Embed Size (px)
Citation preview

distinguish between types of penetrating injuries, that is, stabbing ver-sus gunshot, which are known to have disparate outcomes. TRISSunderestimates survival in the lowest predicted survival groupbecause it is based on the ISS. TRISS methodology is currently advo-cated as the standard for benchmarking performance in the UnitedStates, and is widely accepted in many parts of the world. ExistingTRISS coefficients are based on MTOS data that are nearly 20 yearsold, taken from U.S. trauma centers with a high percentage of pene-trating trauma, and thus may not be applicable to foreign trauma cen-ters and too outdated for current trauma systems. TRISS coefficientscan be updated to reflect local databases, which should improve itspredictive properties.
A Severity Characterization of Trauma
To overcome the outcome limitations of TRISS, Champion and theAmerican College of Surgeons Committee on Trauma proposedASCOT, which uses AIS descriptors, physiologic data, mechanism,and age. ASCOT incorporates all severe patient injuries in the predic-tion model via the AP, in contrast to TRISS, which considers only ISSinjuries. ASCOT proved to be equivalent or better than TRISS in moststudies, particularly penetrating trauma, but failed to be widelyaccepted, most likely because of the complex computations involvedin deriving the score. Like TRISS, the coefficients for ASCOT arebased on theMTOS, which is biased toward severely injured and pen-etrating trauma patients.
Risk-adjustment models like TRISS and ASCOT allow outcomesfrom different institutions to be adjusted for differences in injuryseverity, making it possible to compare hospital quality. Inaccuraterisk adjustment may lead to some high-quality hospitals being misla-beled as poor quality and vice versa. However, a study comparingTRISS and ASCOT for identifying high-quality hospitals disagreedon the status of 35 of 69 hospitals studied. A second study comparingtrauma centers using TRISS found an unacceptably high misclassifi-cation rate in patients with severe trauma, further supporting the con-clusion that currently these tools are unable to accurately providebenchmarking for quality improvement. The addition of comorbidconditions was recently shown to improve TRISS performance forprediction of survival.
Mechanism of Injury
The mechanism of injury, particularly blunt versus penetrating, isknown to influence mortality. AIS, TRISS, and ASCOT all accountfor blunt and penetrating trauma in their methodology. More detaileddata on mechanism of injury are collected by trauma registries or asexternal cause of injury codes (E-codes). E-codes refer to a supple-mental code used to provide additional detail to injury ICD-9-CMcodes within the range 800–999. Cause codes allow for the identifica-tion of excess morbidity and mortality rates associated with specificinjury mechanisms for injury prevention programs.
SCORING SYSTEMS EVALUATION
Data Collection
The survival probability model is the most popular tool for evaluatingtrauma care. Current models are based on linear logistic regressionanalysis of patient variables to identify those independently associatedwith mortality. Formulas are then derived to predict the probability ofsurvival using weighted coefficients according to the effect of the var-iable on mortality. To be statistically sound, this multivariate analysisrequires large databases of trauma patients. These databases mustinclude data on a large number of variables, including patient
demographics, comorbid conditions, injury type and severity, mech-anism of injury, prehospital care, ED care, in-hospital care, and post-discharge follow-up. Complete and accurate data gathering into adatabase is dependent on operator input and data availability. Missingdata are a particular problem with multivariate analysis, as often theentire patient record containing the missing piece of data must bediscarded.
Databases
Trauma scores are derived from several types of databases: hospitaladministrative databases, trauma registries, and the NTDB. Admin-istrative databases are derived from ICD-9-CM hospital dischargedata that were collected for billing purposes. They reflect the codingconventions of the institutions from which they were derived, andmay be affected by reimbursement considerations. Furthermore, onlythe most significant injuries may be coded. Administrative databasessuffer from significant gaps in data, lacking such details as prehospitaland ED care, physiologic data, and postdischarge follow-up. Traumaregistries are designed to have no such gaps, capturing all phases oftrauma care, but require dedicated personnel to administer. Traumaregistries vary from hospital to hospital, mostly in the manner inwhich AIS and ISS scores are coded, which render comparisonsbetween them difficult or even invalid.
