEE Conf. Robot. Autom. Mechatronics., 2010, pp. 1–8.
[12] P. Gibbs and H. Asada, “Wearable conductive fiber sensors for multi-axishuman joint angle measurements,” J. NeuroEng. Rehabil., vol. 2, pp. 1–18,2005.
[13] J.-W. Lee, L.-Y. Hong, J.-H. Jun, K.-H. Lee, K.-S. Kim, D.-J. Kim, andK.-H. Kim, “A simple optical angular sensors to measure the human jointangle,” in Proc. IEEE Int. Joint Conf. SICE-ICASE, 2006, pp. 1125–1126.
[14] M. El-Gohary, S. Pearson, and J. McNames, “Joint angle tracking withinertial sensors,” in Proc. 30th Annu. Int. IEEE Eng. Med. Biol. SocietyConf., 2008, pp. 1068–1071.
[15] S. Bakhshi, M. H. Mahoor, and B. S. Davidson, “Development of a bodyjoint angle measurement system using imu sensors,” in Proc. Annu. Int.Conf. Eng. Med. Biol. Soc., 2011, pp. 6923–6926.
[16] J.-H. Kim, N. D. Thang, H. S. Suh, T. Rasheed, and T.-S. Kim, “Forearmmotion tracking with estimating joint angles from inertial sensor signals,”in Proc. IEEE Biomed. Eng. Informatics, 2nd Int. Conf., 2009, pp. 1–4.
[17] K. J. O’Donovan, R. Kamnik and D. T. O’Keeffe, G. M. Lyons, “An iner-tial and magnetic sensor based technique for joint angle measurement,” J.Biomechanics, vol. 40, no. 12, pp. 2604–2611, 2007.
[18] P. Picerno, A. Cereatti, and A. Cappozzo, “Joint kinematics estimate usingwearable inertial and magnetic sensing modules,” Gait Posture, vol. 28,no. 4, pp. 588–595, 2008.
[19] Great Lakes NeuroTechnologies. (2012) “Movement disorder as-sessment systems: Kinesia,” [Online]. Available: http://glneurotech.com/Kinesia/kinesia-hardware.php
[20] D. Alvarez, J. C. Alvarez, R. C. Gonzalez, and A. M. Lopez, “Ambulatoryhuman upper limb joint motion monitoring,” in Proc. IEEE Int. Instrum.Meas. Technol. Conf., 2012, pp. 15–19.
[21] XSens. (2011). “MTW wireless motion tracker,” [Online]. Available:http://www.xsens.com/en/mtw
[22] APDM movement monitoring solutions. (2010). “Opals available now,”[Online]. Available: http://apdm.com/products/movement-monitors/opal/
[23] P. Baronti, P. Pillai, V. W. Chook, S. Chessa, A. Gotta, and Y. F. Hu,“Wireless sensor networks: A survey on the state of the art and the 802.15.4 and Zigbee standards,” Comput. Commun., vol. 30, no. 7, pp. 1655–1695,2007.
[24] P. E. O’Suilleabhain and J. Y. Matsumoto, “Time-frequency analysis oftremors,” Brain, vol. 121, no. 11, pp. 2127–2134, 1998.
[25] S. O. Madgwick, A. J. Harrison, and R. Vaidyanathan, “Estimation ofIMU and MARG orientation using a gradient descent algorithm,” in Proc.IEEE Int. Conf. Rehabil. Robot., 2011, pp. 1–7.
[26] J. L. Marins, X. Yun, E. R. Bachmann, R. B. McGhee, and M. J. Zyda, “AnextendedKalman filter for quaternion-based orientation estimation usingMARG sensors,” in Proc. IEEE/RSJ IntIntell. Robots Syst. Conf., 2001,vol. 4, pp. 2003–2011.
LEE et al.: SMARTPHONE-CENTRIC SYSTEM FOR THE RANGE OF MOTION ASSESSMENT IN STROKE PATIENTS 1847
[27] E. Pervin and J. Webb, Quaternions in Computer Vision and Robotics.Defense Technical Information Center, Pittsburgh, PA, USA: Departmentof Computer Science, Carnegie-Mellon University, 1982.
[28] H. M. Clarkson, Musculoskeletal Assessment: Joint Range of Motion andManual Muscle Strength. Baltimore, MD, USA: Williams & Wilkins,2000.
[29] J. M. Bland and D. G. Altman, “Statistical methods for assessing agree-ment between two methods of clinical measurement,” Int. J. NursingStudies, vol. 47, no. 8, pp. 931–936, 2010.
[30] K. McGraw and S. Wong, “Forming inferences about some intraclasscorrelation coefficients,” Psychological Methods, vol. 1, no. 1, pp. 30–46,1996.
[31] J. Lee, D. Koh, and C. Ong, “Statistical evaluation of agreement betweentwo methods for measuring a quantitative variable,” Comput. Biol. Med.,vol. 19, no. 1, pp. 61–70, 1989.