The NTDB functions as a national repository of trauma data to beused for epidemiology, injury prevention, clinical research, education,and resource allocation. The NTDB voluntarily collects data from 565U.S. hospitals, including 70% of the Level I trauma centers and 50% ofthe Level II trauma centers. It has a standardized data entry formatthat can be hand entered or automatically derived from existingtrauma registry data. The NTDB collects data on a large number ofvariables felt to potentially impact quality of care, in addition topatient demographics, complications, diagnosis, TRISS/ISS scores,and outcomes. It also documents the methodology used to determineAIS, ISS, and TRISS scores and diagnosis. The NTDB was created in1989 by the American College of Surgeons, and participation bytrauma centers has increased substantially in the past few years.The NTDB is nonproprietary, and its reports are available at nocharge with a benchmark report for quality improvement processesprovided annually to each participating hospital.
Outcome Measures
The most common outcome measured by trauma scores is mortality.The time frame for inclusion of mortality is not uniformly defined;thus, data on all fatalities may not be captured. Fatality after injurymay be variously defined as prehospital, in-hospital, 30- or 60-daypostinjury, or all injury-related postdischarge fatalities identified,regardless of time period. For example, elderly patients are less ableto survive mild to moderate injuries, and more likely to die of compli-cations several weeks or months after the incident. Such patients wouldnot meet the fatality inclusion criteria of in-hospital or 30-day fatalitydefinition. Postdischarge fatality is not captured by administrativedatabases, and is only sporadically captured by trauma registries. Esti-mates of injury fatality substantially increase when usingmultiple inde-pendent databases to capture postdischarge fatalities.
Prehospital deaths are not captured by trauma registries or admin-istrative databases, but may affect mortality predictions for manyinjuries. Due to improved emergency medical services, patients suf-fering fatal injuries, who previously would have died, now make itto the hospital only to die soon after arrival. In-hospital fatality is alsoaffected by withdrawal of care practices. Hospitals with more liberalpolicies for withdrawal of care during the in-hospital period willreport artificially higher in-hospital mortality rates. Lower in-hospitalmortality rates will be reported by hospitals whose policy is to transferearly significantly disabled trauma patients to skilled nursing
6.e23TRAUMA SCORING

facilities. Withdrawal of care is usually documented in trauma regis-tries but not in administrative databases.
Injury outcome is dependent on which outcome is measured, andmay be impacted by factors not related to quality. Type of injury, age,and comorbid conditions affect various outcomes differently. Forexample, aortic injuries have a high mortality rate but low disabilityrate, compared with head injuries, which have moderate mortality rateand high disability rate. Young patients with head injuries have less dis-ability and lower mortality rates than elderly patients. Trauma patientswith significant comorbid conditions are more likely to have compli-cations. For example, diabetics are more likely to develop infections,obese patients are more likely to develop organ failure, and patientswith significant aortic stenosis have increased risk of death after injury.The reported intensive care unit or hospital length of stay can beimpacted by availability of ward beds or skilled nursing beds, and delayin discharge may be related to transportation and patient or familyissues. Length of stay is increased in elderly patients and those with sig-nificant comorbid conditions. Length of stay is shorter when patientsdie early in their hospitalization, and these patients should be excludedfrom length-of-stay analysis. Trauma registries perform better thanadministrative databases for analyzing these situations.
Disability is a significant problem in trauma patients, and is animportant outcome measure for quality improvement processes.The Functional Capacity Index (FCI), Glasgow Outcome Scale score,and modified Functional Independence Measure are all measures offunctional impairment used in trauma research. The predicted FCI(pFCI12), which predicts functional capacity 12 months after injury,is matched to descriptors in AIS-90 and measures the impact of inju-ries on function at 1 year. The original pFCI12 did not discriminatewell, and a consensus group was convened to address these issues.Those changes are currently being validated in the new version ofAIS 2005. Hopefully, the pFCI12 and other measures of functionalimpairment will prove useful in trauma research and quality improve-ment processes in the future.
SUMMARY
Trauma scoring systems are tools for ranking injury severity to allowrisk adjustment for comparative analysis. The ideal trauma scoringsystem would accurately predict risk of death or functional disability,and would provide a standard by which performance could be bench-marked for quality improvement processes.
Currently, there are no trauma scoring systems capable of fullysupporting the quality improvement process because they fail toassess risk accurately enough to detect quality differences.
The AIS remains the foundation of most trauma scoring systems.Its widespread use in both the health care and transportation safetyindustries for injury description ensures its continued use. Further-
more, the availability of ICD mapping software and improved ICDinjury descriptors will allow expanded use of the AIS by abstractionfrom nontrauma administrative databases. ISS score functions well asa predictor of fatality, despite its statistical limitations. It will continueto find use in risk stratification of patients as a stand-alone function oras part of TRISS for trauma program quality improvement. Fatality,however, is best predicted by ICISS SSRs derived from comparabledatabases. Furthermore, in most patients, the single worst injury pre-dicts fatality the best.
Trauma scoring systems that only consider injury severity are use-ful, but insufficient, for risk adjustment. It is not known which patientvariables, in addition to injury severity, contribute most to accuraterisk assessment. These variables are likely to differ depending onthe outcome of interest. The design and validation of trauma scoringsystems that can perform accurate risk adjustment will require accessto large databases containing these variables of interest. These data arenot available in administrative databases and are best capturedthrough trauma databases. The NTDB fulfills that role in the UnitedStates. Data collection for the NTDB is dependent on trauma regis-tries. To maximize accurate and complete data acquisition, an effortshould be made to upgrade all trauma registries to a minimum stan-dard including the following:
n Automatic data transfer to the NTDBn Use of the latest version of AIS or ICD injury descriptorsn Accurate mapping software to convert ICD to AISn A method by which older data can be upgraded into the new
systemn Well-defined quality outcome measures
Standardization would also allow trauma registry data to be easilymeshed with other relevant databases for injury research, treatment,and prevention.
The ultimate goal of risk adjustment for quality improvement is toseparate outcomes due to patient injury and reserve from issues ofpatient care. Trauma scoring systemsmust be developed that can sup-port accurate risk adjustment, a vital component to continual qualityimprovement in trauma care.
S U G G E S T E D R E A D I N G S
Baker SP, O’Neill B, HaddonW, LongWB: The injury severity score: a methodfor describing patients with multiple injuries and evaluating emergencycare. J Trauma 14:167–196, 1974.
Champion HR, Copes WS, Sacco WJ, et al: The Major Trauma OutcomeStudy: establishing national norms for trauma care. J Trauma30:1356–1365, 1990.
Meredith JW, Kilgo PD, Osler TM: Independently derived survival risk ratiosyield better estimates of survival than traditional survival risk ratios whenusing the ICISS. J Trauma 55:933–938, 2003.
6.e24 TRAUMA SCORING

RESULTS OF THE MEDICAL
STRATEGY FOR MILITARY
TRAUMA IN COLOMBIA
William Sánchez Maldonado, Erwin Rodriguez-García,David Rojas Tirado, and Juan A. Asensio
T hroughout history, wars have resulted in the development ofmedical and surgical techniques for the care of the wounded
that have been later adopted successfully in civilian trauma. Colombiahas faced more than 50 years of irregular armed conflict with theresult of multiple experiences gained, particularly regarding the man-agement of complex trauma. We present our care plan in militarytrauma and our results of the project.
The impact on medical care of the many wounded from a long-standing irregular war with guerrillas, and more recently with drugdealers and criminal gangs, prompted the development of a medicalcare strategy designed to ensure fast, effective, and optimal treatmentwith the highest probability of survival of the wounded and a satisfac-tory rehabilitation.
The finding that fueled the strategic plan was an analysis conductedin early 2000 that revealed a worrying figure of 32% average immediatemortality rate in the battlefield, the absence of specialized medical careafter the traumatic event, and deficient medical transportation logisticswith long evacuation delays, but at the same time there was a higherprobability of survival (6% mortality rate) at the Hospital Militar Cen-tral, as a result of high-level specialized medical care.
The initial design of the strategy was developed by Lieutenant Col-onel Erwin Rodríguez García, MD, and Major David Rojas Tirado,MD, with the support of the U.S. Army Southern Command. The
plan received the name of PANTERA and was based on the modelby William Haddon, who described in New York in 1970 a matrixfor analyzing trauma care in which the injury-promoting factors wereinterrelated—human, environmental, and technical—in each of thethree possible phases of the event—before, during, and after trauma.After 1 year of strategic planning, the PANTERA project was imple-mented in February 2004 with the participation of multiple playersfrom the administrative, military, training, and medical areas. Eightyears later, it is still active.
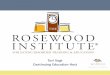
Seven consecutive steps are described in the planning and actionflowchart (Fig. 1).
KNOWING THE PRIMARY ENEMY
The main characteristic of the primary enemy (guerrillas, drug traf-fickers, and criminal gangs) is lack of respect for the principles ofinternational humanitarian law in their criminal warfare:
1. Many of their combatants are children who are drafted by forceand who suffer from profound psychological disorders as aresult of their abnormal development amidst violence duringtheir childhood and adolescence, further aggravated by socialrejection.