[32] A. D. Armstrong, J. C. MacDermid, S. Chinchalkar, R. S. Stevens, andG. J. King, “Reliability of range-of-motion measurement in the elbow andforearm,” J. Shoulder Elbow Surg., vol. 7, no. 6, pp. 573–580, 1998.
[33] D. L. Riddle, J. M. Rothstein, and R. L. Lamb, “Goniometric reliabilityin a clinical setting shoulder measurements,” Physical Therapy, vol. 67,no. 5, pp. 668–673, 1987.
[34] R. Gajdosik, “Comparison and reliability of three goniometric methodsfor measuring forearm supination and pronation,” Perceptual Motor Skills,vol. 93, no. 2, pp. 353–355, 2001.
[35] B. Carstensen, Comparing Clinical Meas. Methods: A Practical Guideser. Statistics in Practice. Hoboken, NJ, USA: Wiley, 2010.
Wang Wei Lee received the the B.Eng degree (withthe First Class Hons.) in computer engineering fromthe Department Electrical and Computer Engineerin,National University of Singapore, in 2012, where heis currently working toward the Ph.D. degree underthe supervision of Prof. N. Thakor, Dr. Y. Shih-Chengand Dr. Y. Haoyong.
His current research interests include Neuromor-phic Tactile Sensing and its applications.
Shih-Cheng Yen received the B.S.E. and M.S.E. in1993, and the Ph.D. in 1998, all from the Depart-ment of Bioengineering, University of Pennsylvania,Philadelphia, PA, USA.
He is currently an Assistant Professor in the De-partment of Electrical and Computer Engineering,National University of Singapore, and also servesas the Deputy Director of the Singapore Institute ofNeurotechnology (SINAPSE). His research focuseson the neural coding, neuroprostheses, and neuro-therapeutic devices.
Arthur Tay received the B.Eng. and Ph.D. degreesin electrical engineering from the National Universityof Singapore, Singapore, in 1995 and 1998, respec-tively.
He is currently an Associate Professor with theDepartment of Electrical and Computer Engineering,National University of Singapore, Singapore. His re-search interests include applications of mathematicalsystem science tools in biomedical engineering, semi-conductor manufacturing, and process control.
Ziyi Zhao, photograph and biography not available at the time of publication.
Tim Ma Xu graduated from Nanyang Polytechnic in2000. He completed Bachelor in Sciences (Occupa-tional Therapy) at Curtin University of Technology,Australia, in 2005 and Master of Occupational Ther-apy degree from La Trobe University, Australia, in2008.
He is currently the Operations Manager and Prin-cipal Occupational Therapist at the THK TherapyServices, Thye Hua Kwan Moral Charities.
Karen Koh Mui Ling received the Bachelor’s degreein health sciences (Physiotherapy) from The Univer-sity of Sydney, Sydney, Australia, in 1999.
She is currently a Research Coordinator at the SawSwee Hock School of Public Health, National Uni-versity of Singapore. Her research interests includerehabilitation.
Yee-Sien Ng received the Bachelor of Medicine andSurgery from the National University of Singaporeand completed a Fellowship in Neuro-rehabilitationfrom Harvard Medical School.
He is currently the Head and Senior Consultantof the Department of Rehabilitation Medicine at theSingapore General Hospital in Singapore. He is alsoa member of the Royal Colleges of Physicians in theU.K. His main research interests are in neurorehabil-itation, spasticity, rehabilitation engineering, and theepidemiology of disability.
Effie Chew completed her medical degree at theUniversity of Melbourne, Australia and advancedspecialist training in Rehabilitation Medicine inSingapore.
She obtained her fellowship in neurorehabilitationat Spaulding Rehabilitation Hospital, Department ofPhysical Medicine and Rehabilitation, Harvard Med-ical School. She is currently a Consultant in Reha-bilitation Medicine, Division of Neurology, Univer-sity Medicine Cluster, National University Hospital(NUH).
Angela Lou Kuen Cheong received the Bachelor’sdegree in helath sciences (Nursing) from The Uni-versity of Sydney, Darlington, N.S.W., Australia, in2009.
She is currently a Research Assistant at the SawSwee Hock School of Public Health, National Uni-versity Health System, National University of Singa-pore, Singapore. Her research interests include strokeand geriatric rehabilitation.
Gerald Koh Choon Huat received the Master’s de-gree in family medicine in 2000, the Master’s de-gree in gerontology and geriatrics from the Euro-pean Institute of Gerontology, University of Malta,Msida, Malta, in 2009, and the Ph.D. degree in familymedicine from Western University, Canada, in 2012.
He is currently an Associate Professor and Direc-tor of Medical Undergraduate Education at Saw SweeHock School of Public Health. His current researchinterests include stroke and geriatric rehabilitation,and medical education.





