2. The use of nonconventional elements of war is also character-istic, including land mines, biologic contamination of weapons,and nontraditional explosives.
3. The use of extortion, kidnapping, and torture as social intim-idation maneuvers is also characteristic.
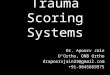
Consequently, the military actions of the primary enemy areinsane by nature and the secondary wounds resulting from this irreg-ular warfare are usually high-energy injuries with great tissue destruc-tion, a high proportion of limb amputation and dismemberment, andhigh levels of contamination (Fig. 2).Therefore, medical care must beplanned around critically injured patients with considerable traumaand a high probability of morbidity and mortality.
Rehabilitation
Remotecare
Secondarycare
Primarycare
Strategy plan
Knowsecondary enemy
Knowprimary enemy
Strategy Evolution & Military Trauma Colombia
MultidisciplinaryPermanent Evaluation
“Preserve and Functional Life”
FIGURE 1 Military medical care plan.
7TRAUMA SYSTEMS

KNOWING THE SECONDARY ENEMY
Immediately after the attack, the enemy for the victims and the med-ical team changes, and bleeding and infection become the new foes.
After trauma in the battlefield or after military action, control ofacute bleeding becomes a priority in primary care. All measures ofmedical care must focus on controlling continuous persistent bleed-ing that may lead to shock and exsanguination. Our managementguidelines are based on five sequential components:
1. The first immediate step is an attempt at controlling local acutebleeding with external compression or a tourniquet in the caseof injured limbs. All military personnel are trained in first aid,and a team of medics is always present to provide support inevery military operation. In some critical situations, good med-ical judgment may lead to considering risking the viability of anextremity rather than risking the patient’s life.
2. The second step is the use of local hemostatic agents such asmatrices or thermal coagulants by the primary care team. Theseelements are always part of the first aid kit.
3. The third step is to secure venous access and initiate fluidresuscitation under a hypotensive technique, preferably withhypertonic solutions.
4. After evacuation, the patient is received at the combat hospital(GATRA), where whole blood transfusion is initiated, if neces-sary, always considering the possibility of autotransfusion, ifindicated.
5. Finally, we have developed for each military unit a database ofpotential, immediately available blood bank donors, and eachmedical support team must check the availability of blood ordonors for all soldiers going into action.
The second new enemy is infection. Our guidelines for the man-agement of war injury infections include the following:
1. Immediate irrigation and cleaning of the wound with salinesolution in the battlefield. This is done simultaneously withthe control of bleeding.
2. Coverage and isolation of the wound with aseptic dressings.Some rescue teams and all combat hospitals (GATRA) havenegative pressure VAC (vacuum-assisted closure) systems thatare very useful for the management of wounds with significanttissue losses, bearing in mind that the selection of foams and
pressure variables must be tailored to the needs of the individ-ual patient.
3. A golden rule for us is to consider that all war injuries are con-taminated or potentially infected. This consideration is basedon the observation of guerilla tactical operations (biologic con-tamination of weapons) and a prospective study that we con-ducted, which included 18,627 cultures in order to determinethe most frequent bacteria responsible for infections in ourpatients; The first was Escherichia coli (30%) followed by Staph-ylococcus aureus and Klebsiella pneumoniae. E. coli infectionaccounted for 50% of all gram-negative infections (Table 1).Consequently, antibiotic therapy is therapeutic and focusesmainly on the treatment of gram-negative infections.
Wounded Soldiers
FIGURE 2 Soldiers wounded in combat with amputations, burns, and severe soft tissue injury.
TABLE 1: Top Ten Microorganisms That CauseInfection in Hospital Militar Central, 2010–2012
Microorganism
NO. OF ISOLATES/YEAR
2012 2011 2010
Escherichia coli 1869 1769 1868
Staphylococcus aureus 352 340 434
Klebsiella pneumoniae 428 413 412
Staphylococcus epidermidis 274 271 378
Pseudomonas aeruginosa 212 262 319
Proteus mirabilis 253 296 303
Enterococcus faecalis 300 336 277
Candida albicans 142 165 171
Enterobacter cloacae 142 165 151
Serratia marcesens 84 108 116
From Hospital Militar Central, Bogota.
8 RESULTS OF THE MEDICAL STRATEGY FOR MILITARY TRAUMA IN COLOMBIA

STRATEGIC PLAN FOR MEDICAL CARE
Our medical care plan was named PANTERA and it was built aroundlevels and types of care teams (Fig. 3):
Level I: This team is called EMEREVAC in Spanish (Combat Res-cue and Evacuation Medical Team) and consists of one physi-cian, one licensed practical nurse, and two soldiers who areexperts in rescue. Themain goals of this team are to ensure sur-vival of the wounded in the battlefield by providing first aidsupport in the form of control of acute bleeding, infection pro-phylaxis, and immediate evacuation (Fig. 4).
Level II: This level comprises combat hospitals. It is calledGATRA in Spanish (Air-Transport Trauma Life SupportTeam) and consists of one general surgeon, one orthopedicsurgeon, one anesthetist, one medical assistant, one headnurse, one laboratory technician, and four licensed practicalnurses. This team receives the wounded from the EMEREVACwithin less than 1 hour and performs all the procedures nec-essary to resuscitate and stabilize them, including resuscitationand damage control surgery. If necessary, this team also initi-ates basic intensive care and prepares the patients for evacua-tion to a higher-complexity center in a condition that enablesthem to survive long distances and undergo major reconstruc-tive surgery. Patients must not remain in a GATRA unit formore than 6 hours (Fig. 5). Every combat hospital has thenumber of GATRA units that are required depending on theneeds of the military operation.
Level III: After receiving treatment in the combat hospital fordamage control, the wounded patient is transferred to the nextlevel, namely, the distant evacuation team behind the lines, inSpanish ECCAT (Air-Transport Critical Care Team). This
team’s mission is to transport the wounded in optimal condi-tions, maintaining hemodynamic stability. The basic teamconsists of a physician with training in critical care, a headnurse, and two licensed practical nurses. The number of teammembers grows depending on the number of victims thatrequire transportation, as is also the case with the type andnumber of aircraft (Fig. 6).
Level IV: The highest level of care is provided at the Hospital Mili-tar Central, a university institution equipped with high-technology infrastructure and wards dedicated only to thewounded in combat. All the hospital staff members, regardlessof their specialty, are trained in trauma and this multidisciplin-ary approach to care allows for comprehensive treatment,ranging from repair surgery to complete rehabilitation, includ-ing psychological rehabilitation. The university hospital pro-vides care to the wounded in a setting of continuing medicaleducation and research projects centered on the issue of wartrauma, using all the current teaching aids (basic and clinicalresearch, simulation, telemedicine, etc.). This ensures high-level training in trauma for the benefit of the patients.
Results of the Strategy
The PANTERA plan has made it possible to provide highly special-ized medical care from the very moment an event occurs and a soldieris wounded in action. An analysis of the warfare techniques used bythe irregular combatants between 2000 and 2005 revealed that 80% ofthe military casualties were wounded by large-caliber high-speed fire-arms, at a time when the war was fought with conventional weaponsand in direct confrontation. The warfare technique evolved to avoiddirect engagement, and by 2009–2010, 75% of the casualties were the
Military Medical Care Levels Panther Strategy
I LevelI LevelOperation fieldOperation field
EMEREVACEMEREVAC
Fly time (minutes)Fly time (minutes)
II LevelII LevelCombat hospitalCombat hospital
((�� 100 miles) 100 miles)
III LevelIII LevelECCAT (medical evacuation team)ECCAT (medical evacuation team)
IV LevelIV LevelMilitary hospitalMilitary hospital((�� 200 miles) 200 miles)
I LevelOperation field
EMEREVAC
Fly time (minutes)Miles 200 140 100 50 10
3 16 34 68
II LevelCombat hospital
(�100 miles)
III LevelECCAT (medical evacuation team)
IV LevelMilitary hospital(�200 miles)
FIGURE 3 Panther (PANTERA) strategy—three operation levels.
9TRAUMA SYSTEMS

EMEREVAC TEAM
Evacuation – Battlefield Team Level I
Grade Profile Number Training
TE–CT MD 1 ATL, Military hospital course
C3–SV Nurse 1 PHTLS, Military hospital course
SLP Paramedic 2CSAR
Rescue techniquesMilitary hospital course
FIGURE 4 EMEREVAC team (Combat Rescue and Evacuation Medical Team)—Level I.
GATRA TEAM
Grade Profile Number Training
CT–CR General surgeon 1 ATLS, Military hospital course
CT–CR Anestesiologic 1 ATLS, ACLS, Military hospital course
CT–CR Traumatologic 1 ATLS, Military hospital course
TN–CR MD (assistant) 1 ATLS, Military hospital course
ST–TC Nurse chief 1 PHTLS, Military hospital course
S3–SP Nurse crew 2 PHTLS, Military hospital course
C3–SP Nurse 3 PHTLS, Military hospital course
Combat Hospital Team – Level II
FIGURE 5 GATRA team (Air-Transport Trauma Life Support Team)—Level II.
10 RESULTS OF THE MEDICAL STRATEGY FOR MILITARY TRAUMA IN COLOMBIA

result of nonconventional explosives and land mines. This explainsthe change in the epidemiology of the wounds, with the emergenceof injuries with significant tissue loss, a high potential for infection,and a high rate of amputations and dismemberments.
The three primary causes of immediate fatality in the battlefieldwere chest wounds (34%), dismemberment caused by land mines(31%), and head injuries (17%). In medical prophylactic strategy,emphasis is placed on the use of bulletproof vests, helmets, and meansfor detecting and dismantling nonconventional explosives during theoperations. However, these measures are not easy to implement in thetropical jungle where the armed conflict takes place in Colombia.
The first important favorable result of this medical strategy wasreflected in the morale and patriotism of the soldiers who feel backedby a highly qualified medical rescue team that can ensure immediatecare and offer the highest probability of survival.
Between January 2005 and December 2010, 8631 Colombian sol-diers were wounded in action, and there were 2462 deaths in the field
of military operations (28.5%). Through their action, the EMERE-VAC and GATRA teams contributed to a significant reduction inmortality rate in the battlefield. In 2005, there were 531 deaths(35%) and this figure dropped to 425 (17%) in 2010 (Table 2). Train-ing of the military personnel in first aid and resuscitation, togetherwith the application of management guidelines for controlling acutebleeding and the use of prophylaxis for infection have been critical inimproving the probability of survival of wounded soldiers. Anotherfactor that has also contributed to these results is the support fromthe EMEREVAC team, with professional treatment, resuscitation,and evacuation within a period of time not greater than 1.30 hours,a critical determinant of patient survival.
Between January 1999 and December 2010, the Hospital MilitarCentral received 4233 critically injured (Injury Severity Score[ISS]>15) patients of a total of more than 15,000 wounded in action.The analysis of the data for three time periods of this special group ofpatients revealed that hospital mortality rate decreased progressively
ECCAT TEAM
Grade Profile Number Training
CT–CR Anestesiologic, critical care 1 ATLS, ACLS, Military hospital course
TN–CR MD (assistant) 1 ATLS, Military hospital course
C3–SP Nurse 1 PHTLS, Military hospital course
Medical Evacuation Team – Level III
FIGURE 6 ECCAT team (Air-Transport Critical Care Team)—Level III.
TABLE 2: Wounded in Combat in the Military Forces of Colombia, 2005–2010: Analysis of Mortality
2005 2006 2007 2008 2009 2010
Total wounded 1543 1538 1419 1248 1355 2500
No. surviving 1002 1080 1042 943 999 2075
No. deaths 541 (35%) 458 (30%) 377 (26%) 305 (24%) 356 (26%) 425 (17%)
Transferred to HMC 433 290 171 227 297 188
Mean age: 24 yearsTotal wounded in combat: 8631Deaths: 2462 (28.5%)Transferred to HMC, ISS > 15: 1606 (26.3%)
From Hospital Militar Central in Bogota.HMC, Hospital Militar Central; ISS, Injury Severity Score.
11TRAUMA SYSTEMS

from 5.2% to 2.3%. These results reflect the high degree of expertise inproviding care to trauma patients with a multidisciplinary approach,without forgetting the process of physical, psychological, and socialrehabilitation as a fundamental pillar of comprehensive patient care(Table 3).
Infection is the main cause of nonacute hospital morbidity andfatality of patients wounded in action, except for the immediatesequelae of exsanguination. At our institution, war injury–associatedinfections are caused mainly by gram-negative bacteria. E. coli is theprimary cause of infection globally (35%), requiring knowledge of thelocal biologic behavior of the microorganisms, in terms of antibiotic
resistance, in order to determine the best therapeutic selection. Inour prospective analysis for 2010–2012, which included 5506 patientswith positive cultures for E. coli, the percentage of resistance toampicillin/sulbactam, trimethoprim-sulfamethoxazole, and cipro-floxacin was 42.9%, 37.1%, 26%, respectively, which means that theselection of antibiotics has to exclude these options andmust be basedon the result of the sensitivity and bacterial resistance (Table 4).
The following are clinical examples of refined damage controltechniques in military trauma care:
1. Patient with penetrating thoracoabdominal gunshot woundthat injured the jejunum, colon, spleen, diaphragm, left lung,and the thoracic aorta. The GATRA team performed a resus-citation thoracotomy with cannulation of the right atrium inorder to recover intravascular volume and then repair the aortaand the lung injury, combined with laparotomy for damagecontrol of the abdominal injuries (Fig. 7).
TABLE 4: Analysis of Antibiotic Resistance in 5506Patients with Escherichia coli Infections, 2010–2012
AntibioticResistance Markers
RESISTANCE (%)
2010 2011 2012
No.UCI UCI
No.UCI UCI
No.UCI UCI
Amikacin 0.4 1.7 1.6 0.0 0.8 0.0
Ampicillin/sulbactam
31.2 44.8 35.7 41.0 27.6 42.9
Beta-lactamase(BLEE)
11.7 22.4 12.5 15.4 11.6 17.1
Cefoxitin (AmpCmarker)
3.2 0.0 4.8 5.1 4.2 8.6
Ciprofloxacin 22.9 29.3 30.6 23.1 27.8 25.7
Gentamicin 13.7 19 16.3 23.1 17.6 15.7
Imipenem 0.4 0.0 0.0 0.0 0.2 0.0
Piperacillin-tazobactam
10.5 24.1 11.3 15.4 6.5 12.9
TMP/SXZ(trimethoprim-sulfamethoxazole)
41.4 42.0 48.0 30.3 39.3 39.2
From Hospital Militar Central in Bogota.UCI, Urinary catheter infection.
TABLE 3: Hospital Militar Central War Trauma—Analysis of In-Hospital Mortality Rate of 4233 PatientsInjured in Combat Over Three Periods of Time
PeriodNo. ofPatients
No. ofDeaths
Mortality Rate(%)
1999–2003 1572 82 5.2
2004–2008 1531 49 3.4
2009–2010 1130 27 2.3
Global hospital mortality rate: 3.6%Total of 4233 patients, Injury Severity Score (ISS)>15
From Hospital Militar Central, Bogota.
FIGURE 7 Soldier wounded in combat, requiring thoracotomy andlaparotomy of damage control and cannulation of right atrium to replaceblood volume.
FIGURE 8 Soldier wounded in combat, requiring femoral arterialbypass as a temporary measure to allow the viability of lower limb.
12 RESULTS OF THE MEDICAL STRATEGY FOR MILITARY TRAUMA IN COLOMBIA

2. Patient injured by a grenade fragment in the right lower limbcausing femoral fracture and popliteal-femoral artery lesion.Acute bleeding was controlled by the combat nurse of theEMEREVAC team using local compression and a tourniquet.Later, in the rescue helicopter, the EMEREVAC physician per-formed an external vascular bypass, securing the viability of thelimb before final repair at the Hospital Militar Central (Fig. 8).
3. An additional example of multidisciplinary management usingmodern technologies is that of a patient wounded in action byan assault rifle grenade causing multiple severe injuries to theliver, right kidney, jejunum, colon, stomach, lung, and abdom-inal wall. The patient required multiple surgical interventionsand treatments by a multidisciplinary team, including VACtherapy, in order to save his life and promote his recovery(Fig. 9).
CONCLUSIONS
1. The strategy for developing the medical care plan for patientswounded in action must consider all possible variables toinclude in the Haddon matrix analysis.
2. The PANTERA plan, as a pillar of care in the Colombian armedforces, has been shown to be successful in improving the prob-ability of survival of war victims.
3. Every medical care plan for trauma and critically ill patients,and in particular in military medicine, must be based on strongcontinuing academic training and education of each and everyone of the team members.
For the chapter’s Suggested Readings list, please visit the book atwww.ExpertConsult.inkling.com.
Combat Wounded & VAC®
Liver, Kidney, Ileum, Colon, Stomach, Lung
FIGURE 9 Soldier wounded in combat, with injury of multiple intra-abdominal organs and abdominal wall.Sequence of treatment with VAC (vacuum-assisted closure) therapy.
13TRAUMA SYSTEMS